mucormycosis in a patient with acute myeloid leukemia successfully treated with liposomal...
TRANSCRIPT
Mucormycosis in a Patient with Acute Myeloid LeukemiaSuccessfully Treated with Liposomal Amphotericin BAssociated with Deferasirox and Hyperbaric Oxygen
Eduardo Flavio Oliveira Ribeiro • Vitorino Modesto dos Santos •
Guilherme Teixeira Guimaraes Paixao • Leonardo Rodrigues Cruz •
Milena Zamian Danilow • Vinicius Ferreira Campos
Received: 27 August 2012 / Accepted: 18 February 2013 / Published online: 27 February 2013
� Springer Science+Business Media Dordrecht 2013
Abstract We report a 38-year-old woman presenting
with febrile neutropenia, acute myeloid leukemia (AML)
and invasive mucormycosis. Bone marrow aspirate was
characteristic of AML minimally differentiated (WHO
classification 2008). Flow cytometric immunophenotyp-
ing analysis showed blasts positive for CD7, CD33,
CD34, CD71, CD117, HLA-DR, MPO, and TdT, with
normal karyotype (46, XX), and the absence of the
FLT3-ITD and NPM1 mutations. The patient’s manage-
ment included chemotherapy with cytarabine and idaru-
bicin, and treatment with liposomal amphotericin B,
deferasirox, hyperbaric oxygen therapy, and antibiotics.
Nowadays, she is in complete hematological remission,
and CT images of control are normal. Invasive mucor-
mycosis is an uncommon and severe condition, which
involves diagnosis and treatment challenges. Clinical
features and predisposing factors should be highlighted
in order to enhance the suspicion index, contributing to
early diagnosis and disease control. Our aim is to report
classical features of this uncommon condition and to
emphasize usual management challenges.
Keywords Acute myeloid leukemia � Candida
zeylanoides � Deferasirox � Hyperbaric oxygen �Liposomal amphotericin B �Mucormycosis/zygomycosis
Introduction
Mucormycosis/zygomycosis is a rare life-threatening
infection caused by filamentous fungi from the orders
of Mucorales and Entomorphtorales [1, 2], which
are ubiquitous in the soil and vegetable- and
E. F. O. Ribeiro
Onco-Hematology Division, Armed Forces Hospital,
Brasılia, DF, Brazil
e-mail: [email protected]
V. M. dos Santos
Department of Internal Medicine of Armed Forces
Hospital, and Medical Course of Catholic University,
Brasılia, DF, Brazil
V. M. dos Santos (&) � G. T. G. Paixao �L. R. Cruz � M. Z. Danilow � V. F. Campos
Department of Internal Medicine, Armed Forces Hospital,
Estrada do Contorno do Bosque s/n, Cruzeiro Novo,
Brasılia, DF 70658-900, Brazil
e-mail: [email protected]
G. T. G. Paixao
e-mail: [email protected]
L. R. Cruz
e-mail: [email protected]
M. Z. Danilow
e-mail: [email protected]
V. F. Campos
e-mail: [email protected]
123
Mycopathologia (2013) 175:295–300
DOI 10.1007/s11046-013-9629-0

animal-decomposing matter [3–7]. The main routes of
infection are percutaneous (trauma, catheters, veni-
punctures, tattoos, bandages, animal bites, insect
pricking) and spores inhalation; people can also
accidentally ingest spores [4, 7]. Predisposing condi-
tions to mucormycosis are uncontrolled diabetes,
hematological malignancies, and hematopoietic stem
cell or organ transplantations [1–10]. This entity
constitutes the third cause of invasive mycosis, after
candidiasis and aspergillosis [5, 7, 11]. Etiological
agents include Mucorales spp., Mucor spp., Rhizopus
spp., Cunninghamella, and Lichtheimia corymbifera
[2, 4, 5, 10]. Mechanisms of disease are related to
conspicuous deficient action of polymorphonuclear
and mononuclear phagocytes [7]. The invasive form of
mucormycosis may occur in 40 % of cases [5], more
often developing in neutropenic patients with acute
leukemia (up to 78 %) [3, 5, 7, 11]. The frequency is
increasing, with high mortality (40–95 %), [1, 5–7, 9],
but case reports are scarce. Diagnosis challenges are
usual in daily practice [1, 5], and routine investigation
includes radiological, microbiological, histological,
and cytological findings [3, 5, 7, 11, 12]. Characteristic
histopathologic findings include necrosis and angio-
invasion by hyaline, broad thin-walled nonseptate
hyphae, with variable diameters, irregular branching,
and ending in right angles [3, 4, 7, 8, 11]. Although
polymerase chain reaction (PCR) might constitute a
promissory tool, it is not widely available and is not
clinically validated yet [3, 11, 12]. Control of mucor-
mycosis may be favorably influenced by amphotericin
B, deferasirox, and hyperbaric oxygen [3, 6, 9, 13].
Good outcomes depend on high suspicion index, early
diagnosis, and adequate therapy schedules [3, 4, 8].
Patients with febrile neutropenia must be closely
followed with special attention on prophylaxis and
early treatment of possible opportunistic infections
caused by bacteria or fungi [4, 8, 11]. Considering that
true incidence of mucormycosis seems to be underes-
timated [3], descriptions of case studies could con-
tribute to better knowledge about this life-threatening
and scarcely reported condition.
Case Report
A 38-year-old woman was admitted to Internal Med-
icine ward with four days history of odynophagia and
fever. Laboratory tests showed hemoglobin 9.4 g/dl,
leukocytes 1,400/mm3, 700 neutrophils/mm3 and
platelets 54,000/mm3 (Table 1). Three months before
admission, her blood counts revealed leucopenia
without anemia or low platelets. With diagnosis of
febrile neutropenia, her initial treatment consisted of
cefepime 2.0 g tid IV. Bone marrow aspirate detected
90 % of undifferentiated small blasts, morphologically
compatible with AML minimally differentiated (WHO
classification 2008). Flow cytometric immunopheno-
typing analysis showed 87.8 % of blasts that were
positively marked for CD7, CD33, CD34, CD71,
CD117, HLA-DR, MPO, and TdT, with normal
karyotype (46, XX), and the absence of the FLT3-
ITD and NPM1 mutations. She underwent the chemo-
therapy protocol 7 ? 3 (continuous infusion of cyt-
arabine 100 mg/m2 IV D1-7, and idarubicin 12 mg/m2
IV 1 h infusion D1-3). Initial thoracic and abdominal
tomography studies showed only a discrete pleural
effusion, and repeated blood cultures were negative.
Due to the persistence of fever, vancomycin was
associated on D2 and cefepime was further changed by
meropenem on D4, with addition of liposomal ampho-
tericin B (L-AmB) on D7. Her left ventricle ejection
fraction decreased from 67 % (pretreatment) to 39 %
on D12, with clinical features of congestive car-
diac insufficiency. Pro-BNP serum levels (normal:
\125 pg/dl) were 3,498 pg/dl on D18 and 576.9 pg/dl
on D22, findings highly indicative of cardiotoxicity by
chemotherapy, which was clinically controlled.
Because of a febrile reaction during amphotericin
infusion, supportive measures were undertaken on D11
and the L-AmB infusion was stopped. Administration
of voriconazole was started on D12. She evolved with
abdominal pain and diarrhea, but stools cultures were
negative and Clostridium difficile toxins A and B were
absent. Abdominal CT showed voluminous ascites,
while thoracic CT revealed pleural effusion and
bilateral interstitial infiltrate. The test for galactoman-
nan antigen detection was negative. Control abdominal
CT showed minute hepatic lesions and conspicuous
splenic lesions (Fig. 1a, b). With hypothesis of hepa-
tosplenic candidiasis, caspofungin was associated with
voriconazole on D21. In addition to a persistent fever,
the patient had dyspnea, low arterial O2 saturation,
and progressive bilateral pleural effusions. Moreover,
bronchoalveolar lavage detected development of Can-
dida spp., and blood cultures were positive for
Candida zeylanoides on D22. Isolates cultured on
Sabouraud-dextrose-agar were seeded and incubated
296 Mycopathologia (2013) 175:295–300
123

for selective yeast isolation, showing colonies of
C. zeylanoides by morphology and color reaction.
The patient evolved with cough and hyaline sputum,
but her respiratory pattern did not improve despite
antifungal therapy. Images of CT obtained on D33
showed nonspecific pulmonary nodules and a more
voluminous splenomegaly with scattered hypoattenu-
ated lesions. Even after the improvement of neutrope-
nia on D35, the patient persisted with daily fever and
CT imaging of conspicuous splenomegaly (Fig. 1a, b).
For diagnosis purpose, total splenectomy (Fig. 1c, d)
and excision of some hepatic implants were performed
on D52, and the specimens were submitted to histo-
pathology and culture evaluations. Respective studies
contributed to characterize the histopathology
diagnosis of hepatosplenic mucormycosis (Fig. 1e, f).
L-AmB was reintroduced (3 mg/kg) in association
with deferasirox (20 mg/kg), and a significant
improvement was observed in her clinical status and
blood counts on D12 of therapy. Because of the high-
risk AML, the option for the consolidation therapy
schedule was high-dose cytarabine—HD-AraC (3 g/
m2 12/12 h)—on D1, D3, and D5. L-AmB and
deferasirox constituted the secondary prophylaxis until
the bone marrow recovery, which occurred on D12 of
24 days of antifungal therapy. After hospital dis-
charge, there was recurrence of fever and leukocytosis,
and CT also showed implants in the vertebrae, pelvic
bones, and lungs, in addition to the liver and kidneys.
The schedule of choice was reintroduction of L-AmB
and deferasirox, at the same previous doses, but
associated with sessions on the hyperbaric camera.
After the first session of hyperbaric oxygen, there were
accentuated leukocytosis (38,000 mm3) and moderate
low platelet level (98,000/mm3), which rapidly
improved after 3 days under this treatment. The patient
underwent 60 sessions on the hyperbaric camera
(5 days a week, during 12 weeks). Concomitant use
of L-AmB was utilized for 21 days, while deferasirox
was used during all the time of hyperbaric oxygen
therapy. After the first consolidation therapy, the
patient is in total hematological remission and CT
images of control remain unremarkable.
Discussion
The case study described herein is about a young woman
with febrile neutropenia secondary to chemotherapy
for AML minimally differentiated, who presented with
an invasive disseminated mucormycosis successfully
controlled by L-AmB in association with deferasirox
and hyperbaric oxygen therapy. The actual increase
in mucormycosis incidence may be related to the
enhanced life expectancy of general population and
growing number of patients with predisposing condi-
tions, in special the immunosuppressant therapies
[1, 4]. Pagano et al. [5] reviewed data from 59 patients
with mucormycosis and hematological malignancies
and found the following distribution by frequency:
AML (51 %), acute lymphoid leukemia (27 %), non-
Hodgkin lymphoma (10 %), hairy cell leukemia and
myelodysplastic syndrome (3 % each), and multiple
myeloma, chronic myeloid leukemia, and Hodgkin’s
lymphoma (2 % each). The mortality rate by mucor-
mycosis is over 40 %, mainly among patients
with hematological malignancies (65 %) or bone
marrow transplants (90 %) [5]. Clinical presentations
of mucormycosis include rhino-orbital-cerebral,
pulmonary, cutaneous, gastrointestinal, disseminated,
and miscellaneous [2, 7, 9, 10]. According to Marques
et al. [4], the most common affected sites are rhino-
sinusoidal (44–49 %), primary cutaneous—localized
or generalized—(10–19 %), pulmonary (10–11 %),
disseminated (6–11 %), and gastrointestinal (2–11 %).
Fever, cough, dyspnea, thoracic pain, and hemoptysis
are usual symptoms of the pulmonary infection [4].
Features of the rhino-sinusoidal disease include fever,
facial pain and edema, nasal obstruction, rhinorrhea,
proptosis, chemosis, and palate damage [4, 10]. Fever,
headache, ptosis, diplopia, hemiplegia, and seizures
can be hallmarks of central nervous system involve-
ment [4]. Fever was the most common finding (80 %)
in patients studied by Pagano et al. [5] who considered
clinical diagnosis of mucormycosis a challenging task.
Disseminated infections more frequently have origin
from pulmonary involvement and the agent causes
scattered foci by hematogenous route. Clinical features
of disseminated disease are nonspecific, leading to
diagnostic pitfalls and late diagnoses, with high
mortality rates. Amphotericin B is not effective to
treat disseminated disease. Routine laboratory data are
nonspecific, but CT and MRI images can reinforce the
early suspicion and contribute to prompt initiation of
adequate therapy [12]. Imaging studies can disclose
hypodense nodules in abdominal viscera or in central
nervoussystem[12,14].ThoraxCTcanshowsuggestive
images of an angiotropic fungal infection, which can be
Mycopathologia (2013) 175:295–300 297
123
distinguished from aspergillosis by the presence of
multiple nodules ([10 mm) and pleural effusions [3].
Quantitative PCR has been a potential molecular
biology resource for diagnosis in developed countries,
but is not included in general routine practice, and
prospective studies are necessary to confirm the initial
results [3, 11, 12]. Fungal culture constitutes the best
method to establish the diagnosis, but this procedure is
time consuming and cannot contribute to the early
treatment for the life-threatening invasive infections
[12]. Moreover, identification of the fungus by seeding
on Sabouraud-dextrose-agar occurs in only one-third
of the surgical specimens [4]. Therefore, biopsy
histopathologic study constitutes the main definitive
diagnostic method in daily practice [3, 11, 12].
Mucorales typically appear as broad nonseptate
hyphae with right angle branching, and vascular
invasion, thrombosis, and necrosis [5, 7, 8, 11]. Our
initial concern was about the finding of Candida spp.
in bronchopulmonary secretions [10] and the further
positivity for Candida zeylanoides in blood cultures.
This novel agent of opportunistic infection produces
blue-green colonies on CHROM-agar Candida culture
medium [15] and presents 50 % of sensitivity to
voriconazole [16]. According to Ricciardi et al. [16],
the in vitro resistance of C. zeylanoides is 100 %
to amphotericin B, flucytosine, fluconazole, and
itraconazole. Therefore, the blood-born infection due
to C. zeylanoides was treated with caspofungin
associated with voriconazole [16, 17]. Association
between caspofungin and voriconazole is scarcely
used, but was prescribed because of Candida growing
in blood cultures, and spleen lesions were initially
attributed to disseminated candidiasis. Moreover, we
were not certain about possible existence of concom-
itant aspergillosis; so, other major concern was about
this angiotropic fungal infection, which is more
frequent than mucormycosis [5, 7, 11, 12]. As the
serum galactomannan test was negative, this differ-
ential diagnosis might be discarded; nevertheless,
inadequate antibody responses are usual in immuno-
suppressed patients, and the sensitivity of serum test
for aspergillosis varies from 22 to 91 % [12]. Alter-
native hypothesis of some more common invasive
infection was further ruled out by direct microscopic
exclusive detection of Mucorales in tissue samples
from the spleen [2]. Although prophylactic antifungal
therapy could be of real benefit to high-risk neutro-
penic patients with hemato-oncological diseases, there
is no consensual drug schedule to be utilized [12].
Successful treatment of mucormycosis is based on
four steps: (1) early diagnosis, (2) elimination of risk
factors if possible, (3) surgical debridement whenever
indicated, (4) and adequate antifungal therapy [3, 4,
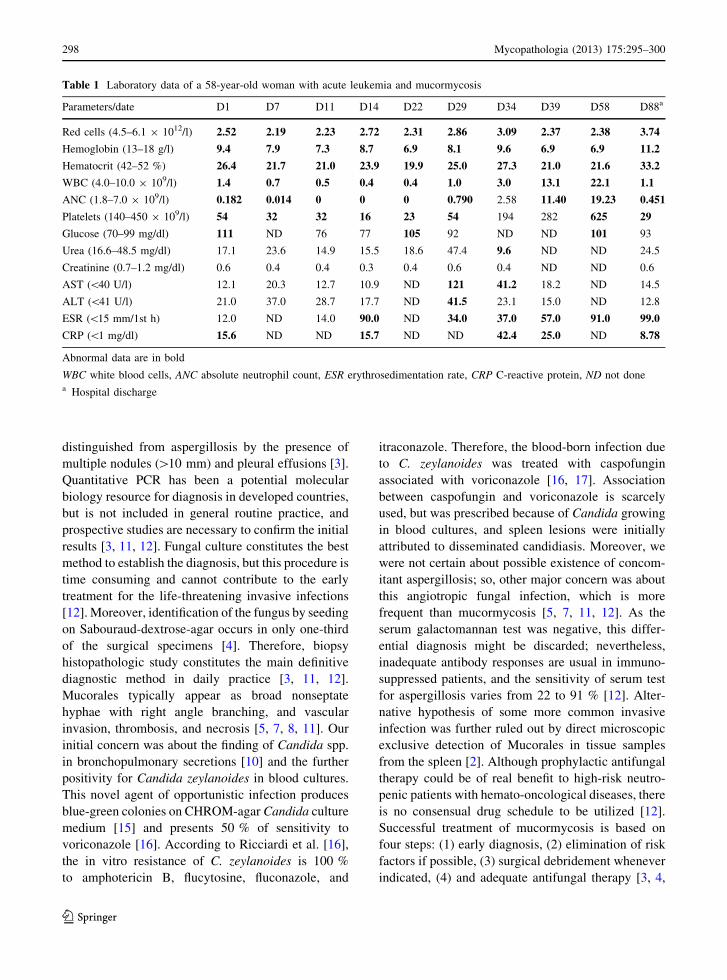
Table 1 Laboratory data of a 58-year-old woman with acute leukemia and mucormycosis
Parameters/date D1 D7 D11 D14 D22 D29 D34 D39 D58 D88a
Red cells (4.5–6.1 9 1012/l) 2.52 2.19 2.23 2.72 2.31 2.86 3.09 2.37 2.38 3.74
Hemoglobin (13–18 g/l) 9.4 7.9 7.3 8.7 6.9 8.1 9.6 6.9 6.9 11.2
Hematocrit (42–52 %) 26.4 21.7 21.0 23.9 19.9 25.0 27.3 21.0 21.6 33.2
WBC (4.0–10.0 9 109/l) 1.4 0.7 0.5 0.4 0.4 1.0 3.0 13.1 22.1 1.1
ANC (1.8–7.0 9 109/l) 0.182 0.014 0 0 0 0.790 2.58 11.40 19.23 0.451
Platelets (140–450 9 109/l) 54 32 32 16 23 54 194 282 625 29
Glucose (70–99 mg/dl) 111 ND 76 77 105 92 ND ND 101 93
Urea (16.6–48.5 mg/dl) 17.1 23.6 14.9 15.5 18.6 47.4 9.6 ND ND 24.5
Creatinine (0.7–1.2 mg/dl) 0.6 0.4 0.4 0.3 0.4 0.6 0.4 ND ND 0.6
AST (\40 U/l) 12.1 20.3 12.7 10.9 ND 121 41.2 18.2 ND 14.5
ALT (\41 U/l) 21.0 37.0 28.7 17.7 ND 41.5 23.1 15.0 ND 12.8
ESR (\15 mm/1st h) 12.0 ND 14.0 90.0 ND 34.0 37.0 57.0 91.0 99.0
CRP (\1 mg/dl) 15.6 ND ND 15.7 ND ND 42.4 25.0 ND 8.78
Abnormal data are in bold
WBC white blood cells, ANC absolute neutrophil count, ESR erythrosedimentation rate, CRP C-reactive protein, ND not donea Hospital discharge
298 Mycopathologia (2013) 175:295–300
123
7, 9]. L-AmB has been used for primary antifungal
therapy [2, 9, 18] and may be utilized at higher doses
and for longer periods with lower renal toxicity and
can yield better therapeutic responses [3, 4, 7, 19]. The
dose of L-AmB usually employed is 5–10 mg/kg [3, 4,
6, 19], and clinical improvement depends on the site of
infection and the predisposing conditions. Low dose of
L-AmB (3 mg/kg) was utilized because of the asso-
ciation with other therapeutic agents. The poorest
prognosis has been described in patients with hema-
tological malignancies, who have 32 % of complete or
partial responses [18]. Higher concentrations of
L-AmB have been detected in the following sites, in
a decreasing order: liver, spleen, kidney, lung, myo-
cardium and brain [19]. Monotherapy with azoles
(fluconazole, voriconazole) is not considered useful for
patients with mucormycosis [3, 8]. Association of
caspofungin with amphotericin B showed better results
than monotherapy with this antifungal agent [3, 9].
Although seemingly paradoxical, posaconazole (tria-
zole derivative of second generation) and deferasirox
(iron chelator) are employed as salvage therapy options
for patients refractory or intolerant to amphotericin
utilization [3, 4, 6, 13]. Deferasirox (20 mg/kg) for
2–4 weeks can block the iron influx bomb used by
Mucorales to stabilize its lipid membrane, phenome-
non that makes the fungi more vulnerable to the action
of amphotericin [3]. Although not consensual, invasive
fungal infections may be improved by enhanced
arterial perfusion of infected tissues exposed to oxy-
gen in supra-atmospheric pressures, and potentially
positive results were reported with hyperbaric oxygen
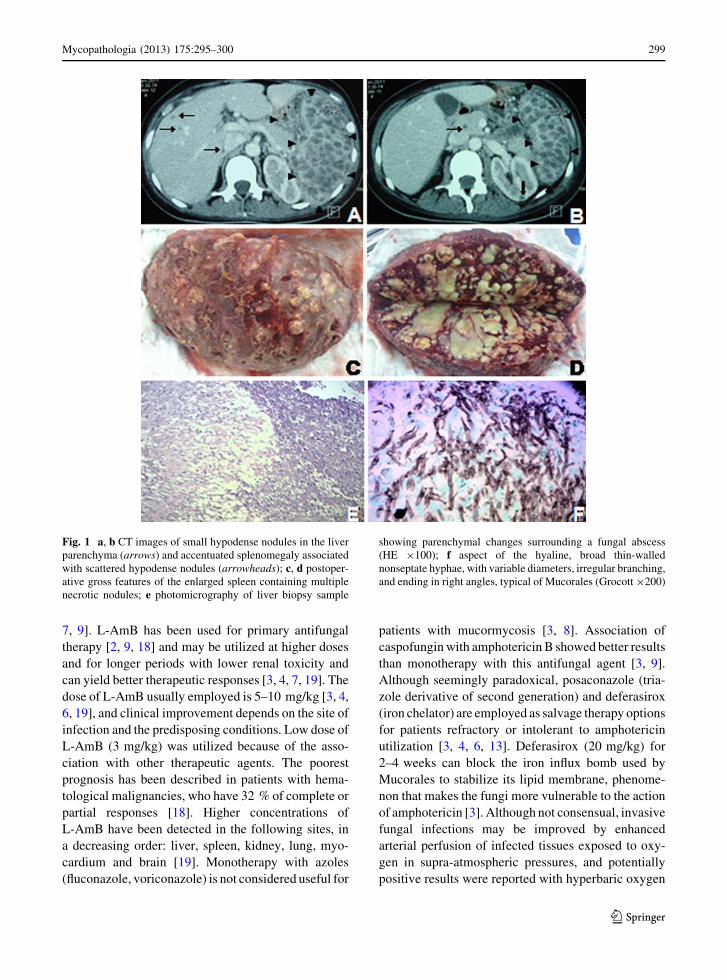
Fig. 1 a, b CT images of small hypodense nodules in the liver
parenchyma (arrows) and accentuated splenomegaly associated
with scattered hypodense nodules (arrowheads); c, d postoper-
ative gross features of the enlarged spleen containing multiple
necrotic nodules; e photomicrography of liver biopsy sample
showing parenchymal changes surrounding a fungal abscess
(HE 9100); f aspect of the hyaline, broad thin-walled
nonseptate hyphae, with variable diameters, irregular branching,
and ending in right angles, typical of Mucorales (Grocott 9200)
Mycopathologia (2013) 175:295–300 299
123

[3, 9, 13]. Local reduction of tissue acidosis can play a
favorable role, but the entire mechanisms of these
favorable results are not yet well understood [13].
Interestingly, Gonzales et al. [20] described a 59-year-
old neutropenic male with disseminated infection
by Rhizomucor pusillus (mucormycosis) successfully
treated with L-AmB and granulocyte colony-stimulat-
ing factor (G-CSF). The opportunistic infection devel-
oped after administration of a protocol for aplastic
anemia (cyclosporine, antithymocyte globulin, and
methylprednisolone). The authors highlighted their
novel therapeutic schedule to improve the severe
prognosis of this condition, emphasizing the search for
efficacious and less toxic agents [20]. Lin et al. [9]
reported successful control of mucormycosis with
posaconazole and hyperbaric oxygen. Our case study
focuses in the association of L-AmB (3 mg/kg) with
deferasirox (20 mg/kg) and hyperbaric oxygen (60
daily sessions, 5 times per week) as alternative
potential therapy for severe mucormycosis, which
should merit further experimental studies. The thera-
peutic association of L-AmB and deferasirox was
performed in the initial febrile stage of disease, with
good response. The triple association, which included
hyperbaric oxygen, was utilized after the patient
discharge from induction chemotherapy. It was main-
tained through the first and second consolidation
chemotherapy with HD-AraC, including the highly
dangerous neutropenic period after consolidation.
Notably, AML treatment was concluded and the
patient is in a good health status.
Conflict of interest There are no conflicts to disclaim.
References
1. Kivivuori SM, Karikoski R, Koukila-Kahkola P, Anttila VJ,
Saarinen-Pihkala UM. Zygomycosis presenting a major
clinical challenge: case report on Rhizomucor pusillusinfection in a stem-cell-transplant recipient. Mycopatholo-
gia. 2011;172(3):241–5.
2. Nawange SR, Singh SM, Naidu J, Jain S, Nagpal T, Behrani
DS, et al. Zygomycosis caused by Rhizopus microsporus and
Rhizopus oryzae in Madhya Pradesh (M.P.) Central India: a
report of two cases. Mycopathologia. 2012;174(2):171–6.
3. Kontoyiannis DP, Lewis RE. How I treat mucormycosis.
Blood. 2011;118(5):1216–24.
4. Marques AS, Camargo RMP, Abbade LPF, Marques MEA.
Mucormicose: infeccao oportunıstica grave em paciente
imunossuprimido. Relato de caso. Diagn Tratamento.
2010;15(2):64–8.
5. Pagano L, Offidani M, Nosari A, Candoni A, Piccardi M,
Corvatta L, et al. Mucormycosis in hematologic patients.
Haematologica. 2004;89(2):207–14.
6. Spellberg B, Walsh TJ, Konyoyannis DP, Edwards J Jr, Ibra-
him AS. Recent advances in the treatment of mucormycosis:
from bench to bedside. Clin Infect Dis. 2009;48(12):1743–51.
7. Tager FM, Zaror CL, Martınez DP. Cutaneous mucormy-
cosis in an immunocompromised patient. Rev Chilena
Infectol. 2012;29(1):101–7.
8. Karthaus M, Hentrich M. Wait and see or rush and switch?
New questions for the management of patients with febrile
neutropenia receiving antifungal prophylaxis. Mycoses.
2011;54(Suppl 1):1–6.
9. Lin SY, Lu PL, Tsai KB, Lin CY, Lin WR, Chen TC, et al.
A mucormycosis case in a cirrhotic patient successfully
treated with posaconazole and review of published litera-
ture. Mycopathologia. 2012;174(5–6):499–504.
10. Ribeiro LC, Wanke B, da Silva M, Dias LB, Mello R,
Canavarros FA, et al. Mucormycosis in Mato Grosso, Bra-
zil: a case reports, caused by Rhizopus microsporus var.
oligosporus and Rhizopus microsporus var. rhizopodifor-mis. Mycopathologia. 2012;173(2–3):187–92.
11. Zavrelova A, Matejkova A, Nova M, Hoffmann P, Buchta
V, Zak P. Case 3–2011: invasive mucormycosis (zygomy-
cosis) after bone marrow transplantation in a 26-year-old
man with relapsing acute myeloid leukaemia. Acta Medica.
2011;54(4):163–6.
12. Gompelman D, Heussel CP, Schuhmann M, Herth FJF. The
role of diagnostic imaging in the management of invasive
fungal disease—report from an interactive workshop.
Mycoses. 2011;54(Suppl 1):27–31.
13. Segal E, Menhusen MJ, Simmons S. Hyperbaric oxygen in
the treatment of invasive fungal infections: a single-center
experience. Isr Med Assoc J. 2007;9(5):355–7.
14. Horger M, Hebart H, Schimmel H, Vogel M, Brodoefel H,
Oechsle K, et al. Disseminated mucormycosis in haemato-
logical patients: CT and MRI findings with pathological
correlation. B J Radiol. 2006;79(945):e88–95.
15. Casal M, Linares MJ, Solis F, Rodriguez FC. Appearance of
colonies of Prototheca on CHROMagar Candida medium.
Mycopathologia. 1997;137(2):79–82.
16. Ricciardi AM, Ricciardi R, Danzi M, Mungiguerra M, Pi-
sano L, Marino A. In vitro activity of voriconazole and other
antifungal agents against clinical isolates of 138 Candidaspp. Infez Med. 2009;17(1):24–7.
17. Grandesso S, Sapino B, Mazzucato S, Solinas M, Bedin M,
D’Angelo M, et al. Study on in vitro susceptibility of
Candida spp. isolated from blood culture. Infez Med.
2012;20(1):25–30.
18. Shoham S, Magill SS, Merz WG, Gonzalez C, Seibel N,
Buchanan WL, et al. Primary treatment of zygomycosis
with liposomal amphotericin B: analysis of 28 cases. Med
Mycol. 2010;48(3):511–7.
19. Moen MD, Lyseng-Williamson KA, Scott LJ. Liposomal
amphotericin B: a review of its use as empirical therapy in
febrile neutropenia and in the treatment of invasive fungal
infections. Drugs. 2009;69(3):361–92.
20. Gonzales CE, Couriel DR, Walsh TJ. Disseminated zygo-
mycosis in a neutropenic patient: successful treatment with
amphotericin B lipid complex and granulocyte colony-
stimulating factor. Clin Infect Dis. 1997;24(2):192–6.
300 Mycopathologia (2013) 175:295–300
123