morphine bioavailability from a topical gel formulation in volunteers
TRANSCRIPT
314 Journal of Pain and Symptom Management Vol. 35 No. 3 March 2008
Original Article
Morphine Bioavailability from a Topical GelFormulation in VolunteersJudith A. Paice, PhD, RN, Jamie H. Von Roenn, MD, J. Craig Hudgins, BS,Lynn Luong, BS, Tom C. Krejcie, MD, and Michael J. Avram, PhDDepartment of Medicine, Division of Hematology-Oncology (J.A.P., J.H.V.R., J.C.H.), Department of
Anesthesiology and Mary Beth Donnelley Clinical Pharmacology Core Facility (L.L., T.C.K., M.J.A.),
and the Robert H. Lurie Comprehensive Cancer Center (J.A.P., J.H.V.R., T.C.K., M.J.A.),
Northwestern University Feinberg School of Medicine, Chicago, Illinois, USA
AbstractAlthough available therapies provide relief to many patients with cancer-related pain,swallowing difficulties or intestinal obstruction may preclude oral analgesic delivery in some.Topical morphine might provide an alternate delivery form but morphine bioavailability froma topical gel formulation has not been reported in humans. We conducted a randomized,placebo-controlled, double-blind, crossover study of five volunteers after they providedinstitutionally-approved, written, informed consent. They were admitted to the NorthwesternUniversity General Clinical Research Center twice, being randomly assigned to receive either1 mL of morphine compounded at 10 mg/mL in pluronic lecithin organogel (PLO) baseapplied to the wrist and 1 mL of normal saline administered subcutaneously, or 1 mL oftopical drug-free PLO base and 1 mL of subcutaneous morphine, 3 mg/mL, the first timeand the opposite combination the second. Seventeen blood samples were collected from5 minutes to 10 hours after dose administration for morphine concentration determination.Plasma samples were prepared by solid-phase extraction and morphine concentrationsmeasured by a mass spectrometric technique with a linear range of 0.5e500 ng/mL.Bioavailability of the topical formulation relative to the subcutaneous dose was to beestimated from doses and the plasma morphine concentration versus time relationships.Because morphine was seldom detected in plasma samples after topical administration andwas unquantifiable when it was, the low bioavailability of topical morphine wasunquantifiable. These results suggest that topical administration of morphine compoundedin a PLO base for transdermal drug delivery is unlikely to provide relief of cancer-relatedpain. J Pain Symptom Manage 2008;35:314e320. � 2008 U.S. Cancer Pain ReliefCommittee. Published by Elsevier Inc. All rights reserved.
Key WordsCancer-related pain, morphine, topical formulation, pluronic lecithin organogel (PLO) base,randomized controlled trial, volunteers, bioavailability, pharmacokinetics
Supported in part by a grant from excelleRx andGrant M01 RR-00048 from the National Center forResearch Resources, National Institutes of Health.
Address correspondence to: Michael J. Avram, PhD,Department of Anesthesiology, Northwestern
� 2008 U.S. Cancer Pain Relief CommitteePublished by Elsevier Inc. All rights reserved.
University Feinberg School of Medicine, 303 EastChicago Avenue, Ward 13-199, Chicago, IL 60611-3008, USA. E-mail: [email protected]
Accepted for publication: April 17, 2007.
0885-3924/08/$esee front matterdoi:10.1016/j.jpainsymman.2007.04.016

Vol. 35 No. 3 March 2008 315Topical Morphine Bioavailability
IntroductionAlthough most patients with cancer-related
pain obtain relief with available therapies, dif-ficulties with swallowing or intestinal obstruc-tion may preclude oral analgesic delivery.1
Because drugs such as fentanyl have been suc-cessfully delivered transdermally, other drugs,including analgesics, have been compoundedfor topical administration.2 To facilitate drugdelivery across the epidermis after topical ap-plication, these agents have been formulatedin a matrix, such as pleuronic lecithin orga-nogel (PLO), which is theoretically designedto enhance drug absorption.3 Topical 0.1%morphine hydrochloride gel administrationhas been reported to provide rapid relief ofcutaneous and other localized pain in a seriesof six patients receiving palliative care.4 Topi-cal administration of morphine in a PLO gelhas also been reported to provide relief ofdiffuse chronic arthritic pain in a series ofthree patients.5 Based upon these reportsand other anecdotal experiences, topical ad-ministration of morphine compounded asa gel formulation and applied to the wristhas been suggested as an alternate deliveryform.
Because the bioavailability of topically ad-ministered morphine, compounded as a gelformulation and applied to the wrist, is un-known, the purpose of the present study wasto determine its bioavailability. To determinethe bioavailability of topically administeredmorphine, the absorption, distribution, andelimination pharmacokinetics of topicallyadministered morphine must be referencedto the pharmacokinetics of morphine adminis-tered by a route for which 100% bioavailabilitycan be assumed, such as subcutaneouslyadministered morphine.6 Therefore, to mea-sure the bioavailability of topical morphinewith respect to subcutaneously administeredmorphine, the pharmacokinetics of each routewas determined in a randomized, doubleblind, placebo-controlled, crossover study inhealthy volunteers. Bioavailability was to bedetermined by simultaneously modeling theplasma morphine concentrations obtainedafter separate and independent administrationof the drug by the two routes.7 Preliminaryresults of this study appeared in abstract form.8
MethodsExperimental Protocol
Five healthy adult volunteers were studiedon two occasions each, separated from the firstby at least 48 hours, after obtaining institution-ally-approved, written, informed consent. Afteran overnight fast, they were admitted to theGeneral Clinical Research Center (GCRC) ofNorthwestern University’s Feinberg School ofMedicine. Volunteers were supine for at leastthe first hour after drug and placebo adminis-tration and limited their activity for the subse-quent 9 hours. An intravenous catheter wasplaced in an antecubital vein of the rightarm. A low volume loop, connected to a three-way stopcock, was attached to the catheter toenable blood sampling throughout the study.An intravenous infusion set was connected tothe proximal end of the stopcock and normal(0.9%) saline was infused at an appropriaterate to keep the intravenous catheter patent.
The subjects were randomly assigned, ina double-blind manner, to receive 1 mL ofmorphine compounded at 10 mg/mL inPLO base applied to the left wrist and 1 mLof normal saline administered subcutaneouslyin the soft tissue of the left forearm (of thearm opposite that used for blood drawing) or1 mL of the PLO base applied to the left wristand one mL of morphine, 3 mg/mL, adminis-tered subcutaneously in the soft tissue of theleft forearm (of the arm opposite that usedfor blood drawing) on the first occasion andthe opposite combination on the second occa-sion. The manufacturer of the compoundedmorphine gel (excelleRx, Philadelphia, PA)estimates that 10 mg of topical morphine isapproximately equal to 10 mg of oral mor-phine and recommends this as a startingdose.9 The subcutaneous morphine dose wascalculated to be approximately equal inpotency, using the standard 1:3 conversionbetween parenteral and oral morphine.10
The assignment of the volunteers to the or-der of treatment was determined by a randomnumber generator. Treatment assignmentswere recorded by subject and session numberon index cards that were sealed in opaque en-velopes labeled with the subject and sessionnumber. On the day of a session, the appropri-ate envelope was opened by a pharmacy staff

316 Vol. 35 No. 3 March 2008Paice et al.
member who then prepared the assigned mor-phine and placebo formulations and labeledthem with the subject and session number.
Blood (5 mL) was drawn before (�10 min-utes) and 5, 10, 15, 20, 30, 45, 60, 75, 90,120, 150, 180, 240, 300, 360, 480, and 600 min-utes after drug and placebo administration forthe determination of plasma morphine con-centrations. The heparinized blood sampleswere centrifuged at high speed for 10 minutesand the plasma was removed and transferredto labeled polypropylene tubes in which itwas stored at �80 �C until assayed.
Physiologic MeasurementsTo ensure safety, vital signs (blood pressure,
heart rate, temperature, and respiratory rate)were assessed every 15 minutes for the firsthour following topical and subcutaneousdrug administration and then hourly for theremainder of the 10 hour study. The bloodpressure cuff was placed only on the arm inwhich the intravenous catheter was inserted(i.e., not on the arm in and on which drughad been administered). Arterial oxygen satu-ration and heart rate were monitored continu-ously for the first two hours by a pulseoximeter (Datascope Accusat, Montvale, NJ).
Analytical MethodsPlasma morphine concentrations were mea-
sured by liquid chromatography-tandem massspectrometry after sample preparation bysolid-phase extraction. In brief, 10 mL ofa methanolic 100 ng/mL morphine-D3 (theinternal standard; Cerilliant pharmaceutical/forensic science analytical reference standard,Round Rock, TX) solution and 0.2 mL ofa plasma sample were added to a 1.5-mL poly-propylene tube, which was capped and thecontents mixed with the aid of a vortex mixer.The sorbent of each well of an Oasis HLB30 mm (30 mg) Extraction Plate (Waters Chro-matography, Milford, MA) was conditionedwith 1 mL of methanol and 1 mL of 0.1% tri-fluoroacetic acid in water, the prepared sam-ple was applied to the conditioned sorbent,and vacuum applied. The sorbent was thenwashed with 1 mL of 0.1% trifluoroaceticacid in water. Samples were eluted into a 96-well plate with 100 mL of methanol:water(50:50, vol:vol) followed by 100 mL of aqueoustriethylamine, dried under vacuum, and
reconstituted with 200 mL of mobile phase(described below). Twenty microliters of theeluent were analyzed by an API 3000 LC-MS/MS system (Applied Biosystems, Foster City,CA) equipped with an Agilent 1100 seriesHPLC system (Agilent Technologies, Wilming-ton, DE). Samples were eluted isocraticallyfrom a Synergi 4 m Hydro-RP 80A column(50� 2.0 mm, Phenomenex, Torrance, CA),protected by a Synergi 4 m Max-RP Security-Guard cartridge (4� 2.0 mm, Phenomenex),with a mobile phase consisting of water:metha-nol (93:7, vol:vol) containing 0.1% trifluoro-acetic acid at a flow rate of 0.225 mL/min.The tandem mass spectrometer was operatedwith its electrospray source in the positive ion-ization mode. The mass-to-charge ratios of theprecursor-to-product ion reactions monitoredwere 286 / 153 for morphine and 289 / 152for morphine-D3. Drug concentrations were cal-culated by comparing morphine/morphine-D3
ratios to a standard curve (0.5e500 ng/mLmorphine as the base) prepared in humanplasma. The morphine/morphine-D3 reten-tion time was approximately 2.8 minutes.The plasma morphine standard curve was lin-ear for morphine concentrations (as thebase) from 0.5 to 500 ng/mL, with interassaycoefficients of variation ranging from 0.7% to5.8%.
Pharmacokinetic ModelingVenous plasma morphine concentration ver-
sus time data were modeled using the SAAM IIsoftware system (SAAM Institute, Seattle, WA),implemented on a Windows�-based PC, usinga traditional two-compartment mammillarypharmacokinetic model. Drug absorption wasdescribed using a tanks-in-series delay elementto characterize the noninstantaneous firstappearance of the drug in the body.7 In themodel, the transfer rate constant kin was fixedas a large value so the drug appeared virtuallyinstantaneously in the delay element, which, inturn, accounted for the absorption profile.The SAAM II objective function used was theextended least-squares maximum likelihoodfunction using data weighted with the inverseof the model-based variance of the data atthe observation times.11 Systematic deviationsof observed data from the calculated valueswere sought using the one-tailed one-sampleruns test (results not shown), with P< 0.05,

Vol. 35 No. 3 March 2008 317Topical Morphine Bioavailability
corrected for multiple applications of the runstest, as the criterion for rejection of the nullhypothesis. Model misspecification was soughtby visual inspection of the measured and pre-dicted drug concentrations versus time rela-tionships. The maximum plasma morphineconcentration (Cmax) and its associated time(tmax) were determined for each of the routesof administration. Because bioavailability ofthe subcutaneously administered dose couldbe assumed to be 100%,6 the bioavailabilityof the topical formulation was to have been es-timated relative to that of the subcutaneousdose from doses and areas under the plasmamorphine concentration versus time curvesfor the two routes of administration.
StatisticsData are expressed as mean� SD.
ResultsThree females and two males, who were
29� 5 (mean� SD) years of age and weighed66� 9 kg, participated in both arms of thisstudy.
Peak plasma morphine concentrations of9.4e15.9 ng/mL were observed within15e20 minutes of rapid subcutaneous mor-phine administration to the volunteers (Table1). Plasma morphine concentrations wereabove the limit of quantification (0.5 ng/mL)for 6e10 hours (the latter time being thetime at which the last blood sample wasobtained) after subcutaneous administrationof the drug in all subjects. The plasma mor-phine concentration versus time relationshipsfollowing subcutaneous administration werewell characterized by the two compartment
pharmacokinetic model with an absorptiondelay (Fig. 1). The pharmacokinetics of thesubcutaneously administered morphine weredescribed by an absorption delay mean transittime (MTT) of 8.0� 3.9 minutes, a volume ofthe central compartment (VC) of 168� 55 L,a volume of the peripheral compartment(VP) of 212� 101 L, a volume of distributionat steady state (VSS) of 380� 118 L, an inter-compartmental clearance (CLI) of 2.4� 0.6L/minute, an elimination clearance (CLE) of1.8� 0.9 L/minute, and an elimination half-life (t1/2b) of 3.4� 0.7 hour.
No quantifiable morphine concentrationswere detected in any plasma samples obtainedfrom any subject after topical morphineadministration. Plasma morphine was notdetected in any of the plasma samples fromtwo of the volunteers following topical mor-phine administration. In the other three vol-unteers, plasma morphine was detected inonly three samples from each of two subjectsand in only six samples from the other subjectafter topical morphine administration, but themorphine concentrations in all of these sam-ples were below the limit of quantification.Because morphine was seldom detected inplasma samples and unquantifiable in thefew samples in which it was detected, it wasnot possible to quantify the maximum plasmamorphine concentration (Cmax), its associatedtime (tmax), or the extremely low bioavailabil-ity of morphine following topical administra-tion of 10 mg morphine compounded ina PLO base for transdermal drug delivery.Because it produced unmeasurable plasmaconcentrations, it was also not possible tocharacterize the pharmacokinetics of mor-phine absorption and disposition followingtopical administration.
Table 1Pharmacokinetic Parameters
Model Cmax (ng/mL) tmax (min) AUC (ng$min/mL)
Subcutaneous 12.4� 2.37 16.0� 2.2 1653.7� 934Topical <0.5a NQb NQb
Data are presented as Mean � SD (n¼ 5).Shown are the maximum concentration (Cmax), the time to the maximum concentration (tmax), and the area under the plasma concentrationversus time relationship (AUC).aAll plasma samples obtained after topical morphine administration had either no detectable morphine present or detectable morphine at con-centrations below the limit of quantification, 0.5 ng/mL.bNot quantifiable (NQ) because all plasma samples obtained after topical morphine administration had either no detectable morphine present ordetectable morphine at concentrations below the limit of quantification, 0.5 ng/mL. Because the AUC of topical morphine could not be quan-tified, the bioavailability of topical morphine relative to subcutaneous morphine could not be quantified.
318 Vol. 35 No. 3 March 2008Paice et al.
DiscussionThe peak plasma morphine concentrations
and the times to reach them after subcutane-ous administration in the present study arevery similar to those observed after subcutane-ous bolus administration by Stuart-Harris andcolleagues.6 In addition, the AUC observedfollowing subcutaneous administration in thepresent study is identical to the AUC theyreported, after making appropriate dose ad-justment.6 The pharmacokinetics of subcuta-neously administered morphine in thepresent study are consistent with the pharma-cokinetics of intravenously administered mor-phine reported by Ward and colleagues12 aswell as others.13 Thus, while the dispositionof subcutaneously administered morphinewas well characterized in the present study,the topically administered morphine wasfound to have essentially no measurable bio-availability. This conclusion was based on thefact that all blood samples collected in up to10 hours following topical morphine adminis-tration had either no detectable morphine inthem or had morphine at concentrationsbelow our very low limit of quantification,
Minutes
0 120 240 360 480 600
Plasm
a m
orp
hin
e
co
ncen
tratio
n (n
g/m
L)
0.5
5
50
1
10
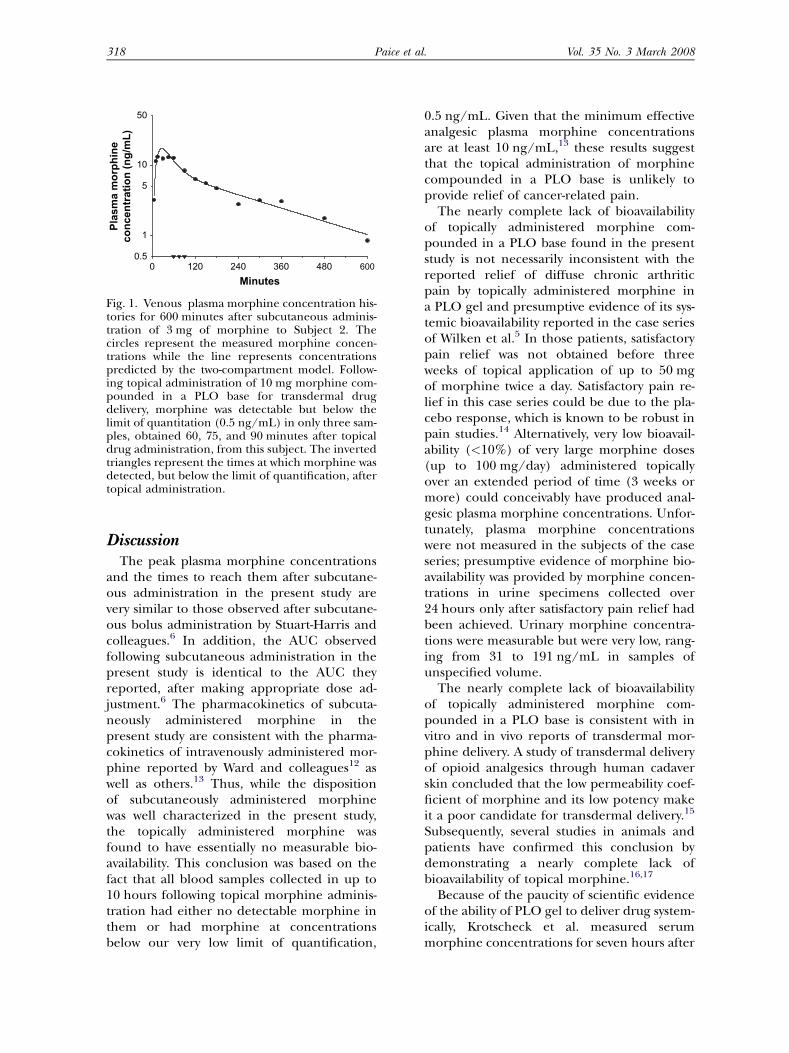
Fig. 1. Venous plasma morphine concentration his-tories for 600 minutes after subcutaneous adminis-tration of 3 mg of morphine to Subject 2. Thecircles represent the measured morphine concen-trations while the line represents concentrationspredicted by the two-compartment model. Follow-ing topical administration of 10 mg morphine com-pounded in a PLO base for transdermal drugdelivery, morphine was detectable but below thelimit of quantitation (0.5 ng/mL) in only three sam-ples, obtained 60, 75, and 90 minutes after topicaldrug administration, from this subject. The invertedtriangles represent the times at which morphine wasdetected, but below the limit of quantification, aftertopical administration.
0.5 ng/mL. Given that the minimum effectiveanalgesic plasma morphine concentrationsare at least 10 ng/mL,13 these results suggestthat the topical administration of morphinecompounded in a PLO base is unlikely toprovide relief of cancer-related pain.
The nearly complete lack of bioavailabilityof topically administered morphine com-pounded in a PLO base found in the presentstudy is not necessarily inconsistent with thereported relief of diffuse chronic arthriticpain by topically administered morphine ina PLO gel and presumptive evidence of its sys-temic bioavailability reported in the case seriesof Wilken et al.5 In those patients, satisfactorypain relief was not obtained before threeweeks of topical application of up to 50 mgof morphine twice a day. Satisfactory pain re-lief in this case series could be due to the pla-cebo response, which is known to be robust inpain studies.14 Alternatively, very low bioavail-ability (<10%) of very large morphine doses(up to 100 mg/day) administered topicallyover an extended period of time (3 weeks ormore) could conceivably have produced anal-gesic plasma morphine concentrations. Unfor-tunately, plasma morphine concentrationswere not measured in the subjects of the caseseries; presumptive evidence of morphine bio-availability was provided by morphine concen-trations in urine specimens collected over24 hours only after satisfactory pain relief hadbeen achieved. Urinary morphine concentra-tions were measurable but were very low, rang-ing from 31 to 191 ng/mL in samples ofunspecified volume.
The nearly complete lack of bioavailabilityof topically administered morphine com-pounded in a PLO base is consistent with invitro and in vivo reports of transdermal mor-phine delivery. A study of transdermal deliveryof opioid analgesics through human cadaverskin concluded that the low permeability coef-ficient of morphine and its low potency makeit a poor candidate for transdermal delivery.15
Subsequently, several studies in animals andpatients have confirmed this conclusion bydemonstrating a nearly complete lack ofbioavailability of topical morphine.16,17
Because of the paucity of scientific evidenceof the ability of PLO gel to deliver drug system-ically, Krotscheck et al. measured serummorphine concentrations for seven hours after
Vol. 35 No. 3 March 2008 319Topical Morphine Bioavailability
administration of 1 mg/kg and 2 mg/kg mor-phine in a 50 mg/mL PLO gel to the hair-free skin of the inguinal region or the earpinna of dogs.16 Serum morphine concentra-tions were below their limit of quantification(10 ng/mL) in all serum samples collectedafter both doses. One possible impedimentto effective transdermal delivery of morphineby the PLO gel cited by the authors was theintact epidermis. An additional impedimentto effective transdermal morphine deliverymight have been the PLO gel in which it wascompounded since transdermal delivery of fen-tanyl, which readily penetrates intact skin (seebelow), was also investigated and most serumfentanyl concentrations were below the limitof quantification (0.5 ng/mL) after adminis-tration of 0.88 mg/kg in 5 and 20 mg/mLPLO gels.16
Transdermal delivery of morphine mixedwith a gel applied to cutaneous ulcers hasbeen studied in humans. Ribeiro andcolleagues17 reported that morphine was notdetected in the plasma of five of six adult hos-pice patients within 24 hours of topical appli-cation of 10 mg of morphine sulfate mixedwith 8 g of Intrasite gel to skin ulcers with sur-face areas ranging from 5 to 23 cm2. In thesixth hospice patient, with a 60-cm2 ulcer, thebioavailability of the topical morphine wasonly 19.6%. This led the authors to concludethat the suggestion of local analgesic effectsof topical morphine applied to the painfulsacral pressure sores of five hospice patientsin a randomized controlled trial18 were indeedlocally rather than systemically mediated. Theantinociceptive effect of opioid agonists actingon peripheral opioid receptors is certainly anarea of great research interest,19 despitenegative randomized controlled trials.20 Thepotential local availability of topically appliedmorphine is not addressed by the presentstudy.
Effective transdermal morphine delivery hasbeen demonstrated in humans. Westerlinget al. de-epithelialized skin on the volar sideof the forearm of 12 volunteers using a vacuumsuction device and the next day administered10 mg of aqueous morphine hydrochloridefrom an occlusive reservoir applied to the de-epithelialized skin.21 They found first-orderabsorption of morphine produced relativelyconstant plasma morphine concentrations for
eight hours. Morphine delivered transdermallyin this manner had an average absolute bio-availability of 75%. The inconsistencies ofthese results with those of the studies discussedabove raises the question of whether it was thede-epithelialized skin or the nongel morphineformulation or both that led to significant bio-availability of morphine in this but not theother studies. Regardless of the reason forthe difference in bioavailability, this methodof drug delivery is not practical in the clinicalsetting.22
Despite the nearly incomplete bioavailabilityof topically administered morphine com-pounded in a PLO base, other opioids havebeen successfully formulated for transdermaldrug delivery, as demonstrated by clinical tri-als. One of the best known of these is fentanyl.The study of transdermal delivery of opioid an-algesics through human cadaver skin discussedabove also concluded that fentanyl can bedelivered by this method.15 A transdermalfentanyl delivery system has been demon-strated to produce and maintain effectiveplasma fentanyl concentrations23 and hasbeen show to be effective in the treatment ofa variety of severe pains, including severecancer pain.22,24
It has been noted16,25 that there are fewscientific data supporting the use of mostdrugs being administered topically in a PLOgel. The lack of data regarding the efficacy ofPLO as a drug delivery vehicle has been attrib-uted to the assumption by investigators that ifit is commercially available and being usedclinically it must have been studied.25 How-ever, this assumption is unfounded. The drugsbeing administered topically in a PLO gel areavailable from compounding pharmaciesrather than from traditional pharmaceuticalmanufacturers,25 hence, they are exemptfrom standard Food and Drug Administrationregulation, including the requirement fordemonstration of efficacy. Concerns haverecently been raised about topically adminis-tered drugs compounded as a gel formulationfor transdermal delivery to veterinary pa-tients.2 It seems appropriate to also be con-cerned about drugs similarly compoundedfor use in human patients. It would be prudentto forgo prescription of topically administereddrugs, including morphine, compounded asa gel formulation for transdermal delivery

320 Vol. 35 No. 3 March 2008Paice et al.
until the formulation has been shown toproduce effective plasma drug concentrationsand its efficacy has been established inrandomized, controlled clinical trials.
AcknowledgmentsThe authors would like to thank the
volunteers for graciously agreeing to partici-pate in this study; and Marcia Phillips, Mariqui-ta Sumague, Jacqui Grullon, Eileen Carter,Connie Nicolas, Joan Pasquesi, ElizabethTadina, and Monica Wover, of the Northwest-ern University General Clinical Research Cen-ter, for their assistance in the conduct of thisstudy.
References1. Mercadante S, Fulfaro F. Alternatives to oral
opioids for cancer pain. Oncology (Williston Park)1999;13:215e220.
2. Papich MG. Drug compounding for veterinarypatients. AAPS J 2005;7:E281eE287.
3. Kumar R, Katare OP. Lecithin organogels asa potential phospholipid-structured system fortopical drug delivery: a review. AAPS PharmSciTech2005;6:E298eE310.
4. Krajnik M, Zylicz Z, Finlay I, Luczak J, VanSorge AA. Potential uses of topical opioids inpalliative caredreport of 6 cases. Pain 1999;80:121e125.
5. Wilken M, Ineck JR, Rule AM. Chronic arthritispain management with topical morphine: caseseries. J Pain Palliat Care Pharmacother 2005;19:39e44.
6. Stuart-Harris R, Joel SP, McDonald P,Currow D, Slevin ML. The pharmacokinetics ofmorphine and morphine glucuronide metabolitesafter subcutaneous bolus injection and subcutane-ous infusion of morphine. Br J Clin Pharmacol2000;49:207e214.
7. Avram MJ, Henthorn TK, Spyker DA, et al.Recirculatory pharmacokinetic model of theuptake, distribution, and bioavailability of prochlor-perazine administered as a thermally generatedaerosol in a single breath to dogs. Drug MetabDispos 2007;35:262e267.
8. Paice J, Von Roenn J, Hudgins J, et al. Topicalmorphine bioavailability in volunteers. [abstract].J Pain 2007;8(4):S48.
9. The Hospice Pharmacia Pharmaceutical CareTool Kit�, 6th ed. Philadelphia: excelleRx, 2004.
10. Lugo RA, Kern SE. Clinical pharmacokinetics ofmorphine. J Pain Palliat Care Pharmacother 2002;16:5e18.
11. Barrett PHR, Bell BM, Cobelli C, et al. SAAM II:Simulation, analysis, and modeling software fortracer and pharmacokinetic studies. Metabolism1998;47:484e492.
12. Ward ME, Woodhouse A, Mather LE, et al.Morphine pharmacokinetics after pulmonaryadministration from a novel aerosol delivery system.Clin Pharmacol Ther 1997;62:596e609.
13. Glare PA, Walsh TD. Clinical pharmacokineticsof morphine. Ther Drug Monit 1991;13:1e23.
14. Vase L, Riley JL 3rd, Price DD. A comparison ofplacebo effects in clinical analgesic trials versusstudies of placebo analgesia. Pain 2002;99:443e452.
15. Roy SD, Flynn GL. Transdermal delivery ofnarcotic analgesics: comparative permeabilities ofnarcotic analgesics through human cadaver skin.Pharm Res 1989;6:825e832.
16. Krotscheck U, Boothe DM, Boothe HW. Evalua-tion of transdermal morphine and fentanyl pluroniclecithin organogel administration in dogs. Vet Ther2004;5:202e211.
17. Ribeiro MDC, Joel SP, Zeppetella G. Thebioavailability of morphine applied topically tocutaneous ulcers. J Pain Symptom Manage 2004;27:434e439.
18. Zeppetella G, Paul J, Ribeiro MDC. Analgesicefficacy of morphine applied topically to painfululcers. J Pain Symptom Manage 2003;25:555e558.
19. Janson W, Stein C. Peripheral opioid analgesia.Curr Pharm Biotechnol 2003;4:270e274.
20. Lilleso J, Hammer NA, Pedersen JL, Kehlet H.Effect of peripheral morphine in a human modelof acute inflammatory pain. Br J Anaesth 2000;85:228e232.
21. Westerling D, Hoglund P, Lundin S, Svedman P.Transdermal administration of morphine to healthysubjects. Br J Clin Pharmacol 1994;37:571e576.
22. Grond S, Radbruch L, Lehmann KA. Clinicalpharmacokinetics of transdermal opioids: Focuson transdermal fentanyl. Clin Pharmacokinet2000;38:59e89.
23. Gourlay GK, Kowalski SR, Plummer JL, et al.The transdermal administration of fentanyl in thetreatment of postoperative pain: pharmacokineticsand pharmacodynamic effects. Pain 1989;37:193e202.
24. Gourlay GK. Treatment of cancer pain withtransdermal fentanyl. Lancet Oncol 2001;2:165e172.
25. Murdan S. A review of pluronic lecithinorganogel as a topical and transdermal drugdelivery system. Hospital Pharmacist 2005;12:267e270.