morning star spring 2009 newsletter
DESCRIPTION
Morning Star Birth Center Spring 2009 NewsletterTRANSCRIPT
Spring 2009Volume 5, Issue 20
Birth Announcements 2
News of Interest 2
Calendar 3
Cesarean Surgery Rising 4
Exploration in Breech Birth 5
Quote of the Quarter 6
Two Breech Babies 8
The Other Side of the Glass 9
Birth Story: Hope Restored, A Father’s Story 10
The other day while checking email, I came across an essay, written by an obstetrician, regarding her perspective of the medicalization of childbirth. It was published in the In-ternational Journal of Feminist Approaches to Bioethics, Spring 2009 (see the full essay at http://wiki.naissance.asso.fr/index.php/articles/2322). In this amazing and insightful essay, the author addresses the issues of autonomy, locus of power, and the idea of womens’ need to be “special” by being labeled “high risk”. She questions if the trend of normalizing c-section stems as much from physician convenience and fear of litigation as from the “Disneyfication of a primal human endeavor, longing for the synthetic and dramatized experience in preference to the authentic”. Very thought provoking indeed.
In this issue, the topic of breech vaginal birth is explored. The art and skill of breech vaginal delivery is being lost to most obstetrical providers in our country due to the normalization of surgical delivery. When fear prevails and providers lose their trust and skill, birth becomes more dangerous. Women can and have always birthed babies in the breech presentation. Breech presentation is a variation of normal. From the essay: “Industrial obstetrics strips the locus of power definitively away from women. The history of childbirth in America reflects a persistent trend of increased control by physicians and increased medicalization. Childbirth moves, first, out of the home, and now out of the vagina. Stipulate that antibiotics and blood banks are good and necessary things, and that emergencies may, in fact, develop: still, the majority of births will be normal. Or they would be, without interference. The species that cannot birth its young becomes extinct. But fear has pushed nearly all American childbirth into the hospital, a campaign which continues even now that that battle looks to have been won. (American College of Obstetricians and Gynecologists, 2008) Still, despite the implied promise of safety if all the rules are followed–ID bracelets, intravenous lines, electronic fetal monitoring–labor may follow an unpredictable path. The definition of “normal” becomes ever narrower, and toleration of deviance ever lower. The final stage of this philosophy takes the process of birth away from the woman entirely and turns it into a surgical procedure performed by the doctor. Childbirth becomes a manufactured experience, shorn of any real risk or real
power, one in which the woman is so far alienated from the capa-bilities of her body that she is only a package on an operating
table for a professional to open.”
As it has always been, midwives around the world will continue to pass down their trust, knowledge and skill to others and work together with our medical counterparts to serve women and protect the safety and integrity of birth experiences and outcomes.
Happy Spring!
Love, Paula Bernini Feigal, CPMOwner/Director Morning Star Birth Center
Happy Spring!Happy Spring!
The World Needs Midwives Now More Than Ever!
Celebrate International Day of the Midwife on May 5, 2009! Learn more about this year’s goals, theme and mission by v i s i t i n g ICM’s web-site at www.internationalmidwives.org.
The
wor
ldne
eds midwives nowm
orethan
ever
International day ofthe midwife
May 5th 2009www.internationalmidwives.org

Page 2 The Morning Star Newsletter - Volume 5, Issue 20
Son, Benedict Joseph Buntz, January 13, 2009 at 12:18 am. 8 lbs. 0 oz., 20 in. Born to Sonia and Eric of Chippewa Falls.
Daughter, Onaleigh Emeline Rand, January 14, 2009 at 7:17 am. 6 lbs. 13.5 oz., 20.5 in. Born to Lynette and Keith of Eau Claire.
Daughter, Emma Jane Burgraff, January 18, 2009 at 6:36 am. 7 lbs. 8 oz., 20 in. Born to Billie Jo and Adam of Colfax.
Son, Dylan John Tholen, January 26, 2009 at 8:19 pm. 8 lbs. 2.5 oz., 21 in. Born to Stephanie and Lucas of Mankato, MN.
Son, Eric Christopher Clark Endrizzi, February 5, 2009, at 3:17 pm. 8 lbs. 8.5 oz., 20.5 in. Born to Collen and Dan of Inver Grove Heights, MN.
Son, Daniel James Holm, February 17, 2009, at 8:35 pm. 9 lbs, 14 oz., 22 in. Born to Mariann and Doran of Elk Mound.
We will be placing an order for a few new books to add to our library. If you have a suggestion for titles to include, please let us know by June 1st.
Our Library is Now Open!
Our Library is Now Open!
Art Corner
Go to www.thebirthsurvey.com/Press.html and read the press release “Need for Transparency Increases as Cesarean Section Rates Rise” (scroll down to see this press release listed near the middle of the page). This article points out the variations among hospitals and providers, and the need for information and transparency to enable pregnant women to make informed decisions about their care. You can also learn more about the work of The Birth Survey projects.
b a
c d
Think About It2008 was the first year of com-
mercial planting of genetically modified (GM) sugar beets in the US, with that sugar expected to enter the nation’s food supply this year. The Monsanto Round-up Ready sugar beet is geneti-cally engineered to be resistant to Monsanto’s herbicide glypho-sate (marketed as Roundup). The Environmental Protection Agency (EPA) recently agreed to
a Monsanto request to increase the allowable levels of glyphosate residue on sugar beet roots by 5000 percent.
A representative of Amalgam-ated Sugar estimated that 95 percent of the sugar beet crop in Idaho would be of the new GM variety in 2008. Sugar beets ac-count for about half the sugar in processed foods.
http://breastmilkproject.org
This is an amazing organization that collects donated breast milk from qualified donors and distributes 75% of it to US babies in need, and 25% of it to malnourished or sick babies in Africa. The process for applying to become a donor is easy, and the organization sets up collection, storage and shipment details with the donor. Check it out and spread the word!
Emily Cisco is pleased to be joining the Morning Star staff this May 2009. She has been actively supporting and promoting nor-mal birth in Northern Minnesota since 2004 as a Birth Doula and Maternal/Child Public Health Nurse. Emily received her BA in Nursing from the College of St. Scholastica in Duluth, MN and is currently pursuing a degree in Nurse-Midwifery from The Frontier School of Midwifery and Family Nursing in Kentucky. Born and raised south of Eau Claire, Emily is thrilled to be coming “home” and living her dreams with Morning Star.
She will be supporting families through education and prenatal, labor/birth and postpartum support.
“I’m looking forward to meeting you!” stated Emily.
Morning Star Welcomes Emily Cisco
1 2
3 4 5 6 7 8 9
10 11 12 13 14 15 16
17 18 19 20 21 22 23
24 25 26 27 28 29 30
The Morning Star Newsletter - Volume 5, Issue 20 Page 3
Morning Star Women’s Health and Birth Center321 13th St. SE • Menomonie, WI 54751
715.231.3100“Wisdom of Ages, Science of Today” ™
May 2009
Schedule of EventsMay 7th - Early Home Care
- 3:30-5 pm
May 12th - Handling Complications - 4:30-6 pm
May 21st - Mother’s Tea - Join us to learn what pregnant and new moms need to know about Pediatric Dentistry. We will be having a guest speaker from All Family Dental of Eau Claire. 12-2 pm
May 23rd - Handling Complications 1-2:30 pm
May 28th - Early Home Care 6-7:30 pm
Early Home Care 3:30-5 pm
31
Mother’s Tea 12-2 pmPediatric Dentistry
Handling Complications
4:30-6 pm
Handling Complications
1-2:30 pm
Early Home Care 6-7:30 pm
1 2 3 4 5 6
7 8 9 10 11 12 13
14 15 16 17 18 19 20
21 22 23 24 25 26 27
28 29 30
June
200
9Schedule of EventsJune 1st - Child Birth
Education I 5:30-8 pmJune 4th - Child Birth
Education II 5:30-8 pmJune 6th - Handling
Complications 1-2:30 pmJune 8th - Child Birth
Education III 5:30-8 pmJune 11th - Child Birth
Education IV 5:30-8 pmJune 16th - Early Home Care
4:30-6 pmJune 18th - Mother’s Tea - We
will be having a baby bracelet making workshop. Our host will be Carmen Tubeszewski of A’Cute Bead. Please call (715)231-3100 by 6/12 to register. The average cost for materials will be $15.
June 23rd - Handling Complications 4:30-6 pm
June 25th - Early Home Care 6-7:30 pm
Mother’s Tea 12-2 pm
Baby Bracelet Workshop
Child Birth Education I 5:30-8 pm
Early Home Care 6-7:30 pm
Handling Complications
4:30-6 pm
Child Birth Education II 5:30-8 pm
Handling Complications
1-2:30 pm
Child Birth Education III
5:30-8 pm
Child Birth Education IV
5:30-8 pm
Early Home Care 4:30-6 pm

Page 4 The Morning Star Newsletter - Volume 5, Issue 20
...peace, joy, comfort
WASHINGTON (March 18, 2009)—As research continues to mount for the risks of cesarean surgery, the Centers for Disease Con-trol released new, staggering statistics reporting that 31.8% of women endure birth by cesarean in the United States (2007). This announce-ment comes after the release of significant findings from the New Eng-land Journal of Medicine reinforcing that birth by cesarean surgery before 39 weeks of pregnancy causes increased complications in newborns.
Despite the latest advances in medical technology, health care pro-viders cannot determine a baby’s due date with 100% accuracy. There-fore, cesarean surgeries scheduled before a woman’s estimated due date could result in a baby born as early as 36 weeks to a few days before the baby is actually due. During the last few weeks of pregnancy, a baby’s lungs mature and a protective layer of fat forms, both of which are vital developments for a healthy baby. In addition, babies need time for their lung cells to shift from being fluid producing to fluid absorbing cells. Without time during labor to prepare the baby to breathe, lungs cells may not be ready. Thus, babies born by cesarean surgery, even when they are full-term, need to go to an intensive care unit more frequently than babies who were born vaginally to get help breathing.
Research published in the New England Journal of Medicine (NEJM) supports earlier findings that cesarean surgery performed prior to 39 weeks of pregnancy increases poor outcomes in babies. Of the babies in the NEJM study born before 39 weeks, more than 26% had com-plications, including the need to be on a ventilator, respiratory distress syndrome, low blood sugar and severe infection (sepsis).
“Overuse of cesarean surgery complicates the otherwise natural pro-cess of birth,” says Lamaze Institute Chair Debra Bingham, LCCE, MS, RN, DrPH, “Allowing the natural process to occur not only reduces risks for mothers in this and future pregnancies, but also reduces health risks for her baby.”
Spontaneous labor is almost always the best indication for a baby’s
physical readiness for life outside of the womb. As one of the key steps to a healthy birth, La-maze International recommends that women let labor begin on its own. Allowing labor to begin naturally increases the likelihood that a baby is healthy and ready for birth. When a birth outcome is good, mother and baby can bond and start breastfeeding immediately after birth—both of which provide the best start for a baby’s growth and development.
Lamaze International President Pam Spry, PhD, CNM, FACNM, LCCE says, “Maternity care in the United States is at a crossroads. The most commonly used practices don’t align with the best evidence for a healthy birth.” The Milbank Report’s Evidence-Based Maternity Care: What It Is and What It Can Achieve reveals that several routine maternity care practices, including cesarean surgery, contradict best evidence and are overused in the United States.
Cesarean surgery—a major abdominal surgery—also carries risks for women, such as blood loss, clotting, infection and severe pain, and poses future risks, such as infertility and complications during future pregnancies such as stillbirth and placenta problems like percreta and accreta, which can lead to excessive bleeding, bladder injury, hysterec-tomy and maternal death. The research is clear, however, that when medically necessary, cesarean surgery can be a lifesaving procedure for both mother and baby, and worth the risks involved.
Two of the most important decisions a woman can make are where she gives birth and who she chooses as her care provider. Lamaze In-ternational has developed tools to help women with these decisions, including the questions to ask and other reference material. Visit http://magazine.lamaze.org/ to learn more about the Lamaze during pregnan-cy, birth and beyond.
Evidence Increases for Risks in Cesarean Surgery as National Rate Continues to Rise
Morning Star to Sponsor Upcoming EventsPREGNANT IN AMERICA - Twin Cities Screening!
Tuesday, June 23rd from 6:30pm - 9:30pm at the Metro State University Founders Hall Auditorium, located at 700 E. 7th Street in St. Paul, MN with panel discussion following. Tickets and more information are available online through Ten Moons Rising at www.tenmoonsrising.org.
Pregnant in America is a documentary made by filmmaker Steve Buonagurio, who was trained as a sociologist and teacher. When Steve’s wife Mandy became pregnant, he immediately saw that something was wrong with the way women were being treated in the American maternity system. He was inspired to create a movie to help educate families and spark some much-needed change.
Primary Development as the Source of Core Life PatternsThursday, June 11th from 8:30am - 5:00pm also at the Metro
State University. Early registration (before May 15th) available at www.tenmoonsrising.org and CEU also available.
During the past decade, brain imaging, developmental neurosci-ences, attachment and trauma research and clinical findings have ig-nited new understandings of human development and relationships. Zero-to-three is currently considered the “critical period” of devel-opment, when intervention and support is most needed to prevent long-term repercussions from early issues. Now science and clinical findings from Prenatal and Perinatal Psychology (PPN) call for us to
once again redefine the landscape of early development and un-
derstanding human relationships.
The day will include powerpoint lecture, clinical videos, skill prac-tice, and plenty of Q & A to answer questions.
Healing Unresolved Birth Experiences in Moms, Babies & Children Saturday, June 13th at 9:00am - 5:00pm at the Marriott West,
located at 9960 Wayzata Boulevard in Minneapolis, MN. Register online at www.tenmoonsrising.org before May 15th for Early Bird savings.
Clinical findings from Prenatal and Perinatal Psychology indicate that what happens during pregnancy, birth and bonding are of pri-mary importance to mother, baby, and dad. For baby, this formative period establishes the foundation of life patterns and can be the dif-ference between life-enhancing or life-diminishing patterns.
Please join us at this remarkable, one-day workshop that provides an opportunity to come together with other moms to address unre-solved issues (in both mother and baby), and leave with tools to work with at home! Dr. McCarty’s experience helping moms and babies to heal these wounds has revealed the potential for truly elegant trans-formation and relief.
breech
The Morning Star Newsletter - Volume 5, Issue 20 Page 5
An Exploration in Breech Options and Breech Vaginal Birth: Information to Consider
A breech presenting baby is one who has his head up and bottom down. Breech vaginal birth is safe with a patient doctor with breech experience. The outcome of vaginally delivered breech babies is excellent.
The chance of complication is quite rare. The one problem is a hyper-extended neck. While there are some doctors who are willing to deliver breech babies, too often they are more willing to perform a cesarean. This makes it important to try to turn the baby to vertex position. First, check with your caregiver to see if there is any medical reason why you should not try these things. Do not be discouraged if he or she laughs and says “It will not work!” You can encourage your baby to turn.
breech noun \’bre_
ch\
Water WorksImmersing yourself in water will increase your amniotic
fluid, which can help the baby turn. Try the tub. Fill it with warm water and soak, while visualizing and verbally encouraging your baby to turn.
If you have access to a pool, get in it. Simply playing, turning somersaults, doing handstands, and swimming can encourage the baby to turn. Try diving headfirst into the pool, if the pool is deep enough. Be sure the pool is warm enough for you to relax.
Chiropractor VisitsA visit or two to the chiropractor can be a great benefit.
An adjustment called the ‘Webster breech-turn technique’ can give the baby the extra space she needs to turn.
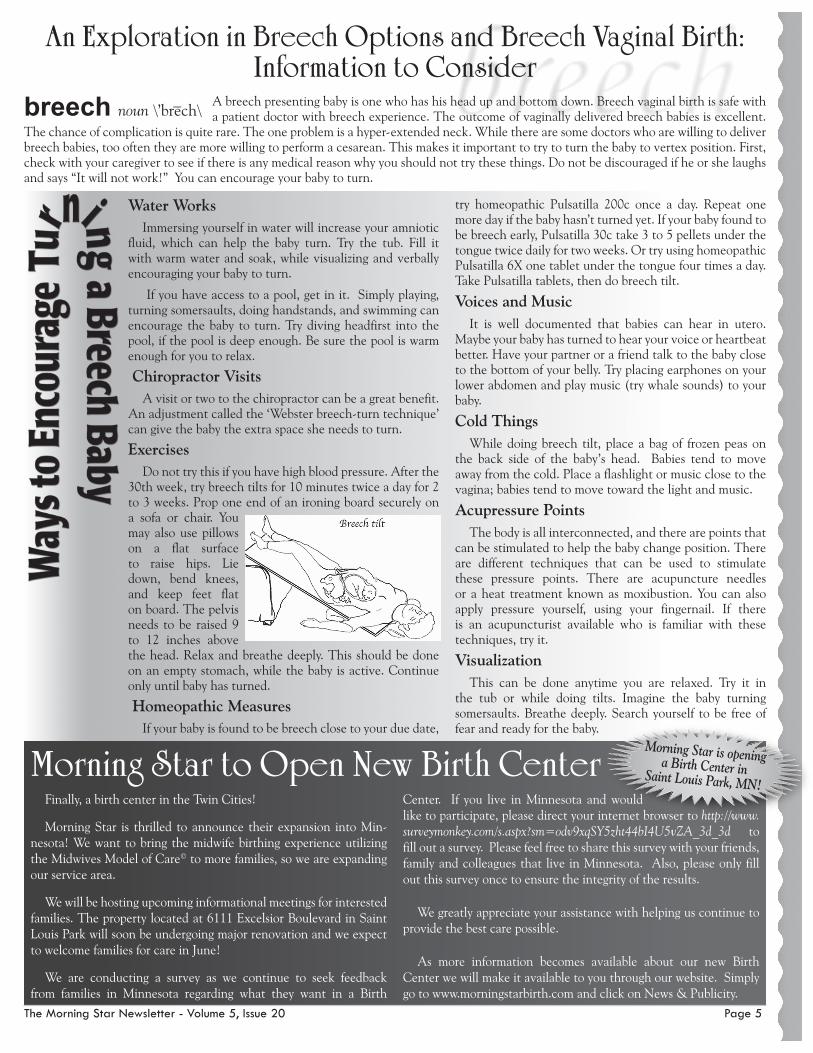
ExercisesDo not try this if you have high blood pressure. After the
30th week, try breech tilts for 10 minutes twice a day for 2 to 3 weeks. Prop one end of an ironing board securely on a sofa or chair. You may also use pillows on a flat surface to raise hips. Lie down, bend knees, and keep feet flat on board. The pelvis needs to be raised 9 to 12 inches above the head. Relax and breathe deeply. This should be done on an empty stomach, while the baby is active. Continue only until baby has turned.
Homeopathic MeasuresIf your baby is found to be breech close to your due date,
try homeopathic Pulsatilla 200c once a day. Repeat one more day if the baby hasn’t turned yet. If your baby found to be breech early, Pulsatilla 30c take 3 to 5 pellets under the tongue twice daily for two weeks. Or try using homeopathic Pulsatilla 6X one tablet under the tongue four times a day. Take Pulsatilla tablets, then do breech tilt.
Voices and MusicIt is well documented that babies can hear in utero.
Maybe your baby has turned to hear your voice or heartbeat better. Have your partner or a friend talk to the baby close to the bottom of your belly. Try placing earphones on your lower abdomen and play music (try whale sounds) to your baby.
Cold ThingsWhile doing breech tilt, place a bag of frozen peas on
the back side of the baby’s head. Babies tend to move away from the cold. Place a flashlight or music close to the vagina; babies tend to move toward the light and music.
Acupressure PointsThe body is all interconnected, and there are points that
can be stimulated to help the baby change position. There are different techniques that can be used to stimulate these pressure points. There are acupuncture needles or a heat treatment known as moxibustion. You can also apply pressure yourself, using your fingernail. If there is an acupuncturist available who is familiar with these techniques, try it.
VisualizationThis can be done anytime you are relaxed. Try it in
the tub or while doing tilts. Imagine the baby turning somersaults. Breathe deeply. Search yourself to be free of fear and ready for the baby.
Finally, a birth center in the Twin Cities!
Morning Star is thrilled to announce their expansion into Min-nesota! We want to bring the midwife birthing experience utilizing the Midwives Model of Care© to more families, so we are expanding our service area.
We will be hosting upcoming informational meetings for interested families. The property located at 6111 Excelsior Boulevard in Saint Louis Park will soon be undergoing major renovation and we expect to welcome families for care in June!
We are conducting a survey as we continue to seek feedback from families in Minnesota regarding what they want in a Birth
Center. If you live in Minnesota and would like to participate, please direct your internet browser to http://www.surveymonkey.com/s.aspx?sm=odv9xqSY5zht44bI4U5vZA_3d_3d to fill out a survey. Please feel free to share this survey with your friends, family and colleagues that live in Minnesota. Also, please only fill out this survey once to ensure the integrity of the results.
We greatly appreciate your assistance with helping us continue to provide the best care possible.
As more information becomes available about our new Birth Center we will make it available to you through our website. Simply go to www.morningstarbirth.com and click on News & Publicity.
Morning Star to Open New Birth CenterMorning Star is opening a Birth Center in Saint Louis Park, MN!
Page 6 The Morning Star Newsletter - Volume 5, Issue 20
Breech Vaginal Delivery
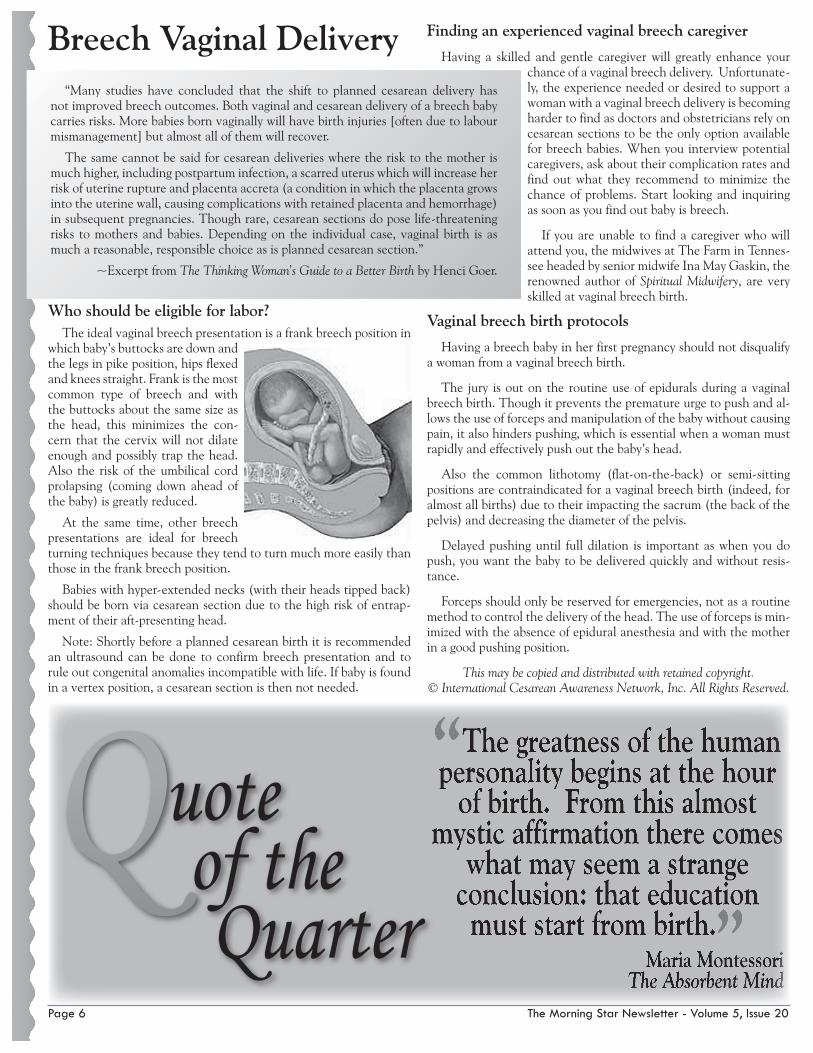
Who should be eligible for labor?The ideal vaginal breech presentation is a frank breech position in
which baby’s buttocks are down and the legs in pike position, hips flexed and knees straight. Frank is the most common type of breech and with the buttocks about the same size as the head, this minimizes the con-cern that the cervix will not dilate enough and possibly trap the head. Also the risk of the umbilical cord prolapsing (coming down ahead of the baby) is greatly reduced.
At the same time, other breech presentations are ideal for breech turning techniques because they tend to turn much more easily than those in the frank breech position.
Babies with hyper-extended necks (with their heads tipped back) should be born via cesarean section due to the high risk of entrap-ment of their aft-presenting head.
Note: Shortly before a planned cesarean birth it is recommended an ultrasound can be done to confirm breech presentation and to rule out congenital anomalies incompatible with life. If baby is found in a vertex position, a cesarean section is then not needed.
Finding an experienced vaginal breech caregiver
Having a skilled and gentle caregiver will greatly enhance your chance of a vaginal breech delivery. Unfortunate-ly, the experience needed or desired to support a woman with a vaginal breech delivery is becoming harder to find as doctors and obstetricians rely on cesarean sections to be the only option available for breech babies. When you interview potential caregivers, ask about their complication rates and find out what they recommend to minimize the chance of problems. Start looking and inquiring as soon as you find out baby is breech.
If you are unable to find a caregiver who will attend you, the midwives at The Farm in Tennes-see headed by senior midwife Ina May Gaskin, the renowned author of Spiritual Midwifery, are very skilled at vaginal breech birth.
Vaginal breech birth protocols
Having a breech baby in her first pregnancy should not disqualify a woman from a vaginal breech birth.
The jury is out on the routine use of epidurals during a vaginal breech birth. Though it prevents the premature urge to push and al-lows the use of forceps and manipulation of the baby without causing pain, it also hinders pushing, which is essential when a woman must rapidly and effectively push out the baby’s head.
Also the common lithotomy (flat-on-the-back) or semi-sitting positions are contraindicated for a vaginal breech birth (indeed, for almost all births) due to their impacting the sacrum (the back of the pelvis) and decreasing the diameter of the pelvis.
Delayed pushing until full dilation is important as when you do push, you want the baby to be delivered quickly and without resis-tance.
Forceps should only be reserved for emergencies, not as a routine method to control the delivery of the head. The use of forceps is min-imized with the absence of epidural anesthesia and with the mother in a good pushing position.
This may be copied and distributed with retained copyright. © International Cesarean Awareness Network, Inc. All Rights Reserved.
“Many studies have concluded that the shift to planned cesarean delivery has not improved breech outcomes. Both vaginal and cesarean delivery of a breech baby carries risks. More babies born vaginally will have birth injuries [often due to labour mismanagement] but almost all of them will recover.
The same cannot be said for cesarean deliveries where the risk to the mother is much higher, including postpartum infection, a scarred uterus which will increase her risk of uterine rupture and placenta accreta (a condition in which the placenta grows into the uterine wall, causing complications with retained placenta and hemorrhage) in subsequent pregnancies. Though rare, cesarean sections do pose life-threatening risks to mothers and babies. Depending on the individual case, vaginal birth is as much a reasonable, responsible choice as is planned cesarean section.”
~Excerpt from The Thinking Woman’s Guide to a Better Birth by Henci Goer.
“The greatness of the human personality begins at the hour
of birth. From this almost mystic affirmation there comes
what may seem a strange conclusion: that education must start from birth.”Maria Montessori
The Absorbent Mind
Quote of the
Quarter
The Morning Star Newsletter - Volume 5, Issue 20 Page 7
Questions?Go to www.MorningStarBirth.com
What is Breech Presentation?• Breech presentation is the most common human malpresentation
and occurs in 3-4% of all term pregnancies.1
• Three types of breech presentation occur: Frank (baby’s hips are flexed and knees extended bilaterally) , Complete (baby’s hips and knees are flexed bilaterally), and Incomplete (baby may present with one or two feet – ‘footling’- or one knee extended and the other flexed with hips flexed).2,3
• Early in pregnancy about half of all babies are breech presentation.4 Babies continue to turn to cephalic presentation throughout all weeks of pregnancy.1
What Causes Breech Presentation?• Only about 15% of breech presentations have an identifiable etiol-
ogy.5
• Established risks for breech presentation are: Previous breech presen-tation pregnancy,5,6,7,8 Late or lack of antenatal care,8,9 Prematurity (<37 weeks gestation),6,7,8 Comparatively lower birth weight,8,9 and Congenital anomalies.8,9,10
Recent Rates of Vaginal Delivery for Breech Presentation By Country• Japan 56%.11 Findings: Poor outcome 1.2% vaginal delivery : 0.0%
cesarean• Sweden 52%.12 Findings: No statistically significant difference be-
tween vaginal birth and cesarean section babies for perinatal/neona-tal outcomes.
• Norway 40%.13
• Finland 39%.14 Findings: Less birth trauma for vaginal breech deliv-eries than vaginal vertex deliveries. More trauma for breech vaginal delivery than breech CS, but lower long-term morbidity for breech vaginal than breech cesarean deliveries. Breech vaginal death 0.07%, vertex vaginal delivery death 0.02%.
• Sweden 37%.15 Findings: Infant mortality, birth injury and convul-sions higher for breech vaginal birth than breech CS
• Ireland 23%.16 Findings: No nonanomalous perinatal deaths, signifi-cant trauma, or neurological dysfunctions for vaginally or CS deliv-ered breech babies.
• Denmark 15.3%.17 Findings: Higher rates of puerperal fever and pel-vic infections for CS breech delivery.
• California 4.9%.18 Findings: Neonatal mortality, asphyxia, brachial plexus injury, and birth trauma higher for vaginally delivered breech than CS. If woman had a previous vaginal delivery no difference in neonatal mortality by delivery mode.
• Canada <5%.19
Other Research on Breech Presentation Outcomes by Delivery Method• Meta analysis 1: 24 studies published between 1966-199220
Findings: Higher perinatal mortality, traumatic morbidity, short-term morbidity, and long-term morbidity in vaginal delivery than in CS for breech presentation. Lower maternal morbidity and mortality for vaginal delivery of breech.
• Meta analysis 2: nine randomized trials or cohort studies published between January 1981 to June 199321
Findings: No statistically significant difference between infant mor-tality and morbidity between vaginal and CS delivery of breech pre-sentation.
• Term Breech Trial: randomized controlled clinical trial in 121 centers in 26 countries and included 2088 women with term singleton breech
pregnancies who were randomly assigned to give birth vaginally or by cesarean section22
Findings: Perinatal mortality, neonatal mortality, and serious neonatal morbidity higher for vaginal breech delivery than for CS in countries with low levels of infant mortality. No difference in infant outcomes by delivery method in countries with high infant mortality. No differ-ence in maternal morbidity and mortality by delivery mode.
Turning Options
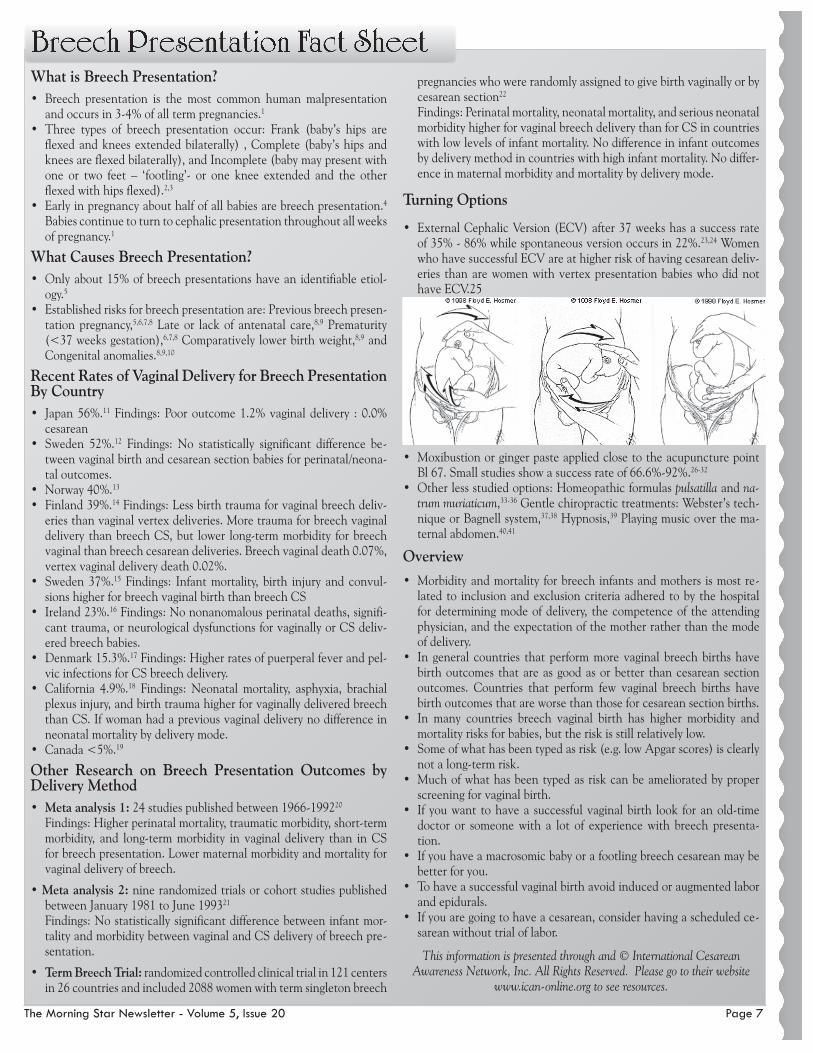
• External Cephalic Version (ECV) after 37 weeks has a success rate of 35% - 86% while spontaneous version occurs in 22%.23,24 Women who have successful ECV are at higher risk of having cesarean deliv-eries than are women with vertex presentation babies who did not have ECV.25
• Moxibustion or ginger paste applied close to the acupuncture point Bl 67. Small studies show a success rate of 66.6%-92%.26-32
• Other less studied options: Homeopathic formulas pulsatilla and na-trum muriaticum,33-36 Gentle chiropractic treatments: Webster’s tech-nique or Bagnell system,37,38 Hypnosis,39 Playing music over the ma-ternal abdomen.40,41
Overview• Morbidity and mortality for breech infants and mothers is most re-
lated to inclusion and exclusion criteria adhered to by the hospital for determining mode of delivery, the competence of the attending physician, and the expectation of the mother rather than the mode of delivery.
• In general countries that perform more vaginal breech births have birth outcomes that are as good as or better than cesarean section outcomes. Countries that perform few vaginal breech births have birth outcomes that are worse than those for cesarean section births.
• In many countries breech vaginal birth has higher morbidity and mortality risks for babies, but the risk is still relatively low.
• Some of what has been typed as risk (e.g. low Apgar scores) is clearly not a long-term risk.
• Much of what has been typed as risk can be ameliorated by proper screening for vaginal birth.
• If you want to have a successful vaginal birth look for an old-time doctor or someone with a lot of experience with breech presenta-tion.
• If you have a macrosomic baby or a footling breech cesarean may be better for you.
• To have a successful vaginal birth avoid induced or augmented labor and epidurals.
• If you are going to have a cesarean, consider having a scheduled ce-sarean without trial of labor.
This information is presented through and © International Cesarean Awareness Network, Inc. All Rights Reserved. Please go to their website
www.ican-online.org to see resources.
Breech Presentation Fact Sheet
Page 8 The Morning Star Newsletter - Volume 5, Issue 20
by Billie Jo BurgraffBefore ever becoming pregnant, my husband Adam and I were research-
ing gentle birth options. We read books, articles, spoke with people we knew, and then looked into what was available to us in our area. We made the decision to have our children naturally at Morning Star Birth Center.
Our first pregnancy went very well. I worked up until the day before birth with little to no complaints. At thirty-six weeks, I had the GBS (Group B Strep) swipe and that had come back positive. We received in-formation from Paula and did some more research of our own. We decided to only receive antibiotics if there were other circumstances that would increase the likelihood of our baby becoming sick.
On June 5, 2007, I woke up at 7 am and my water broke. I was just at thirty seven weeks. I called Paula and informed her and set up a time to go in and have the baby’s heart rate checked. I called Adam and set up a time to pick him up from the shop because he was working out of town and had been away since the morning before. My first contraction occurred after all of that, around 10:30 am. The con-tractions were not very pain-ful and not close together. So we got things ready, run-ning errands around town. At approximately 4:30 pm, the contractions were ten minutes apart. We went into the birth center again to check the fetal heart tones. Everything was going great. We went back home to labor some more. We called Paula at 7:45 pm and set up to meet her at the birth center because the contractions were about 5-7 minutes apart.
At the birth center, Paula did a check to see how dilated I was and she informed me that she believed our baby was breech. We were given the option of going to the hospital or to continue to labor at Morning Star. We all agreed that things were progressing well and we chose to stay there. We walked the steps and paced around, then we got into the tub to help the back labor pain I was having.
Paula then asked us to get out of the tub because the baby had passed meconium. Adam jumped out to change out of his swim trunks while Paula, Krista, and Erin were helping me out of the tub. As soon as I was out, I felt the baby coming and said, “Here comes the baby!” I then squatted as Paula and Erin held me while Krista caught our baby. Adam got out just in time to see the baby born bottom first, feet by the ears at 9:32 pm. They sat me down on a stool and handed me our beautiful, healthy baby girl. She was
5 lbs. and 13 oz. and wide awake. We named her Gracie May.
Our second pregnancy was completely different from our first. I was sick on and off at anytime of the day for the first four months. Then I had migraines for about a month. Three times I had urine tests come back positive for GBS. We treated it with 2 treatments of oral antibiotics. The fourth test came back good. I had no other
symptoms so we chose no IV antibiotics during birth, unless other circum-stances arouse.
On January 6, 2009, Paula noticed that our baby was breech. I was hoping to birth a baby head first. I tried doing flips in the motel pool, and using hot and cold packs on my belly to try and turn the baby. On the 8th we had an ultrasound. The baby was indeed breech. Paula and Dr. Feigal pressed their hands on my belly try-
ing to turn the baby’s head down. The baby’s heart rate was monitored the whole time. The baby still would not go head down. We went to see Dr. Emily Smith the same day to try a chiropractic technique. I continued the hot/cold packs and went to the pool a few more times. The baby still did not turn. The ultrasound had revealed we were having a baby girl so we tried to put a positive focus on finding “the” name.
On January 17, at 11:30 am, my water broke. We called Paula and went in to the birth center to check the baby’s heart tones. No labor yet, so we ran errands and got Gracie ready to go and stay with my parents. We went and walked at the mall, came home and hung out trying to figure out a middle name for our new daughter. At midnight we went to bed with sporadic contractions. At approximately 2:00
am, I was awoken from strong regular contractions. I was excited, it was progress. We called Paula and set up to meet her around 3:30 am.
We met Paula and Amy at the birth center and got everything set up. Adam and I walked around a bit but it felt best to stand and sway back and forth. Adam had his hands on my waist and my arms were on his shoulders. The contractions were picking up pace and growing in intensity at about 5:30 am. We got into the tub where I used the buoyant water to rock my hips back and forth through each contraction.
Paula asked us to get out of the tub and go to the bed. As we stood up to get out, I could feel the baby coming. I got sick at this point and my legs be-came shaky. Adam helped hold me up as I pushed out two little feet first, a body, and then her head. Paula was holding her body right away and handed her to me as she and Amy cleaned out her airways and gave
her a little oxygen as a precautionary measure. It was 6:36 am on January 18, 2009, when Emma Jane was born weighing 7 lbs. 8 oz., both feet first.
Two healthy girls, born breech, with no drugs, no surgery, not even a stitch. Just the knowledge and support from wonderful people who helped me to feel confident in listening to my body. Thank you Adam, Paula, and Morning Star Birth Center Staff for helping me give our daughters a gentle, loving welcome into this world.
Two Breech Babies

The Morning Star Newsletter - Volume 5, Issue 20 Page 9
posted on www.theothersideoftheglass.comFriday, April 3, 2009 - I got this
comment on the trailer on Youtube:“Where does this overwhelming
respect for authority come from, that it allows hospital staff to abuse mom & baby?
I sure don’t have it.For five bucks I’ll attend your birth
and if an attendant ignores a “No” or a direct request, I’ll break their freaking face.”
You might make a lot of money if you could be in so many places at once. Since that’s not possible, I hope the film shows the medical based caregivers–doctors, nurses, and midwives–how they can support and protect the father as well.
How is it that we have “this overwhelming respect for authority?” I would not use the word “respect” to describe how men and women acquiesce the control of their body, mind, and soul to strangers who sadly do not remember that this other human being before them, in their care, is a also sacred being, a soul in this body, a whole human being.
I think it is fear; a physiological response to the generational impact of giving it over and being dominated. As I interviewed men this year, as the filming and editing evolved, I came to see the true nature and role of the male is not to be the big, powerful protector against invaders and predators. It’s like asking him to protect his family from a home invader who just happened to break in as he and his partner have just made love. Right in the middle of that glow, in that rush of love hormones, taking a drag on his cigarette, a man disrupted is a man who can be easily toppled. He is the least likely to be able to protect anything but his own jewels.
A man is physiologically, emotionally, psychologically, and spiritually vulnerable at the moment of his baby’s birth. He is witnessing his baby, the result of his love and sperm, emerge, and he is taking in how amazing and powerful his partner is – all of this a product, and a consequence of his making this baby. Darn right, in the hospital setting, clearly demonstrated to be one invasion after another, he needs another man there who can protect him so that he can experience the climax of his conception of his baby. Birth. His creation emerging. To have his moment of awe – see, touch, smell and take in his creation, to gather his partner and baby into the strength and power of his loving, protective heart and arms, that is what he needs.
Imagine, if we lived in a world where we didn’t have our homes as fortresses with security systems, walls, fences, gates, and laws to protect our ownership and privacy. And, imagine the only way to ensure that you could have uninterrupted, quality, private lovemaking, and feel vulnerable enough to have an orgasm, and to collapse in the heights of the ecstasy of the moments after was to have your buddy guard the perimeter of your space from predators. Darn right, you’d need your buddy (or two or three) there, willing to “break their freaking face” if an intruder insisted on disrupting or endangering you and your loved one. Men need that in the hospital. And, thank you for offering it.
One thing I hope to accomplish with this film is shifting our current acceptance and perception about it being OK, and the responsibility
of a man and woman and a need to prepare to be so fierce in birthing their baby in the hospital. That’s a huge social imprint that creates a lot of our issues. I am concerned about this dynamic of having to be educated, armed, and prepared to fight for your rights in the hospital; to fight for what is physiologically natural, and seemingly simple, logical, respectful, kind, and science-based care. What is up with that anyway, that in 2009, in such a “civilized” time and nation, a woman has to go to the hospital prepared to fight for her life against intrusions, drugs, invasions of privacy, and to keep her body and soul intact?
I tire of hearing, even from the medical caregivers I’ve interviewed who DO honor the mother-baby-father trinity, that THE CONSUMERS have to create the change.
Part of me screams, NO! #*#&%@! It is the medical establishment, the people doing it, who must stop what they do that harms a man and his family. Right now. NOW! The science is there, on the side of natural birth and homebirth, and kindness and compassion, but they are allowed to do whatever they wish – until a movement of consumers hurts their assets enough to make them stop. These caregivers I interviewed have all gone through their own evolution to become the caregivers they are. They need support too. They know that the consumers are the only way that changes happen in their profession. They know too well that those who try from the inside are ostracized and persecuted. I think the shift can happen... but it will take an uprising of men.
Men have been telling me they need support of other men... and it is one of the goals of a group I am supporting to grow, Fathers For Better Birth.com, website coming. Contact Kris Amick at [email protected]. And, it is why part of my Baby Keeper training, on the back burner simmering away while I finish this film, includes training midwives, doulas, nurses, and doctors how to support men to support men in birth.
“The Other Side of the Glass - The Film” is a film by L. Janel Martin
Men are Vulnerable at Birth but Powerful in Numbers
Delivery Room Footballby Emmet Miller, M.D.
“Hold on a minute!” I said. “I want her to go to her mother.” I looked over at Sandy’s exhausted, filmy eyes and the look of panic on her face.
“No, we’re sorry,” they replied firmly. “Hospital policy.” Having proclaimed this, they strode purposely forward toward the door just to my left.
Quickly I stepped in front of them, blocking their way. “Hospital policy or not, I’m her father and she’s staying here!”
Suddenly it seemed time began to slow. Looking back, it seems almost like some sort of bizarre operating-room football game. The doctor, with my child tucked under his right arm like a halfback, decided he would simply ignore this irrational father, take a step to his right and scoot on past my left elbow and through the swinging door. I don’t know what he expected I would do, but I certainly know his eyes looked surprised when I made my move.
Continue to read the rest of Delivery Room Football at http://tinyurl.com/42yhyc
The Other Side of the Glass
From boiling water to waiting in smoke-filled waiting rooms only to see baby from “the other side of the glass,” to now hold-ing his partner’s hand during surgery, men’s role in birth has been defined by the medical establishment. Now, finally on “the other side of the glass,” men are still disempowered and pre-vented from connecting with their newborn baby in those first minutes of life.
by Mike Erath
If you had told me when my wife and I were first married in 1996 that we would have three children I would have not believed you. If you had told me we would have had one of them with a midwife I would have been all the more skeptical.
On June 1, 2008, we welcomed our daughter into the world. However, the road to her birth started not nine months earlier but six years earlier with the birth of our first son, Turner, and then two years later with the birth of our second son, Lee.
Joy and I had been married for five years when Joy became preg-nant with Turner. We had put off having children for concern that maybe we weren’t “baby people”. We both worked full-time; I in sales and Joy as a P.E. teacher. Our first pregnancy was not easy. Joy faced almost constant nausea ac-companied by intense feelings of depression and feeling that preg-nancy was the worst thing in the world. During this time we followed conventional medical care with Joy seeing her doctor routinely. We attributed Joy’s depression to just being pregnant. After finally men-tioning these feelings to her doctor toward the end of her 2nd trimes-ter her doctor prescribed anti-depressants. The medication was defi-nitely beneficial. Her pregnancy continued without issue until I got a call from one of Joy’s students saying that her water had broke while she was sitting in her office. The only challenge was the baby was not due for another five weeks. Her labor progressed steadily until
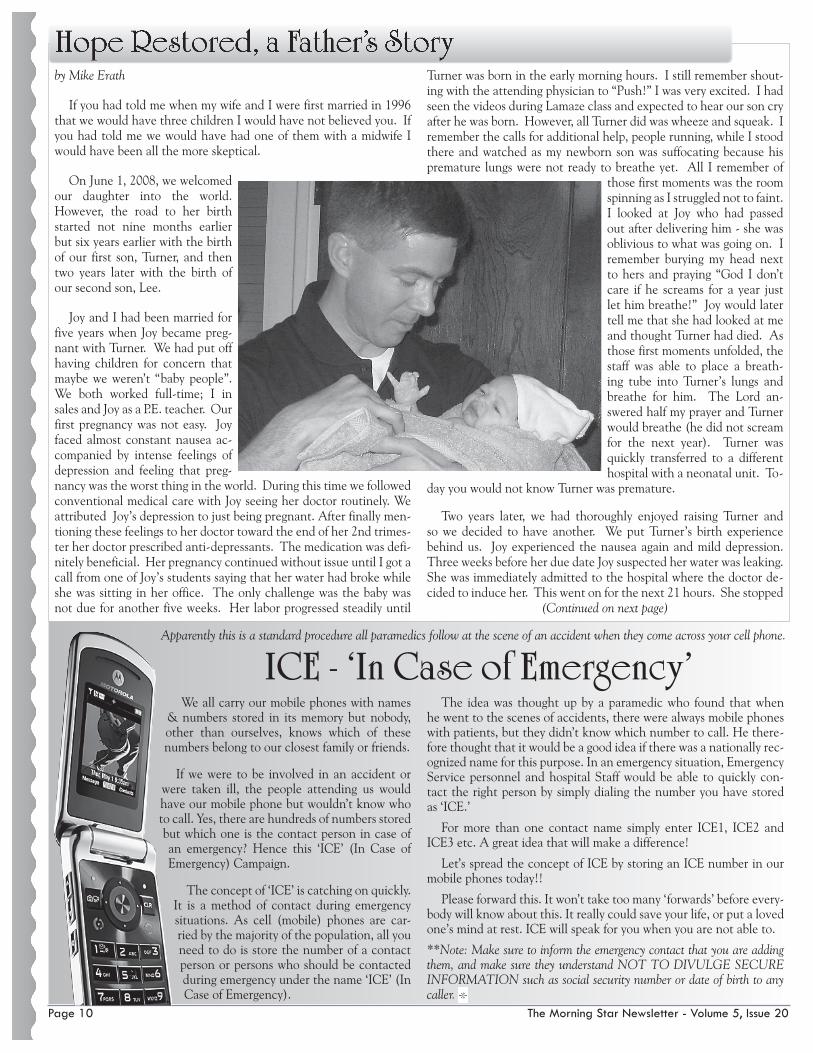
Turner was born in the early morning hours. I still remember shout-ing with the attending physician to “Push!” I was very excited. I had seen the videos during Lamaze class and expected to hear our son cry after he was born. However, all Turner did was wheeze and squeak. I remember the calls for additional help, people running, while I stood there and watched as my newborn son was suffocating because his premature lungs were not ready to breathe yet. All I remember of
those first moments was the room spinning as I struggled not to faint. I looked at Joy who had passed out after delivering him - she was oblivious to what was going on. I remember burying my head next to hers and praying “God I don’t care if he screams for a year just let him breathe!” Joy would later tell me that she had looked at me and thought Turner had died. As those first moments unfolded, the staff was able to place a breath-ing tube into Turner’s lungs and breathe for him. The Lord an-swered half my prayer and Turner would breathe (he did not scream for the next year). Turner was quickly transferred to a different hospital with a neonatal unit. To-
day you would not know Turner was premature.
Two years later, we had thoroughly enjoyed raising Turner and so we decided to have another. We put Turner’s birth experience behind us. Joy experienced the nausea again and mild depression. Three weeks before her due date Joy suspected her water was leaking. She was immediately admitted to the hospital where the doctor de-cided to induce her. This went on for the next 21 hours. She stopped
Hope Restored, a Father’s Story
(Continued on next page)
We all carry our mobile phones with names & numbers stored in its memory but nobody, other than ourselves, knows which of these numbers belong to our closest family or friends.
If we were to be involved in an accident or were taken ill, the people attending us would have our mobile phone but wouldn’t know who to call. Yes, there are hundreds of numbers stored but which one is the contact person in case of an emergency? Hence this ‘ICE’ (In Case of Emergency) Campaign.
The concept of ‘ICE’ is catching on quickly. It is a method of contact during emergency situations. As cell (mobile) phones are car-ried by the majority of the population, all you need to do is store the number of a contact person or persons who should be contacted during emergency under the name ‘ICE’ (In Case of Emergency).
The idea was thought up by a paramedic who found that when he went to the scenes of accidents, there were always mobile phones with patients, but they didn’t know which number to call. He there-fore thought that it would be a good idea if there was a nationally rec-ognized name for this purpose. In an emergency situation, Emergency Service personnel and hospital Staff would be able to quickly con-tact the right person by simply dialing the number you have stored as ‘ICE.’
For more than one contact name simply enter ICE1, ICE2 and ICE3 etc. A great idea that will make a difference!
Let’s spread the concept of ICE by storing an ICE number in our mobile phones today!!
Please forward this. It won’t take too many ‘forwards’ before every-body will know about this. It really could save your life, or put a loved one’s mind at rest. ICE will speak for you when you are not able to.
**Note: Make sure to inform the emergency contact that you are adding them, and make sure they understand NOT TO DIVULGE SECURE INFORMATION such as social security number or date of birth to any caller.
Apparently this is a standard procedure all paramedics follow at the scene of an accident when they come across your cell phone.
ICE - ‘In Case of Emergency’
Page 10 The Morning Star Newsletter - Volume 5, Issue 20
The Morning Star Newsletter - Volume 5, Issue 20 Page 11
dilating after being induced and each contraction would last up to 15 minutes. She developed a fever and started to show signs of going into shock. Joy was very upset as the doctor told us she would have to have an emergency C-section. She had fo-cused the whole pregnancy on having a natural birth. Again I found myself fac-ing what should have been a wonderful experience but instead I was full of fear and grief. I met Lee for the first time ten minutes later. Joy returned from recovery an hour and a half later green, bloated, and exhausted. She really could not hold the baby. Because Joy did not look like herself Turner
would not go to her. You can imagine how rejected Joy felt. Things did not get any better. Joy developed intense postpartum depression and was not bonding with the baby. Again, she was prescribed an-tidepressants. I remember our first night home as Joy tried to nurse Lee. He would not nurse and screamed. I lay in bed thinking, “What have we done? We have ruined our perfect family by having another child.” This of course made no sense; Lee was just as much of a bless-ing to us as Turner. I was traumatized as well from this experience. In hindsight, it became obvious that the medical advice we had ac-cepted turned out to have failed us. At some points, it bordered on negligence. Our son’s birth did not need to have been forced.
Over the next four years, Joy and I talked of another child but I wanted no part of another birth experience. I would experience anxiety attacks when I thought of what had happened. Despite my fear, I knew we were not done having children. In the meantime, I felt that in order to be emotionally ready for another child I would have to accept the fact that during birth I might lose Joy, the baby, or both.
We learned of Paula and her staff at Morning Star through a friend of Joy’s who had also had some very negative experiences delivering in a traditional hos-pital. She highly recommended Morning Star. She too had unnecessary cesarean births and was able to have a natural delivery after. We visited Paula prior to being pregnant and had a chance to talk with her. We were both able to talk about what had gone wrong with Lee’s birth. Joy felt all the more angry with what had happened and I was still very fearful. I was impressed, however, with the amount of prenatal care Joy and the baby would receive. After talking with Paula, I was still apprehensive about birth but felt we could deliver at Morning Star. In the fall of 2008 Joy became pregnant. I was excited but still fearful of what the delivery experience would be. Our family was also concerned and questioned the wisdom of delivering with a midwife given the past and also that we lived two and a half hours away.
Joy still experienced nausea through the first half of the pregnancy but no significant depression. I was very reassured to see Joy preg-
nant, full of energy, and glowing. Our delivery experience started on a Friday night at 10:30. Joy noticed she was having contractions. We had everything already packed and had our next-door neighbor (Grandma) come over to stay with our boys. We picked up Joy’s sister who had been pres-ent for the births of our boys and got to Morning Star at 3:30 am, only to find Joy’s contractions had stopped. On Paula’s advice we checked into our hotel. We got up the next morning and Joy decided to take us on a three-hour walk. She likes walking which is actu-ally slow running by most standards. Her labor started back up so we went shop-ping for the afternoon. We also ate dinner at a friend’s house. Later that evening Joy wanted to go back to the hotel as her contractions were getting harder. She did most of her hard labor at the hotel and we left for Morning Star at 11:30 that night.
Paula and her staff met us and Joy was overjoyed that she was fully dilated and ready to start pushing. We were ready for a natural deliv-ery! Joy opted to labor and deliver in the bathtub. Throughout the whole day, I did not have any reservations or any fear. I continued to be fully confident and completely peaceful as Joy pushed through each contraction. I was there and completely vested in what was happening. We were actually doing this together. Paula monitored Joy’s progress and the baby’s vital signs. At 1:47 am, Joy gave one final push and our baby was born. It was obvious to me as Paula im-mediately lifted our baby out of the water that we had a girl. At the same time she asked Joy if she would like to hold her baby. Joy under-standably was tired and had been kneeling as she delivered, but she
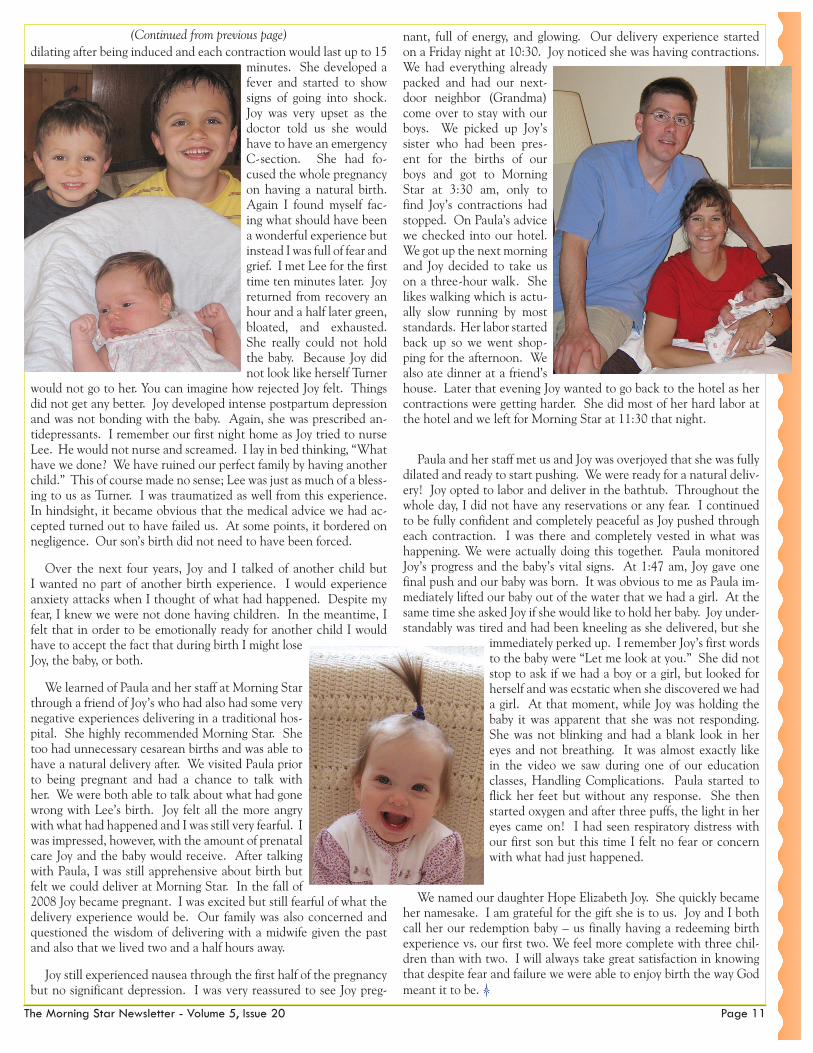
immediately perked up. I remember Joy’s first words to the baby were “Let me look at you.” She did not stop to ask if we had a boy or a girl, but looked for herself and was ecstatic when she discovered we had a girl. At that moment, while Joy was holding the baby it was apparent that she was not responding. She was not blinking and had a blank look in her eyes and not breathing. It was almost exactly like in the video we saw during one of our education classes, Handling Complications. Paula started to flick her feet but without any response. She then started oxygen and after three puffs, the light in her eyes came on! I had seen respiratory distress with our first son but this time I felt no fear or concern with what had just happened.
We named our daughter Hope Elizabeth Joy. She quickly became her namesake. I am grateful for the gift she is to us. Joy and I both call her our redemption baby – us finally having a redeeming birth experience vs. our first two. We feel more complete with three chil-dren than with two. I will always take great satisfaction in knowing that despite fear and failure we were able to enjoy birth the way God meant it to be.
(Continued from previous page)
We are happy to serve women and families from manycounties of northwestern Wisconsin and easternMinnesota. We are committed to offering holisticmaternity services in the Midwives’ Model of Care©
and to empower women and families throughprinciples of education, communication and shareddecision making.
Morning Star Women’sHealth and Birth Center321 13th St. SEMenomonie, WI 54751715.231.3100
“Wisdom of Ages, Science of Today” ™
New Location Opening Soon in
Saint Louis Park, MNCheck out
www.morningstarbirth.com for details!