misattribution of external speech in patients with hallucinations and delusions
TRANSCRIPT

www.elsevier.com/locate/schres
Schizophrenia Research 69 (2004) 277–287
Misattribution of external speech in patients with hallucinations
and delusions
Paul P. Allen*, Louise C. Johns, Cynthia H.Y. Fu, Matthew R. Broome,Goparlen N. Vythelingum, Philip K. McGuire
Section of Neuroimaging, Division of Psychological Medicine, Institute of Psychiatry, P.O. Box 67, Denmark Hill, London SE5 8AF, UK
Received 1 August 2003; accepted 24 September 2003
Available online 26 November 2003
Abstract
Background: One of the main cognitive models of positive symptoms in schizophrenia proposes that they arise through
impaired self-monitoring. This is supported by evidence of behavioural deficits on tasks designed to engage self-monitoring, but
these deficits could also result from an externalising response bias. We examined whether patients with hallucinations and
delusions would demonstrate an externalising bias on a task that did not involve cognitive self-monitoring.Method: Participants
passively listened (without speaking) to recordings of single adjectives spoken in their own and another person’s voice, and made
self/nonself judgements about their source. The acoustic quality of recorded speech was experimentally manipulated by altering
the pitch. Fifteen patients with schizophrenia who were currently experiencing hallucinations and delusions, 13 patients with
schizophrenia not experiencing current hallucinations and delusions and 15 healthy controls were compared. Results: When
listening to distorted words, patients with hallucinations and delusions were more likely than both the group with no
hallucinations and delusions and the control group to misidentify their own speech as alien (i.e. spoken by someone else). Across
the combined patient groups, the tendency to misidentify self-generated speech as alien was positively correlated with current
severity of hallucinations but not with ratings of delusions or positive symptoms in general. Conclusions: These findings indicate
that patients with hallucinations and delusions are prone to misidentifying their own verbal material as alien in a task which does
not involve cognitive self-monitoring. This suggests that these symptoms are related to an externalising bias in the processing of
sensory material, and not solely a function of defective self-monitoring.
D 2003 Elsevier B.V. All rights reserved.
Keywords: Speech; Hallucination; Delusion
1. Introduction Most cognitive models of AVHs suggest that internally
Auditory verbal hallucinations (AVHs) are a key
feature of schizophrenia (Slade and Bentall, 1988) and
are usually associated with delusions (Liddle, 1987).
0920-9964/$ - see front matter D 2003 Elsevier B.V. All rights reserved.
doi:10.1016/j.schres.2003.09.008
* Corresponding author.
E-mail address: [email protected] (P.P. Allen).
generated thoughts or images are mistaken for exter-
nally generated events as a consequence of a malfunc-
tion in either a central monitor (Hoffmann, 1986; Frith
and Done, 1988) or in a reality discrimination process
(Bentall, 1990). Reality or source monitoring tasks
require participants to distinguish between memories
of their self-generated material and externally generat-

P.P. Allen et al. / Schizophrenia Research 69 (2004) 277–287278
ed events. Patients who experience hallucinations are
more likely than controls and nonhallucinating patients
to misattribute self-generated items to an external
source (Bental et al., 1991; Morrison and Haddock,
1997). Furthermore, these source-monitoring errors
occur more often when the material is emotional as
opposed to neutral.
However, these tasks require participants to identify
the source of verbal material some time after presenta-
tion or generation. ‘Immediate’ source-monitoring
models propose that AVHs result from impaired moni-
toring of intended speech. Frith and Done’s model
proposes that AVHs and delusions of control result from
a breakdown in the awareness of self-generated action.
The theory is specific to current or the immediate
perception of all motor actions including the genera-
tion of speech. To distinguish between self-generated
and externally generated actions, we rely on a ‘feed
forward’ signal of our intentions to an internal monitor
(Blakemore et al., 2002). According to this model,
hallucinations and other positive symptoms can be
conceptualised as resulting from a breakdown in the
systemsmonitoring the current intention tomake actions
(including the generation of inner speech). Consequent-
ly, self-generated inner speech is misidentified as ‘alien’
and perceived as externally generated ‘voices’.
According to Frith’s model, self-monitoring applies
to all thoughts and motor actions (including verbal
actions) and impairments should effect the monitoring
of overt speech as well as inner speech. This model is
supported by data from studies that have engaged
verbal self-monitoring by experimentally manipulat-
ing auditory verbal feedback while patients spoke
aloud (Cahill et al., 1996; Johns et al., 2001). Altering
the acoustic characteristics of participants’ speech (by
distorting it) introduced a disparity between the
expected and perceived sound of the speech. Partic-
ipants were required to make self/nonself judgements
about the source of speech that was fed back to them.
In both studies, patients with schizophrenia who were
experiencing hallucinations and delusions were more
likely than controls to make errors of misattribution
(misidentify their own speech as alien) when it was
distorted. Moreover, they made more identification
errors when the words they read were derogatory as
opposed to neutral or positive (Johns et al., 2001).
While all these findings are consistent with Frith’s
model, they could equally be explained by an external-
ising response bias (Bentall, 1990; Brebion et al.,
2000) independent of impairments in verbal self-mon-
itoring. A response bias is apparent when participants
fail to recognise the source of a word or a thought and
misattribute it to an external speaker.
The aim of the present study was to measure
response bias independent of self-monitoring. Spe-
cifically, we examined whether the misidentification
of speech described by Cahill et al. (1996) and Johns
et al. (2001) would still be evident if their paradigm
was modified such that participants did not generate
speech, but made auditory judgements about the
source of recorded speech. Thus, participants pas-
sively listened to recordings of their own and an-
other person’s previously recorded speech, with the
speech distorted on a proportion of the trials to
increase uncertainty as to its source. The rationale
for the use of alien speech in the design of this study
was to test whether or not the hypothesised response
bias was specific to the subjects own speech, as
opposed to a general perceptual or voice discrimi-
nation failure that would affect both self-generated
and external speech.
We tested the hypothesis that, even in the absence
of a self-monitoring component, patients with halluci-
nations and delusions would still demonstrate a sig-
nificant externalising response bias.
2. Method
2.1. Participants
2.1.1. Patient groups
All patients were recruited through the South
London and Maudsley NHS Trust, met DSM-IV
criteria for schizophrenia and were on regular stable
doses of antipsychotic medication (as assessed from
the patient’s medication charts). Medication com-
prised of both typical and atypical antipsychotics.
Patients’ symptoms were assessed on the day of
testing using the Scale for the Assessment of Positive
Symptoms (SAPS; Andreason, 1984), the Scale for
Assessment of Negative Symptoms (SANS; Andrea-
son, 1984) and the Calgary Depression Scale (CDSS).
Reports of symptoms were corroborated with medical
notes. IQ was estimated using the NART 2nd edition
(Nelson and O’Connell, 1978).
nia Research 69 (2004) 277–287 279
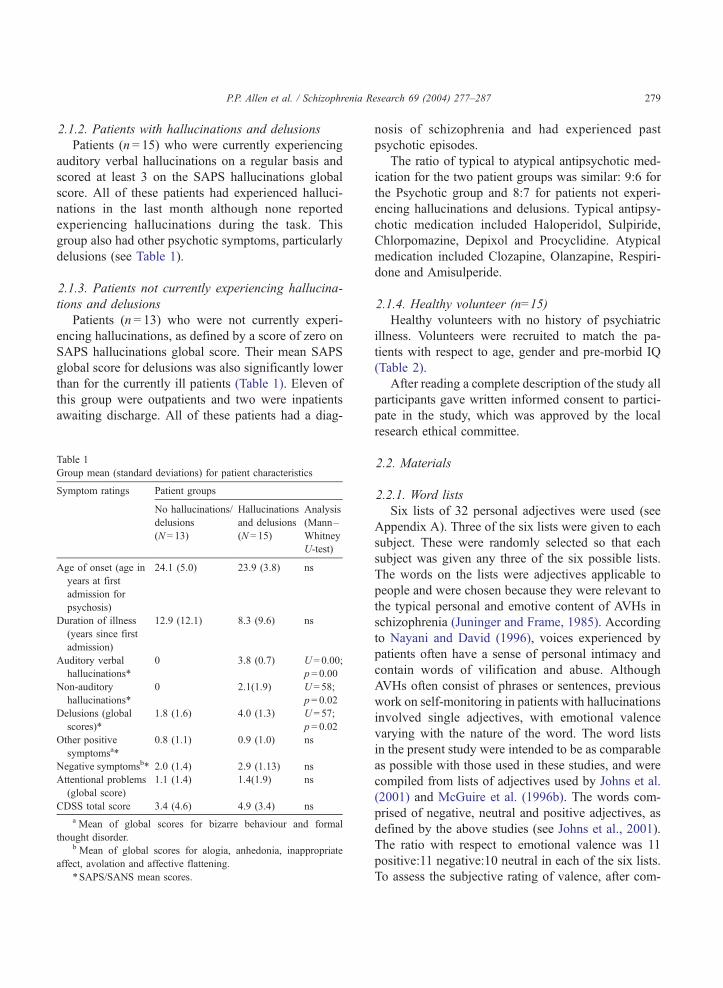
2.1.2. Patients with hallucinations and delusions
Patients (n = 15) who were currently experiencing
auditory verbal hallucinations on a regular basis and
scored at least 3 on the SAPS hallucinations global
score. All of these patients had experienced halluci-
nations in the last month although none reported
experiencing hallucinations during the task. This
group also had other psychotic symptoms, particularly
delusions (see Table 1).
2.1.3. Patients not currently experiencing hallucina-
tions and delusions
Patients (n = 13) who were not currently experi-
encing hallucinations, as defined by a score of zero on
SAPS hallucinations global score. Their mean SAPS
global score for delusions was also significantly lower
than for the currently ill patients (Table 1). Eleven of
this group were outpatients and two were inpatients
awaiting discharge. All of these patients had a diag-
P.P. Allen et al. / Schizophre
Table 1
Group mean (standard deviations) for patient characteristics
Symptom ratings Patient groups
No hallucinations/
delusions
(N= 13)
Hallucinations
and delusions
(N= 15)
Analysis
(Mann–
Whitney
U-test)
Age of onset (age in
years at first
admission for
psychosis)
24.1 (5.0) 23.9 (3.8) ns
Duration of illness
(years since first
admission)
12.9 (12.1) 8.3 (9.6) ns
Auditory verbal
hallucinations*
0 3.8 (0.7) U = 0.00;
p= 0.00
Non-auditory
hallucinations*
0 2.1(1.9) U = 58;
p= 0.02
Delusions (global
scores)*
1.8 (1.6) 4.0 (1.3) U = 57;
p= 0.02
Other positive
symptomsa*
0.8 (1.1) 0.9 (1.0) ns
Negative symptomsb* 2.0 (1.4) 2.9 (1.13) ns
Attentional problems
(global score)
1.1 (1.4) 1.4(1.9) ns
CDSS total score 3.4 (4.6) 4.9 (3.4) ns
a Mean of global scores for bizarre behaviour and formal
thought disorder.b Mean of global scores for alogia, anhedonia, inappropriate
affect, avolation and affective flattening.
*SAPS/SANS mean scores.
nosis of schizophrenia and had experienced past
psychotic episodes.
The ratio of typical to atypical antipsychotic med-
ication for the two patient groups was similar: 9:6 for
the Psychotic group and 8:7 for patients not experi-
encing hallucinations and delusions. Typical antipsy-
chotic medication included Haloperidol, Sulpiride,
Chlorpomazine, Depixol and Procyclidine. Atypical
medication included Clozapine, Olanzapine, Respiri-
done and Amisulperide.
2.1.4. Healthy volunteer (n=15)
Healthy volunteers with no history of psychiatric
illness. Volunteers were recruited to match the pa-
tients with respect to age, gender and pre-morbid IQ
(Table 2).
After reading a complete description of the study all
participants gave written informed consent to partici-
pate in the study, which was approved by the local
research ethical committee.
2.2. Materials
2.2.1. Word lists
Six lists of 32 personal adjectives were used (see
Appendix A). Three of the six lists were given to each
subject. These were randomly selected so that each
subject was given any three of the six possible lists.
The words on the lists were adjectives applicable to
people and were chosen because they were relevant to
the typical personal and emotive content of AVHs in
schizophrenia (Juninger and Frame, 1985). According
to Nayani and David (1996), voices experienced by
patients often have a sense of personal intimacy and
contain words of vilification and abuse. Although
AVHs often consist of phrases or sentences, previous
work on self-monitoring in patients with hallucinations
involved single adjectives, with emotional valence
varying with the nature of the word. The word lists
in the present study were intended to be as comparable
as possible with those used in these studies, and were
compiled from lists of adjectives used by Johns et al.
(2001) and McGuire et al. (1996b). The words com-
prised of negative, neutral and positive adjectives, as
defined by the above studies (see Johns et al., 2001).
The ratio with respect to emotional valence was 11
positive:11 negative:10 neutral in each of the six lists.
To assess the subjective rating of valence, after com-

Table 2
Participants’ mean age, mean NART (standard deviations) and gender ratio
Controls (N = 15) No hallucinations/delusions
(N = 13)
Hallucinations/delusions
(N= 15)
Analysis
Age in years 33.1 (10.45) 34.7 (8.71) 32.9 (9.78) F = 0.82; p= 0.37
NART 112 (7.11) 108 (6.13) 105 (8.8) F = 0.193; p= 0.19
Gender ratio M/F 13:2 12:1 13:2
P.P. Allen et al. / Schizophrenia Research 69 (2004) 277–287280
pletion of the task, participants rated each of the words
that had been presented on a scale of � 3 to + 3.
Words were considered negative if their mean rating
was between � 3 and � 1, neutral between � 0.9 and
+ 1 and positive between + 1.1 and + 3.
2.2.2. Auditory stimuli
Recorded speech was distorted by a DSP.FX digital
effects processor (Windows 95), which lowered the
pitch by 4 semitones (for words in the distorted
condition). This degree of pitch shift was chosen
because it made the speaker’s voice harder to recog-
nise without making the word incomprehensible.
Members of staff at the Institute of Psychiatry (one
male and one female) recorded the words for the
nonself condition (48 words in total). The rationale
for the use of alien speech in the design of this study is
to test whether or not the hypothesised response bias is
specific to external misattributions (i.e. self to other
misattributions) as opposed to a general perceptual or
voice discrimination failure. Purpose-built software
(programmed in visual basic V4) was used to present
the stimuli and to record the response of the subject.
2.3. Design
There were two sources of speech (self, alien) and
two levels of distortion (0, � 4 semitones). Thus, each
list of 32 words consisted of eight self, eight self distor-
ted, eight alien and eight alien distorted words. Three
lists were given to each subject making a total of 96
trials (24 for each experimental condition). The order of
conditions was randomised across the set of six lists.
2.3.1. Independent variables
Speech source (self, alien), distortion level (0, � 4
semitones), word type (negative, neutral, positive),
subject group (controls, patients not experiencing
hallucinations and delusions, patients with hallucina-
tions and delusions).
2.3.2. Dependent variables
Errors in identifying word source and the reaction
time for a response. This was therefore a mixed within
and between subjects repeated measures design.
2.4. Procedure
Participants were informed upon recruitment that
the experiment would be conducted over two ses-
sions. It was explained by the researcher that the first
session would be used to record their speech and the
second session would be used to administer the task.
2.4.1. First session
The participants were asked to read all 96 words
even though half would subsequently be presented
to them in an alien voice. This particular measure
was undertaken to ensure that participants could not
make judgements based on source information
when subsequently presented with the recorded
words. Participants were not instructed to try and
remember the words they had read. Thus, the task
relied on perceptual discrimination as opposed to
source memory.
Before the second session, the designated words on
each list were pitch shifted by � 4 semitones or
replaced with the alien version of the word. Care
was taken to ensure that the volume levels of both
the participants’ speech and the alien speech were as
close as possible to ensure that differential volume
could not subsequently be used to discriminate be-
tween the two types of speech. Three play lists (one for
each word list) were then constructed on the computer
for use in the task itself.
2.4.2. Second session
This took place 1–2 days after the first session.
This interval was the same for all participants. The
subject sat opposite the experimenter across a desk
on which the computer was placed. The computer

P.P. Allen et al. / Schizophrenia Research 69 (2004) 277–287 281
monitor could be clearly seen by the participants,
who sat approximately 30–40 cm from the com-
puter monitor and fixated on a central cross. To
minimise articulation of the words by participants
no words were presented on the computer screen
(only through the headphones). Participants wore
headphones and the volume was checked to ensure
that it was at a level sufficient for them to hear the
speech without difficulty. A button box connected
to the computer was placed in front of the subject.
Participants did not generate any speech and were
told to listen carefully to the stimuli presented in
the headphones. If they thought the speech they
heard was their own they were to press the button
marked ‘self’. If they were unsure of its source
they were to press the button marked ‘unsure’, and
if they thought the speech belonged to someone
else they were asked to press a button marked
‘other’. Participants were asked to make responses
as quickly as possible and not to talk during the
task.
After hearing each word participants had 4.5 s to
respond. The computer recorded the response
choice and the reaction time. When participants
made their response an ‘S’ ‘U’ or ‘O’ (for ‘self’/
‘unsure’/‘other’) appeared on the computer monitor
to confirm that the participants’ response choice
had been logged by the computer (this helped the
experimenter to assess if participants were under-
taking the task properly). There was 14 s between
the presentations of each word (a long ISI was
chosen so that the task could be used in a func-
tional magnetic resonance imaging study at a later
date). The total testing time was 40–45 min.
All participants successfully completed the three
word lists. None of the patients reported experiencing
hallucinations while attempting to complete the task.
The assessment of psychopathology and IQ testing
were carried out after completion of the task. The
entire second session took approximately 1 h for
controls and 1.5 h for patients (mainly due to the
SAPS/SANS interview).
2.4.3. Hypotheses
(1) Patients with hallucinations and delusions will
make more misattribution errors when identifying
their own distorted speech than the patients not
experiencing hallucinations and delusions and the
control group.
(2) Patients with hallucinations and delusions will be
more prone than the other groups to making errors
when the words are emotional (as opposed to
neutral).
2.4.4. Data analysis
The data were analysed using Excel V7 (prelimi-
nary analysis) and Statistical Package for Social Sci-
ence (SPSS).
2.4.5. Analysis of variance
Arcsine transformations were performed so that all
error data met the assumption of normal distribution.
Arcsine transformation is recommended for propor-
tional data (Howell, 1992). The transformed data were
analysed using an ANOVA for repeated measures. The
within-subjects factors were source of speech (self,
alien), distortion (0, � 4 semitones) and emotional
valence (negative, neutral, positive). The between
subjects factor was group (controls, patients not expe-
riencing hallucinations and delusions, patients with
hallucinations and delusions). Separate ANOVAs were
conducted with total errors, unsure responses, misat-
tribution errors and reaction times as the dependent
variable. Misattribution errors occurred when partic-
ipants misattributed the source of the speech (i.e.
responding with ‘other’ when the source of the speech
was self and vice versa), as opposed to errors when
participants responded with ‘unsure’ or made a null
response.
3. Results
3.1. Errors
The groups were compared in terms of (a) total
errors (unsure +misattributed responses), (b) unsure
responses and (c) misattribution errors. The mean
proportions of correct, unsure and misattributed
responses are shown in Tables 3 and 4.
3.1.1. Total errors
There was a significant main effect of source of
speech (F = 9.71 df = 1, 40 p = 0.003). Participants
generally made more errors during the self-trials than
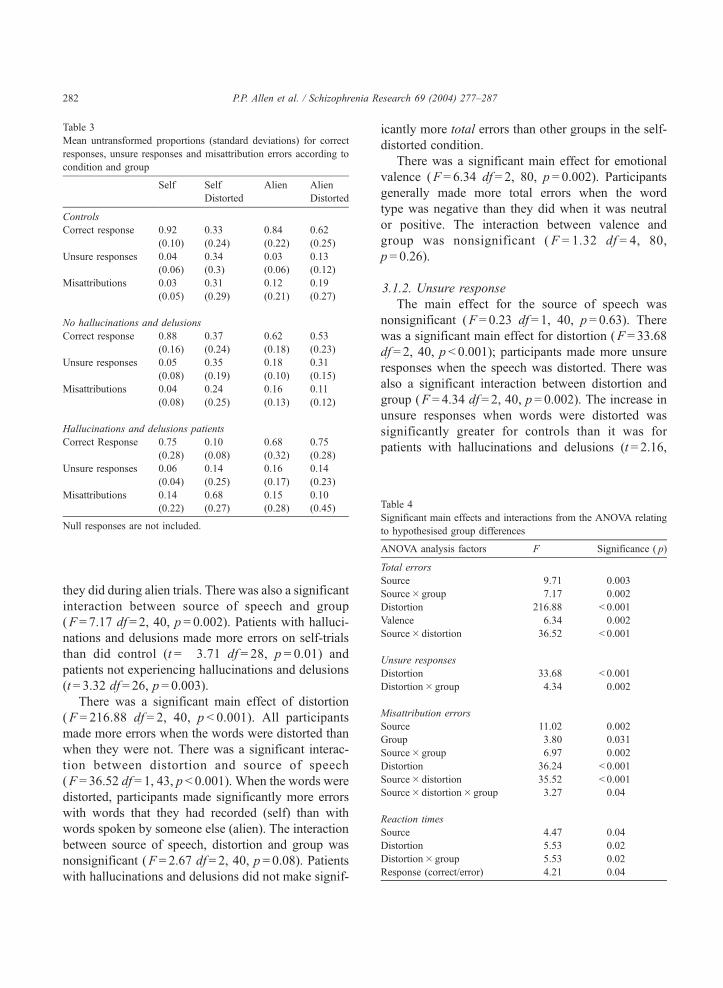
Table 3
Mean untransformed proportions (standard deviations) for correct
responses, unsure responses and misattribution errors according to
condition and group
Self Self
Distorted
Alien Alien
Distorted
Controls
Correct response 0.92
(0.10)
0.33
(0.24)
0.84
(0.22)
0.62
(0.25)
Unsure responses 0.04
(0.06)
0.34
(0.3)
0.03
(0.06)
0.13
(0.12)
Misattributions 0.03
(0.05)
0.31
(0.29)
0.12
(0.21)
0.19
(0.27)
No hallucinations and delusions
Correct response 0.88
(0.16)
0.37
(0.24)
0.62
(0.18)
0.53
(0.23)
Unsure responses 0.05
(0.08)
0.35
(0.19)
0.18
(0.10)
0.31
(0.15)
Misattributions 0.04
(0.08)
0.24
(0.25)
0.16
(0.13)
0.11
(0.12)
Hallucinations and delusions patients
Correct Response 0.75
(0.28)
0.10
(0.08)
0.68
(0.32)
0.75
(0.28)
Unsure responses 0.06
(0.04)
0.14
(0.25)
0.16
(0.17)
0.14
(0.23)
Misattributions 0.14
(0.22)
0.68
(0.27)
0.15
(0.28)
0.10
(0.45)
Null responses are not included.
Table 4
Significant main effects and interactions from the ANOVA relating
to hypothesised group differences
ANOVA analysis factors F Significance ( p)
Total errors
Source 9.71 0.003
Source� group 7.17 0.002
Distortion 216.88 < 0.001
Valence 6.34 0.002
Source� distortion 36.52 < 0.001
Unsure responses
Distortion 33.68 < 0.001
Distortion� group 4.34 0.002
Misattribution errors
Source 11.02 0.002
Group 3.80 0.031
Source� group 6.97 0.002
Distortion 36.24 < 0.001
Source� distortion 35.52 < 0.001
Source� distortion� group 3.27 0.04
Reaction times
Source 4.47 0.04
Distortion 5.53 0.02
Distortion� group 5.53 0.02
Response (correct/error) 4.21 0.04
P.P. Allen et al. / Schizophrenia Research 69 (2004) 277–287282
they did during alien trials. There was also a significant
interaction between source of speech and group
(F = 7.17 df = 2, 40, p = 0.002). Patients with halluci-
nations and delusions made more errors on self-trials
than did control (t =� 3.71 df = 28, p = 0.01) and
patients not experiencing hallucinations and delusions
(t= 3.32 df = 26, p = 0.003).
There was a significant main effect of distortion
(F = 216.88 df = 2, 40, p < 0.001). All participants
made more errors when the words were distorted than
when they were not. There was a significant interac-
tion between distortion and source of speech
(F = 36.52 df = 1, 43, p < 0.001). When the words were
distorted, participants made significantly more errors
with words that they had recorded (self) than with
words spoken by someone else (alien). The interaction
between source of speech, distortion and group was
nonsignificant (F = 2.67 df= 2, 40, p = 0.08). Patients
with hallucinations and delusions did not make signif-
icantly more total errors than other groups in the self-
distorted condition.
There was a significant main effect for emotional
valence (F = 6.34 df = 2, 80, p = 0.002). Participants
generally made more total errors when the word
type was negative than they did when it was neutral
or positive. The interaction between valence and
group was nonsignificant ( F = 1.32 df = 4, 80,
p = 0.26).
3.1.2. Unsure response
The main effect for the source of speech was
nonsignificant (F = 0.23 df = 1, 40, p = 0.63). There
was a significant main effect for distortion (F = 33.68
df = 2, 40, p < 0.001); participants made more unsure
responses when the speech was distorted. There was
also a significant interaction between distortion and
group (F = 4.34 df = 2, 40, p = 0.002). The increase in
unsure responses when words were distorted was
significantly greater for controls than it was for
patients with hallucinations and delusions (t = 2.16,

Table 5
Mean reaction times (in milliseconds + standard deviation) for
correct and errors trials (standard deviation) by source condition
Self
correct
Self
error
Alien
correct
Alien
error
Controls 531
(58)
884
(100)
784
(94)
1021
(183)
No hallucinations
and delusions
667
(99)
974
(136)
1074
(405)
1158
(112)
Hallucinations
and delusions
945
(180)
772
(124)
1078
(145)
1075
(225)
P.P. Allen et al. / Schizophrenia Research 69 (2004) 277–287 283
p = 0.04). The comparison between the two patient
groups was nonsignificant (t = 1.22, p = 0.20). The
interaction between source of speech, distortion and
group was nonsignificant ( F = 0.55 df = 2, 40,
p = 0.58).
3.1.3. Misattribution errors
There was a significant main effect for source of
speech (F = 11.02 df = 1, 40, p = 0.002); participants
made significantly more misattribution errors when
hearing their own speech. There was a significant
main effect of distortion (F = 36.24 df = 1, 40,
p < 0.001). For all participants, misattribution errors
were significantly more common when the words
were distorted. There was a significant between-
subjects effect for group (F = 3.80 df = 1, 40,
p = 0.031). Also, there was a significant interaction
between source of speech, distortion and group
(F = 3.27 df = 2, 40, p = 0.04). Table 3 showed that
in the self-distorted condition patients with halluci-
nations and delusions made more misattribution
errors (selecting ‘other’ when hearing their own
voice) than both controls (t =� 3.6, p= 0.001) and
patients not experiencing hallucinations and delu-
sions (t =� 4.2, p < 0.001). There were no signifi-
cant variations between the groups in the other
three conditions (self undistorted, alien undistorted
or alien distorted). We predicted that the proportion
of errors that were misattributions as opposed to
unsure responses would be greater in the patients
with hallucinations and delusions. To test this the
proportion of misattribution errors was calculated
for only those trials on which participants had
made errors. Thus the types of errors made by
participants could be examined. The data was
analysed using a one-way ANOVA. There was a
significant difference between the groups when
listening to self distorted speech (F = 5.11 df = 2,
40, p = 0.01): 75% of errors made by patients with
hallucinations and delusions were misattribution
errors compared to 39% for patients not experienc-
ing hallucinations and delusions and 46% for con-
trols. The main effects and interactions for valance
were nonsignificant.
A bivariate correlational analysis was performed
to examine the association between misattribution
errors and symptom ratings other than hallucination
scores in the patient groups. Neither SAPS global
delusions score (r = 0.27 p = 0.20) nor SAPS total
scores (r = 0.27 p = 0.17) were significantly correlat-
ed with misattribution errors in the self-distorted
condition. As would be expected, SAPS global
hallucination scores were positively correlated with
errors in the self-distorted condition (r= 0.52 p =
0.009). There were no significant correlations be-
tween SAPS hallucination scores and any of the
other stimuli conditions.
3.2. Reaction times
To assess if task accuracy across groups was related
to response speed, mean reaction times were calculated
for correct and error trials and are shown in Table 5
(mean, as opposed to median, reaction times were used
as the data were not skewed). There was no main effect
of group across conditions ( F = 0.83 df = 1, 40,
p= 0.92). Patients were not generally slower or faster
than controls. For all participants, there was a main
effect for source of speech (F = 4.47 df = 1, 40,
p= 0.04): reaction times were significantly faster for
the participants’ own speech. There was also a signif-
icant main effect for distortion (F = 5.53 df= 1, 40,
p = 0.02): reaction times were significantly slower
when the words were distorted. There was an interac-
tion between distortion and group (F = 9.18 df = 2, 40,
p = 0.01). Controls had significantly faster reaction
times during nondistorted trials than both the patient
groups. Conversely they were significantly slower to
respond than both patient groups when the words were
distorted.
Reaction times for correct responses were signifi-
cantly faster than those for incorrect responses
(F = 4.21, df = 1, 40, p = 0.04). A multiple compari-

P.P. Allen et al. / Schizophrenia Research 69 (2004) 277–287284
sons test revealed that correct responses were signif-
icantly faster than unsure responses ( p < 0.001). How-
ever, the difference in reaction times between correct
responses and misattribution errors was nonsignificant
( p = 0.33). There was a trend for patients with hallu-
cinations and delusions to make incorrect decisions
faster than controls when responding in the self-
condition. However, this interaction just failed to
reach significance (F = 2.92 df = 1, 40, p = 0.06).
4. Discussion
This study examined whether the link between
hallucinations and delusions in schizophrenia and
the tendency to make external misattributions was
related to defective self-monitoring or alternatively,
could be explained in terms of an externalising re-
sponse bias.
Participants made judgements about the source
of pre-recorded speech, which was either their own
or somebody else’s, and was either distorted or
undistorted. The results indicated that patients with
schizophrenia currently experiencing hallucinations
and delusions were more likely to make external
misattributions about the source of their own dis-
torted speech than controls and patients not expe-
riencing these symptoms. This distinction between
patients with hallucinations and delusions and the
other groups was specific to the effect of distortion
on self-generated words, and was specific to errors
of attribution (i.e. misidentification of self-generated
speech as alien), as opposed to being unsure.
Patients with hallucinations and delusions did make
more total errors than the other groups for self
generated words; however, this was not specific to
the effects of distortion. The tendency to misattrib-
ute distorted self-generated speech to an external
source was particularly associated with hallucina-
tions as opposed to delusions or positive symptoms
in general.
Since the paradigm did not involve participants
generating verbal material, performance of the task
did not require verbal self-monitoring (although we
cannot exclude the possibility that subjects may
have been covertly generating the words as they
heard them). Cognitive models in which defective
self-monitoring is central to AVHs (Frith, 1987,
1992) would therefore predict that there would be
no difference (or less difference) between patients
with hallucinations and controls on this task. How-
ever, we found that patients with hallucinations and
delusions were prone to making external misattri-
butions about their own distorted speech. Indeed,
the results resembled those previously evident when
patients with hallucinations and delusions were
studied using the original version of the paradigm
in which participants read the words aloud (Cahill
et al., 1996; Johns et al., 2001). The present data
indicate that impaired self-monitoring cannot entire-
ly account for the tendency for patients with
hallucinations and delusions to make external attri-
butions, suggesting that another factor, such as an
externalising bias when processing unusual percep-
tual information (Bentall, 1990), might be operative.
A deficit in top-down processing which effected the
interpretation of auditory stimuli would produce
similar effects whether patients were evaluating
words that they spoke ‘on-line’ or that they were
listening to.
In all participants, the greatest proportion of total
errors was seen for negative words, although partic-
ipants were also prone to making more errors when
the words they heard were positive (rather than
neutral). This is consistent with previous studies
which have demonstrated that both psychiatric and
nonpsychiatric participants make more source moni-
toring errors with emotional rather than neutral mate-
rial (Morrison and Haddock, 1997). However, even
though patients with current hallucinations and delu-
sions tended to make more errors than controls and
patients not experiencing these symptoms when the
word type was negative this trend was nonsignificant.
This may have been due to the small group sizes:
previous research involving larger groups has found
that patients with current psychotic symptoms are
particularly likely to make more errors with negative
material, especially when the feedback is ambiguous
(Johns et al., 2001).
Analysis of the participants’ reaction times indi-
cated that all participants were significantly faster
when making correct as opposed to incorrect
responses. This trend was due to slower reaction
times for unsure responses rather than misattribution
errors. However, there was a tendency (just missing
significance) for patients with hallucinations and

P.P. Allen et al. / Schizophrenia Research 69 (2004) 277–287 285
delusions to respond more quickly than controls when
they made errors in the self-condition. Interestingly,
controls had the fastest reaction times in the non-
distorted condition but the slowest reaction times
when the speech was distorted, taking longer than
both patient groups (due to control participants’
tendency to make unsure responses in this condition).
The reaction times for the patient groups were similar
in both distortion conditions. Thus, when presented
with ambiguous stimuli, patients with schizophrenia
were faster at making judgements (whether correct or
incorrect) about the source of the speech than con-
trols. People with delusions may make probabilistic
judgements faster than healthy volunteers because
they ‘jump to conclusions’ (Hemsley, 1988). As all
our patients had delusions, it is possible that their
faster reaction times reflected the use of a similar
reasoning style in making judgements about the
source of ambiguous sensory stimuli (Fleminger,
1994).
As well as differing with respect to the severity
of delusions, patients not experiencing hallucina-
tions and delusions had lower levels of positive
symptoms in general than the currently ill patients,
raising the possibility that differences in task per-
formance were a function of the overall severity of
illness at the time of testing. Although the tendency
to misattribute self-generated speech was not corre-
lated with the severity of psychotic symptoms, this
might be better clarified by repeating the study with
patients matched more closely on the severity of
their illness. For example, patients could be
grouped according to specific symptoms (i.e.
patients with both hallucinations and delusions
compared to a group with delusions but not hallu-
cinations). When a group of subjects with delusions
but no hallucinations were studied using the ‘on-line’
version of the task (in which subjects did articulate the
words), their performance regarding misattribution
errors was intermediate between patients with both
hallucinations and delusions and a control group (Johns
et al., 2001).
Two other possibilities should be discussed regard-
ing the interpretation of these results as an external-
ising bias specific to patients with current psychotic
symptoms. Firstly, it is possible that the results reflect a
tendency of an individual to claim that an item was
presented from a specific source when they are actu-
ally unsure about its origin (Snodgrass and Corwin,
1988). In other words, when subjects were uncertain
regarding the source of the speech and ‘made a guess’
they may have been bias to respond with an external
attribution. However, in the present study, in addition
to the ‘self’ and ‘other’ responses, subjects were also
able to register an ‘unsure’ response. Thus, when
participants were in doubt about the source of the
speech, they were not obliged to make a forced choice
between ‘self’ and ‘other’, making it more likely that
when they did select either of these responses they did
so with some degree of confidence.
The results could also be interpreted in terms of
a more general problem with voice discrimination,
rather than a specific externalising bias. However,
one would assume that if patients had problems
with voice discrimination (as oppose to source
attribution) they would be more likely to make
‘unsure’ responses. However, this was not the case:
patients with hallucinations and delusions made
more misattribution errors than the other groups
but fewer unsure responses.
Moreover, one would expect a problem with
voice discrimination to have similar effects on self
and alien speech, but patients with hallucinations
and delusions were particularly likely to make
misattributions when it was their own speech (as
opposed to alien speech) that was distorted. This is
reflected in the currently ill patients’ increased
accuracy in the alien-distorted condition. This can
be considered an artefact of an externalising re-
sponse bias (i.e. if patients tend to answer ‘other’
when confronted with ambiguous stimuli they will
inevitably be correct when the speech is indeed that
of another). Finally, when presented with unambig-
uous speech (i.e. undistorted speech) patients with
hallucinations and delusions made correct responses
well above chance. Therefore, we believe that the
findings do not provide evidence for a voice
discrimination failure.
Acknowledgements
We are grateful to The Wellcome Trust Travelling
Fellowship awarded to Cynthia H.Y. Fu and The
Medical Research Council UK Studentship to Paul P.
Allen.
d e f
careful (AD) brainy (A) scruffy (S)
hot (AD) unbiased (SD) blamed (SD)
Appendix (continued)
P.P. Allen et al. / Schizophrenia Research 69 (2004) 277–287286
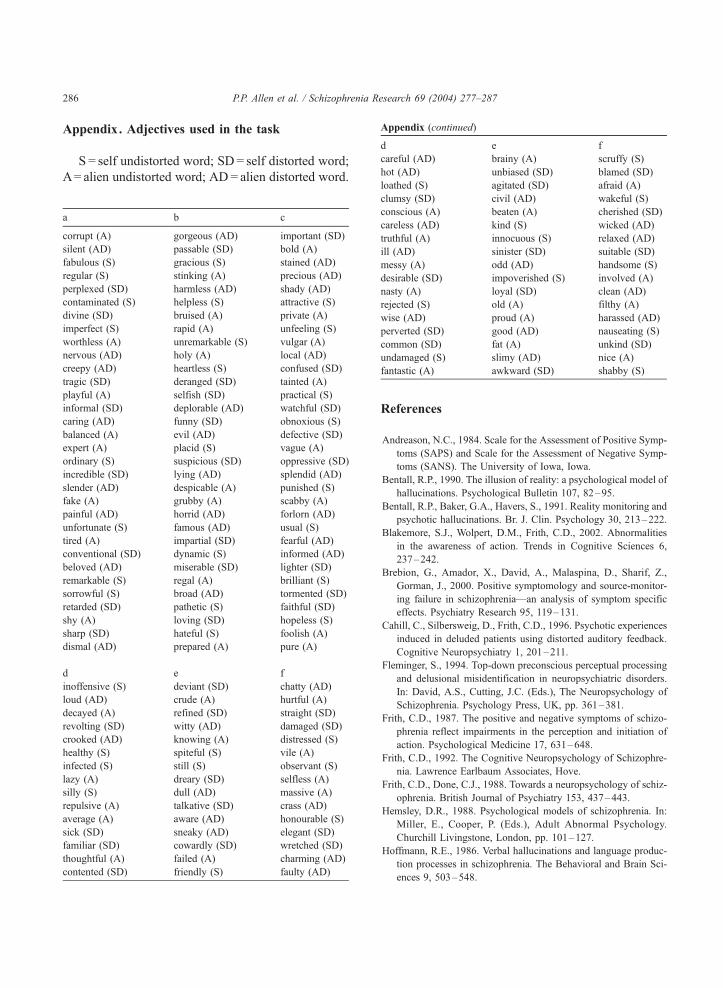
Appendix. Adjectives used in the task
S = self undistorted word; SD= self distorted word;
A= alien undistorted word; AD= alien distorted word.
a b c
corrupt (A) gorgeous (AD) important (SD)
silent (AD) passable (SD) bold (A)
fabulous (S) gracious (S) stained (AD)
regular (S) stinking (A) precious (AD)
perplexed (SD) harmless (AD) shady (AD)
contaminated (S) helpless (S) attractive (S)
divine (SD) bruised (A) private (A)
imperfect (S) rapid (A) unfeeling (S)
worthless (A) unremarkable (S) vulgar (A)
nervous (AD) holy (A) local (AD)
creepy (AD) heartless (S) confused (SD)
tragic (SD) deranged (SD) tainted (A)
playful (A) selfish (SD) practical (S)
informal (SD) deplorable (AD) watchful (SD)
caring (AD) funny (SD) obnoxious (S)
balanced (A) evil (AD) defective (SD)
expert (A) placid (S) vague (A)
ordinary (S) suspicious (SD) oppressive (SD)
incredible (SD) lying (AD) splendid (AD)
slender (AD) despicable (A) punished (S)
fake (A) grubby (A) scabby (A)
painful (AD) horrid (AD) forlorn (AD)
unfortunate (S) famous (AD) usual (S)
tired (A) impartial (SD) fearful (AD)
conventional (SD) dynamic (S) informed (AD)
beloved (AD) miserable (SD) lighter (SD)
remarkable (S) regal (A) brilliant (S)
sorrowful (S) broad (AD) tormented (SD)
retarded (SD) pathetic (S) faithful (SD)
shy (A) loving (SD) hopeless (S)
sharp (SD) hateful (S) foolish (A)
dismal (AD) prepared (A) pure (A)
d e f
inoffensive (S) deviant (SD) chatty (AD)
loud (AD) crude (A) hurtful (A)
decayed (A) refined (SD) straight (SD)
revolting (SD) witty (AD) damaged (SD)
crooked (AD) knowing (A) distressed (S)
healthy (S) spiteful (S) vile (A)
infected (S) still (S) observant (S)
lazy (A) dreary (SD) selfless (A)
silly (S) dull (AD) massive (A)
repulsive (A) talkative (SD) crass (AD)
average (A) aware (AD) honourable (S)
sick (SD) sneaky (AD) elegant (SD)
familiar (SD) cowardly (SD) wretched (SD)
thoughtful (A) failed (A) charming (AD)
contented (SD) friendly (S) faulty (AD)
loathed (S) agitated (SD) afraid (A)
clumsy (SD) civil (AD) wakeful (S)
conscious (A) beaten (A) cherished (SD)
careless (AD) kind (S) wicked (AD)
truthful (A) innocuous (S) relaxed (AD)
ill (AD) sinister (SD) suitable (SD)
messy (A) odd (AD) handsome (S)
desirable (SD) impoverished (S) involved (A)
nasty (A) loyal (SD) clean (AD)
rejected (S) old (A) filthy (A)
wise (AD) proud (A) harassed (AD)
perverted (SD) good (AD) nauseating (S)
common (SD) fat (A) unkind (SD)
undamaged (S) slimy (AD) nice (A)
fantastic (A) awkward (SD) shabby (S)
References
Andreason, N.C., 1984. Scale for the Assessment of Positive Symp-
toms (SAPS) and Scale for the Assessment of Negative Symp-
toms (SANS). The University of Iowa, Iowa.
Bentall, R.P., 1990. The illusion of reality: a psychological model of
hallucinations. Psychological Bulletin 107, 82–95.
Bentall, R.P., Baker, G.A., Havers, S., 1991. Reality monitoring and
psychotic hallucinations. Br. J. Clin. Psychology 30, 213–222.
Blakemore, S.J., Wolpert, D.M., Frith, C.D., 2002. Abnormalities
in the awareness of action. Trends in Cognitive Sciences 6,
237–242.
Brebion, G., Amador, X., David, A., Malaspina, D., Sharif, Z.,
Gorman, J., 2000. Positive symptomology and source-monitor-
ing failure in schizophrenia—an analysis of symptom specific
effects. Psychiatry Research 95, 119–131.
Cahill, C., Silbersweig, D., Frith, C.D., 1996. Psychotic experiences
induced in deluded patients using distorted auditory feedback.
Cognitive Neuropsychiatry 1, 201–211.
Fleminger, S., 1994. Top-down preconscious perceptual processing
and delusional misidentification in neuropsychiatric disorders.
In: David, A.S., Cutting, J.C. (Eds.), The Neuropsychology of
Schizophrenia. Psychology Press, UK, pp. 361–381.
Frith, C.D., 1987. The positive and negative symptoms of schizo-
phrenia reflect impairments in the perception and initiation of
action. Psychological Medicine 17, 631–648.
Frith, C.D., 1992. The Cognitive Neuropsychology of Schizophre-
nia. Lawrence Earlbaum Associates, Hove.
Frith, C.D., Done, C.J., 1988. Towards a neuropsychology of schiz-
ophrenia. British Journal of Psychiatry 153, 437–443.
Hemsley, D.R., 1988. Psychological models of schizophrenia. In:
Miller, E., Cooper, P. (Eds.), Adult Abnormal Psychology.
Churchill Livingstone, London, pp. 101–127.
Hoffmann, R.E., 1986. Verbal hallucinations and language produc-
tion processes in schizophrenia. The Behavioral and Brain Sci-
ences 9, 503–548.

P.P. Allen et al. / Schizophrenia Research 69 (2004) 277–287 287
Howell, D.C., 1992. Statistical Methods for Psychologists, 3rd ed.
Duxburry Press, Belmont, CA.
Johns, L.C., Rossell, S., Frith, C., Ahmad, F., Hemsley, D., Kuipers,
E., McGuire, P.K., 2001. Verbal self-monitoring and auditory
verbal hallucinations in patients with schizophrenia. Psycholog-
ical Medicine 31, 705–715.
Juninger, J., Frame, C.L., 1985. Self report of the frequency and
phenomenology of verbal hallucinations. Journal of Nervous
and Mental Diseases 73, 149–155.
Liddle, P.F., 1987. Schizophrenic syndromes, cognitive perform-
ance and neurological dysfunction. Psychological Medicine
17, 49–57.
McGuire, P.K., Silbersweig, D.A., Frith, C.D., 1996b. Functional
neuroanatomy of verbal self-monitoring. Brain 119, 907–917.
Morrison, A.P., Haddock, G., 1997. Cognitive factors in source
monitoring and auditory hallucinations. Psychological Medicine
27, 669–679.
Nayani, T.H., David, S., 1996. The auditory hallucination:
a phenomenological survey. Psychological Medicine 26,
177–189.
Nelson, H.E., O’Connell, A., 1978. Dementia: the estimation of
premorbid intelligence levels using the new adult reading test.
Cortex 14, 234–244.
Slade, P.D., Bentall, R.P., 1988. Sensory Deception: Towards a
Scientific Analysis of Hallucinations. Croom Helm, London.
Snodgrass, J.G., Corwin, J., 1988. Pragmatics of measuring recog-
nition memory: application to dementia and amnesia. Journal of
Experimental Psychology. General 117, 34–50.