minneapolis / st. paul (minnesota) - department of pain...
TRANSCRIPT
Stefan J. Friedrichsdorf, MD, FAAPMedical Director, Department of Pain Medicine, Palliative Care & Integrative MedicineChildren's Hospitals and Clinics of Minnesota, Minneapolis/St. Paul, MN
Associate Professor of Pediatrics, University of Minnesota Medical School
[email protected] Twitter: @NoNeedlessPain
From Schrödinger’s Cat to Myths, Magic, and Methadone: Advanced Pain Treatment in Children with Serious Hematologic/Oncologic Disease
Minneapolis / St. Paul (Minnesota)
Learning Objectives• Critically review risks & safety of analgesic under-treatment
versus over-treatment in children with serious hematologic/oncologic diseases
• Evaluate assumptions about opioid use in children
• Discuss how multiple agents, interventions, rehabilitation, psychological & integrative therapies act synergistically for more effective pediatric pain control with fewer side effects than a single analgesic or modality - and improves patient experience
• Explore how principles of quantum physics might explain effectiveness of pediatric pain treatment modalities

5-year old Marius: Procedural Pain Management
”Redningskvinder” Channel Tv3 - Http://Www.Tv3.Dk/Redningskvinder. (Episode 7, Season 4.) 2014
Don't have enough staff for pediatric pain control...?
Funny, how there is
always enough staff to restrain a child.
Pediatric Analgesia in 1985 “Papoose Boards”
• Breaking News: Gravitational waves (warped space time) from 2 pairs of black holes detected - confirming Einstein
• History of science discovered sequence of better and better theories and models, from Plato to classical theory of Newton to modern quantum theories
• Then came quantum uncertainty, curved space, quarks, strings, and 7 extra
dimensions: Net result of this labor is 10500
universes, each with different laws, only one corresponds to the universe, as we know it it
• “Because the operating system of nature, as far as we understand it, is quantum physics” Hartmut Neven, Director of Quantum Artificial Intelligence Laboratory at Google (Dec 9, 2015)
So, how do we treat the individual pain patient in front of us ?
Hmhh... Spoiler Alert: Crystal-clear answer on 3rd last slide!
• The way we observe the quantum field decide what we see, thus our belief systems determine the reality we experience

Pediatric Cancer: Epidemiology USA
• New cancer diagnosis: > 16,000 children (0-19 years) / year
• Large majority are cured of their malignancy (> 80% of children with cancer are alive 5 years after diagnosis [62% in the mid-1970s]).
• However, children with good fortune to attain cure nonetheless experience considerable suffering
• 1,960 children and adolescents are expected to die due to a malignancy in 2014
1. Ries LAG, Smith MA, Gurney JG, Linet M, Tamra T, Young JL, Bunin GR (eds). Cancer Incidence and Survival among Children and Adolescents: United States SEER Program 1975-1995, National Cancer Institute, SEER Program. NIH Pub. No. 99-4649. Bethesda, MD, 1999; 2. Li J, Thompson TD, Miller JW, Pollack LA, Stewart SL: Cancer Incidence Among Children and Adolescents in the United States, 2001–2003. Pediatrics 2008. 121(6):e1470-7 3. Ries LAG, Melbert D, Krapcho M, et al. (eds). SEER Cancer Statistics Review, 1975–2005. Bethesda, MD: National Cancer Institute. http://seer.cancer.gov/csr/1975_2005 4. Linet MS, Ries LA, Smith MA, Tarone RE, Devesa SS. Cancer surveillance series: recent trends in childhood cancer incidence and mortality in the United States. J National Cancer Inst 1999;91(12):1051-8 5. Morbidity and Mortality Weekly Report. Centers for Disease Control and Prevention, Atlanta, GA. December 7, 2007. 56(48);1257-1261
Heron, M. Deaths: Leading Causes for 2010. National Vital Statistics Reports 2013 May 3, 2014]; Volume 62, Number 6:[Available from: http://www.cdc.gov/nchs/data/nvsr/nvsr62/nvsr62_06.pdf.
Symptom prevalence and distress reported by children with advanced cancer
Wolfe J, Orellana L, Ullrich C et al Symptoms and Distress in Children with Advanced Cancer: Prospective Patient-Reported Outcomes from the PediQUEST Study, JCO 2015.
Outcomes Improved with PPC Involvement
• Parents of children with cancer report less distress from pain, dyspnea and anxiety at EOL Wolfe et al. J Clin Onc 2008
• Children who received PPC/Oncology more likely to have fun (70% versus 45%) and to experience events that added meaning to life (89% versus 63%) Friedrichsdorf SJ et al. J Palliat Med 2015
• Families who received PPC/Oncology report improved communication Kassam A, Skiadaresis J, Alexander S et al Differences in End-of-Life Communication for Children with Advanced Cancer who were Referred to a Palliative Care Team. Pediatr Blood Cancer, 2015. 62(8): p. 1409-13.
• Children receiving PPC experience shorter hospitalizations and fewer emergency department visits Ananth, P., et al., Hospital Use in the Last Year of Life for Children With Life-Threatening Complex Chronic Conditions. Pediatrics, 2015. 136(5): p. 938-46.
Pediatric Pain - Status Quo
• Under treatment of pain in children
• Parents expect pain to be relieved Forgeron PA, Finley GA, Arnaout M. Pediatric pain prevalence and
parents' attitudes at a cancer hospital in Jordan. J Pain Symptom Manage. 2006; 31(5):440-8.
• Priorities of parents of hospitalized children "Taking care of pain" rated as second highest priority (1st: getting right diagnosis) Ammentorp J, Mainz J, Sabroe S. Parents’
priorities and satisfaction with acute pediatric care. Arch Pediatr Adolesc Med 2005;159:127-131
• Parents’ greatest distress: failing to protect their child from pain Tiedeman, M. (1997). Anxiety responses of parents during and
after the hospitalisation of their 5 - to -11 year old children. Journal of Pediatric Nursing, 12(2), 110-119. Melnyk BM. Intervention studies involving parents of hospitalized young children: an analysis of the past and future recommendations. J Pediatr Nurs. 2000 Feb;15(1):4-13.
• Assumption: everything possible is done Anand’s neonatal surgery studies
Pediatric Pain - Status Quo
• USA: adults receive more than two - three times as many analgesic doses as children (with identical diagnoses) (1) Eland JM, Anderson JE: The experience of pain in
children. In: Jacox A (ed). Pain: a source book for nurses and other health care professionals. Boston: Little Brown & C0; 1977:453-78 (2) Beyer JE, DeGood DE, Ashley LC, Russell GA. Patterns of postoperative analgesic use with adults and children following cardiac surgery. Pain. 1983 Sep;17(1):71-81. (3) Schechter NL, Allen DA, Hanson K. Status of pediatric pain control: a comparison of hospital analgesic usage in children and adults. Pediatrics. 1986 Jan;77(1):11-5.
• Compared to adults, pediatric patients receive fewer and/or incorrectly dosed analgesics in daily routine Ellis, J. A., O’Connor, B. V., Cappelli, M., Goodman, J., Blouin, R.,
& Reid, C. W. (2002). Pain in hospitalized pediatric patients: How are we doing? Clinical Journal of Pain, 18, 262-269.
• The younger children are, the less likely they receive appropriate analgesia Broome ME,
Richtsmeier A, Maikler V, Alexander M. Pediatric pain practices: a national survey of health professionals. J Pain Symptom Manage. 1996 May;11(5):312-20.; Nikanne E, Kokki H, Tuovinen K. Postoperative pain after adenoidectomy in children. Br J Anaesth. 1999 Jun;82(6):886-9.
Inappropriate Analgesia: Why Bother...?
• Children with persistent pain suffer more physical symptoms in adult life, more anxiety and more depression 1946 Medical Research Council and 1958 National Child
Development Study
• Inadequate analgesia for initial procedures in children diminishes effect of adequate analgesia in subsequent procedures Weisman SJ, Bernstein B,
Schechter NL: Consequences of inadequate analgesia during painful procedures in children. Arch Pediatr Adolesc Med 1998. 152:147-9
• NICU: increased morbidity & mortality Anand KJ, Barton BA, McIntosh N, Lagercrantz H, Pelausa E, Young TE,
et al. Analgesia and sedation in preterm neonates who require ventilatory support: results from the NOPAIN trial. Neonatal Outcome and Prolonged Analgesia in Neonates. Arch Pediatr Adolesc Med. 1999 Apr;153(4):331-8
• Higher morphine doses = less PTSD in months after major trauma Stoddard FJ, Jr., Sorrentino EA, Ceranoglu TA, Saxe G, Murphy JM, Drake JE,
et al. Preliminary evidence for the effects of morphine on posttraumatic stress disorder symptoms in one- to four-year-olds with burns. J Burn Care Res. 2009 Sep-Oct;30(5):836-43.
• Up to 25% of adults have fear of needles with most fears developing in childhood: avoidance of health care (including non-adherence with vaccination schedules Taddio A, Chambers CT, Halperin SA, et al. Inadequate pain
management duringchildhood immunizations: the nerve of it. Clin Ther 2009;31(Suppl 2):S152-67.)
Myths and Barriers to Using Opioids
Case Scenario:
• You are taking care of a child with severe acute somatic nociceptive pain (e.g. advanced cancer, sickle-cell crisis). It crosses your mind to administer a strong opioid such as morphine or fentanyl.
• What would be the most common concerns you might hear from your colleagues or parents arguing against opioid use in this child?
Common Opioid Assumptions
• Addiction “chronic relapsing condition characterized by persistent, compulsive dependence on a behavior or substance despite adverse consequences”
• Tolerance ≠ addiction
• Pseudo-addiction
• Over Sedation / Respiratory Depression
• Ileus / Constipation
• Medication “Too strong”
• Masking symptoms
• Abdominal Pain Ranji SR, Goldman LE, Simel DL, Shojania KG. Do opiates affect the clinical evaluation of patients with abdominal pain? JAMA 2006: 296:1764-74
• Opioids after major cranial surgery in children do NOT result in altered mental status nor respiratory depression Maxwell LG. PAIN MANAGEMENT FOLLOWING
MAJOR INTRACRANIAL SURGERY IN PEDIATRIC PATIENTS: A PROSPECTIVE COHORT STUDY IN THREE ACADEMIC CHILDREN’S HOSPITALS Pediatric Critical Care Medicine: May 2014 - Volume 15 - Issue 4_suppl - p 77. Abstracts of the 7th World Congress on Pediatric Critical Care
• As always... Think first !(e.g. compartment syndrome?)... analgesia second...
CDC Guideline for Prescribing Opioids for Chronic Pain — United States, 2016
http://www.cdc.gov/mmwr/volumes/65/rr/rr6501e1.htm
• Scope: “patients aged ≥18 years with chronic pain outside of palliative and end-of-life care” and “treating patients with chronic pain (i.e., pain lasting >3 months or past the time of normal tissue healing) in outpatient settings”
• “recommendations do not address the use of opioid pain medication in children or adolescents aged <18 years”
• 12 recommendations, including
• 1. Nonpharmacologic therapy and nonopioid pharmacologic therapy are preferred for chronic pain
• 4. When starting opioid therapy for chronic pain, clinicians should prescribe immediate-release opioids instead of extended-release/long-acting opioids
• 6. Acute pain opioid prescribing: Three days or less will often be sufficient; more than seven days will rarely be needed
• 12. Evidence-based treatment (usually medication-assisted treatment with buprenorphine or methadone in combination with behavioral therapies) for patients with opioid use disorder
Opioid Safety & Long-Term Outcome
• Studies in neonatal rats suggest potential adverse effects of opioids (changes in behavior and brain functioning) Handelmann GE, Dow-Edwards D. Modulation of brain development by morphine: effects on central motor systems and behavior. Peptides. 1985;6 Suppl 2:29-34.
• NEOPAIN multicenter trial: Detailed secondary analysis: Although morphine associated with hypotension among ventilated preterm neonates, it does NOT increase the risk of severe IVH, any IVH, or death Anand KJS, Lancet 2004;363:1673-1682; Richard W, Pediatrics 2005;115:1351-1359
• Higher cumulative fentanyl dose in preterm infants correlated with higher incidence of cerebellar injury, lower cerebellar diameter: No correlation was detected between cumulative fentanyl dose and development at 2 years of age. McPherson, C., Haslam M, Pineda R,
Rogers C, Neil JJ, Inder TE: Brain Injury and Development in Preterm Infants Exposed to Fentanyl. Ann Pharmacother, 2015. 49(12): p. 1291-7.
Long-Term Outcome• Low-dose morphine analgesia
received on NICU associated with early alterations in cerebral structure, short-term neurobehavioral problems; did not persist into childhood: at 7 years no detrimental impacts of morphine on neurobehavioral outcome observed Steinhorn R1, McPherson C2, Anderson
PJ3, Neil J4, Doyle LW5, Inder T6. J Pediatr. 2015 May;166(5):1200-1207.e4. doi: 10.1016/j.jpeds.2015.02.012. Neonatal morphine exposure in very preterm infants-cerebral development and outcomes.
• Long-term outcome at 5-6 years among formerly preterm babies exposed to continuous morphine infusion: No adverse effect of morphine on intelligence, motor function, or behavior MacGregor R, Evans D, Sugden D, Gaussen T, Levene M. Outcome at 5-6 years of prematurely born children who received morphine as neonates. Archives of disease in childhood Fetal and neonatal edition. 1998 Jul;79(1):F40-3.
• Continuous morphine infusion of 10 mcg/kg/h during the neonatal period does not harm general functioning and may even have a positive influence on executive functions at 8 to 9 years. de Graaf, J., R. A. van Lingen, et al. (2013). "Does neonatal morphine use affect neuropsychological outcomes at 8 to 9 years of age?" Pain 154(3): 449-458.
Does analgesia improve outcome?
• Yes, in animal model (Suellen Walker, PhD, London)
• Walker SM, Fitzgerald M, Hathway GJ. Surgical injury in the neonatal rat alters the adult pattern of descending modulation from the rostroventral medulla. Anesthesiology. Jun 2015;122(6):1391-1400.
• Walker SM, Tochiki KK, Fitzgerald M. Hindpaw incision in early life increases the hyperalgesic response to repeat surgical injury: critical period and dependence on initial afferent activity. Pain. Dec 15 2009;147(1-3):99-106.

Heisenberg's Uncertainty Principle
• According to principles of quantum physics (which is an accurate description of nature) a particle has neither a definite position nor definite velocity unless and until those quantities are measured by an observer
• The act of measurement forces the particle to relinquish all the possible place it could have been and select one location where you can find it.
• According to principles of quantum physics (which is an accurate description of nature) a
What are we measuring...?
(1) Nociceptive Pain: arises from the activation of peripheral nerve endings (nociceptors) that respond to noxious stimulation
• Somatic (for example, muscles, joints)
• Chronic somatic pain typically well localized & often results from degenerative processes (such as arthritis)
• Visceral (internal organs)
(2) Neuropathic Pain: resulting from injury to, or dysfunction of, the somatosensory system.
• Central pain: caused by a lesion or disease of the central somatosensory nervous system
(3) Psycho-social-spiritual-emotional Pain / Total Pain
(4) Chronic Pain
• Pain beyond expected time of healing
Pain in children with impaired communication
• Non-communicating Children’s Pain Checklist - Revised (NCCPC-R); postoperative Version (NCCPC-PV) (Breau, 2002)
• Pediatric Pain Profile (PPP) (Hunt, 2003)
• r-FLACC (Malviya 2006)
How Do We Manage Acute Pain in Children?
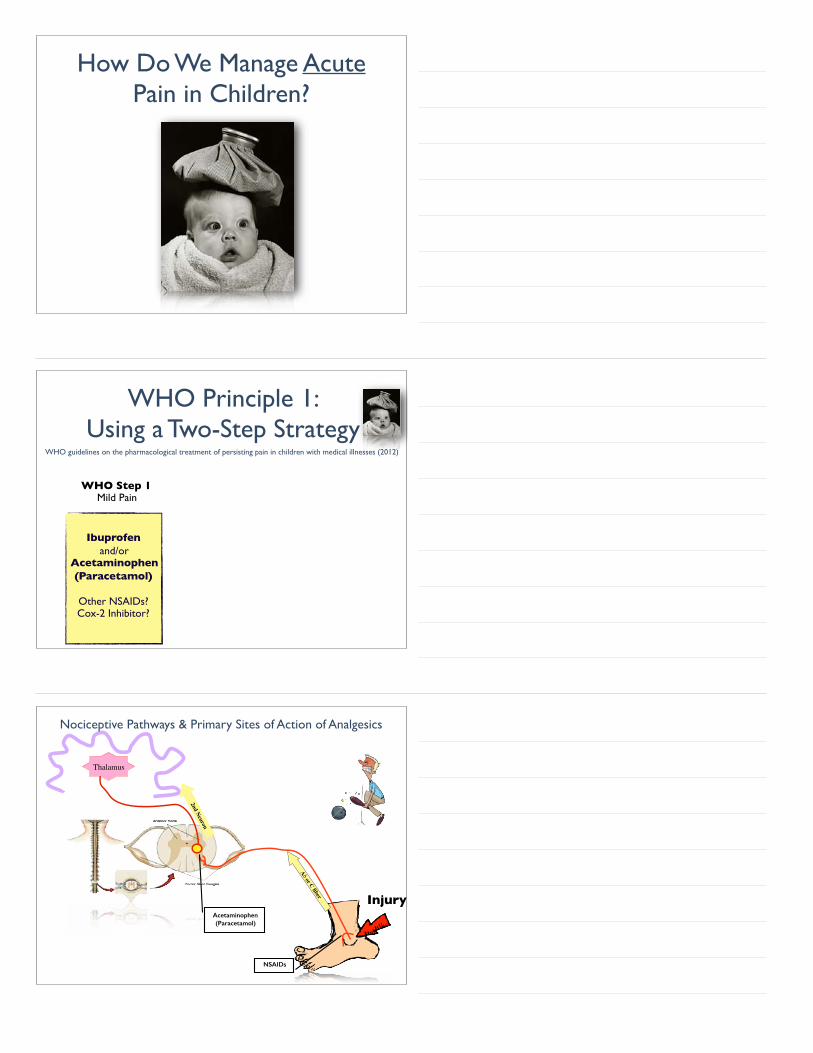
WHO Principle 1: Using a Two-Step Strategy
WHO Step 1Mild Pain
Ibuprofenand/or
Acetaminophen(Paracetamol)
Other NSAIDs?Cox-2 Inhibitor?
WHO guidelines on the pharmacological treatment of persisting pain in children with medical illnesses (2012)
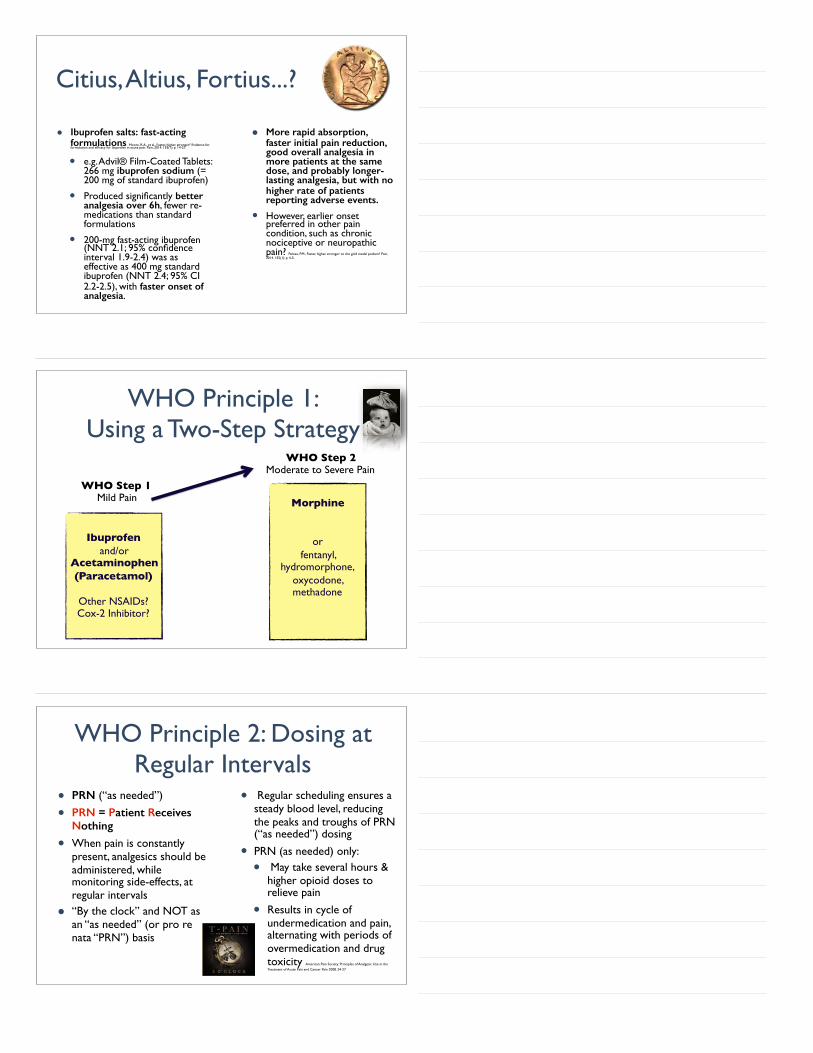
Aδ or C fiber Injury
Thalamus
NSAIDs
Acetaminophen (Paracetamol)
2nd Neuron
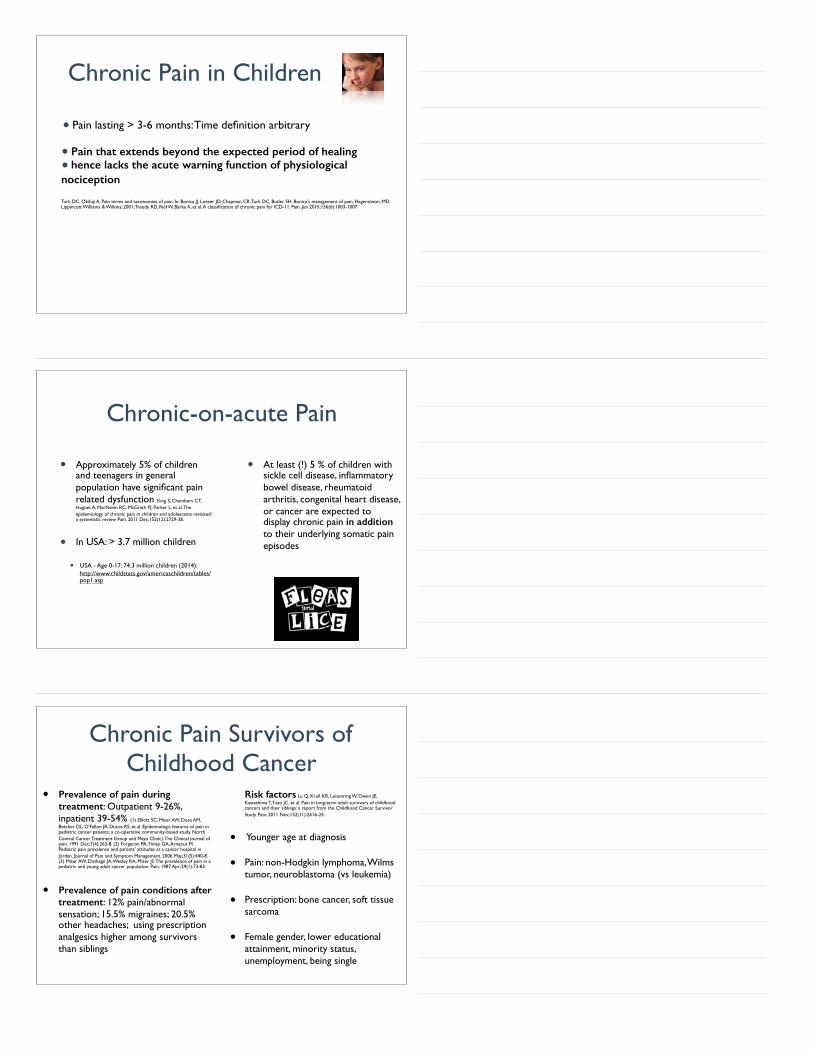
Nociceptive Pathways & Primary Sites of Action of Analgesics
Citius, Altius, Fortius...?
• Ibuprofen salts: fast-acting formulations Moore, R.A., et al., Faster, higher, stronger? Evidence for formulation and efficacy for ibuprofen in acute pain. Pain, 2014. 155(1): p. 14-21.
• e.g. Advil® Film-Coated Tablets: 266 mg ibuprofen sodium (= 200 mg of standard ibuprofen)
• Produced significantly better analgesia over 6h, fewer re-medications than standard formulations
• 200-mg fast-acting ibuprofen (NNT 2.1; 95% confidence interval 1.9-2.4) was as effective as 400 mg standard ibuprofen (NNT 2.4; 95% CI 2.2-2.5), with faster onset of analgesia.
• More rapid absorption, faster initial pain reduction, good overall analgesia in more patients at the same dose, and probably longer-lasting analgesia, but with no higher rate of patients reporting adverse events.
• However, earlier onset preferred in other pain condition, such as chronic nociceptive or neuropathic pain? Peloso, P.M., Faster, higher, stronger: to the gold medal podium? Pain, 2014. 155(1): p. 4-5.
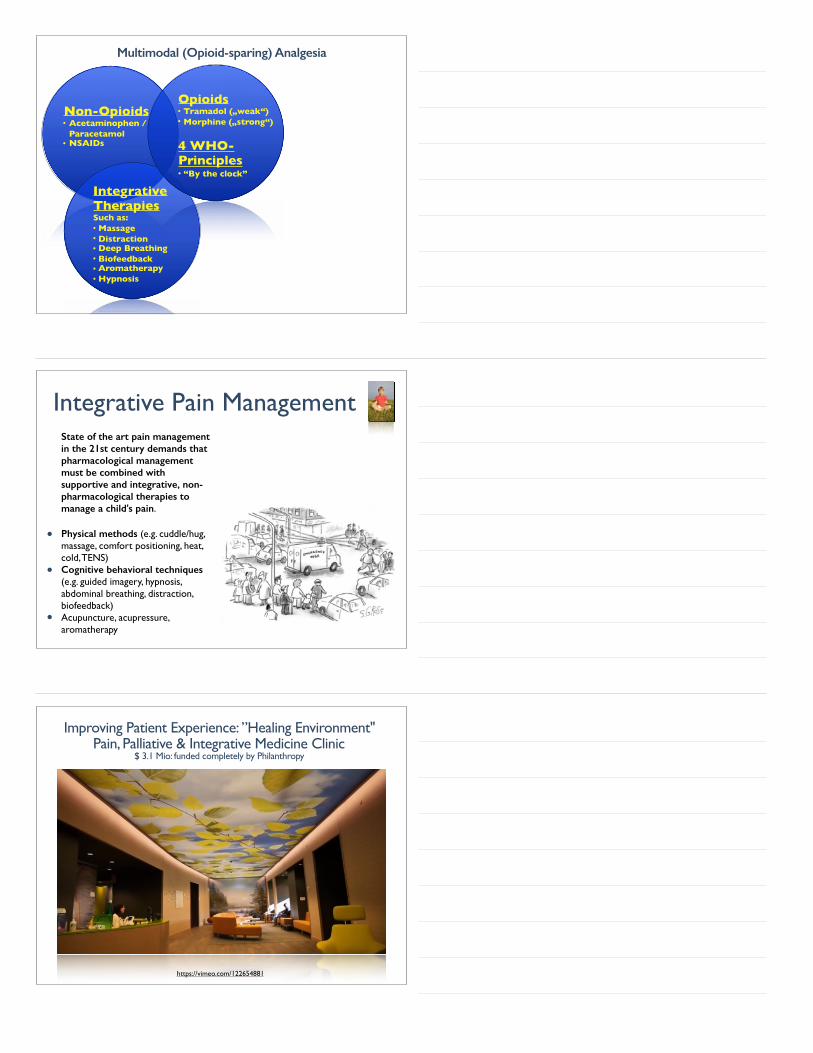
WHO Principle 1: Using a Two-Step Strategy
WHO Step 1Mild Pain
Ibuprofenand/or
Acetaminophen(Paracetamol)
Other NSAIDs?Cox-2 Inhibitor?
Morphine
or fentanyl,
hydromorphone, oxycodone, methadone
WHO Step 2Moderate to Severe Pain
WHO Principle 2: Dosing at Regular Intervals
• PRN (“as needed”)
• PRN = Patient Receives Nothing
• When pain is constantly present, analgesics should be administered, while monitoring side-effects, at regular intervals
• “By the clock” and NOT as an “as needed” (or pro re nata “PRN”) basis
• Regular scheduling ensures a steady blood level, reducing the peaks and troughs of PRN (“as needed”) dosing
• PRN (as needed) only:
• May take several hours & higher opioid doses to relieve pain
• Results in cycle of undermedication and pain, alternating with periods of overmedication and drug toxicity American Pain Society: Principles of Analgesic Use in the
Treatment of Acute Pain and Cancer Pain 2008. 24-27
Non-Opioids• Acetaminophen / Paracetamol• NSAIDs
Multimodal (Opioid-sparing) Analgesia
Integrative TherapiesSuch as:• Massage• Distraction• Deep Breathing• Biofeedback• Aromatherapy• Hypnosis
Opioids• Tramadol („weak“)• Morphine („strong“)
4 WHO-Principles• “By the clock”
Integrative Pain ManagementState of the art pain management in the 21st century demands that pharmacological management must be combined with supportive and integrative, non-pharmacological therapies to manage a child's pain.
• Physical methods (e.g. cuddle/hug, massage, comfort positioning, heat, cold, TENS)
• Cognitive behavioral techniques (e.g. guided imagery, hypnosis, abdominal breathing, distraction, biofeedback)
• Acupuncture, acupressure, aromatherapy
Improving Patient Experience: ”Healing Environment" Pain, Palliative & Integrative Medicine Clinic
$ 3.1 Mio: funded completely by Philanthropy
https://vimeo.com/122654881
Integrative Pain & Symptom Management
• A Pediatrician’s Top 10 Apps for Distraction & Pain Management http://NoNeedlessPain.org
Aδ or C fiber
Nociceptive Pathways & Primary Sites of Action of Analgesics
Injury
Thalamus
NSAIDs
Acetaminophen (Paracetamol)
2nd Neuron
Opioids
Periaqueductalgrey (endorphins)
Descending
Inhibition
+
Integrative (non-pharmacological)
therapies
Descending pathways that modulate transmission of nociceptive signals originate in periaqueductal gray, locus
coeruleus, anterior cingulate gyrus, amygdala & hypothalamus: are relayed through brainstem nuclei in the
PEG and medulla to spinal cord.
Inhibitory transmitters involved in these pathways incl. norepinephrine, 5-hydroxytryptamine, dopamine, &
endogenous opioids.

How does this stuff work...?
• The periaqueductal gray and descending pain modulation: Hemington KS,
Coulombe MA. The periaqueductal gray and descending pain modulation: Why should we study them and what role do they play in chronic pain? Journal of neurophysiology. Feb 11 2015:jn 00998 02014.
• Distraction significantly increased activation of cingulo-frontal cortex including orbitofrontal & perigenual anterior cingulate cortex (ACC), as well as periaquaeductal gray (PAG) & the posterior thalamus.
• Active distraction techniques, such as imagery, appear to modulate endorphine release in the midbrain, including the periaqueductal grey and thereby increase activity of descending inhibiting pathways thereby decreasing nociception from the dorsal horn resulting in gate pain modulation during distraction. Valet M,
Sprenger T, Boecker H, et al. Distraction modulates connectivity of the cingulo-frontal cortex and the midbrain during pain--an fMRI analysis. Pain. Jun 2004;109(3):399-408.; Tracey I, Ploghaus A, Gati JS, et al. Imaging attentional modulation of pain in the periaqueductal gray in humans. The Journal of neuroscience : the official journal of the Society for Neuroscience. Apr 1 2002;22(7):2748-2752.; Derbyshire SW, Osborn J. Modeling pain circuits: how imaging may modify perception. Neuroimaging clinics of North America. Nov 2007;17(4):485-493, ix.; Bingel U, Wanigasekera V, Wiech K, et al. The effect of treatment expectation on drug efficacy: imaging the analgesic benefit of the opioid remifentanil. Sci Transl Med. Feb 16 2011;3(70):70ra14
Aδ or C fiber
Nociceptive Pathways & Primary Sites of Action of Analgesics
Injury
Thalamus
NSAIDs
Acetaminophen (Paracetamol)
2nd Neuron
Opioids
Periaqueductalgrey (endorphins)
“OFF”
Integrative (non-pharmacological)
therapies
“ON”
CORTEX:-Stress- Anxiety- Catastrophizing- Depression- perceived injustice- disturbed Sleep
Regional anesthesia approaches to pain management in PC
• Regional anesthesia: pediatric knowledge limited to case reports and case series: Rork, J.F., C.B. Berde,
and R.D. Goldstein, Regional anesthesia approaches to pain management in pediatric palliative care: a review of current knowledge. J Pain Symptom Manage, 2013. 46(6): p. 859-73.
• central neuraxial infusions
• peripheral nerve and plexus blocks or infusions
• neurolytic blocks
• implanted intrathecal ports & pumps for baclofen, opioids, local anesthetics, and other adjuvants
• Neurolytic Sympathectomy: Amr YM, Makharita MY.
Neurolytic sympathectomy in the management of cancer pain-time effect: a prospective,
randomized multicenter study. J Pain Symptom Manage. Nov 2014;48(5):944-956 e942.
• RCT (n=109) inoperable abdominal or pelvic cancer: better pain control, less opioid consumption, and better quality of
life
Non-Opioids• Acetaminophen / Paracetamol• NSAIDs
Multimodal (Opioid-sparing) Analgesia Friedrichsdorf S: 8th Annual Pediatric Pain Master Class, Minneapolis, MN, June 20-26, 2015
Integrative TherapiesSuch as:• Massage• Distraction• Deep Breathing• Biofeedback• Aromatherapy• Hypnosis
OpioidsSuch as:
• Tramadol („weak“)• Morphine („strong“)
4 WHO-Principles• “By the clock”
AdjuvantsSuch as:• Alpha-Agonist• Gabapentinoids • TCA/Antidepressants• NMDA-Antagonists• Na-channel blockers• Antispasmodics• Benzodiazepines• Corticosteroids• Muscle relaxants• Radiopharmaceuticals • Bisphosphonates
Rehabilitation• Exercise• Physical Therapy• Sleep Hygiene• Occupational Therapy• Child Life
Psychology• CBT
Regional Anesthesia• Neuraxial infusion• Peripheral/Plexus Nerve block• Neurolytic block• Intrathecal port/pump• Intraventricular opioids?• Percutaneous cervical cordotomy?
Multimodal AnalgesiaNo Needless Pain
• On the smallest scale of matter, the whole is more than the sum of its parts
• One could know everything there is to know about a quantum system (particles A + B), and yet know nothing definite about either piece separately
• Our natural inclination to analyze systems into subsystems, and to build up knowledge of the whole from careful study of it's parts, grinds to a halt in the quantum domainKaiser D: How the Hippies Saved Physics. WW Norton & Co. New York, London, 2011
• According to principles of quantum physics
• Pain lasting > 3-6 months: Time definition arbitrary
• Pain that extends beyond the expected period of healing • hence lacks the acute warning function of physiological nociception
Turk DC, Okifuji A. Pain terms and taxonomies of pain. In: Bonica JJ, Loeser JD, Chapman CR, Turk DC, Butler SH. Bonica's management of pain. Hagerstwon, MD: Lippincott Williams & Wilkins; 2001; Treede RD, Rief W, Barke A, et al. A classification of chronic pain for ICD-11. Pain. Jun 2015;156(6):1003-1007.
Chronic Pain in Children
Chronic-on-acute Pain
• Approximately 5% of children and teenagers in general population have significant pain related dysfunction King S, Chambers CT, Huguet A, MacNevin RC, McGrath PJ, Parker L, et al. The epidemiology of chronic pain in children and adolescents revisited: a systematic review. Pain. 2011 Dec;152(12):2729-38.
• In USA: > 3.7 million children
• USA - Age 0-17: 74.3 million children (2014): http://www.childstats.gov/americaschildren/tables/pop1.asp
• At least (!) 5 % of children with sickle cell disease, inflammatory bowel disease, rheumatoid arthritis, congenital heart disease, or cancer are expected to display chronic pain in addition to their underlying somatic pain episodes
Chronic Pain Survivors of Childhood Cancer
• Prevalence of pain during treatment: Outpatient 9-26%, inpatient 39-54% (1) Elliott SC, Miser AW, Dose AM, Betcher DL, O'Fallon JR, Ducos RS, et al. Epidemiologic features of pain in pediatric cancer patients: a co-operative community-based study. North Central Cancer Treatment Group and Mayo Clinic). The Clinical journal of pain. 1991 Dec;7(4):263-8. (2) Forgeron PA, Finley GA, Arnaout M. Pediatric pain prevalence and parents' attitudes at a cancer hospital in Jordan. Journal of Pain and Symptom Management. 2006 May;31(5):440-8. (3) Miser AW, Dothage JA, Wesley RA, Miser JS. The prevalence of pain in a pediatric and young adult cancer population. Pain. 1987 Apr;29(1):73-83.
• Prevalence of pain conditions after treatment: 12% pain/abnormal sensation; 15.5% migraines; 20.5% other headaches; using prescription analgesics higher among survivors than siblings
Risk factors Lu Q, Krull KR, Leisenring W, Owen JE, Kawashima T, Tsao JC, et al. Pain in long-term adult survivors of childhood cancers and their siblings: a report from the Childhood Cancer Survivor Study. Pain. 2011 Nov;152(11):2616-24.
• Younger age at diagnosis
• Pain: non-Hodgkin lymphoma, Wilms tumor, neuroblastoma (vs leukemia)
• Prescription: bone cancer, soft tissue sarcoma
• Female gender, lower educational attainment, minority status, unemployment, being single
Chronic Sickle Cell Pain
• Does chronic SCD pain state only result from patients with nociceptive or inflammatory (vasculopathic) pain, recurrent nearly every day?
• Ischemic veno-occlusive pain not opioid-responsive?
• Model of “Chronic post surgical pain” transition from acute to chronic pain applies?
• Does persistent pain state represent neuropathic pain?
• “Daily” SCD pain in fact chronic musculo-skeletal pain?
Communication with Patient / Family
• Pain is real!
• First “function” gets better, then “pain” (not other way around)
• Positive Expectation = Self-fulfilling prophecy
• Physical Therapy • Daily home exercise
• Integrative Medicine • Self-Hypnosis• Biofeedback• Progressive Muscle relaxation• Daily home exercise
• Passive: Massage, Acupuncture • Psychology (...if missing school) • Normalize Life
• Sports/Exercise• Sleep-hygiene• Social: Having daily fun• School: Attending full-time (or school-re-entry plan)
• Family Coaching • Medications...???
Communication with Patient / Family What is the Hard Work...and non-negotiable...?
Medications ???
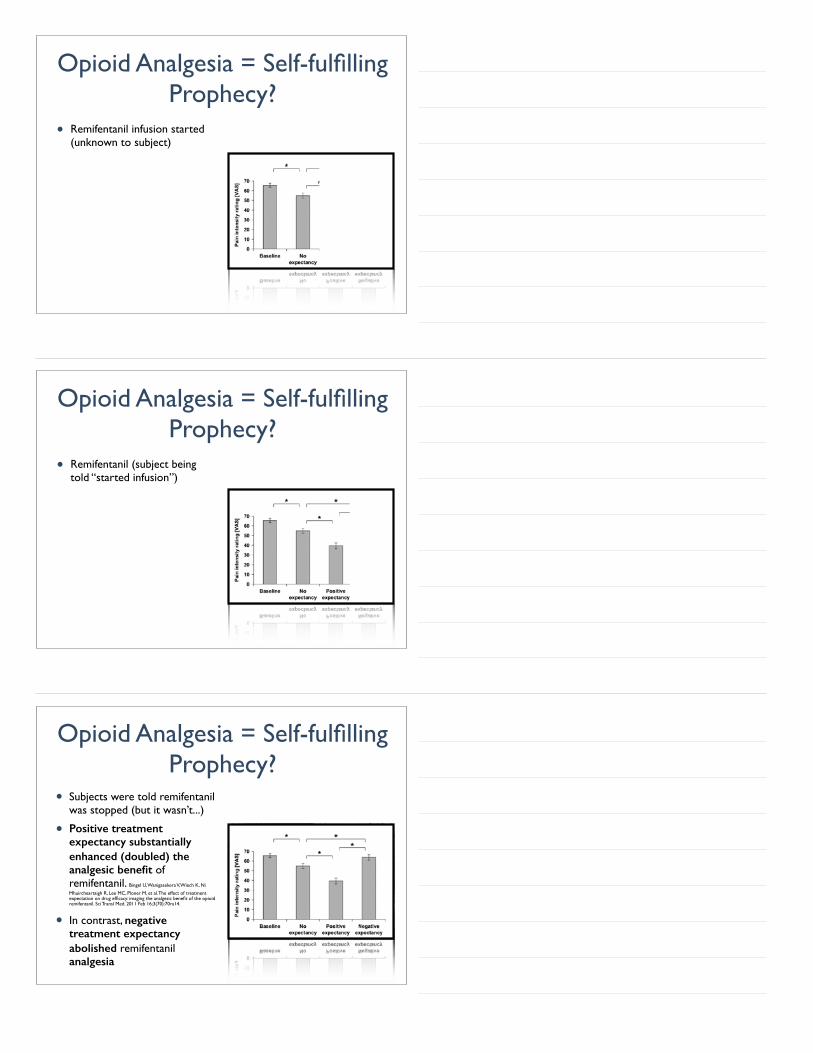
1. Low-dose Amitriptyline(stimulates)
Opioids in the absence of tissue injury or inflammation
not indicated!
2. Gabapentin(inhibits)
3. Acetaminophen 4. Ibuprofen (Celecoxib?)
5. Lidocain 5% patch6. Melatonin7. Vitamin D ?8. SSRI ?9. Co-Q10, Fish-Oil/Omega 3000, Peppermint oil
(coated) [for abdo pain]?
Exit Interview
Multimodal Analgesia• Multimodal (opioid-sparing)
analgesia: Multiple agents, interventions, rehabilitation, psychological and integrative therapies act synergistically for more effective pediatric pain control with fewer side effects than single analgesic or modality
• 2016 Guidelines on the Management of Postoperative Pain Management of Postoperative Pain: A Clinical Practice Guideline From the American Pain Society, the American Society of Regional Anesthesia and Pain Medicine, and the American Society of Anesthesiologists' Committee on Regional Anesthesia, Executive Committee,
and Administrative Council Tegethoff, M., et al., Comorbidity of Mental Disorders
and Chronic Pain: Chronology of Onset in Adolescents of a National Representative Cohort. J Pain, 2016. 17(2): p. -131-57
• (Adults): Multimodal analgesia therapy (versus PCA only) reduces length of hospitalization in patients undergoing surgery Michelson, J.D., R.A. Addante, and M.D. Charlson, Multimodal analgesia therapy reduces length of hospitalization in patients undergoing fusions of the ankle and hindfoot. Foot Ankle Int, 2013. 34(11): p. 1526-34.
Multimodal=
Awesome!

Schrödinger’s famous, or notorious, Cat
• cat imagined as being enclosed in a box with a radioactive source and a poison that will be released when the source (unpredictably) emits radiation, the cat being considered (according to quantum mechanics) to be simultaneously both dead and alive until the box is opened and the cat observed - caught between two irreconcilable states
Does a strong opioid treat acute pain… or not?
Opioid Analgesia = Self-fulfilling Prophecy?
• Saline (Placebo)
• 22 healthy adults were exposed to pain-provoking heat and also given the opioid remifentanil Bingel U, Wanigasekera V, Wiech K, Ni Mhuircheartaigh R, Lee MC, Ploner M, et al. The effect of treatment expectation on drug efficacy: imaging the analgesic benefit of the opioid remifentanil. Sci Transl Med. 2011 Feb 16;3(70):70ra14.
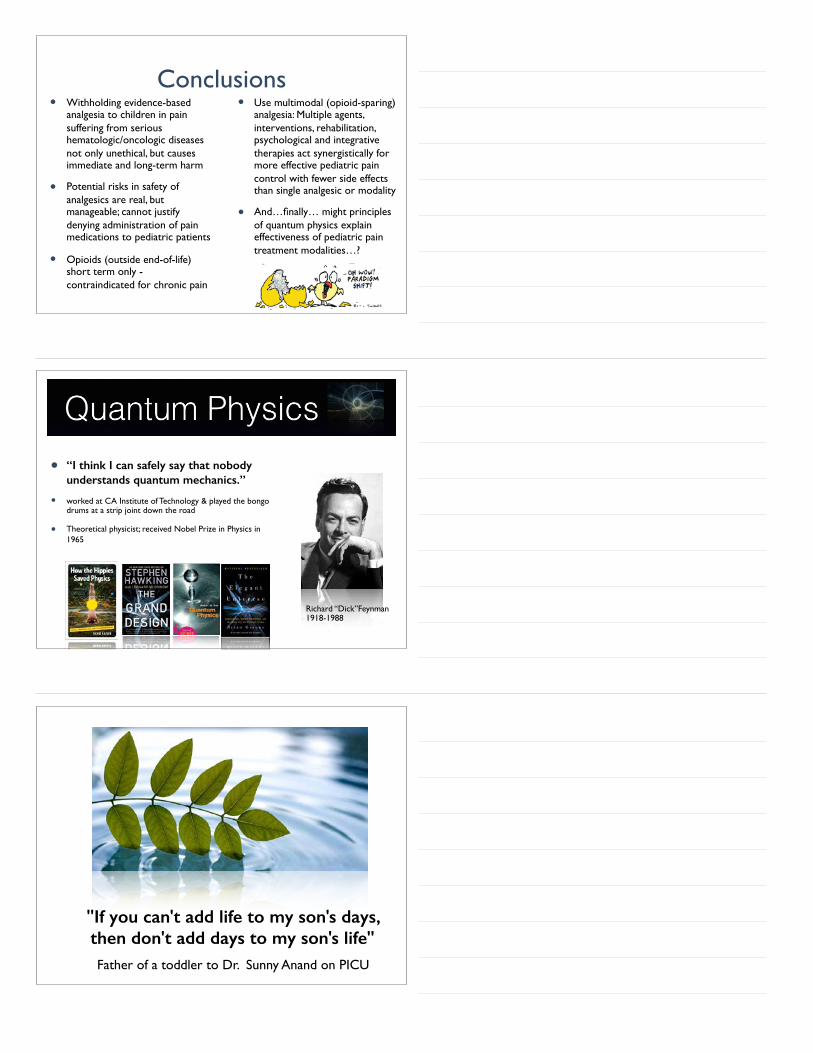
Opioid Analgesia = Self-fulfilling Prophecy?
• Remifentanil infusion started (unknown to subject)
• Remifentanil (subject being told “started infusion”)
Opioid Analgesia = Self-fulfilling Prophecy?
• Subjects were told remifentanil was stopped (but it wasn’t...)
• Positive treatment expectancy substantially enhanced (doubled) the analgesic benefit of remifentanil. Bingel U, Wanigasekera V, Wiech K, Ni
Mhuircheartaigh R, Lee MC, Ploner M, et al. The effect of treatment expectation on drug efficacy: imaging the analgesic benefit of the opioid remifentanil. Sci Transl Med. 2011 Feb 16;3(70):70ra14.
• In contrast, negative treatment expectancy abolished remifentanil analgesia
Opioid Analgesia = Self-fulfilling Prophecy?
Do you remember Marius...?How about a Plan B?
LET Anesthesia• Sitting upright
• Distraction
• Topical Anesthesia
• 3mL LET-gel: Lidocaine 4%-Epinephrine 0.18% -Tetracaine 0.5%
Singer AJ, Stark MJ. Pretreatment of lacerations with lidocaine, epinephrine, and tetracaine at triage: a randomized double-blind trial. Acad Emerg Med. 2000 Jul;7(7):751-6.
Crystal clear answer:
So, how do we treat the individual pain patient in front of us ?
Σωκράτη Sōkrátēs; 470/469 – 399 BC
Conclusions• Withholding evidence-based
analgesia to children in pain suffering from serious hematologic/oncologic diseases not only unethical, but causes immediate and long-term harm
• Potential risks in safety of analgesics are real, but manageable; cannot justify denying administration of pain medications to pediatric patients
• Opioids (outside end-of-life) short term only - contraindicated for chronic pain
• Use multimodal (opioid-sparing) analgesia: Multiple agents, interventions, rehabilitation, psychological and integrative therapies act synergistically for more effective pediatric pain control with fewer side effects than single analgesic or modality
• And…finally… might principles of quantum physics explain effectiveness of pediatric pain treatment modalities…?
• “I think I can safely say that nobody understands quantum mechanics.”
• worked at CA Institute of Technology & played the bongo drums at a strip joint down the road
• Theoretical physicist; received Nobel Prize in Physics in 1965
Richard “Dick”Feynman 1918-1988
"If you can't add life to my son's days, then don't add days to my son's life" Father of a toddler to Dr. Sunny Anand on PICU
With profound gratitude to our interdisciplinary Pain, Palliative & Integrative Medicine team
Physician
• Kris Catrine, MD
• Kaci Osenga, MD
• Kathleen Farah, MD
• Stefan Friedrichsdorf, MD
• Matt Armfield, MD, Pain Fellow
• Meghan Young, MD, Palliative Care Fellow
Nurse Practitioner
• Barb Symalla, RN, CNS
• Nancy Jaworski, RN, CNS
• Kathy Popp, RN, CNS
• Sarah Thu, RN, CNS
• Anna Hoffman, RN, CNS
• Maura Fitzgerald, RN, CNP
• Jennifer Worley, RN, CNSPsychology
• Kavita Desai, PhD
• Jade Raffety, PhD
• Jennifer Waters, PhD
Physical Therapy
• Andrew Warmuth, DPT
• Eva Frank, PT
Research / Quality Improvement / Lean
• Andrea Postier
• Donna Eull, RN
• Christian Weidner, BS
• Lexie Goertzen
• Laurie Foster
• Jule Yang
Palliative Nursing
• Sarah Hasse, RN
• Michael McLoone
Social Work
• Martha Schermer, LiCSW
• Cyndee Daughtree
• Jessica Convey
• Chaplain: Hal Weiden
• Child Life: Margaret Monsoon
• Music Therapy: Mark Burnet
• Clinic nurse: Blanche Amar
Massage
• Candace Linaris
• Jill Maltrud
• Laura Beck
Admin Assistants
• Katie McQuire
• Cheryl Puumala
Clinic staff
• Brock Hebert
• Allison McQuade
Manager
• Tracey Crocoll
• Liz Leighton, RN
Further Links• The New York Times (Dec 16, 2015) essay by Dr. Stefan Friedrichsdorf “When a Baby Dies” http://
opinionator.blogs.nytimes.com/2015/12/16/when-a-baby-dies/?_r=1
• Video: Kiran Stordalen and Horst Rechelbacher Pediatric Pain, Palliative and Integrative Medicine Clinic Tour https://vimeo.com/122654881
• “Children’s Comfort Promise: Doing everything possible to treat and prevent pain.” Eliminating Needle Pain in children (Feb 2015) Staff video: http://vimeo.com/106286508
• Short Movie: Meet the Interdisciplinary Chronic Pain Clinic Team at Children’s Minnesota: LittleStars TV https://www.youtube.com/watch?t=13&v=Bb1fHxfjdWI
• Video: Tour of the Kiran Stordalen and Horst Rechelbacher Pediatric Pain, Palliative and Integrative Medicine Clinic at Children's Hospitals and Clinics of Minnesota and an overview of the three programs that are offered at Children's under this clinic. https://vimeo.com/123357296
• Short Movie: LittleStarsFilm 'Kali's Story - Beyond the NICU': This amazing pediatric palliative care short movie (7 min) features 8-year-old Kali's journey at Children's Hospitals and Clinics of Minnesota from NICU to today, receiving care by the Pain & Palliative & Integrative Medicine program while inpatient, in the clinic, and at home (Jan 22, 2015) http://www.littlestars.tv/short-films/beyond-the-nicu
Twitter: @NoNeedlessPain
Stefan J. Friedrichsdorf, MD, FAAP Medical Director, Department of Pain Medicine, Palliative Care & Integrative Medicine
Associate Professor of Pediatrics, University of Minnesota Medical School
Children's Hospitals and Clinics of Minnesota2525 Chicago Ave S | Minneapolis, MN 55404 | USA
612.813.6450 phone | 612.813.7199 fax
[email protected]://www.childrensmn.org/painpalliativeintegrativemed
Further Training: [email protected]
10th Annual Pediatric Pain Master Class • Minneapolis, Minnesota, USA | June 17-23, 2017
Education in Palliative & End-of-life Care [EPEC]: Become an EPEC-Pediatrics Trainer • Montréal, Québec, Canada | April 29-30, 2017 (Professional Development Workshop: 04/28/17)
Blog: http://NoNeedlessPain.org