methods for improving drug release from poly( ethyl)methacrylate bone cement
TRANSCRIPT
Clinical Materials 7 (1991) 221-231
r Improving Drug Rel 1)methacrylate Bone
Institute of Brthopaedics, Stanmore, Middlesex HA7 4LP, UK
(Received IQ September 1990 ; accepted 15 December 1990)
Abstract: Poly(methylmethacrylate) (PMMA) is a widely used material with both dental and orthopaedic applications. The acrylic cement is produced by the combination of polymethylacrylate beads with methylmethacrylate monomer. After polymerisation, a heterogeneous and porous matrix is formed which can be used to deliver therapeutic agents. In this work, the release of antibiotic, growth hormone and serum albumin is demonstrated. The mechanism is similar for all agents; a rapid release followed by a slow continuous release. The quantity of drug released depends upon the formulation of both the PMMA and the drug. The polymer-to-monomer ratio can greatly affect the ratio of drug release; increased polymer-to-monomer ratio leads to increased release of antibiotic. Optimum release is achieved if a crystalline formulation of the drug is used rather than a fine powder.
Experimental methods to improve the drug release performance of bone cements are presented
TRODUCTION
Poly(methylmethacrylate) (PMMA) bone cement has been widely used in orthopaedic surgery to fix the metal prosthesis to bone in total joint replace- ment. Its secondary function has been to act as a carrier and delivery agent for therapeutic agents. The use of poly(methylmethacrylate) to deliver antibiotics to prevent deep wound infection has been well documented by Bucholzl and is now commonly used to prevent sepsis. In more recent experimental studies, PMMA has been used to deliver human growth hormone which may stimu- late new bone formation at the bonexement interface.2 Several mechanisms of drug release from PMMA have been suggested.3m7 The controversy over the mode of release appears to be due to the fact that the release is not simple diffusion nor does the drug transfer across the cement matrix via the pores and channels in the cement. The release is a surface phenomenon and the total quantity of drug released arises only from the outer surface layer of the cement.’ In this work, the author demonstrates
how PMMA can be used to deliver a range of therapeutic agents and investigates experimental methods to increase the performance of P a drug delivery agent.
MATERIALS AN S
Preparation of bone cement
Poly(methylmethacrylate) bone cements are com- posed of a powder polymer component and a liquid monomer component, which are mixed in the ratio 2: 1. The powder component consists of prepolymerised methylmethacrylate and benzoyl peroxide (catalyst). The liqui monomeric methylmethacrylate and N, p-toluidine (catalyst). In these additives (antibiotic, growth hor were added to the powder thoroughly mixed before the liquid component was added. The cement was mixed for l-3 min, until a dough-like paste was formed whit was placed in a PTFE mould. The cement was allowed to poly-
227
Clinical Ma/e&is 0267-6605/9!/$03.50 0 1991 Elsevier Science Publishers Ltd, England
228 Sandra Downes
merise for 30 min at room temperature and then the cement discs (3 mm diameter, 2 mm thickness) were removed.
Elution studies
The elution of antibiotic (gentamicin sulphate), human growth hormone and bovine serum albumin from PMMA was monitored in vitro. Ten blocks of each cement were placed in 10 ml phosphate buffered saline (PBS) in individual containers and continuously mixed at 37 “C. The elution fluid was removed at regular time intervals and assayed for the additive. A fresh aliquot of PBS was added to the cement blocks and the container returned to the rolamixer. The gentamicin assay was performed using Syva EMIT with a Cobas Bio Analyser. The growth hormone assay was a specific Enzyme- Linked-Immunoassay. Albumin was assayed by the Bio-Rad protein method (Bio-Rad Laboratories GmbH, Watford, UK).
Effect of monomer-to-polymer ratio
Antibiotic-loaded bone cement blocks were made, using 0.25 g Gentamicin sulphate to IO g polymer. Three different monomer-to-polymer ratios were used: 1: 1.5, 1: 2 and 1: 2.5. Five blocks of each cement type were placed in 5 ml PBS and the samples continuously rolamixed at 37 “C. At regular time intervals the PBS was removed and replaced. The gentamicin concentration was moni- tored using an EMIT assay (Syva). The surface morphologies of these blocks of cement were investigated using scanning electron microscopy. The blocks of cement were fixed to aluminium stubs (31 x 5 mm). The surfaces were sputter-coated with gold prior to examination in the microscope (IS1 Super) with a 15 kV accelerating voltage.
Formulation of the drug
Blocks of cement were made using 30 mg albumin in 5 g polymer with the addition of 2.5 ml monomer to make up the cement. One set of cement samples was made up using albumin as a lyophilised powder and one set with albumin in the crystalline form. A number of cement discs were placed in individual bottles containing 2 ml phosphate buffered saline (PBS). The bottles were rolamixed constantly at 37 “C. At regular time intervals the PBS was removed and replaced with fresh PBS. The elutant was assayed for protein using the Bio-Rad protein
method (Bio-Rad Laboratories GmbH, Watford, UK).
RESULTS
Release of antibiotic, growth hormone and albumin from PMMA
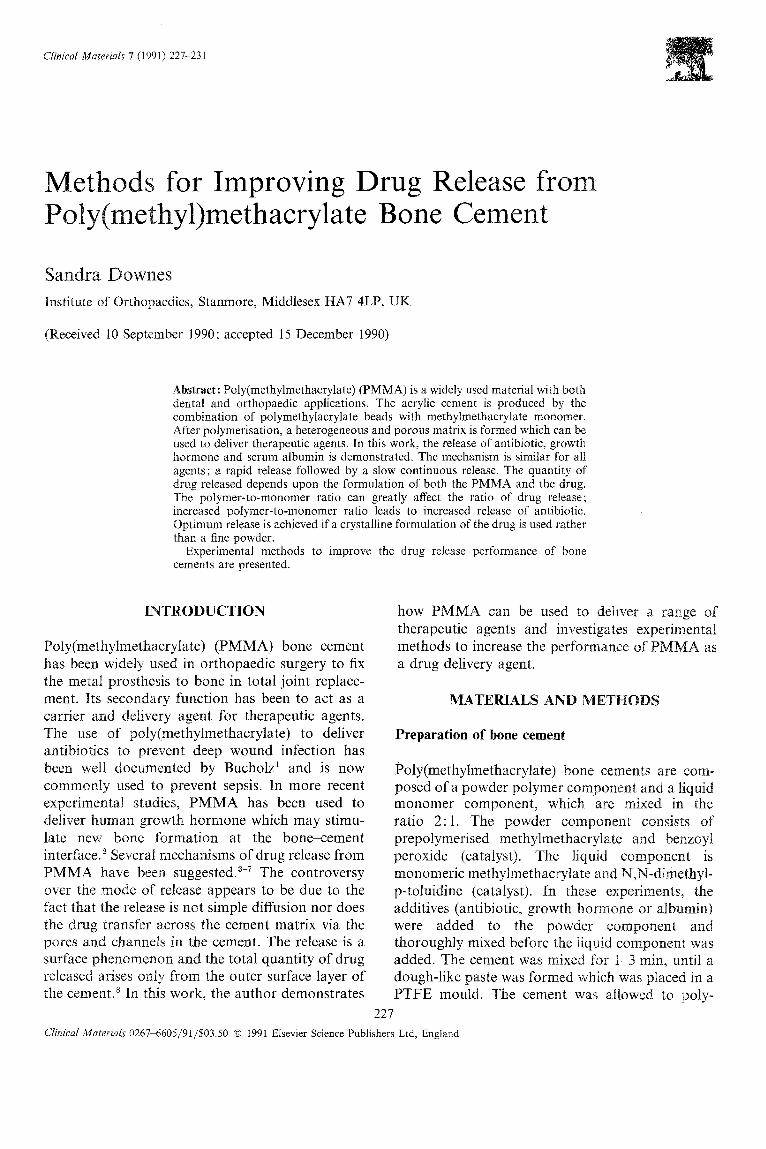
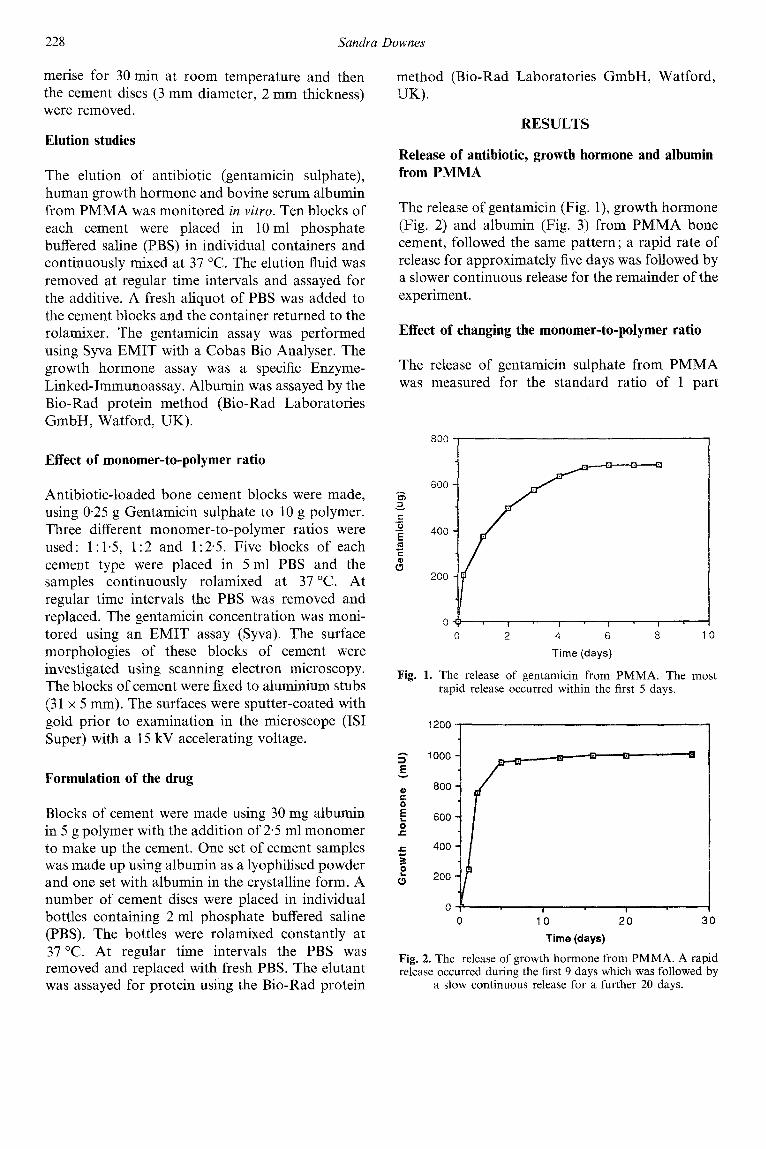
The release of gentamicin (Fig. l), growth hormone (Fig. 2) and albumin (Fig. 3) from PMMA bone cement, followed the same pattern ; a rapid rate of release for approximately five days was followed by a slower continuous release for the remainder of the experiment.
Effect of changing the monomer-to-polymer ratio
The release of gentamicin sulphate from PMMA was measured for the standard ratio of 1 part
800,
600
400
200
0 2 4 6
Time (days)
8 10
Fig. 1. The release of gentamicin from PMMA. The most rapid release occurred within the first 5 days.
5 1000
5 i? 800
i! 0’ 600
Jz
0 10 20 :
Time (days)
1
Fig. 2. The release of growth hormone from PMMA. A rapid release occurred during the first 9 days which was followed by
a slow continuous release for a further 20 days.
Drug release from poly(meth,yl)methacrylate bone cement 229
10 20 30 Time (days)
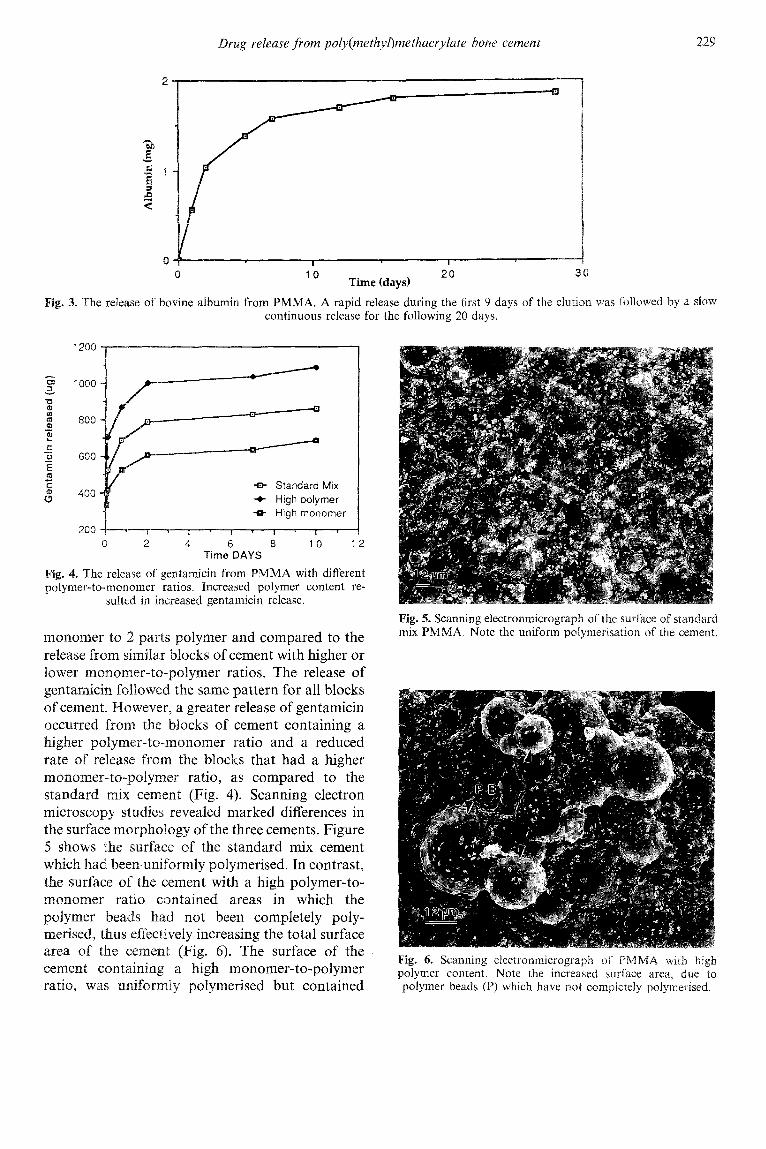
Fig. 3. The release of bovine albumin from PMMA. A rapid release during the first 9 days of the elution. was followed by a ~10~ continuous release for the following 20 days.
G 3
1000
-u 2
4 800
tz t z 600
5 E
s -EF Standard Mix
400 + High polymer +B- High monomer
200
Time DAYS
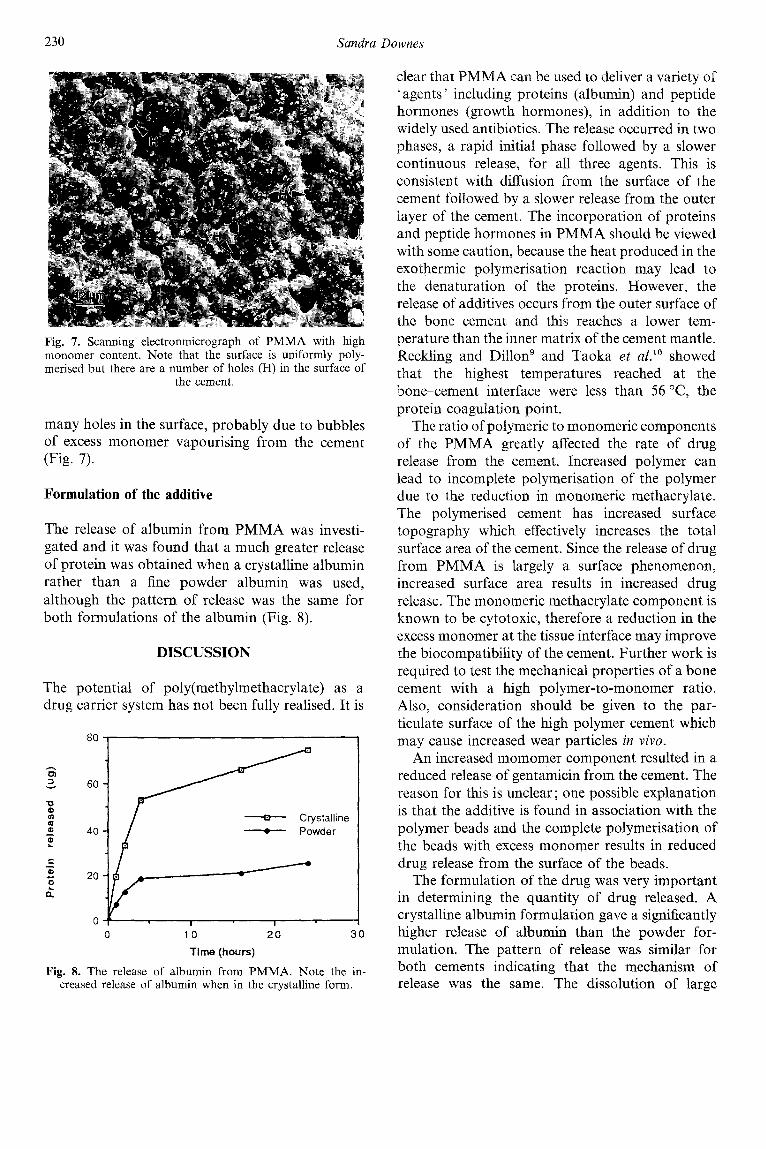
Fig. 4. The release of gentamicin from PMMA with different polymer-to-monomer ratios. Increased polymer content re-
sulted in increased gentamicin release.
monomer to 2 parts polymer and compared to the release from similar blocks of cement with higher or lower monomer-to-polymer ratios. The release of gentamicin followed the same pattern for all blocks of cement. Wowever, a greater release of gentamicin occurred from the blocks of cement containing a
olymer-to-monomer ratio and a reduced rate of release from the blocks that had a higher monomer-to-polymer ratio, as compared to the standard mix cement (Fig. 4). Scanning electron microscopy studies revealed marked differences in the surface morphology of the three cements. Figure 5 shows the surface of the standard mix cement which had been-uniformly polymerised. In contrast, the surface of the cement with a high polymer-to- monomer ratio contained areas in which the polymer beads had not been completely poly- merised, thus effectively increasing the total surface area of the cement (Fig. 6). The surface of the cement containing a high monomer-to-polymer ratio, was uniformly polymerised but contained
Fig. 5. Scanning electronmicrograph of the surface of standard mix PMMA. Note the uniform polymerisation of the cement.
Fig. 6. Scanning electronmicrograph of PMMA with high polymer content. Note the increased surface area, due to polymer beads (P) which have not compieteiy polymerised.
230 Sandra Downes
Fig. 7. Scanning electronmicrograph of PMMA with high monomer content. Note that the surface is uniformly poly- merised but there are a number of holes (H) in the surface of
the cement.
many holes in the surface, probably due to bubbles of excess monomer vapourising from the cement (Fig. 7).
Formulation of the additive
The release of albumin from PMMA was investi- gated and it was found that a much greater release of protein was obtained when a crystalline albumin rather than a fine powder albumin was used, although the pattern of release was the same for both formulations of the albumin (Fig. 8).
DISCUSSION
The potential of poly(methylmethacrylate) as a drug carrier system has not been fully realised. It is
80 , I
0 : I I I 0 10 20 30
Time (hours)
Fig. 8. The release of albumin from PMMA. Note the in- creased release of albumin when in the crystalline form.
clear that PMMA can be used to deliver a variety of ‘agents’ including proteins (albumin) and peptide hormones (growth hormones), in addition to the widely used antibiotics. The release occurred in two phases, a rapid initial phase followed by a slower continuous release, for all three agents. This is consistent with diffusion from the surface of the cement followed by a slower release from the outer layer of the cement. The incorporation of proteins and peptide hormones in PMMA should be viewed with some caution, because the heat produced in the exothermic polymerisation reaction may lead to the denaturation of the proteins. However, the release of additives occurs from the outer surface of the bone cement and this reaches a lower tem- perature than the inner matrix of the cement mantle. Reckling and Dillon9 and Taoka et aLlo showed that the highest temperatures reached at the bone-cement interface were less than 56 “C, the protein coagulation point.
The ratio of polymeric to monomeric components of the PMMA greatly affected the rate of drug release from the cement. Increased polymer can lead to incomplete polymerisation of the polymer due to the reduction in monomeric methacrylate. The polymerised cement has increased surface topography which effectively increases the total surface area of the cement. Since the release of drug from PMMA is largely a surface phenomenon, increased surface area results in increased drug release. The monomeric methacrylate component is known to be cytotoxic, therefore a reduction in the excess monomer at the tissue interface may improve the biocompatibility of the cement. Further work is required to test the mechanical properties of a bone cement with a high polymer-to-monomer ratio. Also, consideration should be given to the par- ticulate surface of the high polymer cement which may cause increased wear particles in viva.
An increased momomer component resulted in a reduced release of gentamicin from the cement. The reason for this is unclear; one possible explanation is that the additive is found in association with the polymer beads and the complete polymerisation of the beads with excess monomer results in reduced drug release from the surface of the beads.
The formulation of the drug was very important in determining the quantity of drug released. A crystalline albumin formulation gave a significantly higher release of albumin than the powder for- mulation. The pattern of release was similar for both cements indicating that the mechanism of release was the same. The dissolution of large
Drug release from poly(methyl)methacrylate bone cement
crystalline structures from the surface of PMMA may be more rapid than that of the fine powder which may be more closely associated with the polymer.
PMMA can be used to deliver various agents, including proteins. The mechanism is similar for all the agents-a rapid release followed by a slower continuous release. The polymer-to-monomer ratio in the cement can greatly affect the rate of drug release. Optimum release is achieved if a large crystalline formulation is used, rather than a fine powder.
ACKNOWLEDGEMENT
The author wishes to thank Dr G. Blunn, Biomedical Engineering, Institute of Orthopaedics, Stanmore, for help with the scanning electro- microscopy studies.
REFERENCES
1. Bucholz, H. W., Elson, R. A. & Lodenkamper, H., The infected joint implant. In Recent Advances in Orthopaedics,
2.
3.
4.
5.
6.
7.
a.
9.
10.
vol. 3, ed. B. McKibbin. burgh, 1979, p. 61. Downes, S., Wood, D.,
231
Churchil:, Livingstone, Edin-
Malcolm, A. J. & Ali, S. Y,, Growth hormone in ~olymethylmethac~y~ate cement. Clin. Orthop. and Rel. Res., 252 (1990) 293-8. Medcraft, J. W. & Gardner, A. D. H., The use of an antibiotic bone cement as a different approach to the elimination of infection in total hip replacement. Med. Lab. Techno!., 31 (1974) 347-53. Elson, R. A., Jephcott, A. E., McGechie, D., Antibiotic loaded acrylic cement. J. Borze Joint Surg., 59B (1977) 200-05. Marks, K. E., Nelson, C. L. & Lammenschlager, E. I?., Antibiotic impregnated acrylic bone cement. .i. Rovze Joint Surg., 58A (1976) 358-63. Wroblewski, B. M., Leaching out from acrylic bo cement : Experimental evaluation, Clin. Orthopaedics, 1 (1977) 311-12. Hughes, S., Robertson, S., Want, S., arrell, J., Kennedy, M. & Dash, C. H., Cefluroxime in bone. Royal Society Medical Congress Symposium, Series 38, Academic Press, London and The Royal Society of Medicine, 1980, pp. 163-71. Downes, S. & Maughan, P. A., Mechanism of antibiotic release from poly(methyl)methacrylate bone cement. Clini- cal materials, 4 (1989) 109-22. Reckling, F. W. & Dillon, W. L., The bone-cement interface temperature during total joint replacement. J. Bone and Jt. Surg., 59A (1977) 80.-2. Taoka, H., Kinoshita, I., Morimoto, II., Sasaki, T., Ogawa, Y. & Shimakawa, T., Temperature in the interface between bone and acrylic bone cement. The Tokushima J. Exp. Med., 27 (1980) 89-92.