methadone was originally developed in germany during the 1930s as a synthetic alternative to opium
TRANSCRIPT

Methadone was originally developed in Germany during the 1930s as a synthetic alternative to
opium. Post World War II, the United States obtained all research records for the substance and
noted that it was less sedating and less of a respiratory depressant thaMethadone was originally developed in Germany during the 1930s as a synthetic alternative to opium. Post World War II, the United States obtained all research records for the substance and noted that it was less sedating and less of a respiratory depressant than morphine. In 1947, Methadone was approved by the FDA for the treatment of opioid dependence.
Methadone was considered a form of opioid replacement therapy and was used to help patients transition off of more addictive opioids like heroin. Eventually “Methadone Clinics” began sprouting throughout the United States, offering treatment to those with opioid dependence. Unfortunately, most individuals ended up becoming nearly as dependent upon the Methadone as illicit drugs like heroin.
For a long time, Methadone was considered the preeminent opioid replacement therapy option. Eventually, Reckitt Benckiser Pharmaceuticals developed the drug Suboxone, a partial opioid agonist as a competitor to Methadone. Suboxone hit the market in 2002 and is regarded as similar in efficacy to Methadone, but favorable in that it has a reduced potential for abuse.
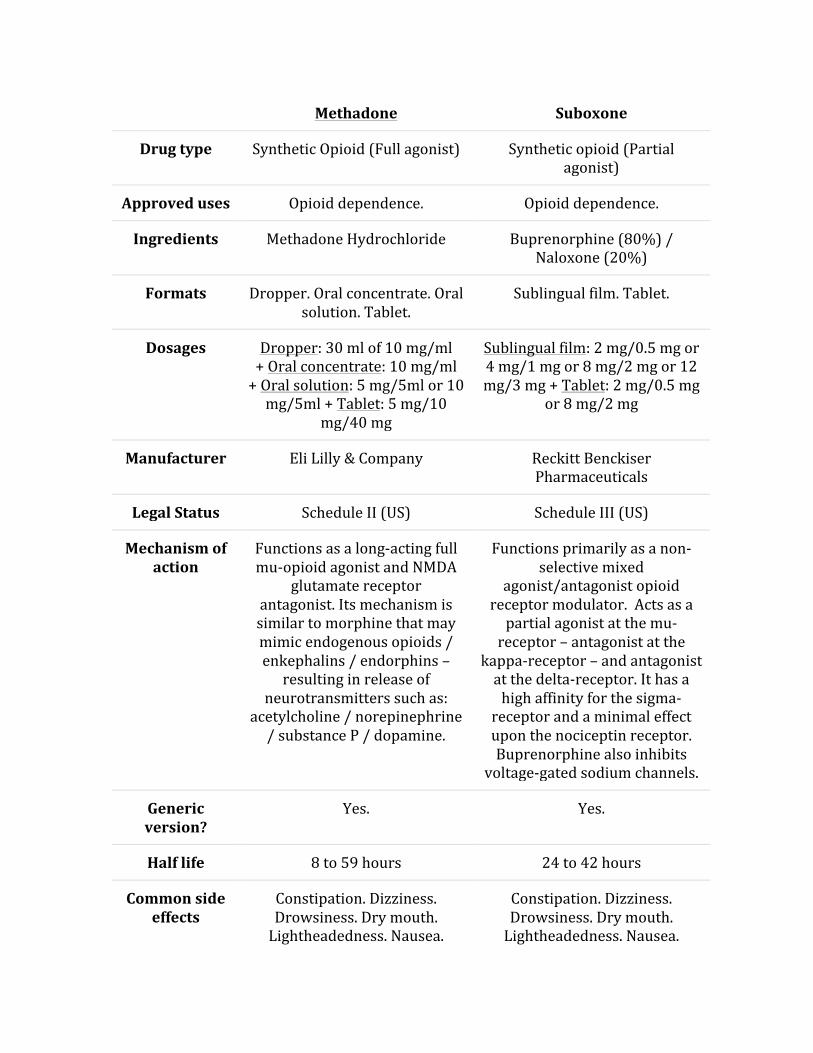
Methadone vs. Suboxone Comparison Chart Below is a chart comparing some general similarities and differences between Methadone and Suboxone. As you can tell, Methadone is a much older drug that hit the market in the late 1940s, whereas Suboxone wasn’t released until the early 2000s. Both drugs are synthetic opioids, but Suboxone is a partial opioid agonist, whereas Methadone is a full opioid agonist.
Methadone Suboxone
Methadone Suboxone
Drug type Synthetic Opioid (Full agonist) Synthetic opioid (Partial agonist)
Approved uses Opioid dependence. Opioid dependence.
Ingredients Methadone Hydrochloride Buprenorphine (80%) / Naloxone (20%)
Formats Dropper. Oral concentrate. Oral solution. Tablet.
Sublingual film. Tablet.
Dosages Dropper: 30 ml of 10 mg/ml + Oral concentrate: 10 mg/ml + Oral solution: 5 mg/5ml or 10 mg/5ml + Tablet: 5 mg/10
mg/40 mg
Sublingual film: 2 mg/0.5 mg or 4 mg/1 mg or 8 mg/2 mg or 12 mg/3 mg + Tablet: 2 mg/0.5 mg
or 8 mg/2 mg
Manufacturer Eli Lilly & Company Reckitt Benckiser Pharmaceuticals
Legal Status Schedule II (US) Schedule III (US)
Mechanism of action
Functions as a long-‐acting full mu-‐opioid agonist and NMDA
glutamate receptor antagonist. Its mechanism is similar to morphine that may mimic endogenous opioids / enkephalins / endorphins – resulting in release of
neurotransmitters such as: acetylcholine / norepinephrine / substance P / dopamine.
Functions primarily as a non-‐selective mixed
agonist/antagonist opioid receptor modulator. Acts as a partial agonist at the mu-‐receptor – antagonist at the
kappa-‐receptor – and antagonist at the delta-‐receptor. It has a high affinity for the sigma-‐receptor and a minimal effect upon the nociceptin receptor. Buprenorphine also inhibits
voltage-‐gated sodium channels.
Generic version?
Yes. Yes.
Half life 8 to 59 hours 24 to 42 hours
Common side effects
Constipation. Dizziness. Drowsiness. Dry mouth. Lightheadedness. Nausea.
Constipation. Dizziness. Drowsiness. Dry mouth. Lightheadedness. Nausea.

Methadone Suboxone
Sweating. Vomiting. Sweating. Vomiting.
Date approved (1947) October (2002)
Effect duration 24 to 36 hours (Analgesic: 6 to 8 hours)
24 hours (Analgesic: 8 to 12 hours)
Investigational uses
Chronic Pain. Chronic Pain. Neonatal abstinence syndrome.
Treatment-‐resistant depression. (Read: Suboxone for
depression).
Methadone vs. Suboxone: What’s the difference? Methadone and Suboxone are similar in that they are both synthetic opioids engineered as a replacement option for those addicted to illicit drugs like heroin. Although the side effect profile associated with each drug is similar, there are many differences between the two drugs. Methadone is regarded as a full mu-opioid receptor agonist, whereas Suboxone is considered a partial agonist.
The fact that Suboxone is a partial agonist makes it less potent than the full agonist that is Methadone. Suboxone has less potential for abuse due to the fact that it was engineered with a ceiling effect. This means that when taken at increasingly higher doses, a user will not derive any additional psychological euphoria from Suboxone, but they will from Methadone.
Abuse Potential Upon comparison, the abuse potential of Methadone is greater than that of Suboxone. Methadone is classified as a “Schedule II” controlled-substance, meaning it has significant potential for abuse and may result in

dependence. Users of Methadone often build up tolerance to the effects of the drug, meaning the therapeutic effect diminishes in time.
This results in users increasing their doses or taking more than necessary to maintain a sense of well-being. Furthermore, when ingested at higher than recommended doses, Methadone can produce a “high.” For this reason, a person is usually required to stay at a “Methadone Clinic” for awhile so that professionals can monitor their dosing – which prevents initial abuse.
The problem is that once users leave the Methadone Clinic and have a prescription for Methadone, they do not have the professional supervision to monitor their usage. This may result in a person taking abnormally high doses in attempt to attain an opioid-induced euphoria. By comparison, Suboxone isn’t regarded as having significant potential for abuse.
Suboxone was designed to have a “ceiling effect” to prevent users from abusing the drug. This means that past a certain dose, a user will not be able to attain any additional effect or “high.” In addition to the “ceiling effect,” Suboxone is only a partial opioid agonist, meaning its “high” isn’t considered as potent as that of Methadone, which leads to reduced potential for abuse.
By comparison, Suboxone is classified as a “Schedule III” controlled-substance. Under this classification, it is thought to have a lower potential for abuse than “Schedule II” substances (e.g. Methadone). Methadone clearly has greater potential for abuse due to its full opioid agonist effect and its lack of a ceiling effect.
Cost: Which is more expensive? Those comparing Methadone to Suboxone may want to consider the prices of each drug. Buying “brand name” Methadone is considerably cheaper than purchasing Suboxone. Even generic Methadone is significantly less expensive than purchasing generic Suboxone. For “Dolophine,” a brand name tablet form of Methadone, you’ll end up paying between $26 and $50 for 60 tablets.

For Methadose oral concentrate, the price ranges between $60 and $75 for a 720 ml prescription. For Methadose tablet formats the prices range between $17 and $45 for 60 tablets. Generic oral concentrate of Methadone can cost up to $60 for 950 ml, while the generic tablet form of Methadone costs between $13 and $35 for a supply of 120 tablets.
For a supply of 30 “brand name” Suboxone films, the price typically falls within the range of $130 and $470. The cost for 30 generic sublingual Suboxone tablets (buprenorphine / naloxone) ranges from $75 to $185 and depends on the dosage. The lower dose of 2 mg/0.5 mg is generally a bit cheaper than the higher dose of 8 mg/2 mg.
If you don’t have as much money to spend on prescriptions or have poor insurance, Methadone is by far the cheaper option. That said, people often forget the total cost associated with staying at a Methadone Clinic. Should you end up at a clinic, you may end up accruing additional costs ranging from $10 to $20 per day.
Dosage & Formats Methadone is manufactured with more dosing options and formats than Suboxone. Formats of Methadone administration include: liquid (dropper, oral concentrate, oral solution) and tablet. Formats of administration for Suboxone include: sublingual film and tablet. The “Dropper” is prescribed with 30 ml of 10 mg/ml, the “Oral concentrate” contains 10 mg/ml as well, and the “Oral solution” contains doses of 10 mg/5 ml or 5 mg/5 ml.
In tablet format, Methadone is manufactured in three dosing options of 5 mg, 10 mg, and 40 mg. Suboxone is unique in that it is manufactured in a sublingual film – a strip that delivers the drug under the tongue. The sublingual format of Suboxone is manufactured with dosing options of: 2 mg/0.5 mg, 4 mg/1 mg, 8 mg/2 mg, and 12 mg/3 mg; the first number indicates the amount of buprenorphine, while the second indicates the amount of naloxone.

Suboxone is also manufactured in tablet formats of 2 mg/0.5 mg and 8 mg/2 mg. The dosing options are considered more limited for the tablet than they are for the sublingual film. Many people prefer the novel sublingual delivery of Suboxone over the oral and tablet formats of Methadone. Both Suboxone and Methadone are thought to provide sufficient dosing options for titration upwards or downwards.
Efficacy: Which drug is more effective? Those who are attempting to use opioid replacement therapy as a way to overcome opioid dependence often want to know whether Methadone is more effective than Suboxone, or vice-versa. A meta-analysis published in 2014 evaluated all randomized controlled trials of buprenorphine and methadone compared to a placebo for the management of opioid dependence. The goal of this research was to determine whether one substance was safer and/or more effective than the other.
The researchers included 31 trials with a cumulative total of 5430 individuals. The study authors determined that buprenorphine was effective in maintenance treatment of heroin dependence at doses above 2 mg. It also suppressed illicit opioid usage when administered at doses exceeding 16 mg.
Methadone was considered more effective than Suboxone for treatment retention when used flexibly at low fixed quantities. At medium and high doses, there was no significant difference in treatment retention and both drugs suppressed the usage of illicit opioids. Due to the fact that doses are often used flexibly and are seldom “fixed” in clinical practice, the authors suggested that Methadone leads to greater treatment retention.
That said, both drugs were equally effective at suppressing illicit opioid use. If you’re using Suboxone at a fixed medium or high dose, there shouldn’t be much of a difference in regards to treatment-retention or efficacy compared to Methadone. However, if you’re using Suboxone at flexible doses, particularly

within the range of 2 mg to 6 mg, treatment retention is often poorer compared to Methadone.
§ Source: http://www.ncbi.nlm.nih.gov/pubmed/18425880 Mechanisms of action The mechanisms of action differ between Methadone and Suboxone. Methadone is comprised of two enantiomers: levomethadone (R-methadone) and dextromethadone (S-methadone). The levomethadone acts as a full mu-opioid receptor agonist. It binds to the mu-receptor site and elicits effects akin to endogenous opioids, enkephalins, and endorphins.
This may produce a cascade effect that may stimulate the release of other neurotransmitters including: acetylcholine, norepinephrine, substance P, and dopamine. Methadone also functions as an NMDA glutamate receptor antagonist, which may aid in decreasing pain. It also has very minor effects as a nicotinic acetylcholine receptor antagonist.
By comparison, Suboxone acts as partial mu-opioid receptor agonist. Technically, it is regarded as a non-selective, mixed agonist/antagonist opioid receptor modulator. In addition to its agonist effect at the mu-receptor, it also acts as an angatonist at the kappa and delta opioid receptors. It has a high affinity for the sigma receptor, and elicits minor effects on the nociceptin receptor.
While both drugs primarily target the mu-receptor, their secondary mechanisms differ in that Suboxone doesn’t act as an NMDA receptor antagonist. Suboxone affects the kappa and delta receptors as an antagonist, whereas Methadone isn’t known to elicit this effect.
§ Source: http://www.ncbi.nlm.nih.gov/pubmed/22504149 § Source: http://www.ncbi.nlm.nih.gov/pubmed/12435410 § Source: http://www.ncbi.nlm.nih.gov/pubmed/24903063 § Source: http://www.ncbi.nlm.nih.gov/pmc/articles/PMC1070723/

Medical Uses Medically, both Methadone and Suboxone are used to primarily treat opioid dependence and addiction. They are also commonly prescribed off-label as analgesics for low-grade or moderate chronic pain. The FDA recommended uses for Methadone and Suboxone aren’t subject to significant variation.
That said, investigative uses for Suboxone and Methadone are known to differ. Methadone isn’t commonly prescribed off-label or utilized as an investigational treatment. Suboxone has been investigated for the treatment of neonatal abstinence syndrome. This is a condition affecting newborns that have been exposed to opioids during pregnancy that experience symptoms of withdrawal upon birth.
The usage is limited to FDA trials and is being used in a specifically calibrated neonatal formulation. Another off-label use is that of Suboxone for treatment-resistant depression. This is especially common among those who have refractory depression and a history of opioid dependence.
An offshoot of Suboxone called “ALKS-5461” (Buprenorphine / Samidorphan) is showing significant promise as an antidepressant augmentation strategy. Due to the reduced potency and abuse potential of Suboxone compared to Methadone, it is more commonly utilized as an off-label treatment. Popularity As of 2013, Suboxone was estimated to be prescribed 9.3 million times. There isn’t exact data for the number of Methadone prescriptions. Estimates from the CDC (Centers for Disease Control) suggest that Methadone accounted for 2% of analgesic prescriptions in the United States in 2012. It is thought that both drugs remain extremely popular among those involved in opioid replacement therapy.
Suboxone may have surpassed the popularity of Methadone in recent years due to the fact that it is a newer drug, is thought to be slightly less potent, with an equal comparative efficacy. Doctors may prefer prescribing Suboxone due to its “ceiling effect” which mitigates its potential for abuse. Patients may also prefer

taking Suboxone in the form of sublingual film as opposed to the liquid formats of Methadone.
Among opioid addicts, Methadone is likely to be more popular due to the fact that it has a greater propensity for abuse. Methadone does not have a ceiling effect and is therefore likely to produce a physical and psychological “high” when ingested at high doses. Methadone also remains popular due to the fact that there are many “Methadone Clinics” throughout the United States, making the drug widely available.
Side Effects The side effects associated with Methadone and Suboxone are nearly identical. Common side effects associated with both drugs include: constipation, dizziness, drowsiness, dry mouth, lightheadedness, nausea, sweating, and vomiting. Most side effects are subject to individual variation or how your physiology responds to the particular drug.
Differences in side effects may also be due to the slight differences in mechansim of action associated with Methadone and Suboxone. Methadone may produce more severe and or different side effects due to the fact that it is a full mu-receptor agonist and NDMA receptor antagonist. Suboxone is a partial mu-receptor agonist and has effects on a variety of other opioid receptors (e.g. kappa).
Withdrawal Discontinuation of Methadone or Suboxone is likely to result in severe withdrawal symptoms. These symptoms are often most severe within the first 1 to 2 weeks of discontinuation, but may persist for months after the drug has been discontinued as “post-acute withdrawal syndrome” or PAWS. The degree of difficulty associated with discontinuation of Methadone and Suboxone largely depends on the time span over which the drug was taken and the dosage.

It could be argued that since Methadone is a full mu-receptor agonist, its discontinuation effects may be more pronounced than Suboxone. In any regard, there are numerous anecdotal reports of Methadone withdrawal andSuboxone withdrawal that highlight their respective degrees of difficulty. Since Methadone doesn’t have a “ceiling effect,” its withdrawal effects from high doses may be more pronounced than Suboxone. Based on a comparison of the most addictive drugs, Street Methadone has an estimated addiction rating of “2.08” and Buprenorphine’s estimated addiction rating is “1.64” – meaning it should theoretically be tougher to discontinue Methadone. Assuming no addiction or abuse of either substance, the difficulty of discontinuation may be relatively similar. Individual physiology and subjectivity may dictate whether one is tougher than the other.
Similarities (Recap): Methadone vs. Suboxone Below is a recap of the commonalities shared by Methadone and Suboxone.
§ Drug type: Both drugs are classified as synthetic opioids and are considered first-line options for treating opioid dependence.
§ Efficacy: Methadone and Suboxone are regarded as equally effective in reducing usage of illicit opioids like heroin.
§ Generic availability: Each drug is available in generic formats of Methadone (methadone hydrochloride) and Suboxone (buprenorphine / naloxone).
§ Medical uses: The FDA has approved Methadone and Suboxone for treating opioid dependence, opioid addiction, and chronic pain.
§ Side effects: The side effects are regarded as similar among these drugs and include: constipation, dizziness, drowsiness, nausea, and vomiting.
§ Withdrawal: Discontinuation from Methadone and Suboxone is regarded as being highly difficult, especially when utilized for a long-term and/or at a high dosage.

Differences (Recap): Methadone vs. Suboxone Below are some differences between Methadone and Suboxone.
§ Abuse potential: Methadone is considered to have a higher potential for abuse, whereas Suboxone has a lower abuse potential due to its built-in “ceiling effect.”
§ Cost: Both brand name and generic formulations of Methadone are cheaper than brand name Suboxone. From a cost-perspective, Methadone is the better bargain.
§ Duration of effect: The duration of effect for Suboxone is approximately 24 hours, whereas Methadone is thought to last between 24 and 36 hours. The window of analgesic effect from Suboxone is an estimated 8 to 12 hours, whereas that of Methadone is 6 to 8 hours.
§ Formats: Although Methadone and Suboxone are both manufactured in tablet formats, Methadone is also prescribed in a liquid solution and Suboxone in a sublingual film.
§ Half-life: The elimination half-life for Methadone is estimated between 8 and 59 hours, while Suboxone’s half-life is estimated between 24 and 42 hours.
§ Ingredients: Methadone is comprised of “methadone hydrochloride” and Suboxone is comprised of Buprenorphine and Naloxone.
§ Investigational uses: Methadone doesn’t have many investigational uses, while Suboxone has been investigated as an antidepressant and to treat neonatal abstinence syndrome.
§ Legal status: Methadone is considered a “Schedule II” drug and Suboxone is a “Schedule III” drug.
§ Manufacturers: Methadone is manufactured by Eli Lilly & Company and Suboxone is manufactured by Reckitt Benckiser Pharmaceuticals.
§ Mechanisms of action: Methadone is considered a full mu-receptor agonist, while Suboxone is a partial mu-receptor agonist. Methadone also acts

as an NMDA receptor antagonist (Suboxone doesn’t), and Suboxone acts on other opioid receptors (Methadone doesn’t).
§ Popularity: Throughout the 1990s, Methadone became the most popular opioid replacement therapy option. However, since Suboxone’s approval in 2002, the number of prescriptions for Suboxone has continued to rise. Methadone may have more appeal to addicts, whereas Suboxone is often considered safer by medical professionals.
Which drug is a better opioid replacement therapy? Methadone vs. Suboxone. As was already mentioned, there appears to be no significant difference in the efficacy of Methadone and Suboxone for the treatment of opioid dependence. They are both synthetic opioids that primarily act as agonists of the mu-receptor. Certain individuals may prefer Methadone over Suboxone for its increased potency, while others may respond better to the mechanisms of Suboxone.
Some people may find that they both work equally well in managing opioid dependency and reducing their propensity to use illicit opioids. The research shows that those receiving Methadone at flexible doses are more likely to adhere to treatment compared to those receiving Suboxone at flexible doses. That said, both were found to have equal efficacy in terms of reducing illicit opioid usage.
Among individuals that may be likely to abuse Methadone, Suboxone may be preferred. Suboxone’s ceiling effect mitigates additional opioid effects past a certain dosage. Methadone can be abused, and some patients may take large quantities to “get high.” Therefore, Methadone is more strictly regulated by professionals.
For this reason, patients generally need to stay at a “Methadone Clinic” in order to receive their medication. Only when the patient is adhering to the treatment are they allowed to take their Methadone home for self-administration. Anecdotal reports have suggested that Methadone may be better at combating physical symptoms of opioid replacement compared to Suboxone.

Those taking Suboxone may have an easier time dealing with side effects and withdrawal symptoms due to its slightly reduced potency. For individuals with mild or moderate opioid dependence, Suboxone is usually the preferred option. Methadone can be used for all levels of dependence, but may be better than Suboxone for severe forms.
Which drug do you prefer: Methadone or Suboxone? If you have used both Methadone and Suboxone, feel free to share which one you found to be the better opioid replacement therapy. Did one drug feel more potent than the other or do a better job at reducing cravings to use illicit opioids? Mention any reasons that you prefer Methadone over Suboxone or vice-versa.
n morphine. In 1947, Methadone was approved by the FDA for the treatment of opioid dependence.
Methadone was considered a form of opioid replacement therapy and was used to help patients transition off of more addictive opioids like heroin. Eventually “Methadone Clinics” began sprouting throughout the United States, offering treatment to those with opioid dependence. Unfortunately, most individuals ended up becoming nearly as dependent upon the Methadone as illicit drugs like heroin.
For a long time, Methadone was considered the preeminent opioid replacement therapy option. Eventually, Reckitt Benckiser Pharmaceuticals developed the drug Suboxone, a partial opioid agonist as a competitor to Methadone. Suboxone hit the market in 2002 and is regarded as similar in efficacy to Methadone, but favorable in that it has a reduced potential for abuse.
Methadone vs. Suboxone Comparison Chart

Below is a chart comparing some general similarities and differences between Methadone and Suboxone. As you can tell, Methadone is a much older drug that hit the market in the late 1940s, whereas Suboxone wasn’t released until the early 2000s. Both drugs are synthetic opioids, but Suboxone is a partial opioid agonist, whereas Methadone is a full opioid agonist.
Methadone Suboxone
Drug type Synthetic Opioid (Full agonist) Synthetic opioid (Partial agonist)
Approved uses Opioid dependence. Opioid dependence.
Ingredients Methadone Hydrochloride Buprenorphine (80%) / Naloxone (20%)
Formats Dropper. Oral concentrate. Oral solution. Tablet.
Sublingual film. Tablet.
Dosages Dropper: 30 ml of 10 mg/ml + Oral concentrate: 10 mg/ml + Oral solution:
5 mg/5ml or 10 mg/5ml + Tablet: 5 mg/10 mg/40 mg
Sublingual film: 2 mg/0.5 mg or 4 mg/1 mg or 8 mg/2 mg or 12 mg/3 mg + Tablet: 2
mg/0.5 mg or 8 mg/2 mg
Manufacturer Eli Lilly & Company Reckitt Benckiser Pharmaceuticals
Legal Status Schedule II (US) Schedule III (US)
Mechanism of action
Functions as a long-acting full mu-opioid agonist and NMDA glutamate receptor antagonist. Its mechanism is similar to morphine that may mimic endogenous opioids / enkephalins / endorphins – resulting in release of
neurotransmitters such as: acetylcholine / norepinephrine / substance P /
dopamine.
Functions primarily as a non-selective mixed agonist/antagonist opioid receptor
modulator. Acts as a partial agonist at the mu-receptor – antagonist at the kappa-receptor – and antagonist at the delta-
receptor. It has a high affinity for the sigma-receptor and a minimal effect upon the
nociceptin receptor. Buprenorphine also inhibits voltage-gated sodium channels.
Generic version?
Yes. Yes.
Half life 8 to 59 hours 24 to 42 hours
Common side effects
Constipation. Dizziness. Drowsiness. Dry mouth. Lightheadedness. Nausea.
Sweating. Vomiting.
Constipation. Dizziness. Drowsiness. Dry mouth. Lightheadedness. Nausea. Sweating.
Vomiting.

Methadone Suboxone
Date approved (1947) October (2002)
Effect duration 24 to 36 hours (Analgesic: 6 to 8 hours) 24 hours (Analgesic: 8 to 12 hours)
Investigational uses
Chronic Pain. Chronic Pain. Neonatal abstinence syndrome. Treatment-resistant depression.
(Read: Suboxone for depression).
Methadone vs. Suboxone: What’s the difference? Methadone and Suboxone are similar in that they are both synthetic opioids engineered as a replacement option for those addicted to illicit drugs like heroin. Although the side effect profile associated with each drug is similar, there are many differences between the two drugs. Methadone is regarded as a full mu-opioid receptor agonist, whereas Suboxone is considered a partial agonist.
The fact that Suboxone is a partial agonist makes it less potent than the full agonist that is Methadone. Suboxone has less potential for abuse due to the fact that it was engineered with a ceiling effect. This means that when taken at increasingly higher doses, a user will not derive any additional psychological euphoria from Suboxone, but they will from Methadone.
Abuse Potential Upon comparison, the abuse potential of Methadone is greater than that of Suboxone. Methadone is classified as a “Schedule II” controlled-substance, meaning it has significant potential for abuse and may result in dependence. Users of Methadone often build up tolerance to the effects of the drug, meaning the therapeutic effect diminishes in time.
This results in users increasing their doses or taking more than necessary to maintain a sense of well-being. Furthermore, when ingested at higher than

recommended doses, Methadone can produce a “high.” For this reason, a person is usually required to stay at a “Methadone Clinic” for awhile so that professionals can monitor their dosing – which prevents initial abuse.
The problem is that once users leave the Methadone Clinic and have a prescription for Methadone, they do not have the professional supervision to monitor their usage. This may result in a person taking abnormally high doses in attempt to attain an opioid-induced euphoria. By comparison, Suboxone isn’t regarded as having significant potential for abuse.
Suboxone was designed to have a “ceiling effect” to prevent users from abusing the drug. This means that past a certain dose, a user will not be able to attain any additional effect or “high.” In addition to the “ceiling effect,” Suboxone is only a partial opioid agonist, meaning its “high” isn’t considered as potent as that of Methadone, which leads to reduced potential for abuse.
By comparison, Suboxone is classified as a “Schedule III” controlled-substance. Under this classification, it is thought to have a lower potential for abuse than “Schedule II” substances (e.g. Methadone). Methadone clearly has greater potential for abuse due to its full opioid agonist effect and its lack of a ceiling effect.
Cost: Which is more expensive? Those comparing Methadone to Suboxone may want to consider the prices of each drug. Buying “brand name” Methadone is considerably cheaper than purchasing Suboxone. Even generic Methadone is significantly less expensive than purchasing generic Suboxone. For “Dolophine,” a brand name tablet form of Methadone, you’ll end up paying between $26 and $50 for 60 tablets.
For Methadose oral concentrate, the price ranges between $60 and $75 for a 720 ml prescription. For Methadose tablet formats the prices range between $17 and $45 for 60 tablets. Generic oral concentrate of Methadone can cost up to $60 for

950 ml, while the generic tablet form of Methadone costs between $13 and $35 for a supply of 120 tablets.
For a supply of 30 “brand name” Suboxone films, the price typically falls within the range of $130 and $470. The cost for 30 generic sublingual Suboxone tablets (buprenorphine / naloxone) ranges from $75 to $185 and depends on the dosage. The lower dose of 2 mg/0.5 mg is generally a bit cheaper than the higher dose of 8 mg/2 mg.
If you don’t have as much money to spend on prescriptions or have poor insurance, Methadone is by far the cheaper option. That said, people often forget the total cost associated with staying at a Methadone Clinic. Should you end up at a clinic, you may end up accruing additional costs ranging from $10 to $20 per day.
Dosage & Formats Methadone is manufactured with more dosing options and formats than Suboxone. Formats of Methadone administration include: liquid (dropper, oral concentrate, oral solution) and tablet. Formats of administration for Suboxone include: sublingual film and tablet. The “Dropper” is prescribed with 30 ml of 10 mg/ml, the “Oral concentrate” contains 10 mg/ml as well, and the “Oral solution” contains doses of 10 mg/5 ml or 5 mg/5 ml.
In tablet format, Methadone is manufactured in three dosing options of 5 mg, 10 mg, and 40 mg. Suboxone is unique in that it is manufactured in a sublingual film – a strip that delivers the drug under the tongue. The sublingual format of Suboxone is manufactured with dosing options of: 2 mg/0.5 mg, 4 mg/1 mg, 8 mg/2 mg, and 12 mg/3 mg; the first number indicates the amount of buprenorphine, while the second indicates the amount of naloxone.
Suboxone is also manufactured in tablet formats of 2 mg/0.5 mg and 8 mg/2 mg. The dosing options are considered more limited for the tablet than they are for the sublingual film. Many people prefer the novel sublingual delivery of

Suboxone over the oral and tablet formats of Methadone. Both Suboxone and Methadone are thought to provide sufficient dosing options for titration upwards or downwards.
Efficacy: Which drug is more effective? Those who are attempting to use opioid replacement therapy as a way to overcome opioid dependence often want to know whether Methadone is more effective than Suboxone, or vice-versa. A meta-analysis published in 2014 evaluated all randomized controlled trials of buprenorphine and methadone compared to a placebo for the management of opioid dependence. The goal of this research was to determine whether one substance was safer and/or more effective than the other.
The researchers included 31 trials with a cumulative total of 5430 individuals. The study authors determined that buprenorphine was effective in maintenance treatment of heroin dependence at doses above 2 mg. It also suppressed illicit opioid usage when administered at doses exceeding 16 mg.
Methadone was considered more effective than Suboxone for treatment retention when used flexibly at low fixed quantities. At medium and high doses, there was no significant difference in treatment retention and both drugs suppressed the usage of illicit opioids. Due to the fact that doses are often used flexibly and are seldom “fixed” in clinical practice, the authors suggested that Methadone leads to greater treatment retention.
That said, both drugs were equally effective at suppressing illicit opioid use. If you’re using Suboxone at a fixed medium or high dose, there shouldn’t be much of a difference in regards to treatment-retention or efficacy compared to Methadone. However, if you’re using Suboxone at flexible doses, particularly within the range of 2 mg to 6 mg, treatment retention is often poorer compared to Methadone.
§ Source: http://www.ncbi.nlm.nih.gov/pubmed/18425880

Mechanisms of action The mechanisms of action differ between Methadone and Suboxone. Methadone is comprised of two enantiomers: levomethadone (R-methadone) and dextromethadone (S-methadone). The levomethadone acts as a full mu-opioid receptor agonist. It binds to the mu-receptor site and elicits effects akin to endogenous opioids, enkephalins, and endorphins.
This may produce a cascade effect that may stimulate the release of other neurotransmitters including: acetylcholine, norepinephrine, substance P, and dopamine. Methadone also functions as an NMDA glutamate receptor antagonist, which may aid in decreasing pain. It also has very minor effects as a nicotinic acetylcholine receptor antagonist.
By comparison, Suboxone acts as partial mu-opioid receptor agonist. Technically, it is regarded as a non-selective, mixed agonist/antagonist opioid receptor modulator. In addition to its agonist effect at the mu-receptor, it also acts as an angatonist at the kappa and delta opioid receptors. It has a high affinity for the sigma receptor, and elicits minor effects on the nociceptin receptor.
While both drugs primarily target the mu-receptor, their secondary mechanisms differ in that Suboxone doesn’t act as an NMDA receptor antagonist. Suboxone affects the kappa and delta receptors as an antagonist, whereas Methadone isn’t known to elicit this effect.
§ Source: http://www.ncbi.nlm.nih.gov/pubmed/22504149 § Source: http://www.ncbi.nlm.nih.gov/pubmed/12435410 § Source: http://www.ncbi.nlm.nih.gov/pubmed/24903063 § Source: http://www.ncbi.nlm.nih.gov/pmc/articles/PMC1070723/ Medical Uses Medically, both Methadone and Suboxone are used to primarily treat opioid dependence and addiction. They are also commonly prescribed off-label as

analgesics for low-grade or moderate chronic pain. The FDA recommended uses for Methadone and Suboxone aren’t subject to significant variation.
That said, investigative uses for Suboxone and Methadone are known to differ. Methadone isn’t commonly prescribed off-label or utilized as an investigational treatment. Suboxone has been investigated for the treatment of neonatal abstinence syndrome. This is a condition affecting newborns that have been exposed to opioids during pregnancy that experience symptoms of withdrawal upon birth.
The usage is limited to FDA trials and is being used in a specifically calibrated neonatal formulation. Another off-label use is that of Suboxone for treatment-resistant depression. This is especially common among those who have refractory depression and a history of opioid dependence.
An offshoot of Suboxone called “ALKS-5461” (Buprenorphine / Samidorphan) is showing significant promise as an antidepressant augmentation strategy. Due to the reduced potency and abuse potential of Suboxone compared to Methadone, it is more commonly utilized as an off-label treatment. Popularity As of 2013, Suboxone was estimated to be prescribed 9.3 million times. There isn’t exact data for the number of Methadone prescriptions. Estimates from the CDC (Centers for Disease Control) suggest that Methadone accounted for 2% of analgesic prescriptions in the United States in 2012. It is thought that both drugs remain extremely popular among those involved in opioid replacement therapy.
Suboxone may have surpassed the popularity of Methadone in recent years due to the fact that it is a newer drug, is thought to be slightly less potent, with an equal comparative efficacy. Doctors may prefer prescribing Suboxone due to its “ceiling effect” which mitigates its potential for abuse. Patients may also prefer taking Suboxone in the form of sublingual film as opposed to the liquid formats of Methadone.

Among opioid addicts, Methadone is likely to be more popular due to the fact that it has a greater propensity for abuse. Methadone does not have a ceiling effect and is therefore likely to produce a physical and psychological “high” when ingested at high doses. Methadone also remains popular due to the fact that there are many “Methadone Clinics” throughout the United States, making the drug widely available.
Side Effects The side effects associated with Methadone and Suboxone are nearly identical. Common side effects associated with both drugs include: constipation, dizziness, drowsiness, dry mouth, lightheadedness, nausea, sweating, and vomiting. Most side effects are subject to individual variation or how your physiology responds to the particular drug.
Differences in side effects may also be due to the slight differences in mechansim of action associated with Methadone and Suboxone. Methadone may produce more severe and or different side effects due to the fact that it is a full mu-receptor agonist and NDMA receptor antagonist. Suboxone is a partial mu-receptor agonist and has effects on a variety of other opioid receptors (e.g. kappa).
Withdrawal Discontinuation of Methadone or Suboxone is likely to result in severe withdrawal symptoms. These symptoms are often most severe within the first 1 to 2 weeks of discontinuation, but may persist for months after the drug has been discontinued as “post-acute withdrawal syndrome” or PAWS. The degree of difficulty associated with discontinuation of Methadone and Suboxone largely depends on the time span over which the drug was taken and the dosage.
It could be argued that since Methadone is a full mu-receptor agonist, its discontinuation effects may be more pronounced than Suboxone. In any regard, there are numerous anecdotal reports of Methadone withdrawal andSuboxone withdrawal that highlight their respective degrees of difficulty. Since Methadone

doesn’t have a “ceiling effect,” its withdrawal effects from high doses may be more pronounced than Suboxone. Based on a comparison of the most addictive drugs, Street Methadone has an estimated addiction rating of “2.08” and Buprenorphine’s estimated addiction rating is “1.64” – meaning it should theoretically be tougher to discontinue Methadone. Assuming no addiction or abuse of either substance, the difficulty of discontinuation may be relatively similar. Individual physiology and subjectivity may dictate whether one is tougher than the other.
Similarities (Recap): Methadone vs. Suboxone Below is a recap of the commonalities shared by Methadone and Suboxone.
§ Drug type: Both drugs are classified as synthetic opioids and are considered first-line options for treating opioid dependence.
§ Efficacy: Methadone and Suboxone are regarded as equally effective in reducing usage of illicit opioids like heroin.
§ Generic availability: Each drug is available in generic formats of Methadone (methadone hydrochloride) and Suboxone (buprenorphine / naloxone).
§ Medical uses: The FDA has approved Methadone and Suboxone for treating opioid dependence, opioid addiction, and chronic pain.
§ Side effects: The side effects are regarded as similar among these drugs and include: constipation, dizziness, drowsiness, nausea, and vomiting.
§ Withdrawal: Discontinuation from Methadone and Suboxone is regarded as being highly difficult, especially when utilized for a long-term and/or at a high dosage.
Differences (Recap): Methadone vs. Suboxone

Below are some differences between Methadone and Suboxone.
§ Abuse potential: Methadone is considered to have a higher potential for abuse, whereas Suboxone has a lower abuse potential due to its built-in “ceiling effect.”
§ Cost: Both brand name and generic formulations of Methadone are cheaper than brand name Suboxone. From a cost-perspective, Methadone is the better bargain.
§ Duration of effect: The duration of effect for Suboxone is approximately 24 hours, whereas Methadone is thought to last between 24 and 36 hours. The window of analgesic effect from Suboxone is an estimated 8 to 12 hours, whereas that of Methadone is 6 to 8 hours.
§ Formats: Although Methadone and Suboxone are both manufactured in tablet formats, Methadone is also prescribed in a liquid solution and Suboxone in a sublingual film.
§ Half-life: The elimination half-life for Methadone is estimated between 8 and 59 hours, while Suboxone’s half-life is estimated between 24 and 42 hours.
§ Ingredients: Methadone is comprised of “methadone hydrochloride” and Suboxone is comprised of Buprenorphine and Naloxone.
§ Investigational uses: Methadone doesn’t have many investigational uses, while Suboxone has been investigated as an antidepressant and to treat neonatal abstinence syndrome.
§ Legal status: Methadone is considered a “Schedule II” drug and Suboxone is a “Schedule III” drug.
§ Manufacturers: Methadone is manufactured by Eli Lilly & Company and Suboxone is manufactured by Reckitt Benckiser Pharmaceuticals.
§ Mechanisms of action: Methadone is considered a full mu-receptor agonist, while Suboxone is a partial mu-receptor agonist. Methadone also acts as an NMDA receptor antagonist (Suboxone doesn’t), and Suboxone acts on other opioid receptors (Methadone doesn’t).
§ Popularity: Throughout the 1990s, Methadone became the most popular opioid replacement therapy option. However, since Suboxone’s approval in

2002, the number of prescriptions for Suboxone has continued to rise. Methadone may have more appeal to addicts, whereas Suboxone is often considered safer by medical professionals.
Which drug is a better opioid replacement therapy? Methadone vs. Suboxone. As was already mentioned, there appears to be no significant difference in the efficacy of Methadone and Suboxone for the treatment of opioid dependence. They are both synthetic opioids that primarily act as agonists of the mu-receptor. Certain individuals may prefer Methadone over Suboxone for its increased potency, while others may respond better to the mechanisms of Suboxone.
Some people may find that they both work equally well in managing opioid dependency and reducing their propensity to use illicit opioids. The research shows that those receiving Methadone at flexible doses are more likely to adhere to treatment compared to those receiving Suboxone at flexible doses. That said, both were found to have equal efficacy in terms of reducing illicit opioid usage.
Among individuals that may be likely to abuse Methadone, Suboxone may be preferred. Suboxone’s ceiling effect mitigates additional opioid effects past a certain dosage. Methadone can be abused, and some patients may take large quantities to “get high.” Therefore, Methadone is more strictly regulated by professionals.
For this reason, patients generally need to stay at a “Methadone Clinic” in order to receive their medication. Only when the patient is adhering to the treatment are they allowed to take their Methadone home for self-administration. Anecdotal reports have suggested that Methadone may be better at combating physical symptoms of opioid replacement compared to Suboxone.
Those taking Suboxone may have an easier time dealing with side effects and withdrawal symptoms due to its slightly reduced potency. For individuals with mild or moderate opioid dependence, Suboxone is usually the preferred

option. Methadone can be used for all levels of dependence, but may be better than Suboxone for severe forms.
Which drug do you prefer: Methadone or Suboxone? If you have used both Methadone and Suboxone, feel free to share which one you found to be the better opioid replacement therapy. Did one drug feel more potent than the other or do a better job at reducing cravings to use illicit opioids? Mention any reasons that you prefer Methadone over Suboxone or vice-versa.

Subutex vs. Suboxone: What’s the Difference? Subutex and Suboxone are drugs that were approved by the FDA in 2002 for the treatment of opioid dependence. Both drugs contain the active ingredient buprenorphine, a semisynthetic opioid that acts as primarily as a partial mu-opioid receptor agonist. Buprenorphine also acts as an antagonist at the kappa and delta opioid receptors.
Buprenorphine’s mechanism of action mitigates severe withdrawals associated with illicit opioid use, and serves as a “replacement” drug for illicit opioids. The goal is to help those dependent on illicit opioids transition off of them and onto a replacement therapy like Subutex or Suboxone. Once a patient has stabilized on the replacement (e.g. Subutex or Suboxone), the next step is to gradually titrate off of the replacement drug, and ultimately for the individual to remain sober.
Although Subutex and Suboxone are similar, the most notable difference between the two is the additional component of Naloxone in Suboxone. The Naloxone component makes the Buprenorphine component no longer effective past a certain dose (“ceiling effect”), and if crushed or injected, an individual will experience a withdrawal rather than a “high.” This means that Suboxone has slightly less abuse potential among those with opioid dependence compared to Subutex.
Subutex vs. Suboxone Comparison Chart As you can see, there really aren’t many differences between Subutex and Suboxone. The primary difference is that Suboxone contains a unique formulation of 80% buprenorphine and 20% naloxone, whereas Subutex contains only buprenorphine hydrochloride.

Subutex Suboxone
Drug type Synthetic opioid (Partial agonist)
Synthetic opioid (Partial agonist)
Approved uses Opioid dependence. Opioid dependence.
Ingredients Buprenorphine Hydrochloride Buprenorphine (80%) / Naloxone (20%)
Formats Sublingual tablet. Sublingual film. Sublingual tablet.
Dosages 2 mg or 8 mg Sublingual film: 2 mg/0.5 mg or 4 mg/1 mg or 8 mg/2 mg or 12 mg/3 mg + Tablet: 2 mg/0.5 mg
or 8 mg/2 mg
Manufacturer Reckitt Benckiser Pharmaceuticals
Reckitt Benckiser Pharmaceuticals
Legal Status Schedule III (US) Schedule III (US)
Mechanism of action
Functions primarily as a non-‐selective mixed
agonist/antagonist opioid receptor modulator. Acts as a partial agonist at the mu-‐receptor – antagonist at the kappa-‐receptor – and antagonist at the delta-‐
receptor. It has a high affinity for the sigma-‐receptor and a minimal effect upon the nociceptin receptor.
Buprenorphine also inhibits voltage-‐gated sodium channels.
Functions primarily as a non-‐selective mixed
agonist/antagonist opioid receptor modulator. Acts as a partial agonist at the mu-‐receptor – antagonist at the kappa-‐receptor – and antagonist at the delta-‐
receptor. It has a high affinity for the sigma-‐receptor and a minimal effect upon the nociceptin receptor.
Buprenorphine also inhibits voltage-‐gated sodium channels. The Naloxone
component of Suboxone has a high affinity for the mu-‐receptor as a competitive antagonist. It also elicits antagonist effect upon the kappa and delta receptors.
Generic Yes. Yes.

Subutex Suboxone
version?
Half life 24 to 42 hours 24 to 42 hours
Common side effects
Constipation. Dizziness. Drowsiness. Headaches.
Constipation. Dizziness. Drowsiness. Dry mouth. Lightheadedness. Nausea. Sweating. Vomiting.
Date approved October (2002) October (2002)
Effect duration 24 hours (Analgesic: 8 to 12 hours)
24 hours (Analgesic: 8 to 12 hours)
Investigational uses
Chronic Pain. Chronic Pain. Neonatal abstinence syndrome. Treatment-‐resistant
depression. (Read: Suboxone for depression).
Subutex vs. Suboxone: What’s the difference? These drugs both contain buprenorphine, which means they act as partial opioid agonists, most notably at the mu-receptor. However, since Subutex does not contain Naloxone, it has a greater potential for abuse and misuse. Naloxone is a drug that was developed in the 1960s to counteract the effects of opioids, especially in the event of an overdose.
It counteracts opioid effects by functioning as a competitive opioid antagonist, meaning it binds to opioid receptors with a higher affinity than agonists. After binding to the receptors it prevents activity and thus an individual will feel no opioid-based effects. Naloxone in particular has a high affinity for the mu-receptor, which offsets the buprenorphine partial agonism, especially when ingested at high doses.

Reckitt Benckiser Pharmaceuticals first developed Subutex, which contained just buprenorphine hydrochloride as the active component. In effort to further reduce abuse potential and make the drug safer, they formulated the drug Suboxone with both buprenorphine and naloxone at a 4:1 ratio. For many individuals, Subutex is administered during early stages of opioid replacement therapy, and Suboxone is given during the maintenance phase.
Abuse Potential Since both Subutex and Suboxone are classified as “Schedule III” controlled-substance, it would be logical to conclude that both have equal potential for abuse. Schedule III substances are regarded as having less abuse potential than Schedule II drugs and are known to have medically accepted uses. Additionally, Schedule III drugs like Subutex and Suboxone may lead to some physical dependence and significant psychological dependence.
Some speculate that Subutex has a greater potential for abuse than Suboxone, especially when administered at high doses. The Naloxone component of Suboxone acts as a competitive opioid antagonist with a high affinity for the mu-receptor. At higher doses, enough Naloxone binds to the mu-receptor and is thought to inhibit additional Buprenorphine mu-receptor stimulation.
Many individuals attempting to abuse Buprenorphine inject it intravenously in attempt to get “high” during opioid replacement therapy. This intravenous injection is thought to provide individuals with a more potent opioid “high.” Should an individual attempt to take intravenous Suboxone, the Naloxone component is thought to trigger severe withdrawal symptoms rather than a Buprenorphine-induced “high.”
Evidence suggests that individuals dependent on potent opioids experience an array of unpleasant symptoms should they attempt to administer Suboxone via intravenous injection or intranasal insufflation. Individuals that are dependent on less potent opioids may not experience as many unpleasant symptoms following intravenous Suboxone administration as those who are highly

dependent. That said, the Naloxone will still mitigate the opioid effect of the Buprenorphine, thus making it unlikely to achieve opioid intoxication.
Among non-dependent opioid abusers, it seems as if Subutex and Suboxone are equal in their abuse potential. A very small-scale study revealed that high doses of Subutex and Suboxone resulted in similar opioid agonist-like effects. The researchers suggested that there was not enough evidence to suggest that Naloxone mitigated Buprenorphine’s opioid agonist effects in non-dependent abusers when administered sublingually.
As a recap, Subutex has a significant abuse potential among individuals with opioid dependence and among non-dependent addicts. Suboxone has less potential for abuse, especially among those dependent upon potent opioids – this is due to the presence of Naloxone. Among non-dependent abusers, the abuse potential is regarded as being relatively similar.
§ Source: http://www.ncbi.nlm.nih.gov/pubmed/10928310 § Source: http://www.ncbi.nlm.nih.gov/pubmed/20403021 § Source: http://www.ncbi.nlm.nih.gov/pubmed/25060839 Cost: Which is more expensive? Those comparing Subutex and Suboxone may want to consider the cost of each medication. Due to the fact that both drugs contain mostly Buprenorphine as the active ingredient, they are similar. If you have poor insurance or have to pay out-of-pocket for your medications, you may decide to opt for the least expensive formulation.
Subutex is only manufactured in generic format as “buprenorphine” and can be obtained at a price of $45 to $70 for 30 sublingual 2 mg tablets, and between $75 and $110 for 30 sublingual 8 mg tablets. Brand name Suboxone can be purchased for a price between $128 and $470 for a 30 sublingual films. The greater the dosage of the Suboxone films, the greater the cost.

Generic Suboxone (Buprenorphine / Naloxone) can be purchased in the format of sublingual tablets for a price between $75 and $190 for a 30 day supply; the greater the dosage, the higher the cost. Clearly the cheapest option is Subutex, followed by generic Suboxone tablets, and the most expensive option is brand-name Suboxone films. Some people may prefer the sublingual films over the tablets and therefore may be willing to pay extra for them.
Dosage & Formats Subutex is manufactured in the format of sublingual tablets with dosages of 2 mg and 8 mg. Sublingual tablets are a formulation of the drug that can be placed under the tongue and that dissolve in the mouth. The dosing options and formats of Subutex are relatively limited by comparison to Suboxone.
Suboxone is manufactured in the format of both sublingual tablets and sublingual film. The dosing options for the sublingual film are as follows: 2 mg/0.5 mg, 4 mg/1 mg, 8 mg/2 mg, and 12 mg/3 mg. The first number of each dose indicates the amount of buprenorphine, while the second indicates the amount of naloxone; each dose is engineered to have a 4:1 ratio.
Like the sublingual Subutex tablets, sublingual Suboxone tablets are only manufactured in 2 dosing options including: 2 mg/0.5 mg and 8 mg/2 mg. There really isn’t much difference in the sublingual tablet dosing options by comparison of Subutex to Suboxone, but there are 2 additional dosing options associated with the Suboxone sublingual film.
Most individuals would agree that sublingual film and sublingual tablets are similar. Some people may prefer to put a film under their tongue, while others may find the tablets easier to administer; it’s ultimately a personal preference. Suboxone may be considered advantageous over Subutex due to the fact that it offers multiple sublingual formats and extra dosing increments.
Efficacy: Which drug is more effective?

Everyone wants to know whether Subutex or Suboxone is more effective for treating opioid dependence. There is no definitive evidence suggesting that one drug is superior to the other in regards to efficacy. Both contain the active ingredient buprenorphine, which acts as a partial agonist with most of its effect elicited upon the mu-receptor.
Certain individuals may respond better to higher doses of Subutex than Suboxone in early stages of treating opioid dependence. This is due to the fact that at high doses, it is speculated that Naloxone may counteract some of the mu-receptor stimulation from the Buprenorphine. Therefore some professionals may initially treat someone with Subutex and transition them to Suboxone after several weeks.
A study published in 2010 analyzed the effects of switching individuals from Subutex to Suboxone. The study involved 94 participants that were initially treated with 8 mg per day of buprenorphine monotherapy for an average of 840 days. They were eventually switched to Suboxone (buprenorphine / naloxone) and the outcomes were monitored.
The participants rated their level of satisfaction with Suboxone in respect to management of withdrawal symptoms. Urinary toxicology data was collected throughout the study and revealed a reduction in positive toxicology tests after switching to Suboxone. This meant that they were less likely to abuse other drugs (e.g. heroin, cocaine, etc.) on Suboxone than Subutex.
Researchers also discovered that the time between clinic visits was increased with Suboxone compared to Subutex, in part due to less extracurricular drug abuse (as revealed by toxicology reports). Both drugs are considered well-tolerated, but there may be subtle advantages associated with Suboxone including: reduced abuse potential and reduced likelihood to abuse illicit drugs during treatment of opioid dependence.
§ Source: http://www.ncbi.nlm.nih.gov/pubmed/20450243 Mechanisms of action

The mechanisms of action associated with Subutex and Suboxone are nearly the same. Subutex contains Buprenorphine Hydrochloride, which acts as a partial mu-opioid receptor agonist. Buprenorphine also elicits effects as a kappa receptor antagonist, delta receptor antagonist, and has a fairly high affinity for the sigma receptor. It is thought to have a minor affinity for the nociceptin receptor as well and inhibit voltage-gated sodium channels.
Since Suboxone is comprised of 80% buprenorphine, its mechanism of action is nearly identical to that of Subutex. However, Suboxone was engineered to contain the additional component of Naloxone, which functions as a pure opioid-receptor antagonist. It has a high affinity for the mu-receptor as a competitive antagonist and modest antagonist effects on kappa and delta opioid receptors.
As a pure antagonist, Naloxone is capable of binding to opioid receptors and ultimately preventing stimulation from opioid receptor agonists. Since 20% of Suboxone is formulated with Naloxone, it elicits these additional effects, compared to Subutex which solely contains Buprenorphine.
§ Source: http://www.ncbi.nlm.nih.gov/pubmed/22504149 § Source: http://www.ncbi.nlm.nih.gov/pubmed/12435410 § Source: http://www.ncbi.nlm.nih.gov/pubmed/24903063 Medical Uses Subutex and Suboxone are FDA approved for the treatment of opioid dependence. Despite the fact that they are sometimes prescribed off-label to treat chronic pain, they are not technically approved for that condition. Subutex and Suboxone are different in that Suboxone is considered to have slightly less potential for abuse and therefore is prescribed more frequently as an investigational drug.
Investigational uses for Suboxone include the treatment of neonatal abstinence syndrome and treatment-resistant depression. Neonatal abstinence syndrome is a condition in which a baby is exposed to opioids via a pregnant mother and experienced withdrawal symptoms when the mother stops using and/or after

birth. Specially formatted Suboxone for infants is currently being studied for this condition.
In rare cases, individuals are prescribed Suboxone as an antidepressant augmentation strategy. While Suboxone may be highly effective in treating depressive symptoms, it is seldom prescribed due to its lacking of approval and the presence of safer, more established options. A drug similar to Suboxone called “ALKS-5461” has demonstrated significant efficacy in alleviating depressive symptoms. Popularity Subutex and Suboxone are considered relatively popular drugs in the realm of opioid replacement therapy. Suboxone is the more popular drug by comparison due to the fact that it is regarded as a safer, upgraded version of Subutex. From the perspective of a hardcore opioid addicts, Subutex may be the more sought out format of the drug.
That said, among medical professionals, Suboxone is clearly the favorable treatment for opioid dependence. In part, this popularity is due to the added presence of Naloxone, a component that has been marketed to produce a “ceiling effect.” This purported “ceiling effect” is thought to prevent any additional “high” or intoxication past a certain dose, making abuse less likely.
In addition, the Naloxone within Suboxone inhibits the intravenous and intranasal potential for a “high” compared to Subutex. Popularity of Suboxone has largely increased due to the belief that it is both newer and regarded as being a safer treatment for opioid dependence.
Side Effects Theoretically, the side effect profiles of Subutex and Suboxone shouldn’t be much different. Common side effects associated with both drugs include: constipation, dizziness, drowsiness, headaches, and nausea. Some speculate that since Subutex does not contain Naloxone, that it has a favorable side effect profile.

Rationally it would make sense that among individuals sensitive to the effect of Naloxone, side effects may emerge. There is an extra substance within Suboxone, and therefore is likely an increased potential for side effects. Examples of common side effects associated with Naloxone include: constipation, dizziness, drowsiness, dry mouth, lightheadedness, and sweating.
The presence of Naloxone may amplify certain side effects derived from Buprenorphine, and may trigger additional side effects. Naloxone has potential to induce catecholamine release, cause pulmonary edema, and cardiac arrythmias. For this reason, Subutex may have a slightly favorable side effect profile.
That said, the counterpoint could be made that Naloxone may mitigate certain side effects associated with Buprenorphine. The number and severity of side effects experienced may be subject to significant individual variation. Some people may report reductions in side effects when taking Subutex, while others may find that they have less side effects on Suboxone.
§ Source: http://www.ncbi.nlm.nih.gov/pubmed/17367258 Withdrawal The withdrawal symptoms associated with Subutex and Suboxone tend to be most severe within the first couple weeks of discontinuation. Most individuals find that withdrawal gets easier as time continues to pass. This is in part due to the fact that a person’s neurophysiology is being restored back to homeostatic functioning.
Those that took Subutex or Suboxone for a long-term and/or a high dose are likely to have the most severe withdrawal periods. Many long-term, high-dose users will experience protracted discontinuation effects in the form of “post-acute withdrawal syndrome” (PAWS) which can last for months (or longer) following the date of discontinuation. Some individuals may have a tougher time discontinuing Subutex, while others may have a more difficult time coping with Suboxone withdrawal.

Both should produce similar symptoms due to the fact that individuals are primarily withdrawing from Buprenorphine. While users may not experience any withdrawal symptoms from the Naloxone component, to suggest that there’s no discontinuation effect (even if undetectable) from Naloxone is relatively short-sighted. Certain individuals may have a slightly easier time discontinuing Subutex for this reason.
Similarities (Recap): Subutex vs. Suboxone Listed below are the similarities shared between Subutex and Suboxone.
§ Drug type: Subutex and Suboxone are regarded as semisynthetic opioids and are first-line treatments for opioid dependence.
§ Duration of effect: The duration of effect associated with these drugs is 24 hours, with a 8 to 12 hour analgesic window.
§ Efficacy: Subutex and Suboxone are regarded as having nearly identical efficacy due to the same dosage content of buprenorphine.
§ Generic availability: Generic formats are available for both drugs. Subutex is manufactured as “buprenorphine hydrochloride” and Suboxone is sold as “buprenorphine/naloxone.”
§ Half-life: The elimination half-life for both drugs is thought to range between 24 and 42 hours.
§ Legal status: Both drugs are classified as “Schedule III” controlled-substances.
§ Medical uses: Both medications have been FDA approved for the treatment of opioid dependence.
§ Manufacturers: Reckitt Benckiser Pharmaceuticals is responsible for manufacturing both Subutex and Suboxone.
§ Withdrawal: Discontinuation from Subutex and Suboxone is thought to be relatively difficult. There is no evidence that discontinuation from one is more or less severe than the other.
Differences (Recap): Subutex vs. Suboxone Listed below are some differences between Subutex and Suboxone.
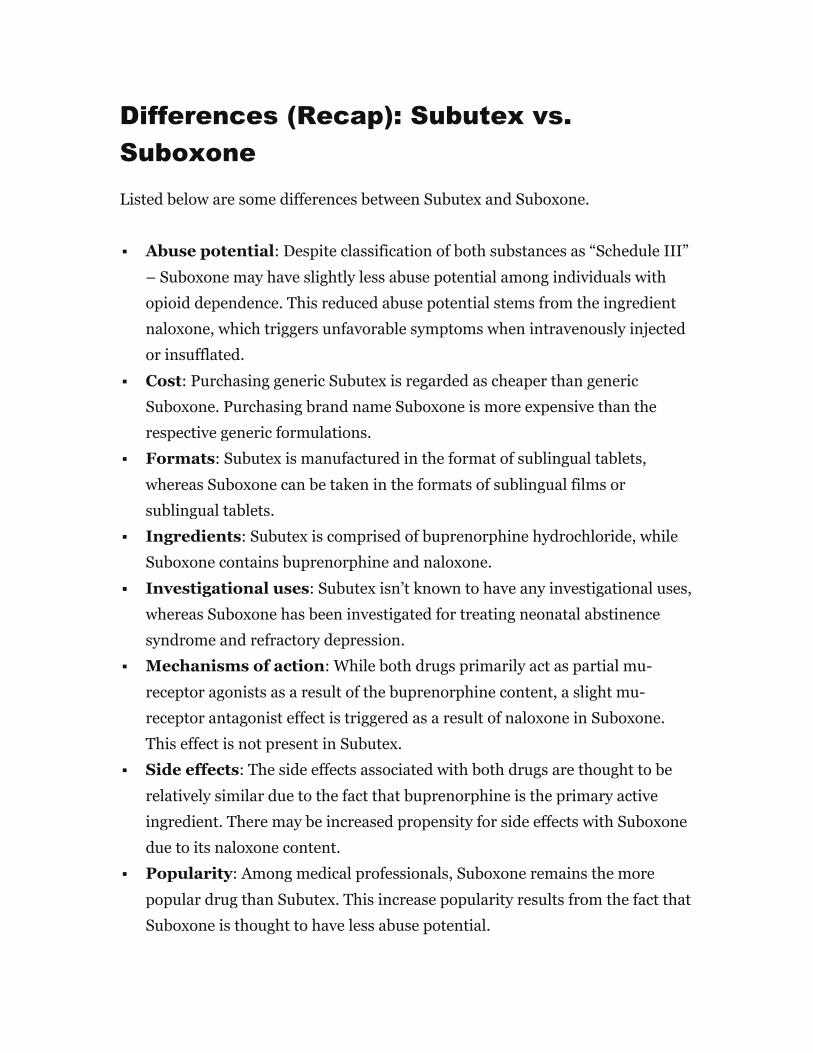
§ Abuse potential: Despite classification of both substances as “Schedule III” – Suboxone may have slightly less abuse potential among individuals with opioid dependence. This reduced abuse potential stems from the ingredient naloxone, which triggers unfavorable symptoms when intravenously injected or insufflated.
§ Cost: Purchasing generic Subutex is regarded as cheaper than generic Suboxone. Purchasing brand name Suboxone is more expensive than the respective generic formulations.
§ Formats: Subutex is manufactured in the format of sublingual tablets, whereas Suboxone can be taken in the formats of sublingual films or sublingual tablets.
§ Ingredients: Subutex is comprised of buprenorphine hydrochloride, while Suboxone contains buprenorphine and naloxone.
§ Investigational uses: Subutex isn’t known to have any investigational uses, whereas Suboxone has been investigated for treating neonatal abstinence syndrome and refractory depression.
§ Mechanisms of action: While both drugs primarily act as partial mu-receptor agonists as a result of the buprenorphine content, a slight mu-receptor antagonist effect is triggered as a result of naloxone in Suboxone. This effect is not present in Subutex.
§ Side effects: The side effects associated with both drugs are thought to be relatively similar due to the fact that buprenorphine is the primary active ingredient. There may be increased propensity for side effects with Suboxone due to its naloxone content.
§ Popularity: Among medical professionals, Suboxone remains the more popular drug than Subutex. This increase popularity results from the fact that Suboxone is thought to have less abuse potential.

Which drug is a better opioid replacement therapy? Subutex vs. Suboxone. Anecdotal reports across the internet may claim that Subutex is better than Suboxone, while others may claim the opposite. There is some evidence that the presence of naloxone within Suboxone may result in more favorable opioid withdrawal symptoms during the transition from an illicit drug (e.g. heroin) to the replacement. This favorable mitigation of withdrawal symptoms during the transition may be due to the presence of naloxone.
One study involving patients transitioning from Subutex to Suboxone noted that after 2 weeks of Suboxone usage, participants were less likely to abuse illicit opioids. They were able to detect a reduction in illicit opioid abuse as a result of toxicology data collected. Some people like the fact that Suboxone is manufactured in multiple formats (sublingual film and sublingual tablet) compared to Subutex which is only sold in the format of sublingual tablets.
In terms of side effects, some individuals may respond slightly better to Subutex due to the fact that it contains zero naloxone, while others may respond better to the Suboxone as a result of the naloxone content. In some cases, a doctor may prescribe Subutex in early stages of opioid replacement therapy and transition a patient to Suboxone after a couple weeks. This is due to the fact that Suboxone is less likely to be abused, particularly intravenous or intranasal due to the naloxone content.
Some have argued that the naloxone content within Suboxone was mostly added for marketing purposes and that it doesn’t really provide a “ceiling effect” or reduce abuse potential. This speculation has to do with the fact that the patent expired for Subutex, whereas the patent had not expired for Suboxone. This may have lead the developers to create a campaign suggesting that their revised formulation of Suboxone is favorable to the generic Subutex.
Ultimately there is some evidence to suggest that Suboxone may be the safer option with reduced abuse potential when compared to Subutex. For this reason,

Suboxone is generally regarded as the superior option for the treatment of opioid dependence. However, cost differences and unfavorable side effects associated with naloxone may prompt some patients to request Subutex over Suboxone.
Which drug do you prefer: Subutex or Suboxone? If you have experience using both Subutex and Suboxone, feel free to share a comment regarding any differences you noticed between the two drugs. Specifically, you may want to mention whether you experienced an increased number of unfavorable side effects while taking one drug compared to the other. If you’ve had the experience of withdrawing from both, mention whether one was easier than the other.
Keep in mind that some perceived differences between the two drugs may be due to: naloxone content, dosage differences, a nocebo effect, and/or subjectivity.
Zubsolv vs. Suboxone: What’s the Difference? There are many new medications that have been engineered specifically for the treatment of opioid dependence. Those dependent on opioids tend to experience debilitating physical and psychological withdrawal symptoms upon discontinuation. To help individuals discontinue illicit opioids like heroin, an “opioid replacement therapy” drug is often prescribed.
Two of the most common opioid replacement therapy drug options include Zubsolv and Suboxone. Suboxone is a drug that hit the market in 2002 as a treatment for opioid dependence. It differed from previous opioid replacement therapy drugs in that it was formulated with a 4:1 ratio of buprenorphine to naloxone.

The buprenorphine was thought to elicit partial agonist effects on the mu-receptor, while the naloxone was included in the formulation to limit abuse potential. Zubsolv is similar to Suboxone in that it contains both buprenorphine and naloxone at approximately 4:1 ratios. However, Zubsolv is considered an improvement over Suboxone in that it has a higher bioavailability, faster dissolve time, and smaller tablet size by comparison.
Zubsolv vs. Suboxone Comparison Chart The chart below highlights the general characteristics of both Zubsolv and Suboxone. Both drugs contain the same active ingredients and are administered sublingually. They are manufactured by different companies and are known to differ in dosing options.
Zubsolv Suboxone
Drug type Synthetic opioid (Partial agonist)
Synthetic opioid (Partial agonist)
Approved uses Opioid dependence. Opioid dependence.
Ingredients Buprenorphine (~80%) / Naloxone (~20%)
Buprenorphine (80%) / Naloxone (20%)
Formats Sublingual tablet. Sublingual film. Sublingual tablet.
Dosages 1.4 mg/0.36 mg or 5.7 mg/1.4 mg or 8.6 mg/2.1 mg or 11.4
mg/2.9 mg
Sublingual film: 2 mg/0.5 mg or 4 mg/1 mg or 8 mg/2 mg or 12 mg/3 mg + Tablet: 2 mg/0.5 mg
or 8 mg/2 mg
Manufacturer Orexo Pharmaceuticals Reckitt Benckiser Pharmaceuticals
Legal Status Schedule III (US) Schedule III (US)
Mechanism of action
Functions primarily as a non-‐selective mixed
Functions primarily as a non-‐selective mixed

Zubsolv Suboxone
agonist/antagonist opioid receptor modulator. Acts as a partial agonist at the mu-‐receptor – antagonist at the kappa-‐receptor – and antagonist at the delta-‐
receptor. It has a high affinity for the sigma-‐receptor and a minimal effect upon the nociceptin receptor.
Buprenorphine also inhibits voltage-‐gated sodium channels. The Naloxone
component of Zubsolv has a high affinity for the mu-‐receptor as a competitive antagonist. It also elicits antagonist effect upon the kappa and delta receptors.
agonist/antagonist opioid receptor modulator. Acts as a partial agonist at the mu-‐receptor – antagonist at the kappa-‐receptor – and antagonist at the delta-‐
receptor. It has a high affinity for the sigma-‐receptor and a minimal effect upon the nociceptin receptor.
Buprenorphine also inhibits voltage-‐gated sodium channels. The Naloxone
component of Suboxone has a high affinity for the mu-‐receptor as a competitive antagonist. It also elicits antagonist effect upon the kappa and delta receptors.
Generic version?
No. Yes.
Half life 24 to 42 hours 24 to 42 hours
Common side effects
Constipation. Dizziness. Drowsiness. Dry mouth. Lightheadedness. Nausea. Sweating. Vomiting.
Constipation. Dizziness. Drowsiness. Dry mouth. Lightheadedness. Nausea. Sweating. Vomiting.
Date approved July (2013) October (2002)
Effect duration 24 hours (Analgesic: 8 to 12 hours)
24 hours (Analgesic: 8 to 12 hours)
Investigational uses
Chronic Pain. Chronic Pain. Neonatal abstinence syndrome. Treatment-‐resistant
depression. (Read: Suboxone for depression).

Zubsolv vs. Suboxone: What’s the difference? The primary difference between Zubsolv and Suboxone is the bioavailability of each drug. Zubsolv is regarded as having a significantly greater bioavailability than Suboxone. This means that when you take Zubsolv, the percentage of the drug that has an active effect is greater than that of Suboxone.
The active ingredients of both drugs include buprenorphine and naloxone. These ingredients are present at exact 4:1 ratios in Suboxone and approximate 4:1 ratios in Zubsolv. Since your body uses Zubsolv more efficiently than it uses Suboxone, it takes a greater dose of Suboxone to elicit the same effect as a lower dose of Zubsolv.
In addition, the Zubsolv sublingual formulation dissolves quicker under the tongue than Suboxone and includes a menthol (mint) flavor. Many individuals and doctors regard Zubsolv as an “upgraded” version of Suboxone. Although Suboxone remains a popular opioid replacement therapy option, many believe that the competitor drug Zubsolv is a superior formula.
Abuse Potential Zubsolv and Suboxone are regarded as “Schedule III” controlled-substances, meaning they have equal potential for abuse. Schedule III drugs tend to have reduced potential for abuse compared to those considered “Schedule II” and are known to have medically accepted uses. It is known that Schedule III substances like Zubsolv and Suboxone may cause dependence physical and psychological dependence.
Both of these formulations contain buprenorphine and naloxone. By itself, buprenorphine is regarded as one of the most addictive drugs; its addiction rating is “1.64” on a scale from 0 to 3. However, since naloxone is included in each of

the formulations, it limits potential for abuse, especially by those that attempt to intravenously inject or snort (insufflate) either drug. Should an individual intravenously inject or intranasally insufflate either Zubsolv or Suboxone, the naloxone component is thought to mitigate any “high” that a person would’ve received from the buprenorphine component. While buprenorphine stimulates the mu-receptor as a partial agonist, naloxone acts as a competitive mu-receptor antagonist and serves as a built-in safety mechanism.
As an antagonist, the naloxone binds to the mu-receptor and inhibits any agonist stimulation from the buprenorphine, thus sending the individual into full-blown withdrawal. Individuals that were dependent on highly-potent opioids that attempt to abuse Zubsolv or Suboxone may experience unpleasant symptoms. Those that were dependent on less potent opioids may not experience unpleasant symptoms, but are unlikely to derive any “high” from either drug.
The potential for abuse of Zubsolv and Suboxone is considered high among those who aren’t physically dependent on opioids. Since both drugs contain “naloxone” their potential for abuse is lower than formulations without it (e.g. Subutex). Neither Zubsolv nor Suboxone should be considered to have any greater potential for abuse compared to the other; their ingredient composition is nearly identical.
§ Source: http://www.ncbi.nlm.nih.gov/pubmed/10928310 § Source: http://www.ncbi.nlm.nih.gov/pubmed/20403021 § Source: http://www.ncbi.nlm.nih.gov/pubmed/25060839 Cost: Which is more expensive? Those considering Zubsolv and Suboxone as potential opioid replacement therapy options may also want to consider the price of each drug. Individuals without good insurance coverage may end up having to pay for a prescription out-of-pocket and therefore probably will want to chose the most affordable option. The cost for a 30 day supply of Zubsolv ranges between $221 and $240.

Due to the fact that Zubsolv wasn’t approved until 2013, a generic will not be available for awhile. Therefore if you’re getting Zubsolv without insurance, the associated costs can get quite expensive. The cost for a 30 day supply of “brand name” Suboxone sublingual films will cost between $130 and $470; the higher the dosage, the greater the cost.
Fortunately, Suboxone is sold under the generic “buprenorphine / naloxone” ranging between $75 and $190 for a 30 day supply. This means that if you’re looking to save yourself money, the generic Suboxone is probably your best option. Zubsolv tends to be more expensive than certain doses of brand name Suboxone, but at the highest doses, Suboxone may be more expensive.
Dosage & Formats Zubsolv is manufactured in a sublingual tablet format with a variety of dosages including: 1.4 mg/0.36 mg, 5.7 mg/1.4 mg, 8.6 mg/2.1 mg and 11.4 mg/2.9 mg. The first number associated with each pill is the dosage of buprenorphine, while the second number reflects the dosage of naloxone. As you can see, each pill contains an approximate (but not exact) 4:1 ratio of buprenorphine to naloxone.
Suboxone is manufactured in multiple formats including sublingual films and sublingual tablets. The sublingual Suboxone films have dosages of: 2 mg/0.5 mg, 4 mg/1 mg, 8 mg/2 mg, and 12 mg/3 mg. The generic sublingual Suboxone tablets are manufactured with only 2 dosing options of 2 mg/0.5 mg and 8 mg/2 mg. The first number in each formulation reflects the buprenorphine dose, while the second reflects the naloxone.
As you can see, the ratio of buprenorphine to naloxone in Suboxone is exactly 4:1. The dosage ratios differ in Zubsolv such as: 3.8 to 1, 4.07 to 1, 4.09 to 1, and 3.93 to 1 (from lowest dose to highest). That said, Zubsolv’s is manufactured in 4 doses to match the 4 dosing options of Suboxone. The only difference between the two is that Suboxone is manufactured in sublingual “films” and “tablets” whereas Zubsolv is only manufactured in sublingual “tablets.”

Each dose of Zubsolv is thought to be calibrated to elicit similar potency as higher doses of Suboxone. For example, the Zubsolv 8.6 mg/2.1 mg is thought to correspond with the 12 mg/3 mg of Suboxone. Some individuals may like the idea of taking a lower dosage that has a higher bioavailability (Zubsolv) compared to a higher dosage with a lower bioavailability (Suboxone).
Efficacy: Which drug is more effective? Due to the fact that Zubsolv has a greater bioavailability than Suboxone, a lower dose can be taken to achieve the same effect as a higher dose of Suboxone. The percentage of Zubsolv that has an effect is greater than the percentage of Suboxone that has an effect. Every dosing option of Zubsolv is equivalent to a higher corresponding dosage of Suboxone.
For example, the Zubsolv 1.4 mg/0.36 mg is equivalent to the Suboxone 2 mg/0.5 mg. Similarly the Zubsolv 5.7 mg is equivalent to the Suboxone 8 mg and the Zubsolv 8.6 mg is equivalent to the Suboxone 12 mg. There is even a higher dose of Zubsolv 11.4 mg/2.9 mg that would be equivalent to a Suboxone 16 mg if it was manufactured.
The onset of action is quicker for Zubsolv due to the fact that it dissolves sublingually in seconds rather than minutes like Suboxone. It also may have a slightly longer duration of effect by comparison. Clearly Zubsolv is the more potent drug due to its enhanced bioavailability and as a result, it may be slightly more effective than Suboxone.
That said, the difference in efficacy is unlikely to be significant in a head-to-head comparison. If dosage equivalencies were taken into account, the efficacy in treating opioid dependence should be nearly identical. Subtle differences may result from the ratios of buprenorphine to naloxone, which differ slightly in Zubsolv based on dose compared to Suboxone.
If the naloxone component offsets some of the buprenorphine, the lowest dose (1.4 mg/0.36 mg) and the highest dose of Zubsolv (11.4 mg/2.9 mg) have ratios of

less than 4:1 buprenorphine to naloxone, which may make them slightly less effective than Suboxone; this is assuming the naloxone elicits a slight antagonist effect. However, the middle doses of Zubsolv including the 5.7 mg/1.4 mg and 8.6 mg/2.1 mg may be slightly more effective than Suboxone due to greater than 4:1 ratios of buprenorphine to naloxone.
Mechanisms of action The respective mechanisms of action associated with Zubsolv and Suboxone are the same. The buprenorphine component of each drug functions primarily as a mu-opioid receptor partial agonist. This produces less of an opoioid effect than a full agonist, but still may result in sedation, reduced blood pressure, analgesia, euphoria, nausea, and relaxation.
The primary benefit derived from these drugs is a result of the buprenorphine, hence it accounts for nearly 80% of each formulation. The buprenorphine also acts as a kappa receptor and delta receptor antagonist, meaning it inhibits stimulation at these sites. In addition, it is known to have a subtle affinity for the nocioceptin receptor and is capable of blocking various voltage-gated sodium channels.
The remaining 20% of Zubsolv and Suboxone formulations is comprised of naloxone. Naloxone is a drug that acts as a pure opioid-receptor antagonist. It acts primarily as a competitive antagonist at the mu-opioid receptor and acts as a moderate antagonist at kappa and delta opioid receptors. The effect of naloxone is thought to mitigate abuse and prevent excess intoxication as a result of the buprenorphine.
§ Source: http://www.ncbi.nlm.nih.gov/pubmed/22504149 § Source: http://www.ncbi.nlm.nih.gov/pubmed/12435410 § Source: http://www.ncbi.nlm.nih.gov/pubmed/24903063 Medical Uses Zubsolv and Suboxone are drugs solely approved by the FDA for the treatment of opioid dependence. They are not formally approved to treat chronic pain, despite

the fact that they may be approved off-label for this purpose. Both drugs are regarded as being significantly more effective than a placebo in double-blind, randomized, clinical trials for the treatment of opioid dependence.
Due to the fact that Suboxone has been on the market for a longer period of time, it has been investigated for the treatment of neonatal abstinence syndrome. This is a condition in which a baby was exposed to opioids during pregnancy and experiences withdrawal symptoms while in the womb or following birth. Specially engineered neonatal Suboxone is being investigated by the FDA for the treatment of this condition.
Furthermore, some doctors may prescribe Suboxone as an antidepressant augmentation strategy for individuals suffering from refractory depression with a history of opioid dependence. Many anecdotal reports suggest that it is significantly more effective than standard antidepressant options. A drug similar to Suboxone called “ALKS-5461” which contains buprenorphine and samidorphan has shown promise as an adjunct treatment in cases of refractory depression. Suboxone is more commonly prescribed off-label compared to Zubsolv and has been investigated for the treatment of neonatal abstinence syndrome and depression. Zubsolv is a relatively new drug and therefore hasn’t gained as much widespread off-label use nor investigational use by comparison. That said, the outcomes associated with using either drug should be nearly identical.
Popularity In the mainstream, Suboxone remains the more popular opioid replacement therapy option. Some would argue that there’s a battle between Methadone and Suboxone for the top opioid replacement therapy drug. That said, doctors have recognized that Suboxone is likely safer than Methadone due to its decreased potential for addiction and reduced potency as a partial mu-receptor agonist. Since Suboxone also contains naloxone, it is thought to have a reduce potential for abuse. The reduced abuse potential is appealing to professionals. Although Zubsolv isn’t yet as popular as Suboxone or Methadone, it is gaining

momentum. Professionals are starting to recognize that its higher bioavailability and quicker absorption make it superior to Suboxone; this should bolster Zubsolv’s popularity in forthcoming years.
Among patients that have tried both Suboxone and Zubsolv, most prefer Zubsolv for a number of reasons. Most individuals like the fact that Zubsolv dissolves quickly – in seconds rather than minutes associated with Suboxone. The Zubsolv tablets also are very small and provide a menthol, minty flavor which many individuals prefer over Suboxone.
Side Effects The side effect profiles of Zubsolv and Suboxone aren’t much different. This is due to the fact that both contain approximately 80% buprenorphine and 20% naloxone. Common side effects associated with these medications include: constipation, dizziness, drowsiness, headaches, and nausea.
Due to the fact that both drugs contain the same active ingredients, there shouldn’t be many differences in side effects from Zubsolv compared to Suboxone. Some claim that since Zubsolv is more efficiently absorbed that side effects are less likely; whether this is true is unknown. Those experiencing side effect differences on one drug compared to the other are likely placebo-related.
If you experience more side effects on one drug compared to the other, it may have to do with the dosing. As was already mentioned, lower doses of Zubsolv correspond with higher doses of Suboxone. The higher the dose of either drug that you’re taking, the more likely you’ll be to experience side effects. Subtle differences in perceived side effects may be due to slight increases or decreases in the ratio of buprenorphine to naloxone as occur in Zubsolv.
Withdrawal The discontinuation process associated with Zubsolv and Suboxone can be difficult. In fact, many claim that discontinuing these medications is nearly as difficult as discontinuing more potent opioids. This is due to the fact that many

individuals stay on Zubsolv or Suboxone for an extended duration of time without making any effort to reduce their dosage.
The longer the time span over which a person takes either of these drugs, the more difficult the discontinuation process will be. There are many anecdotal reports highlighting the difficulty of Suboxone withdrawal, but not as many discussing Zubsolv withdrawal due to the fact that it is a newer drug. Both drugs should theoretically have the same degree of difficulty in regards to withdrawal. Since both drugs are manufactured in 4 dosing options, the tapering process shouldn’t be considered more or less difficult with one drug compared to the other. Many individuals discontinuing from high doses may experience post-acute withdrawal syndrome (PAWS). This means that withdrawal symptoms may linger for months following the date of discontinuation from either drug.
Similarities (Recap): Zubsolv vs. Suboxone Below is a recap of the similarities shared between Zubsolv and Suboxone.
§ Abuse potential: Both drugs are considered to have a minimized potential for abuse when used in accordance to medical recommendations.
§ Dosages: Each drug is manufactured with four dosing options. While the dosages differ in milligrams of buprenorphine and naloxone, most are equivalent in potency.
§ Drug type: Zubsolv and Suboxone are considered semisynthetic opioids and are regarded as first-line treatments for opioid dependence.
§ Duration of effect: With both drugs, the duration of effect is thought to be 24 hours, with an 8 to 12 hour analgesic effect.
§ Efficacy: The efficacy associated with Zubsolv is no different than that of Suboxone when dosages are properly calibrated.
§ Half-life: The associated half-life of elimination for both drugs is between 24 and 42 hours.

§ Ingredients: The ingredient composition associated with these drugs is identical with approximately 80% buprenorphine and 20% naloxone.
§ Legal status: Both drugs are classified as “Schedule III” controlled-substances.
§ Mechanisms of action: These drugs have the same mechanisms of action as a result of identical ingredients and nearly identical contents of buprenorphine and naloxone.
§ Medical uses: Each drug has been granted FDA approval to treat opioid dependence.
§ Side effects: The side effect profile of Zubsolv and Suboxone should be identical. Common side effects include dizziness, dry mouth, nausea, and sweating.
§ Withdrawal: Discontinuation of either drug will result in withdrawal symptoms. There is no evidence to suggest that the difficulty of withdrawal is greater with one drug than the other.
Differences (Recap): Zubsolv vs. Suboxone Below is a synopsis of some differences between Zubsolv and Suboxone.
§ Aftertaste: Zubsolv has a built-in “menthol” flavoring which leaves a minty aftertaste following sublingual administration. Many individuals dislike the taste of Suboxone or find that it lacks any flavor.
§ Bioavailability: Zubsolv has a significantly greater bioavailability than Suboxone (approximately 1.4 times). This means that a lower dose of Zubsolv delivers the same effect as a higher dose of Suboxone.
§ Cost: Buying a 30 day supply of generic Suboxone is cheaper than Zubsolv. Purchasing brand name Zubsolv is more expensive than lower-dose Suboxone, but cheaper than higher-dose Suboxone.

§ Dissolving speed: Zubsolv proved in clinical trials that it dissolved significantly faster sublingually than Suboxone. Zubsolv dissolves in seconds, whereas Suboxone dissolves in minutes.
§ Formats: Both drugs are available in sublingual tablet format, but Suboxone is also manufactured in the form of sublingual “films.”
§ Generic availability: Suboxone is manufactured in the generic form of “buprenorphine / naloxone” whereas Zubsolv remains patent-protected.
§ Investigational uses: Suboxone has been subject to significantly greater investigational use including: neonatal abstinence syndrome and depression, whereas Zubsolv has not.
§ Manufacturers: Reckitt Benckiser Pharmaceuticals manufactures Suboxone, and Orexo Pharmaceuticals manufactures Zubsolv.
§ Onset of action: Zubsolv has the quicker onset of action as a result of its faster dissolve time.
§ Popularity: Suboxone remains more popular than Zubsolv due to the fact that it has been on the market since 2002, whereas Zubsolv didn’t enter the market until 2013.
Which drug is a better at treating opioid dependence? Zubsolv vs. Suboxone. Neither Zubsolv nor Suboxone should be regarded as a superior in efficacy when compared to the other. Both are effective options for the treatment of opioid dependence and the respective formulations are nearly identical. Zubsolv is regarded as a newer drug, and therefore may be preferred by doctors and patients alike for the treatment of opioid dependence.
Scientific evidence suggest that Zubsolv has nearly 1.4 times the bioavailability as Suboxone, it dissolves significantly quicker (seconds rather than minutes), and it leaves a preferable (menthol) aftertaste in the mouth following sublingual administration. While nothing really changed in terms of ingredients or efficacy, there are some “upgrades” associated with Zubsolv compared to Suboxone.
For these upgrades such as the: increased bioavailability, quicker onset of action (faster dissolve time), and superior aftertaste – you will pay extra. The cost of

Zubsolv is significantly greater than generic Suboxone. It will also cost more than low doses of brand name Suboxone. If you are taking high doses of brand name Suboxone, Zubsolv is actually a bit cheaper.
Which drug do you prefer: Zubsolv or Suboxone? If you have taken both Zubsolv and Suboxone, be sure to share a comment regarding your preference for one drug over the other. If you prefer Zubsolv, is it due to the fact that it dissolves quicker or tastes better? If you subjectively experienced less side effects or a longer duration of effect associated with one drug or the other – mention that too.
If you believe that Zubsolv is more effective than Suboxone or vice-versa, were you on an equivalent dose? Experiencing greater efficacy with one drug over the other may be a result of the specific dose you were taking. Understand that any perceived differences between the two drugs may be a result of: subjectivity, nocebo effects, and/or subtle variations in buprenorphine to naloxone ratios.