metastatic breast carcinoma from gastric cancermetastatic breast carcinoma from gastric cancer a...
TRANSCRIPT

J Korean Radiol Soc 1998; 38: 1139-1141
Metastatic Breast Carcinoma from Gastric Cancer A Case Reportl
Jeong Mi Park, M.D. , Jin Sook Kwon, M.D. , Gyungyub Gong, M.D. 2
We encountered a patient with a breast mass which had metastasized from gas tric carcinoma representing as an inf1ammatory carcinoma on ultrasonography We described the radiologic and clinical features , and review the literature . The patient had advanced gastric carcinoma and breast ultrasonography d emonstrated the presence of very ill-defined , infiltrating, and mixed echoic lesions indistinguishable from findings of primary inf1ammatory breast carcinoma. Metastatic gastric adenocarcinoma was confirmed pathologically .
Index words : Breast neop1asms, diagnosis Breast neoplasms , US Breast neoplasms , secondary
Metastatic breast 1esions are rare , comprising about 1. 2 to 6.6 % of all breast malignancies(l, 2). Although the incidence of breast metastasis from extramammary malignancies is not high , the etiology of the primary tumors is diverse. Excluding sarcomas and lymphom as, melanomas are the most common metastatic tumor.
The next most common tumor to metastasize to the breast is lung cancer, followed by cancers of the stomach , prostate , ovary or kidney; of other organs such as the cervix, thyroid, co1on, rectum, uterus or bladder; and intestinal carcinoid tumors(l - 3) A1though mammographic patterns have been quite frequently described in the literature(1 - 4), this is not-to our know1edge- the case with ultrasonographic findings . We report our recent experience of a patient with metastatic gastric carcinoma which showed the u1trasonographic features of inf1ammatory breast carClnoma
'Department 0 1' Diagnostic Radiology, Asan ι1ed ica l Ccntcr. Univcrsity 0 1' Ulsan Collegcof Mcdicine 'Dcpartment 0 1' Rathology , Asan Medical Ccnter, University 0 1' Ulsan Col lege 0 1'
Medicinc Reccivcd OCLObcr 29 , 1997; Acceptcd April1S , 1998 Addrcss rcprint requests to : Jeong Mi Park , M.D., Departmcnt 0 1" Diagnostic Radiology, University 0 1' Ulsan, Asan Mcdical Center, F 388-1 Poong Nap-Dong, Song Pa-Gu, Seoul 138 • 736, Korea Tcl. 82-2-224-4400 Fax.82-2-476-4719 E-mail : jmpark @www.amc.seou l.kr
Case Report
A 33-year-old woman was admitted due to stomach cancer diagnosed by gastrofiberscopic biopsy. Abdominal CT showed a mass in the lower body and whole antrum of the stomach , with multiple perigas tric lymphadenopathy, omental carcinomatosis and possible pancreatic invasion. Exploratory laparotomy revealed mesenteric seeding, asc ites and a rectal shel f,
thereby confirming the diagnosis of T4N3Ml Stage IV ad vanced gastric carcinoma. During chemotherapy ,
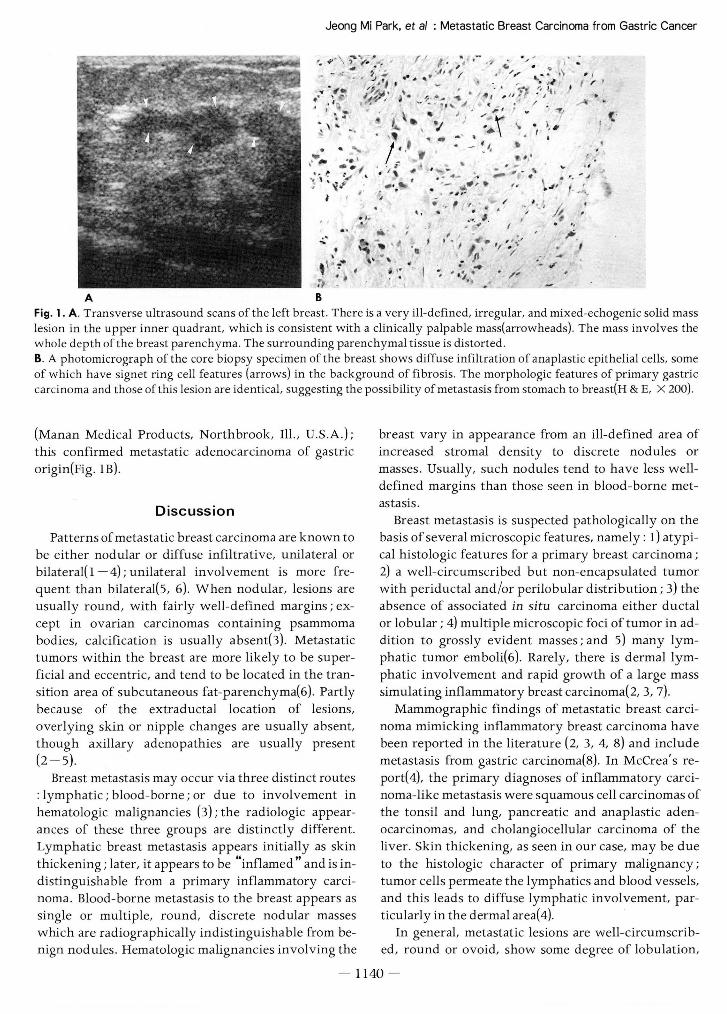
physical examination revea1ed bilateral breast masses ; Ultrasonography was performed with a 5 - 10 MHz linear-array transducer (UItramark 9-HDI, The Advanced Technology Lab. , BothelL W A, U.S. A.) and an ill-defined irregu1ar mixed echoic solid mass lesion was seen to occupy the whole upper inner quadrant of the left breast a finding consistent with a clinically palpable mass(Fig. lA). In this case, the mass invo1ved the whole depth of the breast parenchyma. Ad jacent parenchymal tissue was distorted and spiculation of the mass, indicating infiltration of subcutaneous fat tissue was also identified . The right breast showed no definite abnormality. Ul trasonographic diagnosis was primary breast carcinoma rather than metastatic carcinoma , and an ultrasound-guided core biopsy of the left breast was performed using an 18-gauge needl e
• 1139 -
Jeong Mi Park. et al : Metastatic Breast Carcinoma from Gastric Cancer
.,‘ i
”
’ ·’
‘
4
. ,
‘ ·
’
*
r J
J
r ‘. ·’
‘ ‘ il
/
-“ ,, ·‘,
?
「’
·
!
, f
‘ i
’
’
j·i
、
uhi
?? ’
‘ •
t
/
ι?
‘ ‘ --‘ ,
J
/
·
/
----
’t L ‘
‘·
ιν
)’
---J
?··
/ ·‘
/ ·i
’ ‘,
t
끼
t
.I
*r ‘
‘
κ .
4
‘ “ /
’
’
‘t
J
、
‘ ‘‘ -
t
J
‘
/
“ .. 7
‘ /
r , ·/ /
. ‘ / , t ‘
--t
r---
-
‘
/
•
’ ‘
--
---‘‘,1
ν
--*
;
‘? ?‘ (‘
‘ ‘·
I
,‘ ,
--
/
’ /
.
4
ir ” ‘
μ
i
·
‘ -
i
7, ? -ifJ
‘‘ ”
‘」// ’ * /J
i
·
‘
μ ‘
y
κ . // ··
샤
J’
‘
r 4 --
‘? ‘
‘
ιrψ
>
ι ”
? --‘V
μ、--h ‘
‘,
·,
,
‘ ‘
, . ‘
/
jt
?‘
-
-’
‘ |
’
-
‘
‘,i
/
·
U ‘
‘, ’ • ‘ ,
‘
‘
-, f
” ‘. ‘ ·l
” !
‘•
」/ ”
• ··‘
/ L ‘ /
r
A
애/L .. /
* , 1
u
ι ν
1
긴μ”?
’
, ‘~ ·
‘ •
* ·’ --?”
듀 -I
J’-‘
·/
‘ .
ι ?
i휴‘ ’
에4
ah
”¢i”-‘
‘ 、”--” ??
,
’ *·.ι,
·
/ -‘‘, .
‘、
, ‘ *
i
··’ 、‘
, ,. ‘ i·
‘
.‘‘
t.
‘
f‘‘
‘ ‘ ---‘
ν
‘ .--4 B
‘ ,
.‘‘ ‘
7.i
A Fig. 1. A . Transverse ultrasound scans ofthe left breast. There is a very ill-defined, irregular, and mixed-echogenic solid mass lesion in the upper inner quadrant, which is consistent with a clinically palpable mass(arrowheads). The mass involves the whole depth ofthe breast parenchyma. The surrounding parenchymal tissue is distorted B. A photomicrograph of the core biopsy specimen of the breast shows diffuse infiltration of anaplastic epithelial cells, some of which have signet ring cell features (arrows) in the background of fibrosis. The morphologic features of primary gastric carcinoma and those ofthis lesion are identica l, suggesting the possibility of metastasis from stomach to breast(H & E, X 200).
(Manan Medical Products, Northbrook, Ill., U.S.A .); this confirmed metastatic adenocarcinoma of gastric origin(Fig. lB)
Discussion
Patterns ofmetastatic breast carcinoma are known to be either nodular or diffuse infiltrative, unilateral or bilateral(1 - 4); unilateral involvement is more frequent than bilateral(5, 6). When nodular, lesions are usually round , with fairly well-defined margins; except in ovarian carcinomas containmg psammoma bodies, calcification is usually absent(3). Metastatic tumors within the breast are more likely to be superficial and eccentric, and tend to be located in the transition area of subcutaneous fat-parenchyma(6). partly because of the extraductal location of lesions,
overlying skin or nipple changes are usually absent,
though axillary adenopathies are usually present (2 - 5)
Breast metastasis may occur via three distinct routes : lymphatic; blood-borne ; or due to involvement in hematologic malignancies (3); the radiologic appearances of these three groups are distinctly different. Lymphatic breast metastasis appears initially as skin thickening; later, it appears to be “ inflamed" and is indistinguishable from a primary inflammatory carcinoma. Blood-borne metastasis to the breast appears as single or multiple, round , discrete nodular masses which are radiographically indistinguishable from benign nodules. Hematologic malignancies involving the
breast vary in appearance from an ill-defined area of increased stromal density to discrete nodules or masses. Usually, such nodules tend to have less welldefined margins than those seen in blood-borne metastasls.
Breast metastasis is suspected pathologically on the basis of several microscopic features , namely : 1) atypical histologic features for a primary breast carcinoma; 2) a well-circumscribed but non-encapsulated tumor with periductal and /or perilobular distribution; 3) the absence of associated in situ carcinoma either ductal or lobular ; 4) multiple microscopic foci of tumor in addition to grossly evident masses ; and 5) many lymphatic tumor emboli(6). Rarely, there is dermal lymphatic involvement and rapid growth of a large mass simulating inflammatory breast carcinoma(2, 3, 7)
Mammographic findings of metastatic breast carcinoma mimicking infIammatory breast carcinoma have been reported in the literature (2, 3, 4, 8) and include metastasis from gastric carcinoma(8). In McCrea' s re port( 4), the primary diagnoses of infIammatory carcinoma-like metastasis were squamous cell carcinomas of the tonsil and lung, pancreatic and anaplastic adenocarcinomas, and cholangiocellular carcinoma of the liver. Skin thickening, as seen in our case, may be due to the histologic character of primary malignancy; tumor cells permeate the lymphatics and blood vessels, and this leads to diffuse lymphatic involvement, particularl y in the dermal area( 4)
In general, metastatic lesions are well-circumscribed , round or ovoid, show some degree of lobulation,
- 1140 -
J Korean Radiol Soc 1998; 38: 1139-1141
and emit variable internal echoes ultrasonographcally (2). Derchi et al. (1) reported sonographic findings of metastatic breast tumors in eight patients. They in cluded solitary or multiple nodules, mostly round or oval in shape, and echo patterns were hypoechoic and solid. Multiple masses in the same patient had the same sonographic features. According to H에du(6), gastric carcinoma metastatic to the breast was multinodular ; this was different from our case, which showed diffuse ill-defined mixed echogenic masses mimicking inflam
matory carcinoma of the breast. Most patients experienced disease progression dur
ing pregnancy or (in males) during estrogen therapy,
and it thus appears that their hormonal status predisposed them to metastasis(8). Nearly one quarter of metastatic breast carcinomas are the presenting manifestation of an otherwise occult malignant disease
elsewhere in the body (1, 6). Breast metastasis is usually indicative of diffuse metastatic disease and indicates poor prognosis(2, 4, 8); the recognition of such metastasis can eliminate unnecessary procedures
such as radical surgery, thus resulting in more appro priate patient management(7) .
In the differential diagnosis of breast lesions in
patients with known extramammary malignancies, in
cluding those with radiologic features suggesting pri mary inflammatory breast carcinoma, metastatic disease should therefore be considered.
References
1. Derchi LE, Rizzatto G, Giugeppetti GM, Dini G, Garaventa A Metastatic tumors in the breast ‘ sonographic findings. J
Ultrasound Med 1985; 4: 69-74
2. Yamasaki H, Saw D, Zdanowitz J, Faltz LL. Ovarian carcinoma metastasis to the breast case report and review of the literature Am J Surg Pathol 1993; 17(2): 193-197
3. Paulus DD, Libshitz HI. Metastasis to the breast. Radiol Clin
North Am 1982;20:561-568
4. McCrea ES , Johnston C. Haney PJ. Metastases to the breast AJR 1983; 141 : 685-690
5. Bohman LG , Bassett LW , Gold RH, Voet R. Breast metastases from extramammary malignancies. Radiology 1982; 144: 309-312
6. Hajdu SI, Urban JA. Cancers metastatic to the breast. Cancer
1972; 29: 1691-1696
7. Ward R, Conner G, Delprado W, Dalley D. Metastatic adenocarcinoma of the cervix presenting as an in f1ammatory breast lesion. Gynecol Oncol 1989; 35 : 399-405
8. Nance FC, MacVaugh III H, Fitts W. Metastatic tumor to the breast simulating bilateral primary in f1ammatory carcinoma Am J Surg 1966; 112: 932-935
대한밤시선의학회지 1998; 38: 1139-1141
위암에서 전이된 유방암 : 증례보고1
l 울산대 학교 의 과대 학 진단방사선과학교실 2울산대학교 의과대학 병리과학교실
박 정 미 · 권 진 숙 · 공 경 엽 2
저자들은 최근 유방 초음파 소견상 염증성 유방암과 구분이 되지 않는 소견을 보인 위암에서 전이된 유방암을
경험하였으므로 문헌 고찰과 함께 보고한다. 병변은 유방 초음파 소견상 염증성 유방암의 소견과 유사한 경계가
좋지 않은혼합에코의 종괴로보였으며 생겸으로확진되었다.
- 1141 -
국제 학술대회 일정표[ II ]
•• 16th World Congress on Endo-Urology & Extracoporeal Shock Wave Lithotripsy (1998/10/00-00)
venue: Antwεrp, Belgium. contact: D r. A.D. Smith, Long Island Jewish Med . Ct,
27005 76th Avenue, New Hyde Park Long Island, NY 11042, USA (tel: 1-718-4707221 /5; fax: 1- 718-3438254)
• 23rd Annual San Diego Postgraduate Radiology Review Course (1998/10/00-00)
venue: Hotel Del Coronado San diego , CA, USA. contact: ryals & Ass. , Inι, P.O. Box 1925,
Roswell, GA 30077-1925, USA (tel: 1 -770 여19773 ; fax: 1 -770 - 5529859)
• 18th Annual Comprehensive Review of Vascular and Interventional Radiology (1998/10/00 -00)
venue: Hotel Del Coronado San diego, CA, USA contact: ryals & Ass. , Inc. , P.O. Box 1925,
Roswell , GA 30077-1925, USA (tel: 1 -770 - 6419773; fax: 1 -770 - 5529859)
• 11th Annual Meeting European Society of Head and Neck Radiology(Eshnr) (1998/10/01-03)
venue: General Hospital Vienna, Austria contact: Helga Fischer, AKH-University of Vienna,
Waehringer Guertel 18-20, A-I090 Vienna, austria (tel: 43 - 1 - 404005801 ; fax: 43 - 1 -404003777)
• Musculoskeletal MR (1998/10/05 -08) venue ‘ The Ritz-Carlton Hotel Naples, FL, USA contact: Ryals & Ass. , Inc. , P.O. Box 1925,
Roswell , GA 30077-1925, USA (tel: 1 -770 -6419773; fax ‘ 1 - 770 - 5529859)
• 4th International Symposium on Cardiovascular & Interventional Radiology (1998/10/05 -09)
venue: Hyatt Regency Cambridge, κ1A, USA. contact: Candace Cutler, CME Mngr., Brigham & Women ’s
Hosp. , 75 Francis Street, Boston, MA 02115, USA (tel: 1-617-7326265; fax: 1-617-7326509)
• TCT X (Transcatheter Cardiovascular Therapeutics) (1998/10/07 -11)
venue ’ Washington, DC, USA contact: Karl R. Katterjohn, Cardiology Research Fdn. ,
110 Irving Street, NW, Suite 4B-I , Washington, DC 20010, USA (tel : 1 - 202 - 8778124; fax: 1 - 202 - 8773339)
• 5th Annual Meeting European Society of Musculoskeletal Radiology (1998/10/09-10)
venue: Ljubljana , Slovenia contact: Prof. D r. V. Jevtic, Radiology Institute,
Zaloska 2, SI-1525 Ljubljana, Slovenia (tel:386-61-325570; fax:386-61 - 1331044)
1142
• 49th Annual Session of the American Academy of Oral & Maxillofacial Radiology (1998/10/14-18)
venue: Fort Marcy Condominiums Santa Fe, Nκ1 , USA contact: Dr. M. Kevin 0 Carroll, Executive Secretary,
P.O. Box 55722, Jackson , MS 39296, USA (tel: 1-6이 -9846060; fax: 1 -601 -9846086)
• 8th Radiological Symposium Graz: Prof. Erich Vogler Symposium (1998/10/15-17)
venue: Graz. Austria contact: B. Tieber, Dep t. of Radiology,
Auenbruggerplatz 9, A-8036 Graz, Austria (tel: 43 - 316 - 3853850; fax :43 - 316 - 3853848)
• 49th Annual Gen . & SC. Meeting Royal Australasian College of Radiologists (1998/10/15-19)
venue: Brisbane Convention Ctr ‘ Brisbane, Queεnsland , Aus tralia
contact: Dr. David Lisle, Qld Med. , 4th fl. , Morris Towers, 149 wickham Terrace, Brisbane, Qld 4000, australia (tel:61-7-38314527 ; fax:61 - 7-38397041)
• 30th Annual Meeting of the Western Neuroradiological society (1998/10/16-18)
venue: El Dorado Hotel , USA contact: M r. tim Moses, 2210 Midwest Road ,
Suite 207 , Oak Brook , Il 60521 , USA (tel: 1 -630- 5740220 ; fax: 1 - 630- 5740661)
• MT. Sinai 1998 Body Imaging Update (1998/10/17 - 20)
venue The Plaza Hotel New Y ork, NY, USA contact: Ryals & Ass ., Inc. , P.O. Box 1925,
Roswell , GA 30077-1925, USA (tel: 1 -770 -6419773; fax: 1 -770- 5529859)
• CME Course : MRI/CT Update (1998/10/19-23) venue: Hyatt Regency Cambridge, MA, USA contact: Candace Cutler, CME Mngr., Brigham and Women’s
Hosp. , 75 Francis Street, Boston, MA 02115, USA ‘
(tel: 1 - 617 -7326265; fax: 1 -617 -7326509)
• MT Sinai 1998 Brain Spine, Neurovascular and Ent Imaging Update (1998/10/21 -25)
venue: The Plaza Hotel New York. NY. USA contact: Ryals & Ass. , Inc. , P.O. Box 1925,
roswell, GA 30077-1925, USA (tel: 1 -770 - 6419773; fax: 1 -770 - 5529859)
• 5th Congress of the Asian Fed. of Soc. for Ultras。und in Medicine & Biology (1998/10/23-27)
venue: Taipei Int. Conv. Center Taipeh, Taiwan, R.O.C contact: Taiwan Society of, Ultrasound in Medicine,
No. 1, Chang-Te Street, Taipeh , Taiwan , R.O.C ‘
(tel: 886-2 - 3816933 ; fax: 886 -2 - 3816939)
제공 : 대한방사선의학회 국제협력위원회
O' t 1 효| 흩
학회활동
口 저17 차 상임이사회 개최 주요내용(5월 13일)
*보고사항
1. 4월 중공문접수 20건, 발송 36건 처리
2 . 제증명 발급 55건
3 . 엄태환(울산의대) 통신 클라인 비참 학술상
이도연(연세의대) 유한학술상본상을수상함.
4. 다음의 숙제보고는 추계학회에서 결과 보고가 가능할
것임-(1) 오용호(울산의대) 진단방사선과 전임의 실태파
악과 문제점 노출에 따른 수련 개선방향에 대한
연구
(2) 김기황(연세의대) -진단방사선과 교육과정 개선
에관한연구
(3) 박영근(영등포방사선과의원) -개원의 현황과 문
제점
5. 각종회의 개최
(1) 제6차 싱-임이사회 개최(1998년 4월 1일)
(2) CT의료보험 인정기준 재검토에 대한 회의(1998
년 4월 8일)
(3) 전문의시험 2차시험 Pretest 시험장 사전답사
(1998년 5월 2일 )
(4) 학술 위원회 회의 개최 (1998년 5월 7일)
6. 4월 학회 수지 내역
수 입 J 지 출 58,648,000 I 73,033,982
7. 한국과학기술단체총연합회 지원금이 770만원 배정되
었음.
8. 춘계학술대회 결과보고(5월호 참조)
9. CT인정기준 재검토 안을 마련하여 보건복지부 및 대
한의사협회에 건의문 발송하였음.
10. 컴퓨터 적외선 체열촬영 (DITI)이 의료보험 비급여
10/15 08 : 00 - 08 : 30 Pathology of the Lymphoma
대상으로확정되었음.
11. 초음파 골밀도 검사가 보험급여 대상으로 확정되였음
(피부두께 측정에 대한 골량변화 판정은 제외)
12. 춘계 전공의 연수교육 결과보고(5월호 참조)
13. 4년차 전공의를 대상으로 전문의시험 2차시험 전산화
의 Pretest 시험장 사전답사 및 장소 계약을 하고 사
용료는 1,600,000원으로 합의 하였음.
*토의사항
1. 추계학회의 P lenary Lecture 연사 선정은 이용태 삼
보컴퓨터 회장을 섭외하기로 하고 만약 여의치 않을
경우회장단에 일임하기로함.
2 . 추계학회의 등록비 빛 교재비 인상에 관하여는 등록비
는 예년과 동일하게 하며 Categorical Course의 교재
비는 사전등록시 2,000원에셔 5,000원으로, 현장등록
시 3,000원에서 7,000원으로 인상하기로 함.
3 . 추계학회에서 숙제보고 발표시간은 Categorical Cour
se 시간에 다른 강의실을 배정하여 연제당 약 20분간
발표하기로함.
4. 회원 주소록을 7월호 학회지 뒤쪽에 삽입하여 게재하
기로함.
5. 학회 감사를회계부문만중점적으로해왔으나업무부
분도적극하기로함.
6. 응급방사선과학을 학회 차원에서 지 원 육성하기로 함.
7 . 환자의 안전과 의 사의 Legal Protection을 위 해 진단
방사선과에서의 절차, 진행, 처리 등의 지침서를 대한
방사선의학회에서 발간하기로 하고 차기 회기의 예산
에 반영하기로함.
8. 의료사안의 문건이 계속증가추세고문안작성의 기술
적인 문제 또한중요하다고판단되어 학회의 의료사안
심의위원을 포함한 희망하는 회원과 변호사나 검사가
참여한 워크삽을 개최하기로 하고 실무진에 안을 만들
기로함.
9. 추계학회 기간동안 개최되는 제 20 차 전문의 연수교육
프로그램에 관하여 아래와 같이 결정함.
김 철 우 (서 울의 대)
08: 30-09: 00 Lymphoma of CNS and Head & Neck 한 문 희 (서 울의 대)
09: 00 • 09 : 30 간접촬영필름판독 진 수 일 (원자력병원)
10/ 16 08 : 00 - 08 : 30 Lymphoma of Thorax 겨。 수 (성균관의대)
08: 30-09 : 00 Lymphoma of Musculoskeletal System 서 진 석 (연 세 의 대)
09: 00 - 09 : 30 흉부X선 정도관리 임 정 기 (서 울의 대)
10/17 08: 00 - 08 : 30 Lymphoma of GI Tract and the Abdominal Solid Organ 하 현 권 (울산의 대)
08: 30 - 09: 00 Lymphoma of GU System 고 병 희 (한 양의 대)
11 43 -
학술활동
口 ’98년도 진단방사선과 전공의 평가고사 시행
가. 일 시 1998년 5월 16일(토) 13: 00- 16 : 00 나. 장 소:전국 7개 지역 동시 시행
다.주 최 :대한방사선의학회
라. 참가현황 : 765명중 746명 참가(97.5 %)
口 ’98년도 신입전공의 오리엔테이션 개최
가. 일 시 : 1998년 5월 23일(토) 10: 00 -16 : 20 나. 장 소 연세의대 동문회관지하연극관
다. 주 최 . 대한방사선의학회
라. 후 원 :한국쉐링 , 일성신약, 삼성지야의료기기 , 지
멘스제네럴메디칼, 신기사, 동강무역
마. 등 록 : 200병 대상중 172명 참석 (86%)
바. 내 용 : 대한방사선의학회의 어제와 오늘, 대한방사
션의학회의 선구자분들, 전공의 수련과정 소
개, 학술대회 및 전공의의 학술활동, 논문작
성법, 진단방사선과와 임상과의 관계, 원로
선생념과의 대화, 선배와의 대화 등 다채로
운행사로진행
회원동정
김건상(중앙의대) : 대한병원협회 표준화 수련이사에 임명
되었음.
김홍대(서울의대) : 지난 5월 15일부터 21일까지 미국 필라
델피아에서 개최된 제 16 차 국제신경방사선과학회에서
『해마경화증의 자기공명분광볍 』으로 젊은 의학자 장학상
을받았다.
박용후I (삼성제일병원) : 6월 7일부터 24일까지 캐나다 토
론토에서 개최되는 북미핵의학회 학술대회에 논문 발표차
출국예정이며 이번 학회 기간동안 세계적인 핵의학자들과
만나 가칭 분자핵의학 집필진 구성을 위한 모임도 가질 예
정이다.
이승익, 류창우(포천중문의대 분당차병원) : 지난 5월 15일
부터 21일까지 미국 필라델피아에서 개최된 제 16 차 국제
신경방사선학회에 장학상과 우수상을 받았다.4년마다 개
최되는 이 대회에 총 3백 52편의 논문과 포스터가 제출되
었으며 우리 나라에서도 15편이 제출되었는데 이승익 (R4)
회원은 『쉬멸씨 결절의 자기공명영상 소견과 조영증강에
미치는 인자』로, 류창우(R2)회원은 『자기공명영상에서 자
발성 두개내 저혈압과 두부외상후 경수막 조영증강의 비
교』로 각각 상을 받았다.
천경아(가톨릭의대 ) : 지난 4월 26일부터 5월 l일까지 미국
센프란시스코에서 개최된 제 98 차 미국방사션의학회 학술
대 회 에 서 발표한 WMR lmaging Evaluation of Thoracol -
umbar Fractures ~가 Certificate of Merit상을 받았다.
최 병인(서울의대) : 6월 6일부터 8일까지 중국 북경에서 개
최된 제 7차 아시아 오세아니아 방사선과학 세미나에 초청
되어 『간암 발생기전의 영상진단~ , W미만성 간질환의 영상
진단』 및 『담도춰1장의 나선식 CT~에 대한 강연을 하였다.
口 승 진
최병언(서울의대) : 6월 10일자로교육연구부장으로송진
口 회원이동사항
고병구:울산한길내과의원
김영범 :국군 대전지구병원
김재승:서울중앙병원 핵의학과
검철중:고려의대 구로병원
김홍인:음성군보건지소
노주철:서울시그마병원
박지영.늘푸른병원
박찬구 대전중앙병원
안범규 아산현대의원
양동헌 .가톨릭의대 대전성모병원
이남석.당진성모내과병원
이태우.청도대남병원
장종운 : 칠곡군 지천보건지소
정두영 창녕군보건지소
정진용:서광주병원
정현웅:하남성심병원
조현철 : 군위 산성면 보건지소
최은완:서안복음병원
口 개 원
문웅재 : 전낭 여수시 여서동 490.s번지에 문웅재방사선과
의원을 개원. 전화 ( 0662) 652 -0088 박달수 : 대전광역시 대먹구 신탄진동 118-25번지에 을지
방사선과의원을 개원. 전화 (042) 935-5829 이상현 :충남 당진군 당진읍 읍내려 524 원빌딩 2층에 당 진진단방사선과의원을 개원. 전화 (0457) 357θ257
口 닙 。T "6"
김명진(연세의대) : 6월 4일 모친상
공지사항안내
口 E-mail을 통한 공지사항 안내
대한방사사션의학회에서는 정보화 시대에 부응하여 신
속하고 정확한 정보를 회원들에게 전달하고 우편료 등 비
용 절감의 일환으로 1999년 l월 1일부터 전 수련병원급에
서 근무하는 모든 회 원과 E-mai l 주소를 가진 회 원 중 희
11 44 -
망하는회원은학회에서 발송되는모든공지사항과공문은
전자우편 (E-mail)으로만 공지하도록 지난 4월 정기 이사
회에서 결의 하였습니다. 이점 업무에 참고하시기 바랍니
다.
口 E-mail address를 학회로 알려 주세요.
학회 Internet 구축과 활성화의 일환으로 회원 여러분의
E-mail 주소를 모으고 있습니다.
ID가 여 렷 있으신 분들은 자주 이 용하는 것을 알려 주시
고, 학회 Home Page에 가입 하여 받으신 E -mail 주소 즉
Medidas를 。1 용하여 E-mail을 사용하시는 회원도 반드시
관리자에게 알려 주시기 바랍니다. E -mail 주소를 통보해
주신 회원들께서는 학회 흠페이지 내용 변경시, 혹은 학회
에 새소식이 있을 때 E-mail로 신속하게 알려 드리겠습니
다. 일종의 Semi-push Technique이 오니 많은 협 조를 바랍
니다.
보내실 곳 : E-mail : kkrs @chollian.net
Fax : (02)529-7113
주소변경 회원에게알림
口 학회소식자료수집
회원 여러분의 건승하심을 진심으로 기원합니다
본 학회에서는 매월 발행하고 있는 대한방사선의학회지
의 “학회소식”란에 게재할 자료를 수집하고 있으니 아래
사항을 참조하시어 많은 연락 있으시길 바랍니다.
게재 내용 : 지회소식, 회원동정 (승진 및 임용, 개원, 경조
사,건의사항등)
제출기한:수시
제 출 방법 -학회 사무국 FAX 529-7113
口 구인및구직안내
전문의 구인 및 구직에 대한 광고를 원하시는 분은 본 학
회로 연락하여 주시기 바랍니다.
口 저서 납본안내
회원께서 쓰신 주옥같은 글의 각종 도서나, 소장하고 계
신 그 어떤 자료라도 학회에 기증하여 주시면 소중히 보관
하여 유용하게 활용할 수 있도록 최선을 다하겠습니다.
대한방사선의학회 지를 수취하시던 주소가 변경된 회원은 아래와 같은 내용을 적어 본 학회 사무국으로 우송하여 주시
기 바랍니다.
성 n。킥 | 전문의번호 | 전 근 무 처
근무처명 근무기간
-;z「; λi、-
」 근 무 처
근무처병 j 전화 | -ζ「 -까.l..、-
보내실콧 : 137 - 130 서울시 서초구 양재동 121-8 대한방사선의학회
전화 : 578-8003, 8005 FAX: 529-7113
E-mail: [email protected]
쉰터 원고모집 안내
- 19
| 근무개시일 I 19
| 우편번호 |
쉽터의 원고는 방사션의학 또는 영상과 관계가 있는 사진 또는 그럼으로서 독자들에게 흥미를 줄 수
있는 내용이어야합니다.
한쪽 단위가 되어야 하며 두쪽 이상인 경우는 독럽적으로 가치가 있어야 하고, 게재 여부는 대한방사
선의학회 편집위원회 에서 결정하며 게재료는 학회에서 부담합니다.
1145 -
대한방사선의학회지 투고규정
1998. 1. 1. 개 정
1.원고의 성격 및 종휴
의학적 진단과 치료에 공헌할 수 있는 방사선과학 영상과
관련된 독창성 있는 원고이 어야 하며 원고의 종류는 원저 ,
종설, 증예보고, 임상화보(pi ctorial essay) , 편집인의 글, 편
집인에게 보내는 글과 답 등으로 한다. 제출된 원고와 동일
또는 유사한 원고를 타 학술지에 게재할 수 없으며, 중복출
간(multiple or du plicate publication )은 Uniform R equ
irement s for Manuscri pts Submi tted to Biomedical
Journals (Ann Intern M ed 1997 : 126 : 36-47)에서 규정한
요건을 갖춘 경우에만 가능하다.
2 . 사용언어 한글 또는 영문으로 작성하고 의학용어의 번역은 1997년
대한방사선의학회에서 발간한 의학용어집과 대한방사선의
학회 홈페이지에 수록된 의학용어집에 준하며, 이외의 용어
는 1992년 대한의사협회 발간 의학용어집에 준한다. 한글
원고의 경우 한자를 병용할 수 있으며 , 적절한 번역어가 없
는의학용어, 고유명사, 약품명,단위 등은 원어를그대로사
용한다. 번역어가 있으나 의미전달이 명확하지 않은 경우에
는 그 용어가 최초로 등장할 때 번역어 다음에 소괄호 속에
원어로 표기하고 그 이후로는 번역어만 사용한다. 영문약어
는 최소화하며 최초 사용시 원어를 풀어서 표기한 다음 괄
호안에 약어를쓴다.
3. 원고의 저|훌 원고 및 사진을 각각 2부썩 작성 하여 1부는 다음의 주소
로 제출하고 l부는 저자가 보관한다.
대한방사선의학회
137 -130 서울시 서초구 양재동 121 -8번지
전화 : 578 -8003, 8005, 팩스 : 529-7113,
전자주소 : kkrs @chollian.net
4. 원고의 심으ICPeer Review) 투고된 모든 원고는 게재 적합성에 대하여 2인(심사위원
1인, 편집위원 l인) 이상의 해당분야 전문가에게 심의 ( Peer
Review)을 요청하고, 그 결과에 근거하여 원고 채택 여부를
결정하며 , 저자에게 수정 및 보완사항을 권고한다.
5. 원저 작성에 있어서 일반적 참고사항 1) 초 록 -한글과 영문으로 각각 페이지를 달리하여 작성하 며 한글은 600-^} 이내 , 영문은 200단어 이내로 한다. 연구
의 목적 , 대상 및 방법, 결과, 그리고 결론을 간단 명료하
게 각각한문단으로기술하고구체적 데이터를제시한다.
2) 서 론 연구의 목적을 간결하고, 명료하게 제시하며 배경
에 관한기술은목적과연관이 있는 내용만을포함한다.
3) 대상 및 방법 : 연구의 계획, 대상 빛 방법을 순서대로 기 술한다. 대상환자의 진단이 어떻게 확인되었으며 , 어떻게
관찰되었는지를 상세히 기록한다. 실험방법이 주안점인
경우 재현 가능하도록 구체적으로 기술한다.
4) 결 과 : 연구결과를 명료하고 논리적으로 나열하고, 실험
인 경우 실측치에 변동이 많은 생물학적 계측에서는 통
계처리를 원칙드로 한다. 표(Table)를 사용할 경우 논문
에 표의 내용을 중복 기술하지는 않으나, 중요한 경향 및
요점을기술한다.
5) 고 찰 : 연구의 결과에 대한 고찰 빛 이 에 연관된 다른 자
료와 연관 해석한다. 새롭고 중요한 관찰을 강조하며, 결
과의 내용을 중복 기솔하지 않는다 관찰된 소견의 의미
및 제약을 기솔하며, 연구결과의 내용이 허용하는 범위
내에서 결론과 연구의 목적을 연관시킨다. 마지막 문단에
결과의 요약 및 결론을 기술한다.
6. 저자 점검사항 Cchecklist) 원고는 다음의 점검사항을 확인하고 저작권에 관한 동의
서 및 공저자 확인 양식에 소정 사항을 기록하고 최종 점검표
와 함께 제출한다. [ (@" 1l04Page 참조) 복사하여 사용할
것]
1) 일반적 사항 • 원고는 다음과 같은 순서로 한다. 표지 , 내표지 (제목만 포 함) , 초록, 서론, 대상 빛 방법 , 결과, 고찰, 감사의 글(ac
knowledgments) , 참고문헌, 표(Table) , 사진설명, 사진.
• 원고는 A4 (21 x30cm)용지에 행간 1행의 여백, 좌단 및
상하에 3cm의 여백을 둔다.
· 모든 원고는 초록부터 순서대로 쪽수를 기록하고, 초록
이후의 원고 안에는 저자의 성명이나 소속을 기록하지
않는다.
· 영문약어는 최소화하며 이를 사용할시에는최초에 풀어
쓴후괄호안에 약어를기업한다.
· 기 계 및 약품의 경우 괄호 안에 제조회사, 도시 및 국적
을기업한다.
• 참고문헌을 인용할 때에는 저자병 뒤 또는 문장 끝에 문 헌 변호를괄호안에 표기한다.
• 채택 후 최종원고를 제출할 때 3.5인치 디스켓에 파일명, 프로그램명과 함께 프린트 된 원고1부를 함께 제출한다.
2) 표지
· 표지에는 다음의 사항을 기록한다. 논문의 제목과 전 저
자의 성 명 과 소속을 한글과 영 문으로 표기 한다. 소속이
다른 저자들이 포함된 경우에는 연구가 주로 이루어진
기관을 먼저 기록하고 그 이외의 기관은 해당저자 이름
에 2번부터 어깨번호를 하고 소속기관을 번호 순으로 표
기한다. 표지하단에 통신저자(corresponding author)의
주소, 전화, FAX 번호 및 E -mail 주소를 영문으로 기록
하고, 연구비 수혜 사항을 필요한 경우 기술한다.
·내표지에는 원고의 제목만을 한글과 영문으로 기술한다.
저자의 이륨,소속등은일체 포함시키지 않는다.
3) 초록
• 한글원고의 경우 한글초록을 제 1쪽, 영문초록은 제 2쪽
으로 하며, 영문원고의 경우에는 순서를 반대로 한다.
• 다음과 같이 각 항을 분리하여 기술한다.
목 적 ( Purpose) 왜 본 연구를 수행하였으며 달성하고자
하는목적이 무엇인지를 1 - 2 문장으로간단하고도명료
하게 기술한다. 여기에 기록된 목적은 원고의 제목그리
고 서론에 개진되는 내용과 일치되는 것이어야 한다.
대상 및 방법 ( Materi a l s a n d Methods) 첫 문단에 기술
된 목적을 달성하기 위하여 무엇을 어떻게 하였는가를
구체적으로 기술한다. 어떤 데이터를 수집하였으며, 이
데이터를 어떻게 분석하였고, 비틀림 (bias)을 어떻게 조
정하였는가를 기술한다.
결 과( Results) 전 문단에서 기술된 방법으로 관찰 및
분석한 결과가 어떠하였다는 내용을 논리적으로 기술하
며 구체적 데이터를제시한다.
걸 론(Con clus i on ) 본 연구의 결과로부터 도달된 결론
- 11 46 -
을 1 • 2 문장으로 기숭하며, 이는 첫 문단에 기술된 연구 의 목적에 부합된 것이어야한다.
• 약어 사용이 나 참고문헌 인용은 할 수 없다.
·영문초록의 하단에 대한방사선의학회 발행 색인집 (Rad
iology의 색인집과 동일)에서 등재된 색인단어를 5개 이
내 선택하여 기입한다.
4) 참고문헌 ·새 쪽(페이지)에 본문에서 인용된 순서대로 아라비아숫
자 번호와 함께 기록한다.
• 기록된 모든 참고문헌은 본문에서 반드시 인용되어야 한
다.
·출판되지 않은 데이터는 참고문헌에 기숭될 수 없으며
부득이 인용하고자 하는 경우 본문에 괄호하고 “(홍길
동, 개인적 의견교환)" 혹은 “(홍길동, 미출간 데이터)"
와같이 기술한다.
• 학술지명의 표기는 Index Medicus의 공인 약어를 사용
한다.
- 6인 이하의 저자인 경우는 전원을 기록하며, 7인 이상인
경 우는 최초 3언 이 후에 “등” 빛 “et a1."로 끝맺는다.
·저자명은 한국인은 성과 이름, 외국인은 성 뒤에 이름의
첫 자를대문자로쓴다.
• 인용문헌의 쪽은 시작과 끝을 기록한다.
• 참고문헌의 숫자는 원저 는 40개 이 하, 증예 보고는 1Q7B 이하로한다.
• 기술양식은 다음의 예와 같이 한다.
정기학술지의 논문
1. 검장호, 김성우, 윤정경, 김병영, 이일기, 이종길 반측안
면경련 환자에서 자기공명혈관조영숲의 원천 영양의
진단척 유용성 . 대한방샤션의 학회 ;x. l 1997; 37 ; 25-28
2. Kim M -J, Chung J -J , Lee YH, Lee JT, Yoo HS.
Comparison of the use of the transrectal surface coil
and the pelvic phased -array coil in MR imaging for
preoperati ve evaluation of uterine cervical carci
noma. AJR 1997; 168 ; 1215-1 221
단행본
3. Kang HS, .Resnick D. MRI of the extremities: an
anatomic a t1as. Philadelphia : Saunders, 1991 : 62-79
단행본내의 chapter
4. Choi B I. Comparison of different imaging techni
ques. In Livraghi T , Makuuchi M , Buscarini L. Di
agnosis and treatment of hepatocellular carcinoma.
London: Greenwich Medical Media, 1997: 201-219
5) 표(Table)
·표는 영운과 아라비아숫자로 기록하며 표의 제목을 명료
하게 절 혹은구의 형태로기술한다.병사와행용사는첫
자를대문자로한다.
·분량은 4줄이상의 데이터를포함하며 l쪽을넘지 않는다.
• 본문에서 인용되는 순서대로 변호를 붙인다.
·약어 사용시 해당표의 하단에 풀어서 설영한다.
·기호 사용시 " T , T , ~, 11 , 매 十 T , 千수의 순으로
하며 이를 하단 각주에 설명한다.
· 표의 내용은 이해하기 쉬워야 하며, 독자적 기능을 할 수
있어야한다.
• 이 미 출간된 논문의 표와 동일한 것은 사용할 수 없다.
6) 사진 (Figure)
• 별도의 봉투에 넣어서 제출한다.
• 사진의 크기는 5x7인치 (13x18cm)로 통일하며, 광택
인화지를사용한다.
·사진 뒷면에 사진의 번호와 상하표시를 연필로 기업한
다. 세게 눌러써서 전면에 표시가 나지 않도록 하며, 잉크
나볼펜사용을금한다.
·통일번호에서 2개 이상의 사진인 경우, 아라비아숫자 이
후에 알파뱃 글자를 기업하여 표시한다(예 : Fig. lA, Fig.
1B).
·같은 사진 번호 안에 서로 다른 환자의 사진을 원칙적으
로포함시키지 않는다.
·화살표나 문자를 사진에 표시할 펼요가 있는 경우 이의
제거가 가능하도록 인화된 사진에 직접 붙인다.
·그럼(Jine drawing)의 경우 흰 바탕에 검은 션을 사용하
며 인화된 사진으로 제출한다.
·이미 출판된 사진을 인용할 경우 원저자의 서면 동의를
얻어야하다.
·사진 뒷면에 저자명을 기록하지 않는다.
·사진 배열에 관한 저자의 의견을 필요한 경우 기업할 수
있다
7) 사진 설명 • 본문의 인용된 순으로 아라비 아숫자로 번호를 붙인다.
·별지에 영문으로 구나 절이 아난 문장의 형태로 기술한
다.
·현미경 사진의 경우배율을기록한다.
@원저 이외의 원고@
일반적사항및 점검사항은원저에 준한다.
1.종설
종셜은 특정 제목에 초점을 맞춘 고찰로서 편집위원회에서
위촉하여 게재한다.
‘ 2. 증례보고 초 록 : 영문초록은 150단어 이내, 한글초록은 400 ;x.} 이내로
한 개의 문단으로 하며 서론, 대상 및 방법, 결과, 결론항을
분리하지 않는다.
서 론:서론이라는제목없이 증예와연관된 일반적 배경 빛
의의를 간략하게 기술한다.
증예보고 · 임상소견은 영상진단에 직접 관계 있는 사항만
국한하여 기술한다.
고 찰 : 증예가 강조하고 있는 특성부분에 초점을 맞추며 장
황한문헌고찰은피한다.
참고문헌 : 1Q7B 이내로 한다. 3. 입상화보
임상화보는 사진과 이의 설명을 통하여 내용을 전달하는 것
으로, 이는 독창적 원저와 달리 사진을 통한 교육에 그 주목
적이 있으며, 학숭대회장에서의 학숭전시와 같은 성격을 갖
는다. 이의 형식은 초록, 서론, 원저의 결과와 고찰에 해당하
는 간략한 서술, 참고문헌, 사진설명의 순으로 하며 참고문
헌은 10개 이내, 사진의 숫자는 307B 이내로 한다. 감사의 금
은포함될 수없다.
4. 편집인에게 보내는 글
학회지에 출판된 특정 논문에 대한 건설적인 비평 또는 의
견, 혹은 방사선과 의사의 일반적 관심사항이나 학술분야
특정주제에 관한 개인척 의견을 서술할 수 있다.
낀
1 , i
1 , ‘
gordon instruments, inc.
Imaging Tools for Medical Education Lect:μresJ PresentationsJ αηd ConfereηcesAre Easy
VersαtileJ andJ Most ImportaηtlYJ 핸ectiνe
Gordon’s product line provides a range of solutions to meet every need and to fit every budget. For multimedia presentations and interdisciplinary conferences, the Video Lectern is the perfect too l. rf your video needs are less de-mancling, our TeleMαte offers the same image quality as the Lectern , but with aclclitional output options. For the traclitional slicle presentation, the Likoη Pro copystancl makes quick work of con-verting yo니 r transparencies to slides. Designecl with the meclical eclucator in mind, all of our presentation systems, inclucling the Model 81η Custom-Optic overheacl projector, can accommoclate full 14"-by-17" fi lms and provicle the necessary illumination to keep your images crisp ancl clear. The H쟁hlight HQII is an intense light source for viewing small detai!s in very clense films. For more info rmation, please contact us at
저 L..!
A1 o 뭄 』
산 서울 특별시 강동구 암사동 514 -38 전 화 : ( 02 ) 3427 - 66 1 1 FA X : (02) 3427 - 66 10
Likon Pro Cφystaηd
Model 81n c:μstom-Optic
Overhe,ιld Projector
Highlight HQII Desktop Illumiηator