metabolism of potassium and its clinical significance
TRANSCRIPT

Metabolism of Potassium and its clinical significance
Dr. Rohini C Sane



Dietary sources of potassium
• Oranges
• Bananas
• Pine apple
• Potato
• Tender coconut
• Fresh vegetables
• chicken
• liver
Average diet provides 4 gm of potassium /day

Functions of Potassium (K⁺ ) in human body
Functions of Potassium (K⁺ ) in human body
1. Major intracellular cation
2. Extracellular K⁺ influences skeletal & muscle activities (including cardiac muscles)
3. Transmission of nerve impulse
4. Acid base balance
5. Water & electrolyte balance
6. Intracellular potassium concentration is necessary for protein biosynthesis by ribosomes
Metabolism of Potassium➢Normal serum Potassium levels : 3.5 -5.5 mequ/L
➢Daily dietary requirement : 3-4 gm /day
➢Absorption in gastrointestinal tact -90 % -efficient
➢The whole blood contains much higher levels of potassium. (50 mequ/L ).
➢Since potassium is predominantly intracellular cation, care should be taken to prevent hemolysis of RBC to avoid erroneous high levels of serum potassium.(preanalytical error)

Homoeostasis of Potassium
❖Potassium balance or Homoeostasis is maintained by :
1. Homoeostasis of Potassium by Transcellular movement
2. Role of gastrointestinal tract in Homoeostasis of Potassium
3. Role of Kidney in Homoeostasis of Potassium

Homoeostasis of Potassium by Transcellular movement ❖In cells ,there is significant concentration gradient of Na + and K+ across the cell membrane.
Potassium ions exchange with hydrogen or sodium ions.
1. High intracellular concentration of potassium is maintained by an energy requiring extrusion of 3 Na + out of the cell with replacement by K+ creating an electrochemical gradient across the cell membrane .
2. Intracellular K + is essential for number of enzymes reactions ( such as pyruvate kinase, protein synthesis ,and glycogen synthesis ) and for maintaining acid base balance.
3. Extracellular K+ (5 mequ/L of plasma )is important for its controlling influence upon:
➢neuromuscular irritability
➢Cardiac muscles ( a proper balance between K+ and Ca + + is essential for contraction of heart muscles )
➢The operation of Na + / K+ ATPase (the sodium pump )
❖Insulin stimulates the intracellular uptake of potassium.

Role of gastrointestinal tract in Homoeostasis of Potassium
Role of gastrointestinal tract in Homoeostasis of Potassium is as follows:
▪ Potassium from diet and gastrointestinal tract is reabsorbed in the small intestine and secreted in colon and rectum in exchange for sodium.
▪ Small amount of Potassium (< 1 mmols/day )is excreted in the feces .
▪ In chronic diarrhea and intestinal fistula fecal excretion is increased.

Potassium ions transport across the cell membrane

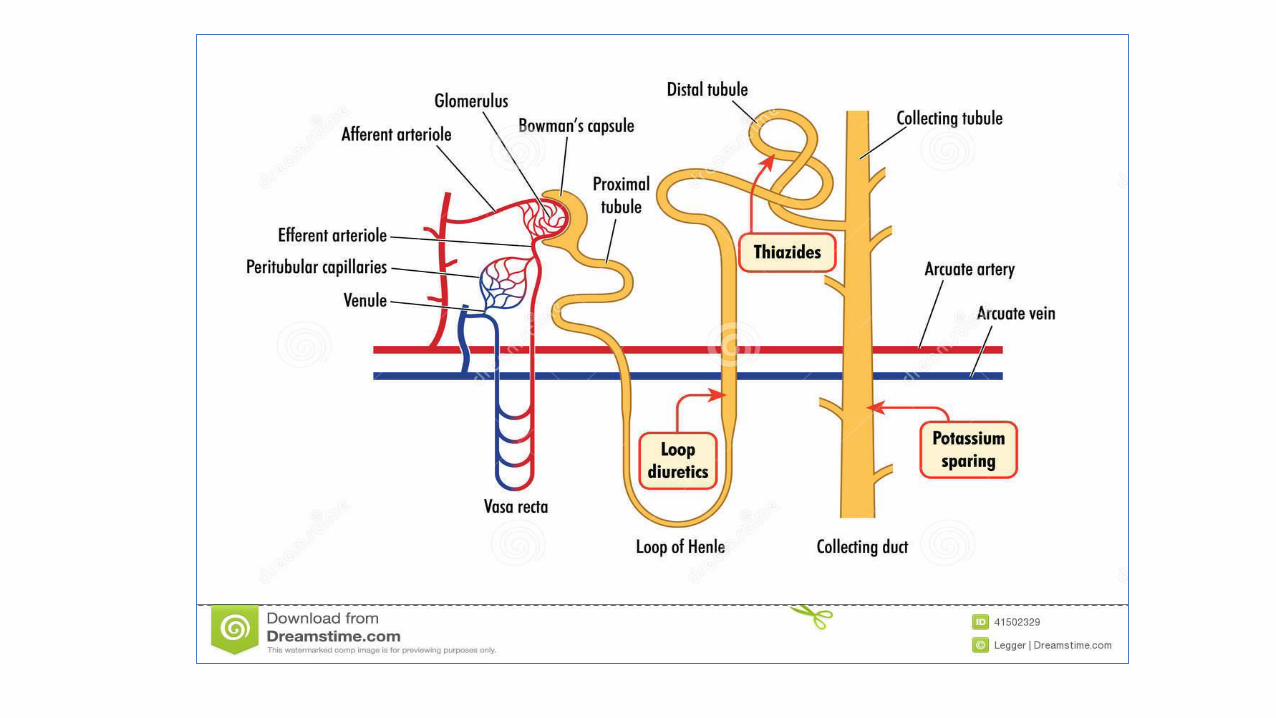
Role of Kidney in Homoeostasis of Potassium
➢Excretion of K⁺ through urine 50 -70 mequ/L (1.5-2gm/day )
➢Potassium is filtered by the glomeruli , reabsorbed in proximal convoluted tubules (PCT) and actively secreted in distal renal tubules in exchange of hydrogen or sodium ions.
➢If K⁺ concentration in blood rises by more than 1 mequ above normal values (3.5-5.5meq/L )stimulation of Aldosterone secretion Aldosterone increases secretion and excretion of K⁺ till Homoeostasis of Potassium isestablished.
➢Decrease in serum /plasma K⁺ inhibit Aldosterone secretion and Aldosterone secretion is brought about by renin –Angiotensin system of kidney.
➢Na ⁺ depletion renin secretion by kidney*Decrease in blood volume and pressure triggering renin secretion formation of Angiotensin II by the action of renin on 2- globulin production of Aldosterone excretion of K⁺.

Role of Kidney in Homoeostasis of Potassium

Role of Kidney in Homoeostasis of Potassium

Role of Kidney in Homoeostasis of Potassium
*
renin from kidney peptidase
Angiotensinogen Angiotensin I Angiotensin II
2- globulin (peptide with10 amino acids) (peptide with 8amino acids)
Angiotensin II stimulates smooth muscles and raises blood pressure (most active vasopressor ) .It action is by constricting arterioles and increasing heartbeats.
Angiotensin II later hydrolyzed by Angiotensinase .


Factors controlling Excretion of Potassium by Kidney in K⁺ Homoeostasis
❖Urinary potassium excretion depends upon:
1. Availability of sodium ions for exchange with potassium ions
2. The relative amount of hydrogen and potassium ions in the distal tubular cells
3. Plasma Aldosterone
4. In acidosis , hydrogen ions excreted and potassium ions reabsorbed.
5. In Alkalosis potassium ions excreted and hydrogen ions reabsorbed /conserved.


Homeostasis of potassium in human body

Homeostasis of potassium in human body

Clinical significance of Potassium Metabolism

Disorders of potassium metabolism
1. Hypokalemia: low serum potassium (deceases heartbeats and interferes with vital muscles such as those involved in respiration)
2. Hyperkalemia : high serum potassium
The capacity of kidney to excrete potassium is so high that Hyperkalemia will not occur normally .However it occurs in renal failure, advanced dehydration and shock.

Potassium metabolism-HypokalemiaHypokalemia1. serum potassium < 3mmol/ lt2. Symptoms : muscular weakness ,cardiac arrhythmias , cardiac arrest3. Correction by orange juice4. K⁺ administration in beneficial effect during insulin therapy as insulin
decreases serum potassium levels 5. Alkalosis associated with influx of potassium ions in exchange of protons 6. Conditions associated with Hypokalemiaa) Renal losses b) Prolonged vomitingc) Diarrhea d) Administration of Diuretics K⁺ excretion 7. Diuretics administration should be adjuvant K⁺ supplementation
Causes of hypokalemia❖Hypokalemia may occur due to :
Decreased intake of potassium
Loss of potassium from gut
Increased urinary excretion
Redistribution from ECF to ICF : after insulin treatment

Causes of hypokalemia-1❖Hypokalemia may occur due to :
Decreased intake of potassium as in
a)Dietary insufficiency of potassium (rare
b)Starvation
c)Severe illness
d)Post operatively after gastrointestinal surgery
e)Kwashiorkor
Loss of potassium from gut as in
a)Prolonged vomiting
b)Diarrhea
c)Steatorrhea
d)Intestinal fistula
Redistribution of potassium from ECF
to ICF
a)after insulin treatment
b)in alkalosis ,where potassium enters cells is associated with increased urinary loss of K+

Causes of hypokalemia-2❖Hypokalemia may occur due to Increased urinary excretion :
Increased urinary excretion observed in:
✓Hyperaldosteronism
✓ Cushing’s syndrome
✓Fanconi syndrome
✓Renal tubular acidosis in which there is availability of H + for exchange with K+
✓Ectopic production of ACTH
✓Thiazide diuretics that enhances Na + - K+ exchange and potassium excretion
✓Drugs that potentiate the action of Aldosterone ( e.g. carbenoxolone
✓Substances with Aldosterone like activity such as tobacco and liquor ice
✓Bartter’s syndrome in which thee is increased secretion of rennin and Aldosterone

Clinical Symptoms of Hypokalemia❖Neuromuscular manifestations
• Weakness • Lethargy
• Hypotonia
• Depression• Cramps
❖Cardiac manifestations
➢ Arrhythmias➢Hypotension
➢ECG changes :ST Depression, flattened T waves ,prolonged P-R intervals, prominent U waves
❖ Renal manifestations: inability to concentrate urine ,polyuria ❖ Alkalosis

ECG changes :ST Depression, flattened T waves ,prolonged P-R intervals,prominent U waves
ECG changes in Hypokalemia

Management of Hypokalemia➢Management of Hypokalemia include:
➢Oral administration of potassium chloride
➢Intravenous infusion of potassium chloride if Oral administration not possible
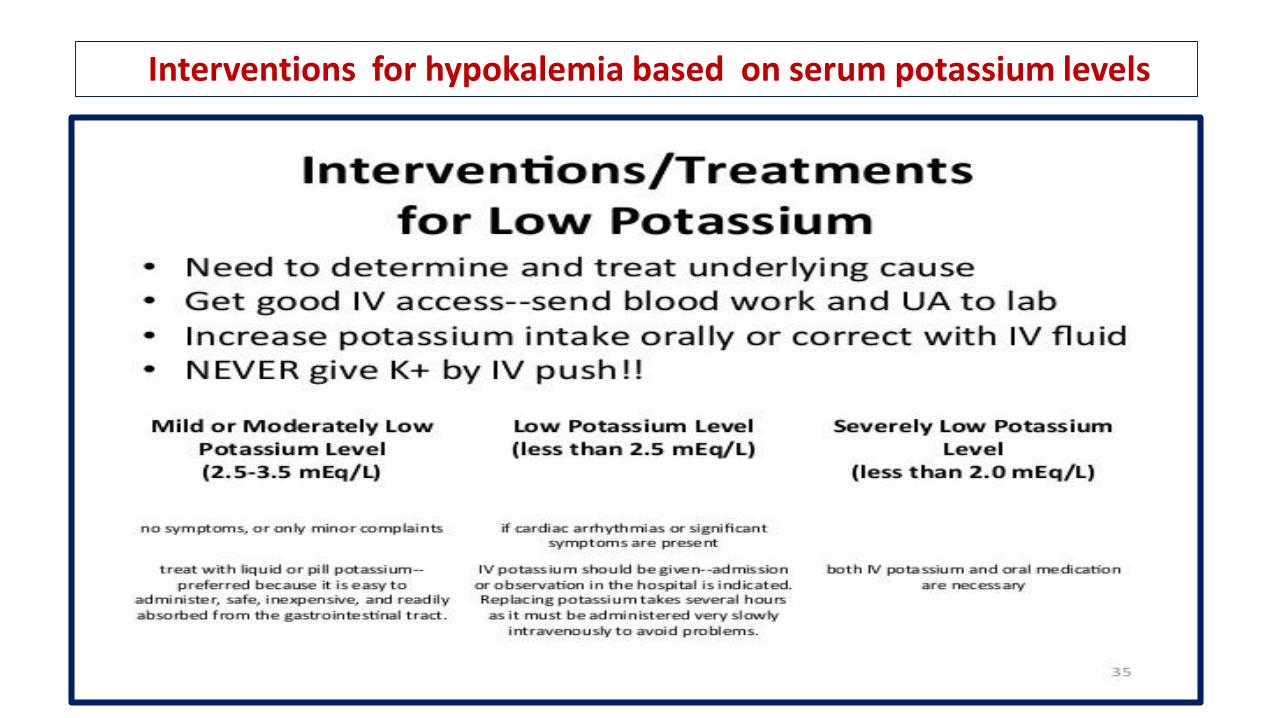
Interventions for hypokalemia based on serum potassium levels



Causes of Hyperkalemia-1❖Hyperkalemia may result from :
increased intake of potassium
Decreased urinary excretion of potassium
Excessive parenteral administration for treatment of hypokalemia
Redistribution of potassium from ICF to ECF
Causes of Hyperkalemia- 2 ❖Hyperkalemia may result from :
Decreased urinary of potassium excretion as in
• Addison’s disease
( adrenocortical insufficiency)
• Congenital adrenal hyperplasia
Redistribution of potassium from ICF to ECF
• Severe tissue damage
• Injury ,burns , postoperative conditions
• Hypoxia with failure of the sodium pump
• Acidosis associated with urinary excretion of potassium

Pathogenesis of Hyperkalemia

Clinical Symptoms of Hyperkalemia❖Neuromuscular manifestations
• Decreased membrane potential
• Increased repolarization
❖Cardiac manifestations
✓Decreased cardiac action potential
✓Bradycardia
✓cardiac arrest
✓Ventricular fibrillation
➢ECG changes : High T waves ,loss of P waves, broad QRS complex

Clinical Symptoms of Hyperkalemia

Clinical Symptoms of Hyperkalemia

ECG changes in Hyperkalemia

Management of Hyperkalemia-1• Management of Hyperkalemia include:
• Dietary control
• Correction of acidosis or water and sodium depletion
• Intravenous administration of calcium gluconate to reverse cardiac changes
• Insulin administration to promote potassium entry into cells
Insulin induced hypoglycemia can be prevented by glucose.
• Bicarbonate infusion to promote potassium entry into cells
• Potassium binding ion exchange resins that increase potassium excretion by exchanging sodium or calcium ions
• Dialysis to remove excess potassium

Management of Hyperkalemia based on its severity-2

Management of Hyperkalemia based on ECG changes-3

Comparison of hypokalemia and Hyperkalemia

Comparison of ECG changes in hypokalemia and Hyperkalemia
