metabolism, infection and immunity in inborn errors of ... · metabolism, infection and immunity in...
TRANSCRIPT

National Institutes of Health
U.S. Department of Health and Human Services
NATIONAL HUMAN GENOME RESEARCH INSTITUTE
Metabolism, Infection and Immunity
in Inborn Errors of Metabolism
Peter J. McGuire MS, MD
Physician-Scientist
Immunometabolism Unit

No conflicts of interest to declare

Medschoolwatercooler.blogspot.com

Acute metabolic decompensation
in IEM
• Defined as a functional deterioration in metabolic status
• Are disease specific
• Can be life threatening
• Can be associated with long-term complications
• Triggers include dietary indiscretion, insufficient calories, infection
• Infection associated with increased morbidity (McGuire et al., 2013)
unstable
stable
Metabolichomeostasis

Outline
• What is the immune system and why is it
important?
• Infection and IEM
• Immune function in IEM

Why is the immune system
important? • Protects us against
Bacteria Viruses Fungi
Cancer Parasites Pollution

The immune system has
multiple lines of defense

The immune system is
composed of organs and
cells Organs Cells

The immune system has many different type of cells
Bone graft
Multipotential stem cell
Hematopoietic stem cell
Platelets
Macrophage
Erythrocytes
Eosinophil
Neutrophil
Megakaryocyte
Mast cell
Basophil
T lymphocyte
Natural killer cell
Dendritic cell
B lymphocyte
Lymphoid progenitor cell
Myeloid progenitor
cell
Monocyte
Marrow
Bone

How does the immune system
protect us?
• Body learns to defend
itself by:
– Natural infection
– Vaccination

vaccina on
YYYYYY
YYY
infec on
Y Y Y Y Y
YYYYYY
YYY
YYYYYY
YYY
YYYYYY
YYY
YYYYYY
YYY
YYYYYY
YYY
“Immunememory”
Y
T-cellsandB-cells
Protec vean bodies
Key:
Weeks Years Days Years
Y Y Y
How does the immune system
protect us?

Why study immune function in
metabolic disorders?
• Because:
– Infection is bad for patients
with IEM
• Our question:
– Does having a IEM affect
immune function?

Infection is bad for patients with IEM
• Point #1: Infection increases
caloric requirements
– For every 1° C of fever, metabolic
rate can increase 10% or more
– Problem: need more calories, but
you don’t feel like eating; ability to
generate energy

Infection is bad for patients with IEM
• Point #2: Infection can cause increased breakdown
Muscle Fat

Infection is bad for patients with IEM
• Point #3: Infection can inhibit metabolism – ammonia metabolism
CPS1 enzyme
McGuire et al., 2014
Sickness
Behaviors
Infection
Sac
Sac
spf-ash controls
spf-ash controls
spf-ash Controls
4-6 week old
Day 0
Day 1
Day 2
Day 3
Day 4
Day 5
A B
N= 5 N= 5
Euthanize
Inhalation based infection
Contr
ol
Infe
cted
0
50
100
150
CP
S1 e
nzym
e a
cti
vit
y
(co
ntr
ol ra
tio
)
Contr
ol
Infe
cted
80
85
90
95
100
105
110
OT
C e
nzym
e a
cti
vit
y
(co
ntr
ol ra
tio
)

Infection is bad for patients with IEM
• Point #3: Infection can inhibit metabolism - fatty acid oxidation
Longchainacyl-coA
CPT1a
Longchainacylcarni ne
Longchainacyl-coA
CACT
Longchainacylcarni ne
ETFDHI
IIIII
IV
V
CPT2
Acetyl-coA
β-oxida on
ETFA/B
e-e-e- e
-
e-e-
e- e-e-
e-
TCAcycle
Ketones
MitochondriaLong chain fats
Metabolomics

13C-palmitate oxidation breath testing
Tarasenko et al (in preparation)
Time (min)
Perc
en
t d
ose o
xid
ized
0 30 60 90 120
150
0
20
40
60
80
Infection
Control

Contr
ol
Infe
cted
0.0
0.5
1.0
1.5
CP
T2 m
RN
A
(co
ntr
ol ra
tio
)
Contr
ol
Infe
cted
0.0
0.5
1.0
1.5
AC
AD
VL
mR
NA
(c
on
tro
l ra
tio
)
Contr
ol
Infe
cted
0.0
0.5
1.0
1.5
AC
AD
L m
RN
A
(co
ntr
ol ra
tio
)
Contr
ol
Infe
cted
0.0
0.5
1.0
1.5
CA
CT
mR
NA
(c
on
tro
l ra
tio
)
Contr
ol
Infe
cted
0.0
0.5
1.0
1.5
HA
DH
A m
RN
A
(co
ntr
ol ra
tio
)
Contr
ol
Infe
cted
0.0
0.5
1.0
1.5
ET
FA
mR
NA
(c
on
tro
l ra
tio
)
A B
VL
CA
D (
co
ntr
ol ra
tio
)
Contr
ol PR8
0.0
0.5
1.0
1.5
2.0
2.5
LC
AD
(co
ntr
ol ra
tio
)
Contr
ol PR8
0.0
0.5
1.0
1.5
HA
DH
A (
co
ntr
ol ra
tio
)
Contr
ol PR8
0.0
0.5
1.0
1.5
VLCAD
b-actin
LCAD
HADHA
Control Infected
Infection decreases components of
hepatic fatty acid oxidation
Tarasenko et al (in preparation)
mRNA protein

Acute metabolic decompensation
in IEM: FAO Long chain acyl-coA
CPT1a
Long chain acylcarnitine
Long chain acyl-coA
CACT
Long chain acylcarnitine
ETFDH I
II III
IV
V
CPT2
Acetyl-coA
β-oxidation
ETFA/B
e-
e-
e- e-
e- e-
e- e-
e- e-
TCA cycle
Ketones
Mitochondria

Infection is bad for patients with IEM
• Point #3: Infection can inhibit metabolism - pyruvate dehydrogenase

13C-Pyruvate
13C-Pyruvate
AcetylcoA+13CO2
TCA
PDH
13C-Lactate13C-Alanine
ALT LDH
Mitochondria
Hyperpolarized 13C-pyruvate:
assessment of in vivo pyruvate dehydrogenase
Contr
olPo
lyI:C 2 ho
urs
Poly I:C
3 da
ys
0
100
200
300
400
Co
ntr
ol % Lac/Pyr
Ala/Pyr
P<0.01
P<0.01
Figure 7: Poly I:C results in increased Lactate/Pyruvate and Alanine/Pyruvate.
Hyperpolarized 13C-pyruvate was injected by tail vein and alanine and lactate production
were measured by MR spectroscopy.
Tarasenko et al (in preparation)

Infection is bad for patients with IEM
• Point #3: Infection can inhibit metabolism – mitochondria
Tarasenko et al (in preparation)
Pairfed
Infected
0
100
200
300
400
500
AS
T (
U/L
)
Pair f
ed
Infected
0
50
100
150
AL
T (
U/L
)Day 0
Day 5
P<0.01P<0.01
Contr
ol Inf
ected
0.0
0.5
1.0
1.5
mtD
NA
(co
ntr
ol ra
tio
)
Figure 2: Influenza causes (A) hepatitis and (B) mtDNA depletion
in B6 mice. Mice were infected with PR8 influenza and euthanized
on Day 5.
A B
P=0.03
Co
mp
lex I / t
ub
ulin
rati
o
Contr
ol
2 hours
72 h
ours0.0
0.5
1.0
1.5 P = 0.04
Co
mp
lex II / tu
bu
lin
rati
o
Contr
ol
2 hours
72 h
ours0.0
0.5
1.0
1.5P <0.01
Contr
ol
2 hours
72 h
ours0.0
0.5
1.0
1.5
Figure 6: Poly I:C results in (A) PDH phosphorylation and
depletion and (B) respiratory chain complex depletion after 72
hours by immunoblot.
Co
mp
lex III / t
ub
ulin
rati
o
Contr
ol
2 hou
rs
72 ho
urs
0.0
0.5
1.0
1.5P <0.01
Co
mp
lex V
/ t
ub
ulin
rati
o
Contr
ol
2 hou
rs
72 ho
urs
0.0
0.5
1.0
1.5P = 0.02
Figure 6: Poly I:C results in (A) PDH phosphorylation and
depletion and (B) respiratory chain complex depletion after 72
hours by immunoblot.

Infection is bad for patients with IEM
• Point #4: The immune response may be
part of the problem - cytokines
PBS
TNF
!IL-
1"
IL-2
IL-6
IFN!
IFN"
IFN#
0.0
0.5
1.0
1.5
NA
GS
/b-a
ctin
(co
ntr
ol ra
tio
)
PBS
TNF
!IL-
1"
IL-2
IL-6
IFN!
IFN"
IFN#
0.0
0.5
1.0
1.5
CP
S1
/b-a
ctin
(co
ntr
ol ra
tio
)
PBS
TNF
!IL-
1"
IL-2
IL-6
IFN!
IFN"
IFN#
0.0
0.5
1.0
1.5
OT
C/b
-ac
tin
(co
ntr
ol ra
tio
)
A B C
0 ng/m
L0.1
ng/m
L1 n
g/mL
10 ng
/mL
0.0
0.5
1.0
Am
mo
nia
me
tab
olis
m
(co
ntr
ol ra
tio
)
IL-1b
0 ng/m
L0.1
ng/m
L1 n
g/mL
10 ng
/mL
0.0
0.5
1.0
Am
mo
nia
me
tab
olis
m
(co
ntr
ol ra
tio
)
IL-6
0 ng/m
L0.1
ng/m
L1 n
g/mL
10 ng
/mL
0.0
0.5
1.0
Am
mo
nia
me
tab
olis
m
(co
ntr
ol ra
tio
)
TNFa
0 ng/m
L0.1
ng/m
L1 n
g/mL
10 ng
/mL
0.0
0.5
1.0
Am
mo
nia
me
tab
olis
m
(co
ntr
ol r
atio
) IL-6
TNFα
IL-1β
A B C D
E F G H
I
Cytokines produced as part of the immune response inhibit
ammonia metabolism in human liver cells.
Immune cells “text”
each other by cytokines
May be innocent
bystanders (e.g. liver)
CPS1 liver cells
cytokines PB
S
TNFα
IL-1βIL
-2IL
-6
IFNαIF
NβIF
Nγ
0.0
0.5
1.0
1.5N
AG
S/b
-ac
tin
(co
ntr
ol r
atio
)
PBS
TNFα
IL-1βIL
-2IL
-6
IFNαIF
NβIF
Nγ
0.0
0.5
1.0
1.5
CP
S1
/b-a
ctin
(co
ntr
ol r
atio
)
PBS
TNFα
IL-1βIL
-2IL
-6
IFNαIF
NβIF
Nγ
0.0
0.5
1.0
1.5
OT
C/b
-ac
tin
(co
ntr
ol r
atio
)
A B C

Infection is bad for patients with IEM
• Point #4: The immune response may be
part of the problem.
cytokines
PolyI:C
TNFα
IL12/18
IFNγKC
NK
T
HSC
PolyI:C
TNFα
IL12/18
IFNγKC
NK
T
HSC
Clodronate
• Point #4: The immune response may be
part of the problem – immune cells

Infection is bad for patients with IEM
• Point #4: The immune response may be
part of the problem.
cytokines
Contr
olPo
lyI:C 2 ho
urs
Poly I:C
3 da
ys
0
100
200
300
400
Figure 7: Poly I:C results in increased Lactate/Pyruvate and Alanine/Pyruvate.
Hyperpolarized 13C-pyruvate was injected by tail vein and alanine and lactate production
were measured by MR spectroscopy.
Tarasenko et al (in preparation)
CD
11
b
F4/80
3.05% 0.053%
CD
11
b
F4/80

Infection is bad for patients with IEM
• Point #5: What do we see clinically with infection?
McGuire et al., 2013
Oth
erDie
t
Infe
ctio
n0
1
2
3
4
5
6
7
Ho
sp
ital d
ays
*
Oth
erDie
t
Infe
ctio
n0
20
40
60
80
100IV
scaven
gers
(%
HA
even
ts ) *
A B
Summary:
hospital admissions
hospital days
Ammonul use
Immune function in IEM
• Since infection can be very
serious...
– How well does the immune
system function in patients with
IEM?
– Can patients with IEM be
protected from illnesses by
vaccination?

Immune function and IEM
• What do we know? Not much,
but…
– Immune cells don’t like high levels
of toxins
– Immune cells don’t like nutritional
deficiencies
– Certain IEM enzyme deficiencies
are also present in immune organs
and cells

Immune function and IEM:
toxins
Wajner et al. (1999)

Immune function and IEM:
nutritional deficiencies PrimaryNutrientDeficiency ImmuneSystem ImmuneResponseProteinCalorieDeficiency Thymicatrophy,↓lymph
nodes/tonsils/T-cells,↑
IgA,↑/-IgG
↓Skinreactivity,↓cytokineresponse,might
respondtovaccines,riskof
infectionProteindeficiency(kwashiorkor) AlteredT-cellsubsets,↑
IgA,↑/-IgG
↓Skinreactivity,↓
cytokineresponse,might
respondtovaccines,riskofinfection
Zinc Lymphopenia,thymicatrophy,alteredT-cell
subsets
↓Skinreactivity,↓cytokineresponse
Iron T-celldefects,↓IgG,↓phagocyticactivity
↓Cytokineresponse,riskofinfection
Copper Lymphopenia ReducedIL-2response
Selenium ↓Antioxidantdefense ↑Viralvirulence
VitaminA Lymphopenia,↓mucosalbarrier
↓T-cellresponse(TH2),↓phagocyticcellandNK
function
VitaminE ↓Antioxidantdefense,↑IgElevels
↑PGE2production,↑viralvirulence
VitaminC ↓Plasmaglutathione ↓Phagocytefunction,riskofinfections
Arginine ↓T-cellproliferation,↓
TCR
Riskofinfections
Citrulline Seearginine Seearginine

Immune function and IEM:
enzymes in immune cells
Naive Ac vated
T-reg
Th17
Th1
Th2
Memory
FAO Glycolysis/Glutaminolysis
FAO
FAO
Glycolysis
Glycolysis
Glycolysis
T-cells need fatty acid oxidation to function!

Immune function and IEM
• What don’t we know? A lot…
– How well do immune cells from patients
with IEM function?
– Do patients with IEM develop immune
protection following vaccination?

Vaccination in IEM
• Regular childhood vaccinations are
recommended including influenza (Barshop
and Summar, 2008)
• Childhood vaccines are not associated
with adverse events (Klein et al, 2011 and Morgan
et al, 2011)
• Do patients with IEM respond? (Brady, 2005)
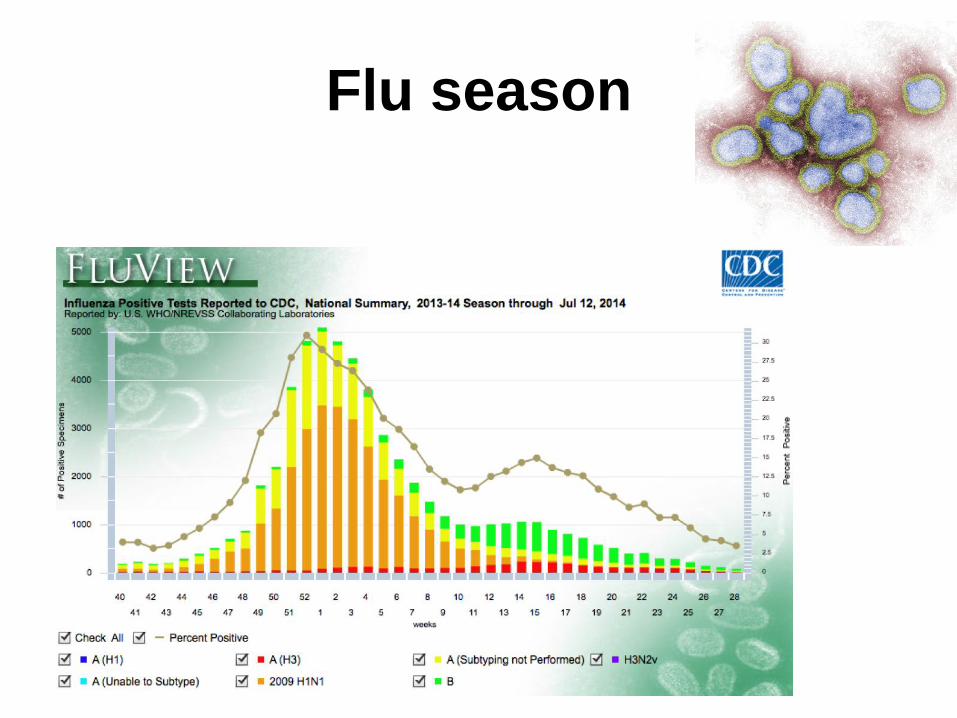
Flu season

Seasonality of elevated blood ammonia H
A e
ven
ts
August
Sep
tem
ber
Oct
ober
Nove
mber
Dec
ember
Januar
y
Febru
ary
Mar
ch
Apri
l
May
June
July
0
5
10
15
20
Infection
Diet
Peter McGuire (unpublished data)

Do IEM patients respond to
influenza vaccines?
Esposito et al (2013)

www.nationaljewish.org

The NIH MINI Study: Metabolism,
Infection, and Immunity in Inborn Errors
of Metabolism (NCT01780168)
Participant travel and lodging is provided

Our focus
• To learn how
inborn errors of
metabolism may
affect the function
of the immune
system and vice
versa
Metabolism
Immunity
IEM

MINI Study Participants
Who can participate?
To be in the study a person must:
• Be at least 2 years of age
• Have a biochemically
confirmed diagnosis of an IEM
or related disorder
We can not enroll anyone who:
• Is under 2 years of age
• Is being treated for an
intercurrent infection with
antibiotics, has evidence of an
acute infection, or has acute
decompensation
• Has received another vaccine
or immune modulating drug
within the past 6 months
• Is currently living in a hospital
• Does not have a local / regular
physician to manage their IEM

How can I participate?
• At the NIH Clinical Center
– Out-patient
– In-patient +/- outpatient
• Samples only

America’s Research Hospital
Travel and lodging arranged and covered by NIH
Meals covered by NIH

Children’s Inn at NIH
How can I participate?
• Participating as an out-patient
– Immune profiling
• Immune cell populations and function, total antibodies,
antibodies to childhood vaccinations, inflammation markers,
offer vaccination for flu, hep A and pneumococcal disease
– Nutritional profiling
• Dietary analysis; body composition; bone density
– Address patient needs
• Dentistry, Neurology, Physical Medicine and Rehabilitation,
Endocrinology, Immunology, etc.
How can I participate?
• Participating as an in-patient +/- out-patient
– Immune profiling
• Immune cell populations and function, total antibodies,
antibodies to childhood vaccinations, inflammation markers,
offer vaccination for flu, hep A and pneumococcal disease
– Nutritional profiling
• Dietary analysis; body composition; bone density; energy
expenditure
– Address patient needs
• Dentistry, Neurology, Physical Medicine and Rehabilitation,
Endocrinology, etc.

How can I participate? • Participating as samples only
– Blood- during infectious illnesses (e.g. Flu) and well
states
– Cord blood – humanized mouse models
– Tissues that result from a medical procedure
including, but not limited to, liver, tonsil, spleen
samples
– Liver Tissue Collection and Distribution System –
University of Minnesota

What is the status of the immune
system in IEM?

What have we found? Screening (Children N=38)
• Ear infections (>4/yr) 18%
• Sinus infections (>2/yr) 18%
• Antibiotics with little effect 13%
• Pneumonia (>2/yr) 8%
• Growth failure 47%
• IV antibiotics 45%
• ICU admission for infection 21%
• Delayed recovery 50%
• Persistent thrush/fungal 13%
• Deep seated infection 13%
• History of immunodeficiency 13%
• Immune evaluation 15%
• IVIG treatment 8%
• Prophylactic antibiotics 29%
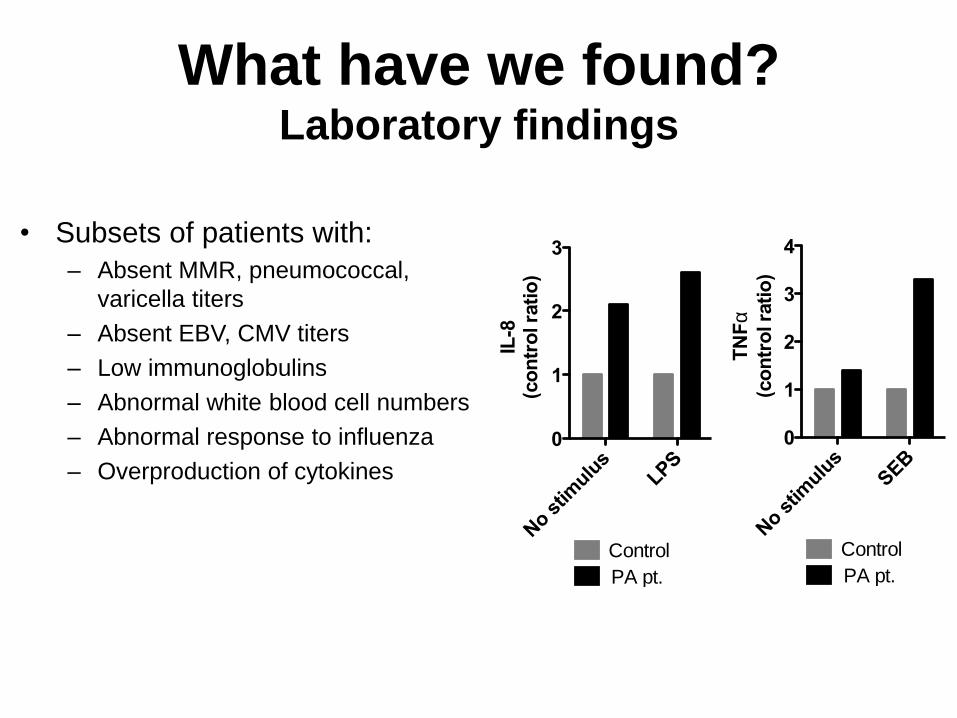
What have we found? Laboratory findings
• Subsets of patients with:
– Absent MMR, pneumococcal,
varicella titers
– Absent EBV, CMV titers
– Low immunoglobulins
– Abnormal white blood cell numbers
– Abnormal response to influenza
– Overproduction of cytokines
No s
timulu
sLP
S0
1
2
3
IL-8
(c
on
tro
l ra
tio
)Control
PA pt.
No s
timulu
sSEB
0
1
2
3
4
TN
Fa
(co
ntr
ol ra
tio
)
Control
PA pt.

Summary
• The immune system is important for vaccination
and protection against infection
• Infection is detrimental to patients with IEM
• Subsets of patients with IEM may have immune
dysfunction – Toxicity
– Metabolic dysfunction
– Nutritional perturbations

www.genome.gov/mini

MINI Study contact information
Principal Investigator
Peter J. McGuire MS, MD
Study Coordinator
Janet Shiffer, NP
Telephone
301-451-9145
Website
http://www.genome.gov/mini
Thank you

Any questions?