meghan shank: how can we be better communication partners?
TRANSCRIPT
How Can We Be Better Communication Partners?: A look at AAC intervention strategies
Rett Syndrome SymposiumOctober 1, 2016
By: Meghan Roe Shank, [email protected]
Augmentative and Alternative Communication Team LeadChildren’s Hospital Colorado
Disclosure
Financial Disclosures: I am a paid employee of Children’s Hospital Colorado.
I have no financial or otherwise affiliations with the devices, equipment, products, or organizations mentioned or shown in this presentation.
Agenda For Today:
1) Inform you of my role within the Rett Clinic here at CHCO, and what services we offer to help you with advocacy, and making appropriate referrals, if needed.
2) Discuss ideas for what “ideal” AAC intervention might look like, and provide ideas related to communication targets (e.g., language functions, literacy).
3) Discuss 7 Communication Partner Training Techniques and how we are measuring their effectiveness in speech therapy.
Rett Clinic at Children’s Hospital Colorado
Purpose: Our services include consultation and evaluation for all people with Rett Syndrome to ensure they are receiving the needed therapies, treatments, and services to live a quality life.
Goal: To provide the best consultative care and therapeutic advice for individuals with Rett Syndrome. We also strive to provide up-to-date information on Rett Syndrome to parents, physicians, therapists, and care providers; participate in ground breaking clinical research trials and work as a team with the family and primary care providers.
Dr. Tim Benke’s Research Questions
•What are appropriate standards of care for patients with Rett?
•What are appropriate therapy guidelines and targets?
•What therapies can improve outcomes?
•What emerging pharmaceuticals/nutraceuticals are appropriate for clinical trials?
•What are the implications of specific genetic mutations for standards of care and therapies?
A Perspective:
“We feel therapy has given our daughter a better quality of life than she would have had. This does not mean we do therapy ten hours a day. Never. It means we found a way to incorporate therapy into her daily life. Using her environment and buddy switches, she helps me make cookies. This could be thought of as practicing switch use but we think of it as plain old fun. Mother and daughter time. Just seeing the big smile she gives and her chest pushed out with pride when Dad makes a fuss over the cookies she helped bake is enough.”
1st step: Consultation
- How does your child currently communicate?
- What therapies are you receiving and where are those taking place?
- What is your therapy frequency/duration?
- Do you have equipment or a Speech Generating Device (SGD) already?
- If not, would you like to look into using some Augmentative and Alternative Communication (AAC) strategies or systems?
- What does hand function look like, and do we need to evaluate your child using alternative access methods?
2nd Step: The Evaluation Process
•Cognition, Understanding of Language, receptively.
•Continuation of a motivating activity, cause/effect.
•Pictures for communicative purposes (photographs, line drawings, visual scenes).
•Access (direct selection with possible key guard, eye gaze, head mouse, scanning)
•Seating/Positioning in consultation with an Occupational therapist.
Evaluation: Cognitive/Receptive Skills
• Alertness
• Attention span
• Understanding of causal and differentiated causal relationships
• Understanding of object permanence
• Understanding of means-end
• Ability to express preferences/make choices
• Understanding of visual representations (objects, pictures, etc.)
• Learning style
(visual, auditory, tactile, motor)
Evaluation: Receptive Language Abilities
•Localize to sounds, name
•Follow directions within context
•Follow directions out of context
•Follow conversation
•Respond to humor
•Understanding of nouns, verbs, prepositions, and adjectives
•Understanding of questions
•Yes/no (request/protest vs. demonstrate knowledge)
•WH
Evaluation: Current Expressive Communication
•vocalizations
•verbal approximations
•gestures
•facial expressions
•postural change/tone
•behavior
•objects
•pictures (labels,
photographs, Picture
Communication Symbols,
Unity, visual scenes)
•digitized and synthesized
speech output
communication system
Evaluation: Motor Abilities
•Positioning- Keeping in mind “the running start”
•Blocking
•Access (easiest means possible with least negative impact)
•direct selection (fingers, toes, head pointer, Head Mouse)
•scanning
•Eye Gaze
Is Eye-Gaze the Answer for Everyone?
•Don’t assume your student recognizes pictures or knows how to use them to communicate, simply because she can see (or has visual acuity).
•Don’t assume your student can’t learn pictures if you’ve never taught them for an extended period of time with the tools. Ex. Snowboarding
Ok, now what do I do?
•Teach V. Test: It’s important to use pictures for communication, not in a testing “show me” manner.
•Teach, teach, teach! The typically developing infant is exposed to language for a year before it ever says its first word. Allow our children to “babble” on their devices.
•Your child is learning a new language through pictures- a visual system of language, not a primarily auditory one.
Treatment Planning and Goals:
•Our team tends to write based on the idea of language functions. The “why” behind communication.•Requesting
•Directing
•Commenting
•Questioning
•Sharing Information
•Greeting
•Participation (Beukelman and Miranda , 2005)
•However, Linda Burkhart, suggests writing goals as overall # of functions used (3 per session, ect.)
•Language based goals- combine 2 words, ect…follow regular language trajectory
Sample Treatment Plan- It’s not about the tool (hit a switch); It’s about the languageShort Term Objective #1 Pt. will request preferred activities, places, or objects using her speech generating device from a field of 4 options 80% of the time given minimal verbal cues over 3 consecutive sessions. Short Term Objective #2 Pt. will protest (e.g., "all done" "stop") using her speech generating device from a field of 4 options 80% of the time appropriately given minimal verbal and visual cues over 3 consecutive sessions. Short Term Objective #3 Pt. will direct activities (e.g., "go" "turn" "come") using her speech generating device from a field of 4 options 80% of the time given minimal verbal and visual cues over 3 consecutive sessions. Short Term Objective #4 Pt. will greet others using her speech generating device given a minimal verbal cue 2x/session over 3 consecutive sessions.
How do I target these goals?
Part II
Strategy #1: Pair Objects with Photos/Pictures
Strategy #2: Aided Language Stimulation
Therapist is modeling visual representation for “go”
(Video)
Strategy #3: Core Words
-The high-frequency words that research shows makes up the majority of adult speech. Hint: They aren’t nouns.
(Video)
Strategy #4: Sabotage
-She doesn’t swing for very long without having to request again!
(Video)
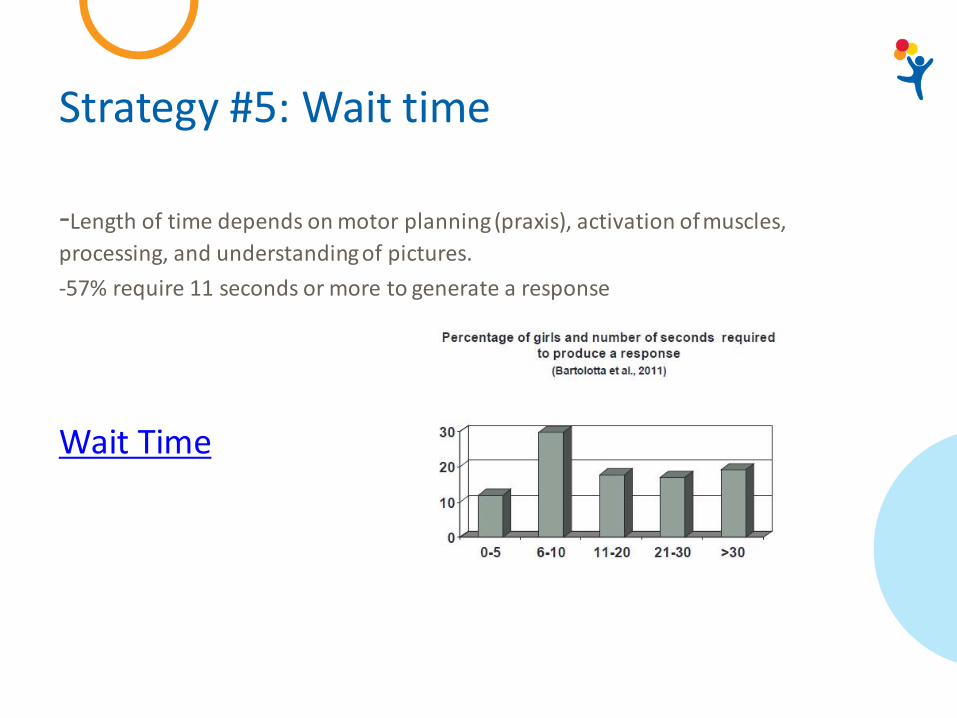
Strategy #5: Wait time
-Length of time depends on motor planning (praxis), activation of muscles,
processing, and understanding of pictures.
-57% require 11 seconds or more to generate a response
Wait Time
Strategy #6: Decrease Cueing Over Time
- Clinician gives a max model at first, starts to give a visual cue, then student is independent
Strategy #7: Communication Expectations In Daily Routines
-See student crossing Mid-line, eye contact upon command
-That’s the first thing we do when she comes into therapy each week.
(Video)
So now that we’ve taught family 1 strategy a week, how do we know that it’s working?
•We are gathering Outcome Data by using a Pre- and Post- Survey completed by each family.
•Likert scale from 1-5, “How comfortable are you with….”
A Look at the Measuring Tool
•Takes Data In the Following Areas:
Communication Partner Strategies
Operational Competence
Linguistic Competence
Strategic Competence
Social Competence
Literacy
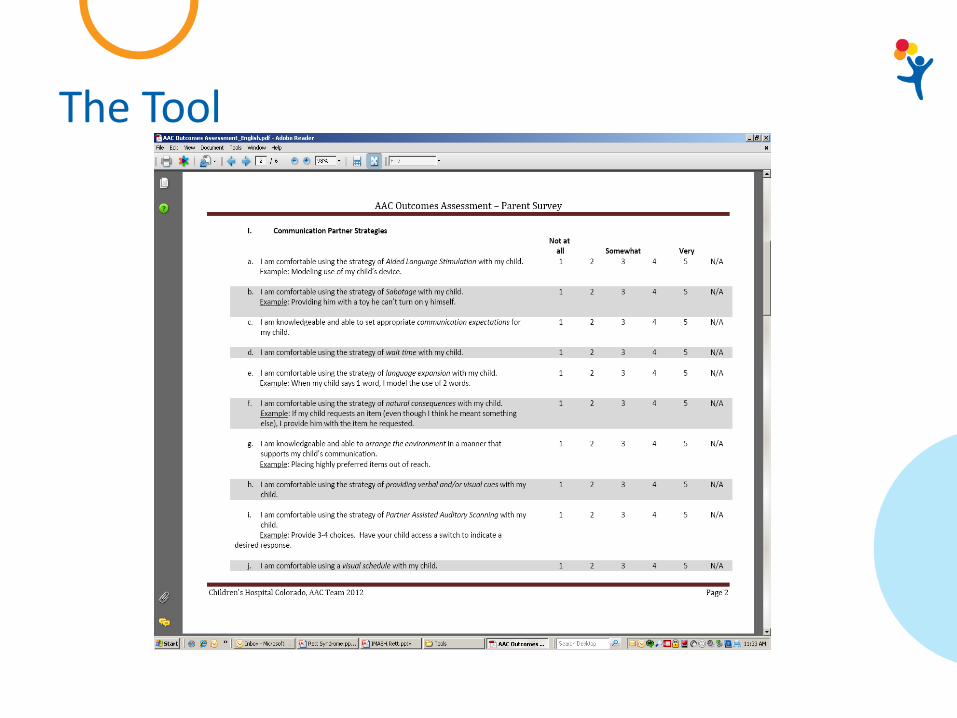
The Tool
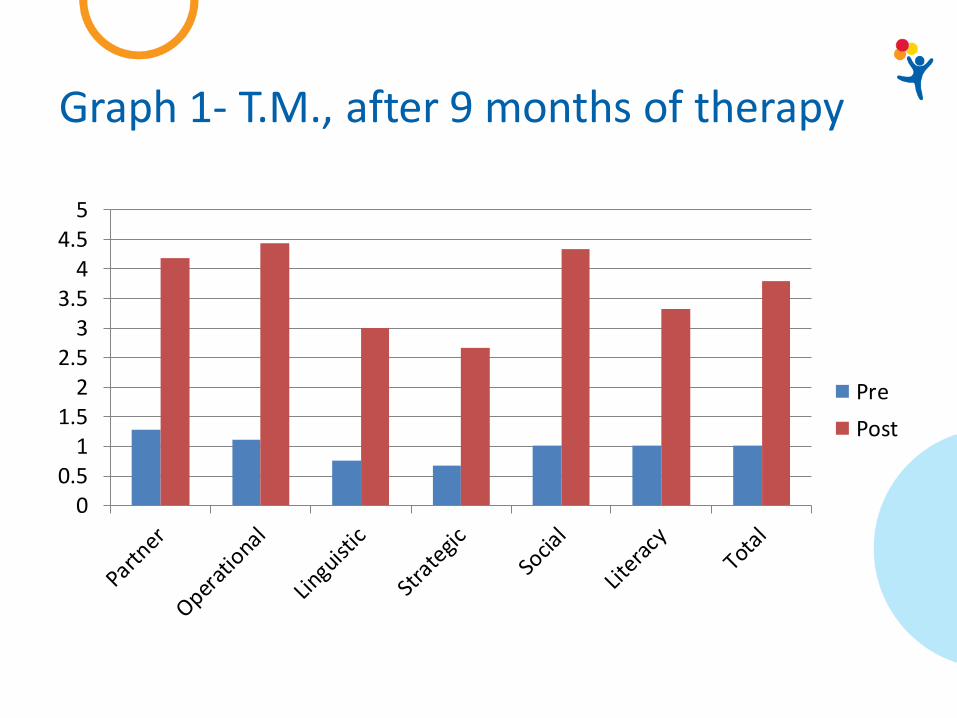
Graph 1- T.M., after 9 months of therapy
00.5
11.5
22.5
33.5
44.5
5
Pre
Post
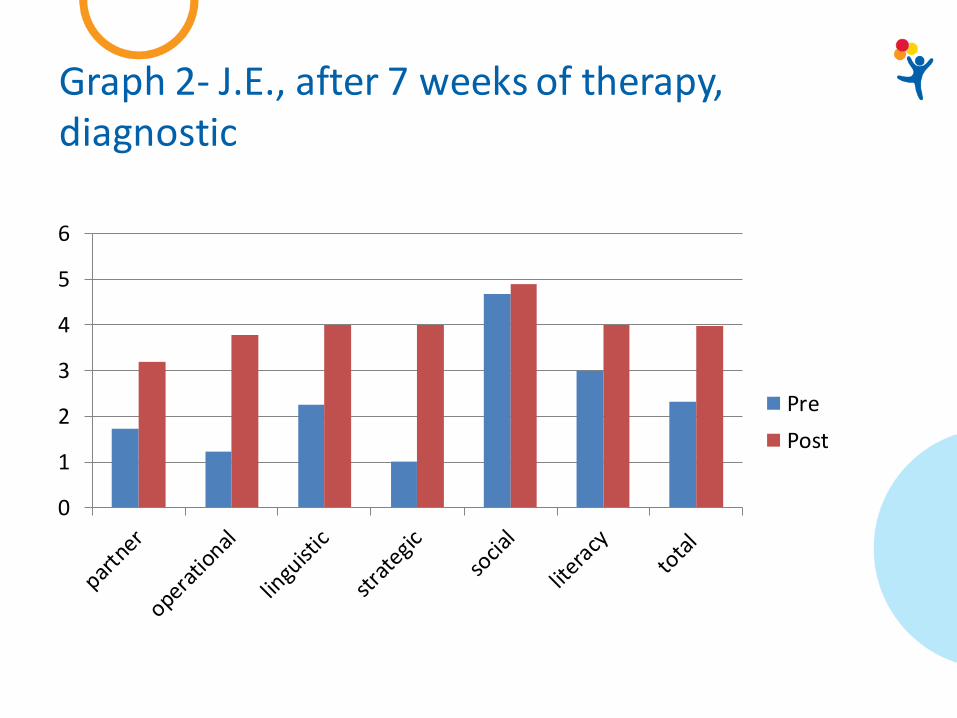
Graph 2- J.E., after 7 weeks of therapy, diagnostic
0
1
2
3
4
5
6
Pre
Post
A note about Literacy Instruction
For ideas on how to develop literacy skills with a speech generating device, consider:1. The A.L.L. Curriculum by Dr. Janice Light: http://www.mayer-johnson.com/all-reading-curriculum. Some districts have this curriculum available through their SWAAAC teams, so it is recommended that you call your district SWAAAC team to inquire. Free webinars by Dr. Janice Light are available to learn more about the program. They can be found at this website: http://aac-rerc.psu.edu/index.php/webcasts/show/id/1. Another great literacy resource is here: http://aacliteracy.psu.edu/
2. Susan Norwell's curriculum through Rett University. Susan's approach incorporates 4 Blocks of reading and is specifically designed for the Rett Syndrome population. For a cost, you can take her online courses/webinars. http://rettuniversity.org/member/susan-norwell/
3. Linda Berkhart's Website regarding Applications and Strategies: http://www.lindaburkhart.com/haacrett.html
Literacy Intervention
ALL Curriculum, Stage 1, Phoneme Recognition
ALL Curriculum, Stage 5, Syllable Segmentation
AAC Evaluation Centers
1. Children’s Hospital Colorado: Contact Felicia Hardney at (720) 777-5537
2. Assistive Technology Partners (ATP): (303) 556-2040
3. Jill Tullman and Associates: (303) 284-4021
4. Inspiring Talkers: (720) 378-6670
5. School district SWAAAC/Assistive Technology Teams
Speech Therapy for Girls with Rett Syndrome: A Parent’s Perspective
“We battled for many months with our insurance company just to prove that our daughter would benefit from private speech therapy. She is non-verbal, so our insurance company didn’t feel it was “medically necessary” for her to receive speech services. Thank goodness we are strong advocates for her, or we may have accepted their denial and never have seen the strides our daughter has made with augmentative communication.
Our daughter has Rett Syndrome. She is non-verbal, so many people feel that since she cannot speak, that she doesn’t understand people or will never learn to communicate. That is far from the truth. The problem is, she suffers from Apraxia. Our daughter has been through the gamut of speech devices and she benefits from direct selection devices. Because of her apraxia, it can seem at times that she is just randomly batting at the buttons. However, she is actually pretty purposeful in her selections.
One thing we want you all to know is Please never give up on our daughters with Rett Syndrome. They really are locked in a shell and need your help to break free from it. It is a long hard road to make a breakthrough with communication, but with patience and perseverance, you can make a huge difference in a girl’s life and her family’s life.”
References
Bartoloatta, T. & Remshifski, P. (2011). Communication and Swallowing in Rett Syndrome: An Update for Clinicians. Slides.
Bartolotta, T. & Remshifski, P. (2012) Coaching communication partners: A preliminary investigation of communication intervention during mealtime in Rett Syndrome. Communication Disorders Quaterly, published online DOI: 10.1177/1525740112453165.
Beukelman, D.R., & Mirenda, P. (2005). Augmentative and Alternative Communication: Supporting Children and Adults with Complex Communication Needs. Baltimore: Paul H. Brooks.
Bruno, J. & Trembath, D. (2004). Use of aided language stimulation to improve syntactic performance during a weeklong intervention program. Manuscript submitted for publication.
Cress, C. & Marvin, C. (2003). Common questions about AAC services and early intervention. Augmentative and Alternative Communication, 19, 254-272.
Gossens’, C., Crain, S., & Elder, P. (1992). Engineering the preschool environment for interactive, symbolic communication . Birmingham, AL: Southeast Augmentative Communication Conference Publications.
Harris, J. & Reichle, J. (2004). The impact of aided language stimulation on symbol comprehension and production in children with moderate cognitive disabilities. American Journal of Speech-Language Pathology, 13, 155-167.
Hunter, Kathy. The Rett Syndrome Handbook. (2007)
Light, J., Collier, B., & Parnes, P. (1985). Communication interaction between young nonspeaking physically disabled children and their caretakers: Part 1: Discourse patterns. Augmentative and Alternative Communication, 1, 63-74.
