mechanism of cardiogenic shock - homepage |...
TRANSCRIPT

Mechanism of Cardiogenic Shock
By Santiago V. Guzman, M.D., Edward Swenson, M.D.,and Robert Mitchell, M.D.
• The mechanism of shock following acutemyocardial infarction is still controversial.Xumerous investigators have applied tech-niques such as: (a) ligation of the differentbranches of the coronary arteries,1"4 (b)chemical or traumatic methods to producemyoeardial injury/" and (c) introduction ofeinbolizing particles into the coronary circu-lation." The results are conflicting, largelybecause the methods used to modify the cor-onary circulation necessitated either the di-rect approach of opening the chest for coro-nary ligation or einbolization, or the indirectapproach of injecting einbolizing particlesthrough an aortic catheter in the vicinity ofthe coronary ostia. Although the latter pro-cedure may be performed in animals Avithoutopening the thorax, it not only lacks selec-tivity of distribution of the einbolizing par-ticles in the coronary vascular bed, but spillsa considerable share of the emboli into thesystemic, circulation.
The method we have used in the presentstudy circumvents previous difficulties be-cause it. permits us to eatheterize selectivelyindividual coronary arteries7 without openingthe chest or interfering with perivaseularnerves and to inject embolizing agents intospecific coronary vascular beds.
Methods
AVe studied 2-t adult mongrel dogs (20 to 25Kg.), anesthetized with morphine (3 ing./.Kg1.)and 0.25 nil./Kg. of a combination of equal vol-umes of Dial-uretliane solution (100 and 400 ing./ml., respectively) and of pentobarbital sodium (60mg./ml.).
From the Cardiovascular Research Institute, Uni-versity of California Medical Center, San Francisco,California.
Supported in part by tlio Morabito .Fund and byGrunt H-4029 from the U. S. Public Health Serviceto the Cardiovascular Besearch Institute, Universityof California Medical Center, San Francisco,California.
Received for publication October 20, 1961.
746
We placed n no. 7, S, or 9 double lumen cardiaccatheter in the right heart (via n jugular vein)for measurement of pulmonary arterial pressureand another in the left heart (via a femoralartery) for measurement of left ventricular andleft a trial pressures. We measured cardiac outputby injecting >T 1S24 dye into the pulmonary arterywhile measuring continuously, with a recordingdensitometer, the concentration of dye in bloodwithdrawn through a plastic tube in the aortas;the latter also served for measurement of systemicarterial blood pressure. We calculated total pe-ripheral resistance by dividing mean aortic pres-sure in nun. Hg by the cardiac output in ml./min.We used Stntham strain gauges attached to amultichannel photographic recorder (Electronicsfor Medicine) for pressure recording and recordedthe electrocardiogram continuously using a pre-cordial lead (A73). We catheterized the anteriordescending branch of the left coronary arteryunder fluoroscopic guidance, using n special coro-nary artery catheter, previously described.7 Weverified the position of the catheter by injectinga radiopaque substance (Cardiografin) into thecatheter. There was no oleetrocardiographie evi-dence of coronary insufficiency following the inser-tion of the catheter. The embolizing agents usedwere one per cent suspension (in saline) of lveo-podium spores or of glass mierospheres. The sizesof the lycopodium spores and glass mierospheresranged between 30 and 40 /x, as measured withan ocular micrometer under the microscope. Thesuspension was agitated before each injection toinsure an even distribution of the particles. Thedead space of the stopcock-catheter system (1 ml.)was first cleared of its heparinized saline solutionand then 2 nil. of coronary arterial blood wasdrawn into a syringe. The syringe containing theemboli was emptied manually in a period of twoto three seconds and the system immediately flushedwith the 2 ml. of blood. In our early experiments,we used a radiopaque substance rather than bloodto flush the injecting system. We were unable tosee, by fluoroscopy and by cinematography, anyreflux of the contrast substance during the injec-tion, indicating that all or practically all of theembolizing material went into the heart and littleor none into the systemic circulation. To minimizevariation of response.*, ire confined embolicationto the left interior descending brunch, using initialand subsequent doses of 0.2 ml. This amount wasselected because previous experiments have shown
Circulation Research, Volume X, May 19GS
by guest on May 25, 2018
http://circres.ahajournals.org/D
ownloaded from
CARDIOGENIC SHOCK 747
NO 410j » i co..i-8L/-.
continued.
^JJAJJUW
FIGURE 1
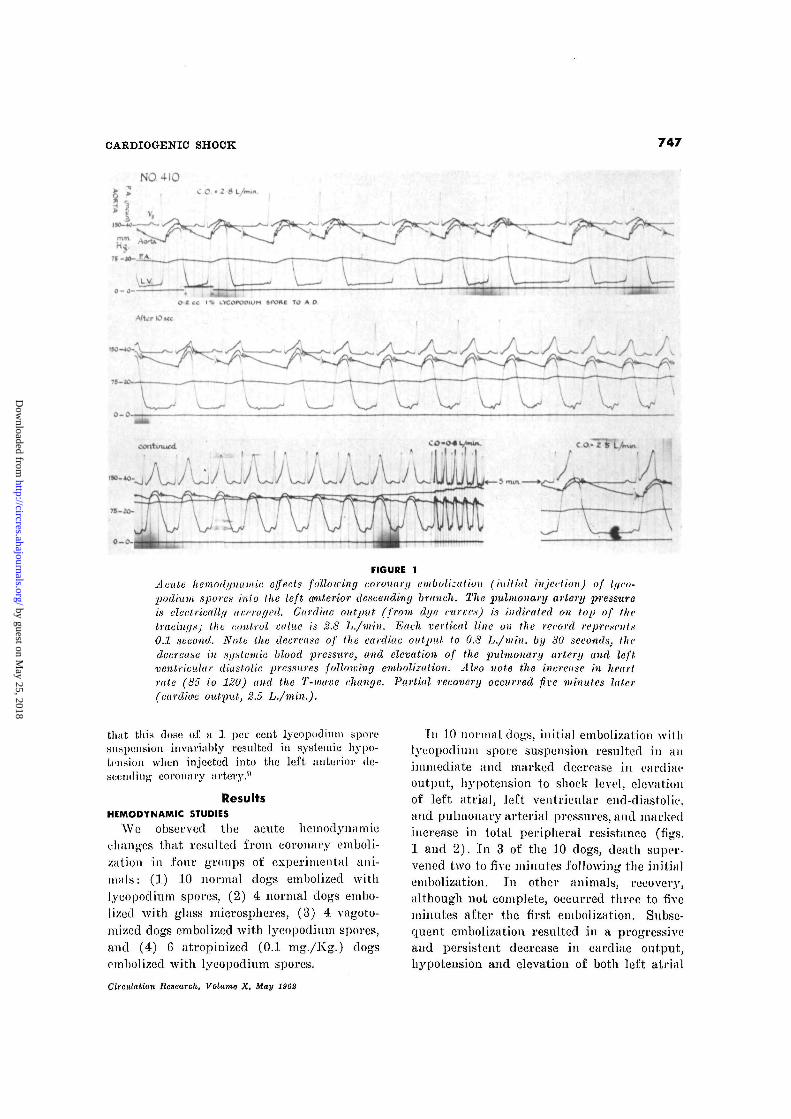
Acute hemodyuainic effects following coronary emboli.:ation (initial injection) of It/co-podium spores inio the left anterior descending branch. The pulmonary artery pressureis electrically av.craged. Cardiac output (from dye curves) is indicated on top of thetracings; the control value is 2.8 L./min. Each vertical line on the record represents0.1 second. Note the decrease of the cardiac output to 0.8 L./min. by 30 seconds, thedecrease in systemic blood, pressure, and elevation of the pulmonary artery and leftventricular diastolic pressures folloiuing embolization. Also note the increase in heartrale (85 io 120) and the T-wave change. Partial recovery occurred five minutes later(cardia'c output, 2.5 L./min.).
tlij11 this tlos<; of n 1 per cent lyeopodiuin sporesuspension invtmnbly resulted in systemic hypo-tension when injected into the left anterior de-scending coronary artery."
ResultsHEMODYNAMIC STUDIES
We observed the acute hemodynamiechanges that resulted from coronary emboli-zation in four groups of experimental ani-mals: (1) 10 normal dogs embolized withlyeopodiuin spores, (2) 4 normal dogs embo-lized with glass microspheres, (3) 4 vagoto-mized dogs embolized with lyeopodinm spores,and (4) 6 atropinized (0.1 mg./Kg.) dogsemholized with lyeopodinm spores.
In 10 normal dogs, initial embolization withlyeopodiuin spore suspension resulted in animmediate and marked decrease in cardiacoutput, hypotension to shock level, elevationof left atrial, left ventricular end-diastolic,and pulmonary arterial pressures, and markedincrease in total peripheral resistance (figs.1 and 2). In 3 of the 10 dogs, death super-vened two to five minutes following the initialembolization. In other animals, recovery,although not complete, occurred three to fiveminutes after the first embolization. Subse-quent embolization resulted in a progressiveand persistent decrease in cardiac output,hypotension and elevation of both left atrial
Circulation Research, Volume X, May 1B0D
by guest on May 25, 2018
http://circres.ahajournals.org/D
ownloaded from
748 GUZMAN, SWENSON, MITCHELL
NORMAL DOGS (10) ATROPINIZED DOGS (6)
• srsr. BLOOD PRESSURE•* CARO/AC OUTPUT• TOTAL PERIPHERAL RESIST.
\EMBOLIZAT/ON
I | I
0 2 4 v 10 0 2 4TIME IN MINUTES
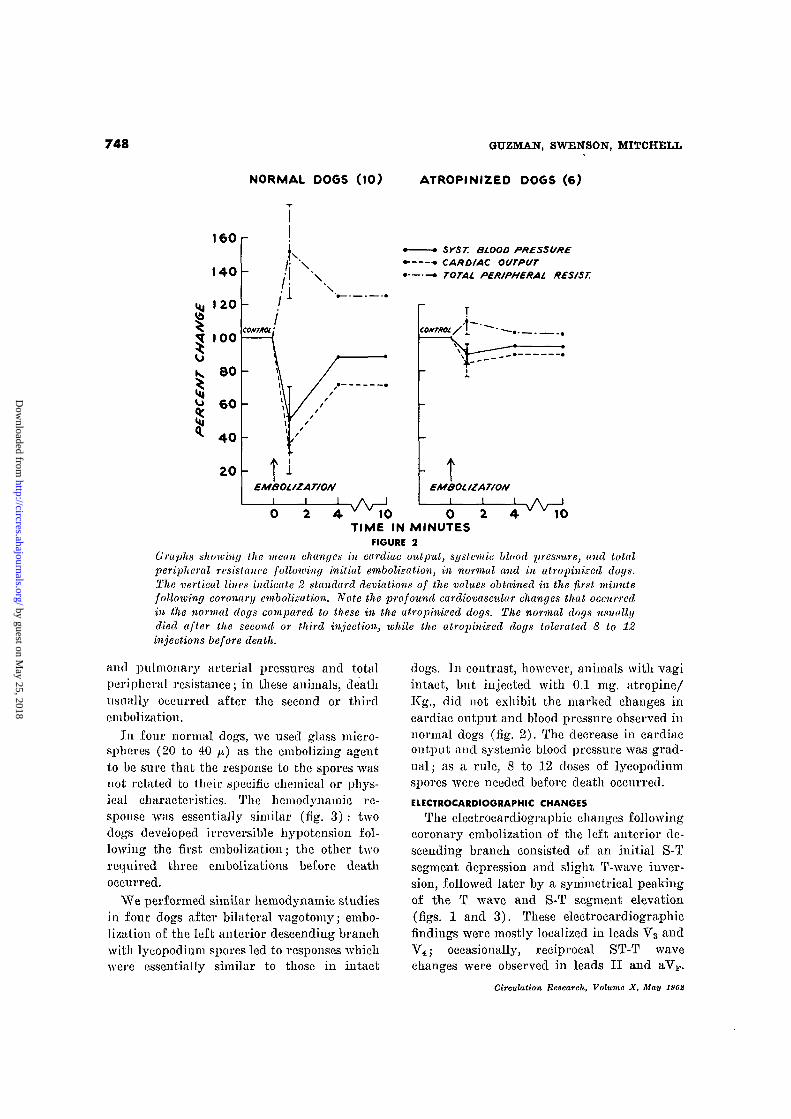
FIGURE 2Graphs showing the mean changes in cardiac output, systemic blood pressure, and totalperipheral resistance following initial embolization, in normal and in alropinized dogs.The vertical lines indicate 2 standard deviations of the values obtained in the first minutefollowing coronary embolization. Note the profound cardiovascular changes that occurred,in the normal dogs compared to these in the atropinized dogs. The normal dogs usuallydied after the second or third injection, ivhile the atropinized dogs tolerated 8 to 12injections before death.
and pulmonary arterial pressures and totalperipheral resistance; in these animals, deathusually occurred after the second or thirdembolization.
In four normal dogs, we used glass micro-spheres (20 to 40 ix) as the embolizing agentto be sure that the response to the spores wasnot related to their specific chemical or phys-ical characteristics. The hemodynamic re-sponse was essentially similar (fig. 3) : twodogs developed irreversible hypotension fol-lowing the first embolization; the other tworequired three enibolizations before deathoccurred.
We performed similar hemodynamic studiesin four dogs after bilateral vagotomy; embo-lization of the left anterior descending branchwith lycopodium spores led to responses whichwere essentially similar to those in intact
dogs. In contrast, however, animals with vagiintact, but injected with 0.1 mg. atropine/Kg., did not exhibit the marked changes incardiac output and blood pressure observed innormal dogs (fig. 2). The decrease in cardiacoutput and systemic blood pressure was grad-ual; as a rule, 8 to 12 doses of lycopodiumspores were needed before death occurred.ELECTROCARDIOGRAPHS CHANGES
The electrocardiographic changes followingcoronary embolization of the left anterior de-scending branch consisted of an initial S-Tsegment depression and slight T-wave inver-sion, followed later by a symmetrical peakingof the T wave and S-T segment elevation(figs. 1 and 3). These electrocardiographicfindings were mostly localized in leads Vg andV4; occasionally, reciprocal ST-T wavechanges were observed in leads II and aVF.
Circulation Research, Volume X, May 19G2
by guest on May 25, 2018
http://circres.ahajournals.org/D
ownloaded from
OARDIOOENIC SHOCK 749
NO. 63
O- O-SA•2ec I v d * <SL/«S MICROSPHER.E5
(30,-) To A.D.
••'-/-«
*0O- 5O-«.5S«c*
I ZMil
FIGURE 3
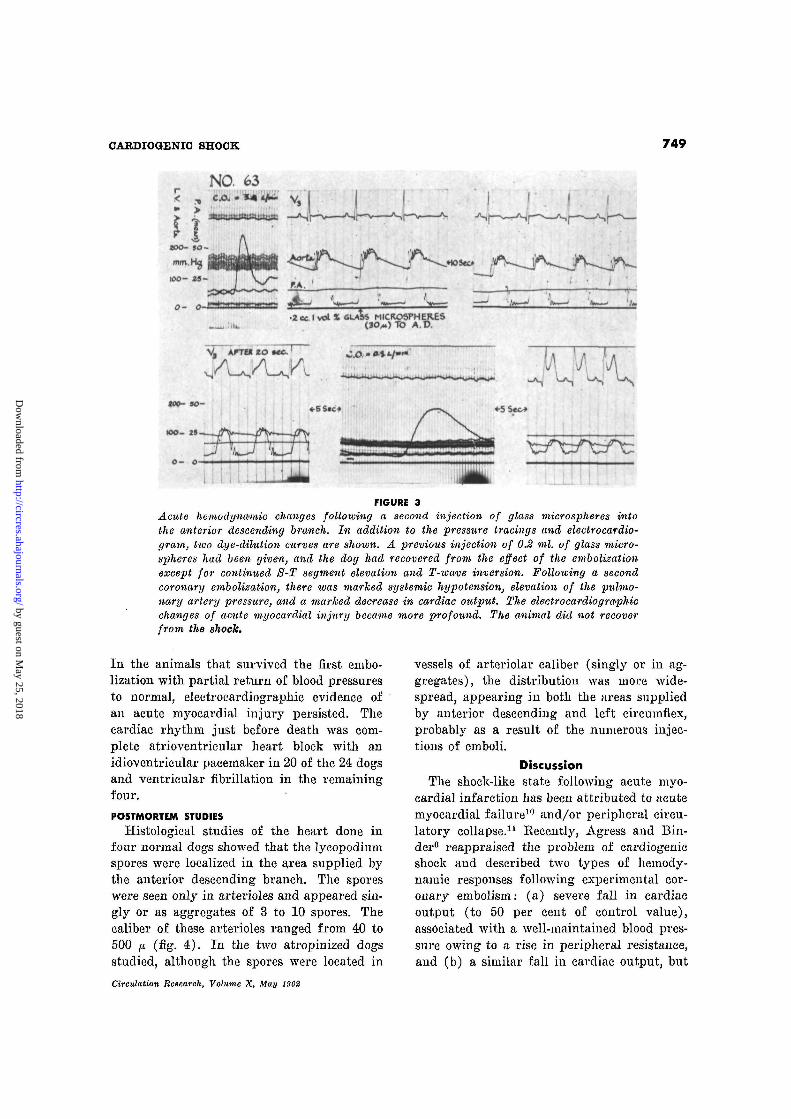
Acute hemodyna/mic changes following a second injection of glass microspheres intothe anterior descending branch. In addition to the pressure tracings and electrocardio-gram, two dye-dilution curves are shown. A previous injection of 0.2 ml. of glass micro-spheres had been given, and the dog had recovered from the effect of the embolizationexcept for continued S-T segment elevation and T-wame inversion. Folloioing a secondcoronary embolization, there was marked systemic hypotension, elevation of the pulmo-nary artery pressure, and a marked decrease in cardiac output. The electrocardiographschanges of acute myocardial injury became more profound. The animal did not recoverfrom the shock.
In the animals that survived the first embo-lization with partial return of blood pressuresto normal, electrocardiographs evidence ofan acute myocardial injury persisted. Thecardiac rhythm just before death was com-plete atrioventricular heart block with anidioventricular pacemaker in 20 of the 24 dogsand ventricular fibrillation in the remainingfour.
POSTMORTEM STUDIES
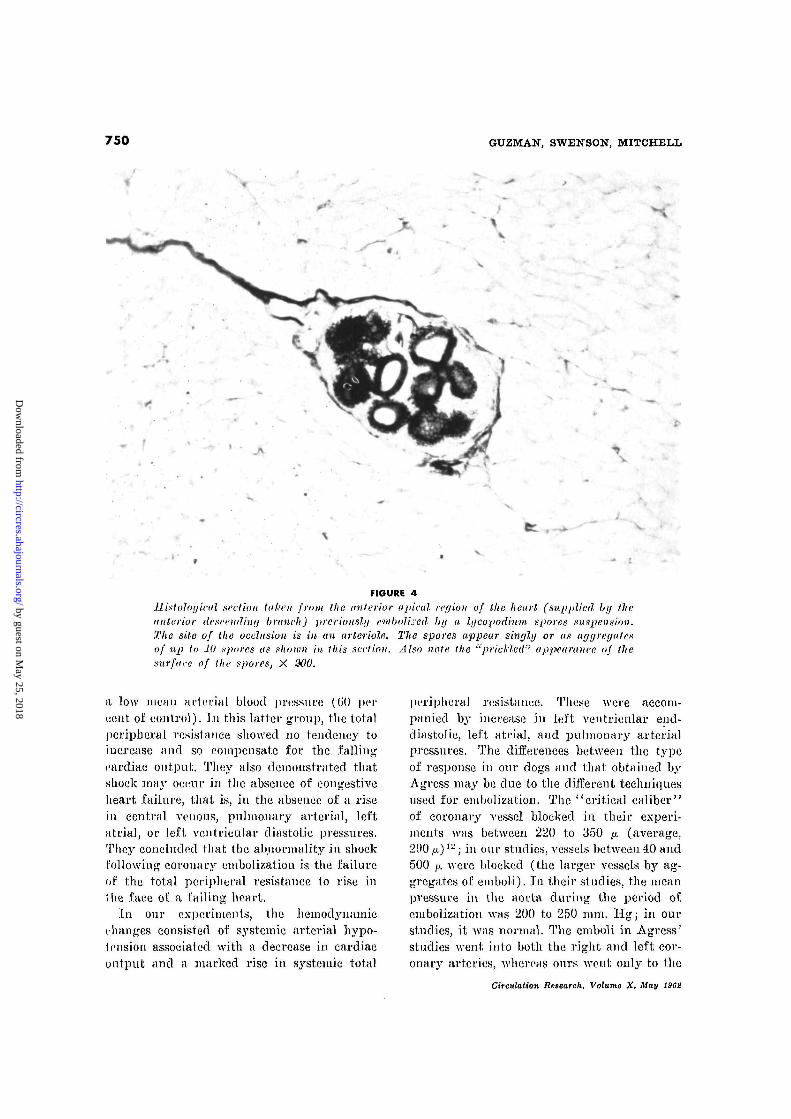
Histological studies of the heart done infour normal dogs showed that the lycopodiumspores were localized in the area supplied bythe anterior descending branch. The sporeswere seen only in arterioles and appeared sin-gly or as aggregates of 3 to 10 spores. Thecaliber of these arterioles ranged from 40 to500 JX (fig. 4). In the two atropinized dogsstudied, although the spores were located in
vessels of arteriolar caliber (singly or in ag-gregates), the distribution was more wide-spread, appearing in both the areas suppliedby anterior descending and left circumflex,probably as a result of the numerous injec-tions of emboli.
DiscussionThe shock-like state following acute myo-
cardial infarction has been attributed to acutemyocardial failure10 and/or peripheral circu-latory collapse.11 Recently, Agress and Bin-der6 reappraised the problem of cardiogenicshock and described two types of hemody-namic responses following experimental cor-onary embolism: (a) severe fall in cardiacoutput (to 50 per cent of control value),associated with a well-maintained blood pres-sure owing to a rise in peripheral resistance,and (b) a similar fall in cardiac output, but
Circulation Research, Volume X, May 1962
by guest on May 25, 2018
http://circres.ahajournals.org/D
ownloaded from
750 GUZMAN, SWENSON, MITCHELL
FIGURE 4
Jlinloloylml section taken from the (interior apical region of the heart (supplied by theanterior descending branch) previously enibolised by a lycopodium spores suspension.The site of the occlusion is in an arteriole. The spores appear singly or as agyreyatesof up to 10 spores as shown in this section. Also note the "prickled" appearance of thesurface of the spores, X 300.
a low mean arterial blood pressure (G'O percent of control). In this latter group, the totalperipheral resistance showed no tendency toincrease and so compensate for the fallingcardiac output. They also demonstrated thatshock may occur in the absence of congestiveheart failure, that is, in the absence of a risein central venous, pulmonary arterial, leftatrial, or left ventricular diastolic pressures.They concluded that the abnormality in shockfollowing coronary embolizatiou is the failure(if the total peripheral resistance to rise inI lie face of a failing heart.
In our experiments, the hemodj'namicchanges consisted of systemic arterial hypo-tension associated with a decrease in cardiacoutput and a marked rise in systemic total
peripheral resistance. These were accom-panied by increase in left ventricular end-diastolic, left atrial, and pulmonary arterialpressures. The differences between the typeof response in our dogs and that obtained byAgress may be due to the different techniquesused for embolization. The "critical caliber"of coronary vessel blocked in their experi-ments was between 220 to 350 JX. (average,290 ix)v-; in our studies, vessels between 40 and500 fji. were blocked (the larger A'essels by ag-gregates of emboli). In their studies, the meanpressure in the aorta during the period ofembolization was 200 to 250 mm. Hg; in ourstudies, it was normal. The emboli in Agress'studies went into both the right and left cor-onary arteries, whereas ours Avent only to the
Circulation Research, Volume X. May 1962
by guest on May 25, 2018
http://circres.ahajournals.org/D
ownloaded from

CARDIOGENIC SHOCK 751
distribution of the left anterior descendingcoronary artery. Finally, almost 50 per centof: their etnboli went to vessels in the skin ormuscles where they may have produced me-chanical, block or reflex changes in vascularcaliber. In our experiments, the embolizingparticles were introduced directly into theleft anterior descending branch and radiologi-cal observations indicated that none of the in-jected material spilled into the systemiccirculation.
Atropine modified the hemodynamie re-sponse following coronary embolization. Onepossible explanation relates to the knownblocking effects of atropine on the parasympa-tlietic nervous system; if embolization of onebranch of a coronary artery leads to vagallymediated vasoconstriction in other branches,atropine could block such vasoconstriction.Tliis would mean that shock and death wouldoccur in the atropinized dogs only after muchof the total coronary circulation was mechan-ically blocked by reflux of emboli from thebranch into which the particles were directed.In the nonutropinized dogs, spores andspheres were found only in the distributionof the injected vessels, while in the atro-pinized dogs, spores were found in bothbranches of the left coronary artery. How-ever, the dogs did not benefit from bilateralvagotomy; this means that if reflexes were infact involved, they could not be mediatedthrough either the afferent or efferent cervicalvagus fibers. This leaves us with the possibil-ity that a local axone or intercoronary reflexis involved which might be blocked by atro-pine but not by cervical vagotomy. It is ofcourse possible that an action of atropineother than its postganglionic parasympatheticblocking effect is involved; atropine mayblock certain cells in autonomic ganglia, al-though our understanding of this effect islimited.13
The coronary ehemoreflex14 does not appearto be involved in the production of hypoten-sion. Activation of it by emboli (or by bloodclots forming about emboli) should lead tobradycardia and systemic vasodilatation;neither was observed. It would be of interest
to determine whether the cat (a species inwhich the coronary chemoreflex is activatedpowerfully by minute doses of serotonin)behaves differently in this respect from theclog (in which serotonin fails to elicit thisresponse).
CLINICAL CONSIDERATIONS
We believe that it is unwise to transfer dataobtained by a specific type of selective coro-nary artery embolization in anesthetized dogsto a variety of types of coronary insufficiencyin unanesthetized man in whom atheroscle-rotic obstruction, thrombi, or emboli might bethe critical etiological factor. However, wedo wish to emphasize certain of our findingsin the hope that they may stimulate furtherclinical investigations.
1. The hypotension was caused by a decreasein cardiac output, and the latter appeared tobe out of proportion to the amount of coro-nary vascular bed selectively blocked. Thissuggests that either reflex coronary vasocou-strietion occurred or that myocardial contrac-tility was inhibited. Coronary angiographicstudies, to be reported separately, suggest: thatembolization of one branch of a coronaryartery does in fact produce at least temporarynarrowing of other nonembolized coronaryvascular beds. Even if this caused or con-tributed to systemic hypotension only briefly,serious damage to the myocardium in generalmight occur in this period. For this reason,the use of agents capable of blocking reflexesshould be considered.
2. Le Roy et al.ir' noted that the incidenceof ventricular fibrillation following ligationof the left anterior descending coronaryartery was diminished considerably followingatropinization. They suggested that ligatiouof a coronary artery induced a reflex vaso-constriction of the unaffected coronary artery,leading to fatal ventricular fibrillation. Ourstudies in the dog suggest that: atropine doeshave some action which minimizes the cardio-vascular changes following embolization. Webelieve that the use of atropine in myocardialinfarction in man deserves further cautiousstudy, especially if it can be given as soou
Circulation Research, Volume X, May 1962
by guest on May 25, 2018
http://circres.ahajournals.org/D
ownloaded from
752 GUZMAN, SWENSON, MITCHELL
as a diagnosis is established, and before shockhas occurred.
SummaryThe acute hemodynamic changes that result
from coronary embolization were studied inthe intact dog. Coronary embolization withlycopodium spore suspension resulted in animmediate and marked decrease in cardiacoutput, hypotension to shock level, elevationof pulmonary arterial and left atrial pres-sures, and marked increase in total peripheralresistance. These profound hemodynamic re-sponses were partially blocked in dogs pre-viously atropinized. The therapeutic implica-tions of the results Avere discussed.
AcknowledgmentWe wish to express our gratitude to Dr. Julius
H. Comroe, Jr. for his advice and encouragement inthis work, and to Dr. Robert Wright of the Depart-ment of Pathology for doing the postmortem studiesof the heart.
References1. ORIAS, 0.: Dynamic changes in the ventricle
following ligation of the ramus descendensanterior. Am. J. Physiol. 100: 629, 1932.
2. GROSS, L., MENDLOWITZ, M., AND SCHAUER, G.:Hemodynamic studies in experimental coronaryocclusion. Am. Heart J. 13: 647, 1937.
3. MANNING, G. W., MCEACHERN, G. G., AND HALL,G. E.: Reflex coronary artery spasm followingsudden occlusion of other coronary branches.Arch. Int. Med. 64: 661, 1939.
4. WEGRIA, B., FRANK, C. W., MISRAHT, G. A.,WANT, H. E., MILLER, B., AND CASE, R. B.:
Immediate hemodynamic effects of acute coro-nary artery occlusion. Am. J. Physiol. 177:123, 1954.
5. TAYLOR, C. B., DAVIS, C. B., VAWTEK, G. F.,
AND HASS, G. M.: Controlled myocardial injuryproduced by a hypothermia method. Circulation3: 239, 1951.
6. AGRESS, C. M., AND BINDER, M. J.: Cardiogenic
shock. Am. Heart J. 54: 458, 1957.7. WEST, J. W., KOBAYASHI, T., AND GUZMAN,
S. V.: Coronary catheterization in the intactdog. Circulation Research 6: 383, 1958.
8. NICHOLSON, J. W., I l l , BURCHELL, H. B., AND
WOOD, E. H.: Method for continuous recordingof Evan's blue dye curves in arterial blood.J. Lab. & Clin. Med. 37: 353, 1951.
9. GUZMAN, S. V., WEST, J. W., AND BELLET, S.:
Increase in myocardial contractility as a fac-tor in the treatment of cardiogenie shock(abstr.). Circulation 14: 947, 1956.
10. BOTER, N. H.: Cardiogenic shock. New EnglandJ. Med. 230: 226, 1944.
11. FlSHBERG, A. M. HlTZIG, W. M., AND KING,
F. H.: Circulatory dynamics in myocardialinfarction. Arch. Int. Med. 54: 6, 1934.
12. JACOBS, H. I., ROSEN, V., AND AGRESS, C. M.:
Further evidence for a critical vessel caliberin experimental coronary shock. CirculationResearch 1: 466, 1953.
13. ROSZKOWSKI, A. F. : Unusual pressor agent.Pharmacologist 2: 73, 1960.
14. DAWES, G. S., AND COMROE, J. H.: Chemoreflexesfrom the heart and lungs. Physiol. Rev. 2:167, 1954.
15. LE ROY, G. V., FENN, G. K., AND GILBERT, N. C.:
Influence of xanthine drugs and atropine onthe mortality rate after experimental occlu-sion of a coronary artery. Am. Heart J.23: 637, 1942.
Circulation Research, Volume X. May 196S
by guest on May 25, 2018
http://circres.ahajournals.org/D
ownloaded from
Santiago V. Guzman, Edward Swenson and Robert MitchellMechanism of Cardiogenic Shock
Print ISSN: 0009-7330. Online ISSN: 1524-4571 Copyright © 1962 American Heart Association, Inc. All rights reserved.is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Circulation Research
doi: 10.1161/01.RES.10.5.7461962;10:746-752Circ Res.
http://circres.ahajournals.org/content/10/5/746World Wide Web at:
The online version of this article, along with updated information and services, is located on the
http://circres.ahajournals.org//subscriptions/
is online at: Circulation Research Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer about this process is available in the
located, click Request Permissions in the middle column of the Web page under Services. Further informationEditorial Office. Once the online version of the published article for which permission is being requested is
can be obtained via RightsLink, a service of the Copyright Clearance Center, not theCirculation Research Requests for permissions to reproduce figures, tables, or portions of articles originally published inPermissions:
by guest on May 25, 2018
http://circres.ahajournals.org/D
ownloaded from