mchip/zimbabwe ldhf and intensive mentorship: improving practice and patient outcomes in zambia...
TRANSCRIPT
MCHIP/ZIMBABWELDHF and Intensive Mentorship: Improving Practice and Patient Outcomes in Zambia
Presenter: Samantha HolcombeMarch 2, 2015

Background
Commenced 1st October 2011 End date 30th June 2014 In-country partners:
Jhpiego – Maternal Health Save the Children – Newborn Health
Context: Key clinical implementing partner of USG-led Saving Mothers, Giving Life endeavor (end date September 2017)
2
Saving Mothers, Giving Life
Conceived as 1-year, USG-led endeavor to reduce maternal mortality by 50% in 4 districts in Zambia→ Now, 5-years, 8+ districts
Interventions focus on labor/delivery and immediate post partum period Service delivery (EmONC) Facility infrastructure (labor wards, MWHs) Emergency transport Demand creation (facility deliveries)
3
Target Districts
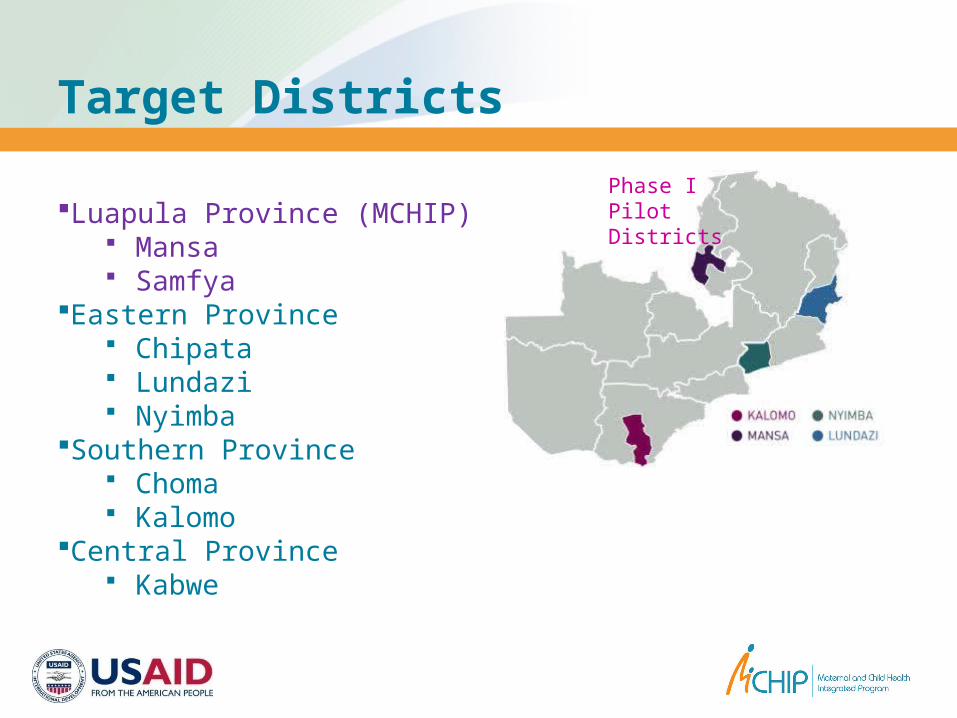
Luapula Province (MCHIP) Mansa Samfya
Eastern Province Chipata Lundazi Nyimba
Southern Province Choma Kalomo
Central Province Kabwe
Phase I Pilot Districts
1) Increase the quality of labor/delivery and postpartum/postnatal care services in MOH facilities in SMGL Districts
2) Build capacity of MOH facilities in Mansa District to increase uterotonic coverage through use of AMTSL in facilities and through distribution of misoprostol for home birth
3) Expand the availability of quality post-partum family planning services in MOH facilities in Mansa District
5
MCHIP/Country Objectives
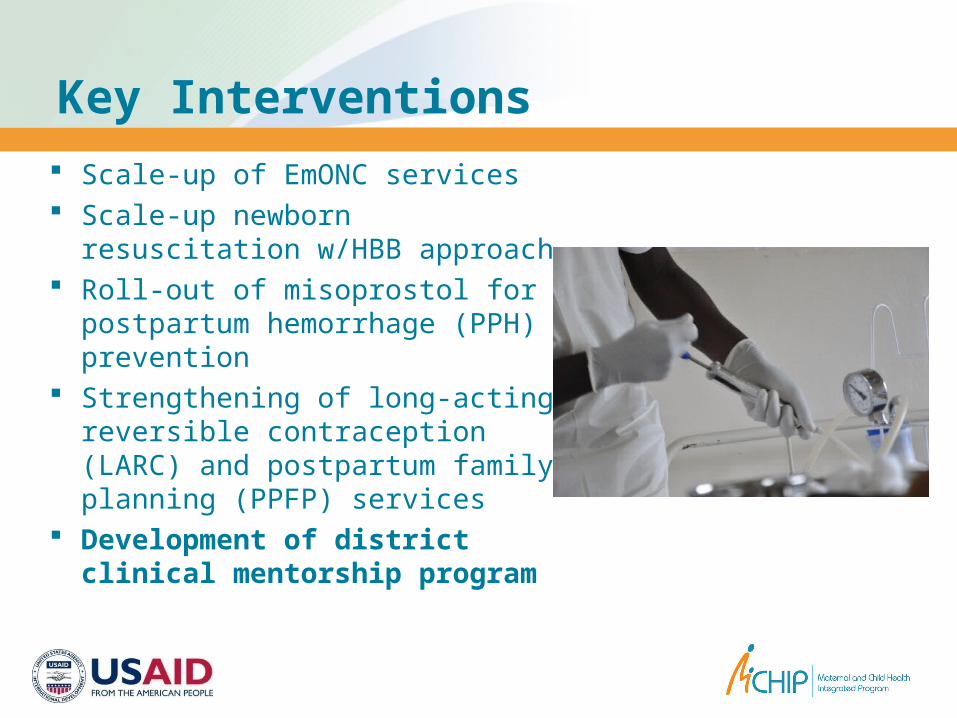
Key Interventions Scale-up of EmONC services Scale-up newborn resuscitation
w/HBB approach Roll-out of misoprostol for
postpartum hemorrhage (PPH) prevention
Strengthening of long-acting reversible contraception (LARC) and postpartum family planning (PPFP) services
Development of district clinical mentorship program
Purpose
To build the capacity of MOH and partner staff in SMGL districts to conduct targeted, clinical, on-site mentorship in EmONC, reinforcing practical knowledge and skills, to ensure that clients receive high-quality, improved services which will help reduce both maternal and child mortality
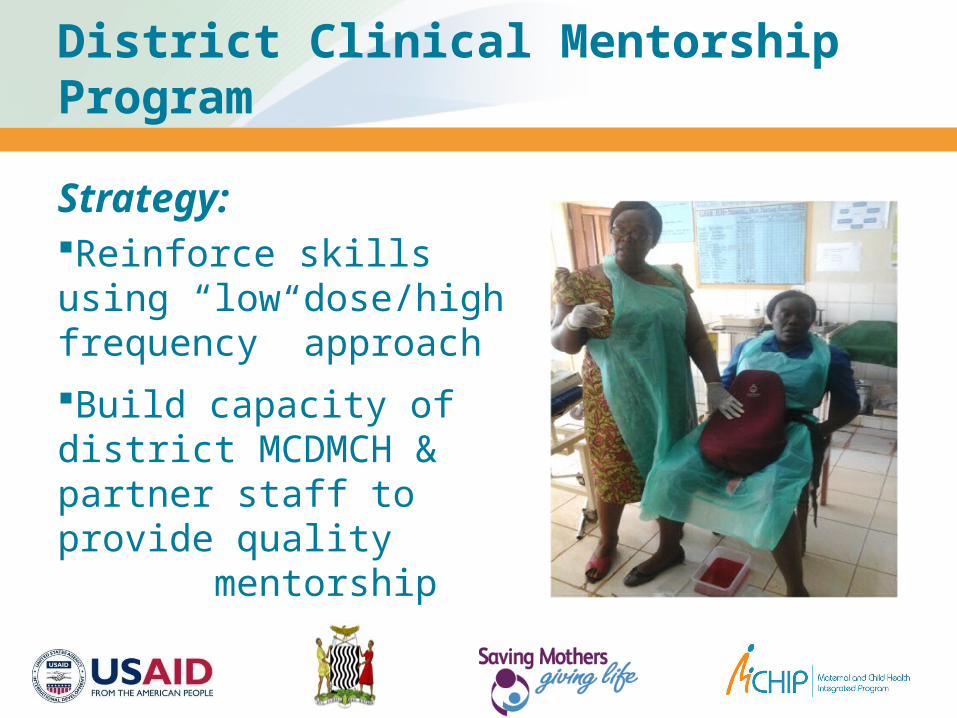
District Clinical Mentorship Program
Strategy:Reinforce skills using “low dose/high frequency” approach
Build capacity of district MCDMCH & partner staff to provide quality mentorship

Mentorship ApproachEstablishing Mentors
1 week clinical mentorship training, including skills update and on-site clinical practicum
16–20 mentor trainees recruited, including the DMO, DNO, SMGL Coordinator, staff from hospitals and large UHCs, and MCHIP and other maternal health implementing partner staff

Facility Visits
Mentors divided into teams of 2-3 persons with diverse clinical expertise
All facilities visited monthly by mentorship team for at least one full day
Mentor teams arrive in morning and help service clients, taking the opportunity for mentorship with any maternity/newborn clients and freeing health care providers’ time for mentorship in the afternoon
Facility Visits
Review files and registers Targeted technical assistance
Identify any challenges encountered with EmONC service delivery
Refer to previous month’s action plan Mentor on focus EmONC function Assess providers’ skill competency on anatomic
models or with clients using skills checklists Mentors fill out report form for DCMO and
MCHIP, develop an action plan to be completed before next month’s mentorship visit
Benefits of Mentorship
Low-cost intervention Can maximize benefits of
complementary, higher-cost interventions Opportunity for building more
sustainable, local capacity Provides clinical support and long-term
morale Addresses site-specific unique challenges
faced by health staff
Outcomes
Immediate and sustained application of skills learned during EmONC training;
Improved provider confidence and morale;
Management of complications at rural health center level that previously were referred to other facilities
Reduced pressure on emergency transport systems and referral facilities
Improved outcomes for pregnant women
Key Achievements
In Mansa Y6 Q2, 100% of pre-eclampsia cases and 95% of PPH cases were treated according to clinical guidelines
From baseline to Y6 Q2, use of the partograph increased from 6 to 45 percent
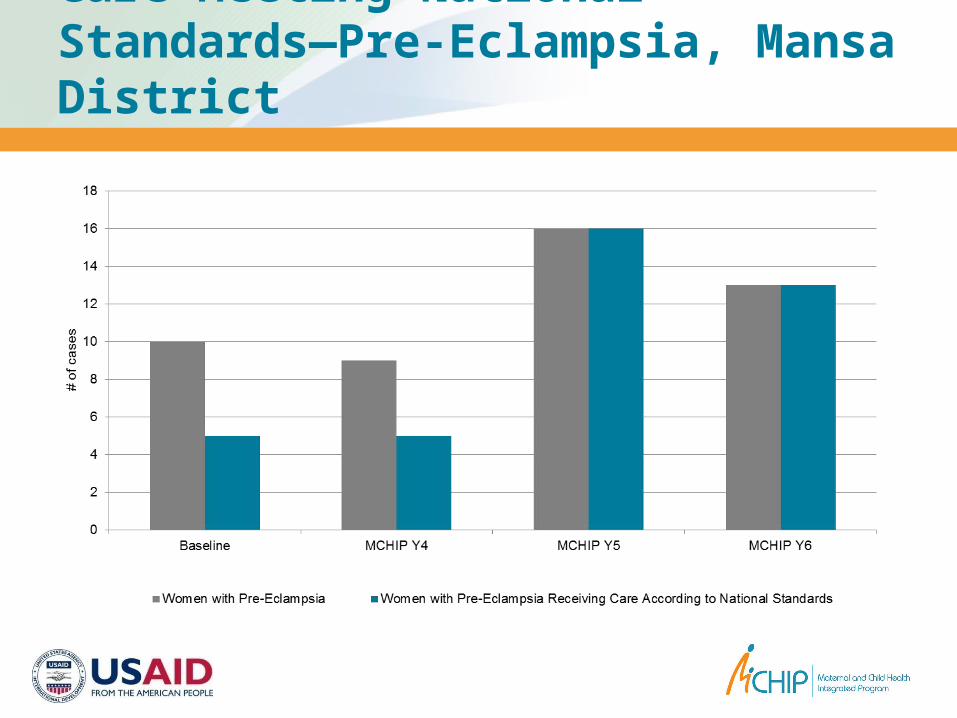
Care Meeting National Standards—Pre-Eclampsia, Mansa District
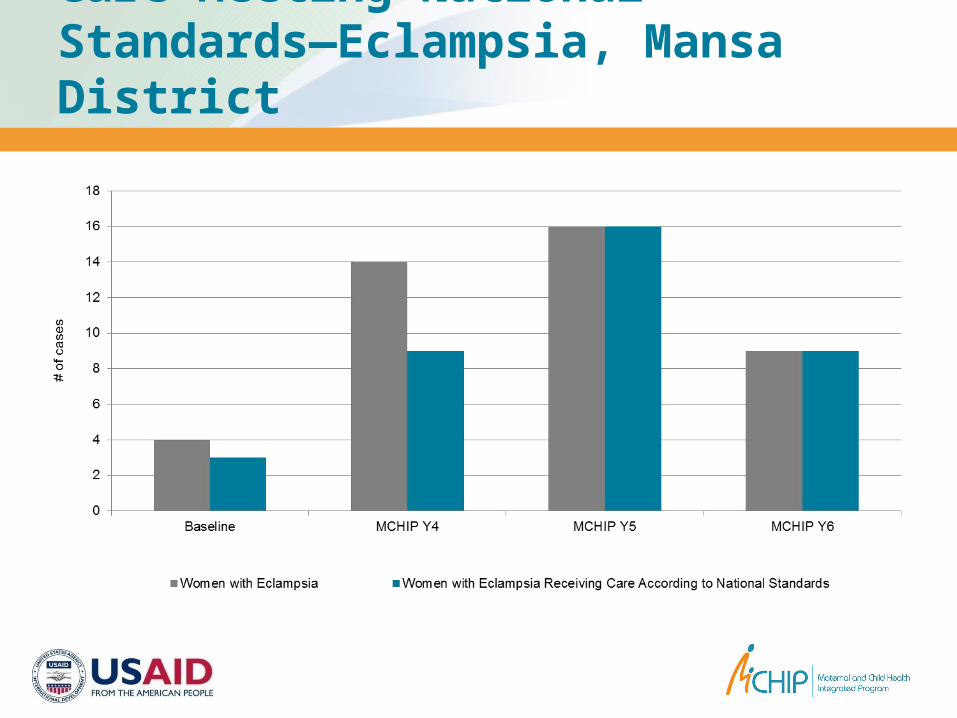
Care Meeting National Standards—Eclampsia, Mansa District
Keys to Success
Strong ownership by the local DCMO Diverse partner involvement and
collaboration Proper training in mentorship skills Use of anatomic models for on-site
clinical simulations Ongoing assessment of providers’
EmONC skills even in the absence of live client cases
Lessons Learned
Mentors’ clinical skills should be routinely assessed
Simple, user-friendly tools help to ensure program success
Monthly targeting of specific EmONC skills with anatomic models ensures skills remain sharp
Peer mentorship through facility exchange visits is critical and can significantly improve service delivery

Video
https://www.youtube.com/watch?v=5-1qY8IzF1o&feature=youtu.be

Twatotela!
20