maxillary sinus hemangioma: usefulness of …maxillary sinus hemangioma: usefulness of embolization...
TRANSCRIPT
B
C
Me
Hc
HS
a
b
c
RA
I
Hlfahcomfaew
m
Tun
O
h1a
raz J Otorhinolaryngol. 2017;83(4):490---493
www.bjorl.org
Brazilian Journal of
OTORHINOLARYNGOLOGY
ASE REPORT
axillary sinus hemangioma: usefulness ofmbolization according to classification�
emangioma de seio maxilar: utilidade da embolizacão de acordo com alassificacão
isashi Hasegawaa, Hiroumi Matsuzakia,∗, Tohru Furusakaa, Takeshi Oshimaa,hinobu Masudab, Toshiyuki Unnoc, Osamu Abec
Nihon University School of Medicine, Department of Otorhinolaryngology, Head and Neck Surgery, Tokyo, JapanNihon University School of Medicine, Department of Pathology, Tokyo, JapanNihon University School of Medicine, Department of Radiology, Tokyo, Japan
C
A
C
AbsscsawimSat
eceived 19 June 2015; accepted 12 September 2015vailable online 17 December 2015
ntroduction
emangioma in the nose and nasal sinuses is rare,1 particu-arly in the maxillary sinus.2 Differentiation of hemangiomarom malignant tumors is important, because both may beccompanied by bone destruction. With regard to giantemangioma, this type has a rich blood supply, and surgi-al treatment requires particular care due to the high riskf massive bleeding and obstructed field of view. Althoughaxillary sinus hemangioma has been sporadically reported,
ew reports have described cases of this type diagnosedccording to the 1996 classification of the International Soci-ty for the Study of Vascular Anomalies (ISSVA) and treatedith arterial embolization.
Here, we report three cases of massive sinonasal hea-angioma that were resected after arterial embolization.
� Please cite this article as: Hasegawa H, Matsuzaki H, Furusaka, Oshima T, Masuda S, Unno T, et al. Maxillary sinus hemangioma:sefulness of embolization according to classification. Braz J Otorhi-olaryngol. 2017;83:490---3.
∗ Corresponding author.E-mail: [email protected] (H. Matsuzaki).Peer Review under the responsibility of Associacao Brasileira detorrinolaringologia e Cirurgia Cervico-Facial.
ttwt
ttp://dx.doi.org/10.1016/j.bjorl.2015.09.002808-8694/© 2015 Associacao Brasileira de Otorrinolaringologia e Cirurgiccess article under the CC BY-NC-ND license (http://creativecommons.
ase report
n overview of the three cases is shown in Table 1.
ase 1
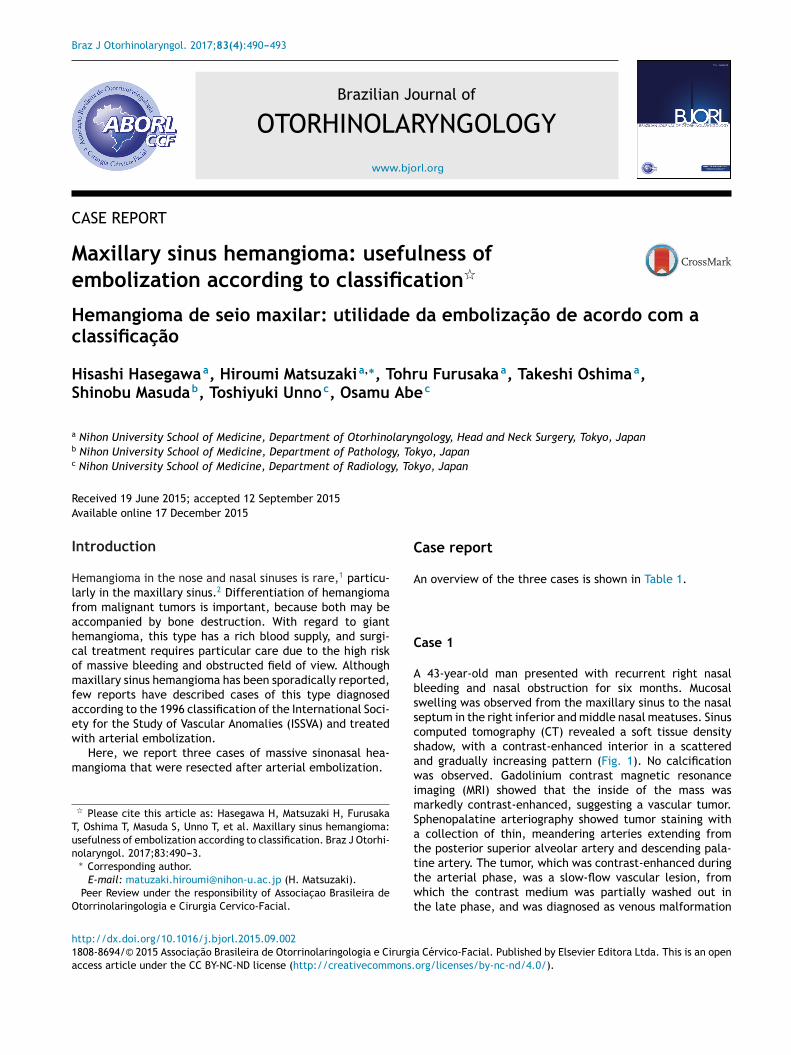
43-year-old man presented with recurrent right nasalleeding and nasal obstruction for six months. Mucosalwelling was observed from the maxillary sinus to the nasaleptum in the right inferior and middle nasal meatuses. Sinusomputed tomography (CT) revealed a soft tissue densityhadow, with a contrast-enhanced interior in a scatterednd gradually increasing pattern (Fig. 1). No calcificationas observed. Gadolinium contrast magnetic resonance
maging (MRI) showed that the inside of the mass wasarkedly contrast-enhanced, suggesting a vascular tumor.
phenopalatine arteriography showed tumor staining with collection of thin, meandering arteries extending fromhe posterior superior alveolar artery and descending pala-
ine artery. The tumor, which was contrast-enhanced duringhe arterial phase, was a slow-flow vascular lesion, fromhich the contrast medium was partially washed out inhe late phase, and was diagnosed as venous malformation
a Cervico-Facial. Published by Elsevier Editora Ltda. This is an openorg/licenses/by-nc-nd/4.0/).
Maxillary sinus hemangioma: usefulness of embolization according to classification 491
Table 1 An overview of the three cases.
Case 1 2 3
Age gender 41 y.o. male 43 y.o. female 74 y.o. malePreoperated biopsy Hematoma Necrotic polypoid Nasal mucosaOrigin Lateral wall Upper wall UnknownArtery Posterior superior alveolar
descending palatineInfraorbital dorsal nasal Sphenopalatine deep temporal
Embolic device Micro coil and gelatin sponge Micro coil and gelatin sponge Micro coil and gelatin spongeTechnique ESS and Watsuji---Denker
operationESS and Watsuji---Denker operation ESS and Watsuji---Denker
operationISSVA classification Low flow venous malformation Low flow venous malformation Low flow venous malformation
Bleeding (g) 60 30 100ernou
3
Diagnosis Sinusoidal hemangioma Cav
according to the ISSVA classification. Both arteries were
embolized. Three days later, the patient underwent com-bined surgery with an endoscopic procedure and theWatsuji---Denker operation. Intraoperative blood loss washIh
Figure 1 Enhanced CT in Case 1. Axial (A) and coronal (B) imagesis seen during the arterial phase.
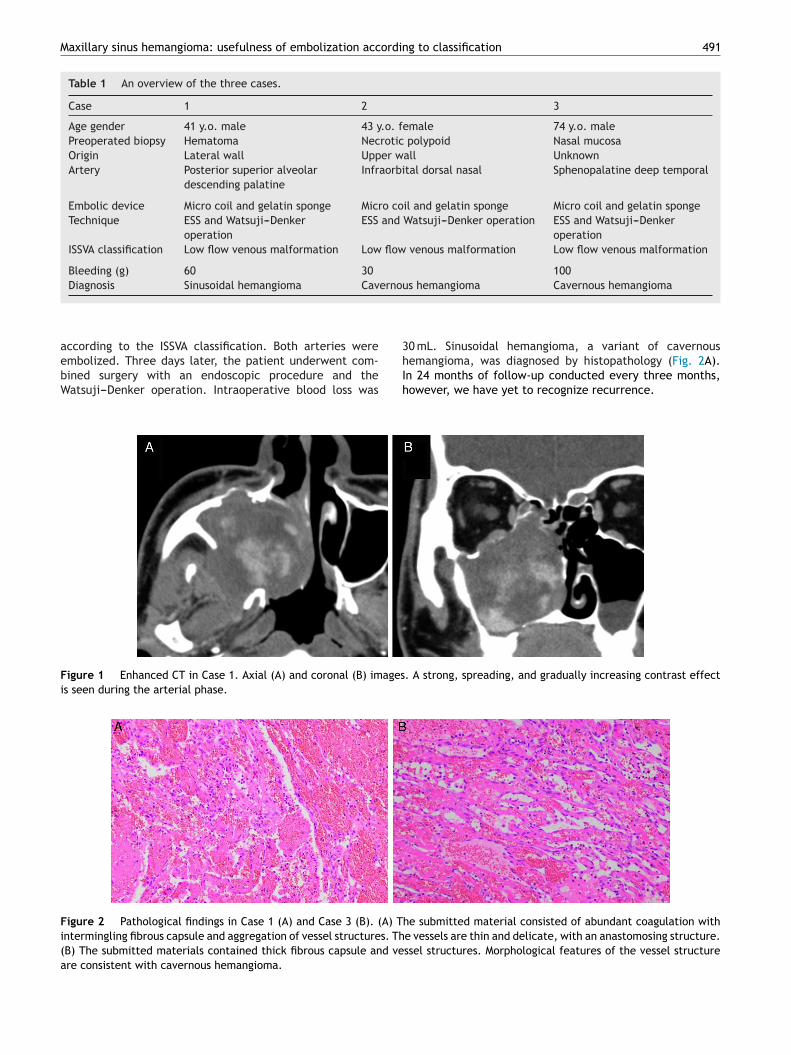
Figure 2 Pathological findings in Case 1 (A) and Case 3 (B). (A) Thintermingling fibrous capsule and aggregation of vessel structures. Th(B) The submitted materials contained thick fibrous capsule and veare consistent with cavernous hemangioma.
s hemangioma Cavernous hemangioma
0 mL. Sinusoidal hemangioma, a variant of cavernous
emangioma, was diagnosed by histopathology (Fig. 2A).n 24 months of follow-up conducted every three months,owever, we have yet to recognize recurrence.. A strong, spreading, and gradually increasing contrast effect
e submitted material consisted of abundant coagulation withe vessels are thin and delicate, with an anastomosing structure.ssel structures. Morphological features of the vessel structure

492 Hasegawa H et al.
Figure 3 Gadolinium-enhanced MRI of Case 2. Axial (A) and coronal (B) images. A heterogeneously enhanced vascular tumor wass
C
AbmClclstset(tssvapplThtr
C
AaeMpooftCcn
tebrtpabsaviuaeo(m
D
Iootnsoroat
iifs1
uspected.
ase 2
41-year-old woman presented with recurrent left nasalleeding and nasal obstruction for a month. Her left com-on nasal meatus was filled with edematous mucosa. SinusT revealed a soft tissue density shadow occupying the
eft maxillary sinus, ethmoid sinus, frontal sinus, and nasalavity, with a bone defect on the medial wall of theeft maxillary sinus. In addition, CT showed a soft tis-ue density shadow including blood retention that filledhe left maxillary sinus. The medial wall of the maxillaryinus showed destruction and was increasingly contrast-nhanced. A 30 mm heterogeneously enhanced vascularumor was suspected, based on gadolinium-enhanced MRIFig. 3). Facial arteriography showed tumor staining fromhe infraorbital artery on the upper wall of the left maxillaryinus, and the artery was embolized. In addition, the dor-al nasal artery was embolized. The tumor was a slow-flowascular lesion, and venous malformation was diagnosedccording to the ISSVA classification. Four days later, theatient underwent combined surgery with an endoscopicrocedure and the Watsuji---Denker operation, and the entireesion was extracted. Intraoperative blood loss was 30 mL.he postoperative pathological diagnosis was cavernousemangioma. In 18 months of follow-up conducted everyhree months, however, we have yet to recognize recur-ence.
ase 3
74-year-old man presented with right nasal bleedingnd nasal obstruction. Two years before, the patient hadxperienced right nasal bleeding lasting a few hours.yelodysplastic syndrome was diagnosed. An edematousolyp occupying the right common nasal meatus wasbserved. Sinus CT showed a soft tissue density shadowccupying the right maxillary sinus, ethmoid sinus, androntal sinus to the left nasal cavity, with bone destruc-
ion on the medial wall of the right maxillary sinus. ContrastT showed a lobulated tumorous lesion that was graduallyontrast-enhanced from the maxillary sinus to the commonasal meatus, as well as microvascular development in thetfrt
umor. Gadolinium-enhanced MRI showed a heterogeneouslynhanced lesion, raising suspicion of a vascular tumor. Tissueiopsy showed only nasal mucosa. External carotid arteriog-aphy showed tumor staining in the area corresponding tohe entire right maxillary sinus. Sphenopalatine arteriogra-hy showed that the infraorbital artery, descending palatinertery, and a number of small medial/lateral posterior nasalranches were involved as feeders. The main trunk of thephenopalatine artery and branches of the deep temporalrtery were embolized (Fig. 4). The tumor was a slow-flowascular lesion diagnosed as venous malformation accord-ng to the ISSVA classification. Four days later, the patientnderwent combined surgery with an endoscopic procedurend the Watsuji---Denker operation, and the entire lesion wasxtracted. Intraoperative blood loss was 100 mL. The post-perative pathological diagnosis was cavernous hemangiomaFig. 2 B). In 18 months of follow-up conducted every threeonths, however, we have yet to recognize recurrence.
iscussion
n a report of 281 cases of hemangioma, 55 percent occurredn the face and extracranial head, and 5 percent occurredn the neck,3 with these lesions only rarely occurring inhe nose or nasal sinuses.1 Of those which do occur in theose and nasal sinuses, about 80 percent occur on the nasaleptum, in Kiesselbach’s area in particular, and 15 percentn the lateral wall of the nasal cavity. Hemangioma occur-ing in the sinus cavity is even rarer. Cavernous hemangiomaccurs far less frequently than capillary hemangioma, usu-lly developing on turbinate bone and rarely on the bonyissue of the maxillary sinus wall.4
Sinusoidal hemangioma,5,6 diagnosed on histopathologyn Case 1, is a markedly rare histological type (Fig. 4) whichs relatively unknown among pathologists. Because only aew cases of sinusoidal hemangioma have been reportedince the initial description by Calonje and Fletcher in991, a clear recognition of the clinicopathological charac-
eristics of this type will avoid diagnostic pitfalls. Patientollow-up has revealed no tendency toward either localecurrence or metastasis5; however, Ciurea et al. reportedhree reoperations for recurrence.7 In our cases, the
Maxillary sinus hemangioma: usefulness of embolization according to classification 493
) anery (
C
TfAdTta
C
T
R
report. Dentomaxillofac Radiol. 2012;41:340---1.10. Song CE, Cho JH, Kim SY, Kim SW, Kim BG, Kang JM. Endoscopic
resection of haemangiomas in the sinonasal cavity. J Laryngol
Figure 4 External carotid arteriography of Case 3. Frontal (Asponding to the entire right maxillary sinus. Sphenopalatine art
preoperative CT showed bone destruction. Given the rar-ity of sinusoidal hemangioma and the possibility that othervascular neoplastic lesions might also be present, a highrisk of local recurrence and metastasis lesions with simi-lar CT and MRI findings, such as hemangiopericytoma andhemangiosarcoma in these cases, cannot be denied.
Hemangioma is commonly diagnosed radiographically,according to the classification adopted at the 1996 ISSVAmeeting. In the ISSVA classification, conventionally diag-nosed hemangiomas are divided into vascular tumors andvascular malformations.8 Vascular malformations, conven-tionally classified as cavernous hemangiomas, do not regressspontaneously and sometimes require treatment when theygradually increase in size. They may be further subdividedinto slow- and fast-flow lesions; fast-flow lesions can betreated with semipermanent and reliable embolization, suchas via micro coils. Knowing the flow speed helps to deter-mine the embolization method and is a useful reference forintravascular treatment.
We considered that our surgical method was effectiveon the basis of two criteria: the low rate of periopera-tive hemorrhage and the reported successful postoperativemanagement. We were able to limit intraoperative bleed-ing to 60 mL, 30 mL, and 100 mL for Cases 1---3, respectively.Further, postoperative bleeding was sufficiently controlledby the placement of gauze tampons. In a previous report, apatient who did not undergo arterial embolization requiredtwo emergency room visits for the treatment of postop-erative bleeding.9 Another study reported that massivesinonasal hemangioma was able to be resected endoscop-ically, albeit with effort, including preoperative arterialembolization and an increase in surgical access to the tumorvia the construction of a control hole at the canine fossa.10
For our three patients, in contrast, we chose the combi-nation of an endoscopic procedure and the Watsuji---Denkeroperation with preoperative arterial embolization, whichfacilitated our investigation and care of the postoperative
lesion.d profile (B) views, showing tumor staining in the area corre-arrow).
onclusion
hese three cases were diagnosed as slow-flow venous mal-ormations, in accordance with the ISSVA classification.ngiography and arterial embolization both aided accurateiagnosis of the primary site and the control of bleeding.hese very rare cases are amenable to relatively rou-ine treatment following careful assessment and a plannedpproach.
onflicts of interest
he authors declare no conflicts of interest.
eferences
1. Fu YS, Perzin KH. Non-epithelial tumors of the nasal cavity,paranasal sinuses, and nasopharynx: a clinicopathologic study.3. Cartilaginous tumors (chondroma, chondrosarcoma). Cancer.1974;34:453---63.
2. Batsakis JG, Rice DH. The pathology of head and neck tumors:vasoformative tumors, part 9A. Head Neck Surg. 1981;3:231---9.
3. Macomber W, Wang M. The hemangioma. GP. 1953;8:41---9.4. Hellquist HB. Pathology of the nose and paranasal sinuses. But-
terworths Editions; 1990.5. Calonje E, Fletcher CD. Sinusoidal hemangioma. A distinctive
benign vascular neoplasm within the group of cavernous heman-giomas. Am J Surg Pathol. 1991;15:1130---5.
6. Jammal H, Barakat F, Hadi U. Maxillary sinus cavernous heman-gioma: a rare entity. Acta Otolaryngol. 2004;124:331---3.
7. Ciurea M, Ciurea R, Popa D, Parvanescu H, Marinescu D, VrabeteM. Sinusoidal hemangioma of the arm: case report and reviewof literature. Rom J Morphol Embryol. 2011;52:915---8.
8. Enjolras O, Wassef M, Chapot R. Color atlas of vascular tumorsand vascular malformations. Cambridge University Press; 2007.
9. Vargas MC, Castillo M. Sinonasal cavernous haemangioma: a case
Otol. 2009;123:868---72.