maternal physiology in pregnancy
TRANSCRIPT
MATERNAL PHYSIOLOGY & ENDOCRINAL CHANGES DURING
NORMAL PREGNANCY
By
Dr. Ram Lochan Yadav
Introduction In all mammalian species, there are extensive
biochemical, physiological and structural changes during pregnancy:
Any female of reproductive age could be pregnant
Virtually every organ system affected
The causes of these changes are:
1.To provide a suitable environment for nutrition, growth and development of fetus
2 . To prepare the mother for the process of parturition and subsequent support of the new born baby.
Mission
Understanding the adaptations to pregnancy
Anatomical
Physiological
Anatomical adaptations
• Uterus
• Cervix
• Ovaries
• Fallopian Tubes
• Vagina & Perineum
• Breast
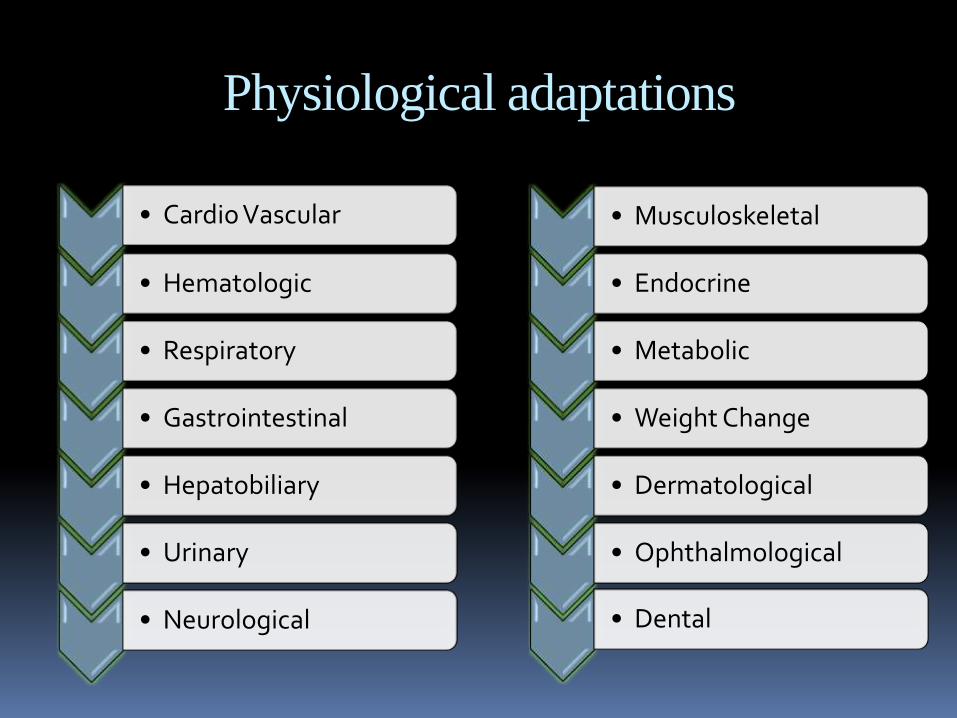
Physiological adaptations
• Neurological
• Respiratory
• Hematologic
• Cardio Vascular
• Gastrointestinal
• Hepatobiliary
• Urinary
• Metabolic
• Endocrine
• Musculoskeletal
• Weight Change
• Dermatological
• Ophthalmological
• Dental
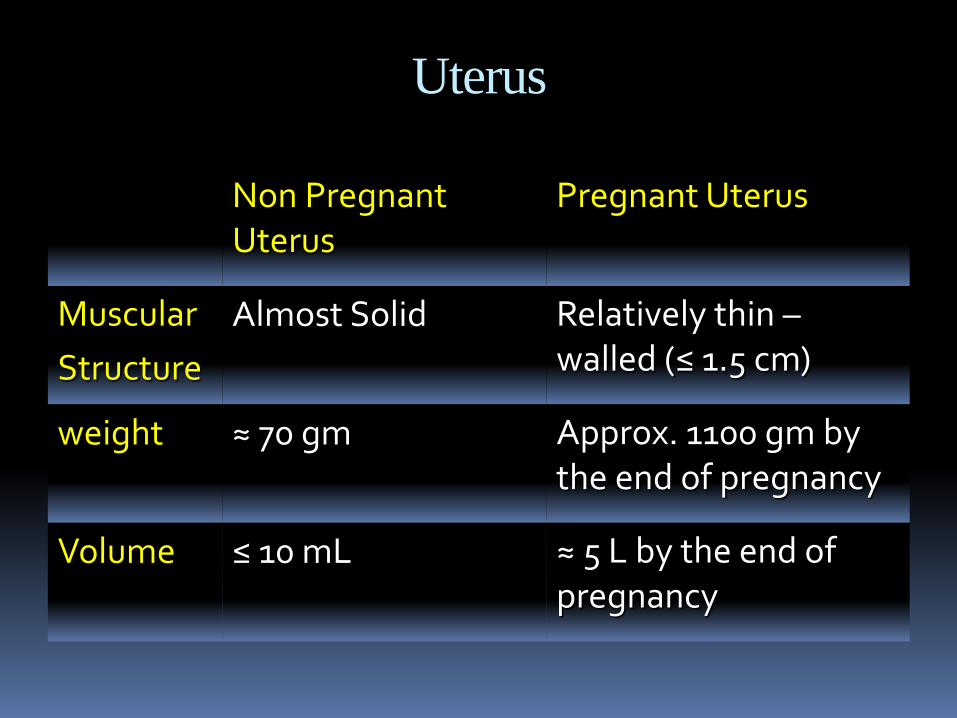
Uterus
Non Pregnant Uterus
Pregnant Uterus
Muscular
Structure
Almost Solid Relatively thin –walled (≤ 1.5 cm)
weight ≈ 70 gm Approx. 1100 gm by the end of pregnancy
Volume ≤ 10 mL ≈ 5 L by the end of pregnancy
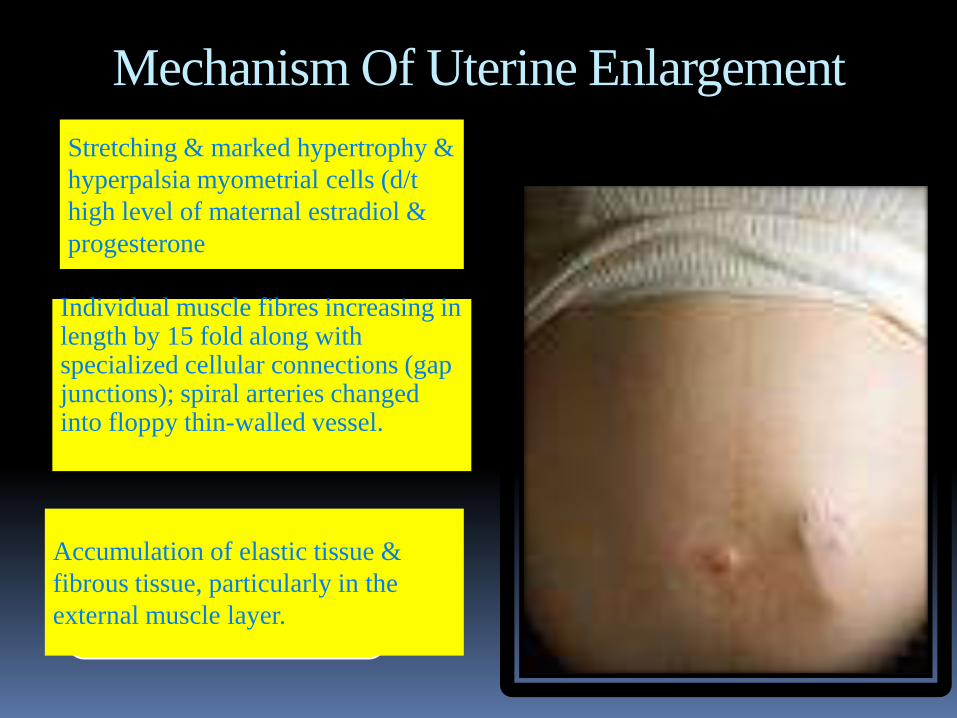
Mechanism Of Uterine Enlargement
Individual muscle fibres increasing in length by 15 fold along with specialized cellular connections (gap junctions); spiral arteries changed into floppy thin-walled vessel.
Stretching & marked hypertrophy &
hyperpalsia myometrial cells (d/t
high level of maternal estradiol &
progesterone
Accumulation of elastic tissue &
fibrous tissue, particularly in the
external muscle layer.
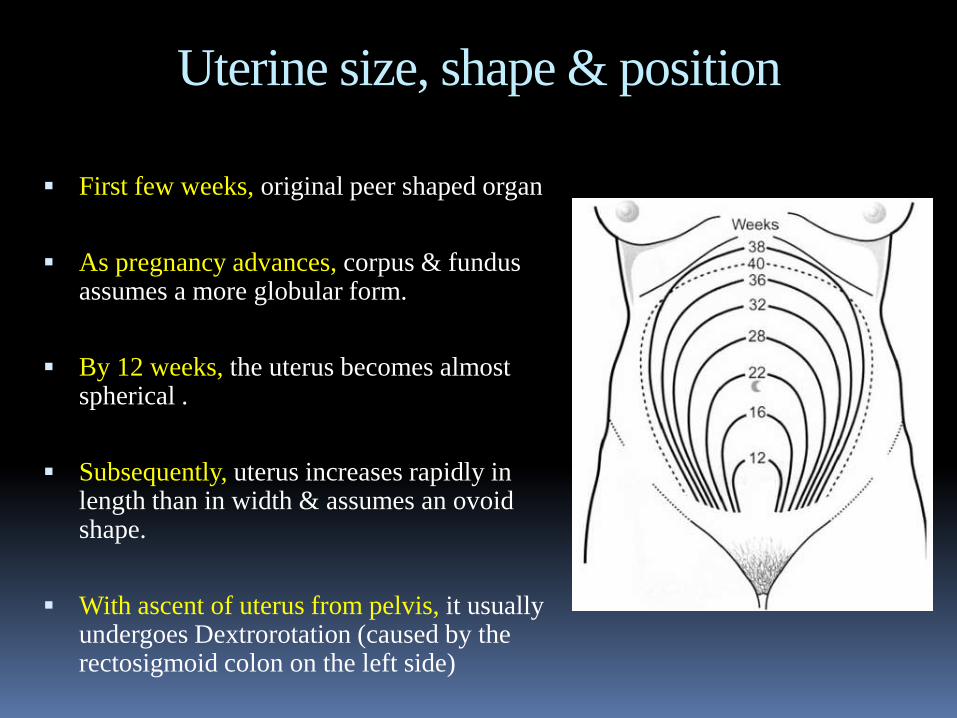
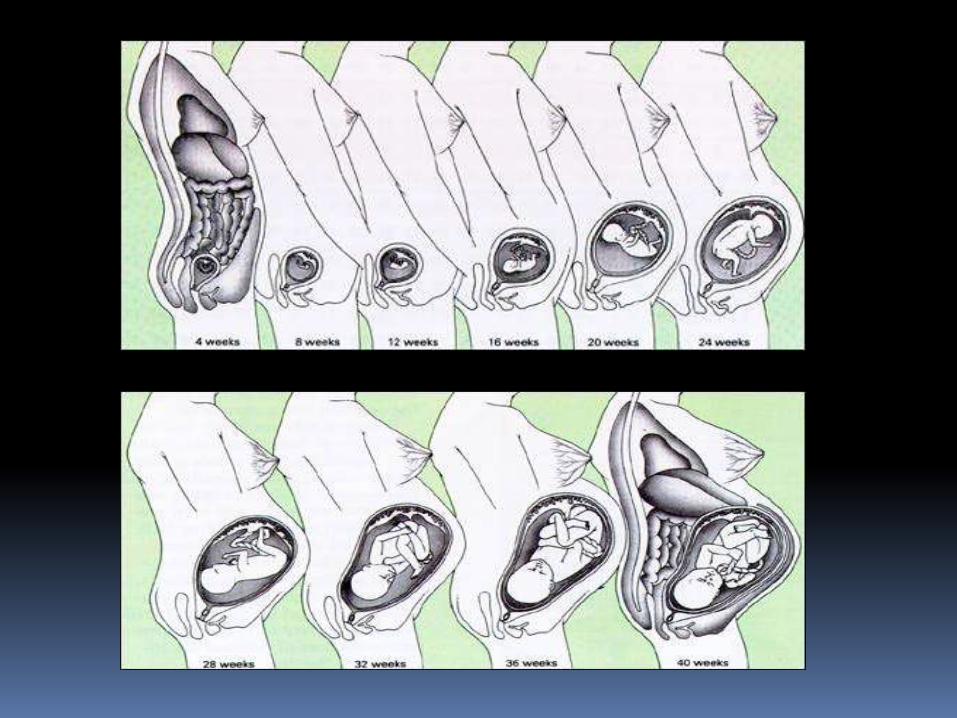
Uterine size, shape & position
First few weeks, original peer shaped organ
As pregnancy advances, corpus & fundus assumes a more globular form.
By 12 weeks, the uterus becomes almost spherical .
Subsequently, uterus increases rapidly in length than in width & assumes an ovoid shape.
With ascent of uterus from pelvis, it usually undergoes Dextrorotation (caused by the rectosigmoid colon on the left side)
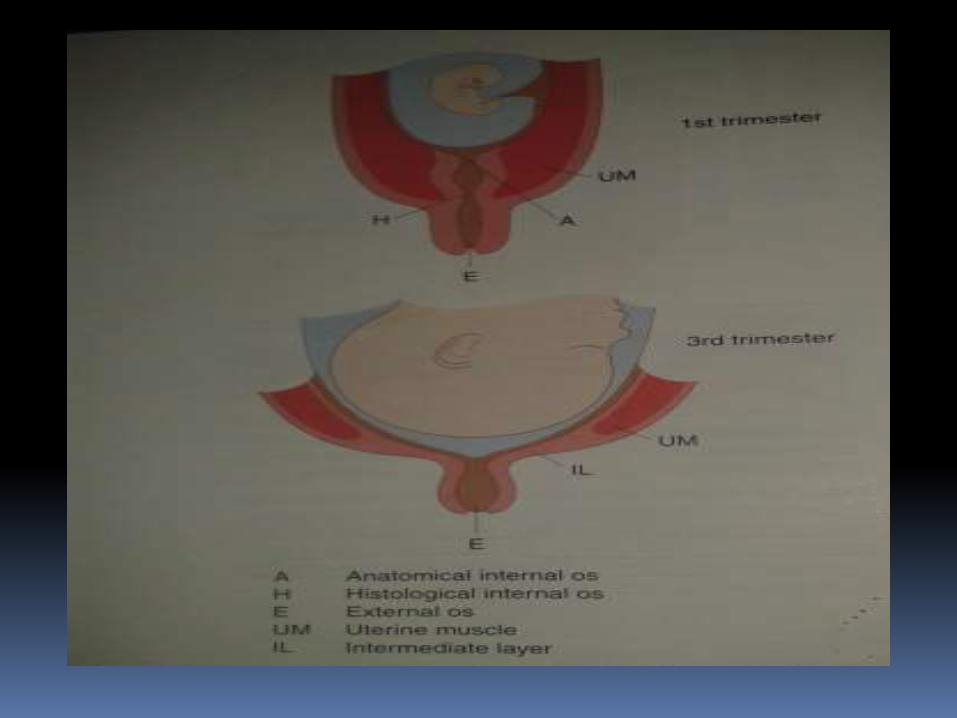
Cervix As early as 1 month after conception the cervix
begins to undergo profound swelling, softening
&cyanosis due to : (estradiol & progesterone)
Increased vascularity & edema of the entire cervix.
Hypertrophy & hyperplasia of the cervical glands.
Endocervical mucosal cells produce copious amounts
of a tenacious mucus that obstructs the cervical canal
soon after conception(mucus plug)
Estradiol stimulates growth of the columnar
epithelium of cervical canal that becomes visible on
ectocervix called ectropion
Ovaries
Cessation of ovulation & arrest of maturation of new follicles.
Single corpus luteum is found in ovaries of pregnant women that contributes to progesterone production maximally during the first 6 to 7 weeks of pregnancy
This explains the rapid fall in serum progesterone & the occurrence of spontaneous abortion upon removal of the corpus luteum before 7 wks.
Fallopian Tubes
The musculature of the fallopian tubes
undergoes little hypertrophy
The epithelium of the tubal mucosa becomes
somewhat flattened
Vagina & Perineum
Increased vascularity prominently affects the vagina resulting in the violet color (chadwick sign).
Considerable increase in the thickness of the vaginal mucosa, loosening of the connective tissue, hypertrophy of smooth muscle cells.
Vaginal epitheliumthickerdesquamationacidic discharge
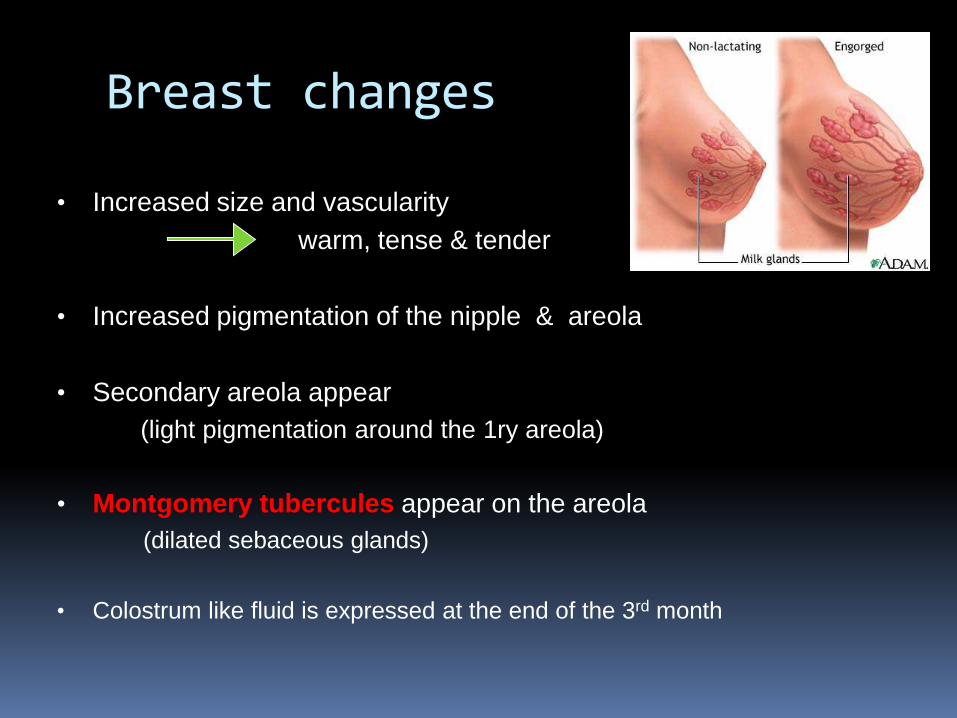
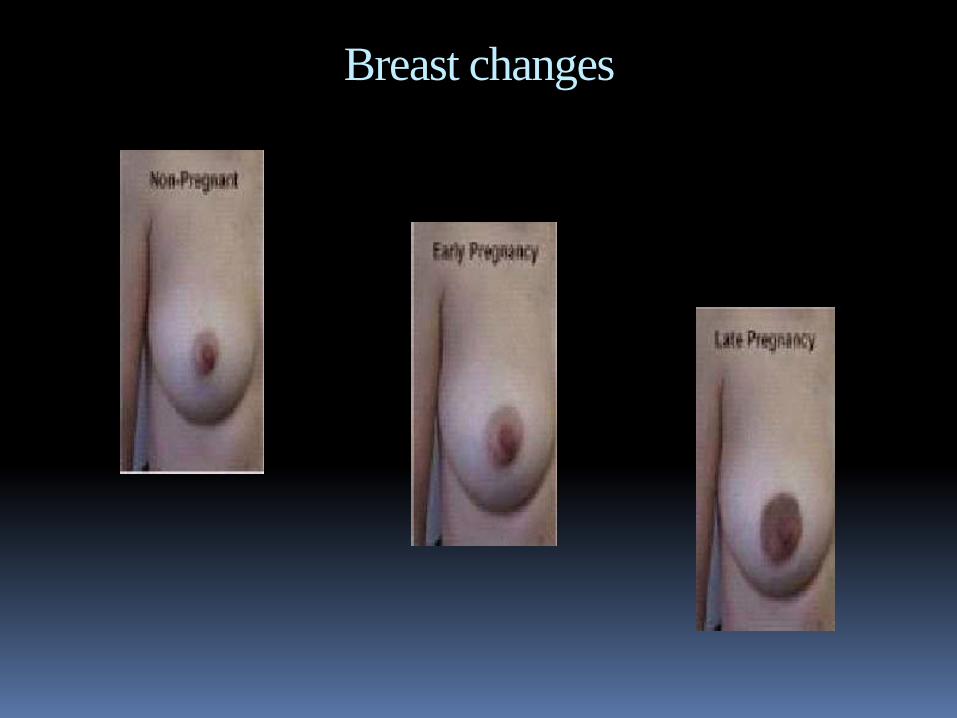
Breast changes
• Increased size and vascularity
warm, tense & tender
• Increased pigmentation of the nipple & areola
• Secondary areola appear
(light pigmentation around the 1ry areola)
• Montgomery tubercules appear on the areola
(dilated sebaceous glands)
• Colostrum like fluid is expressed at the end of the 3rd month
Breast changes
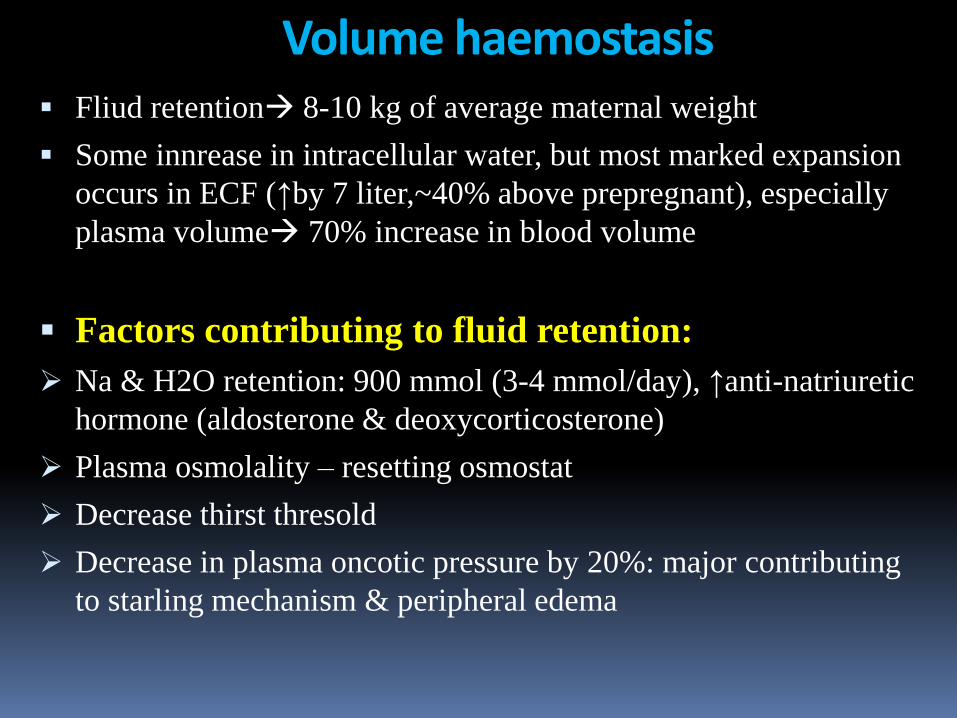
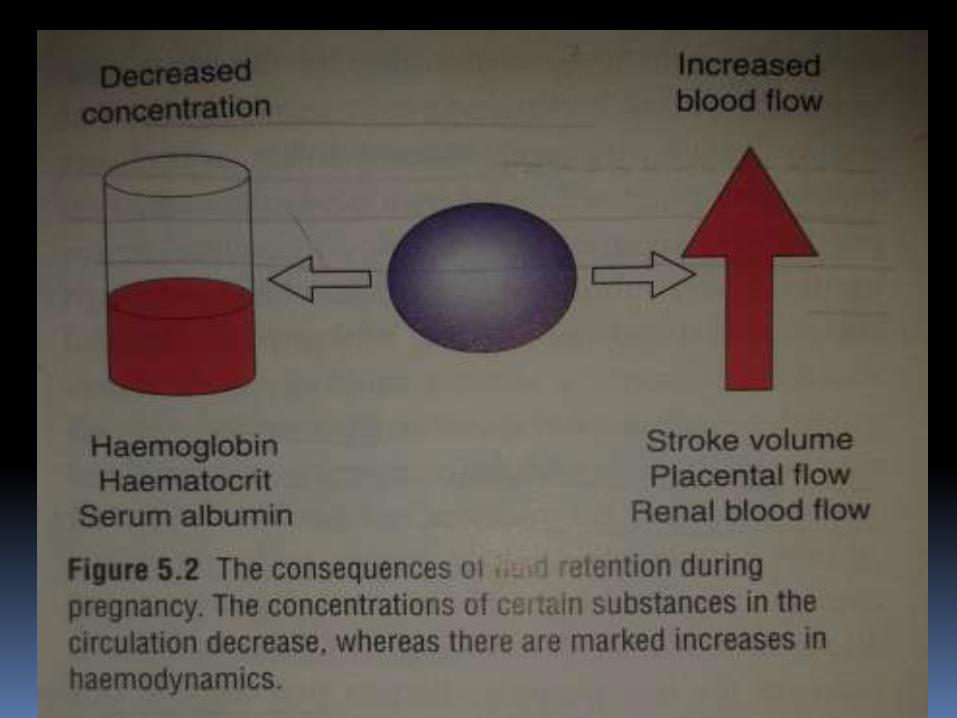
Volume haemostasis Fliud retention 8-10 kg of average maternal weight
Some innrease in intracellular water, but most marked expansion
occurs in ECF (↑by 7 liter,~40% above prepregnant), especially
plasma volume 70% increase in blood volume
Factors contributing to fluid retention:
Na & H2O retention: 900 mmol (3-4 mmol/day), ↑anti-natriuretic
hormone (aldosterone & deoxycorticosterone)
Plasma osmolality – resetting osmostat
Decrease thirst thresold
Decrease in plasma oncotic pressure by 20%: major contributing
to starling mechanism & peripheral edema
HAEMATOLOGY
↑ Erthropoietin & hPL in pregnanacy stimulate hemopoiesis
Erythrocytes rises (no. & size) by 20-30% after 16 wks
↑ in RBC mass is slower & lesser than the ↑ in plasma volume hemodilution physiological anemia of pregnancy
Total WBC count ↑ due to ↑ed polymorphonuclear leukocytes (d/t ↑ estrogen)
T & B lymphocytes counts do not change rather their function is suppressed pregnant women more suceptible to viral infections, malaria & leprosy

HAEMATOLOGY
COAGULATIONSeveral procoagulent factors (factors VII, VIII & X, & Plasma fibrinogen doubles) rise from the end of 1st
trimester hypercoagulable state (advantage or disadvantage??)
Antithombin III (inhibitor of coagulation) falls
ESR rises due to increase in fibrinogen favors rouleaux formation
Protein C (inactivates factor V & VIII)unchanged but protein S fall during 1st two trimesters
Plasma fibrinolytic activity is decresed
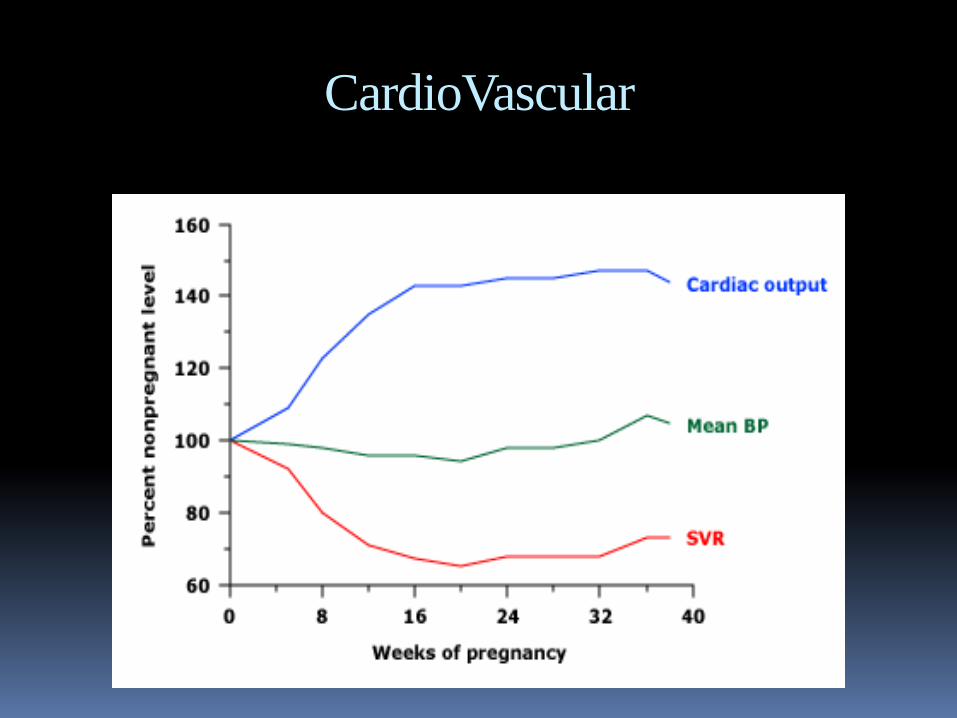
CardioVascular
Elevated progesterone & estrogen vasodilation
Endothelium derived vasoactive (eg.NO)
Vasodilation ↓TPR ↓afterload& BP, & perceived as
circulatory underfilling that acivates RAS↑ALD↑CO
Probably fall in baroreflex sensitivity as pregnancy
progresses & HRV falls & HR increases ↑CO
Small fall in SBP but greter fall in DBP. The BP then rises
steadly in parallel with ↑sympthetic activity (thus, ↑in PP).
MAP usually decreases during mid pregnancy & rises in 3rd
trimester remains at or below nomal (Why??)
No change in pressure in the right ventricle, WHY??
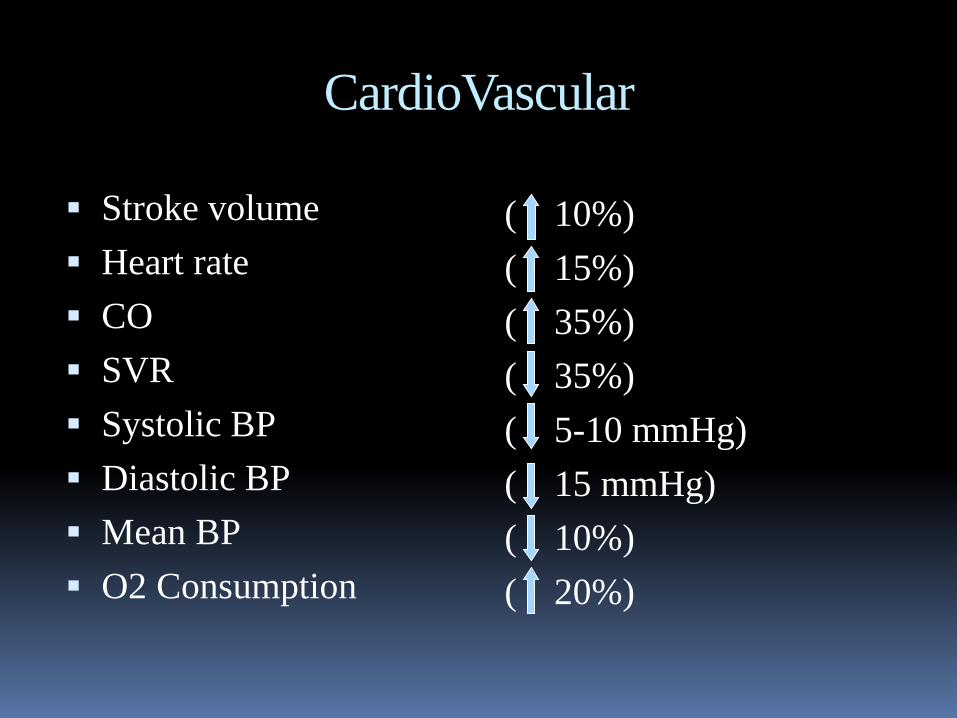
CardioVascular
Stroke volume
Heart rate
CO
SVR
Systolic BP
Diastolic BP
Mean BP
O2 Consumption
( 10%)
( 15%)
( 35%)
( 35%)
( 5-10 mmHg)
( 15 mmHg)
( 10%)
( 20%)
CardioVascular
ECG Changes
Increased heart rate ( 15%)
15° left axis deviation.
Inverted T-wave in lead ІІІ.
Q in lead ІІІ & AVF
Unspecific ST changes
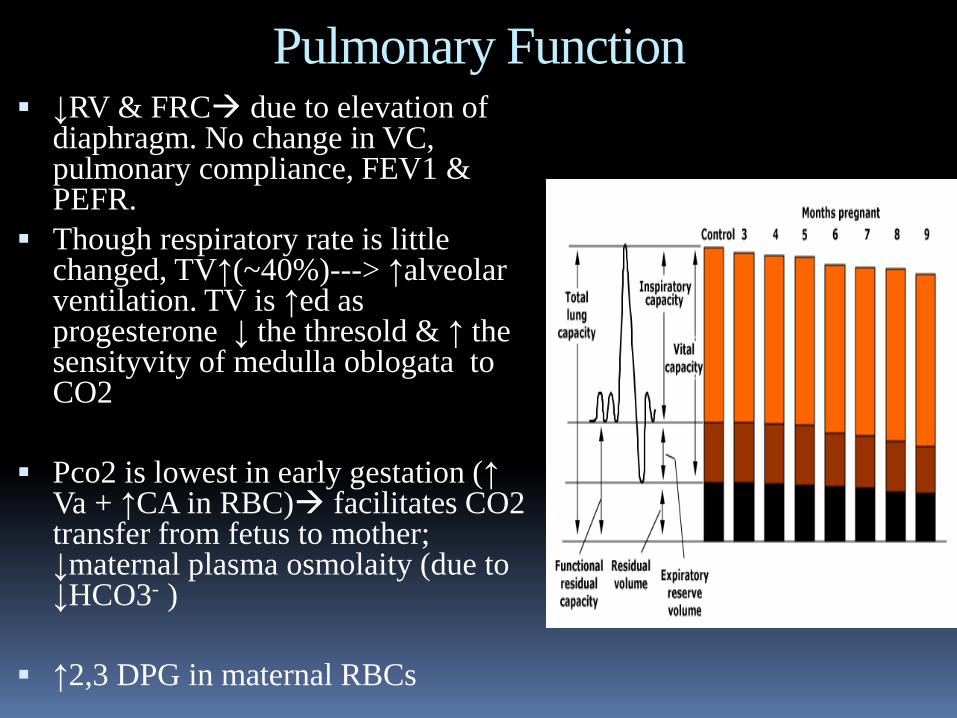
Pulmonary Function ↓RV & FRC due to elevation of
diaphragm. No change in VC, pulmonary compliance, FEV1 & PEFR.
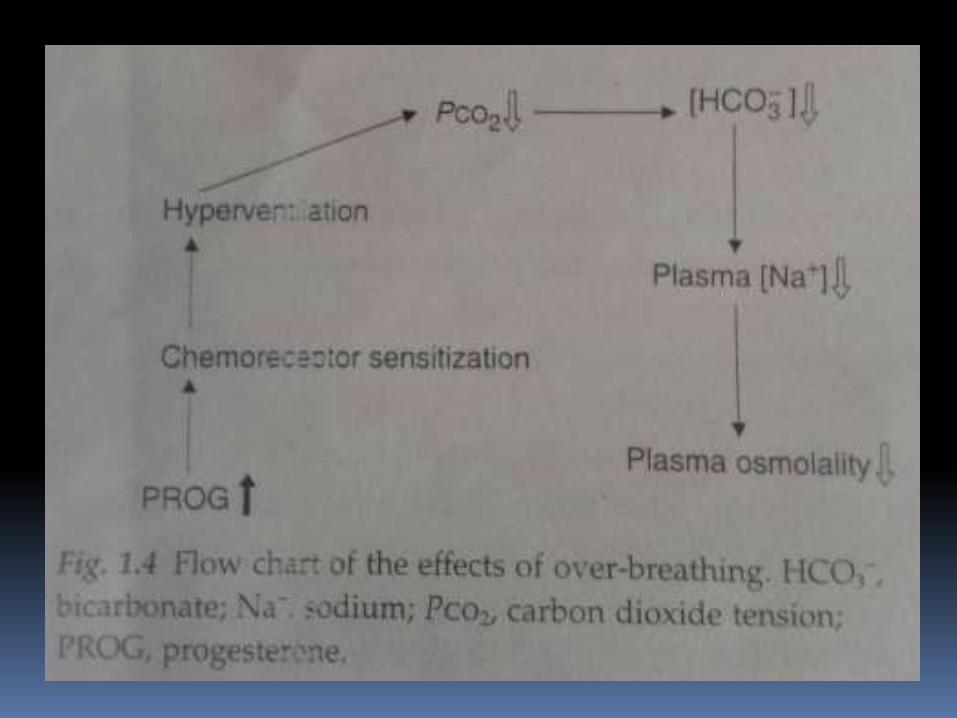
Though respiratory rate is little changed, TV↑(~40%)---> ↑alveolar ventilation. TV is ↑ed as progesterone ↓ the thresold & ↑ the sensityvity of medulla oblogata to CO2
Pco2 is lowest in early gestation (↑ Va + ↑CA in RBC) facilitates CO2 transfer from fetus to mother; ↓maternal plasma osmolaity (due to ↓HCO3- )
↑2,3 DPG in maternal RBCs
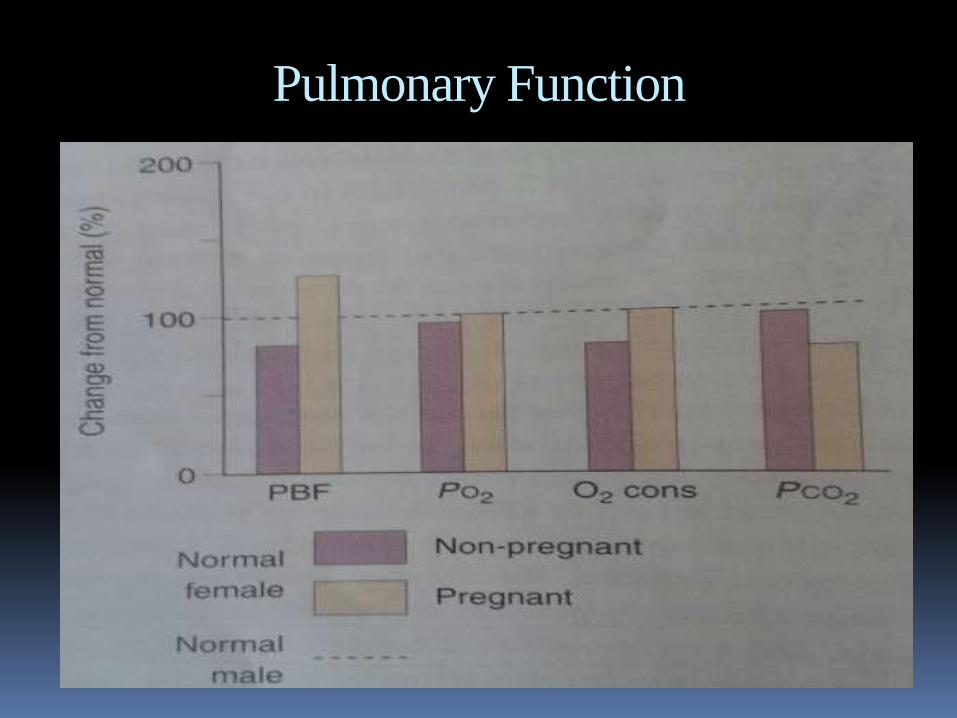
Pulmonary Function
Fig 5.9 baker
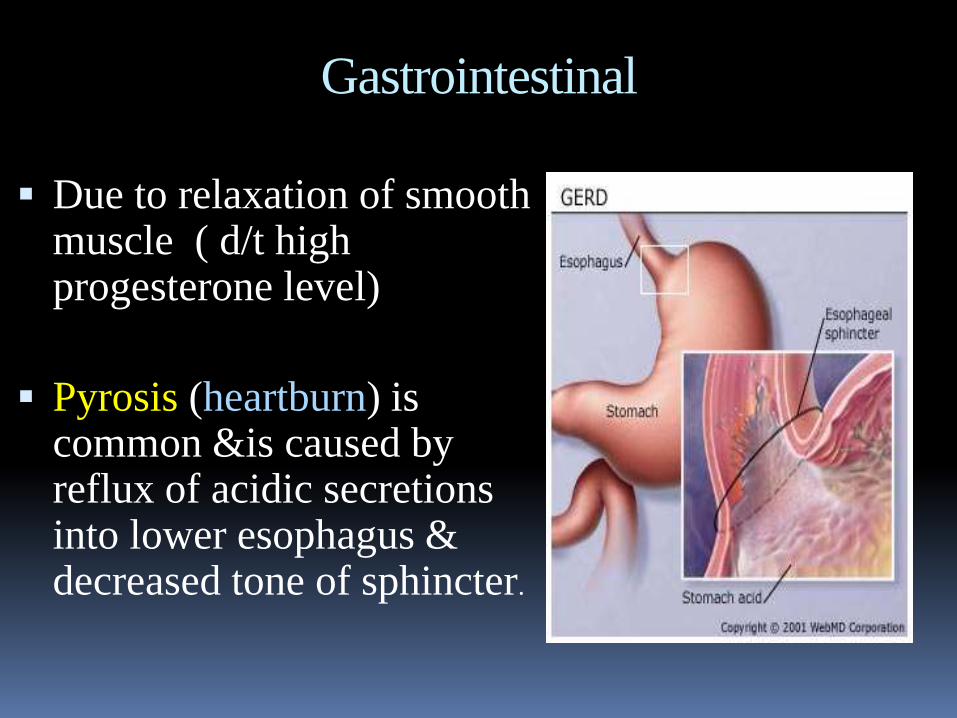
Gastrointestinal
Due to relaxation of smooth muscle ( d/t high progesterone level)
Pyrosis (heartburn) is common &is caused by reflux of acidic secretions into lower esophagus & decreased tone of sphincter.
Gastrointestinal
Slight reduction in gastric secretion and diminished gastric motility result in slow emptying and may lead to nausea.
Reduced intestinal motility lead to increase time for water absorption , which tends to induce constipation
Gastrointestinal
Growth of conceptus and uterus
leads to increase appetite and
thirst.
In late pregnancy pressure of the
uterus reduces capacity for large
meals leads to frequent small
snacks
Hepatobiliary
No distinct changes in morphology & size of liver in pregnancy. Despite this, there is increase in diameter of portal vein &its blood flow
Serum alkaline phosphatase almost doubles (heat stable placental alkaline phosphatase isozymes)
Serum AST,ALT,GGT, bilirubin levels are slightly lower than non pregnant normal values
Decrease in albumin to globulin ratio occurs due to combined reduction in albumin concentration & slight increase in serum globulin levels
Gallbladder changes
Reduced contractility of the gallbladder & rlaxation of biliary tract. Hence, bile flow decreases.
Progesterone impairs gallbladder contraction by inhibiting CCK mediated smooth muscle stimulation (1ry regulator of gallbladder contraction)
Impaired motility leads to stasis, associated with increase in cholesterol saturation of pregnancy.
Pregnancy causes intrahepatic cholestasis from retained bile salts.
Cholestasis of pregnancy is linked to high levels of estrogen which inhibit transductal transport of bile acids.
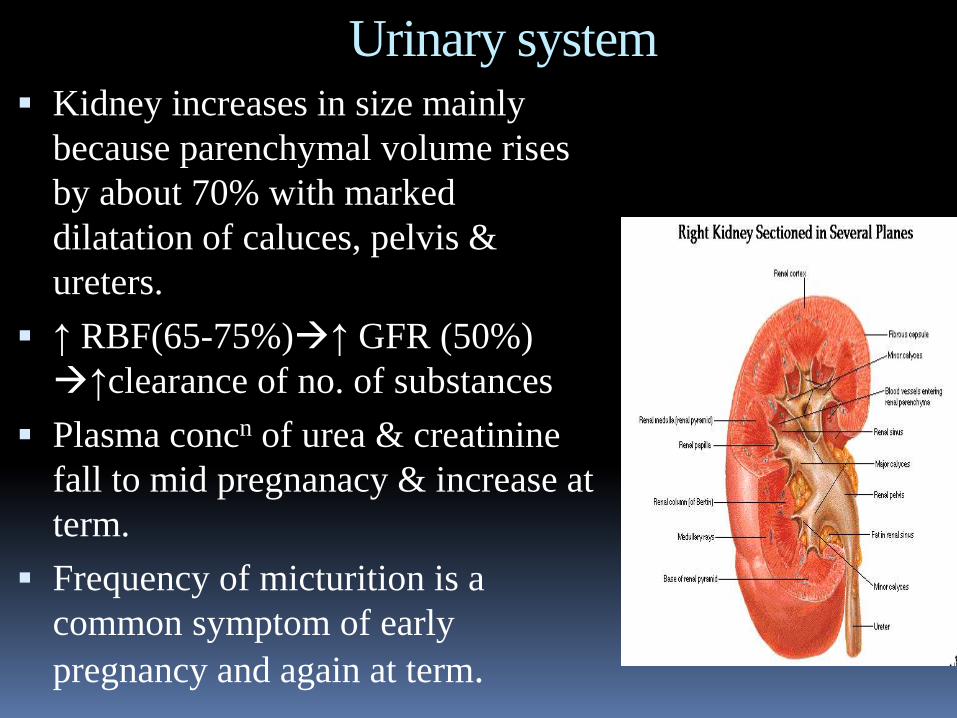
Urinary system Kidney increases in size mainly
because parenchymal volume rises
by about 70% with marked
dilatation of caluces, pelvis &
ureters.
↑ RBF(65-75%)↑ GFR (50%)
↑clearance of no. of substances
Plasma concn of urea & creatinine
fall to mid pregnanacy & increase at
term.
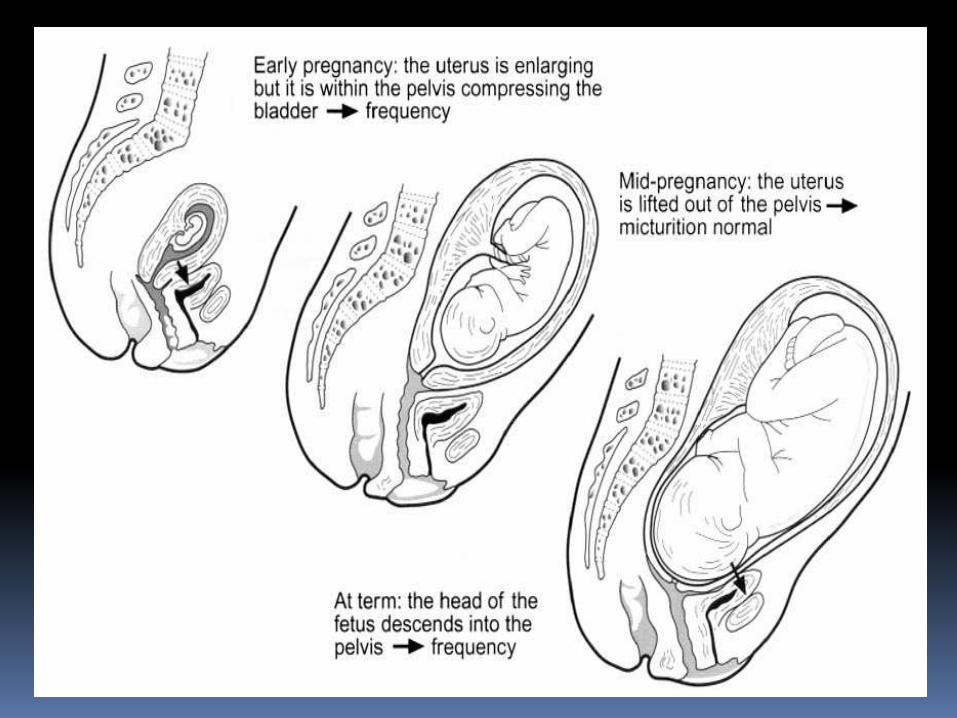
Frequency of micturition is a
common symptom of early
pregnancy and again at term.
Urinary System
Glycosuria - may rise 10-fold as the greater filterd
load exceeds the proximal tubular Tmax for glucose
(~1.6-1.9 mmol/min)
Excretion of most of amino acids increases
microalbuminuria (0.3 g/day)
Urinary Calcium excretion is increased even though
tubular reabsorption is enhanced under the influence
of 1,25-dihydrxyvitamin D.
↑TBW (~20%) with fall in plasma osmolality about
4-6 wks of pregnancy (d/t hCG) edema
Neurological
Women often report
problems with attention,
concentration, &memory
throughout pregnancy &
early postpartum period.
Neurological
In a longtudinal study done by keenan
&colleagues (1998) investigating memory
in pregnant women by a matched control
group, they found pregnancy related
decline in memory limited to 3rd trimester
an attributable to depression, anxiety, sleep
deprivation or any other physical changes
associated with pregnancy
Neurological
Zeeman and co-workers (2003) used MRI to measure cerebral blood flow across pregnancy in 10 healthy women.
They found that mean blood flow bilaterally in the middle and posterior cerebral arteries decreased progressively from 147 and 56 ml/min when non pregnant to 118 and 44 ml/min late in the third trimester, respectively.
The mechanism and clinical significance of this decrease, and whether it relates to the diminished memory observed during pregnancy is unknown.
Musculoskeletal Progressive lordosis compensates
for the anterior position of the
enlarging uterus.
Increased mobility of sacroiliac,
sacrococcygeal &pubic joints
leading to wadling gait, correlated
to increased levels of maternal
estrogen, progesterone & relaxin
levels.
Joint mobility causes low back
pain which is bothersome late in
pregnancy.
Dermatological
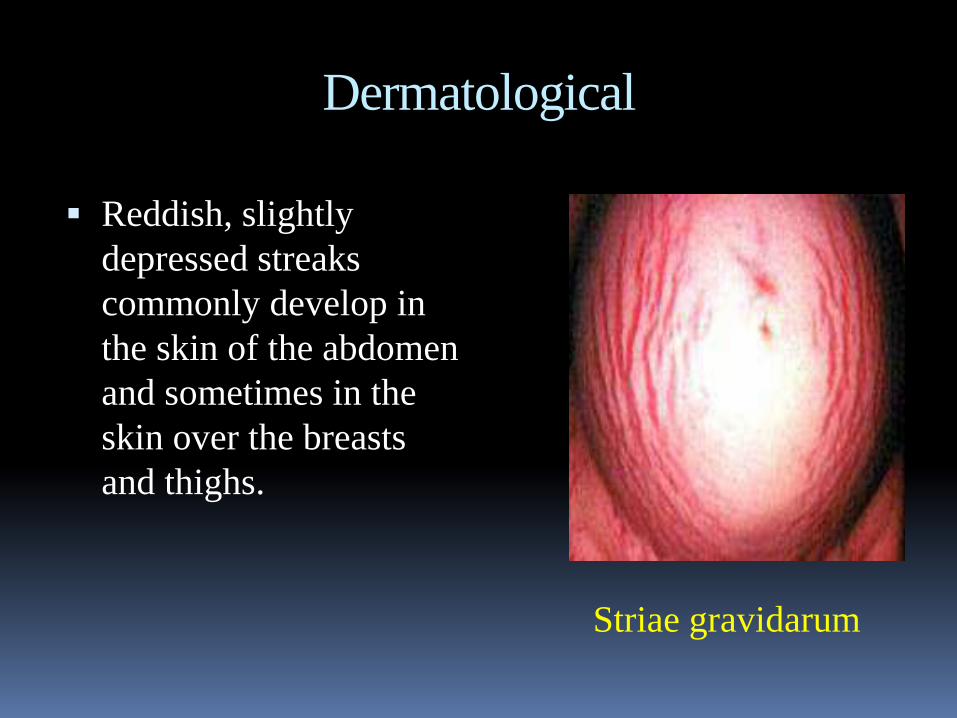
Reddish, slightly
depressed streaks
commonly develop in
the skin of the abdomen
and sometimes in the
skin over the breasts
and thighs.
Striae gravidarum
Dermatological
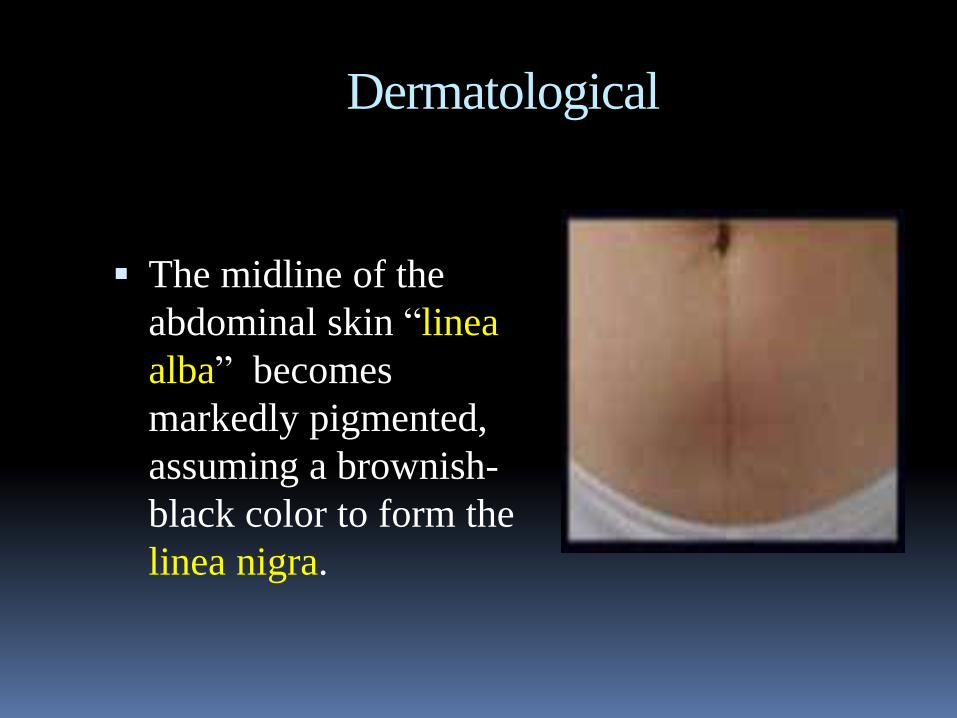
The midline of the
abdominal skin “linea
alba” becomes
markedly pigmented,
assuming a brownish-
black color to form the
linea nigra.
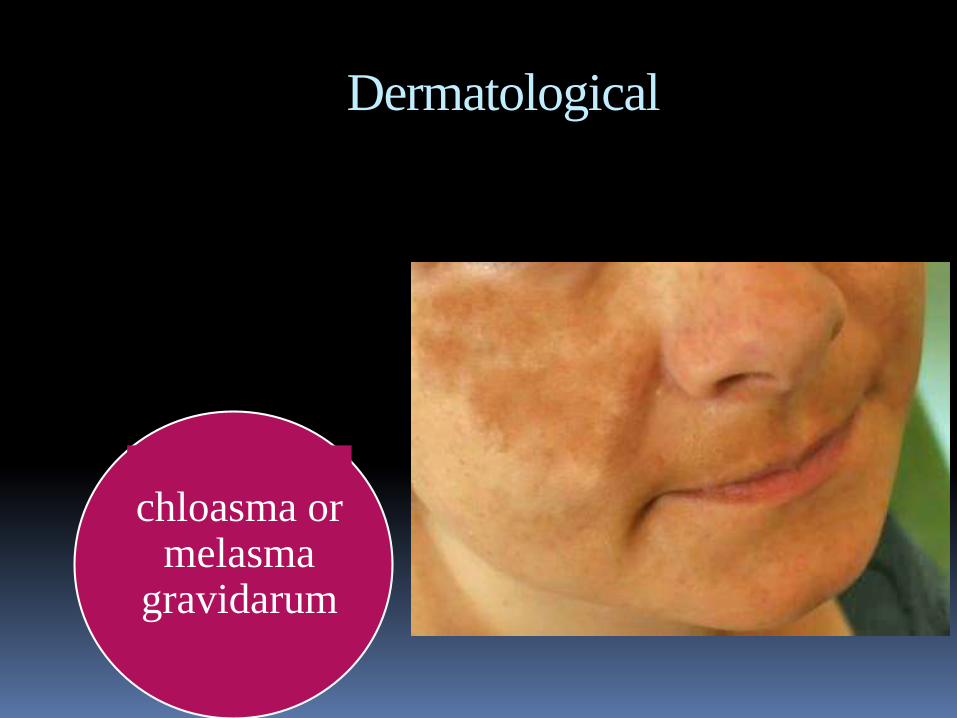
Dermatological
chloasma or melasma
gravidarum
Weight Changes
Metabolic changes, accompanied by fetal growth, result in an increase in weight of around 25% of the non-pregnant weight.
Approximately 12.5 kg in the average woman (usually at a rate of 0.5 kg/wk for the last 20wks).
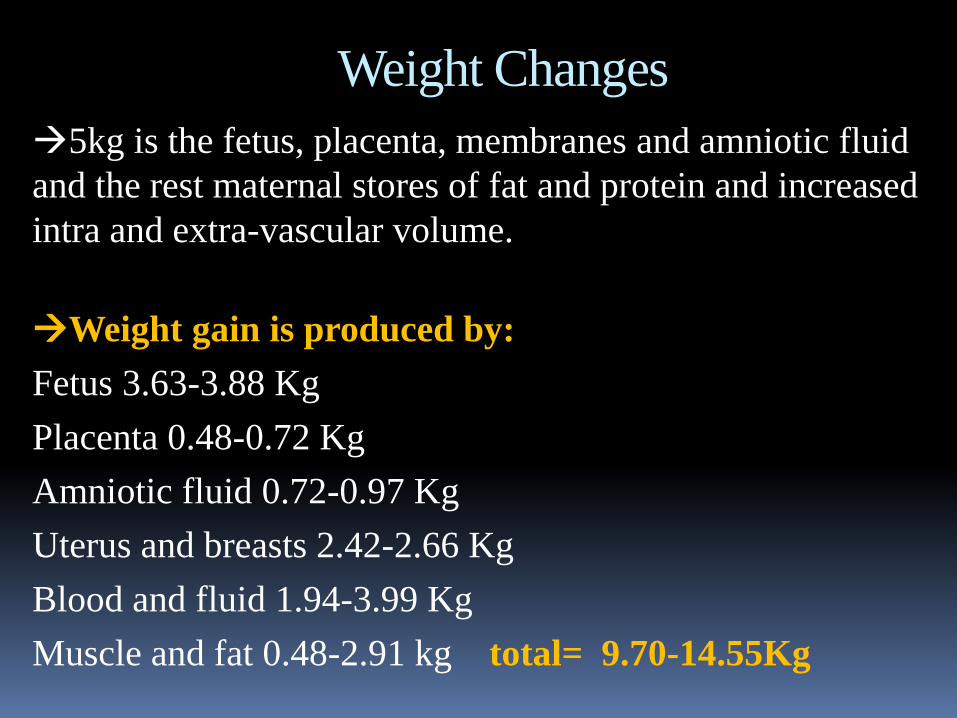
Weight Changes
5kg is the fetus, placenta, membranes and amniotic fluid
and the rest maternal stores of fat and protein and increased
intra and extra-vascular volume.
Weight gain is produced by:
Fetus 3.63-3.88 Kg
Placenta 0.48-0.72 Kg
Amniotic fluid 0.72-0.97 Kg
Uterus and breasts 2.42-2.66 Kg
Blood and fluid 1.94-3.99 Kg
9.70-14.55Kgtotal=Muscle and fat 0.48-2.91 kg
Ophthalmic
Decrease in intraocular pressure due to increased vitreous outflow
Decreased corneal sensitivity especially, late in gestation
Slight increase in corneal thickness thought to be due to edema
Visual function remains unaffected except for transient loss of accomodation
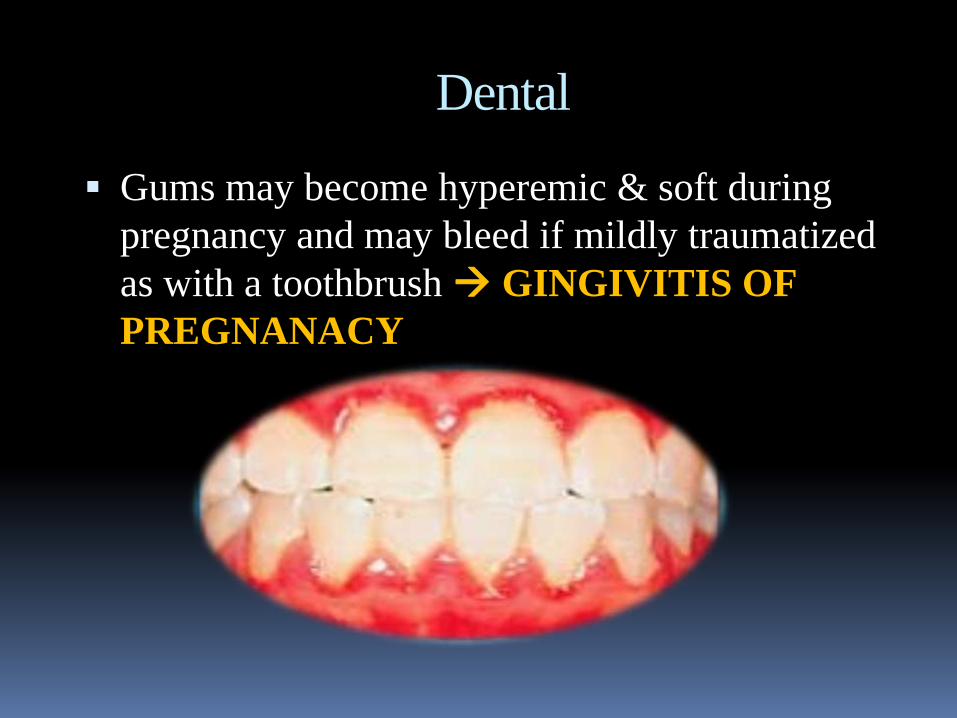
Dental
Gums may become hyperemic & soft during
pregnancy and may bleed if mildly traumatized
as with a toothbrush GINGIVITIS OF
PREGNANACY
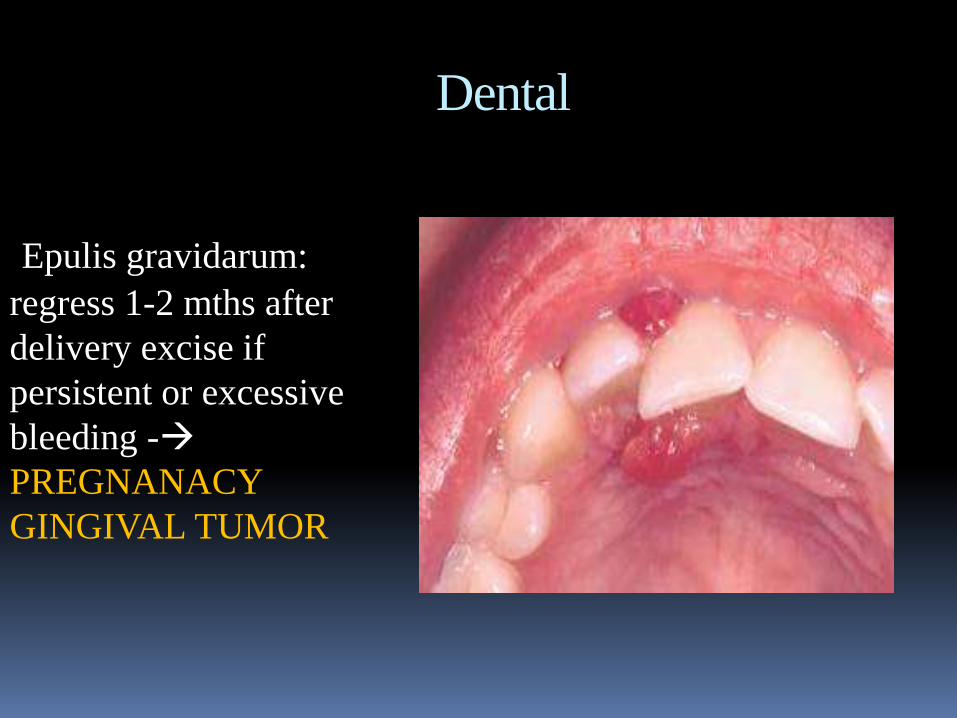
Dental
Epulis gravidarum:
regress 1-2 mths after
delivery excise if
persistent or excessive
bleeding -
PREGNANACY
GINGIVAL TUMOR
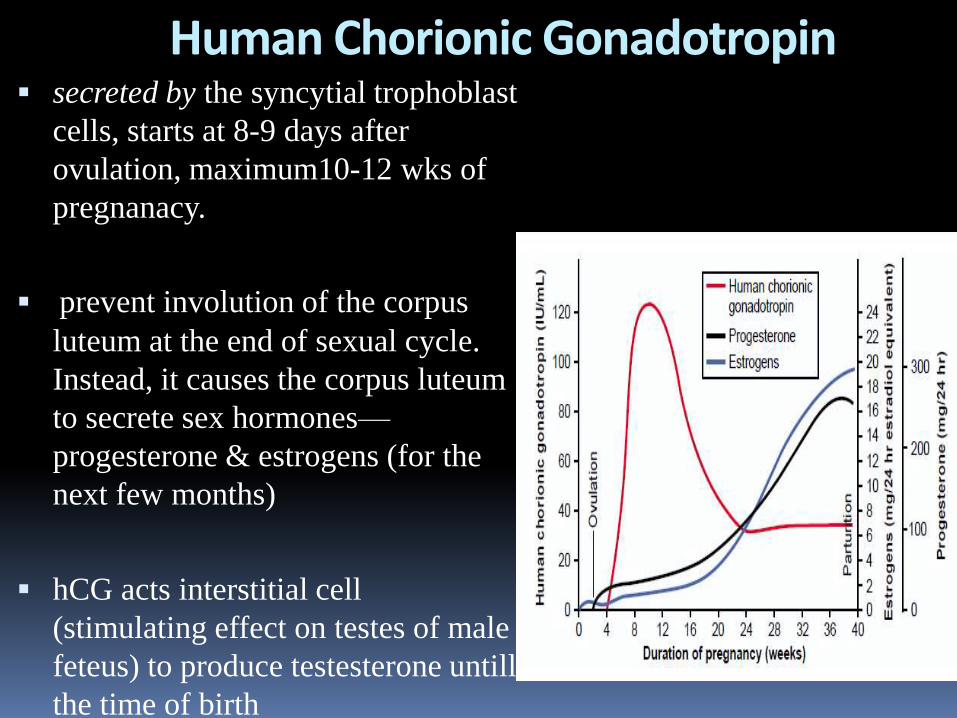
Human Chorionic Gonadotropin secreted by the syncytial trophoblast
cells, starts at 8-9 days after
ovulation, maximum10-12 wks of
pregnanacy.
prevent involution of the corpus
luteum at the end of sexual cycle.
Instead, it causes the corpus luteum
to secrete sex hormones—
progesterone & estrogens (for the
next few months)
hCG acts interstitial cell
(stimulating effect on testes of male
feteus) to produce testesterone untill
the time of birth
Estrogens by the Placenta
Trophoblast cell of placenta form estradiol, estrone, & estriol from dehydroepiandrosterone & 16-hydroxydehydroepiandrosterone, which are formed from adrenal glands of mother & fetus
Functions:
Enlargment of mother’s uterus, breasts & growth of ductal structure, external genitalia
Relax the pelvic ligaments, sacroiliac joints become limber, pubic symphysis becomes elastic
progesterone by the Placenta
Functions:
Causes decidual cells to develop in uterine endometrium & provide nutrition
Prevent uterine contractions from causing spontaneous abortion
Development of conceptus before implantation
During pregnancy helps estrogen prepare the mother’s breasts for lactation
Human chorionic somatomammotropin (hCS):
Partial development of animal’s breast & lactation (also K/A hPL)
Acts like GH; ↓insulin sensitvity & ↓glucose utilisation,
& release free fats in mother to provde more glucose to
fetus
The hypothalamus & pituitary gland
Size of anterior pituitary lobe increases (2-3 times) due to growth of prolactin secreting cells. Prolactin secretion increase by 10-20 times from the end of 1st trimester
Hypothalamo-pituitary-ovarian axis is suppressed by high level of sex steroids. This decrease LH & FSH secretion & thus prevents ovulation in pregnancy.
TSH secretion responds normally to hypothalamic thyrotropin-releasing hormone (also formed by placenta)
ACTH concentrations rise during pregnancy partly because of placental synthesis of ACTH & corticotropin-releasing hormone & do not respond to normal control mechanisms
THE ADRENAL GLAND
Plasma total & unbound cortisol, cortsol binding globulin (CBG) & other corticosteroid concentration increase
Excess glucocorticoid inhibit fetal growth . However, the placenta synthesizes a pregnancy-specific 11β-
hydroxysteroid dehydrogenase, which inhibits transfer
of maternal cortisol.
THE THYROID GLANDMaternal iodine requirements ↑ because of active
transport of iodine to feto-placental unit & because ↑ed iodine renal clearance. Because the plasma level falls, thyroid gland increases iodine uptake from the blood. If there is dietary insufficiency,thyroid gland hypertrophies.
Parathyroid glands & Ca metabolism
The increased demand of Ca for fetal growth is achieved by increased absorption of Ca form GIT by vit. D & by increase in PTH secretion--- so, Ca supplement is imp.
Maternal total plasma Ca falls as albumin level also falls, but unbound ionized Ca unchanged.
PTH regulates synthesis of 1,25-dihydroxycholecalciferol (vit. D) in proximal convoluted tubule.
PTHrP, from fetal parathyroid gland & placenta, is transferred to maternal circulation & affects Ca haemostasis by acting trough PTH receptor
Renal hormones
RAS is activated from early oregnanacy
A vasodilator component of RAS has recently been described in which angiotensin 1-7 is the agonist, which rises during pregnancy, which stimulate the release of NO & prostacyclin
Erthropoietin synthesis stimulated by hCG
THE PANCREAS
No. of β cells & size of islet of Langerhan’s increase in
pregnancy

Energy requirements
BMR increased by ~5% by 3rd trimester
Additional protein (30gm/day): to meet the demand of the growing fetus, placenta, uterus, and breasts, as well as the increased maternal blood volume.
iron (60 mg/day): to support the expanding maternal hemoglobin mass, the placenta, and the fetus . iron uptake increased in pregnancy (from 1.5 to 7 mg/day)
Folate (400 to 800 μg/day): for blood cells formation
Carbohydrate s & lipids Pregnancy is hyperlipiadaemic & glucosuric
After mid pregnancy insulin resistance develops progressively (why??) & plasma glucose concentration rise.
Resistani is beneficial to fetus as glucose crosses the placenta readily & fetus uses glucose as its primary enery substrates.
Increased maternal blood glucose stimulates glycogen synthesis & storage, deposition of fat & transport of amino acids into cells.
↑ VLDL, HDL, free fatty acids, triglycerides
Preclampsia & eclampsia rapid rise in BP to hypertensive levels during the last few
months of pregnancy & with leakage of large amounts of protein into the urine. This condition is called preeclampsia or toxemia of pregnancy.
characterized by excess salt and water retention by the mother’s kidneys and by weight gain and development of edema and hypertension , impaired function of the vascular endothelium, & arterial spasm in many parts of the mother’s body, especially in the kidneys, brain, and liver.
Both the renal blood flow and the glomerular filtration rate are decreased, which is exactly opposite to the changes that occur in the normal pregnant woman.
Preclampsia & eclampsia
Causes: unknown
results from some type of autoimmunity or allergy in the mother caused by the presence of the fetus
caused by excessive secretion of placental or adrenal hormones
insufficient blood supply to the placenta
increased levels of inflammatory cytokines such as tumor necrosis factor-a and interleukin-6.
Dewhurst’s textbook of Obstetrics & Gynaecology, 8th
edt.
Obstetrics by Ten Teachers, N. Baker- 18th ed.
Textbook of medical physiology- GK Pal
Textbook of medical physiology- Guyton, 11th ed
Textbook of medical physiology- Walter F. Boron
References:
