massive hemolysis in clostridium perfringens infections
TRANSCRIPT

Journal of Surgical Oncology 3513-18 (1987)
Massive Hemolysis in Clostridium perfringens Infect ions
RICHARD C. BECKER, MD, MICHAEL GIULIANI, MD, RiCHARD A. SAVAGE, MD, AND
JAMES K. WEfCK, MD, FACP
From the Departments of Internal Medicine (R.C.B.), Neurology (M.G.), Laboratory Hematology (R.A.S.), and Hernatology-Oncology (J. K. W), Cleveland Clinic Foundation,
Cleveland
Over a 14-month period at the Cleveland Clinic Foundation, 424 strains of Clostridium were isolated; of these, 52 strains were Clostridium perfrin- gens isolated from 41 patients. Eight strains of C. peeingens were isolated from the blood of six patients; five of these patients had neoplastic disease and three developed massive intravascular hemolysis with rapidly developing shock and death. Clinical details are given on three patients with fatal Clostridium peijfnngens sepsis, and the nature of presentation and pathophysiologic mechanisms are discussed.
KEY WORDS: Clostridium perfringens, neoplasia, hemolysis, shock
INTRODUCTION Clostridia are anaerobic, nonmotile, spore-forming ,
gram-positive bacilli which commonly inhabit the soil, gastrointestinal tract, and female genital tract. Rarely, they may be isolated from the skin and oral mucosa. There are currently 63 recognized species of clostridia; however, improved laboratory techniques for isolating fastidious anaerobic organisms will likely uncover others UI.
Clostridium perfringens is a species commonly isolated and is capable of causing an extraordinary spectrum of clinical manifestations ranging from transient bacteremia to massive red blood cell hemolysis, shock, and death.
Over a 14-month period (from January 1983 through March 1984) 424 strains of clostridia were isolated from adult patients at the Cleveland Clinic Foundation. Clos- tridium dificile was the most common species, occurring in 108 patients. Clostridium perjkingens was found in 41 patients from sites which included surgical wounds, ab- dominal abscesses, cervical swabs, peritoneal fluid sam- ples, tracheostomies, arteriovenous fistulae, and periph- eral blood. Six cases of bacteremia were documented. Five of the six patients with positive blood
of clinical demise a course of chemotherapy. Death en- sued in each patient, three of whom experienced massive intravascular hemolysis. A potential portal of entry within the gastrointestinal tract was documented in three of the five cases. Autopsies were not performed on the other two cases, and as such a source for their bacteremia remains speculative.
CASE 1 A 58-year-old male presented to the Cleveland Clinic
Foundation in January 1984 for evaluation of generalized weakness, weight loss, and dyspnea on exertion. Admis- sion chest x-ray identified a 2 X 3 cm nodule in the left upper lobe. Tissue obtained by CT-directed needle bi- opsy revealed squamous cell carcinoma. He subsequently received a course of chemotherapy consisting of Velban and cis-platinum. One month later he presented to the emergency room with shortness of breath. On physical examination he was noted to be in respiratory distress. His blood pressure was 130/84 mmHg without orthostatic change. Respirations were 50 per minute and labored. The heart rate was 130 and regular, and the temperature was 36°C (oral). The skin was cool and clammy. There
cultures had neoplastic disease which included carcinoma of the pancreas, lung, and colon; non-Hodgkin's lym- Accepted for December 28? 1985.
Address reprints requests to James K. Weick, MD, Department of Hematology-Oncology, Cleveland Clinic Foundation, Cleveland, OH 44106.
phoma; and acute non-lymphocytic leukemia* five patients were receiving or had received within 4 weeks
0 1987 Alan R. Liss, Inc.

14 Becker et a1
were no rashes, petechiae, purpura, or ecchymoses. Coarse rhonchi were present throughout both lung fields. The heart exam was normal. The abdomen was soft, bowel sounds were present, and stool was positive for blood. He was anxious yet oriented. No focal neurologic deficits were appreciated. Laboratory values were as follows: white blood count 1.00 X lO’/liter, hemoglobin 7.4 gm/dl, platelets 535 x 109/liter, total bilirubin 2.0 mg/dl, LDH 5,360 U/ml, SGOT 780 U/ml, prothrombin time 20 seconds (control 12 seconds), partial thrombo- plastin time 42 seconds (control 21-3 1 seconds), direct and indirect Coombs’ test negative, fibrin degradation products negative (see Table I and Hematopathologic Findings). Blood cultures grew C. pe@ingens. Despite supportive efforts in the Medical Intensive Care Unit, the patient died. An autopsy was requested and denied.
CASE 2 A 58-year-old male presented to the Cleveland Clinic
Foundation with a 1-year history of diffuse intermittent abdominal pain and a 50-pound weight loss. A CT scan of the abdomen revealed a mass in the head of the pancreas and a dilated common bile duct. He underwent an exploratory laparotomy with a choledochoduodenos- tomy, gastrojejunostomy, and a true cut transduodenal biopsy of the pancreas. The biopsy revealed moderately well-differentiated adenocarcinoma. He received a course of chemotherapy consisting of BCNU, thio-tepa, and Cytoxan. Two weeks later he presented to the emergency room with fever, chills, and lethargy. His blood pressure was 70/40 mmHg, pulse 150 and regular, respirations 30 and labored, temperature 38.6”C (oral). Laboratory find- ings were as follows: white blood count 1.00 x lO’/liter, hemoglobin 5.7 gm/dl, platelets 9.00 x lO’/liter, LDH 3000 U / d , Coombs’ test negative, fibrin degradation products negative (see Table I and Hematopathologic Findings). Blood cultures grew C. perfkingens. The pa- tient rapidly deteriorated and died. An autopsy was per- formed and revealed adenocarcinoma of the pancreas with local invasion of the duodenum. The anastomosis from his previous surgery was intact. There were numer- ous gas-filed cysts within the liver. Gram stain of these cystic regions revealed gram-positive bacilli. A perfo- rated diverticulum was found in the descending colon. There was a dense, inflammatory infiltrate surrounding the perforated area, containing gram-positive bacilli.
CASE 3 A 58-year-old male was diagnosed as having diffuse
histiocytic lymphoma in March 1984 following a CT- guided biopsy of an intraabdominal mass. Initial treat- ment consisting of nitrogen mustard, vincristine, procar- bazine, and prednisone was without benefit, and he was referred to the Cleveland Clinic Foundation for autolo-
TABLE I. Complete Antemortern Blood Count Values on Patients 1-3
Patient Parameter 1 2 3
RBC 2.10 1.37 0.13 ( x 10’2/Iiter) Hemoglobin 7.4 5.7 3.9 (gmW Hcmatocrit 0.130 0.069 0.006 MCV 61.8 50.1 46.8
MCH 35.3 41.7
MCHC 51.1 83.2
RDW 35.1 19.6 35.0”
- (fl)
(Pg)
(%)
-
(units)
aCCF RDW normal < 15 units.
gous bone marrow transplanation. Following bone mar- row harvest he received a course of chemotherapy which included cytosine arabinoside and VP- 16. Nearing the completion of the chemotherapy regimen, he experienced a sudden change in mental status, gross painless hematu- ria, and a temperature rise to 40°C (oral). The physical examination revealed a lethargic white male. His blood pressure was 100/50, pulse was 130 and regular, and respirations were 30 and labored. The skin was cool with peripheral livedo reticularis. There were multiple pur- puric areas on the lower extremities. Coarse breath sounds were noted in both lung fields. The heart exam was normal. There was a mass measuring 5 X 6 cm in the right inguinal region. Stool was positive for blood. No focal neurologic deficits were present. Laboratory findings were as follows: white blood count 0.27 X lo9/ liter, hemoglobin 3.9 gm/dl, platelets 11.0 X lO’/liter, prothrombin time 22 seconds (control of 12 seconds), partial thromboplastin time 55 seconds (normal 21-3 1 seconds), fibrin degradation products present (see Table I and Hematopathologic Findings). Blood cultures were positive for C. perfkingens. The patient’s status rapidly deteriorated despite supportive efforts, and he expired. Autopsy revealed malignant lymphoma (large cell type) with extensive involvement of the small bowel, stomach, diaphragm, retroperitoneum, mediastinum, pericardium, and pleura. Perforation of the duodenum and jejunum at sites of tumor infiltration was present.
HEMATOPATHOLOGIC FINDINGS The immediate antemortem CBC values on the three
patients are seen in Table I. Blood counts were generated on a Coulter S+IV instrument with a data terminal. In addition to the usual eight-parameter CBC values, this
a W m z 3 z w ? G J W K
2 5 10 15 20 25
CUBIC MICROMETERS ( fU
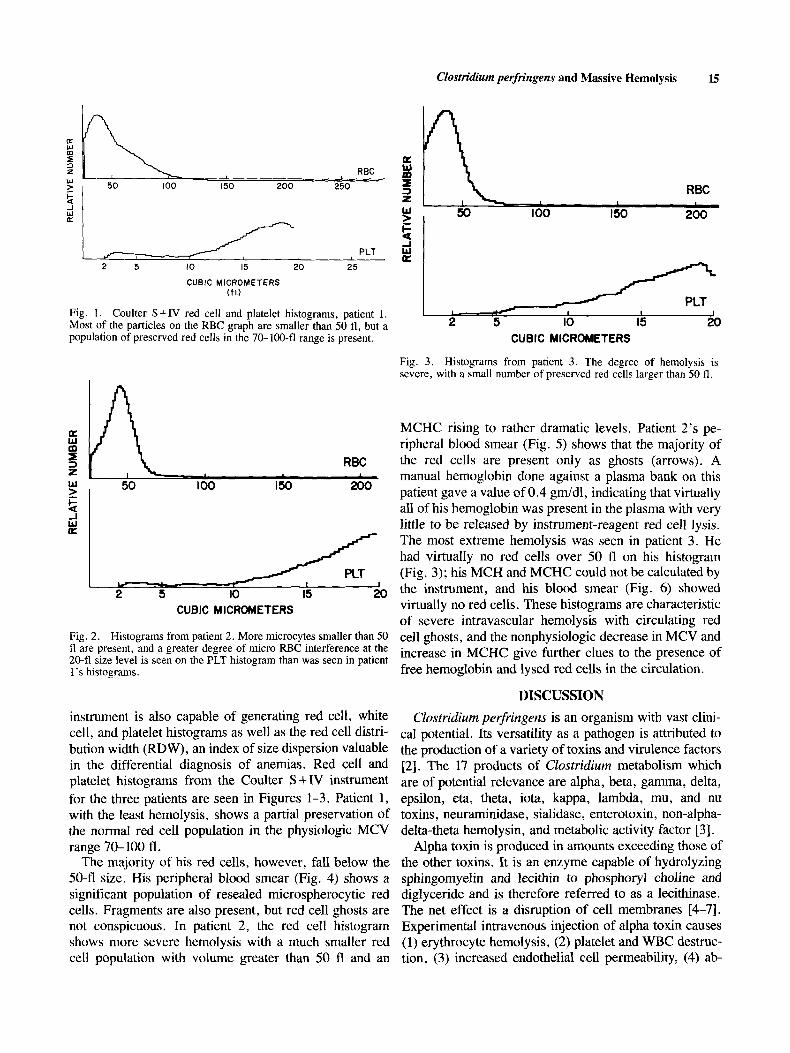
Fig. 1. Coulter S+IV red cell and platelet histograms, patient 1. Most of the particles on the RBC graph are smaller than 50 fl, but a population of preserved red cells in the 70-100-fl range is present.
t I i I
CUBIC MICROMETERS
Fig. 2. Histograms from patient 2. More microcytes smaller than 50 fl are present, and a greater degree of micro RBC interference at the 20-fl size level is seen on the PLT histogram than was seen in patient 1 's histograms.
instrument is also capable of generating red cell, white cell, and platelet histograms as well as the red cell distri- bution width (RDW), an index of size dispersion valuable in the differential diagnosis of anemias. Red cell and platelet histograms from the Coulter S + IV instrument for the three patients are seen in Figures 1-3. Patient 1, with the least hemolysis, shows a partial preservation of the normal red cell population in the physiologic MCV range 70-100 fl.
The majority of his red cells, however, fall below the 504 size. His peripheral blood smear (Fig. 4) shows a significant population of resealed microspherocytic red cells. Fragments are also present, but red cell ghosts are not conspicuous. In patient 2, the red cell histogram shows more severe hemolysis with a much smaller red cell population with volume greater than 50 fl and an
Clostridium perfringens and Massive Hemolysis 15
c w 4 a
PLT L I J 2 5 10 15 20
CUBIC MICROMETERS
Fig. 3. Histograms from patient 3. The degree of hemolysis is severe, with a small number of preserved red cells larger than 50 fl.
MCHC rising to rather dramatic levels. Patient 2's pe- ripheral blood smear (Fig. 5) shows that the majority of the red cells are present only as ghosts (arrows). A manual hemoglobin done against a plasma bank on this patient gave a value of 0.4 gm/dl, indicating that virtually all of his hemoglobin was present in the plasma with very little to be released by instrument-reagent red cell lysis. The most extreme hemolysis was seen in patient 3. He had virtually no red cells over 50 fl on his histogram (Fig. 3); his MCH and MCHC could not be calculated by the instrument, and his blood smear (Fig. 6) showed virtually no red cells. These histograms are characteristic of severe intravascular hemolysis with circulating red cell ghosts, and the nonphysiologic decrease in MCV and increase in MCHC give further clues to the presence of free hemoglobin and lysed red cells in the circulation.
DISCUSSION Clostridium perfringens is an organism with vast clini-
cal potential. Its versatility as a pathogen is attributed to the production of a variety of toxins and virulence factors [2]. The 17 products of Clostridiurn metabolism which are of potential relevance are alpha, beta, gamma, delta, epsilon, eta, theta, iota, kappa, lambda, mu, and nu toxins, neuraminidase, sialidase, enterotoxin, non-alpha- delta-theta hemoly sin, and metabolic activity factor [3].
Alpha toxin is produced in amounts exceeding those of the other toxins. It is an enzyme capable of hydrolyzing sphingomyelin and lecithin to phosphoryl choline and diglyceride and is therefore referred to as a lecithinase. The net effect is a disruption of cell membranes [4-71. Experimental intravenous injection of alpha toxin causes (1) erythrocyte hemolysis, (2) platelet and WBC destruc- tion, (3) increased endothelial cell permeability, (4) ab-

16 Becker et a1
Fig. 4. Blood smear from patient 1. Resealed microspherocytes (M) and an erythroblast (E) are present. An intact red cell is present centrally (Wright’s stain, original magnification X 630).
Fig. 5 . Blood smear from patient 2. A lymphocyte (L) and a few red cells are seen, but most of the erythrocytes are poorly visualized ghosts (arrows) (Wright’s stain, original magnifica- tion X630).
normal blood clotting, (5) marrow suppression of all cell and synergistic role in human infection remains incom- lines, (6) erythrophagocytosis, and (7) hepatic mitochon- pletely defined. Various effects have been recognized and drial dysfunction [S]. include (1) increased gastrointestinal wall permeability,
The other clostridial toxins are felt to be of less clinical (2) increased vascular permeability within the heart, significance than alpha toxin; however, their individual lungs, central nervous system, and peripheral tissues, (3)

Clostridiurn perfringens and Massive Hemolysis 17
Fig. 6. Blood smear from patient 3 . Ghosts (arrow) and a few poorly reserved microcytes are present (Wright’s stain, X630).
pulmonary hemorrhage, (4) myonecrosis, (5) conduction defects within the heart, and (6) erythrocyte hemolysis
The most common sites of C. pelffingens infection are the gastrointestinal and genitourinary tracts. Infection may result from intraabdominal or intrapelvic processes such as trauma, surgery, colonic perforation, cholecysti- tis, liver abscess, peptic ulcer, diverticulitis, septic abor- tion, and ruptured ectopic pregnancy [13-161. Large series reflect the diverse nature of this organism and its potential to infect other areas as well [ 11.
There exists a poor correlation between the underlying disease process and the presence of C. perjkingens bac- teremia. Further, bacteremia may be transient, asympto- matic, and spontaneous [ 17- 191. However, bacteremia may also result in the classic syndrome of massive hem- olysis, hemoglobinemia, hemoglobinuria, hyperkalemia, renal failure, coagulopathy, and hemorrhage followed by shock and death, as evidenced by our three patients [20-
Studies have shown C. peflingens, as well as other species of Clostridium, to be important pathogens in patients with neoplastic disease, particularly those with leukemia, lymphoma, and solid tumors of the colon and genitourinary tract 21-24. Gastrointestinal tract obstruc- tion and/or ulceration is often documented and therefore is felt to be the primary site of entry. However, in many cases the site of entry cannot be identified. [25-281.
A cancer patient’s susceptibility to infection results from (1) significant and often prolonged neutropenia, (2)
[9-121.
221.
inadequate neutrophil function with decreased migration and phagocytosis, (3) decreased antibody synthesis in response to antigenic stimuli, (4) impaired T-cell func- tion, (5 ) frequent and prolonged treatment with broad- spectrum antibiotics favoring the emergence of resistant organisms, and (6) the occurrence of bowel mucosa dis- ruption secondary to malnutrition, tumor infiltration, chemotherapy, and/or radiation therapy [29-321. Once infection has occurred, the cancer patient’s ability to control or limit infection is impaired, favoring progres- sion [33-341.
COMMENT Clostridium perjiiingens is an organism with extraor-
dinary versatility. Infection may vary in its presentation from a transient bacteremia to fatal hemolysis. Patients with malignant disease are prone to developing Clostri- dium infections of the more serious variety. Pathophysi- ologic mechanisms underlying its actions remain incompletely defined, particularly those which are re- sponsible for its ultimate clinical expression. The role of clostridial toxins and the factors which regulate their synthesis, release, and clinical response require further investigation.
REFERENCES 1. Gorbach SL, Thadepalli H: Isolation of Clostridium in human
infections. Evaluation of 114 cases. J Infect Dis [Suppl] 131 S:81- 85, 1975.
2. Smith LDS: Virulence factors of Clostridium perfringens. Rev Infect Dis 1:254-260, 1979.

18 Becker et a1
3. MacLennan JD: The toxicity of clostridial enzymes. Trans NY Acad Sci 16:14-19, 1953.
4. Bull CG, Pritchett JW: Toxin and antitoxin of and protective inoculation against Bacillus welchii. J Exp Med 26: 117-138, 1917.
5. Nagler FPO: Observations on a reaction between the lethal toxin of Clostridium welchii (type A) and human serum. Br J Exp Pathol20:473-485, 1939.
6. MacFarlane MG, Knight BDJG: The biochemistry of bacterial toxins. Biochem J 35:884-902, 1941.
7. Smyth CJ, Arbuthnott JP: Properties of Clostridium perfringens type A alpha toxin (phospholipase C) purified by electrofocusing. J Med Microbiol 7:41-66, 1974.
8. Furr WE, Bourdeau RV, Roach HD, Laufman H: In vivo effects of Clostridium welchii lecithinase. Surg Gynecol Obstet 95:465- 471, 1952.
9. Pivnick H, Hauschild AHW, Gorenstein B, Habeeb AFS: Effect of controlled pH on toxinogenesis by Clostridium perfringens type D. Can J Microbiol 11:45-55, 1965.
10. Buxton D, Morgan KT: Studies of lesions produced in the brains of colostrum deprived lambs by Clostridium welchii-type D toxin. J Comp Pathol 86:435-477, 1976.
11. Mallin ML, Seeley HW: Some relations of hydrogen peroxide to oxygen consumption by Clostridium perfringens. Arch Biochem Biophysiol73:306-314, 1958.
12. Craig JP, Miles AA: Some properties of the iota-toxin of Clostri- dium welchii including its action on capillary permeability. J Pathol Bacteriol 81:481-493, 1961.
13. Bennett JM, Healey PJ: Spherocytic hemolytic anemia and acute cholecystitis caused by Clostridium welchii. N Engl J Med
14. Dayton NA: Gas bacillus infection with perforated gastric ulcer. Boston Med Surg Gen 193:507-508, 1925.
15. Isham RL, Finch SC: Post abortal Clostridium welchii sepsis with massive hemolysis. N Engl J Med 254:317-319, 1956.
16. Smucker EE, Reid SE, Harding HB: Spontaneous fatal gas gan- grene septicemia. JAMA 174:898-900, 1960.
17. Henry H, Lacey M: Anaerobes responsible for gas gangrene in man. J Pathol Bacteriol23:281-288, 1920.
18. Ramsey AM: The significance of Clostridium welchii in the cervical swab and blood stream in post partum and post abortion
268:1070-1072, 1963.
sepsis. J Obstet Gynecol Brit Emp 56:247-258, 1949. 19. Rathbun HK: Clostridial bacteremia without hemolysis. Arch
Intern Med 122:496-501, 1968. 20. Smith LP, McLean APH, Maughan GB: Clostridium welchii
septotoxemia. Am J Obstet Gynecol 110: 135-149, 1971. 21. Mera CL, Freedman MH: Clostridium liver abscess and massive
hemolysis. Clin Pediatr 23: 126-127, 1984. 22. Moore A, Gottfried EL, Stone PH, Coleman M: Clostridium
perfringens septicemia with detection of phospholipase C activity in serum. Am J Med Sci 271:306-314, 1958.
23. Katlic MR, Derkac WM, Coleman WS: Clostridium septicum infection and malignancy. Ann Surg 193:361-364, 1981.
24. McHenry MC, Martin WJ, Hargraves MM, Baggenstoss AH: Bacteremia due to Clostridium perfringens complicating leuke- mia. Report of a case with associated Clostridium pyelonephritis. Proc Staff Meetings Mayo Clinic 38:23-31, 1963.
25. Wynne J, Armstrong D: Clostridial septicemia. Cancer 29:215- 221, 1972.
26. Lehman TJA, Quinn JJ, Siege1 SE, Ortega JA: Clostridium sep- ticum infection in childhood leukemia. Cancer 40:950-953, 1977.
27. Boggs DR, Frei E, Thomas LB: Clostridial gas gangrene and septicemia in four patients with leukemia. N Engl J Med
28. Jones LE, Wirth WA, Farrow CC: Clostridial gas gangrene and septicemia complicating leukemia. South Med J 53: 863-869, 1960.
29. Bodey GP: Infection in cancer patients. Cancer Treat Rev 2:89- 128, 1975.
30. Ketchel SJ, Rodriquez V: Acute infections in cancer patients. Semin Oncol5:167-179, 1978.
31. Brown RS, Haynes HA, Foley HT, Godwin HA, Berard CW, Carbone PP: Hodgkins disease. Immunologic, clinical and histo- logic features. Ann Intern Med 67:291-302, 1967.
32. Holland JF, Senn H, Banerjee T: Quantitative studies of localized leukocyte mobilization in acute leukemia. Blood 37:499-511, 1971.
33. Lehrer RI, Cline MJ: Leukocyte candidacidal activity and resis- tance to systemic candidiasis in patients with cancer. Cancer
34. Inagaki J, Rodriguez VC, Body GP: Causes of death in cancer
259:1255-1258, 1958.
27: 1211-1217, 1971.
patients. Cancer 33:568-573, 1974.