marital quality, marital disruption, and immune functionpni.osumc.edu/kg publications...
TRANSCRIPT

Marital Quality, Marital Disruption, andImmune Function
JANICE K. KIECOLT-GLASER, PHD, LAURA D. FISHER, BS,PAULA OGROCKI, BS, JULIE C. STOUT, BS, CARL E. SPEICHER, MD,and RONALD GLASER, PHD
Marital disruption is associated with significant increases in a variety of psychologic andphysical disorders. In order to examine psychologic and physiologic mediators, self-report dataand blood samples were obtained from 38 married women and 38 separated/divorced women.Among married subjects, poorer marital quality was associated with greater depression and apoorer response on three qualitative measures of immune function. Women who had beenseparated 1 year or less had significantly poorer qualitative and quantitative immune functionthan their sociodemographically matched married counterparts. Among the separated/divorcedcohort, shorter separation periods and greater attachment to the (ex)husband were associatedwith poorer immune function and greater depression. These data are consistent with epide-miologic evidence linking marital disruption with increased morbidity and mortality.
INTRODUCTION
Marital quality appears to be an impor-tant factor in psychologic well-being. Datafrom national surveys suggest that maritalhappiness contributes far more to globalhappiness than any other variable, includ-ing satisfaction with work and friendships(1). Persistent problems within marriagesare reliably associated with increased dis-tress, and unmarried people are happieron the average than those in troubled mar-iages (1, 2).
However, even the end of a troubled re-lationship may have significant conse-
From the Department of Psychiatry (J.K.K.-G.;L.D.F.), Department of Medical Microbiology and Im-munology (P.O.; J.C.S.; R.G.), and Department of Pa-thology (C.E.S.), The Ohio State University Collegeof Medicine, Columbus, OH 43210.
Address reprint requests to: Janice K. Kiecolt-Glaser,Ph.D. Department of Psychiatry, Ohio State Univer-sity College of Medicine, 473 West 12th Avenue, Co-lumbus, OH 43210.
Received for publication March 3, 1986; revisionreceived June 17, 1986.
quences: marital disruption is one of themost stressful life events (3). Divorced andseparated individuals have poorer mentaland physical health than comparable mar-ried, widowed, or single adults (3-5). Sep-arated and divorced adults are dispropor-tionately represented in both inpatient andoutpatient psychiatric populations (5, 6),with admission rates approximately sixtimes as high as married individuals (3).This population also shows a higher in-cidence of clinical depression (7).
In addition to greater psychologicsymptomatology, marital disruption is alsostrongly associated with increased healthrisks. Marital disruption is the single mostpowerful sociodemographic predictor ofstress-related physical illness, with sepa-rated individuals having about 30% moreacute illnesses and physician visits thanmarried adults (8). Separated/divorcedadults have the highest rates of acute med-ical problems, of chronic medical condi-tions that limit social activity, and of dis-ability, even when age, race, and income
Psychosomatic Medicine Vol. 49, No. 1 Oan./Feb. 1987)
Copyright © 1987 by the American Psychosomatic Society, IncPublished by Elsevier Science Publishing Co . Inc52 Vanderbilt Avenue, New York, NY 10017
13
0033-3174/87/S3 50

J. K. KIECOLT-GLASER et al.
are controlled (9); of particular relevanceto the present study is the fact that sepa-rated/divorced individuals have higherrates of mortality from certain infectiousdiseases, including up to six times as manydeaths from pneumonia (10).
Attachment theory (11) is the primaryconceptual framework used in the divorceliterature to explain postseparation in-creases in physical and psychologic symp-tomatology. Defining attachment as abonding to the other [similar to Bowlby(12)], Weiss suggests that such bonds, onceformed, are extremely difficult to break.Within this framework, the intensely am-bivalent feelings toward the spouse are afunction of the persistence of attachmentdespite the erosion of love; the inacces-sibility of the spouse following maritaldisruption leads to "separation distress"characterized by increased symptomatol-ogy (13). Since such bonds are normallyformed within the first 2 years of marriage(11), length of marriage is neither a goodpredictor of attachment nor a good pre-dictor of adjustment following divorce (14).Although attachment and distress are bothrelated to a variety of situational changesproduced by marital disruption, attach-ment feelings appear to cause distress,rather than vice versa (15). Factors that areassociated with less attachment includegreater time since separation, the devel-opment of a new relationship (15), andbeing the initiator of the separation (15-18).
Available data indicate that psychologicadaptation following separation occurs overa several-year period. Weiss (11) suggeststhat the establishment of a more resilientand stable identity may take 2-4 years. Intheir longitudinal sample, Wallerstein andKelly (19) found that it was 3.3 years afterseparation before the average woman's lifeassumed a sense of coherence and stabil-ity; however, it is noteworthy that 5 years
after separation 42% of their female sub-jects had not fully adjusted to their di-vorce. Data from Cartwright (20) showdepression-related alterations in REM sleepthat persisted 2 years after divorce in asample of women. We were interested inthe possibility that there were distress-related alterations in immune function as-sociated with marital disruption, espe-cially in view of the prolonged elevationsin distress found across studies.
Health-related epidemiologic studies onmarital disruption have most often aggre-gated individuals without considering thetime lapse since marital separation or pos-sible psychologic mediators of underlyingphysiologic changes. This study addressesthe psychologic and immunologic con-comitants of marital quality and maritaldisruption. We chose to examine immunefunction because research on the interre-latedness of the immune and neuroendo-crine systems provides evidence of path-ways through which distress-producingevents may modulate immune function andhealth (21-23).
In order to study the psychologic andimmunologic concomitants of maritalquality and marital disruption, we col-lected self-report data and blood samplesfrom 38 married women and 38 separated/divorced women. A battery of six immu-nologic assays provided information onboth qualitative or functional and quan-titative aspects of cellular immunity.
We tested three hypotheses concerningmarital quality and marital disruption inthis cross-sectional study: 1) Among mar-ried subjects, higher marital satisfactionwas expected to be associated with bettermental health and immunologic function-ing (24, 25). 2) Within the separated/di-vorced subject group, it was expected thatattachment to the (ex)husband would beinversely related to psychologic and im-
14 Psychosomatic Medicine Vol. 49, No. 1 (Jan./Feb. 1987)

MARRIAGE, DIVORCE, AND IMMUNITY
munologic functioning. 3) It was expectedthat the short-term consequences of mar-ital disruption would be increased distressand physical symptomatology, i.e., womenwho had been separated for 1 year or lesswould, as a group, have poorer immuno-logic and psychologic functioning than anage- and sociodemographically matchedmarried comparison sample.
METHOD
Subjects
Data were collected from 38 separated/divorcedwomen and 38 married women. Both married andseparated/divorced subjects were recruited in severalways to provide a heterogeneous sample. We placedads in a suburban newspaper distributed free of chargeto households in Columbus. A pastor recruited eightsubjects from his congregation (four married and fourseparated/divorced). We recruited a total of eightwomen from Parents Without Partners (PWP). Thesesubjects were paid $10 for the blood draw and com-pletion of questionnaires, with the exception of thesubjects from Parents Without Partners, where theorganizational bylaws require that the money be paidto the chapter treasury. We also recruited a quarterof the sample (10 married women and 8 separated/divorced women) from the psychology undergradu-ate subject pool by making announcements in theevening classes that had older students. For thesesubjects experimental participation was one methodof fulfilling a course research requirement. The datawere collected from groups of 2 to 20 subjects at atime, with concurrent data collection from marriedand separated/divorced individuals. During the latterphase of the study we had more separated/divorcedwomen than married women; to be sure that we wouldhave matched groups, we selectively recruited mar-ried women of the appropriate age and SES fromresponses to further newspaper ads. Thus, with theexception of the PWP group, the two groups of sub-jects were recruited from similar sources.
As the study progressed we attempted to balancethe two groups on certain interrelated sociodemo-graphic dimensions, including age, education, socio-economic status of the (ex)husband, length of mar-riage, relative number of childless marriages, andnumber of children. Other studies have emphasized
the importance of these variables as mediators ofpostdivorce adjustment (16, 19, 26, 27). The educa-tion of the (ex)wife and the SES of the (ex)husbandhave been important variables in past divorce re-search because they are both related to change (orlack thereof) in the financial circumstances of womenafter divorce. Women most frequently experiencedownward mobility on the economic ladder follow-ing a divorce, and more severe financial strains areassociated with poorer divorce adjustment (26). Inaddition, women who have more education have lessrestricted occupational choices, and may suffer lesseconomic hardship (14).
Subjects were screened by telephone prior to par-ticipation, and the same health-related questions werealso included in their questionnaire packet. Potentialsubjects could not be using any prescription or non-prescription medication with possible immunologicconsequences, nor could they have any acute orchronic health problems that might have an immu-nologic or endocrinologic component. Subjects whowere pregnant or who had recently given birth or hadrecent surgeries were excluded, as were those whoreported drinking more than ten alcoholic drinks perweek.
The separated/divorced group was limited to womenwho had separated from their husbands within theprevious 6 years. We used the date of the actual sep-aration, rather than the divorce date for those whohad completed formal court proceedings, becauseevidence suggests that distress is maximal within thefirst year after separation (27).
The divorce literature clearly indicates that maritaldisruption may be quite different for men and womenfor a variety of reasons (27), including a more pro-longed period of adjustment for certain subgroups ofwomen. Since we were not able to double our sampleto adequately study both sexes, we chose to use onlyfemale subjects.
Self-Report Data
History and Demographic Data. Questions in-cluded length of marriage, timing of separation anddivorce, and frequency and degree of satisfaction withdating relationships since the separation. FollowingPettit and Bloom (18), initiator status was determinedby the response to the question of who made thedecision to separate, with possible responses of 1) itwas completely my decision, 2) it was mostly mydecision, 3) it was a mutual decision, 4) it was mostlymy husband's decision, and 5) it was completely my
Psychosomatic Medicine Vol. 49, No. 1 (Jan./Feb. 1987) 15

J. K. KIECOLT-GLASER et al.
husband's decision. Subjects were classified as ini-tiators if they said that the decision was completelyor mostly theirs or a mutual one.
Health status data included medication usage andrecent alcohol intake. Subjects were asked how manyhours of sleep they had had in the previous 3 days,as well as the amount of any weight changes in theprevious week. They were asked the number of daysthey had been unable to perform their normal dailyactivities in the previous 2 months due to acute ill-ness, and the number of physician visits during thesame period.
Distress/Depression. The 53-item Brief SymptomInventory (BSI; 28) provided information on ninesymptom indices and three global scales. The scalesof particular interest for the present study were thedepression scale and the global severity index (GSI),with the latter providing a summary distress mea-sure. Subjects rated the degree of associated discom-fort during the past week for each item from 0 [notat all) to 4 (extremely). The BSI raw scores for sub-jects were converted to T-scores values, using thenormative tables for nonpsychiatric subject samples,so that the values can be compared to the normalpopulation mean of 50 (SD = 10).
Marital Quality. The 32-item Dyadic AdjustmentScale (DAS; 29) was given to married subjects. TheDAS is one of the most commonly used scales inmarital research, and there are good data supportingits reliability and validity (30-32). Married subjectswere asked to respond based on their relationshipwith their husband over the previous 6 months.
Attachment. The Attachment Scale was devel-oped by Kitson (15) to operationalize attachment af-ter separation and divorce. The items assess preoc-cupation with the (ex)spouse, and disbelief about theseparation/divorce. Responses on the 4-point scalerange from "not at all" to "very much," with higherscores indicating greater attachment. Although at-tachment and distress are both related to a variety ofsituational changes produced by marital disruption,attachment feelings appear to cause distress, ratherthan vice versa (13, 15). Research with the scale hasprovided evidence of its reliability and validity (13,15, 30).
Loneliness. Loneliness has frequently been re-ported as a problem for separated/divorced individ-uals (17, 26, 33). In particular, loneliness may be alonger-term problem for adults after divorce (34).Loneliness is also of interest because of its theoretical
ties to the absence of attachment figures (35) and itsassociation with depressed cellular immunity inmedical students (1, 11) and psychiatric inpatients(36). Therefore, we gave all subjects the four-itemsurvey version of the UCLA Loneliness Scale (37,38).
Life Changes. The Psychiatric EpidemiologicalResearch Inventory Life Events Scale (PERI; 39) wasused to assess the number of major life changes overthe previous year. We were interested in the numberof negative events, since health changes appear to bereliably associated only with negative events (40),and the number of such events is as good a predictoras the weighted sum (41). The PERI data were alsoincluded to help discriminate the contribution of at-tachment from more global distress related to lifechanges, as has been done in previous research (13).
Immunologic Assays. The three functional as-says included blastogenesis with two different mi-togens, concanavalin A (Con A) and phytohemagglu-tinin (PHA), as well as antibody titers to the latentherpesvirus Epstein-Barr virus (EBV), the infectiousagent for infectious mononucleosis. Blastogenesismeasures the proliferative response of lymphocytes,since cellular proliferation following mitogen ex-posure is thought to provide an in vitro model of thebody's response to challenge by infectious agents suchas bacteria or viruses. Bereaved individuals and de-pressed psychiatric patients have lower proliferativeresponses than controls (42, 43), and the respon-siveness of lymphocytes is poorer in blood samplestaken from medical students on examination days,compared to lower-stress baseline days (44).
We measured antibody to EBV because antibodytiters to latent herpesviruses appear to provide anindirect measure of cellular immune system com-petency (45). For example, patients on lmmunosup-pressive therapies like chemotherapy or patients withimmunosuppressive diseases (e.g., AIDS) have char-acteristic elevated herpesvirus antibody titers; ces-sation of an immunosuppressive drug therapy is ul-timately followed by a drop in antibody titers to latentherpesviruses. The increased herpesvirus antibodyproduction in immunosuppressive conditions isthought to reflect the humoral immune system's re-sponse to an increased load of viral antigens. We havepreviously shown large and reliable stress-relatedchanges in antibody titers to EBV and herpes simplexvirus using a Type 1 antigen (HSV-1) in medical stu-dents (46) as well as decrements in HSV-1 antibodytiters in elderly adults following a relaxation inter-vention (47).
Monoclonal antibodies were used to provide data
16 Psychosomatic Medicine Vol. 49, No. 1 (Jan./Feb. 1987)

MARRIAGE, DIVORCE, AND IMMUNITY
on certain quantitative aspects of immune function.Natural killer (NK) cell percentages were assessedbecause NK cells are thought to be an important an-tiviral and antitumor defense. Distress-related changesin NK cell percentages have been found previouslyin medical students (46). Reliable stress-relatedchanges in a functional NK measure, NK cell lysis,have been shown with two different target cells(48-50).
Data on the relative percentages of helper and sup-pressor T lymphocytes were also collected. Helper Tcells stimulate important immunologic activities, in-cluding the production of antibody by B lympho-cytes, an important defense against bacterial infec-tions. Suppressor T cells act to shut off the activityof helper cells when sufficient antibody has beenproduced. Low helper/suppressor cell ratios are as-sociated with immunodeficient conditions (51). Al-terations in the percentages of helper and suppressorcells have been associated with examination stress(44, 49).
NK and T Lymphocyte Subset Assay. The per-centages of helper/inducer T cells, suppressor/cyto-toxic T cells, and helper-to-suppressor cell ratios weredetermined using the monoclonal antibodies OKT-4and OKT-8, respectively (Ortho), as previously de-scribed (49). The Leu-llb monoclonal antibody (Bec-ton-Dickerson) was used to measure the percentageof NK cells.
Briefly, lymphocytes isolated on Hypaque-Ficollgradients were washed with trypsin diluent, thenresuspended in complete RPMI 1640 medium sup-plemented with 20% fetal bovine serum. Monocyteswere removed by placing the cell suspensions inplastic tissue culture flasks and incubating at 37°Cin a CO2 incubator for 2 hr. The nonadherent cellswere washed off and used to determine percentageof T-cell subsets. Lymphocytes (106) were incubatedin 0.01 ml of Leu-llb, OKT-4, or OKT-8 monoclonalantibody for 30 min on ice. Cells were washed withcold RPMI 1640/PBS (1:1), resuspended in goat an-timouse IgG conjugated to fluorescein isothiocyanate(Cappel Laboratories), and incubated for an addi-tional 30 min on ice. The cells were washed andassayed, using an Ortho System 50 fluorescence ac-tivated cell sorter (FACS).
BJastogenesis. Mitogens were used at a final con-centration of 2.5, 5.0, and 10.0 (xg/ml for concana-valin (Con A) and 0.25, 0.5, 1.0 and 2.0 |xg/ml forphytohemagglutinin (PHA). Each assay was per-formed in triplicate. Complete medium supple-mented with 20% fetal bovine serum was used for
baseline controls. One-tenth of a milliliter of mitogenwas added to 1 x 105 lymphocytes (in 0.1 ml com-plete medium) in 96 well plates, and incubated at37°C for 48 hr. Fifty microliters of tritiated thymidine(10 (j.Ci/ml, specific activity 83 Ci/mM) were addedto each well and the plates incubated at 37°C for 4hr. Cells were harvested onto GF/A filters. Radioac-tivity was measured using a Beckman LS7000 scin-tillation counter. The data are presented as the countsper minute (cpm) in the stimulated samples minusthe cpm of the unstimulated samples (A cpm). Alogarithmic transformation was performed on the re-sulting values.
Immuno/luorescence Assay. The indirect im-munofluorescence (IF) assay was used to measureantibodies to EBV virus capsid antigen (VCA) (46).Antibody titers were assayed using smears of HR-lcells. Cells were fixed in acetone at room temperaturefor 10 min, adsorbed with twofold dilutions of plasmaprepared in phosphate-buffered saline (PBS) pH 7.4,for 30 min at 37°C. The cells were washed with PBSand readsorbed with goat antihuman IgG conjugatedto fluorescein isothiocyanate (FITC) for 30 min at37°C. The cells were washed with PBS, counter-stained with Evans blue, mounted in Protex, and ex-amined with a Zeiss UV microscope. Antibody titerswere determined by the highest dilution of plasmastill able to demonstrate IF positive cells. All slideswere read blind coded.
Nutritional Assays
Albumin and transferrin, two nutritional assayswith relatively shorter and longer half-lives, wereincluded to provide objective information on the nu-tritional status of subjects. There are well-docu-mented impairments in various aspects of immunefunction in undernourished individuals, and mod-erate to severe protein-caloric malnutrition is asso-ciated with increased frequency and severity of in-fection (52).
Protein assays provide better information on globalnutritional status than those for carbohydrates andfats, since the former have varied nutritional buildingblocks, as well as very complex synthetic pathways.Different protein markers were used because of thedifferences in their half-lives; the half-life of albuminis 2-3 weeks, in comparison to 8 days for transferrin.
The procedure used to measure albumin is an ad-aptation of the bromcresol green dye-binding methodof Rodkey (53), later modified by Doumas (54). Thisprocedure is recognized as a particularly good pro-cedure as compared to other dye-binding techniques
Psychosomatic Medicine Vol. 49, No. 1 (Jan./Feb. 1987) 17

J. K. KIECOLT-GLASER et a l .
because of its specificity and freedom from interfer-ence.
Transferrin is an iron-transporting protein. Con-centration in plasma is affected by dietary intake ofiron. Nutritionally deficient but calorie-rich diets aregenerally lacking in iron, and, as a result, plasmairon levels tend to be low and transferrin levels high.It has been shown that estimation of transferrin levelsmay be used to assess the effectiveness of total par-enteral nutrition (55).
A rate nephelometry procedure using a Beckmanhuman immunoglobulin reagent kit and a Beckmanimmunochemistry analyzer system was used to ana-lyze transferrin levels. Antibody to human transfer-rin was used in the assay, in which the peak ratesignal caused by the antigen/antibody complex isproportional to the increase in light scatter that isread by the instrument (56).
RESULTS
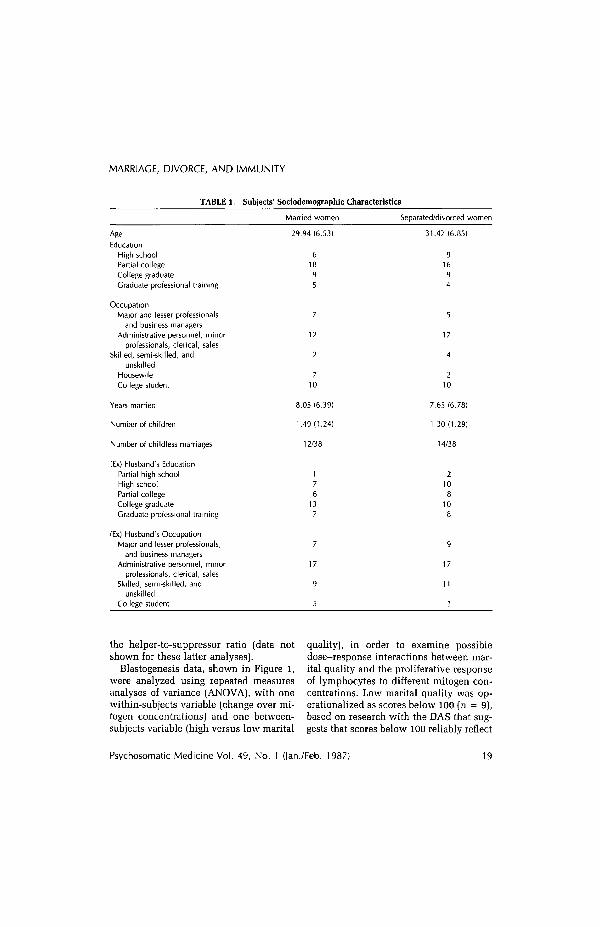
Table 1 provides sociodemographic in-formation on married and separated/di-vorced cohorts. The two groups do not dif-fer reliably on age F(l,75) = 1.30, educationF(l,75) = 1.11, or occupation, F < 1, the(ex)husband's education, F(l,75) = 1.30,or occupation, F < 1, number of years mar-ried, F < 1, or number of children, F < 1.
We do not have data on all immunologicassays for all subjects due to occasionaltechnical problems, e.g., insufficient num-bers of cells for assays, or technical diffi-culties with an assay. In addition, con-sistent with seroepidemiologic studies (57),89% of our subjects were EBV seroposi-tive, i.e., had previously been exposed tothe virus and thereafter were latently in-fected. Thus, those subjects who were notpreviously infected did not have antibodydata.
Marital Quality
The mean DAS score for the 38 marriedsubjects was 110.98 (SD = 13.00). Forcomparison purposes, Spanier (29) re-
ported that the mean score on the DAS ina normative married sample that includedboth men and women was 114.8 (SD =14.8).
Marital quality was not significantly dif-ferent for those subjects who had children(DAS mean = 109.92, SD = 14.27) andthose who did not (mean = 112.67, F <1. DAS scores did not correlate signifi-cantly with number of children, r = - 0.08.There were not significant correlations be-tween marital quality and a number ofvariables, including age (r = -0.15), sub-jects' education (r = - 0.08), or years mar-ried (-0.15).
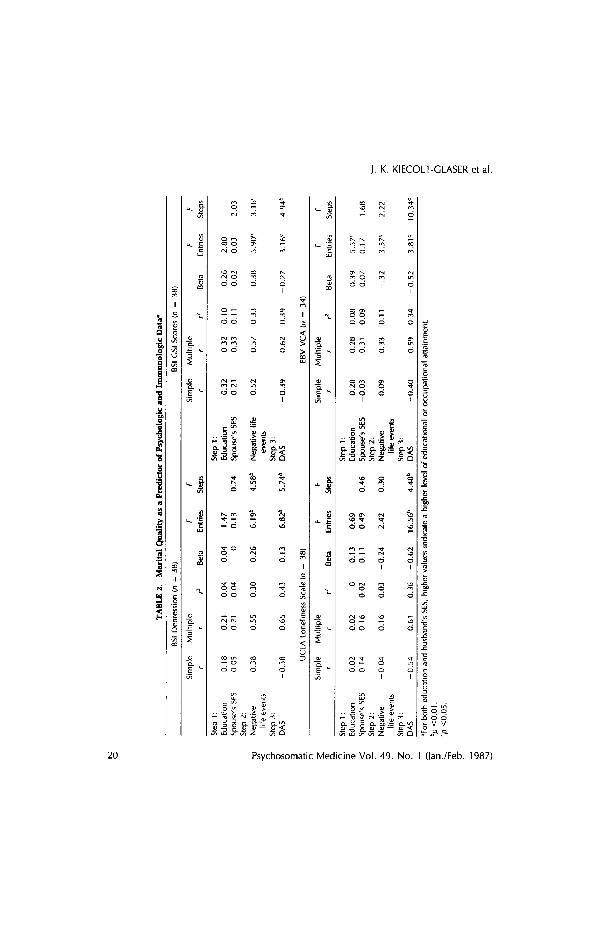
Multiple regression equations were usedto evaluate the contribution of maritalquality to psychologic and immunologicfunctioning. Using a hierarchical proce-dure, the subject's educational level andthe husband's Hollingshead SES were en-tered on the first step, the number of neg-ative life changes in the previous year wasentered on the second step, and maritalquality was entered on the third step. Thisanalysis provides a fairly strict evaluationof the contribution of marital quality, sincelower socioeconomic status and greaternumbers of negative life changes have beenassociated with greater distress and poorerhealth. It also provides information on theextent to which this set of variables pre-dicts certain immunologic and psycho-logic indices.
As can be seen in Table 2, poorer maritaladjustment was a strong and significantpredictor of BSI depression and GSI scores,as well as loneliness, even after taking outthe significant contribution of recent neg-ative life changes. Poorer marital qualitywas also strongly and positively related toEBV VCA antibody titers, or poorer cel-lular immune system control of virus la-tency. None of the variables significantlypredicted the three quantitative assays, or
18 Psychosomatic Medicine Vol. 49, No. 1 Gan./Feb. 1987)
MARRIAGE, DIVORCE, AND IMMUNITY
TABLE 1. Subjects' Sociodemographic Characteristics
Married women Separated/divorced women
EducationHigh schoolPartial collegeCollege graduateGraduate professional training
OccupationMajor and lesser professionals
and business managersAdministrative personnel, minor
professionals, clerical, salesSkilled, semi-skilled, and
unskilledHousewifeCollege student
Years married
Number of children
Number of childless marriages
(Ex) Husband's EducationPartial high schoolHigh schoolPartial collegeCollege graduateGraduate professional training
(Ex) Husband's OccupationMajor and lesser professionals,
and business managersAdministrative personnel, minor
professionals, clerical, salesSkilled, semi-skilled, and
unskilledCollege student
29.94 (6.53)
61895
7
12
2
710
8.05 (6.39)
1.49 (1.24)
31.47(6.85)
5
17
4
210
7.65 (6.78)
1 30(1.29)
14/38
the helper-to-suppressor ratio (data notshown for these latter analyses).
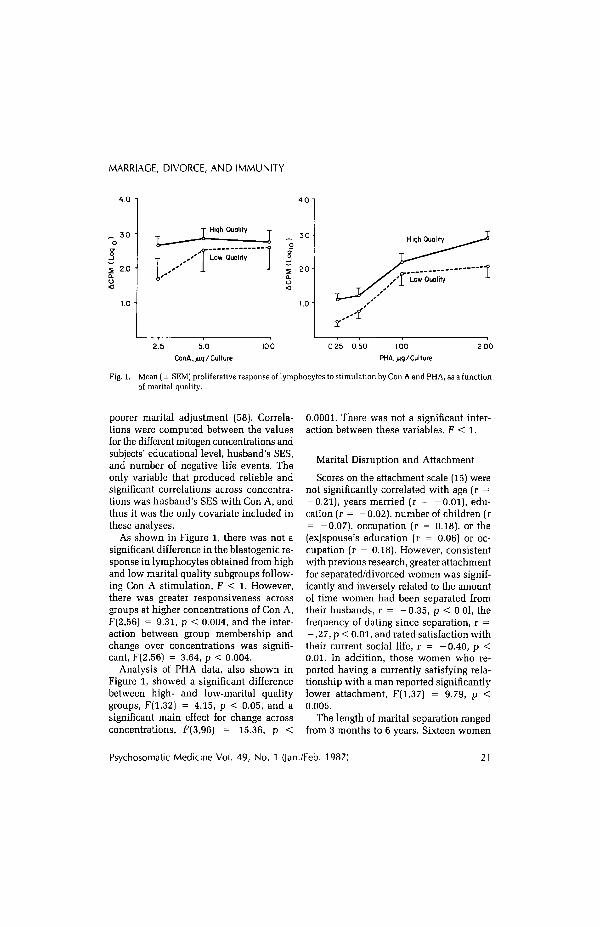
Blastogenesis data, shown in Figure 1,were analyzed using repeated measuresanalyses of variance (ANOVA), with onewithin-subjects variable (change over mi-togen concentrations) and one between-subjects variable (high versus low marital
quality), in order to examine possibledose-response interactions between mar-ital quality and the proliferative responseof lymphocytes to different mitogen con-centrations. Low marital quality was op-erationalized as scores below 100 (n = 9),based on research with the DAS that sug-gests that scores below 100 reliably reflect
Psychosomatic Medicine Vol. 49, No. 1 (Jan./Feb. 1987) 19
MARRIAGE, DIVORCE, AND IMMUNITY
,-. 3 0 •
2.0 •
High QualityT - 30
' I Low Quality
2 0 -
i . o -
High Quality
2.5 5.0ConA,/iq/Culture
100 0 25 0.50 100PHA, jug/Culture
2.00
Fig. 1. Mean (± SEM) proliferative response of lymphocytes to stimulation by Con A and PHA, as a functionof marital quality.
poorer marital adjustment (58). Correla-tions were computed between the valuesfor the different mitogen concentrations andsubjects' educational level, husband's SES,and number of negative life events. Theonly variable that produced reliable andsignificant correlations across concentra-tions was husband's SES with Con A, andthus it was the only covariate included inthese analyses.
As shown in Figure 1, there was not asignificant difference in the blastogenic re-sponse in lymphocytes obtained from highand low marital quality subgroups follow-ing Con A stimulation, F < 1. However,there was greater responsiveness acrossgroups at higher concentrations of Con A,F(2,56) = 9.31, p < 0.004, and the inter-action between group membership andchange over concentrations was signifi-cant, F(2,56) = 3.64, p < 0.004.
Analysis of PHA data, also shown inFigure 1, showed a significant differencebetween high- and low-marital qualitygroups, F(l,32) = 4.15, p < 0.05, and asignificant main effect for change acrossconcentrations, F(3,96) = 15.36, p <
0.0001. There was not a significant inter-action between these variables, F < 1.
Marital Disruption and Attachment
Scores on the attachment scale (15) werenot significantly correlated with age (r =-0.21), years married (r = -0.01), edu-cation (r = -0.02), number of children (r= -0.07), occupation (r = 0.18), or the(ex)spouse's education (r = 0.06) or oc-cupation (r = 0.18). However, consistentwith previous research, greater attachmentfor separated/divorced women was signif-icantly and inversely related to the amountof time women had been separated fromtheir husbands, r = -0.35, p < 0.01, thefrequency of dating since separation, r =- .27, p < 0.01, and rated satisfaction withtheir current social life, r = -0.40, p <0.01. In addition, those women who re-ported having a currently satisfying rela-tionship with a man reported significantlylower attachment, F(l,37) = 9.79, p <0.005.
The length of marital separation rangedfrom 3 months to 6 years. Sixteen women
Psychosomatic Medicine Vol. 49, No. 1 (Jan./Feb. 1987) 21
J. K. KIECOLT-GLASER et al.
had been separated 1 year or less. The meanseparation length was 1.72 years (SD =1.43), and the median was 1.26 years. Sevensubjects were separated but not divorced.Nine of the 38 subjects said they did nothave primary responsibility for the sepa-ration, a percentage consistent with pre-vious research (18).
It was possible that the PWP groups andthose who attended church regularly mightdiffer systematically as a function of greatersocial support. The four groups of subjectsrecruited from the newspaper ads, PWP,the church, and the evening psychologyclasses were compared on loneliness, theBSI depression, and GSI scales. There wereno significant differences within the sep-arated/divorced population on any of thethree dimensions as a function of recruit-ment source, F < 1.
Length of time since separation was en-tered on the first step of the multipleregression equations, since it appears tobe an extremely important factor in ad-justment (e.g., 11,19). Education and hus-band's SES were also entered on the first
step, since education and husband's SEShave been shown to be associated withpostseparation adjustment, as previouslydescribed. The number of negative lifeevents was entered on the second step ofthe equation, to help discriminate the con-tribution of attachment from more globaldistress related to life changes, as has beendone in previous research (13). Subjects'scores on the attachment scale were en-tered on the third step. Thus, the analysesprovide a fairly stringent test of the con-tribution of attachment to the total vari-ance, while concurrently providing infor-mation on the contributions of time sinceseparation, relevant socio demographicvariables, and negative life changes to totalvariance.
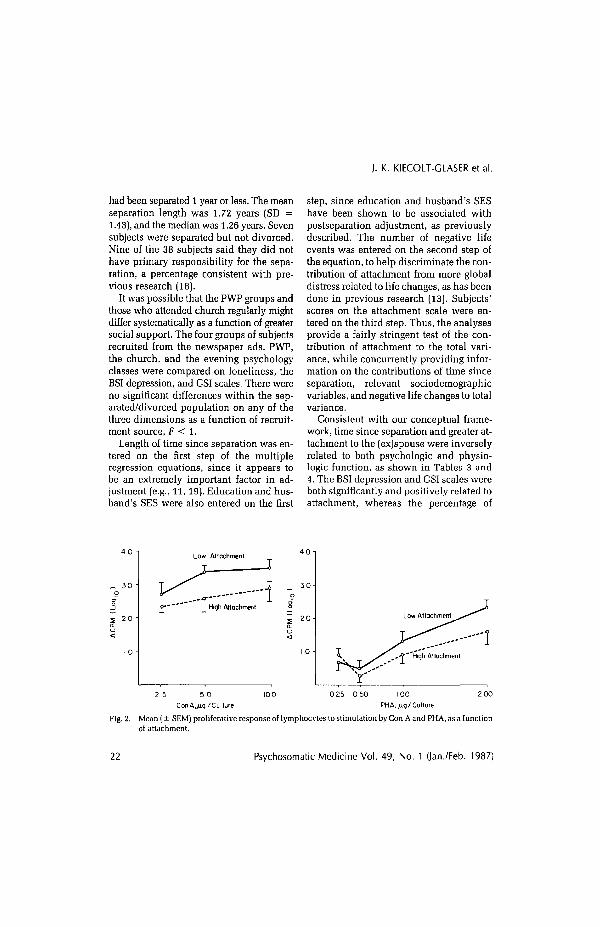
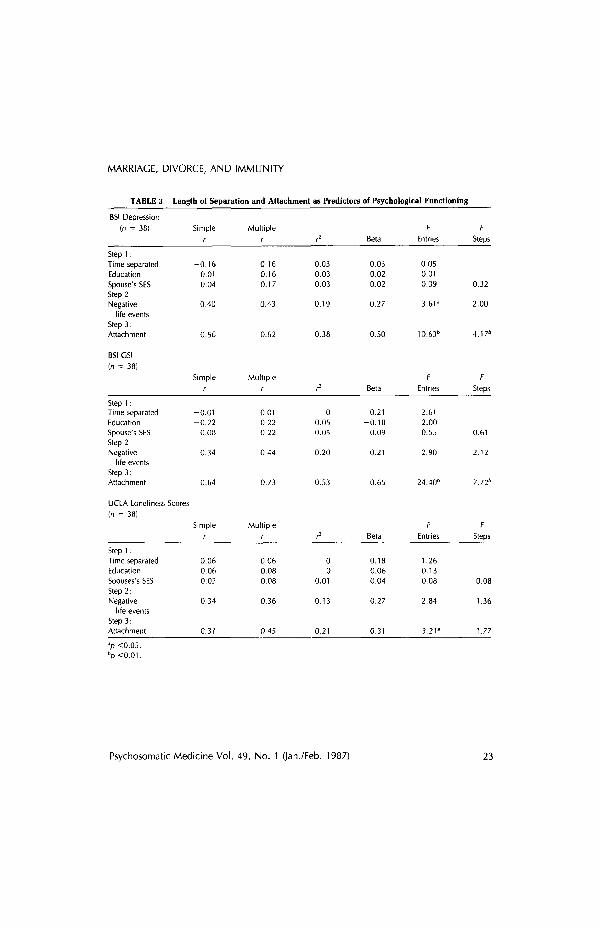
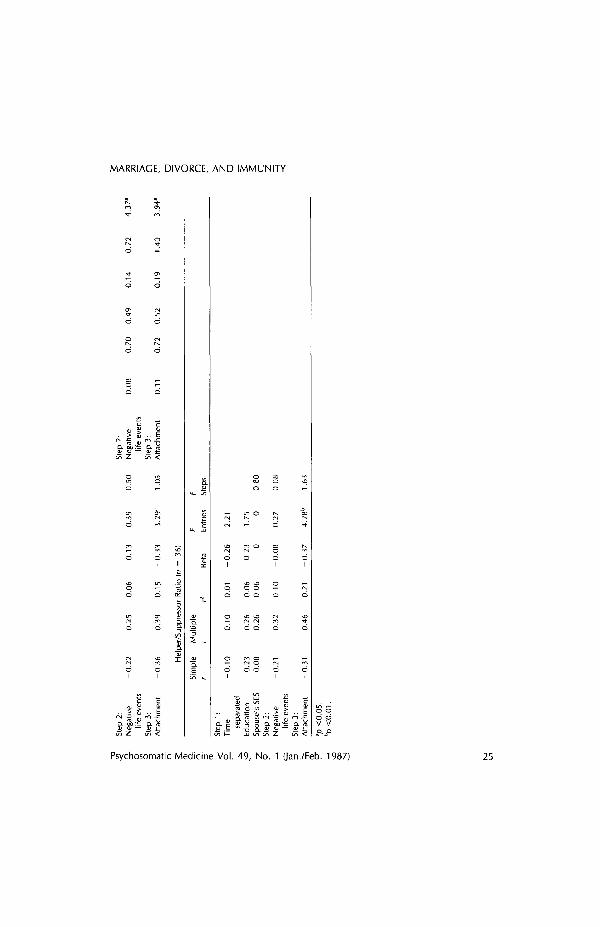
Consistent with our conceptual frame-work, time since separation and greater at-tachment to the (ex)spouse were inverselyrelated to both psychologic and physio-logic function, as shown in Tables 3 and4. The BSI depression and GSI scales wereboth significantly and positively related toattachment, whereas the percentage of
_ 30 •
Low Attachment
£ J High AttachmentLow Attachment
2 002 5 5 0 100 0 25 0 50 100Con A./iq/ Culture PHA./iq/Culture
Fig. 2. Mean (± SEM) proliferative response of lymphocytes to stimulation by Con A and PHA, as a functionof attachment.
22 Psychosomatic Medicine Vol. 49, No. 1 Qan./Feb. 1987)
MARRIAGE, DIVORCE, AND IMMUNITY
TABLE 3. Length of Separation and Attachment as Predictors of Psychological Functioning
BSI Depression
(n = 38)
Step 1:Time separatedEducation
Spouse's SESStep 2.Negative
life eventsStep 3:Attachment
BSI CSI
(n = 38)
Step 1:Time separatedEducationSpouse's SESStep 2:Negative
life eventsStep 3:Attachment
UCLA Loneliness Scores(n = 38)
Step 1:Time separatedEducationSpouses's SESStep 2:Negative
life eventsStep 3:Attachment
Simpler
-0 .160.010.04
0.40
0.56
Simpler
-0 .01-0.22
0.08
0.34
0.64
Simpler
0.060.060.02
0.34
0.31
Multipler
0.160.160.17
0.43
0.62
Multipler
0.010.220 22
0.44
0.73
Multipler
0.060.080.08
0.36
0.45
r2
0.030.030.03
0.19
0.38
r2
00.050.05
0.20
0.53
r2
00
0.01
0.13
0.21
Beta
0.030.020.02
0.27
0.50
Beta
0.21-0.18
0.09
0.21
0.65
Beta
0.180.060.04
0.27
0.31
F
Entries
0.050.010.09
3.61a
10.636
F
Entries
2.612.000.55
2.90
24.40"
F
Entries
1.260.130.08
2.84
3.21a
F
Steps
0.32
2.00
4.176
F
Steps
0.61
2.12
7.726
F
Steps
0.08
1.36
1.773p <0.05.bp<0.01.
Psychosomatic Medicine Vol. 49, No. 1 (Jan./Feb. 1987) 23
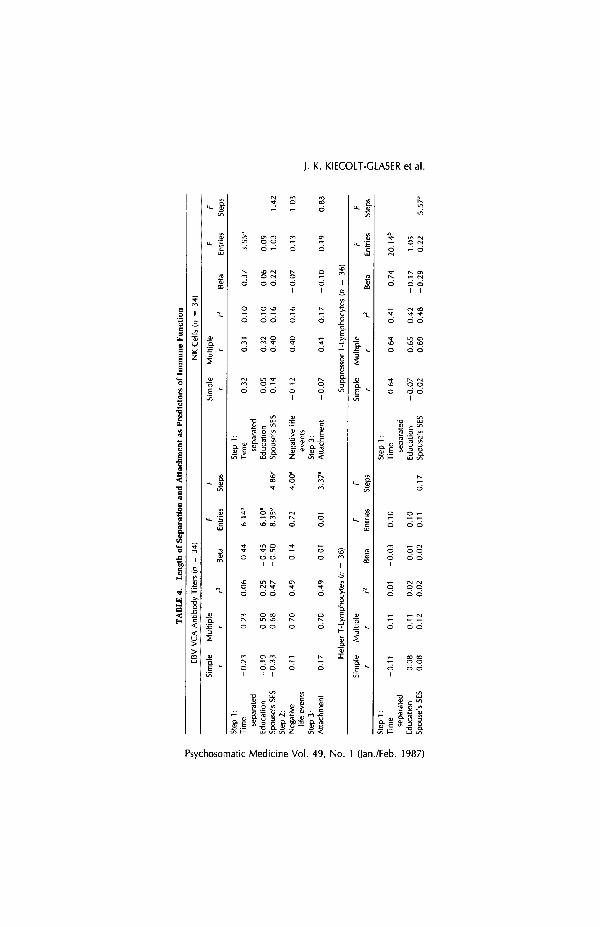
TABLE 4
. L
engt
h of
Sep
arat
ion
an
d A
ttac
hmen
t as
Pre
dic
tors
of
Imm
une
Fu
nct
ion
EB
V V
CA
Ant
ibod
y T
iters
(n
= 3
4)
NK
Cel
ls (
n =
34)
Sim
ple
Mu
ltip
le
F F
S
impl
e M
ult
iple
F
F r
r rZ
B
eta
Ent
ries
Ste
ps
r r
r2
Bet
a E
ntrie
s St
ews
Ste
p 1:
Ste
p 1
: T
ime
-0.2
3
0.2
3
0.0
6
-0.4
4
6.14
" T
ime
0.3
2
0.3
1
0.1
0
0.3
7
3.5
5"
sepa
rate
d se
para
ted
Edu
catio
n -0
.19
0.5
0
0.2
5
-0.4
5
6.1
0a
Edu
cat~
on
0.0
5
0.3
2
0.1
0
0.0
6
0.0
9
Spo
use'
s SE
S -0
.33
0.6
8
0.4
7
-0.5
0
8.
35
b4
.8
6d
Spo
use'
s SE
S 0.1
4
0.4
0
0.1
6
0.2
2
1 .O
3 1.
42
Ste
p 2:
N
egat
ive
0.11
0.7
0
0.4
9
0.1
4
0.7
2
4.00
" N
egat
ive
life
-0
12
0.4
0
0.1
6
-0.0
7
0.1
3
1.0
3
life
eve
nts
even
ts
-
Ste
p 3
. S
tep
3:
Atta
chm
ent
0.1
7
0.7
0
0.4
9
0 0
1 0.
01
3.3
7a
Atta
chm
ent
-0.0
7
0.41
0
.17
-0
.10
0
.19
0.8
3
7C
5
Hel
per
T-L
ymph
ocyt
es (n
= 3
6)
Sup
pres
sor T
-Lym
phoc
ytes
(n
= 3
6)
$;
Sim
ple
Mu
lt~
ple
F
F
S
impl
e M
ult
iple
r
r rZ
B
eta
Ent
ries
Ste
ps
r r
r2
eta
i
s st:ps
Ste
p 1:
S
tep
1 :
P T
ime
-0.1
1
0.11
0.0
1
-0.0
3
0.10
T
ime
0.6
4
0.6
4
0.4
1
0.7
4
20.1
4b
R rn
sepa
rate
d se
para
ted
7~
E
duca
t~on
0.0
8
0.1
1
0.0
2
0.0
1
0.1
0
Edu
catio
n -0
.07
0.6
5
0.4
2
-0.1
7
1.0
5
2
Spo
use'
s SE
S 0.0
8
0.1
2
0.02
0.0
2
0.11
0.1
7
Spo
use'
s SE
S -0
.02
0.6
9
0.4
8
-0.2
9
0.2
2
5.5
7d
MARRIAGE, DIVORCE, AND IMMUNITY
Q. S)^= Q. rg
.11Q. DO "^ Cl.
o od dV V
Psychosomatic Medicine Vol. 49, No. 1 (Jan./Feb. 1987) 25

J. K. KIECOLT-GLASERetal.
helper T lymphocytes and the helper-sup-pressor ratio were inversely related to at-tachment. The percentage of suppressor Tlymphocytes showed a strong positive cor-relation with length of separation, whereasthe percentage of NK cells was inverselyrelated to length of separation.
Attachment scores were divided at themedian, 8.5, to form high- and low-attach-ment subgroups for blastogenesis anal-yses. There were significant differences re-lated to attachment in the proliferativeresponse of lymphocytes exposed to ConA. The difference between groups was sig-nificant, F(l,26) = 4.47, p < 0.05, as wasthe usual increase in responsiveness withdifferent mitogen concentrations, F(2,62)= 10.17, p < 0.0002, whereas the inter-action between these two variables was notsignificant, F < 1. Response of lympho-cytes to PHA stimulation produced a non-significant difference between groups, F <1, and a significant change over concen-trations, F(3,78) = 21.69, p < 0.0001. Theinteraction between these two variables wassignificant, however, with greater differ-ences at higher concentrations, F(3,78) =3.77, p < 0.01. Correlations were com-puted between the values obtained at dif-ferent mitogen concentrations and lengthof separation, education, husband's SES,and number of negative life events. Onlylength of separation showed a reliably sig-
nificant relationship across PHA signifi-cant correlations, so it was the only co-variate used in the analyses (Fig. 2).
Comparisons Between RecentlySeparated Women andMarried Women
The mean BSI depression T-score (58.25,SD = 9.80) in the newly separated subjectswas not significantly different from that oftheir married counterparts (54.47, SD =5.59), F(l,31) = 2.14, p < 0.15. Similarly,there was not a significant difference onthe GSI, F < 1. Data from the UCLA didnot discriminate between the two groups,F < 1.
Comparisons of sociodemographic datadid not show significant differences be-tween the 16 women who had separatedwithin the previous year and the 16matched married women. They did notdiffer in age, number of children, or theHollingshead education or occupationalstatus of themselves or their spouse, withall Fs < 1. The two groups did not differsignificantly in their distribution acrossstages of the menstrual cycle.
As predicted, there were reliable im-munologic differences between the womenwho had been separated 1 year or less andtheir married counterparts, as shown inTable 5. The separated/divorced women
TABLE 5. Mean (± SDS) for the 16 Women Who Were Separated 1 Year or Lessand 16 Matched Married Women
Separated/Divorced Women Married Women
EBV VCAa
Percentage of helper T lymphocytes"Percentage of suppressor T lymphocytesHelper-suppressor ratioPercentage of NK cellsa
520.5026.4320.01
1.497.50
(706.84)(7.59)(6.70)(0.66)(5.05)
147.1232.9122.66
1.6912.79
(191.88)(7.03)(7.76)(1.47)(8.05)
'p <0.05.
26 Psychosomatic Medicine Vol. 49, No. 1 (Jan./Feb. 1987)
MARRIAGE, DIVORCE, AND IMMUNITY
30 -
20 -
10 -
Married
Separated / Divorced
2 5 50ConA,>iq/Culture
3 0
10 0
Separated / Divorced
0 50 100PHA,/iq/ Culture
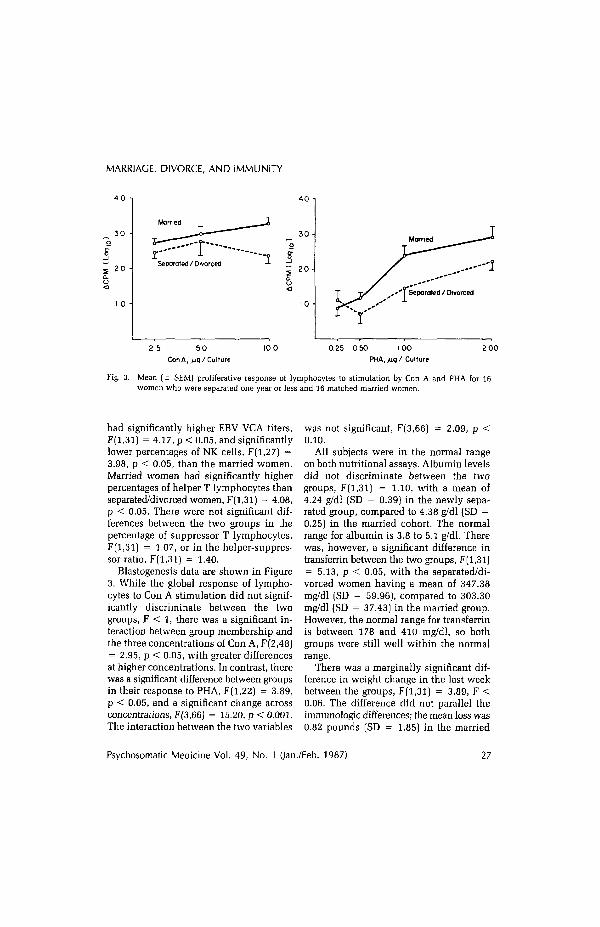
Fig. 3. Mean (± SEM) proliferative response of lymphocytes to stimulation by Con A and PHA for 16women who were separated one year or less and 16 matched married women.
had significantly higher EBV VCA titers,F(l,31) = 4.17, p < 0.05, and significantlylower percentages of NK cells, F(l,27) =3.98, p < 0.05, than the married women.Married women had significantly higherpercentages of helper T lymphocytes thanseparated/divorced women, F(l,31) = 4.08,p < 0.05. There were not significant dif-ferences between the two groups in thepercentage of suppressor T lymphocytes,F(l,31) = 1.07, or in the helper-suppres-sor ratio, F(l,31) = 1.40.
Blastogenesis data are shown in Figure3. While the global response of lympho-cytes to Con A stimulation did not signif-icantly discriminate between the twogroups, F < 1, there was a significant in-teraction between group membership andthe three concentrations of Con A, F(2,48)= 2.95, p < 0.05, with greater differencesat higher concentrations. In contrast, therewas a significant difference between groupsin their response to PHA, F(l,22) = 3.89,p < 0.05, and a significant change acrossconcentrations, F(3,66) = 15.20, p < 0.001.The interaction between the two variables
was not significant, F(3,66) = 2.09, p <0.10.
All subjects were in the normal rangeon both nutritional assays. Albumin levelsdid not discriminate between the twogroups, F(l,31) = 1.10, with a mean of4.24 g/dl (SD = 0.39) in the newly sepa-rated group, compared to 4.38 g/dl (SD =0.25) in the married cohort. The normalrange for albumin is 3.8 to 5.1 g/dl. Therewas, however, a significant difference intransferrin between the two groups, F(l,31)= 5.13, p < 0.05, with the separated/di-vorced women having a mean of 347.38mg/dl (SD = 59.96), compared to 303.30mg/dl (SD = 37.43) in the married group.However, the normal range for transferrinis between 178 and 410 mg/dl, so bothgroups were still well within the normalrange.
There was a marginally significant dif-ference in weight change in the last weekbetween the groups, F(l,31) = 3.89, F <0.06. The difference did not parallel theimmunologic differences; the mean loss was0.82 pounds (SD = 1.85) in the married
Psychosomatic Medicine Vol. 49, No. 1 (Jan./Feb. 1987) 27

J. K. KIECOLT-GLASER et al.
group, compared to a mean gain of 0.43(SD = 1.82) in the newly separated group.
The two groups did not differ in amountof sleep in the previous 3 days, F < 1. Bothreported about 23 hr of sleep, or an averagedeficit of 1 hr. There were not significantdifferences between the newly separatedsubjects in the number of days they wereill during the previous 2 months, or in thenumber of physician visits for the treat-ment of acute illness, Fs < 1.
Overall Group Comparisons:Separated/Divorced vs. Married
We did not predict overall differencesbetween the separated/divorced and themarried cohorts, since our separated/di-vorced subjects, as a group, had been sep-arated for some period of time. However,comparisons between the entire marriedand separated/divorced cohorts showedsome significant differences on the psy-chologic variables, and on the functionalassays, blastogenesis and EBV antibody ti-ters, as well as in NK cell percentages.
There was a strong significant differ-ence between married and separated/di-vorced subjects on depression, F(l,75) =12.11, p < 0.001, but not for the GSI, F(l,75]= 1.45. The means for depression were59.65 (SD = 9.02) in the separated di-vorced group and 53.11 (SD = 7.27) in themarried group. Scores on the short formof the UCLA did not discriminate betweenthe groups, F(l,75) = 1.53, with a meanof 7.75 (SD = 2.29) in the separated/di-vorced group, compared to 7.13 (SD = 2.06)among married women. For comparisonpurposes, in a telephone survey of work-ing adults in a large city, the mean scorefor adults in the same age range as oursubjects was 7.99 (SD = 1.96) (38).
The difference in antibody titers to EBVwas significant, F(l,68) = 4.01, p < 0.05,
with married subjects having significantlylower antibody titers (mean = 149.23, SD= 233.46) than the separated/divorcedgroup (mean = 462.05, SD = 513.96). Theseparated/divorced subjects had signifi-cantly lower percentages of NK cells thanmarried subjects. F(l,65) = 8.96, p < 0.01,with a mean of 7.31 (SD = 6.10) in theformer and 11.93 (SD = 6.42) in the latter.There were not significant differences inthe percentages of helper or suppressor Tlymphocytes, or the helper-suppressorratio, Fs < 1.
The separated/divorced and marriedsubjects were also significantly differentin their lymphocytes' response to PHAstimulation, F(l,58) = 4.28, p < 0.05, andin the interaction between group mem-bership and change over concentrations,F(3,74) = 7.00, p < 0.0003. The main ef-fect for change over concentrations wassignificant as well, F(3,174) = 58.65, p <0.0001. For separated/divorced subjects themeans for the four concentrations of PHAwere 1.14 (SD = 1.24), 0.82 (SD = 1.11),1.53 (SD = 1.25), and 2.16 (SD = 1.32).The comparable means for married sub-jects were 0.90 (SD = 1.17), 1.11 (SD =1.15), 2.45 (SD = 0.76), and 3.05 (SD =0.65).
There was neither a significant differ-ence between these groups on response toCon A, nor a significant interaction be-tween group membership and change overconcentrations, Fs < 1.
The two groups did not differ signifi-cantly in amount of sleep in the last threedays, F < 1. Weight change data paralleledthe newly separated group, with an aver-age loss of 0.86 lb (SD = 2.51) in the mar-ried subjects, compared to a mean gain of0.14 lb (SD = 1.93) in the separated/di-vorced group, F(l,75) = 4.08, p < 0.05.Although there were not significant dif-ferences in albumin, F < 1, there was a
28 Psychosomatic Medicine Vol. 49, No. 1 (Jan./Feb. 1987)

MARRIAGE, DIVORCE, AND IMMUNITY
significant difference in transferrin, F(l,64)= 5.39, p < 0.02, with a mean of 335.22(SD = 62.26) in the separated/divorcedgroup, compared to 302.20 (SD - 49.51)for married subjects, with all values fallingwithin normal limits. There were not dif-ferences in days ill or physician visits, Fs< 1.
The two groups did not show differ-ences in smoking behavior, either on packsper week, F < 1, or in the relative pro-portion of smokers to nonsmokers; roughly20% of each group were smokers. The twogroups did differ significantly in alcoholuse over the previous week, F(l,75) = 7.73,p < 0.01, with a mean of 1.92 drinks perweek (SD = 2.44) in the separated/di-vorced group, compared to 0.70 in themarried group (SD = 1.18). No subject re-ported more than ten drinks in the pre-vious week, and only two subjects re-ported having had more than seven drinks.Subjects in the two groups did not differsignificantly in their distribution acrossstages of the menstrual cycle.
DISCUSSION
Poorer marital quality in the married co-hort was a significant predictor of depres-sion and poorer response on the functionalimmunologic assays. These data are con-sistent with previous reports linking thequality of the marital relationship withmental and physical health (25), and theyprovide further evidence for the impor-tance of satisfactory marital relationships.
Data from Levinson and Gottman (59,60) provide evidence of one physiologicpathway through which chronically ab-rasive relationships might mediate im-mune function. They found that greaterautonomic arousal in interacting marriedcouples was strongly predictive of subse-
quent declines in marital satisfaction 3years later. Moreover, they also reportedthat greater declines in marital satisfactionwere strongly correlated with poorer healthratings at follow-up. If there is consistentphysiologic arousal associated with thepresence of a spouse in a disturbed rela-tionship, then it is quite possible that thereare concurrent persistant alterations in en-docrine function that mediate immuno-logic changes (e.g., 61, 62)
We also found that more recent maritalseparation and greater attachment to the(ex)husband were significant predictors ofboth psychologic symptoms and certainaspects of immune function in separated/divorced women. In addition, as pre-dicted, those women who had separatedfrom their husbands within the previousyear had poorer immune function than so-ciodemographically matched marriedwomen, with significantly poorer prolif-eration in response to two mitogens, sig-nificantly lower percentages of NK cellsand helper cells, and significantly higherantibody titers to EBV VCA. These data areconsistent with evidence from epidemio-logic studies indicating that separated in-dividuals have the greatest incidence ofhealth impairments, followed in turn bydivorced adults (9).
It has been suggested that nonmarriedindividuals may have riskier life-styles thanmarried adults, e.g., they may drink, smoke,or use drugs more, thus exposing them-selves to more chronic risks; nutrition andsleep might also differ by marital status(9). We chose a sample that did not abusedrugs or alcohol, so these factors do notdifferentiate between our married and sep-arated/divorced subjects. Although we didnot select our sample by nutrition or sleepcriteria, we find no evidence of consistentdifferences of a magnitude that would ac-count for the immunologic differences.
Psychosomatic Medicine Vol. 49, No. 1 (Jan./Feb. 1987) 29

J. K. KIECOLT-GLASERetal.
Thus, although it is certainly possible thatrisk-related life-style factors may influ-ence health status, our data suggest thatthere may also be persistent immunologicalterations in certain individuals.
There are also data suggesting that mar-ital disruption is associated with a signif-icantly higher incidence of cancer (64).Speculatively, it is possible that the per-sistence of distress or dysphoria followingseparation and divorce in some more vul-nerable individuals (34) could have ad-verse physiologic consequences that wouldincrease cancer risk, including the lowerpercentages of NK cells in the separated/divorced group. In addition, persistentdepression may have consequences at themolecular level in the speed and qualityof DNA repair that could mediate in-creased cancer risk (65, 66).
It should be noted that although the im-munologic changes are not large, these datado provide evidence of longer-term changesin immune function related to psychoso-cial stressors. Evidence consistent withmore chronic stress-related changes in im-munity has only been described in one otherstudy (63). The actual health impact of theserelatively small but presumably persistentchanges in immune function are not known.Although it is possible that these changesmay make some contribution to the greaterincidence of infectious and malignant dis-ease in separated/divorced adults that hasbeen well-documented by others (9-11),the causal links have not been demon-strated.
There are problems with inferences aboutthe direction of causality in cross-sec-tional studies such as this. For example,in the separated/divorced group of womenit is possible that preexisting depressivesymptoms were an underlying cause forthe divorce (e.g., 3); moreover, such symp-toms might have subsequently hampered
the formation of alternative relationships,a factor associated with lower attachment.Similarly, those married women who aremore depressed may view their marital re-lationship as less supportive, and/or theirdepressive symptoms might have adverseeffects on the quality of the marital rela-tionship (67). Although we cannot ex-clude these possibilities, evidence fromother research supports alternative expla-nations.
Using longitudinal survey data, Men-aghan (68) controlled for level of depres-sion prior to marital termination and foundthat depression appeared more likely to bethe result of marital disruption, and of-fered no support for the argument thatpreexisting depression was an importantprecipitant of changes in marital status.Similarly, a 1-year longitudinal study fromMonroe et al. (69) showed that subsequentdepressive symptoms were predicted bylower marital support in 473 women whowere initially relatively asymptomatic andhad nonconflicted marriages. Moreover,other work provides evidence that anotherform of separation distress is a potent me-diator of immune and endocrine functionin nonhuman primates (70).
Turning to the immunologic data, it ap-pears that the three qualitative assays weremore consistently related to the psycho-logic variables than were the three quan-titative assays. In particular, EBV VCA an-tibody titers were significantly related tothe psychologic variables in all four setsof analyses. Herpesvirus antibody titersappear to be quite sensitive to psychologicstressors (71).
Values from the mitogen assays, partic-ularly PHA, were somewhat low; in ourprotocol we used a 48-hr incubation pe-riod in order to minimize variability. Themitogens we used presumably had low po-tency and, in combination with the 48-hr
30 Psychosomatic Medicine Vol. 49, No. 1 (Jan./Feb. 1987)

MARRIAGE, DIVORCE, AND IMMUNITY
incubation period, resulted in low counts.Once the data collection had begun, wewere committed to using the same mito-gens across all subjects so that meaningfulcomparisons could be made. Thus, the re-sultant values are lower than some of thosereported elsewhere. However, although thevalues are low, the differences betweengroups are consistent and significant, re-flecting differences in the proliferative re-sponses of the groups.
Finally, the data from this study are rel-evant for the growing literature on socialsupport and health. The data linking poorermarital quality with depression and poorerimmune function suggest that the simplepresence of a partner is not equivalent toa supportive relationship. Moreover, inseparated/divorced women, greater attach-ment to a man who is no longer present isalso linked to adverse psychologic and im-munologic consequences; a new and sat-isfying relationship is associated with lowerattachment. We have previously found thatloneliness is associated with poorer im-mune function (36, 46, 48). Taken to-gether, it appears that the quality of one'sinterpersonal relationships may havehealth-related consequences.
SUMMARY
Marital disruption is associated withsignificant increases in a number of psy-chologic and physical disorders. In order
to examine psychologic and physiologicmediators, self-report data and blood sam-ples were obtained from 38 married womenand 38 separated/divorced women. Amongthe married subjects, poorer marital qual-ity was associated with greater depressionand a poorer response on the three qual-itative immunologic assays, lymphocyteproliferation in response to two mitogensand antibody titers to EBV VCA. The 16women who had been separated 1 year orless had significantly poorer immunefunction than a sociodemographically-matched married group, including lowerpercentages of NK and helper cells, poorerblastogenic responsiveness, and higherantibody titers to EBV VCA. Within theseparated/divorced group shorter separa-tion times and greater attachment to the(ex)husband were associated with poorerimmune function and greater depression.These data are consistent with epidemio-logic data linking marital disruption withincreased morbidity and mortality.
This study was supported in part by agrant from the American Cancer ResearchFund, by grant No. 1 R01 MH40787 fromthe National Institute of Mental Health,and hy the Ohio State University Com-prehensive Cancer Center Grant No. CA-16058, from the National Cancer Institute,National Institutes of Health. We are verygrateful for the help given by Rev. EvanFisher, Jane Holliday, and Paul Vespa onthis project.
REFERENCES
1. Glenn ND, Weaver CN: The contribution of marital happiness to global happiness. J Marriage Fam43:161-168, 1981
2. Pearlin LI, Lieberman MA: Social sources of emotional distress. In Simmons R (ed), Research in Com-munity and Mental Health. Greenwich, CT, JAI Press, 1979
Psychosomatic Medicine Vol. 49, No. 1 (Jan./Feb. 1987) 31
J. K. KIECOLT-GLASER et al.
3. Bloom BL, Asher SJ, White SW: Marital disruption as a stressor: A review and analysis. Psychol Bull85:867-894, 1978
4. Briscoe CS, Smith JB, Robins E, Marten S, Gaskin F: Divorce and psychiatric disease. Arch Gen Psy-chiatry 29:119-125, 1973
5. Bachrach LL: Marital Status and Mental Disorder: An Analytical Review. Washington D.C., U.S. PrintingOffice, 1975
6. Crago MA: Psychopathology in married couples. Psychol Bull 77:114-128,19727. Blumenthal MD: Mental health among the divorced: A field study of divorced and never divorced
persons. Arch Gen Psychiatry 16:603-608, 19678. Somers AR: Marital status, health, and use of health services. JAMA 241:1818-1822, 19799. Verbrugge LM: Marital status and health. J Marriage Fam 41:267-285, 1979
10. Lynch J: The Broken Heart. New York, Basic, 197711. Weiss RS: Marital Separation. New York, Basic, 197512. Bowlby J: Attachment and Loss: 1. Attachment. New York, Basic, 197513. Brown P, Felton BJ, Whiteman V, Manela R: Attachment and distress following marital separation. ]
Divorce 3:303-317, 198014. Spanier GB, Thompson LJ: Parting: The Aftermath of Separation and Divorce. Beverly Hills, CA, Sage,
198415. Kitson GC: Attachment to the spouse in divorce: A scale and its application. J Marriage Fam 44:379-393,
198216. Kitson GC, Raschke HJ: Divorce research: What we know: what we need to know. J Divorce 4:1-37,
198117. Kelly JB: Divorce: The adult perspective, In Wolman BB (ed), Handbook of Developmental Psychology.
Englewood Cliffs, NJ, Prentice Hall, 198218. Pettit EF, Bloom BL: Whose decision was it: The effects of initiator status on adjustment to' marital
disruption. J Marriage Fam 46:587-595, 198419. Wallerstein JS, Kelly JB: Surviving the Breakup: How Children and Parents Cope With Divorce. New
York, Basic, 198020. Cartwright RD: Rapid eye movement sleep characteristics during and after mood-disturbing events.
Arch Gen Psychiatry 40:197-201, 198321. Ader R (ed): Psychoneuroimmunology. New York, Academic, 198122. Soloman GF: Emotional and personality factors in the onset and course of autoimmune disease, par-
ticularly rheumatoid arthritis. In Ader R (ed), Psychoneuroimmunology. New York, Academic, 198123. Kiecolt-Glaser JK, Glaser R: Behavioral influences on immune function: Evidence for the interplay
between stress and health. In Field T, McCabe PM, Schneiderman N (eds), Stress and Coping. Hillsdale,NJ, Lawrence Erlbaum, in press, Vol II
24. Furstenberg FF, Spanier GB: Recycling the Family: Remarriage After Divorce. Beverly Hill, CA, Sage,1984
25. Renne KS: Health and marital experience in an urban population. J Marriage Fam 23:338-350, 197126. Albrecht SL, Bahr HM, Goodman KL: Divorce and Remarriage. Problems, Adaptations, and Adjustments.
Westport, CT, Greenwood, 198327. Bloom BL, Hodges WF, Kern MB, McFaddin SC: A preventive intervention program for the newly
separated: Final evaluations. Am J Orthopsychiatry 55:9-26, 198528. Derogatis LR, Spencer PM: The Brief Symptom Inventory (BSI), Administration, Scoring, and Procedures
Manual I. Baltimore, Clinical Psychometrics Research, 198229. Spanier GB: Measuring dyadic adjustment: New scales for assessing the quality of marriage and similar
dyads. J Marriage Fam 38:15-28, 197630. Spanier GB, Thompson LJ: Relief and distress after marital separation. J Divorce 7:31^49, 198331. Kitson GC, Langlie JK: Couples who file for divorce but change their minds. Am J Orthopsychiatry
54:469-489, 1984
32. Spanier GB, Castro RF: In Levinger F, Moles OC (eds), Divorce and Separation: Context, Causes, andConsequences. New York, Basic, 1979
32 Psychosomatic Medicine Vol. 49, No. 1 (Jan./Feb. 1987)

MARRIAGE, DIVORCE, AND IMMUNITY
33. Bloom BL, Hodges WF, Caldwell RA: A preventive program for the newly separated: Initial evaluation.Am J Community Psychol 10:251-164, 1982
34. Wallerstein JS: Women after divorce: Preliminary report from a ten-year follow-up. Am J Orthopsy-chiatry 56:65-77, 1986
35. Weiss RS: Issues in the study of loneliness. In Peplau A, Perlman D (eds), Loneliness: A Sourcebookof Current Theory, Research and Therapy. New York, Wiley, 1982
36. Kiecolt-Glaser JK, Ricker D, George J, Messick G, Speicher CE, Garner W, Glaser R: Urinary cortisollevels, cellular immunocompetency, and loneliness in psychiatric inpatients. Psychosom Med 46:15-24,1984
37. Russell D. Peplau LA, Cutrona CB: The revised UCLA Loneliness Scale: Concurrent and discriminantvalidity evidence. J. Person Soc Psychol 39:472-480, 1980
38. Russell D: The measurement of loneliness, in Peplau LA, Perman D (eds): Loneliness: A Sourcebookof Current Theory Research, and Therapy. New York, Wiley, 1982
39. Dohrenwend BS, Krasnoff L, Askenasy AR, Dohrenwend BP: Exemplification of a method for scalinglife events: The PERI Life Events Scale. J Health Soc Behav 19:205-229, 1978
40. Sarason IG, Sarason BR, Potter EH, Antoni MH: Life events, social support, and illness. PsychosomMed 47:156-163, 1985
41. Blaney PH: Stress and depression in adults: A critical review. In Field T, McCabe P, Schneiderman N(eds), Stress and Coping. Hillsdale NJ, Lawrence Erlbaum, 1985
42. Schleifer SJ, Keller SE, Camerino M, Thornton JC, Stein M: Suppression of lymphocyte stimulationfollowing bereavement. JAMA 250:374-377, 1983
43. Schleifer SJ, Keller SE, Meyerson AT, Raskin MJ, Davis KL, Stein M: Lymphocyte function in majordepressive disorder. Arch Gen Psychiatry 41:484-486, 1984
44. Glaser R, Kiecolt-Glaser JK, Stout JC, Tarr KL, Speicher CE, Holliday JE: Stress-related impairments incellular immunity. Psychiatr Res 16:233-239, 1985
45. Glaser R, Gottleib-Stematsky T: Human Herpesvirus Infections: Clinical Aspects. New York, MarcelDekker, 1982
46. Glaser R, Kiecolt-Glaser JK, Speicher CE, Holliday JE: Stress, loneliness, and changes in herpesviruslatency. J Behav Med 8:249-260, 1985
47. Kiecolt-Glaser JK, Glaser R, Williger D, Stout J, Messick G, Sheppard S, Ricker D, Romisher SC, BrinerW, Bonnell G, Donnerberg R: Psychosocial enhancement of immunocompetence in a geriatric popu-lation. Health Psychol 4:25-41, 1985
48. Kiecolt-Glaser JK, Garner W, Speicher CE, Penn G, Glaser R: Psychosocial modifiers of immunocom-petence in medical students. Psychosom Med 46:7-14, 1984
49. Kiecolt-Glaser JK, Glaser R, Strain E, Stout J, Tarr K, Holliday J, Speicher C: Modulation of cellularimmunity in medical students. J Behav Med 9:5-21, 1986
50. Glaser R, Rice J, Speicher CE, Stout JC, Kiecolt-Glaser JK: Stress depresses interferon production andnatural killer cell activity in humans. Behav Neurosci, in press
51. Reinherz EL, Schlossmen SF: Current concepts in immunology: Regulation of the immune response—Inducer and suppressor T-lymphocyte subsets in human beings. N Engl J Med 303:370-373, 1980
52. Chandra RK, Newberne PM: Nutrition, Immunity and Infection: Mechanisms of Interactions. New York,Plenum, 1977
53. Rodkey FL: Direct spectrophotometric determination of albumin in human serum. Clin Chem 11:478^487,1965
54. Doumas BT, Watson WA, Biggs HG: Albumin and the measurement of serum albumin with bromcresolgreen. Clin Chim Acta 31:87-96, 1971
55. Keyser JW: Human Plasma Proteins. New York, Wiley, 197956. Buffone GJ: Transferrin, ICS-14. Fullerton CA, Beckman Instruments, Inc, 198057. Henle W, Henle G: Epstein-Barr virus and infectious mononucleosis. In Glaser R, Gottlieb-Stematsky
T (eds), Human Herpesvirus Infections: Clinical Aspects. New York, Marcel Dekker, 1982
58. Jacobson NS, McDonald DW, Follette WC, Berley RA: Attributional processes in distressed and non-distressed married couples. Cognit Ther Res 9:35-50, 1985
Psychosomatic Medicine Vol. 49, No. 1 (Jan./Feb. 1987) 33

J. K. KIECOLT-GLASER et al.
59. Levenson RW, Gottman JM: Marital interaction: physiological linkage and affective exchange. J PersonSoc Psychol 3:587-597, 1983
60. Levenson RW, Gottman JM: Physiological and affective predictors of change in relationship satisfaction.J Person Soc Psychol 49:85-94, 1985
61. O'Dorisio MS, Wood CL, O'Dorisio TM: Vasoactive intestinal peptide and neuropeptide modulation ofthe immune response. J Immunol 135:792s-796s, 1985
62. Pert CB, Ruff MR, Weber RJ, Herkenham M: Neuropeptides and their receptors: A psychosomaticnetwork. J Immunol 135:820s-826s, 1985
63. Schaeffer MA, McKinnon W, Baum A, Reynolds CP, Rikli P, Davidson LM, Fleming I: Immune statusas a function of chronic stress at Three Mile Island. Psychosom Med 47:85, 1985
64. Ernster BL, Sacks S, Selvin S, Petrakis NL: Cancer incidence by marital status: US third national cancersurvey. ] Natl Cancer Inst 63:587-585, 1979
65. Kiecolt-Glaser JK, Stephens R, Lipitz P, Speicher CE, Glaser R: Distress and DNA repair in humanlymphocytes. J Behav Med 8:311-320, 1985
66. Glaser R, Thorn B, Tarr K, Kiecolt-Glaser JK, D'Ambrosio S: Effects of stress on methyltransferasesynthesis: An important DNA repair enzyme. Health Psychol 4:403—412, 1985
67. Heller K: The effects of social support: Prevention and treatment implications. In Goldstein AP, KanferFH (eds), Maximizing Treatment Gains: Transfer Enhancement in Psychotherapy. New York, Academic,1979
68. Menaghan, EG: Depressive affect and subsequent divorce. J Fam Issues 6:295-306, 198569. Monroe SM, Bromet EJ, Connell MM, Steiner SC: Social support, life events, and depressive symptoms:
A one-year prospective study. J Consult Clin Psychol, 54:424-431, 198670. Coe CL, Levine S: Psychoimmunology: An old idea whose time has come. In Perez T, Chido J, Harvey,
JH (eds), Biological and Behavorioral Correlates of Psychopathology. Lubbock, Texas Tech UniversityPublications, in press
71. Kiecolt-Glaser JK, Glaser R: Psychosocial stress and human herpesvirus infections. In Kurstak E, Li-powski ZJ, Morozov PV (eds), Viruses, Immunity, and Mental Disorders. New York, Plenum, in press.
34 Psychosomatic Medicine Vol. 49, No. 1 (Jan./Feb. 1987)