mandibular angle fractures
TRANSCRIPT

Mandibular angle fractures
Dr. Ahmed M. Adawy Professor Emeritus, Dep. Oral & Maxillofacial Surg.
Former Dean, Faculty of Dental MedicineAl-Azhar University
Mandibular angle fractures account for 23% to 42% of all facial fractures (1). The most common causes of mandibular angle fractures are motor vehicle accident and assaults or violence. There are two main proposed reasons why the angle of the mandible is commonly associated with fractures. The first reason is the presence of a thinner cross-sectional area relative to the neighboring segments of the mandible (2). Second is the presence of third molars, particularly those that are impacted, which weakens the region (3)
Mandibular angle fractures
An importance of classification of mandibular angle fractures relates to direction of the fracture line and effect of muscle action on the fracture fragments. Thus, fractures have been classified as:a. Vertically favorable or unfavorableb. Horizontally favorable or unfavorableMuscles attached to the ramus masseter, temporalis and medial pterygoid displace the proximal segment upward and medially when the fractures are unfavorable; conversely these same muscles tend to impact the bone, minimizing displacement in horizontal and vertical favorable fractures (4)
Mandibular angle fractures
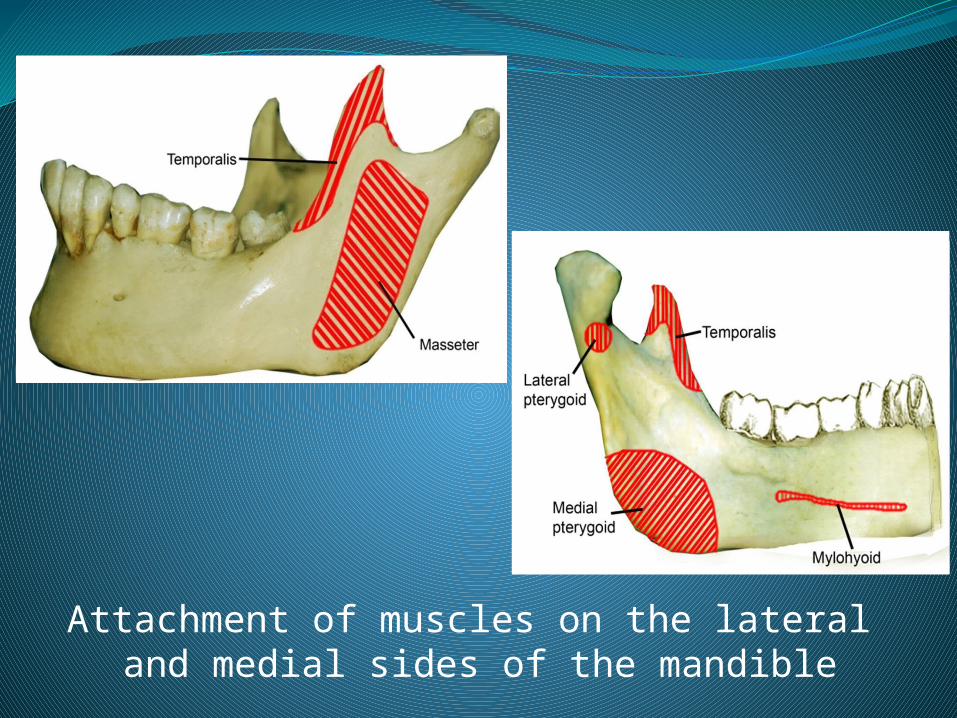
Attachment of muscles on the lateral and medial sides of the mandible
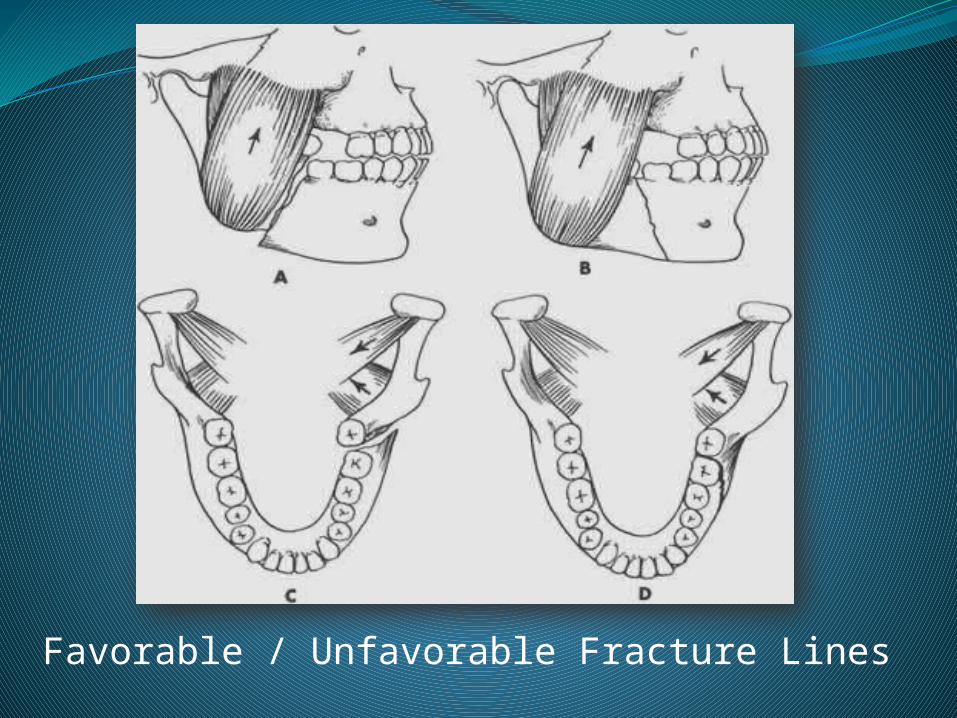
Favorable / Unfavorable Fracture Lines
The traditional way of treating mandibular angle fracture involves reestablishment of a functional dental occlusion with either close reduction and intermaxillary fixation or open reduction and internal fixation with or without intermaxillary fixation. Patients treated with intermaxillary fixation have a restricted airway and loose excess weight. Further, intermaxillary fixation for 8 weeks may cause marked thinning and disruption of the normal organization of the articular cartilage. In addition the use of intermaxillary fixation significantly increased the time patients spent off work (5)
Mandibular angle fractures
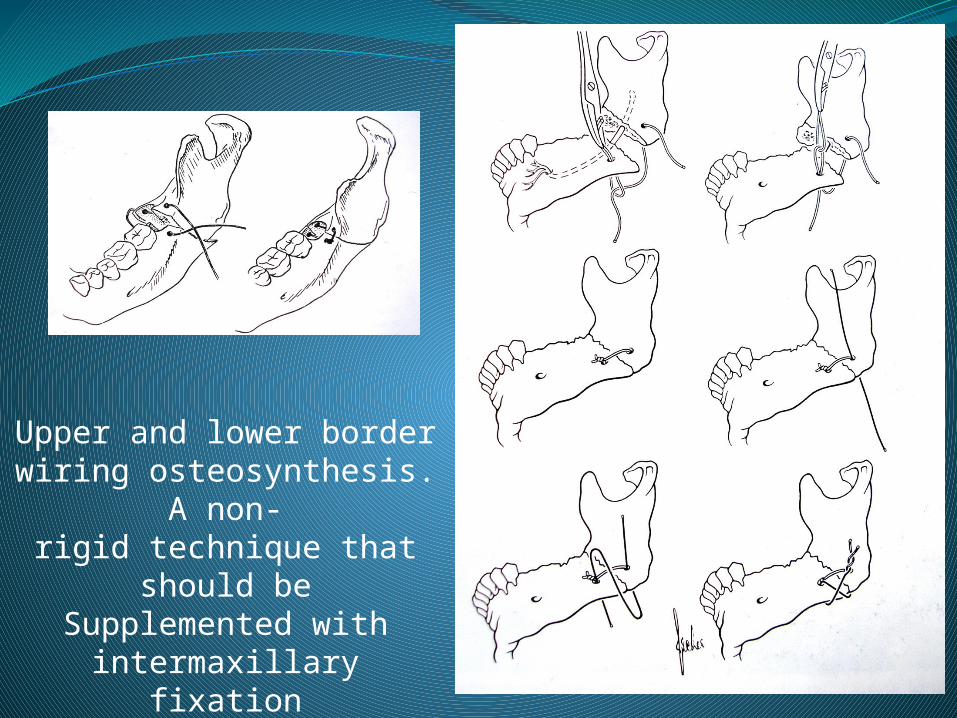
Upper and lower border wiring osteosynthesis. A non-rigid technique that should be
Supplemented with intermaxillary fixation
Rigid internal fixation and early return to function have eliminated the use of wire osteosynthesis and prolonged use of intermaxillary fixation. Meanwhile, rigid fixation is associated with rapid primary bone healing, excellent stabilization at the fracture site, and increased postoperative three-dimensional stability, and results in early and complete restoration of function (6).Traditionally absolute rigid fixation, with reconstruction plate, was believed to be critical to proper union, particularly with comminuted fractures (7). It has been stressed that no other means could be capable of supporting full functional load and withstanding tension forces while maintaining fractures fragments in anatomic position
Mandibular angle fractures
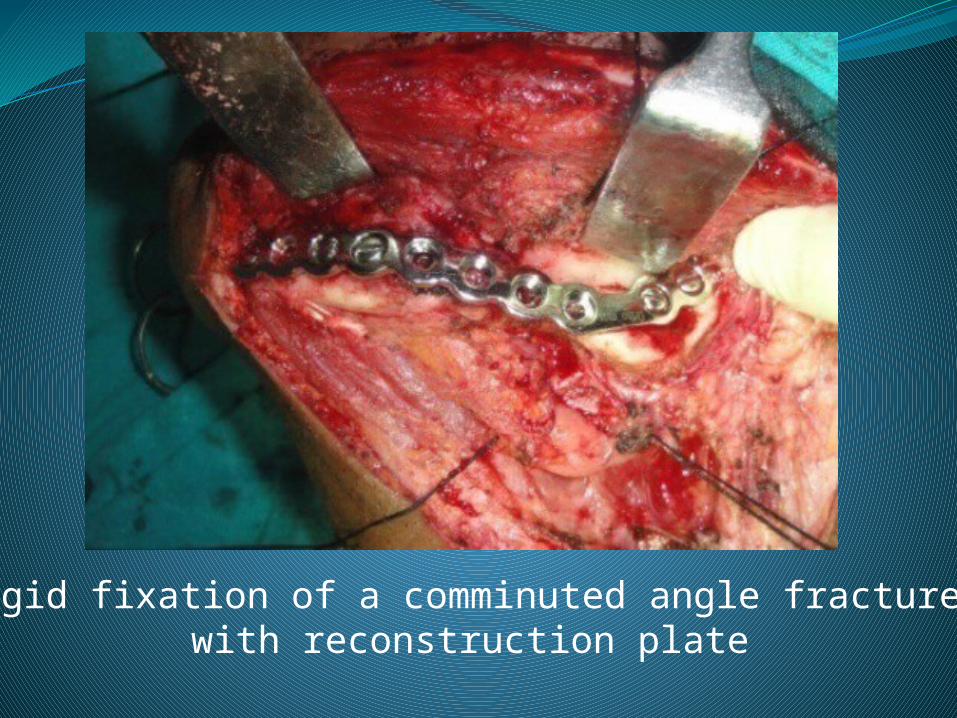
Rigid fixation of a comminuted angle fracture with reconstruction plate
The principle of rigid fixation, however, have an inherent set of disadvantages. The bicortical screws used cause sensory disturbances along path of inferior alveolar nerve in many cases. The possibility of injury to the marginal mandibular branch of facial nerve is high. Postoperative malocclusion rates are also high which attributed to the difficulties in bending the rigid plate. Extraoral scar through which the plate is inserted is an additional complication. Worth mentioning, it has been demonstrated that, up to a point, increased rigidity is associated with increased complications (8)
Mandibular angle fractures
In 1978, Champy et al.(9) proposed the intraoral application of monocortical miniplates to treat mandibular angle fractures. They showed that miniplates achieved the goal of osteosynthesis by neutralizing undesirable tensile forces while retaining favorable compressive forces during function. They studied these movements with regard to a mathematical model of the mandible and as a result was able to determine the ideal line of osteosynthesis to overcome these displacing forces. By placing the plate at the most biomechanically favorable site, the thickness of the plate can be kept to a minimum with consequent advantage of increased malleability
Mandibular angle fractures
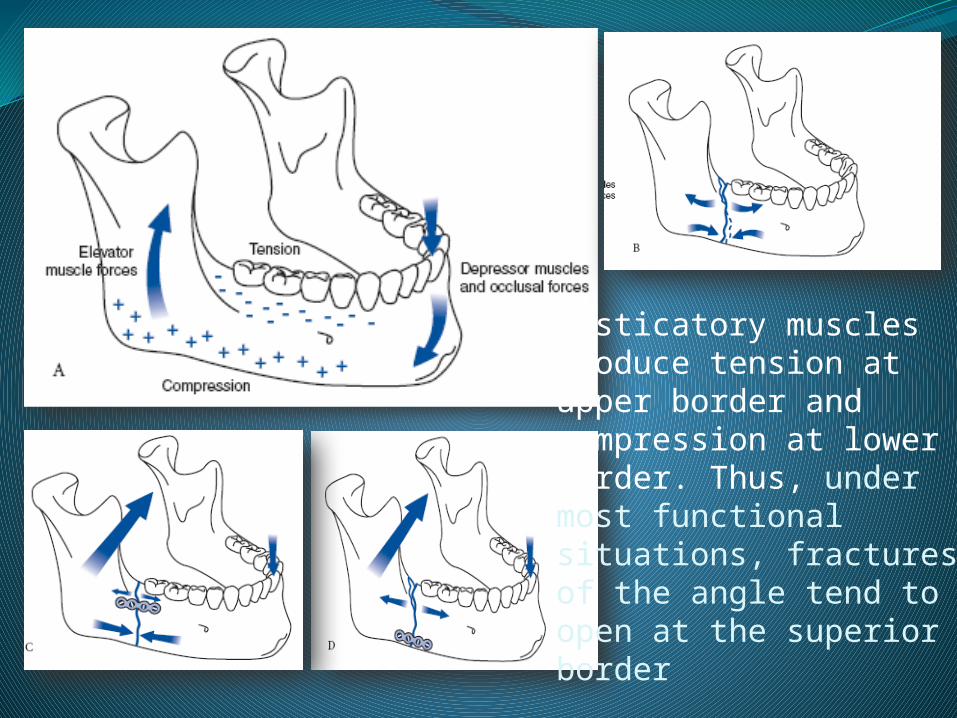
Masticatory muscles produce tension at upper border andcompression at lower border. Thus, under most functionalsituations, fractures of the angle tend toopen at the superiorborder
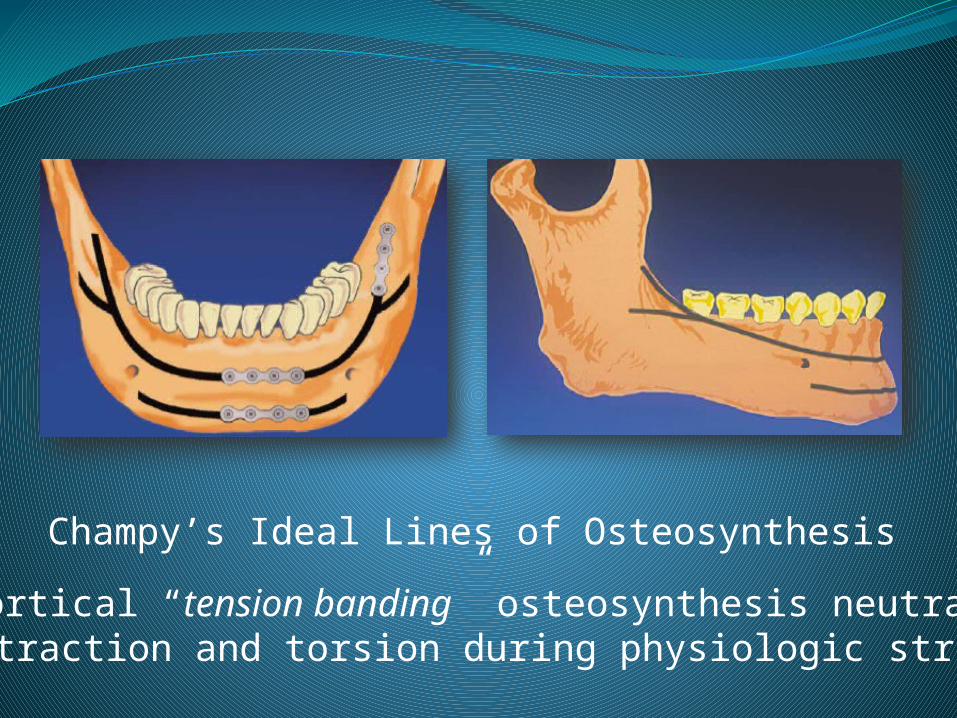
Champy’s Ideal Lines of Osteosynthesis
Monocortical “tension banding” osteosynthesis neutralizes distraction and torsion during physiologic stress
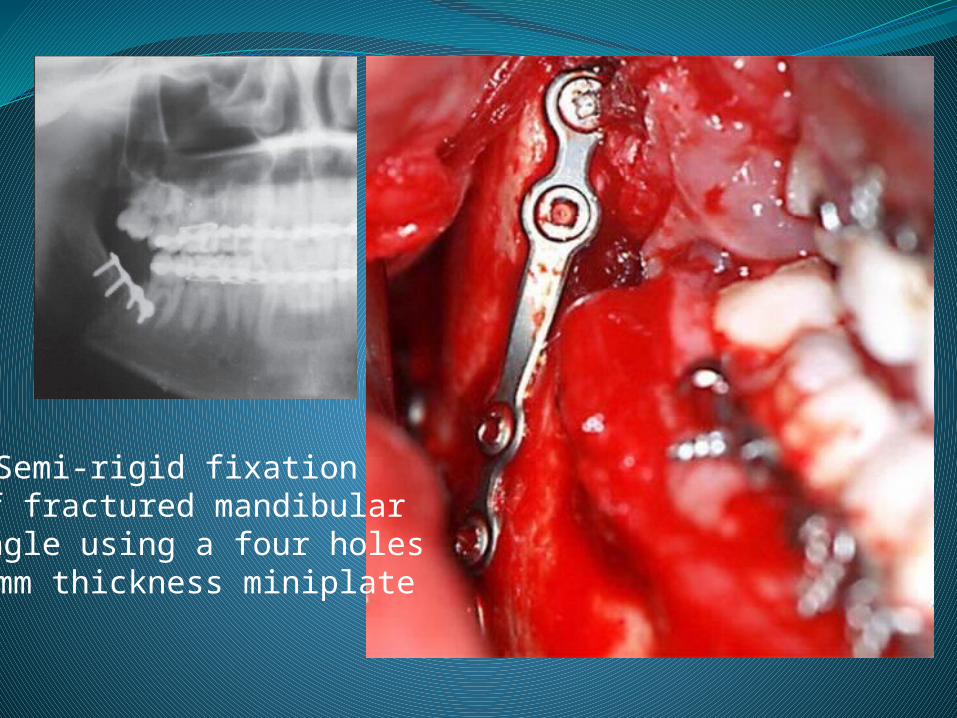
Semi-rigid fixation of fractured mandibular angle using a four holes
2mm thickness miniplate
Gradually, due to simplicity and minimal complications, the “semi-rigid” technique, has gained popularity as a standard treatment approach in different trauma centers. Accordingly, the AO/ASIF have changed the principle of “rigid fixation” to “functionally stable fixation”. Currently, the four revised principles of the AO/ASIF are as follows:1) Anatomic reduction2) Functionally stable fixation (previously “rigid fixation”)3) Atraumatic surgical technique4) Immediate active function (10)
Mandibular angle fractures
The technique involves placement of a single monocortical noncompression miniplate on the superior border of the mandible, either on the external oblique ridge using an intraoral approach or against the outer surface of the mandible using an transbuccal approach. Some in vitro studies suggest that using a second miniplate along the inferior border theoretically creates a second osteosynthesis line and helps stabilize the fixation protecting the fractures against rotation and torsion (11). Whether one or two miniplates should be used at the mandibular angle fracture is still debatable
Mandibular angle fractures
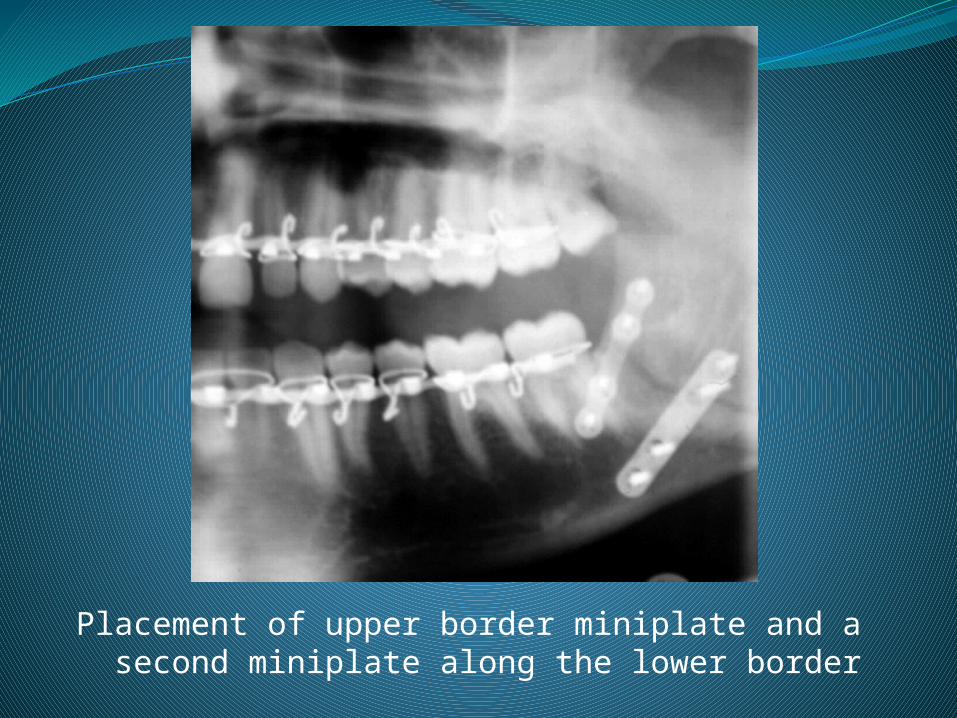
Placement of upper border miniplate and a second miniplate along the lower border
However, clinical studies provide a different picture. Ellis noted that the application of 2 mini-plate is associated with significant complications; 29% as compared to a single one; 2.5% (8). To overcome the disadvantages of 2 plates application and to provide additional stability with a use of a single plate, 3- dimensional (3D) plates were developed (12). It consists of two 4- hole miniplates joined by 4 interconnecting cross struts. This provides room for additional screw placement adding to torsional and 3D stability of the fracture. A recent meta-analysis of the use of 3D plates in angle fractures demonstrated that the geometry of the plate assures a good stability in the three-dimensions of the fracture sites and provides good resistance against torque forces. Further it was noted that 3D plates are associated with lower complication rates as compared to standard miniplate fixation (13)
Mandibular angle fractures
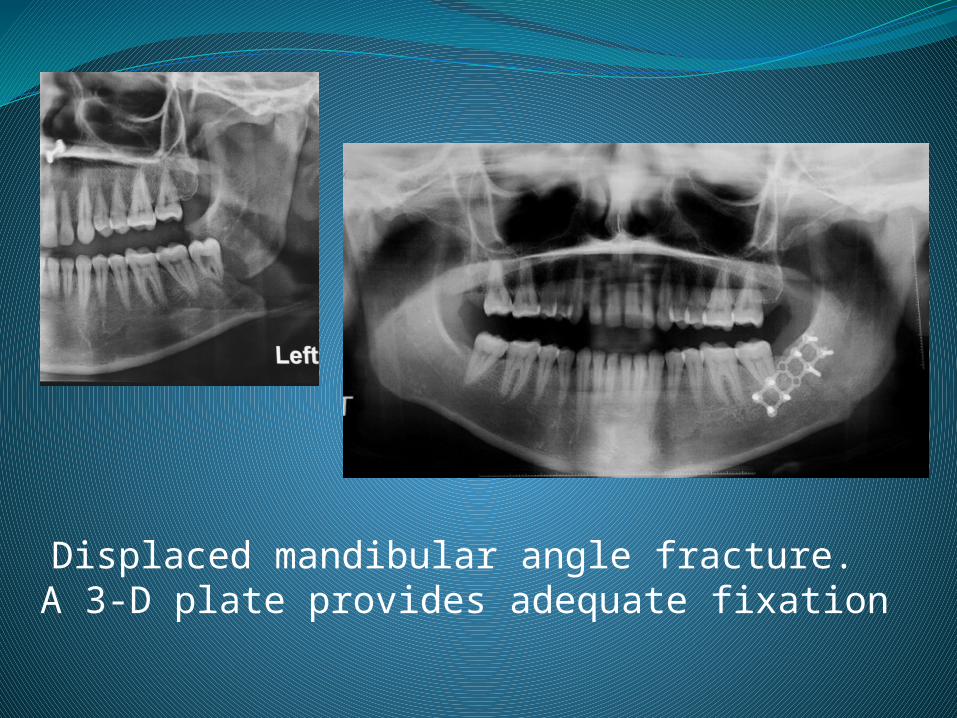
Displaced mandibular angle fracture. A 3-D plate provides adequate fixation
1. Bormann KH, Wild S, Gellrich NC, et al. Five-year retrospective study of mandibular fractures in Freiburg, Germany: incidence, etiology, treatment, and complications. J Oral Maxillofac Surg. 67:1251,2009. 2. Schubert W, Kobienia BJ, Pollock RA. Cross-sectional area of the mandible. J Oral Maxillofac Surg. 55:689,1997.3. Dodson TB. Third molars may double the risk of an angle fracture of the mandible. Evid Based Dent. 5:78,2004.4. Fonseca RJ, Walker RW, Betts NJ, et al. Oral and Maxillofacial Trauma 3rd Ed. Vol. 1:487-490, 2005.5. Brown JS, Grew N, Taylor C, et al. Intermaxillary fixation compared to miniplate osteosynthesis in management of the fractured mandible: An audit. Br J Oral Maxillofac Surg. 29:308,1991.6. Souyris F, Lamarche JP, Mirfakhrai AM. Treatment of mandibular fractures by intraoral placement of bone plates. J Oral Surg. 38:33,1980.7. Scolozzi P, Richter M. Treatment of severe mandibular fractures using AO reconstruction plates. J Oral Maxillofac Surg. 61:458,2003. 8. Ellis E 3rd. Treatment methods for fractures of the mandibular angle. Int J Oral Maxillofac Surg. 28:243,1999.9. Champy M, Lodde JP, Schmidt R, et al. Mandibular osteosynthesis by miniature screwed plates via a buccal approach. J Oral Maxillofac Surg. 6: 14,1978.
References:
10. Ellis E 3rd. Treatment methods for fractures of the mandibular angle. Int J Oral Maxillofac Surg. 28: 243,1999. 11. Alkan A, Çelebi N, Özden B, et al. Biomechanical comparison of different plating techniques in repair of mandibular angle fractures. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 104:752,2007. 12.Farmand M, Dupoirieux L. The value of 3-dimensional plates in maxillofacial surgery. Rev Stomatol Chir Maxillofac. 93:353,1992. 13. Al-Moraissi EA, El-Sharkawy TM, El-Ghareeb TI, et al. Three-dimensional versus standard miniplate fixation in the management of mandibular angle fractures: a systematic review and meta-analysis. Int J Oral Maxillofac Surg. 43:708,2014.
References: