malaria in pregnancy steve meshnick, m.d., ph.d. professor of epidemiology and microbiology
TRANSCRIPT
Malaria in Pregnancy
Steve Meshnick, M.D., Ph.D.
Professor of Epidemiology and Microbiology
Outline
• The global burden of malaria
• Importance of malaria in reproductive health
• UNC research activities
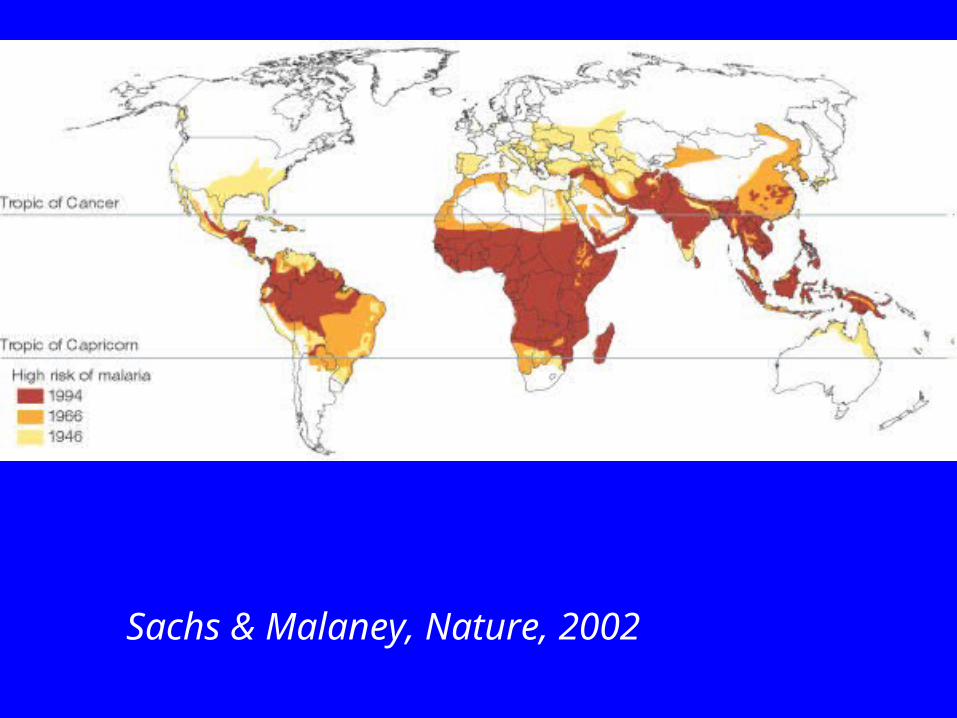
Sachs & Malaney, Nature, 2002
Malaria 2004
• 90% of cases and deaths in Africa
• >300 million cases/year• Periodic fever, chills, prostration
• ~2 million deaths/year, mostly in children <5– Cerebral malaria, severe anemia
Types of malaria
• Plasmodium falciparum– Most common– Multi-drug resistant– Most dangerous
• Plasmodium vivax– Latin America & Asia
• Plasmodium malariae• Plasmodium ovale
Geography of malaria
sub-Saharan AfricaP. falciparum
Year-round transmission
Incidence >1/person/yr
Adults are immune
Affects children < 5 & primigravidae
Asia & Latin AmericaP vivax >P. falciparum
Seasonal transmission
Incidence is low
Little or no immunity
Affects people of all ages and pregnant women of all gravidity
Malaria control toolbox• Antimalarial drugs
– Prophylaxis– Case management (treatment)– Intermittent Preventive Therapy
• Vector control– Household spraying– Insecticide-treated bednets
• Vaccine
Case management
sub-Saharan AfricaLow income
High transmission
Sulfadoxine- pyrimethamine
Presumptive therapy
Asia & Latin AmericaMiddle income
Low transmission
Artemisinin Combination Therapy
Microscopy and treatment of slide-confirmed cases
Intermittent Preventive Therapy (IPT)
• Areas of high transmission
• Therapeutic doses of SP given periodically to all pregnant women or infants at risk
• Takes advantage of– High utilization by pregnant women of
antenatal clinics– High coverage of infants for EPI vaccination
visits (2, 3, 9 mos)
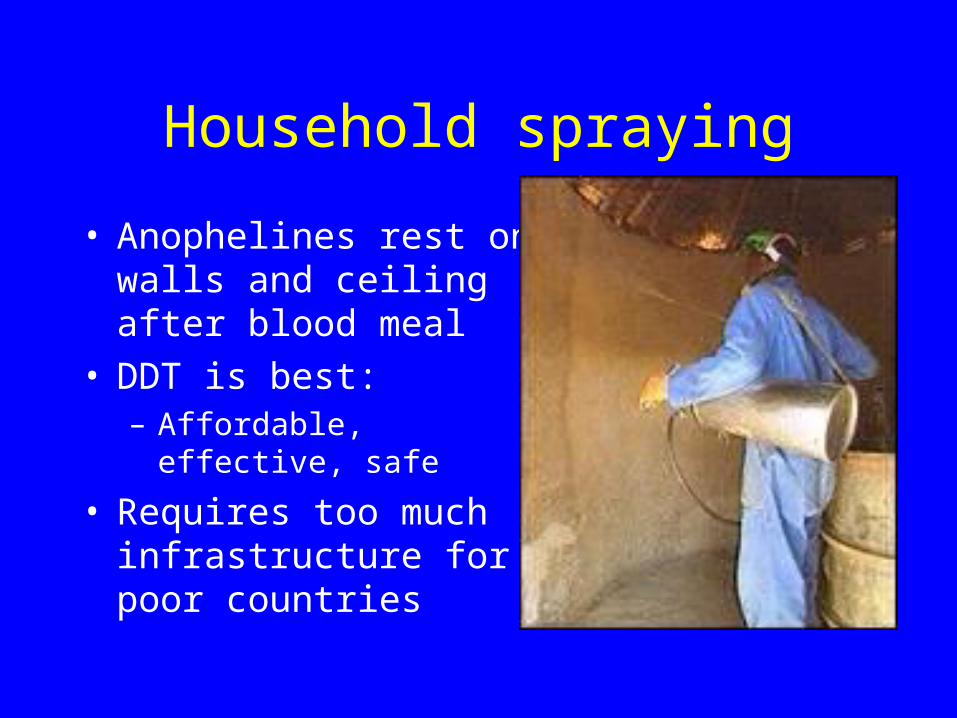
Household spraying
• Anophelines rest on walls and ceiling after blood meal
• DDT is best: – Affordable, effective, safe
• Requires too much infrastructure for poor countries
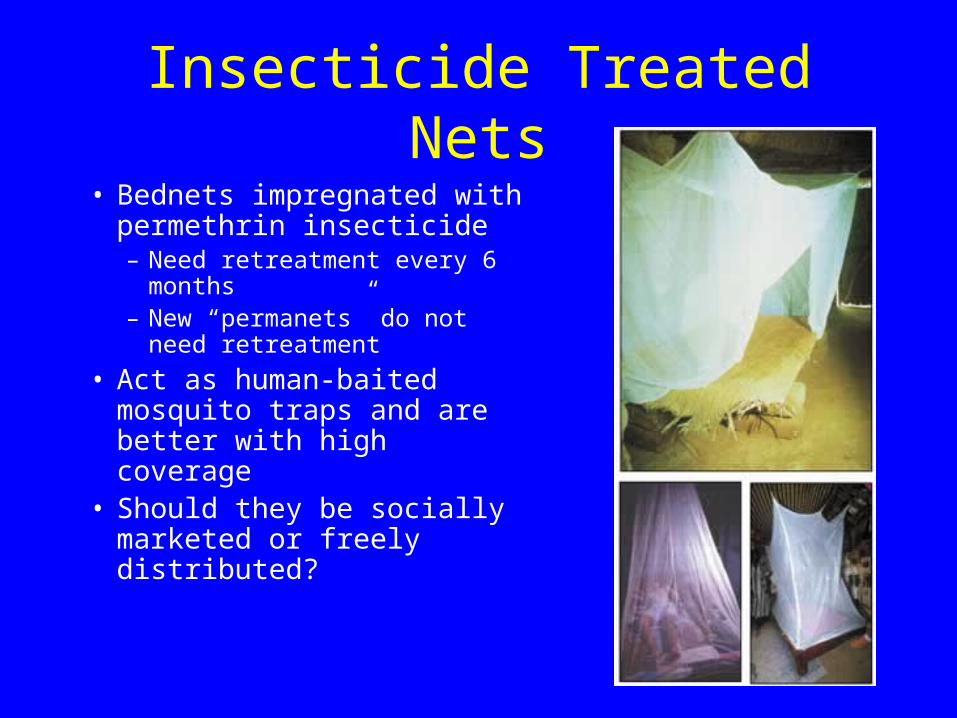
Insecticide Treated Nets• Bednets impregnated with
permethrin insecticide– Need retreatment every 6
months– New “permanets” do not need
retreatment
• Act as human-baited mosquito traps and are better with high coverage
• Should they be socially marketed or freely distributed?
Global efforts to control malaria
• Roll Back Malaria (WHO)– Set achievable goals– Individual country plans
• Global Fund for AIDS, TB and Malaria
• Gates Foundation (MMV, GAVI)
Outline
• The global burden of malaria
• Importance of malaria in reproductive health
• UNC research activities
Malaria in pregnant women
• >50 million pregnant women exposed to malaria each year
• ~3.5 million pregnant women infected
Poor birth outcomes
Poor maternal outcomes
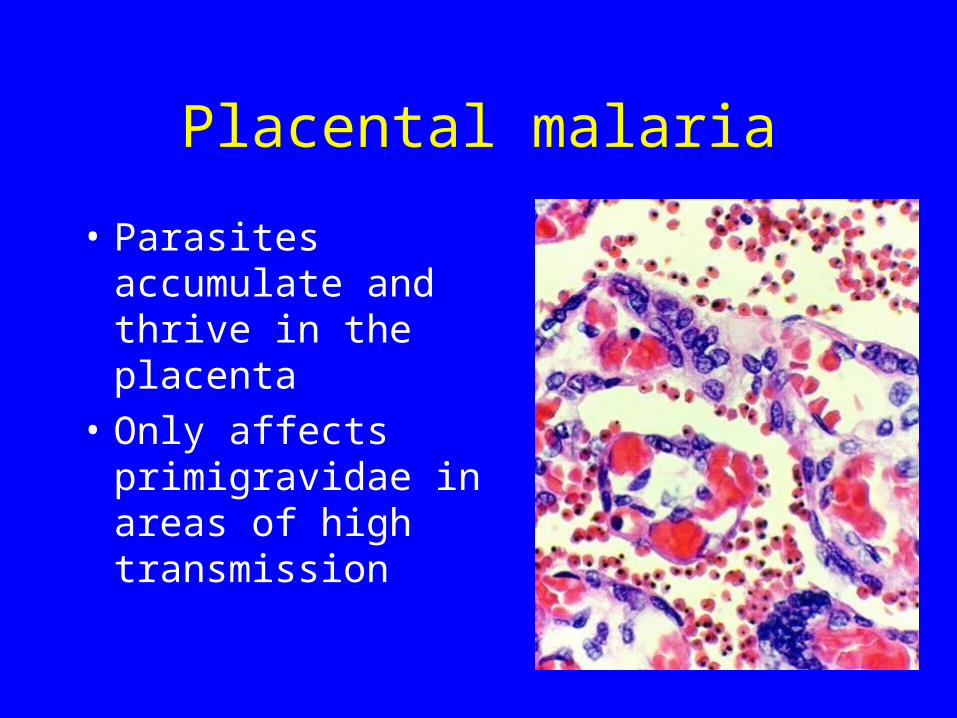
Placental malaria
• Parasites accumulate and thrive in the placenta
• Only affects primigravidae in areas of high transmission
Gravidity and malaria• Primigravidae have no pre-existing
immunity to placental parasites and are highly susceptible
• In high transmission areas, primigravidae develop immunity to placental parasites and are protected in subsequent pregnancies
• In low transmission areas, multigravidae are unexposed and unprotected
Effects of malaria on pregnant women
• Poor birth outcomes– Low birth weight due to preterm delivery
(PTD) and intrauterine growth retardation (IUGR)
– abortions, stillbirths
• Maternal outcomes– Anemia, maternal mortality
Poor birth outcomes
• In African studies, malaria accounts for– 8-14% of all low birth weight
– 3-8% of infant mortality(Steketee et al., Am. J. Trop. Med. Hyg, 2001)

Maternal mortality
• Responsible for 0.5 – 23% of maternal deaths in Africa
• Malaria causes severe anemia and platelets can predispose to death from hemorrhage
www.prema-eu.org
Interventions
• Intermittent Preventive Therapy (IPT)– sulfadoxine-pyrimethamine (SP)
• Insecticide-Treated Nets (ITNs)
• RBM goals – 60% of pregnant women in endemic areas should have access to both by 2005
IPT
• Malawi first to introduce (1993)– Two therapeutic doses of SP to all pregnant
women at quickening and at 28-34 wks Inexpensive (~$0.20)
– 2-dose coverage is still low (<25%)
• New recommendations include 4-doses or monthly SP
• Prevents 23-86% of severe maternal anemia
ITNs
• Cost ~$4.00• Reduce malaria, severe anemia and LBW
by 30-50%• Socially marketed nets (~$1.00)
– Low uptake
• Freely distributed nets– High uptake and well utilized– Less sustainable
Malaria is the most common and easily preventable cause of poor birth outcomes in the world
Programmatic priorities
• Integration of malaria prevention into – Reproductive health programs – Programs to prevent mother-to-child
transmission of HIV
• Increase uptake of IPT and ITNs
• Make programs sustainable
Outline
• The global burden of malaria
• Importance of malaria in reproductive health
• UNC research activities
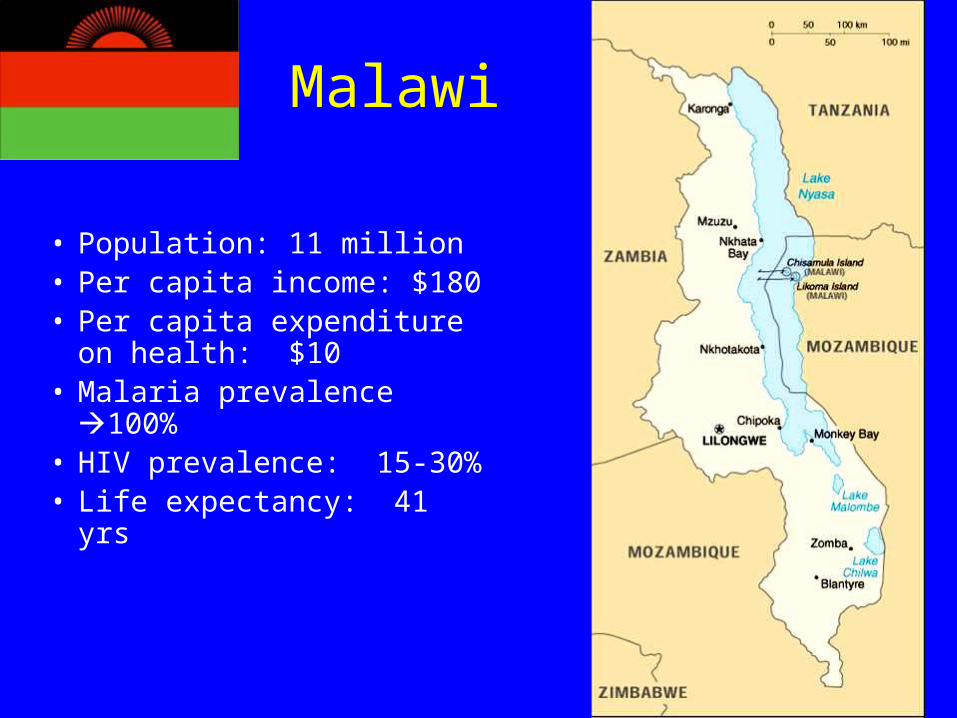
Malawi
• Population: 11 million• Per capita income: $180• Per capita expenditure on
health: $10• Malaria prevalence
100% • HIV prevalence: 15-30%• Life expectancy: 41 yrs




Queen Elizabeth Central Hospital
• QECH provides primary and secondary health services for Blantyre.
• Also referral center for Southern Malawi
Pathologenesis of malaria in pregnancy
• During normal pregnancy, the cellular immune response (Th1) is suppressed to prevent fetal rejection
• Malaria stimulates the Th1 response intrauterine growth retardation
• Malaria stimulates expression of an HIV co-receptor (CCR5) in the placenta
Moormann et al., JID, 1999; Tkachuk et al., JID 2001; Abrams et al., Am. J. Reprod. Immunol., 2004
Malaria and HIV co-infections during pregnancy
• Up to 10% of pregnant women may be co-infected with both HIV and malaria
• HIV-infected pregnant women have more frequent and severe malaria
• Malaria infection might increase mother-to-child transmission of HIV
• Infant mortality rate for offspring of co-infected mothers is 3-8 fold higher than singly infected mothers
Effects of malaria on HIV viral load
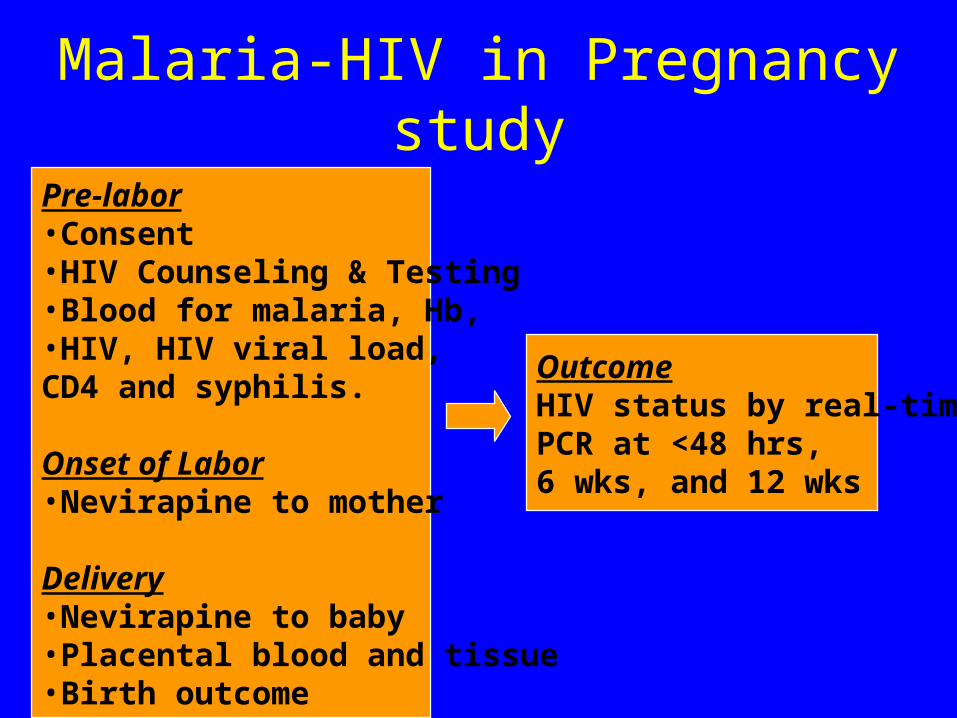
Malaria-HIV in Pregnancy study
Pre-labor•Consent•HIV Counseling & Testing•Blood for malaria, Hb,•HIV, HIV viral load, CD4 and syphilis.
Onset of Labor•Nevirapine to mother
Delivery•Nevirapine to baby•Placental blood and tissue•Birth outcome
OutcomeHIV status by real-timePCR at <48 hrs, 6 wks, and 12 wks
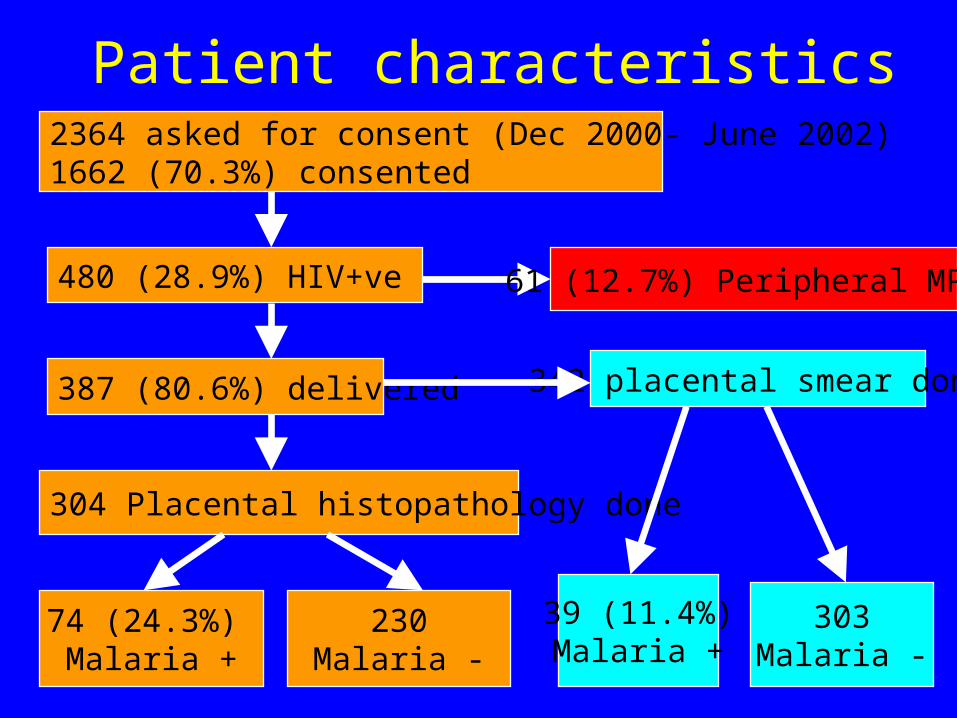
480 (28.9%) HIV+ve
387 (80.6%) delivered
304 Placental histopathology done
74 (24.3%) Malaria +
230Malaria -
342 placental smear done
39 (11.4%)Malaria +
303Malaria -
61 (12.7%) Peripheral MPs+
Patient characteristics2364 asked for consent (Dec 2000- June 2002) 1662 (70.3%) consented
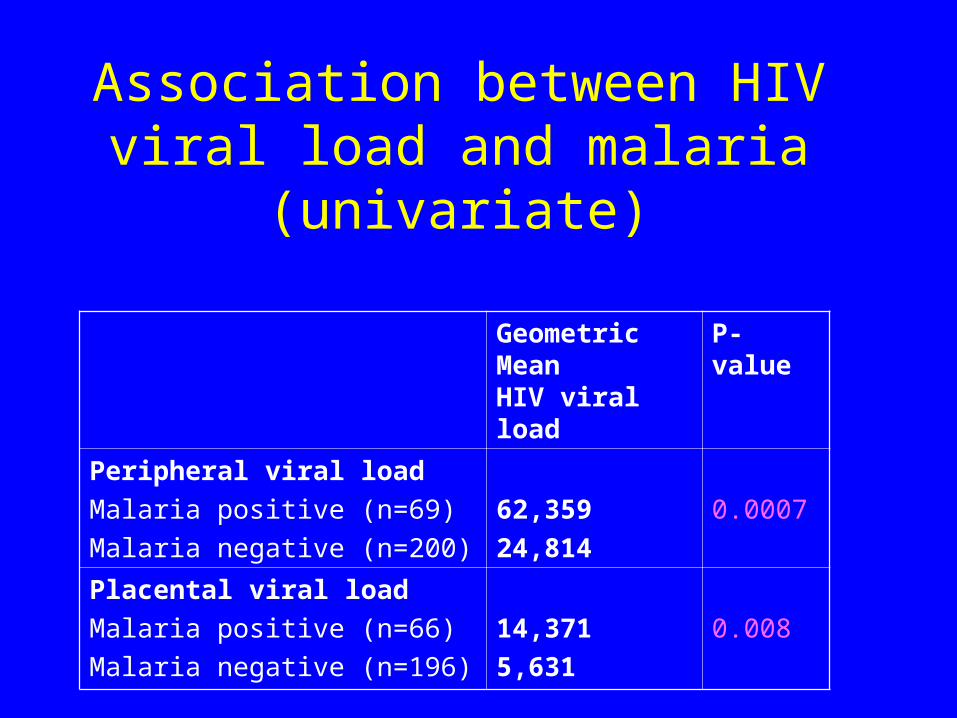
Geometric Mean
HIV viral load
P-value
Peripheral viral load
Malaria positive (n=69)
Malaria negative (n=200)
62,359
24,814
0.0007
Placental viral load
Malaria positive (n=66)
Malaria negative (n=196)
14,371
5,631
0.008
Association between HIV viral load and malaria (univariate)
Multivariate analyses
• Malaria is associated with 1.7-fold increase in peripheral HIV viral load and a 2-fold increase in placental viral load after adjusting for CD4 cell count and hemoglobin concentrations
• Since a 1-log increase in peripheral viral load is associated with a 2.5-fold increase in MTCT, then malaria might increase MTCT by 25%.
Mwapasa, et al., AIDS, 2004
Does malaria promote MTCT of HIV?
• Study on-going, but to date, no association between malaria and MTCT seen
• Currently, only 10% power to detect the 25% difference
• Indirect evidence for an effect on MTCT– Malaria viral load MTCT– Malaria fever MTCT– Malaria LBW MTCT
Public Health Implications 500,000 live births/year in Malawi:
100,000 to HIV(+) women
20,000 HIV(+) babies (if nevirapine used)
6,000 HIV(+) babies born to malaria (+) mothers/yr
Better malaria prevention could prevent 1,200 new infections
HIV and susceptibility to malaria
• HIV-infected pregnant women have more frequent and severe malaria
• Is the effect of HIV on malaria dependent on decreasing CD4’s or decreasing antibody?
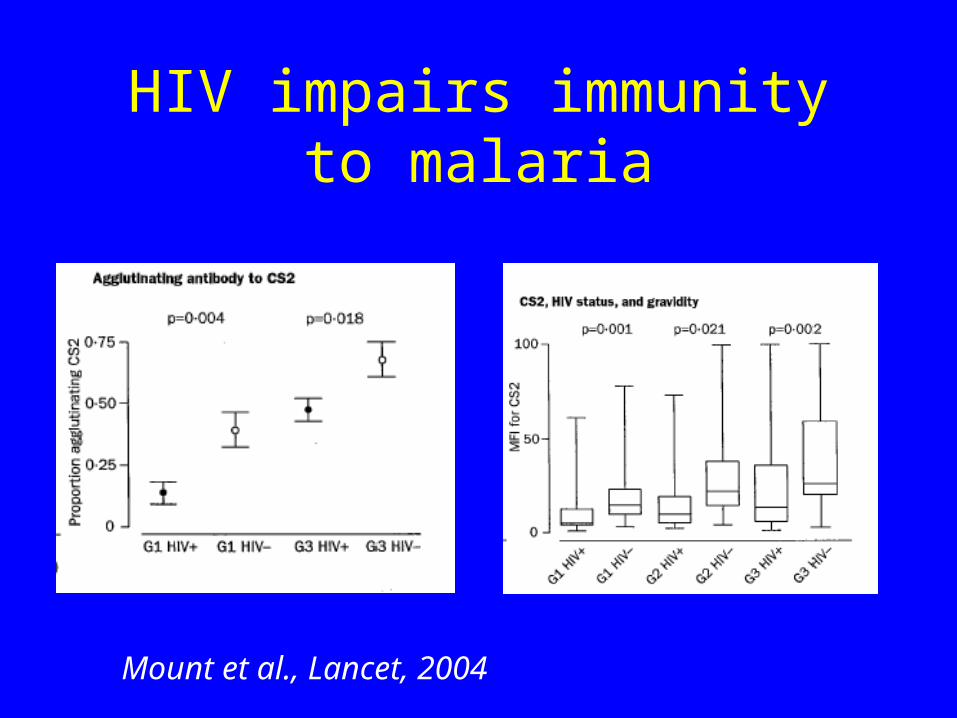
HIV impairs immunity to malaria
Mount et al., Lancet, 2004
Important issues in malaria-HIV interactions
• Can prevention or treatment of malaria delay progression of HIV disease?
• Does HIV affect susceptibility to malarial disease in children?
• Does ART restore immunity to malaria?
IPT 2004
• 2-dose IPT with SP ineffective in HIV-infected women
• SP IPT also losing effectiveness due to drug resistance
• What should replace SP?
Possible alternatives to SP
• SP-artesunate
• SP-azithromycin
• Amodiaquine
• Mefloquine
• Lapdap
SP vs SP-artesunate vs SP-azithromycin
• Study ongoing
• Expected completion of pilot (120 women) by summer 2004
Can new IPT regimens delay the onset of drug
resistance?
• New low-cost assays to measure malaria resistance to:– SP (Alker et al, AAC, in press)– Quinolines (Purfield et al., Malaria J, in press)
New drugs for malaria
• DB289 developed by Tidwell group and for treatment of African sleeping sickness (supported by Gates Foundation)
• Effective in an initial trial against P. falciparum in Thailand curing >90% of patients (supported by MMV)
O N
N H 2H 2N
NOCH3
H3CO
Summary
• Malaria is an enormous reproductive health problem, especially in sub-Saharan Africa
• IPT and ITNs are inexpensive and effective interventions
• Investment in malaria control can do the most good for the least amount of money
Acknowledgements