making surgical practice improvement easy
TRANSCRIPT
Making Surgical practice improvement easy
S Connor, M Sakowska, D MacKay, M Furlong, R Roberts
CDHB and scOPe1 solutions
Introduction• Key component to improving surgical outcomes for patients is
ensuring completion of the audit cycle.
• To do so requires
• seamless mapping of the patient journey
• Accurate collection of coded data
• Leveraging of trusted data into meaningful information to the clinicians
• To obtain buy in any change in process or involvement by
clinicians must make their workflow process easier
Aim• To create an electronic workflow for managing patient journey through
surgical services
• Process change must improve clinicians work flow
• Create data that was as accurate and could be trusted by end viewer
• Data to be captured once by person most likely to be able to verify its
accuracy
• Exportable to meet requirements of multiple end users
Methods• Holistic approach to development
• Especially individual and Dept. “clinical champions”
• DHB
• Developers
• Non clinical champions: administrative and managerial
• End users of potential data
• Apply principles of lean thinking to design and workflow
• Staggered roll out across surgical services as clinical champions came on board
• Agile approach to new ideas

What is ?A clinical audit and outcomes tool using workflow support
to capture data
Waiting List• Streamline entry
• Visibility to surgeon
• Real time accuracy
Theatre Visualisation
• E-whiteboard in Theatre
• Ward viewer
• Accurate Op List
Post Op Note / Ward
Instructions
• Quicker for surgeons (template based)
• Published to core clinical documents system
• Core activity data captured (for list)
Complications / M&M
Meetings
• Core Audit
Results
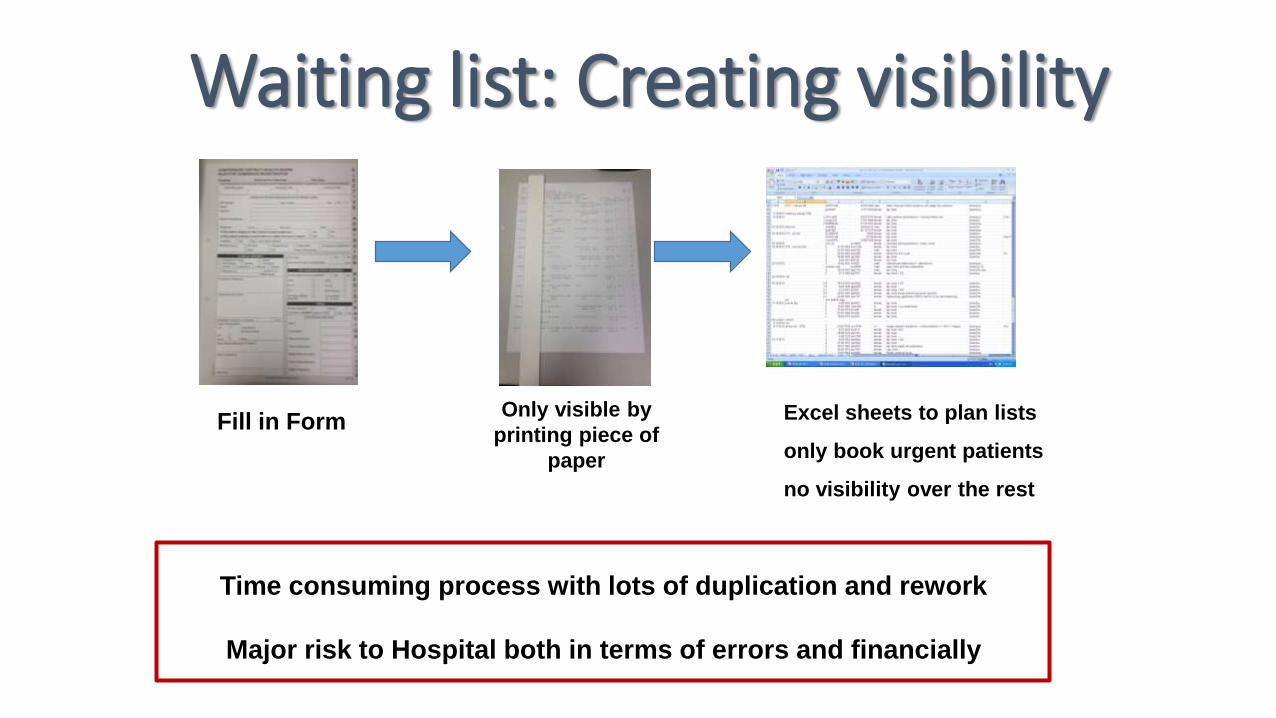
Waiting list: Creating visibility
Time consuming process with lots of duplication and rework
Major risk to Hospital both in terms of errors and financially
Only visible by
printing piece of
paper
Excel sheets to plan lists
only book urgent patients
no visibility over the rest
Fill in Form
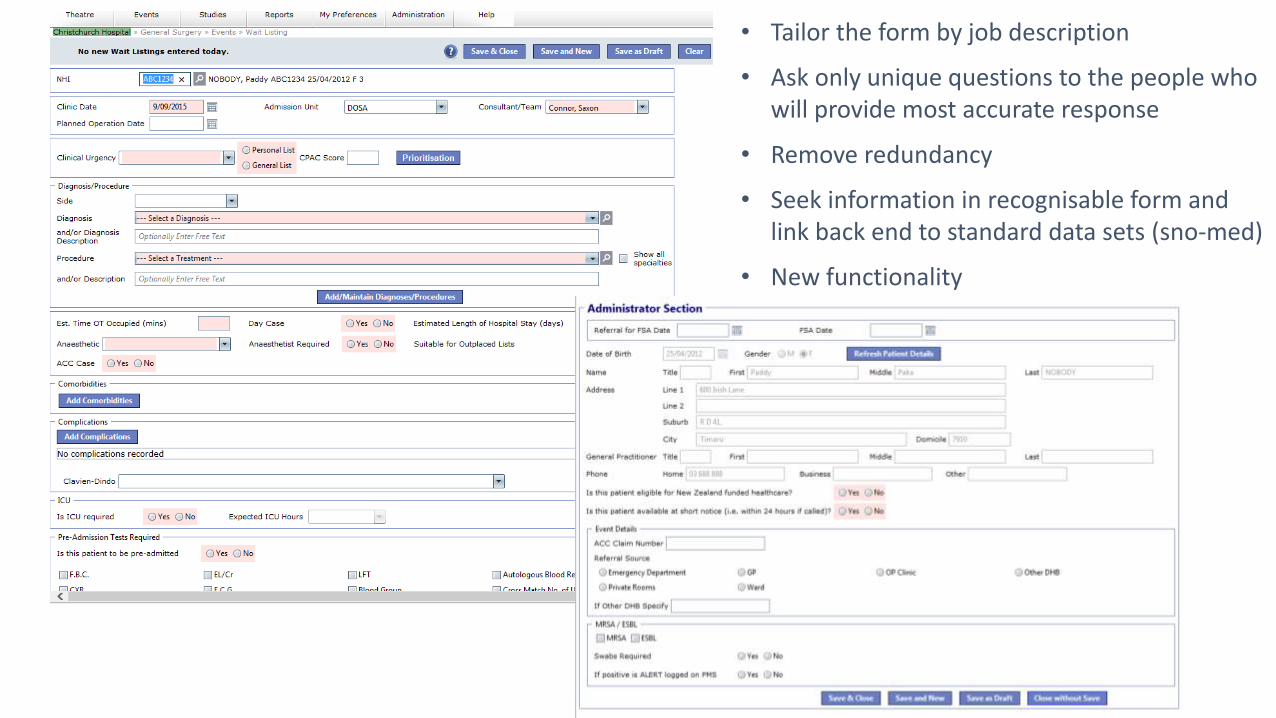
• Tailor the form by job description
• Ask only unique questions to the people who will provide most accurate response
• Remove redundancy
• Seek information in recognisable form and link back end to standard data sets (sno-med)
• New functionality
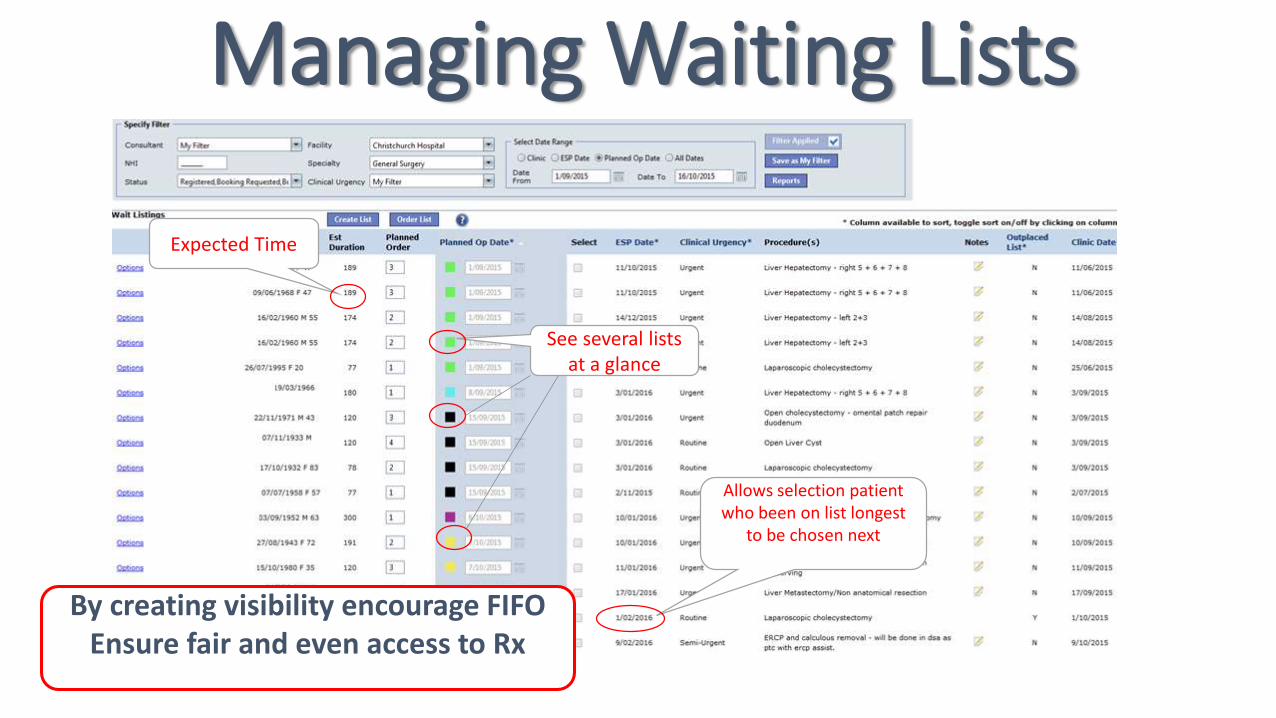
Managing Waiting Lists
Expected Time
Allows selection patient who been on list longest
to be chosen next
See several lists at a glance
By creating visibility encourage FIFOEnsure fair and even access to Rx
Operation Note
Requires data entry
Word template
Can we do Better?
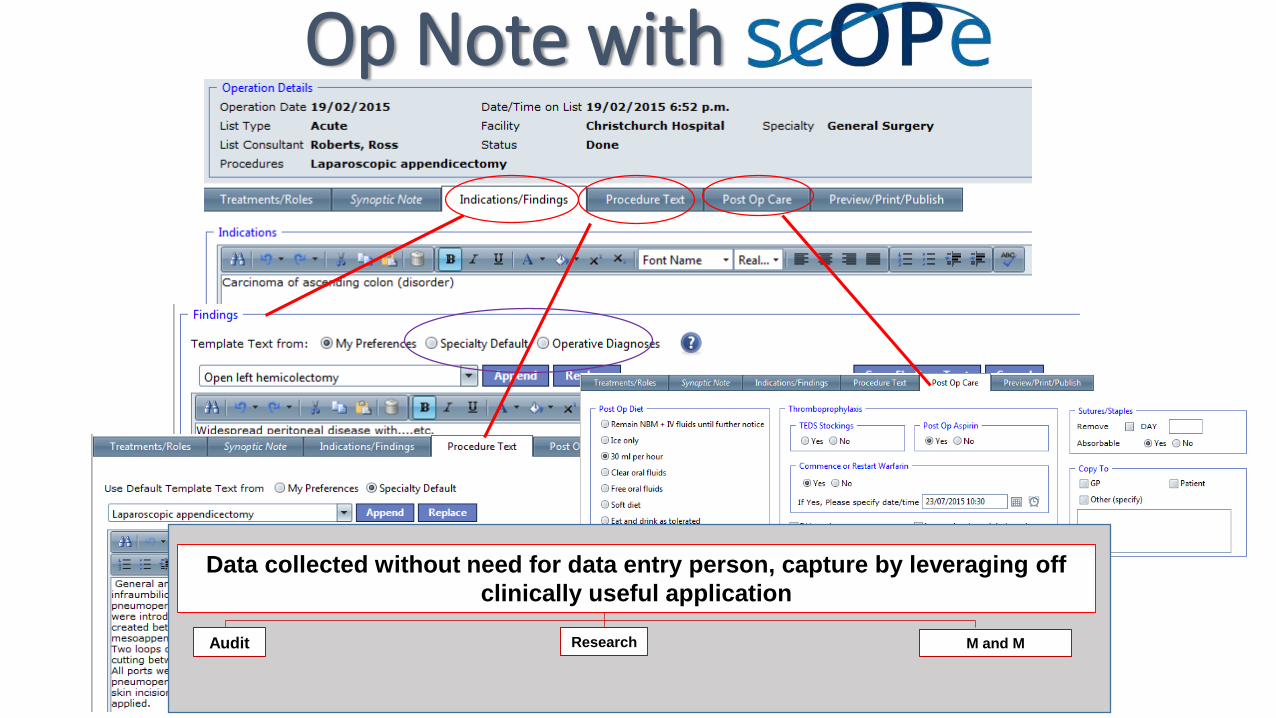
Op Note with
Data collected without need for data entry person, capture by leveraging off
clinically useful application
Audit Research M and M

Synoptic notes
• Common operations can have standardised data and definitions
• Ensure complete information provided for the end user
• Consult the users of the “Op note”
• Re define what is an op notes function

Uptake of synoptic notes: Laparoscopic cholecystectomy
0
20
40
60
80
100
120
140
160
180
1 7
13
19
25
31
37
43
49
55
61
67
73
79
85
91
97
10
3
10
9
11
5
12
1
12
7
13
3
13
9
14
5
15
1
15
7
16
3
Laparoscopic cholecystectomyCumulative use of synoptic note since inception
100%
Cumulative Sum
80%
Method Time
Pre-scope 3 days
Scope template 1 day
Synoptic 4 (3-8) minutes
Time for op note to be viewable
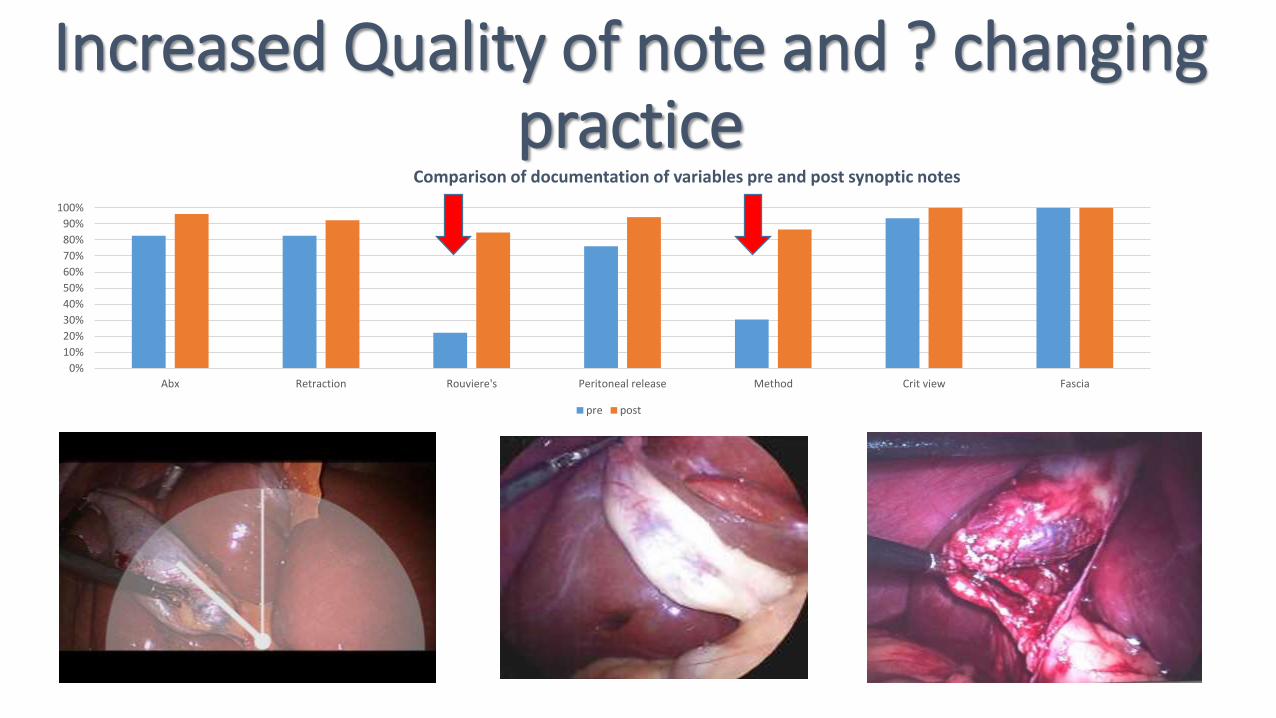
Increased Quality of note and ? changing practice
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Abx Retraction Rouviere's Peritoneal release Method Crit view Fascia
Comparison of documentation of variables pre and post synoptic notes
pre post
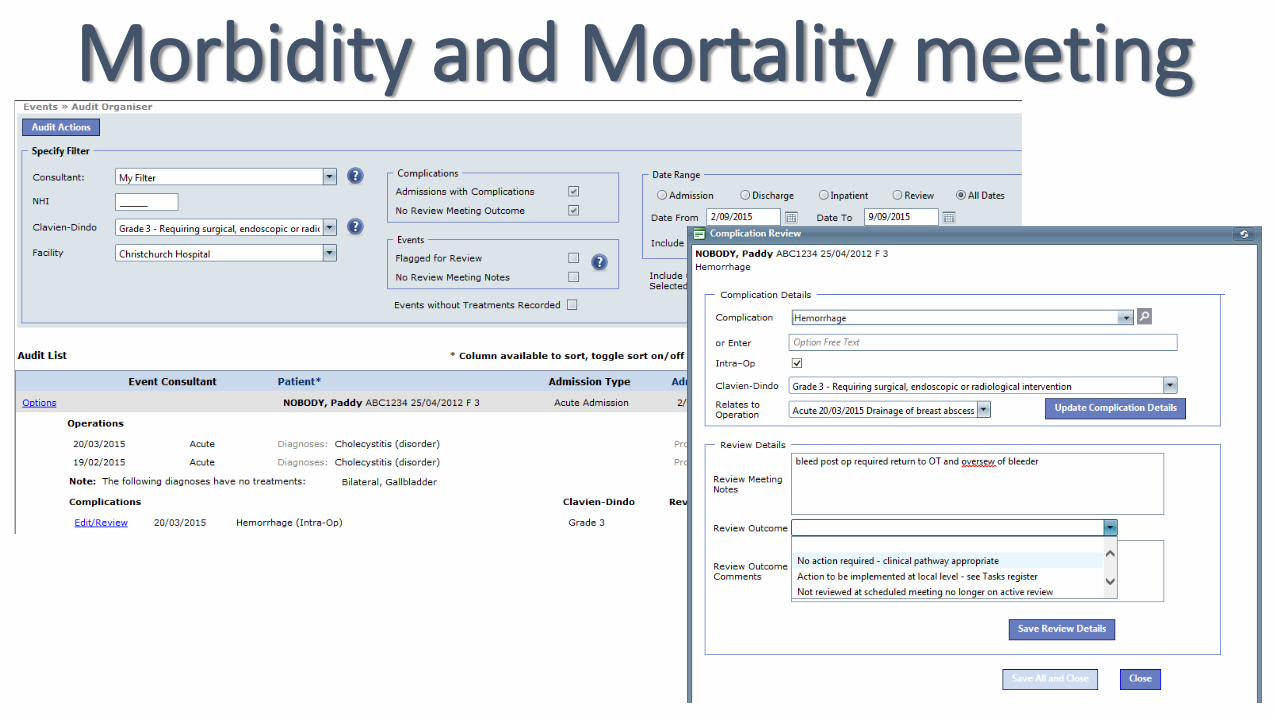
Morbidity and Mortality meeting
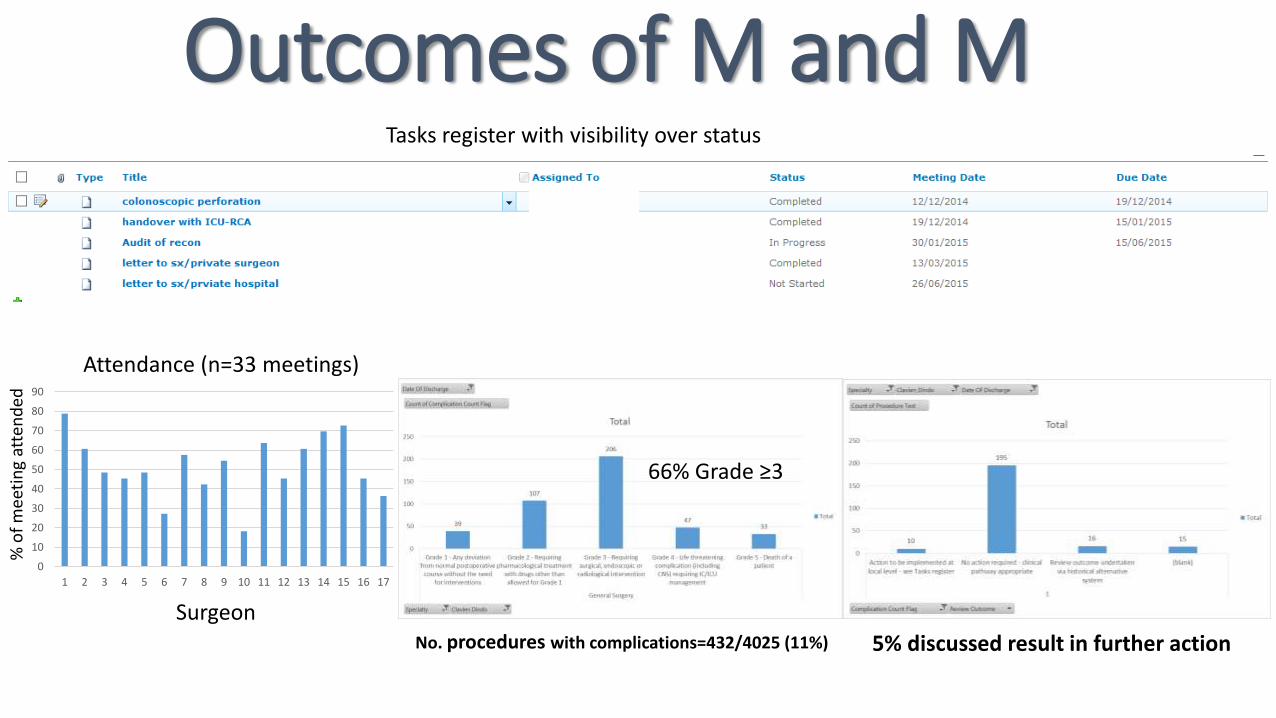
Outcomes of M and MTasks register with visibility over status
0
10
20
30
40
50
60
70
80
90
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17
Surgeon
% o
f m
eeti
ng
atte
nd
ed
Attendance (n=33 meetings)
No. procedures with complications=432/4025 (11%)
66% Grade ≥3
5% discussed result in further action
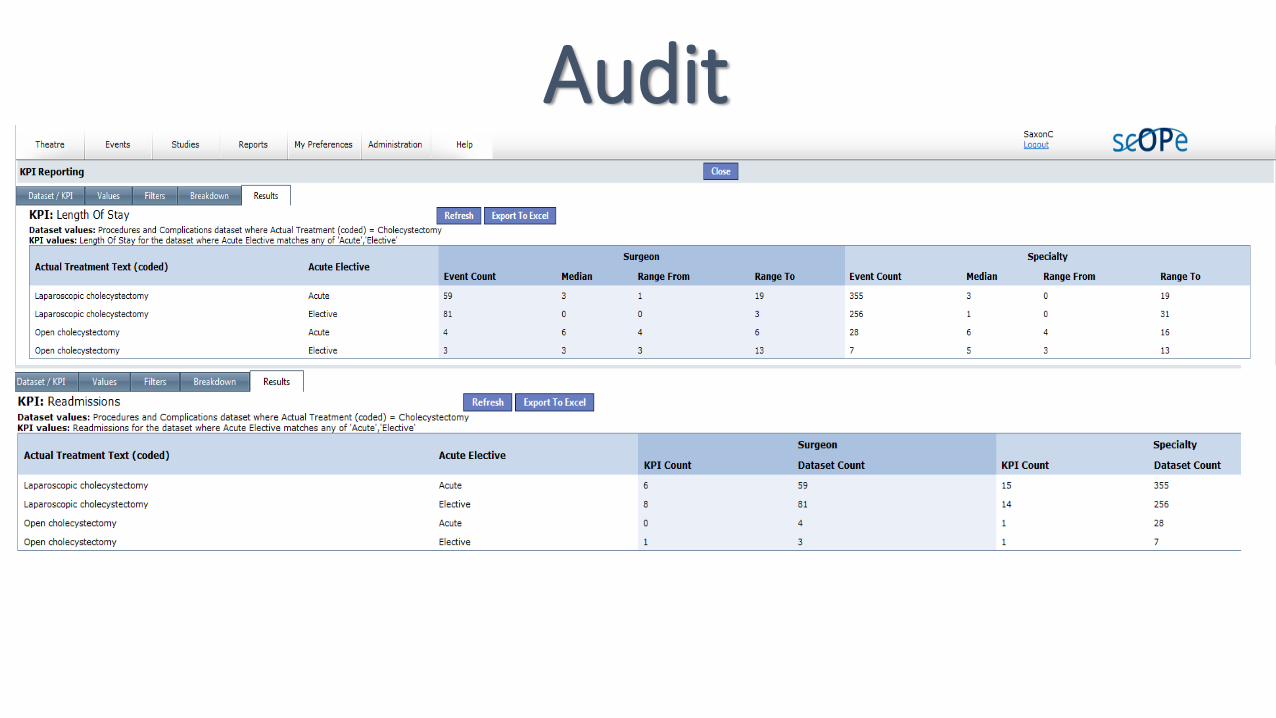
Audit
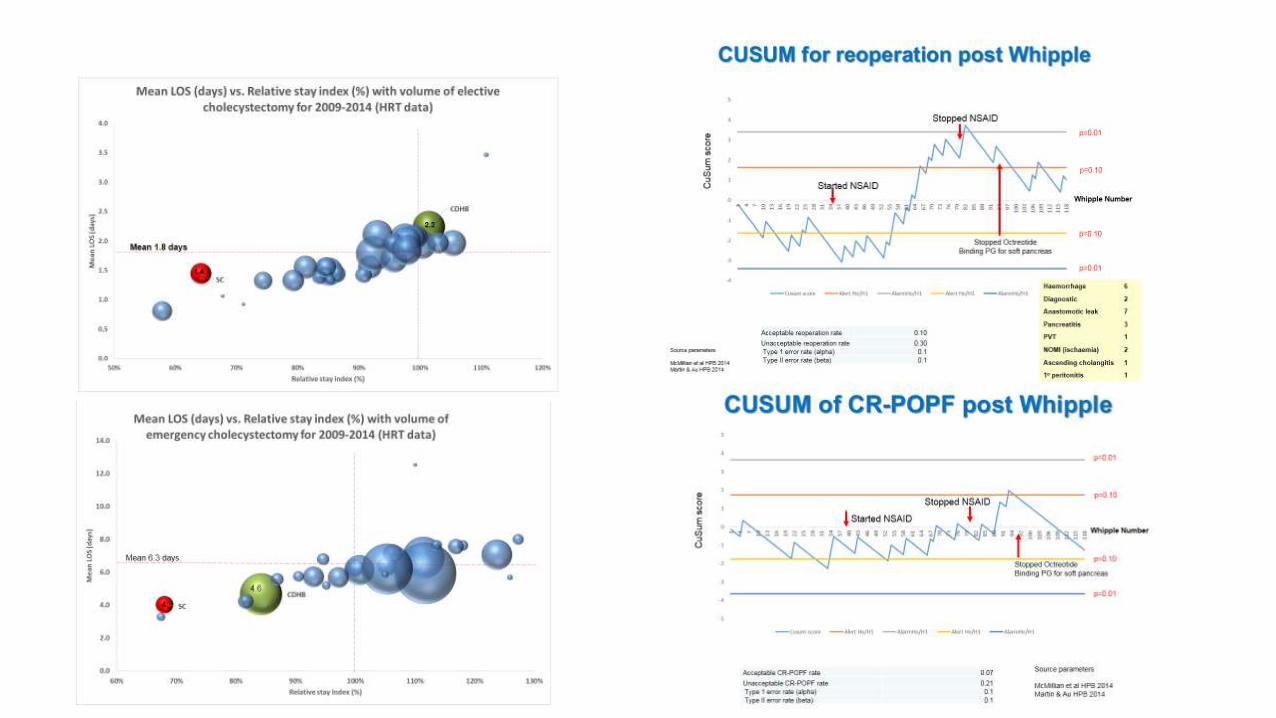

Leveraging the data
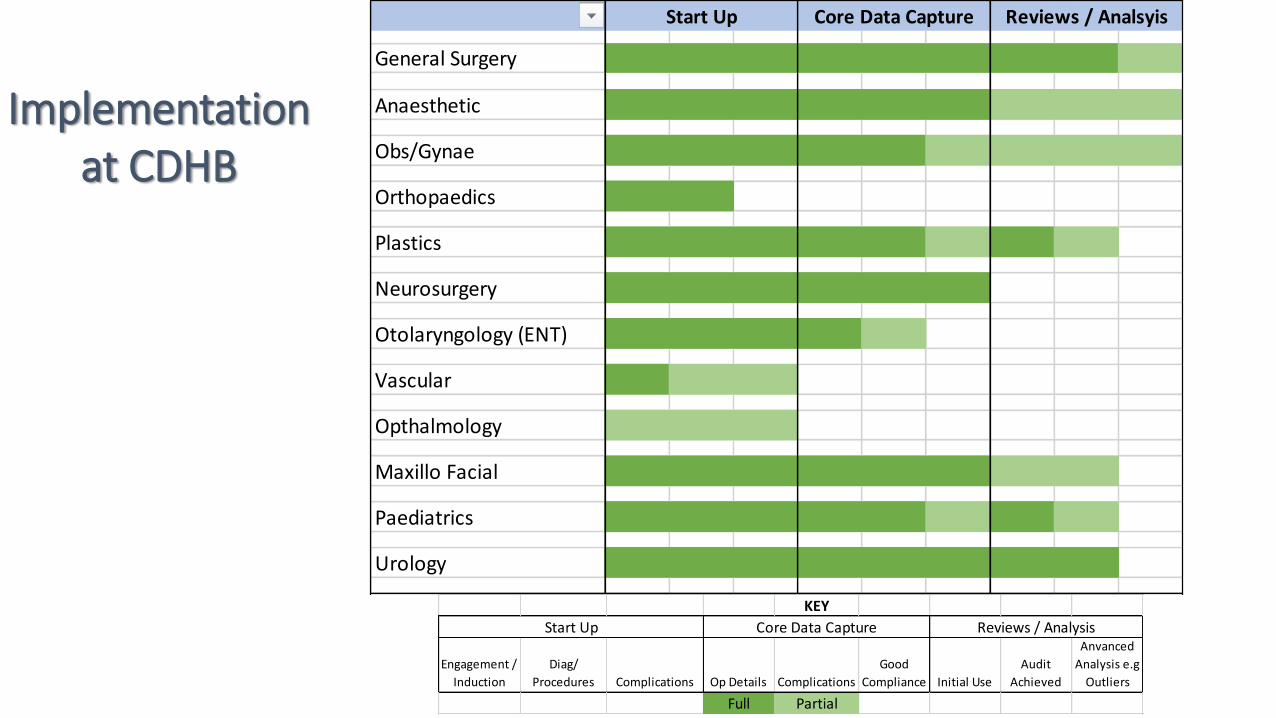
Implementation at CDHB
KEY
Engagement /
Induction
Diag/
Procedures Complications Op Details Complications
Good
Compliance Initial Use
Audit
Achieved
Anvanced
Analysis e.g
Outliers
Full Partial
Start Up Core Data Capture Reviews / Analysis
General Surgery
Anaesthetic
Obs/Gynae
Orthopaedics
Plastics
Neurosurgery
Otolaryngology (ENT)
Vascular
Opthalmology
Maxillo Facial
Paediatrics
Urology
Start Up Core Data Capture Reviews / Analsyis
Conclusion• Have successfully replaced a disconnected and non functioning paper
based system into a seamless e-solution that is being fully implemented
into surgical services at a major DHB
• High degree of clinical buy in, uptake and engagement
• Structured so standardised format but bespoke for granularity to make
clinically useful
• Make the front end easy and will capture data required from the people
who can best provide most accurate data
• Outcomes now trusted which can lead process for practice improvement