maine’s state innovation model (sim) grants state... · maine’s state innovation model (sim)...
TRANSCRIPT

Maine’s State Innovation Model (SIM) Grant
Presented to the Maine Medical Associationby Commissioner Mary C. Mayhew
July 24, 2013
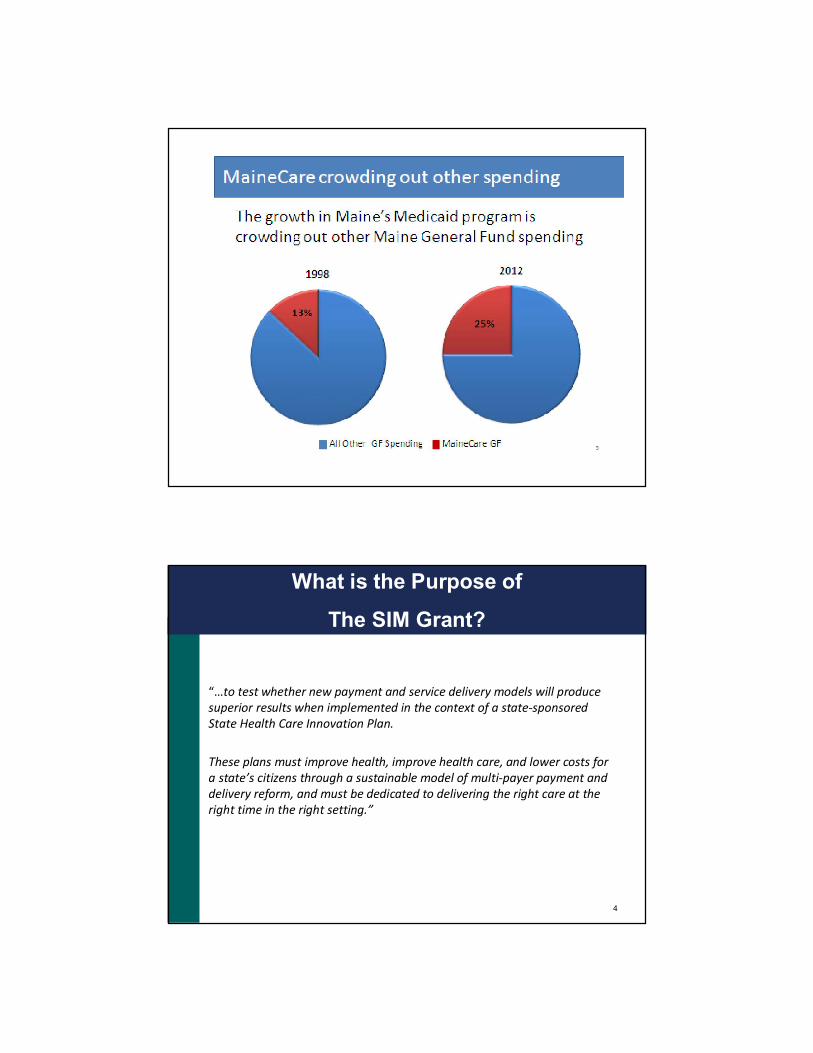
Maine Medicaid
Enrollment and Expenditures
2
General Fund
State Fiscal Year State* DHHS % MaineCare %
2002 $ 2,583,700,000 $ 787,900,000 30.5% $ 476,500,000 18.4%
2003 $ 2,533,200,000 $ 791,600,000 31.2% $ 496,600,000 19.6%2004 $ 2,584,200,000 $ 804,100,000 31.1% $ 514,100,000 19.9%
2005 $ 2,738,100,000 $ 892,300,000 32.6% $ 595,200,000 21.7%
2006 $ 2,824,400,000 $ 970,000,000 34.3% $ 664,500,000 23.5%2007 $ 3,024,400,000 $ 1,008,100,000 33.3% $ 629,100,000 20.8%
2008 $ 3,083,600,000 $ 987,900,000 32.0% $ 643,300,000 20.9%2009 $ 3,019,800,000 $ 935,600,000 31.0% $ 593,300,000 19.6%
2010 $ 2,866,400,000 $ 813,300,000 28.4% $ 469,900,000 16.4%2011 $ 2,859,000,000 $ 859,900,000 30.1% $ 526,300,000 18.4%
2012 $ 3,087,300,000 $ 1,105,100,000 35.8% $ 776,200,000 25.1%
What is the Purpose of
The SIM Grant?
“…to test whether new payment and service delivery models will produce superior results when implemented in the context of a state-sponsored State Health Care Innovation Plan.
These plans must improve health, improve health care, and lower costs for a state’s citizens through a sustainable model of multi-payer payment and delivery reform, and must be dedicated to delivering the right care at the right time in the right setting.”
4

SIM:
A High-Level View
5
This grant will ultimately position Maine to assess the full impact associated with existing healthcare delivery test reform models by moving the test models to the next level through:
•Enhanced care delivery capabilities
•Greater access to high-value care information and data
•Enhanced care delivery “actor” (provider and patient) training / support
•Introduction of targeted incentives
Aligning SIM Strategies
With the Triple Aim
Goals of the “Triple Aim”:
•Improving the individual experience
of care;
•Improving the health of populations;
•Reducing the per capita costs of care
for populations.
6

Building Off
Current Initiatives
7
The existing healthcare delivery test reform models include MaineCare’s:
•Patient-Centered Medical Homes
•Emergency Department initiative
•Health Homes
•Accountable Communities
High-need Individual
Maine PCMH Pilot Community Care Teams
Transportation
Workplace
Environment
Food Systems
Shopping
Income
Heat
Faith Community
Literacy
Coaching
Physical Therapy
Hospital Services
Specialists
Outpatient Services
Med Mgt
HousingCare Mgt
Behav. Health & Sub
Abuse
Family
8

The Emergency
Department Initiative
9
• Identifying high-cost utilizers of hospital Emergency Departments and intensifying the efforts to manage their care
• Providing services in the most appropriate, cost-effective manner
• Establishing solid relationships with primary care providers andimproving patient outcomes
• Understanding the importance of social and non-medical barriers
• Total savings of $4.15 million in SFY ‘12 and $4.2 million in SFY ’13
• 1,700 patients currently participating in the program
Maine Health Homes
A Key to Sustainability
10
Stage A (ongoing):
•Health Home = Medical Home primary care practice + CCT
•Currently have 150 enrolled practices and 10 CCTs
•Payment weighted toward medical home
•Eligible Members:
• Two or more chronic conditions
• One chronic condition and at risk for another
Stage B (Fall Implementation):
•Health Homes = CCT with behavioral health expertise + primary care practice
•Payment weighted toward CCT
•Eligible Members:
• Adults with Serious Mental Illness
• Children with Serious Emotional Disturbance

Maine’s Accountable Communities:
The Basic Components
• Providers will work together and propose an alternative contract to share in any savings achieved
• The amount of shared savings will depend on achieving quality benchmarks
• Open to any willing and qualified providers statewide (through application process)
• Accountable Communities are not limited by geographical area
• Members retain choice of providers
• Alignment with aspects of other emerging ACOs is desired
• Flexible design encourages innovation
11
Benefits
for Providers
12
Patient Accountability
•Resources for shared decision-making
•Assistance with patient incentives, benefit design
Data Analytics
•EHR for behavioral health organizations
•Connection to Health Information Exchange
•Resources for other data analytic needs
Transformation Support
•Leadership training
•Practice transformation learning collaborative
•ACO learning collaborative
Payment Reform
•Greater consistency and alignment across payers/ initiatives
•Potential for performance-based shared savings payments

Benefits
For Patients
13
Ability to Compare Based on Quality and Cost Data
Coordinated CareDoctors and medical staff coordinate with other medical providers to make sure everyone is ‘on the same page’
Chronic Care ManagementAccess to care managers to make connections to non-medical resourcesTools for better self-managementCommunity health navigators
Specialized SupportAdults and children with developmental disabilities will be linked to doctors and caregivers who have been trained to meet their needs
Physical and Mental Health Integration
The Future State
Of HealthCare Delivery
14
System Change and Positive Outcomes Regardless of Payor Source
High Quality, Affordable Care Supported by:•Public Reporting•Pay for Quality•Total Cost of Care Benchmarks
Engaged Patients Supported through:•Review of Performance Measures•Shared decision-making•Access to personal health data/information
Outcome-Based Reimbursement Models•apitated populations•hared savings•lobal payments

The Future State
Of HealthCare Delivery
15
Data-Informed Care•Access to ‘real time’ clinical data•Timely claims data•Public health data
Improved Population Health Management through:•Patient-Centered Medical Homes•Health Homes•Accountable Care
Keys to
Our Success
• Ability to run and provide transparent, accurate and reliable member attribution, cost and quality metrics
• Provider partnership with DHHS in initiatives
• Outreach to potential providers in most rural areas
• Community-based approaches that go beyond a medical model to encompass behavioral health and social supports
• Facilitation of provider use of Electronic Health Records, Health Information Exchange and other secure data sharing methods
16

For More
Information
Mary. C. Mayhew, Commissioner
Maine Department of Health and Human Services
(207) 287-4223
17