lymphoma lab linfoma di hodgkin: terapia di consolidamento ... · linfoma di hodgkin: terapia di...
TRANSCRIPT
www.lymphomalab.it
LYMPHOMA LAB
Start Up Meeting> Roma, 27 Novembre 2018STARHOTELS METROPOLEVia Principe Amedeo, 3
Linfoma di Hodgkin:terapia di consolidamento
post trapianto autologo
A cura di: Francesco Merli, Ematologia AUSL-IRCCS Reggio Emilia
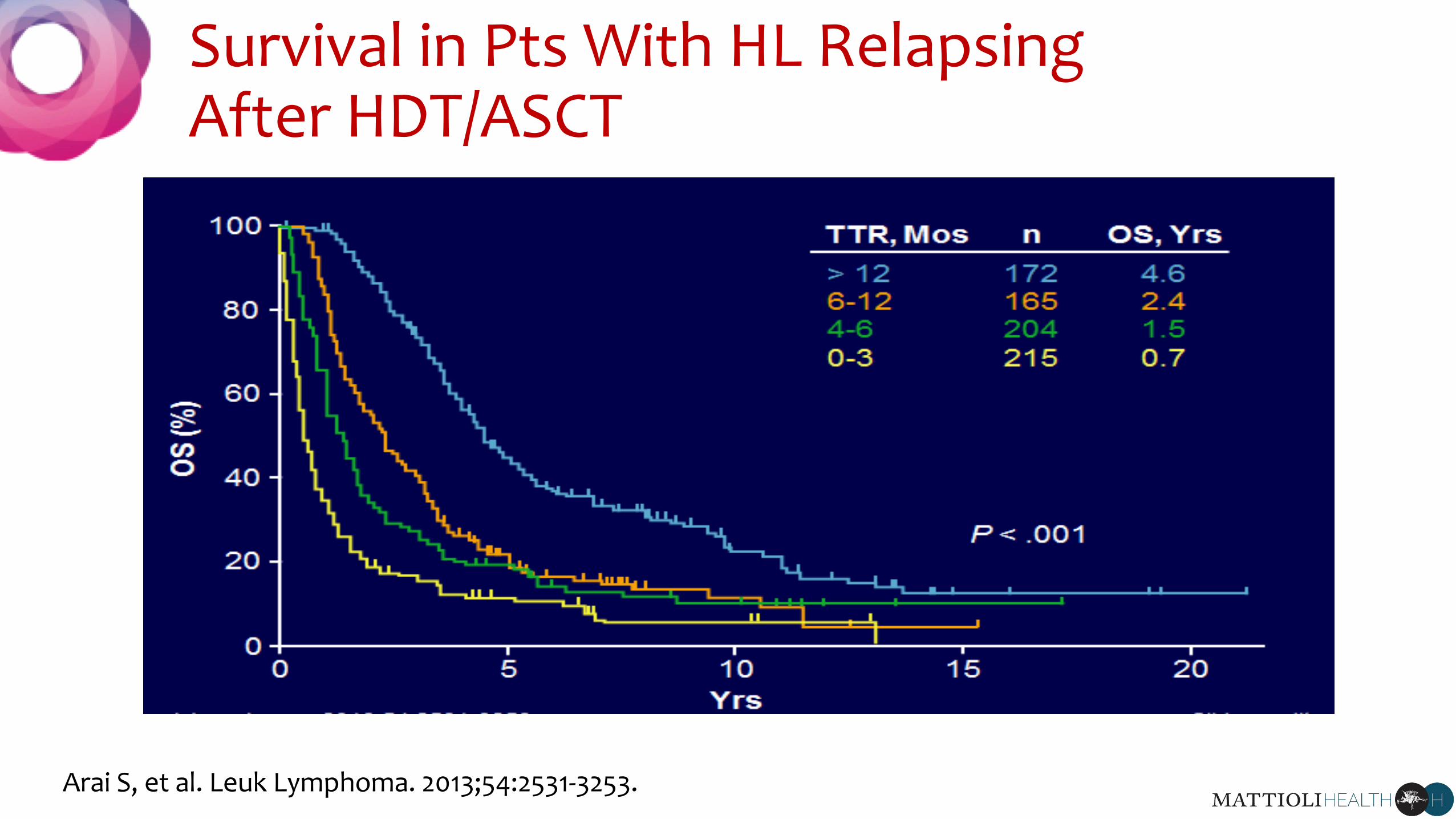
Survival in Pts With HL Relapsing After HDT/ASCT
Arai S, et al. Leuk Lymphoma. 2013;54:2531-3253.
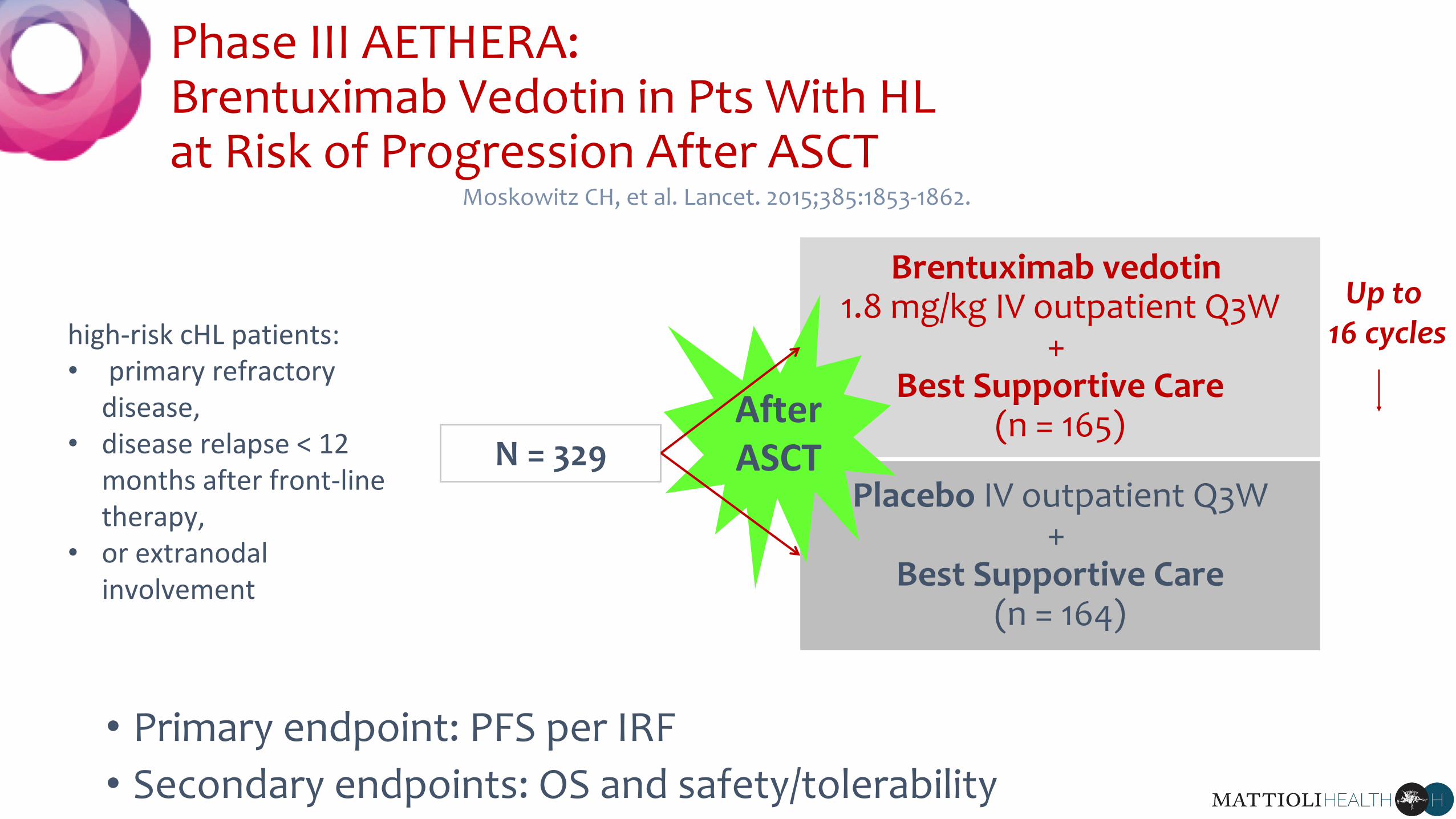
Phase III AETHERA: Brentuximab Vedotin in Pts With HL at Risk of Progression After ASCT
• Primary endpoint: PFS per IRF
• Secondary endpoints: OS and safety/tolerability
N = 329
Brentuximab vedotin1.8 mg/kg IV outpatient Q3W
+ Best Supportive Care
(n = 165)
Placebo IV outpatient Q3W+
Best Supportive Care(n = 164)
Up to 16 cycles
Moskowitz CH, et al. Lancet. 2015;385:1853-1862.
AfterASCT
high-risk cHL patients:• primary refractory
disease, • disease relapse < 12
months after front-line therapy,
• or extranodalinvolvement

AETHERA: Baseline Pt CharacteristicsPt Characteristic BV (n = 165) Placebo (n = 164)
Median age, yrs (range) 33 (18-71) 32 (18-76)
Males, % 46 59
Previous systemic salvage therapies %
1 57 52
≥ 2 (median: 2; range: 2-8) 43 48
HL status after frontline therapy, %
Refractory 60 59
Relapse < 12 mos 32 33
Relapse ≥ 12 mos with extranodal disease 8 8
Response with salvage therapy pre autoHSCT,* %
CR 37 38
PR 35 34
SD 28 28
Moskowitz CH, et al. Lancet. 2015;385:1853-1862. *PET scans not mandatory in protocol.
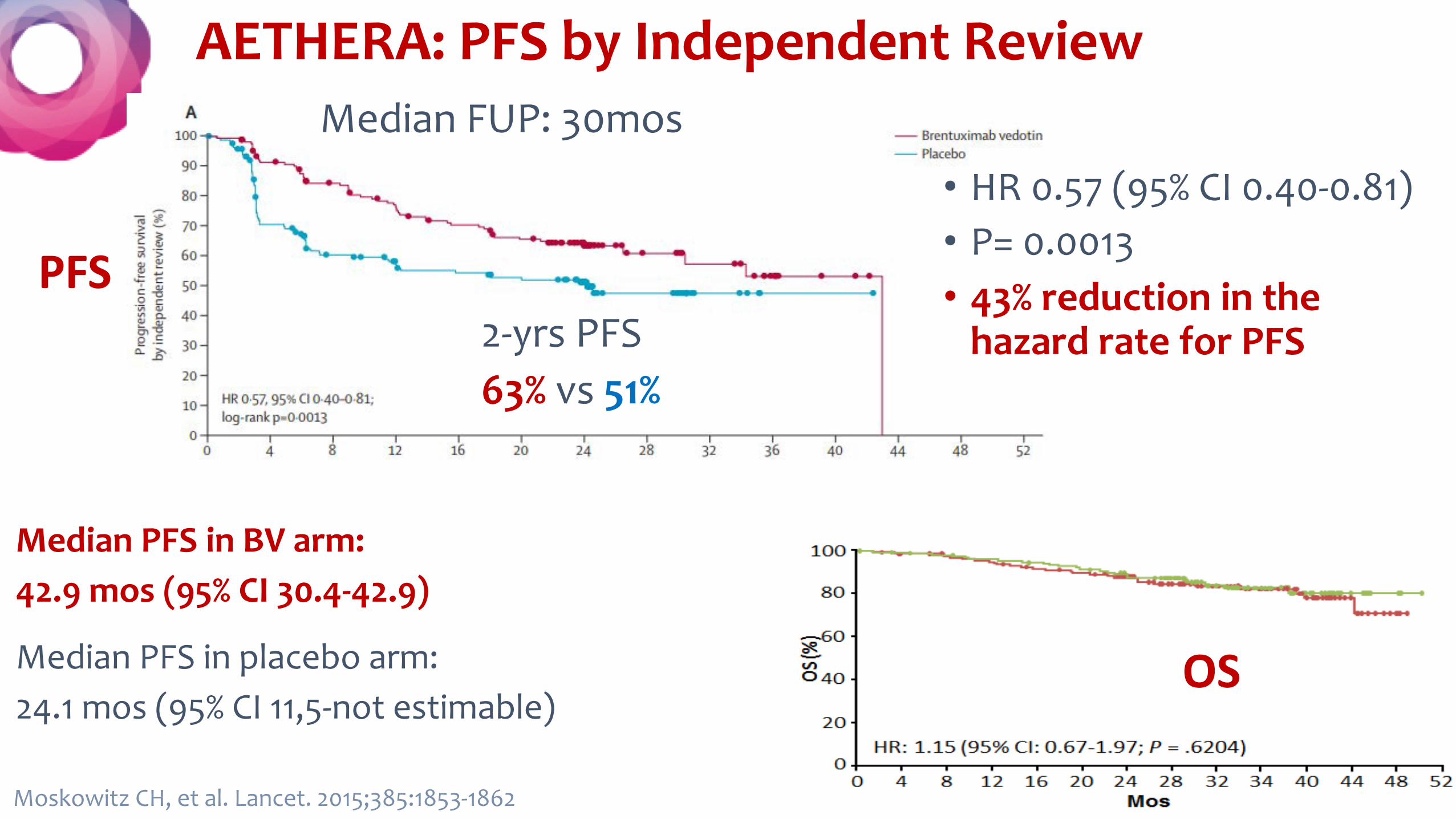
AETHERA: PFS by Independent Review
OS
Moskowitz CH, et al. Lancet. 2015;385:1853-1862
PFS• HR 0.57 (95% CI 0.40-0.81)• P= 0.0013• 43% reduction in the
hazard rate for PFS
Median FUP: 30mos
Median PFS in BV arm: 42.9 mos (95% CI 30.4-42.9)
Median PFS in placebo arm: 24.1 mos (95% CI 11,5-not estimable)
2-yrs PFS63% vs 51%
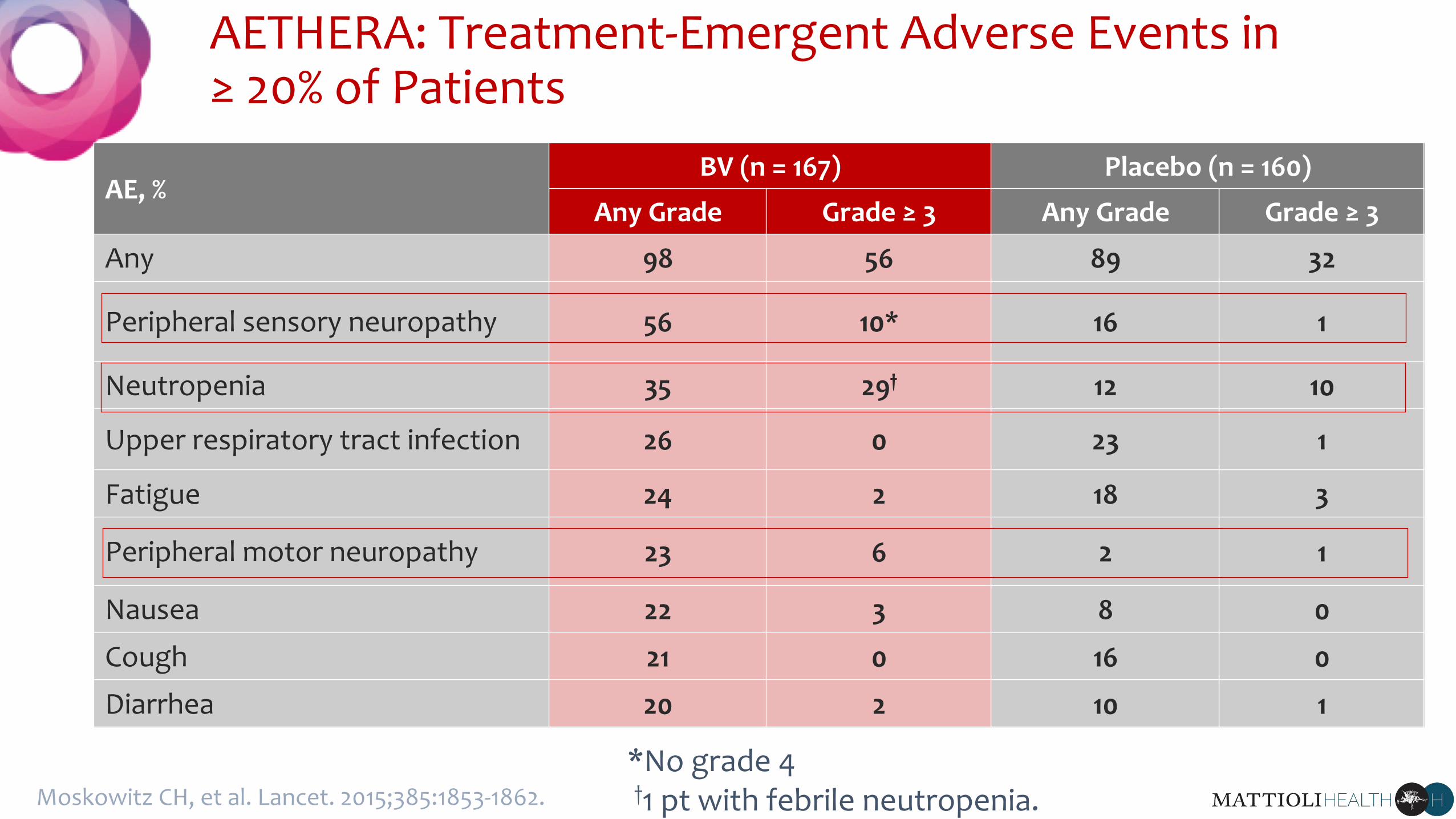
AETHERA: Treatment-Emergent Adverse Events in ≥ 20% of Patients
AE, %BV (n = 167) Placebo (n = 160)
Any Grade Grade ≥ 3 Any Grade Grade ≥ 3
Any 98 56 89 32
Peripheral sensory neuropathy 56 10* 16 1
Neutropenia 35 29† 12 10
Upper respiratory tract infection 26 0 23 1
Fatigue 24 2 18 3
Peripheral motor neuropathy 23 6 2 1
Nausea 22 3 8 0
Cough 21 0 16 0
Diarrhea 20 2 10 1
Moskowitz CH, et al. Lancet. 2015;385:1853-1862.
*No grade 4†1 pt with febrile neutropenia.
Moskowitz CH, et al. Lancet. 2015;385:1853-1862.
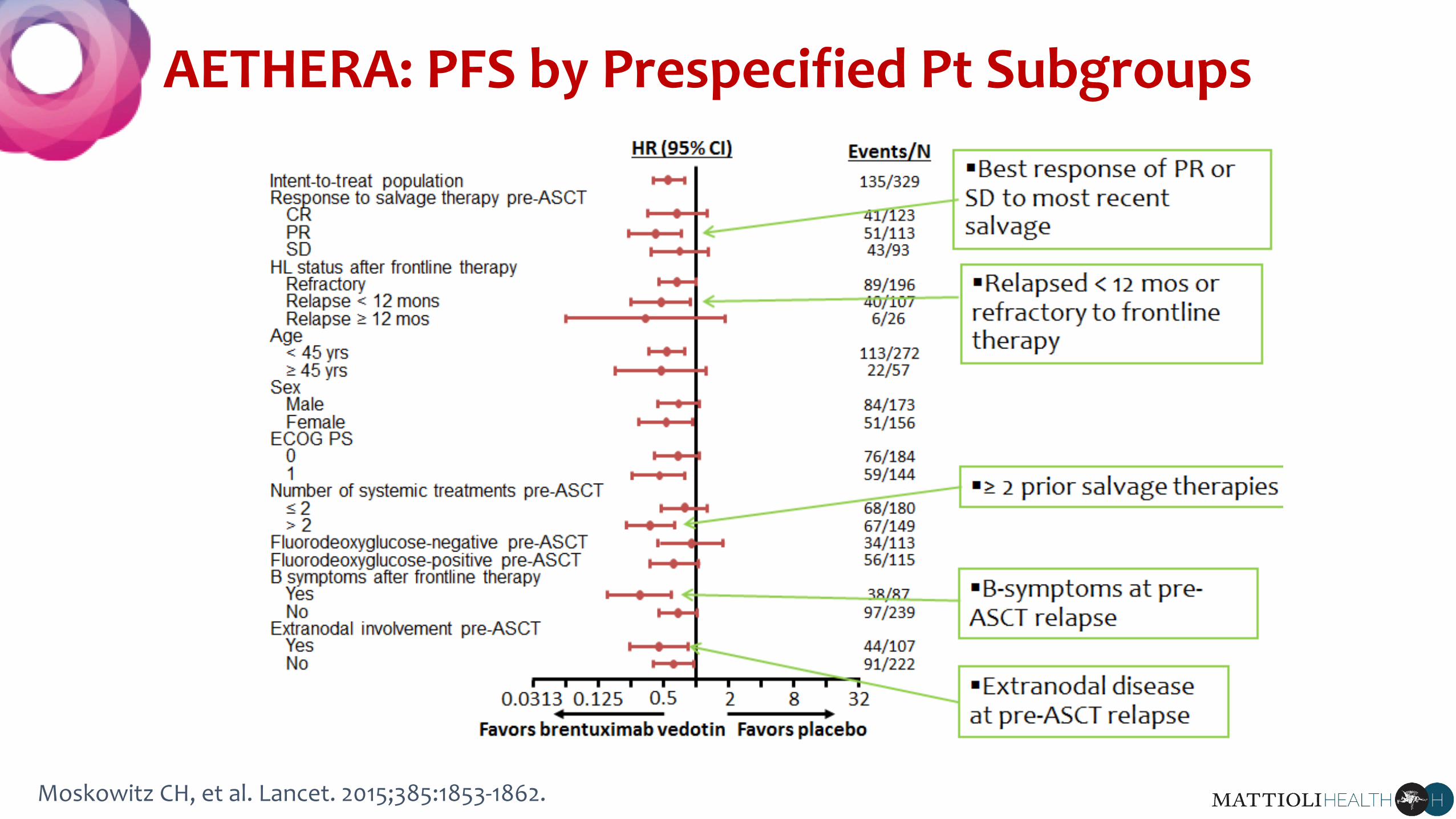
AETHERA: PFS by Prespecified Pt Subgroups
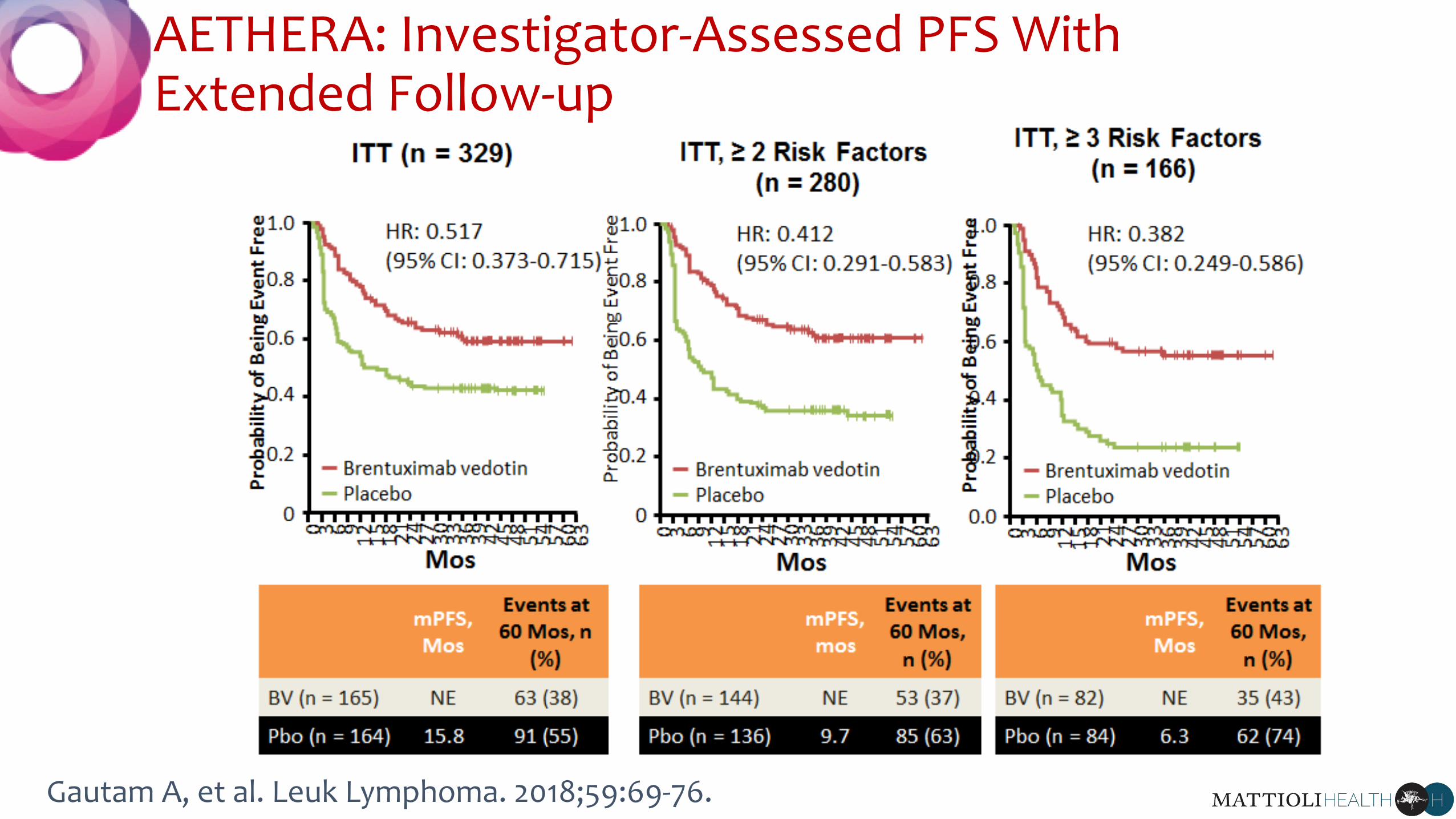
AETHERA: Investigator-Assessed PFS With Extended Follow-up
Gautam A, et al. Leuk Lymphoma. 2018;59:69-76.
AETHERA: Conclusions
“delivery of brentuximab vedotin as consolidation therapy was generally well
tolerated immediately after ASCT and provided a sustained PFS benefit for
patients with HL with risk factors for relapse or progression after autologous
stem-cell transplantation salvage therapy”
“Consolidation therapy with brentuximab vedotin might increase the possibility
of cure or potentially avoid exposure to subsequent toxic therapies, and seems
to be effective in this young cancer population with high unmet need”
Moskowitz CH, et al. Lancet. 2015;385:1853-1862.
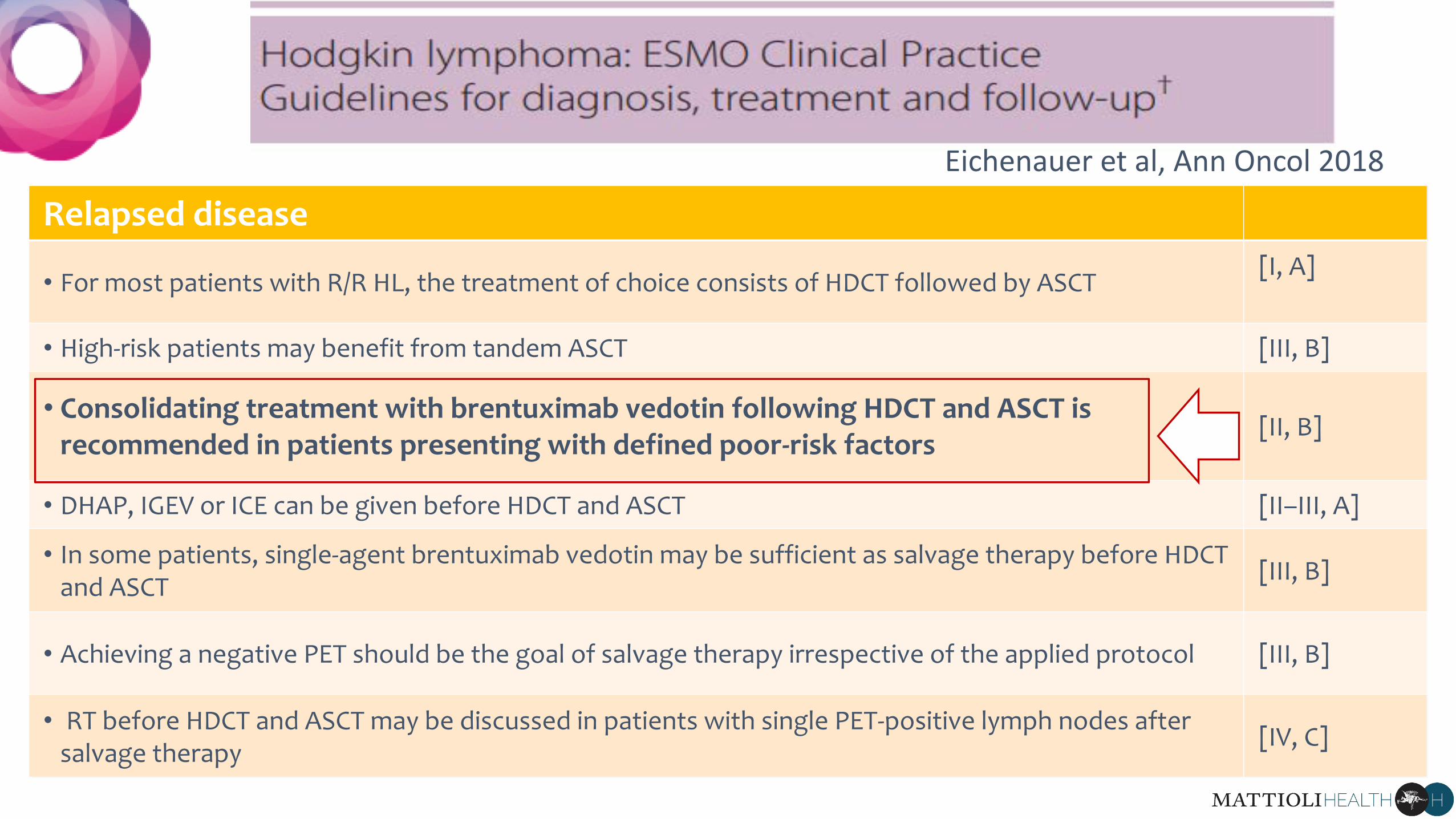
Relapsed disease
• For most patients with R/R HL, the treatment of choice consists of HDCT followed by ASCT [I, A]
• High-risk patients may benefit from tandem ASCT [III, B]
• Consolidating treatment with brentuximab vedotin following HDCT and ASCT is recommended in patients presenting with defined poor-risk factors
[II, B]
• DHAP, IGEV or ICE can be given before HDCT and ASCT [II–III, A]
• In some patients, single-agent brentuximab vedotin may be sufficient as salvage therapy before HDCT and ASCT [III, B]
• Achieving a negative PET should be the goal of salvage therapy irrespective of the applied protocol [III, B]
• RT before HDCT and ASCT may be discussed in patients with single PET-positive lymph nodes after salvage therapy [IV, C]
Eichenauer et al, Ann Oncol 2018
2017
Purpose: to evaluate the addiction of CONSOLIDATIVE RADIATION THERAPY after HD tehrapy and ASCT for R/R HL
80 consecutive patients (2005-2014)
Eligible patients:
• persistent nodal masses >= 2 cm or
• sites suspicious for residual disease involvement on day +28 post ASCT
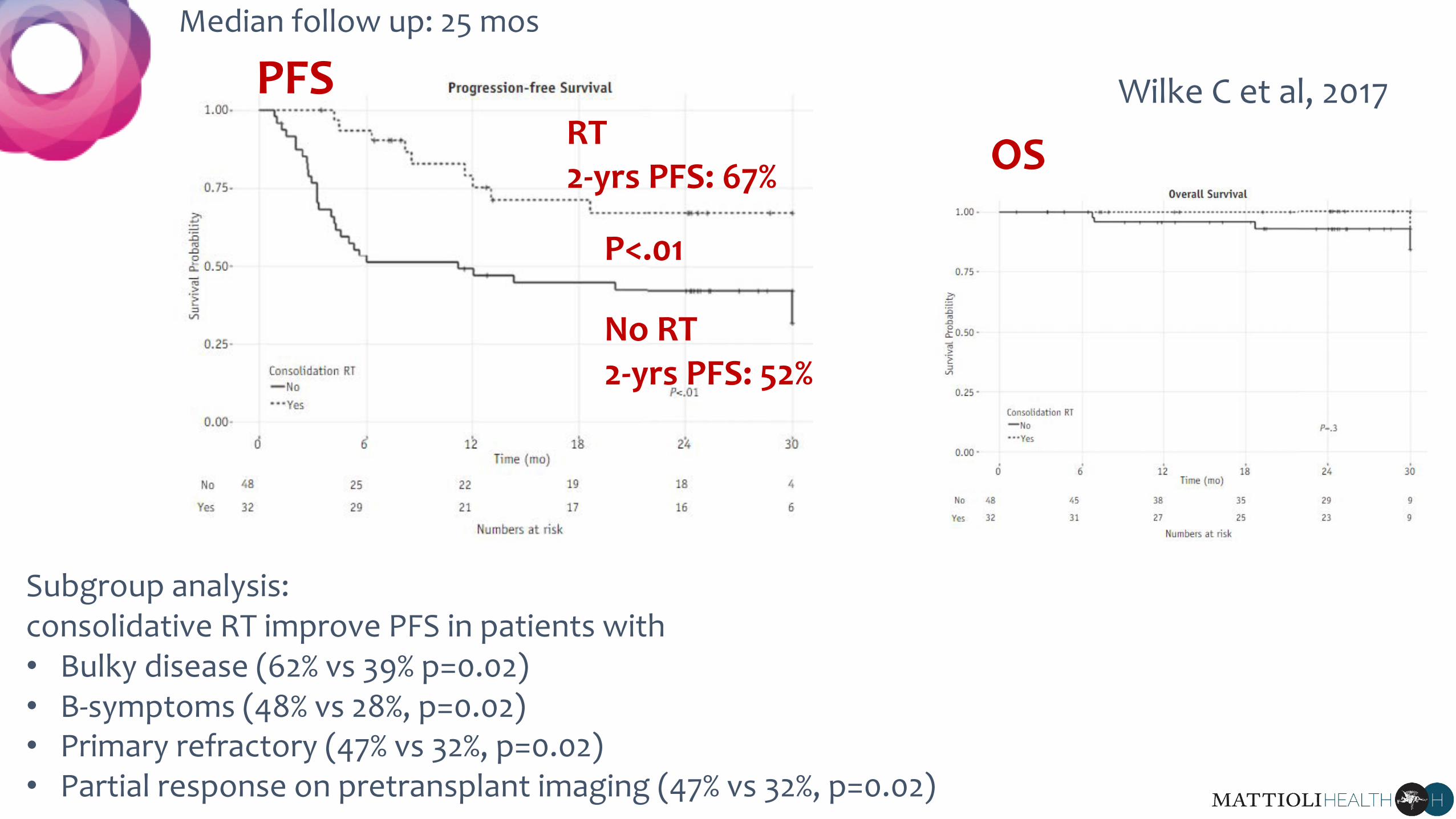
Wilke C et al, 2017 RT2-yrs PFS: 67%
No RT 2-yrs PFS: 52%
PFS OS
Median follow up: 25 mos
P<.01
Subgroup analysis: consolidative RT improve PFS in patients with• Bulky disease (62% vs 39% p=0.02)• B-symptoms (48% vs 28%, p=0.02)• Primary refractory (47% vs 32%, p=0.02)• Partial response on pretransplant imaging (47% vs 32%, p=0.02)
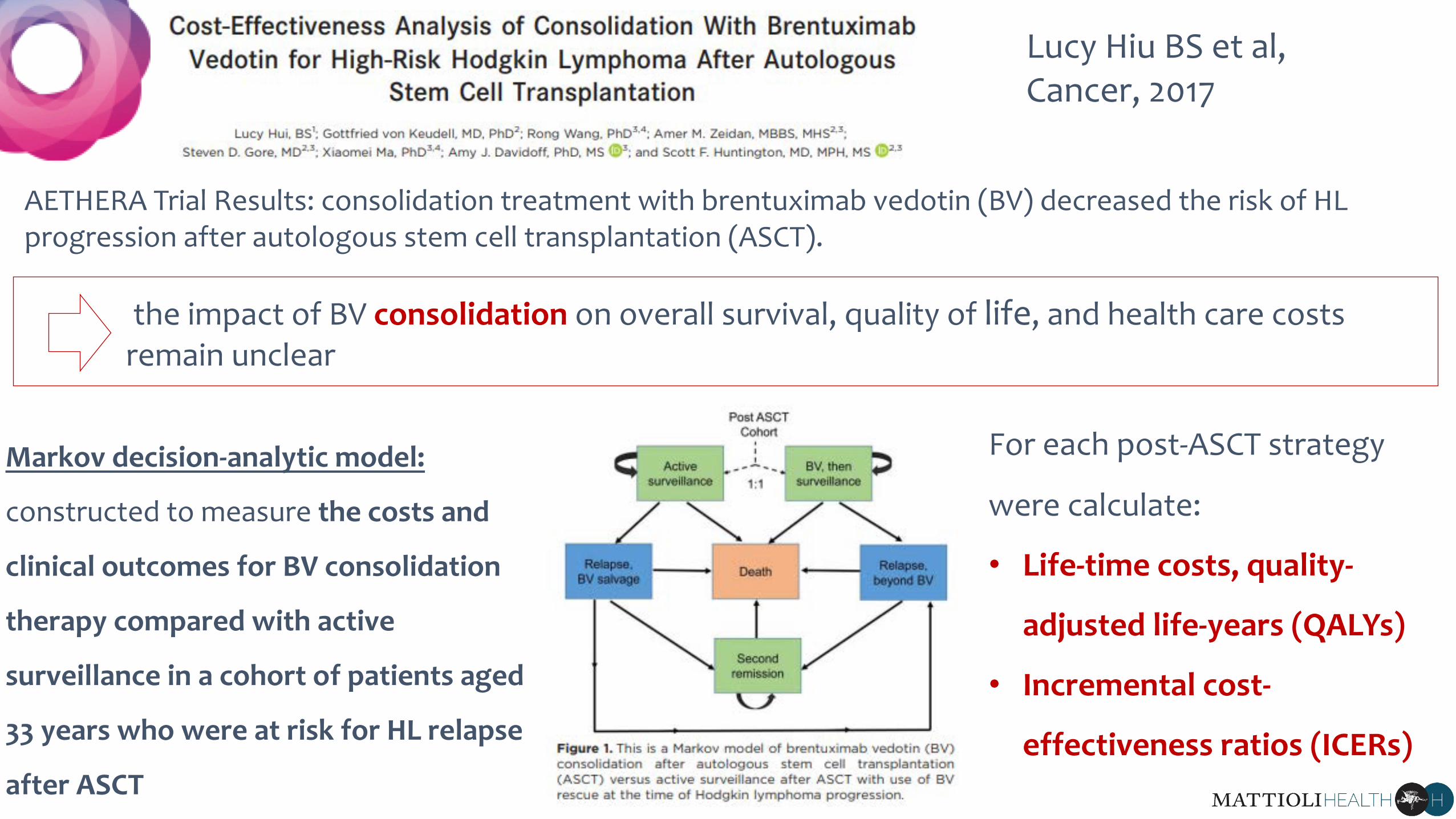
Lucy Hiu BS et al, Cancer, 2017
AETHERA Trial Results: consolidation treatment with brentuximab vedotin (BV) decreased the risk of HL progression after autologous stem cell transplantation (ASCT).
the impact of BV consolidation on overall survival, quality of life, and health care costs remain unclear
Markov decision-analytic model:
constructed to measure the costs and
clinical outcomes for BV consolidation
therapy compared with active
surveillance in a cohort of patients aged
33 years who were at risk for HL relapse
after ASCT
For each post-ASCT strategy
were calculate:
• Life-time costs, quality-
adjusted life-years (QALYs)
• Incremental cost-
effectiveness ratios (ICERs)
ICER
The incremental cost-effectiveness ratio (ICER) is a statistic used in cost-effectiveness analysis to
summarise the cost-effectiveness of a health care intervention. It is defined by the difference in
cost between two possible interventions, divided by the difference in their effect. It represents
the average incremental cost associated with 1 additional unit of the measure of effect.
QALY
The quality-adjusted life year or quality-adjusted life-year (QALY) is a generic measure of disease
burden, including both the quality and the quantity of life lived. It is used in economic
evaluation to assess the value for money of medical interventions
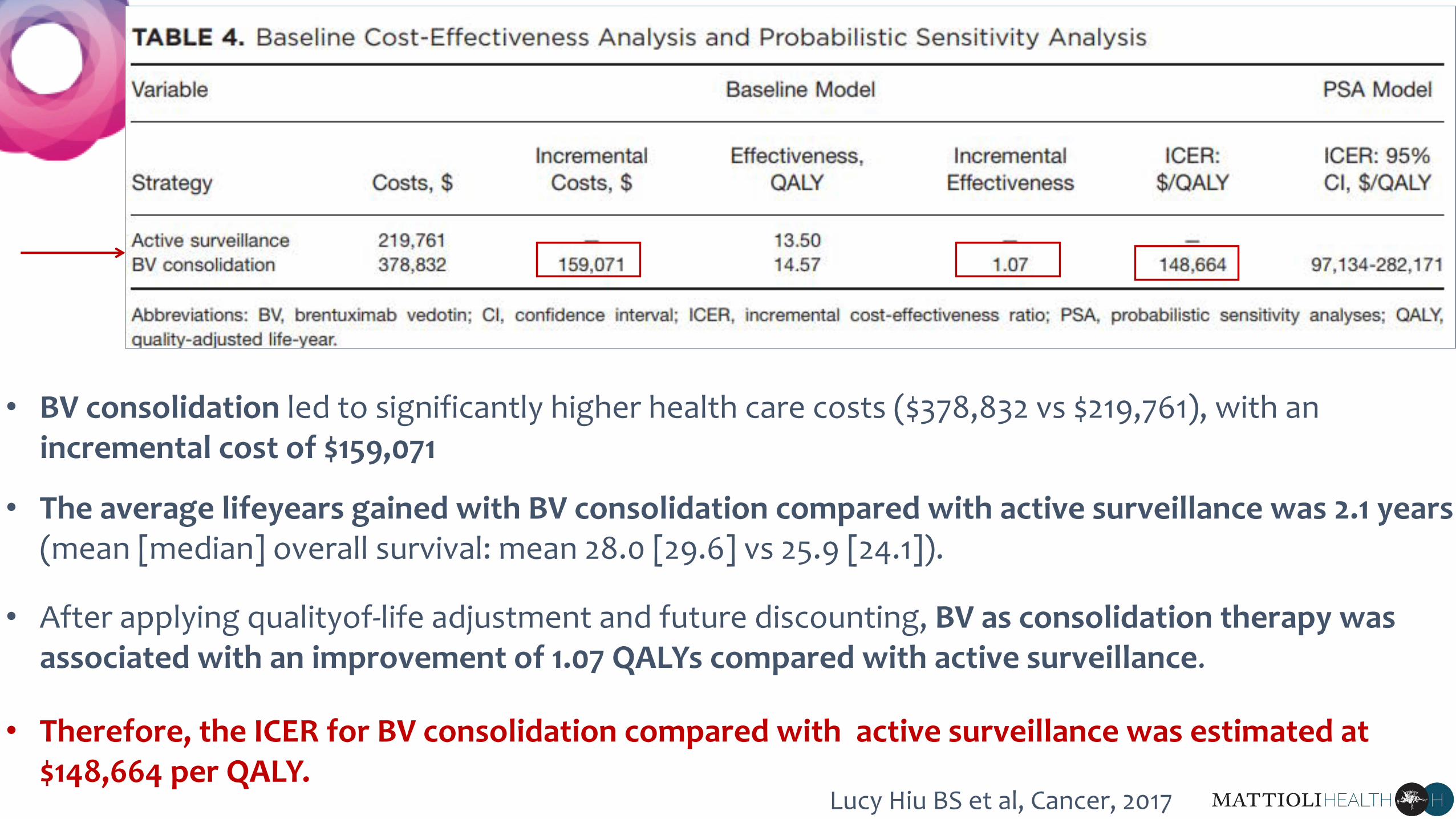
• BV consolidation led to significantly higher health care costs ($378,832 vs $219,761), with an incremental cost of $159,071
• The average lifeyears gained with BV consolidation compared with active surveillance was 2.1 years (mean [median] overall survival: mean 28.0 [29.6] vs 25.9 [24.1]).
• After applying qualityof-life adjustment and future discounting, BV as consolidation therapy was associated with an improvement of 1.07 QALYs compared with active surveillance.
• Therefore, the ICER for BV consolidation compared with active surveillance was estimated at $148,664 per QALY.
Lucy Hiu BS et al, Cancer, 2017
The incremental clinical benefit of BV consolidation was associated with significant
health care expenditures, producing an ICER of $148,664 per QALY.
• In the setting of HL after ASCT, approximately 50% of individuals will remain free from HL
recurrence without additional therapy
• Even when selecting patients at high risk using clinical parameters, considerable
proportions remain in remission post-ASCT and are unlikely to benefit from upfront
consolidation with BV
• Among patients with confirmed HL relapse post-ASCT, an overwhelming majority will
derive clinical benefit from BV therapy
Lucy Hiu BS et al, Cancer, 2017

• Under indication-specific pricing, BV in the consolidation setting would be priced
lower than BV used for post-ASCT salvage
• ultimately, our model indicated that price reductions for BV in the consolidative
setting from 18% to 38% produced more reasonable ICERs of $100,000 per QALY and
$50,000 per QALY, respectively.
CONCLUSIONS:
BV as consolidation therapy under current US pricing is unlikely to be cost
effective at a willingness-to-pay threshold of $100,000 per QALY.
However, indication-specific price reductions for the consolidative setting
could reduce ICERs to widely acceptable values.
Lucy Hiu BS et al, Cancer, 2017
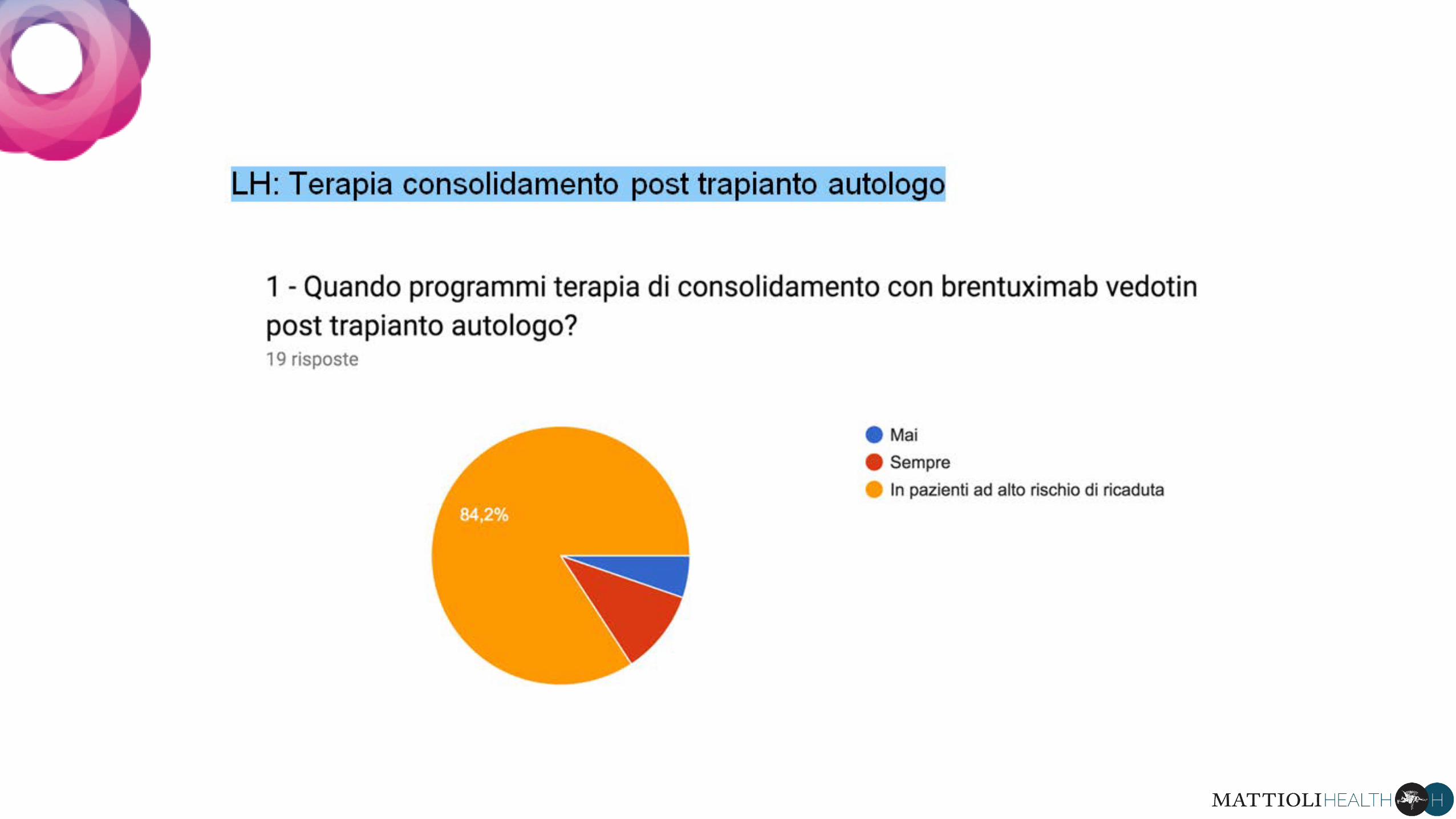
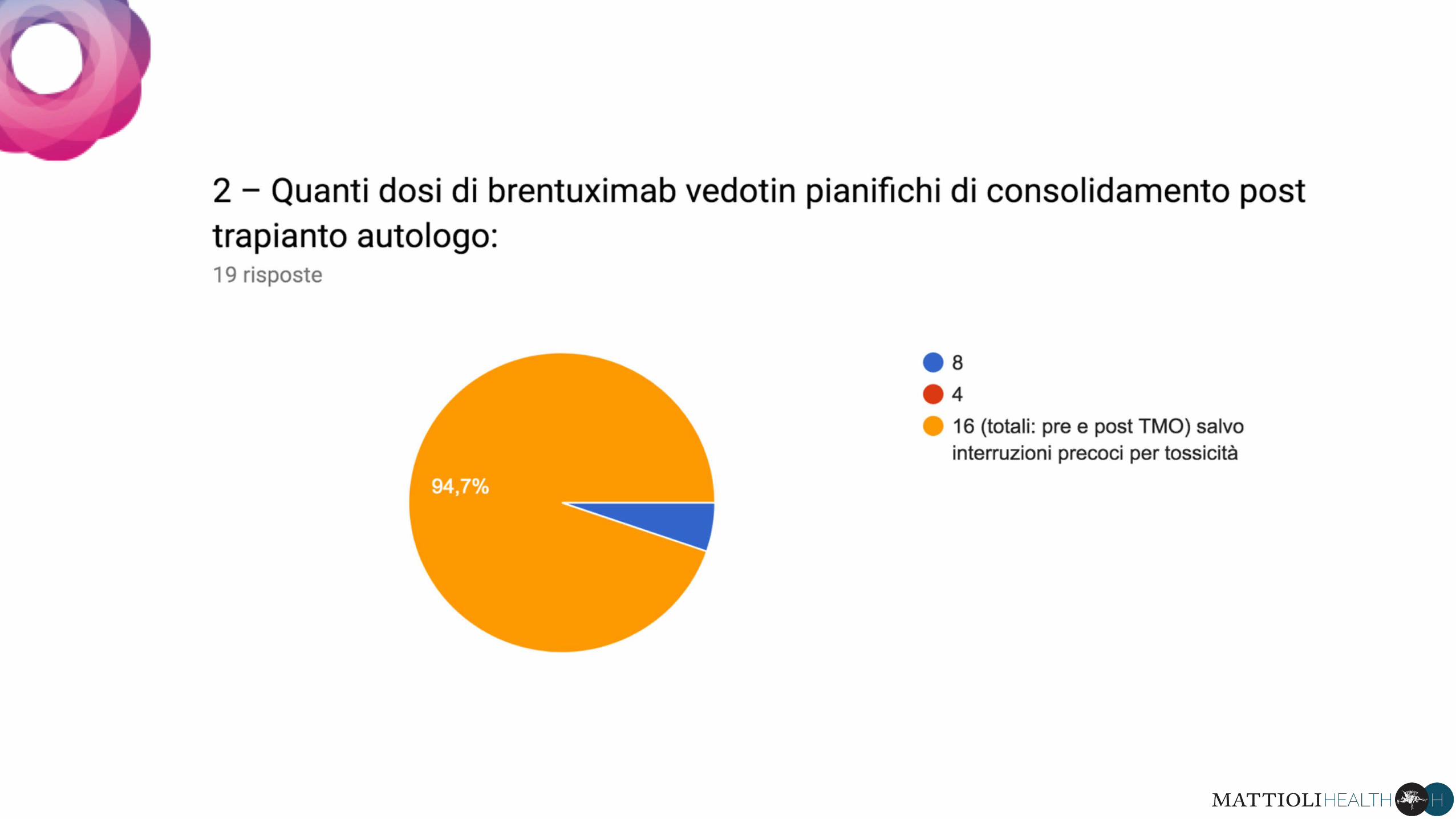
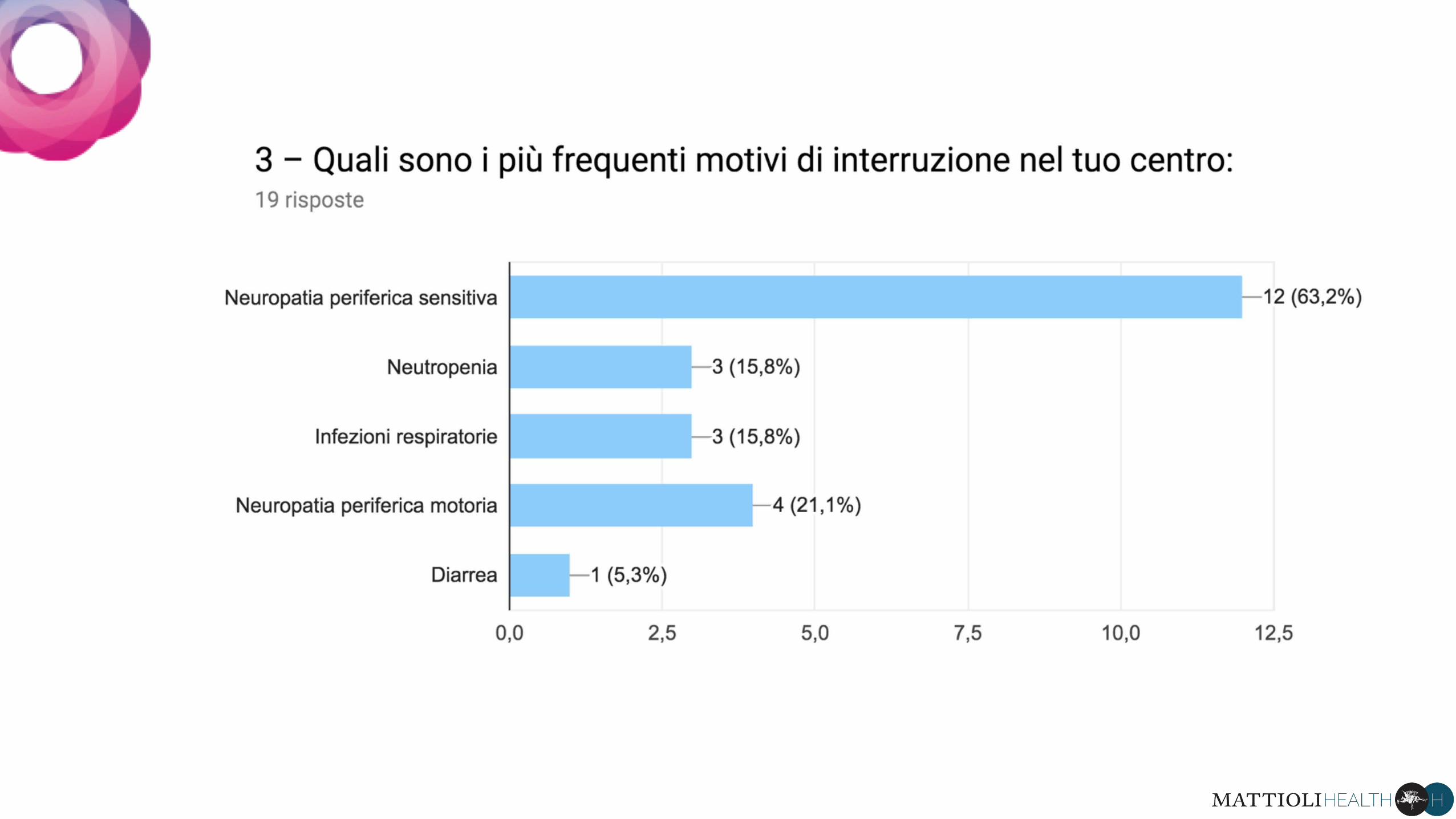
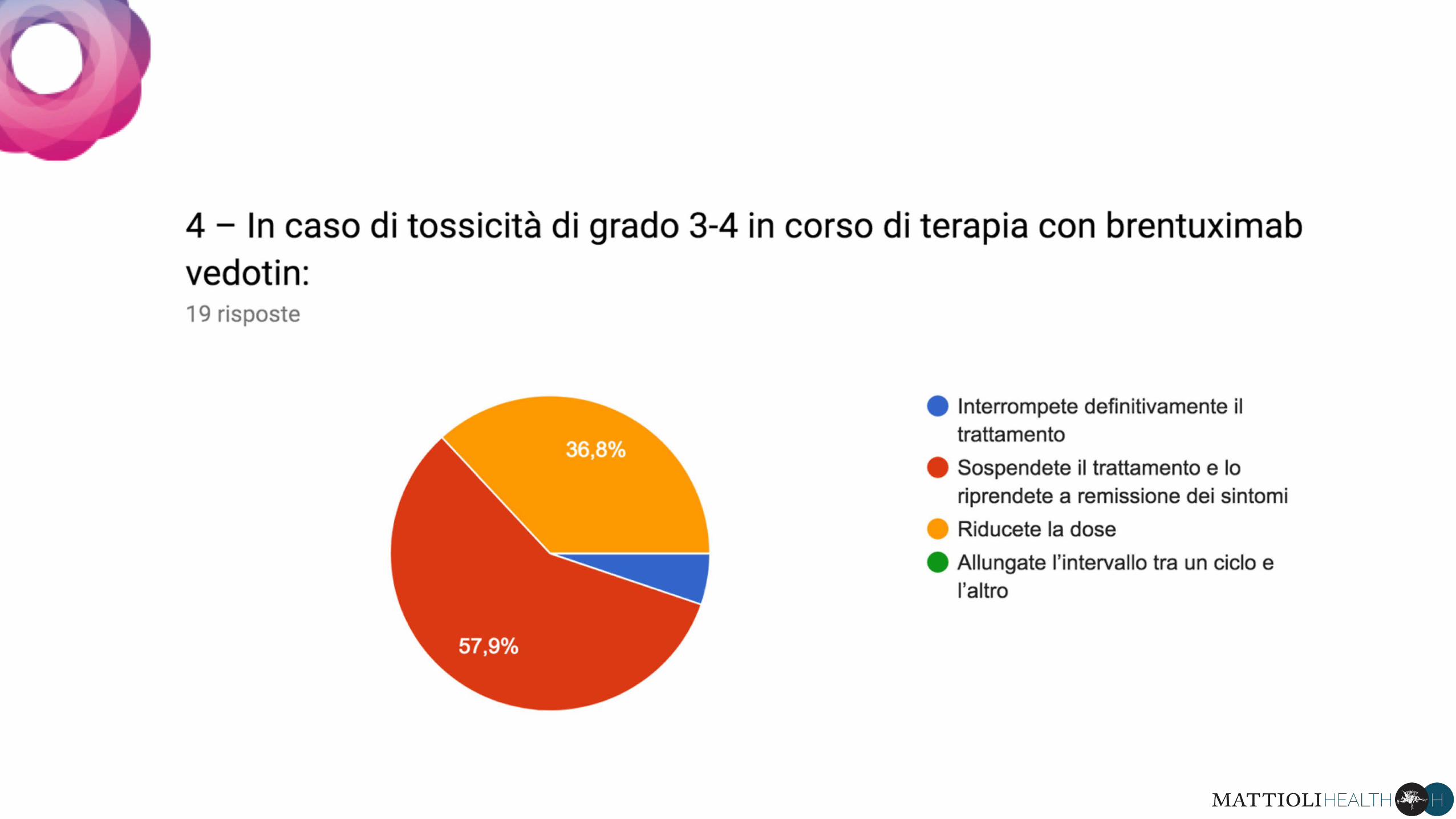
Linfoma di Hodgkin:terapia di consolidamento post
trapianto autologo
RISULTATI DELLA SURVEY