luxation-instabilités carpe aderf - copie.pdf
TRANSCRIPT
Luxations et instabilités du carpe
Christian Dumontier, Sylvie Carmès SOS Mains, CHU de Nice
Très compliqué
Instabilités radio-carpienne
Instabilités intra-carpiennes
Instabilités médio-carpiennes
Dissociatives, non-dissociatives, adaptatives….
Le point commun, une anomalie dans la dynamique du carpe
Les luxations intra-carpiennes
2 formes: Luxation pure ou fracture luxation
Lésions rares
Lésions fréquemment méconnues (1/3 des cas)
Traumatisme à haute énergie ou polytraumatisme (adulte jeune de sexe plutôt masculin)
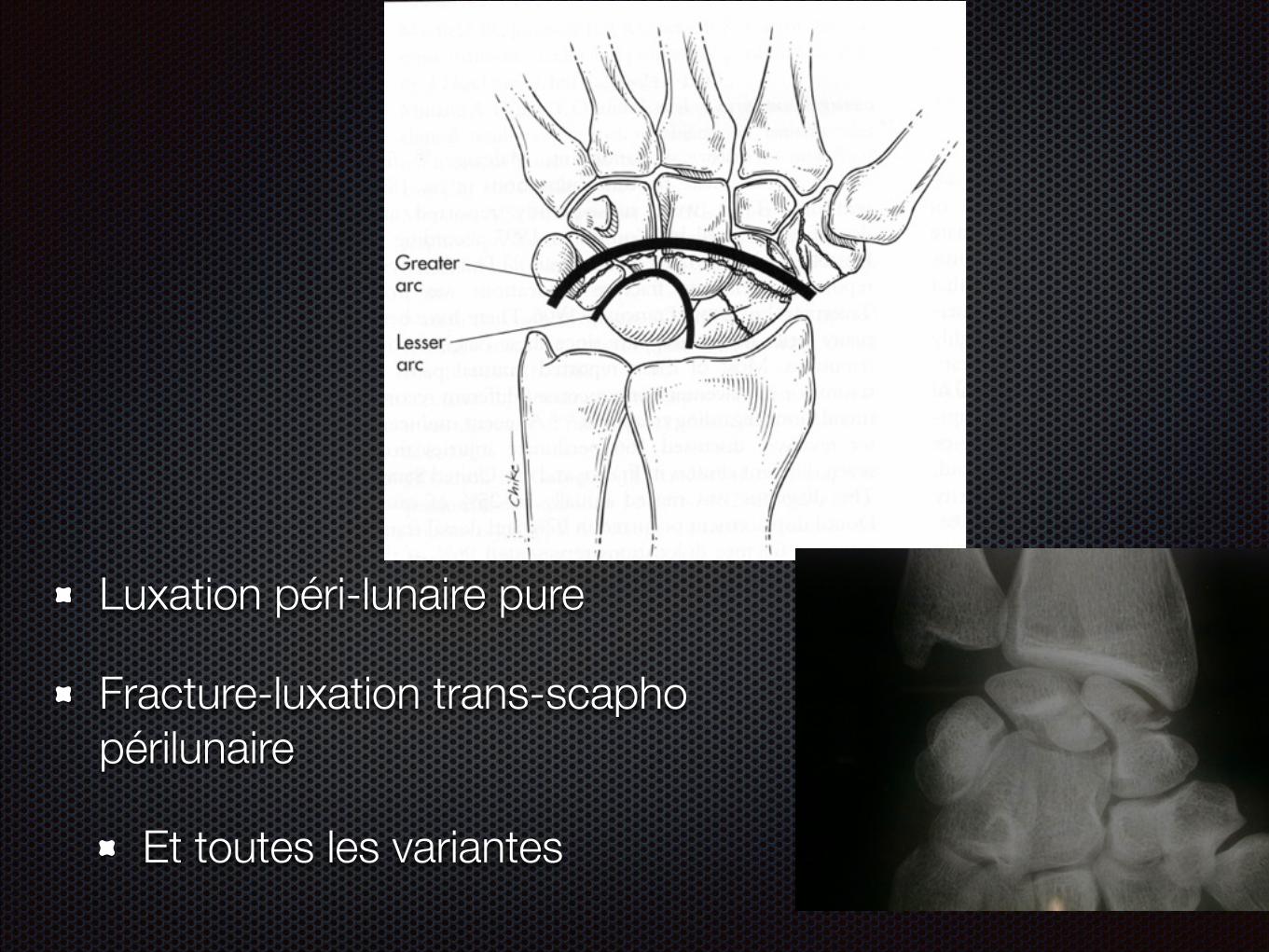
Luxation péri-lunaire pure
Fracture-luxation trans-scapho périlunaire
Et toutes les variantes
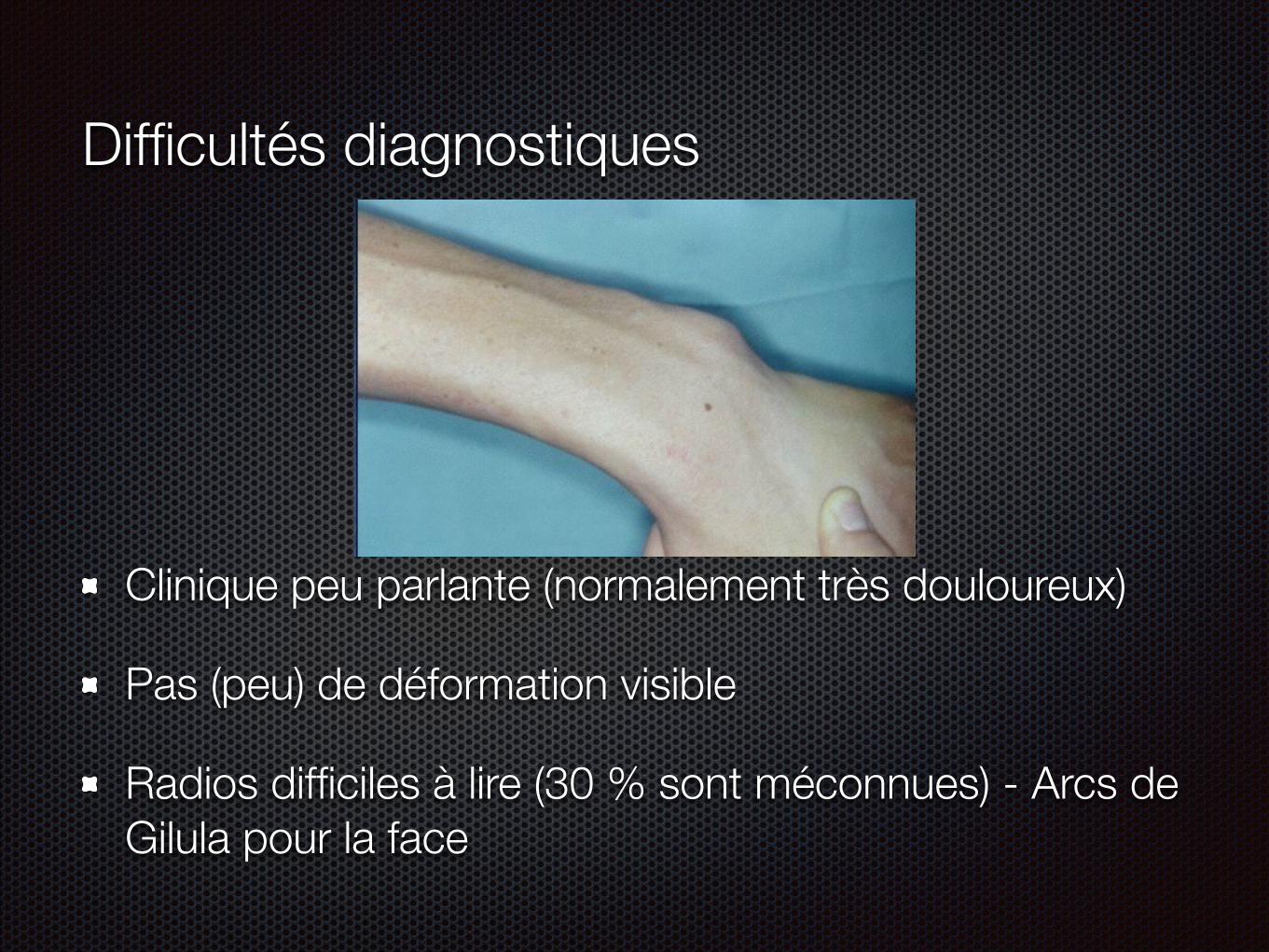
Difficultés diagnostiques
Clinique peu parlante (normalement très douloureux)
Pas (peu) de déformation visible
Radios difficiles à lire (30 % sont méconnues) - Arcs de Gilula pour la face
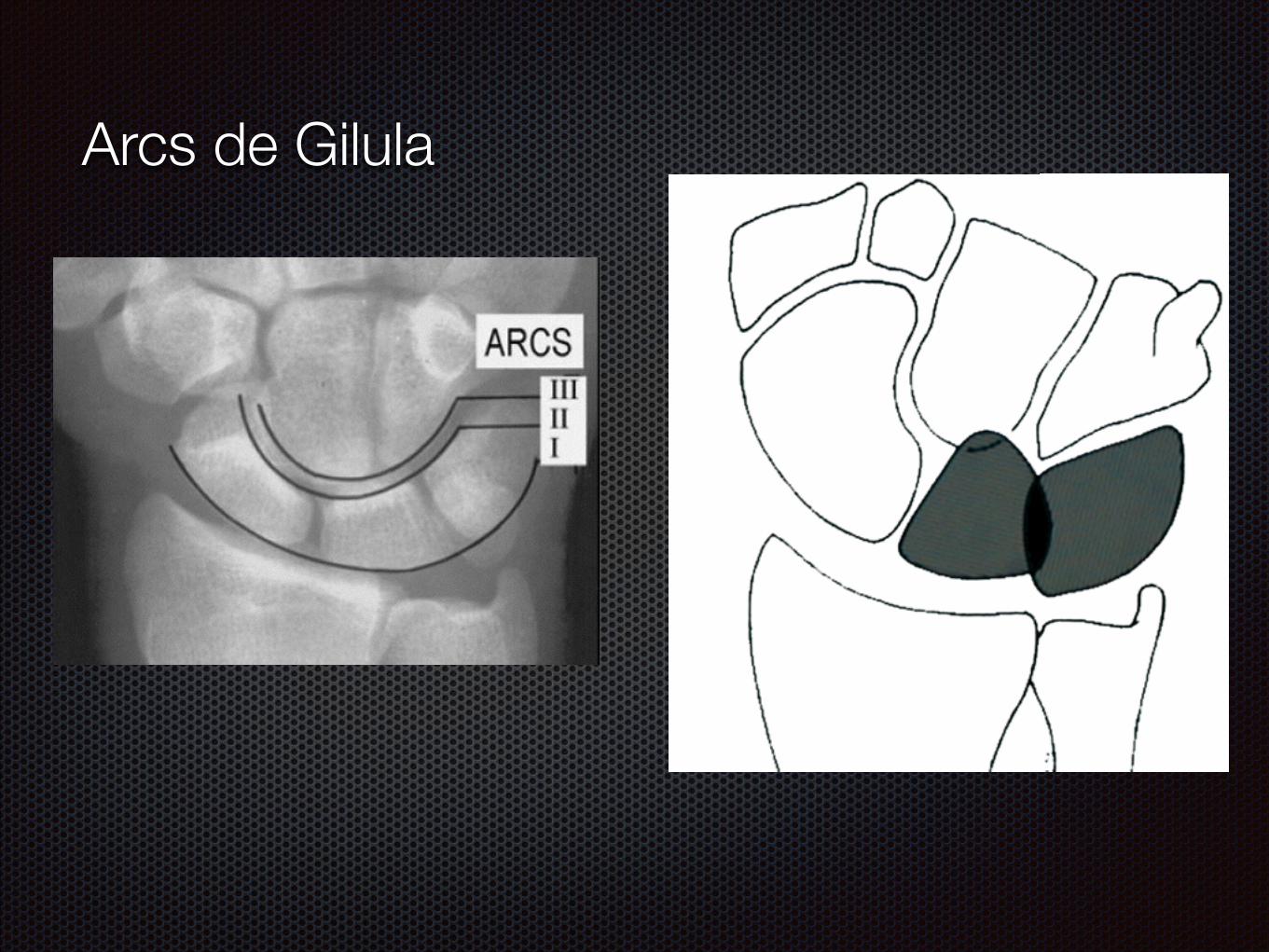
Arcs de Gilula
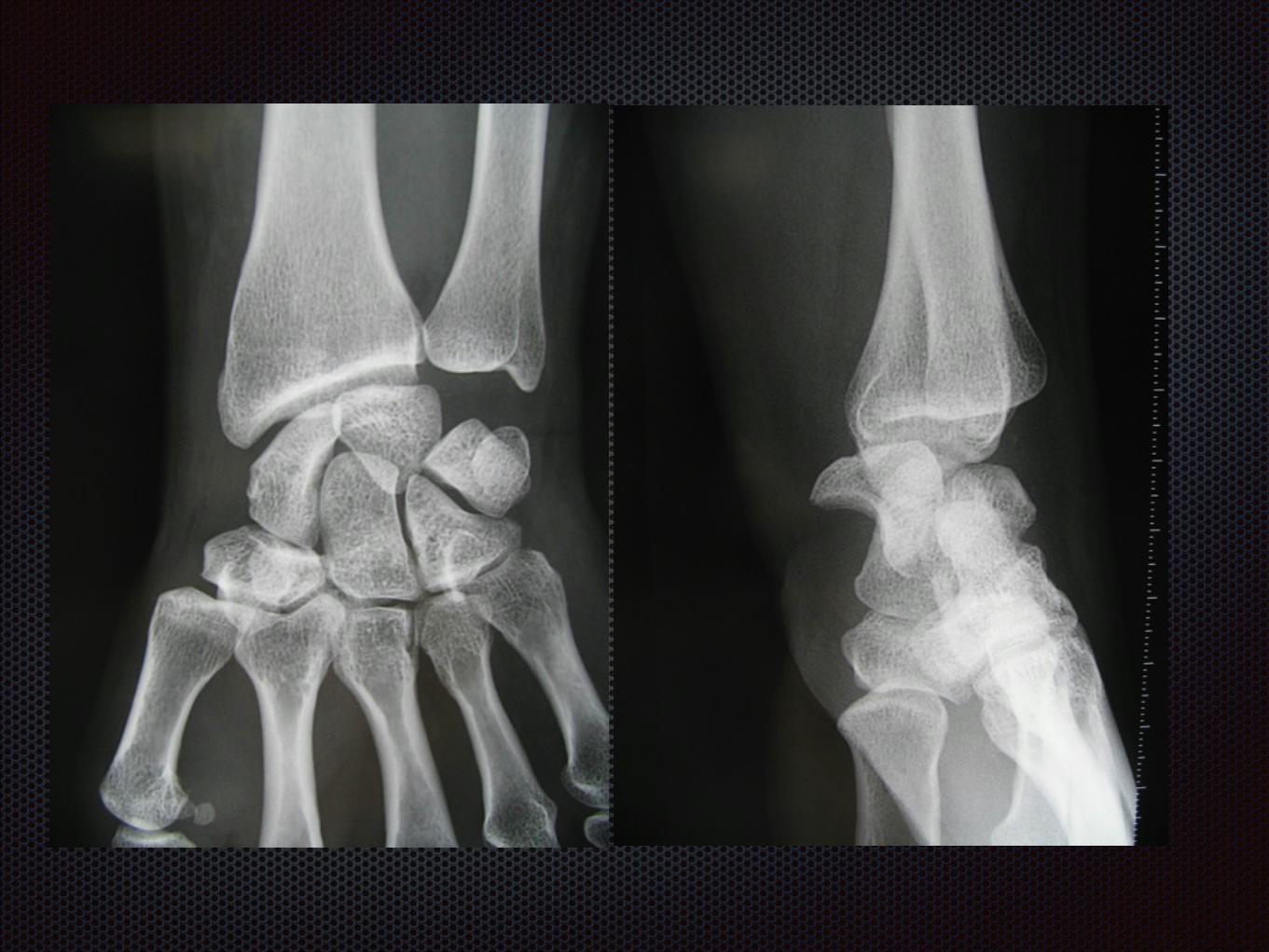


De profil !
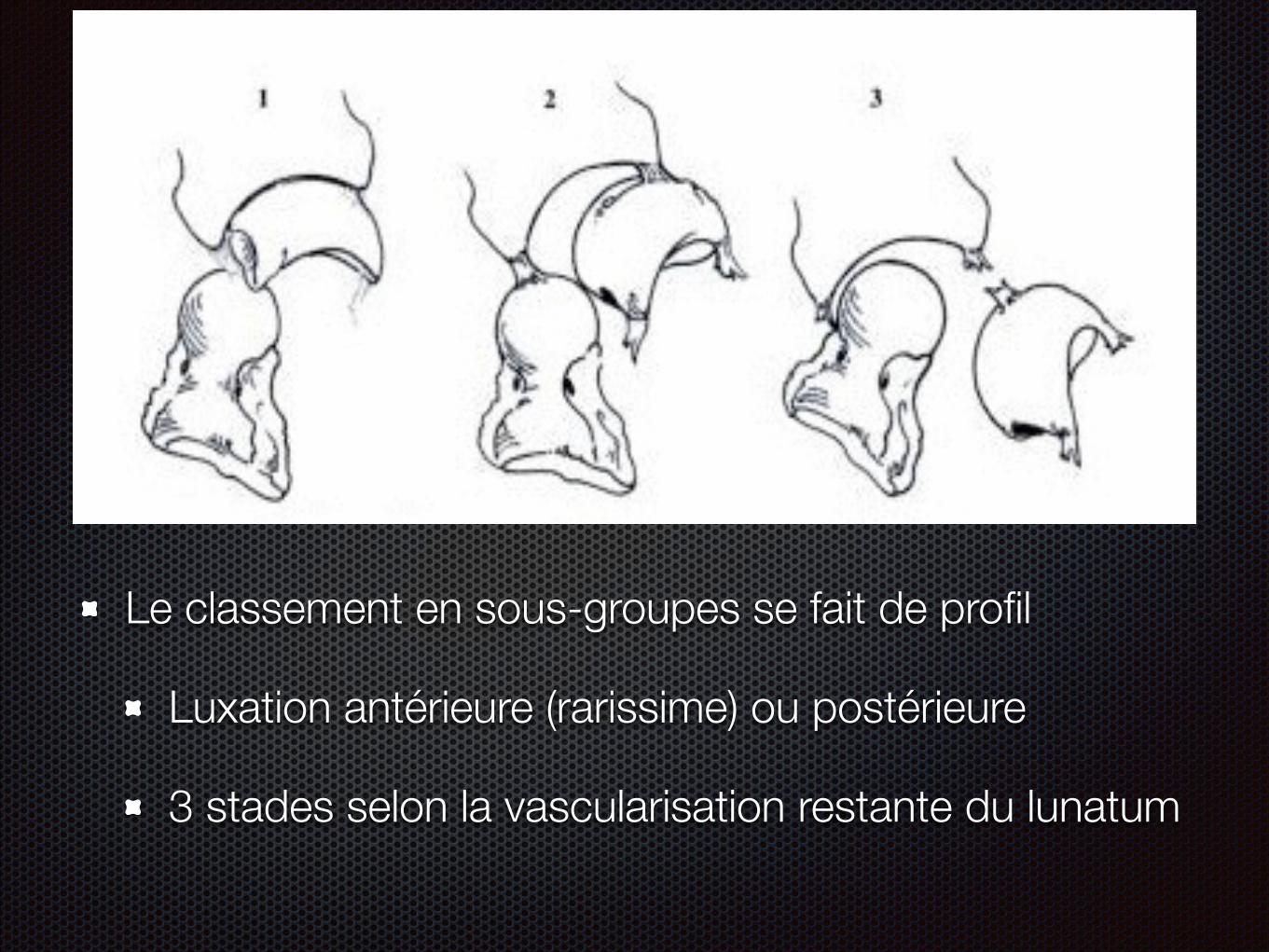
Le classement en sous-groupes se fait de profil
Luxation antérieure (rarissime) ou postérieure
3 stades selon la vascularisation restante du lunatum
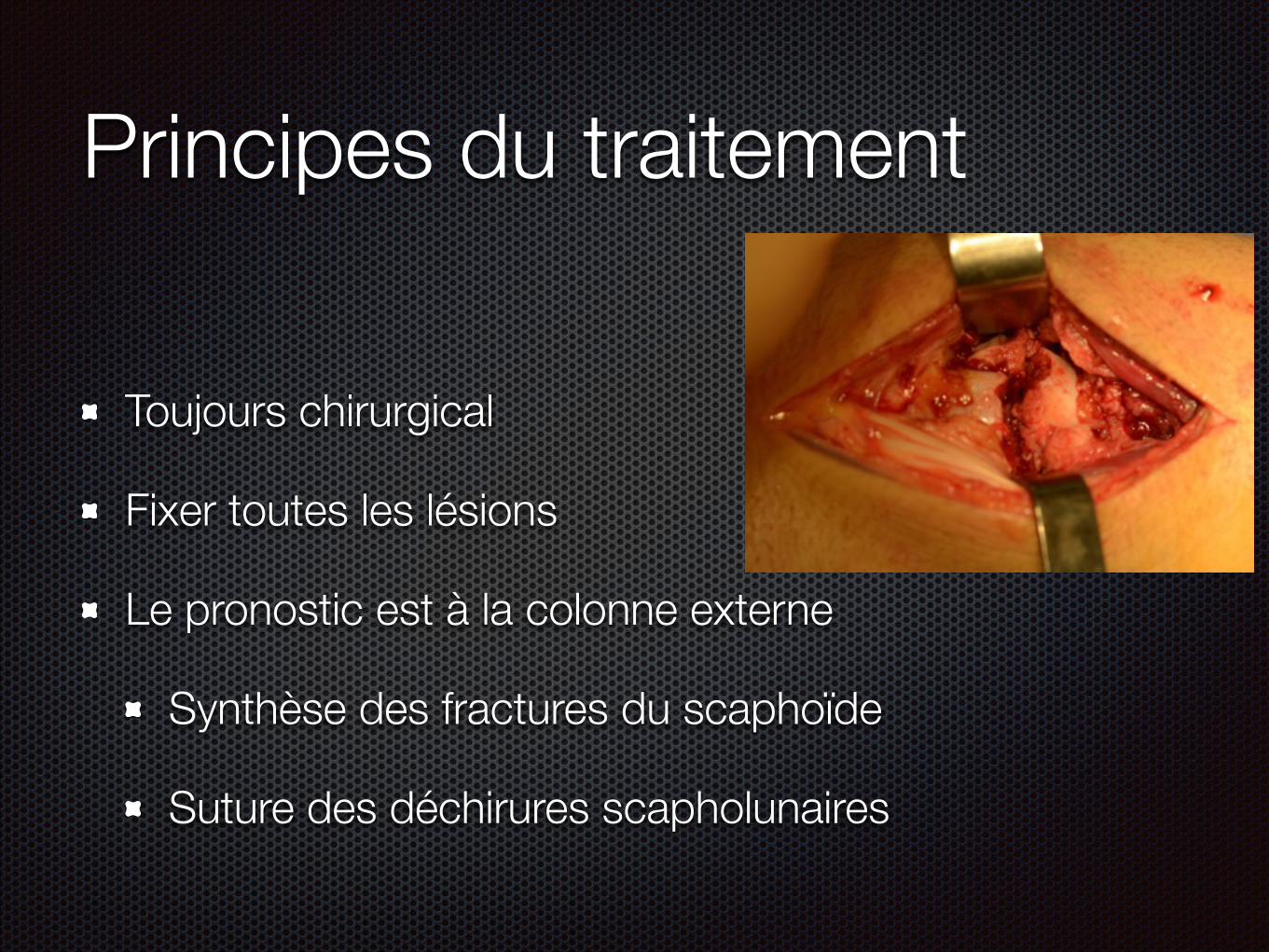
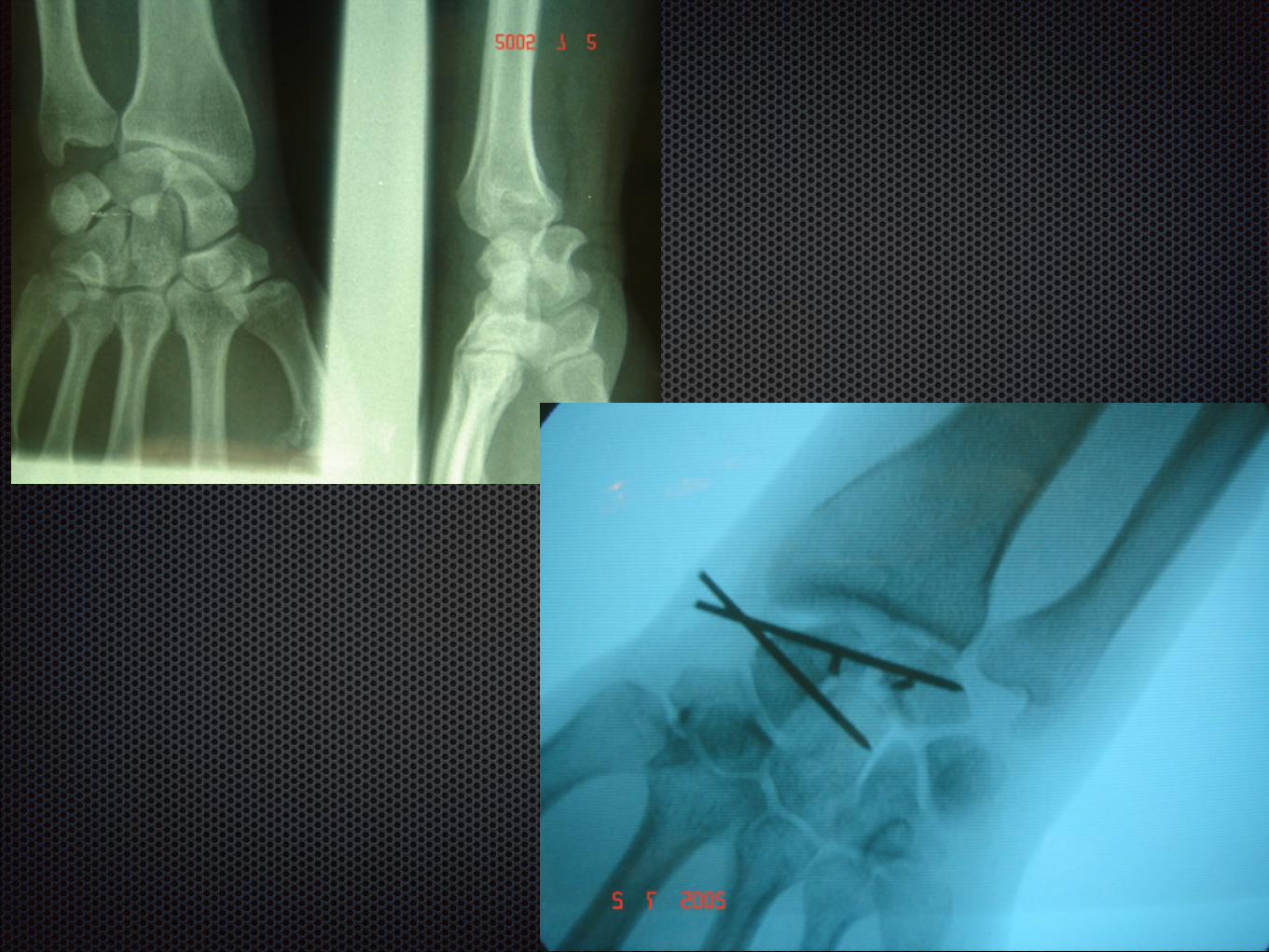
Principes du traitement
Toujours chirurgical
Fixer toutes les lésions
Le pronostic est à la colonne externe
Synthèse des fractures du scaphoïde
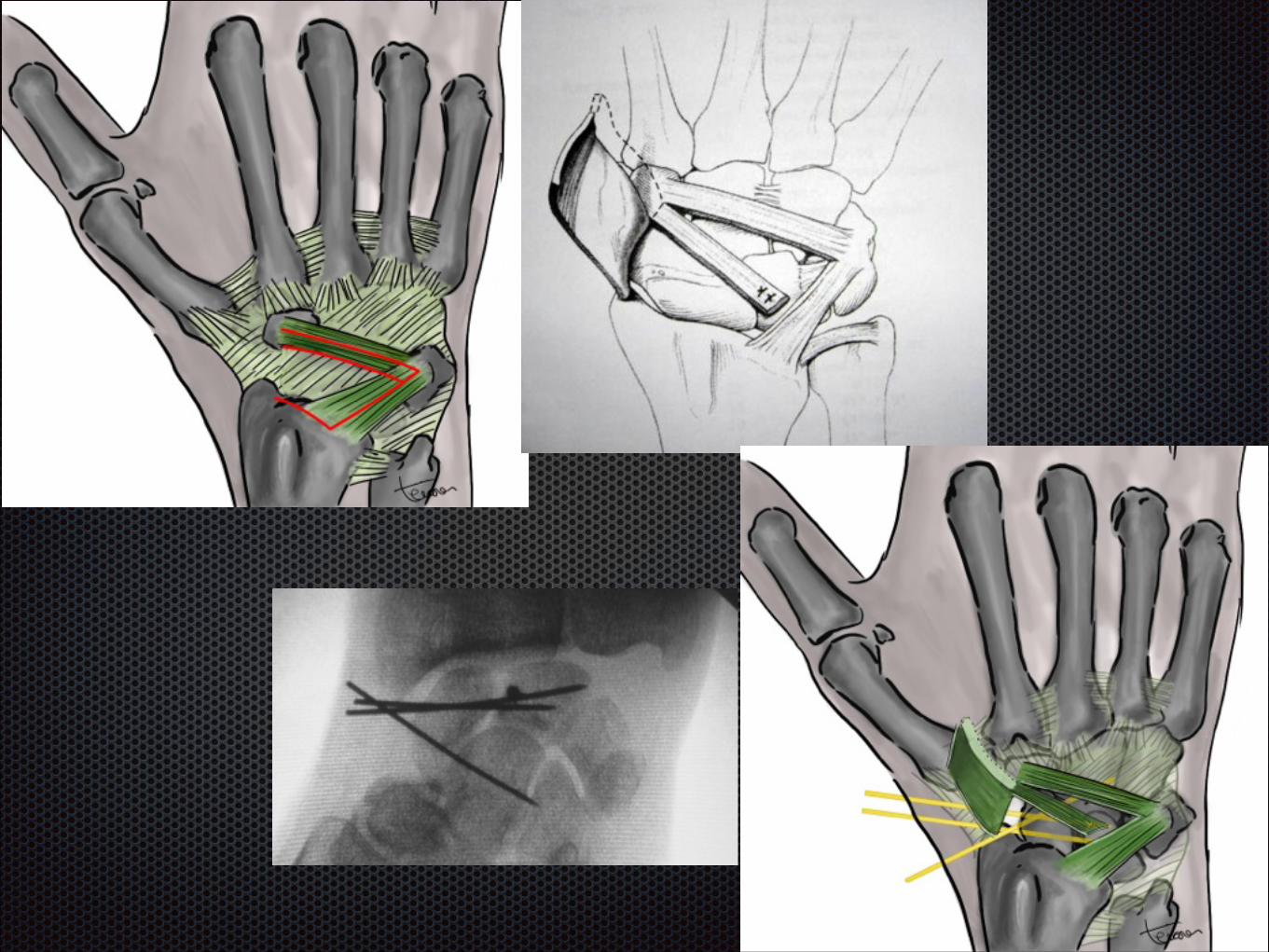
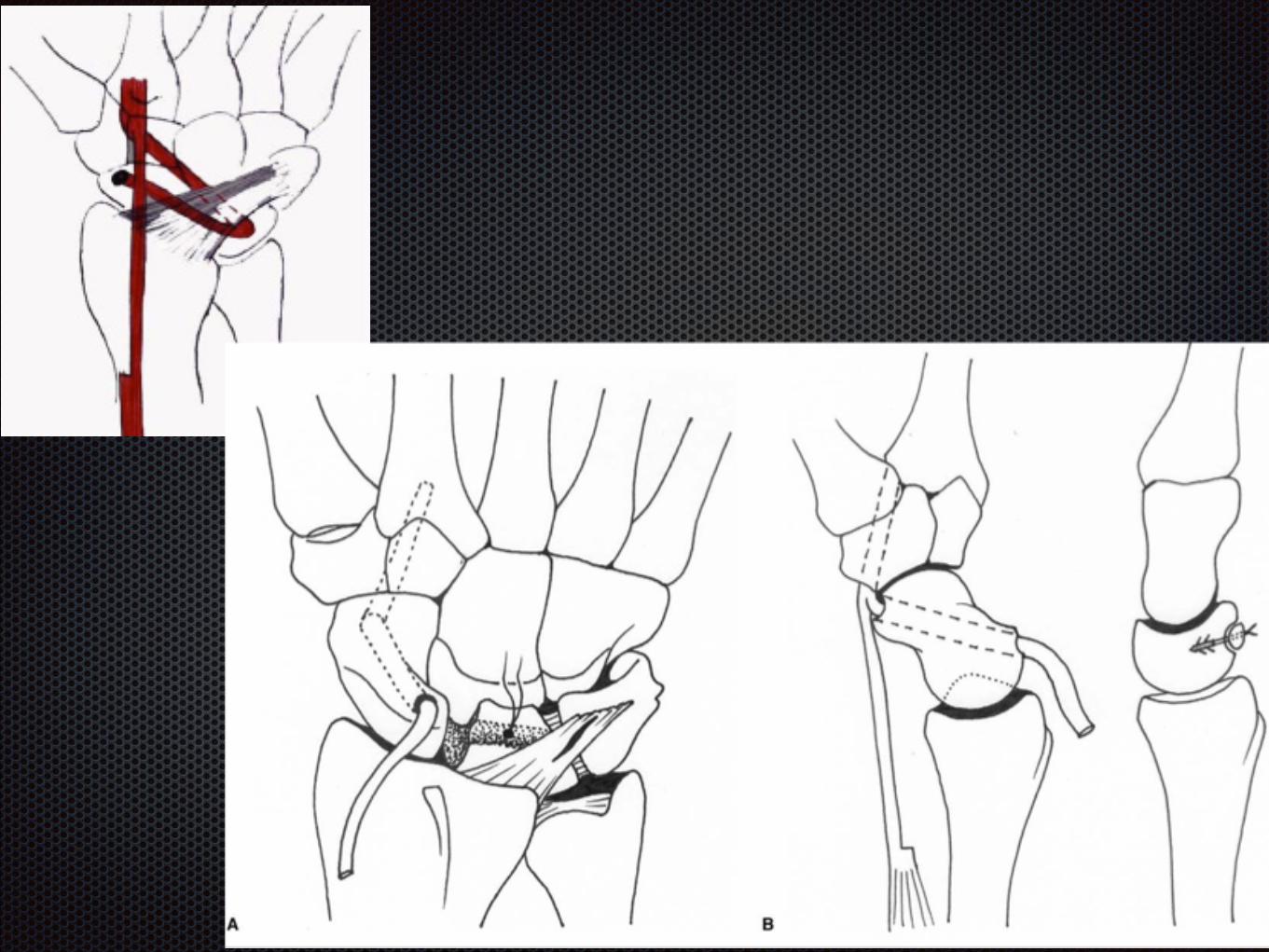
Suture des déchirures scapholunaires

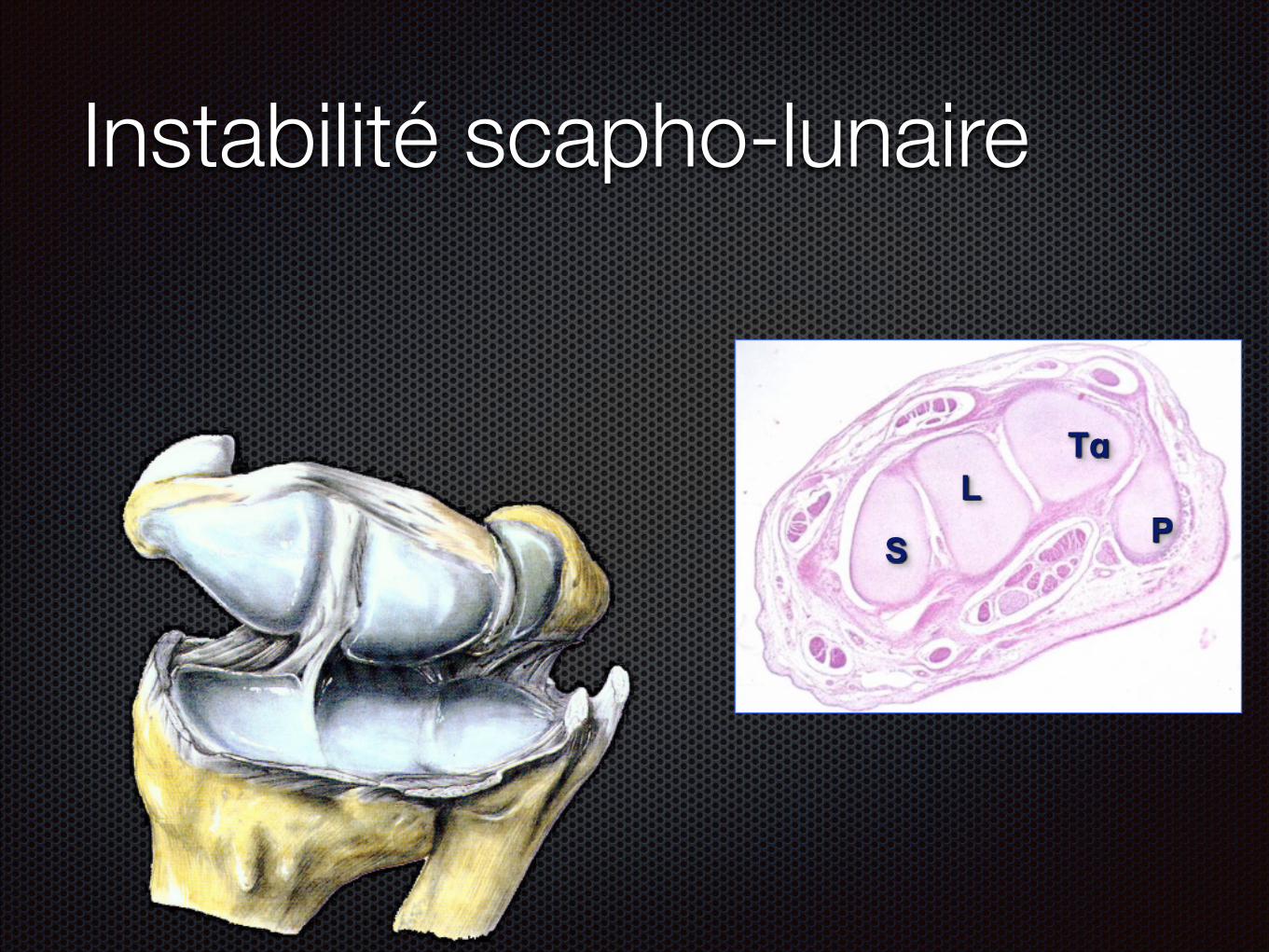
Instabilité scapho-lunaire
S
LTq
P
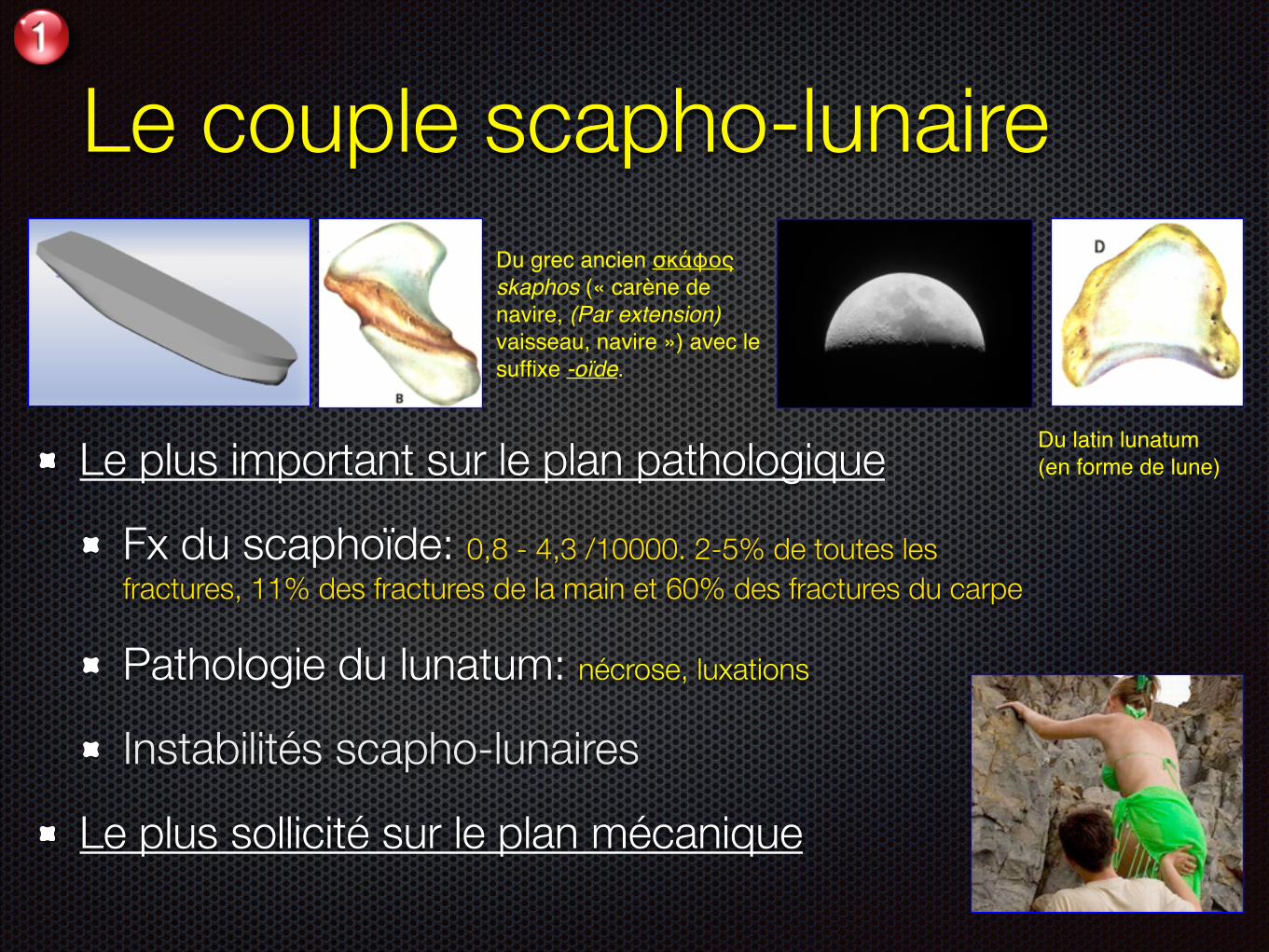
Le couple scapho-lunaire
Le plus important sur le plan pathologique
Fx du scaphoïde: 0,8 - 4,3 /10000. 2-5% de toutes les fractures, 11% des fractures de la main et 60% des fractures du carpe Pathologie du lunatum: nécrose, luxations
Instabilités scapho-lunaires
Le plus sollicité sur le plan mécanique
Du grec ancien σκάφος skaphos (« carène de navire, (Par extension) vaisseau, navire ») avec le suffixe -oïde.
Du latin lunatum (en forme de lune)
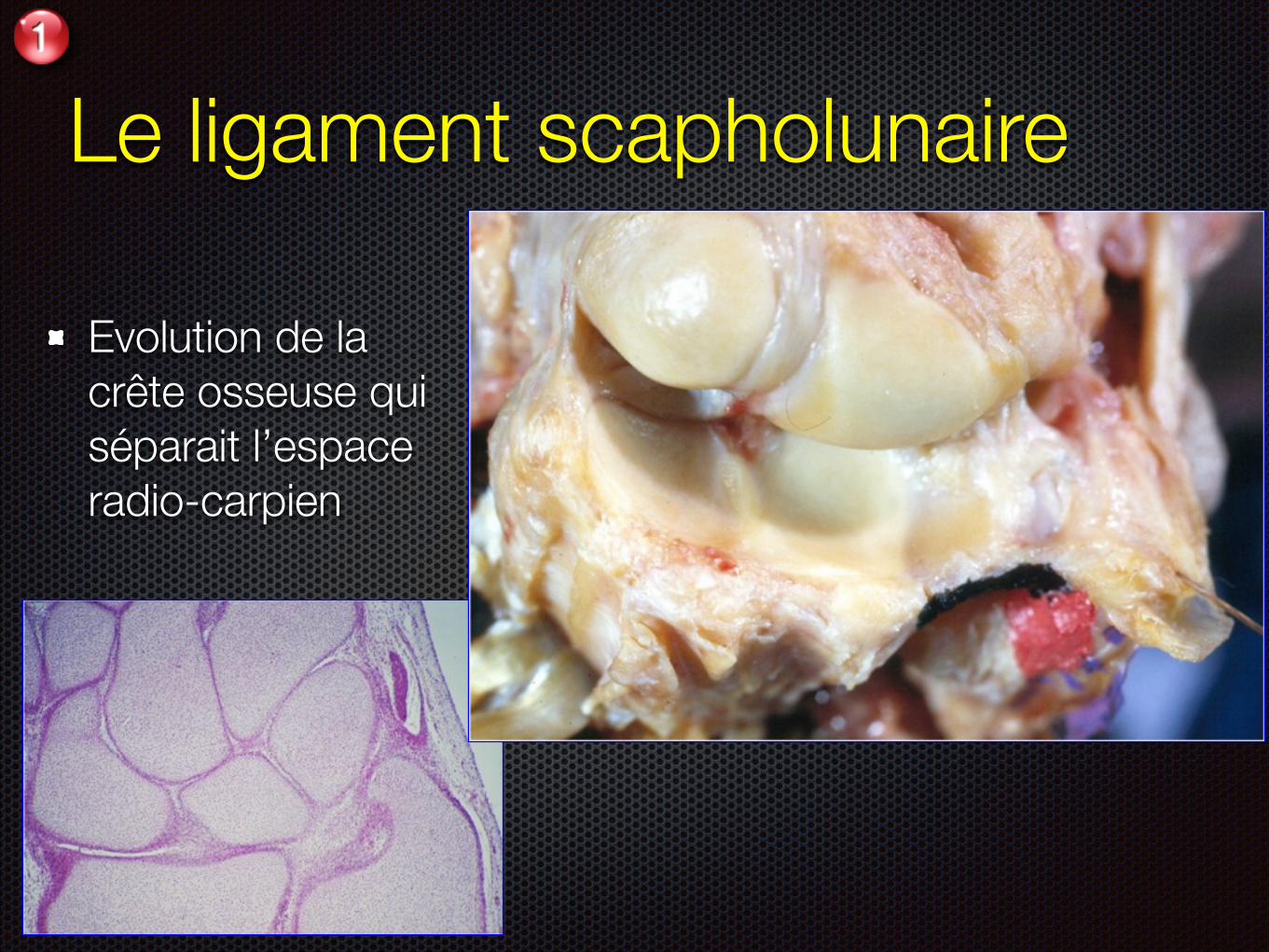
Le ligament scapholunaire
Evolution de la crête osseuse qui séparait l’espace radio-carpien
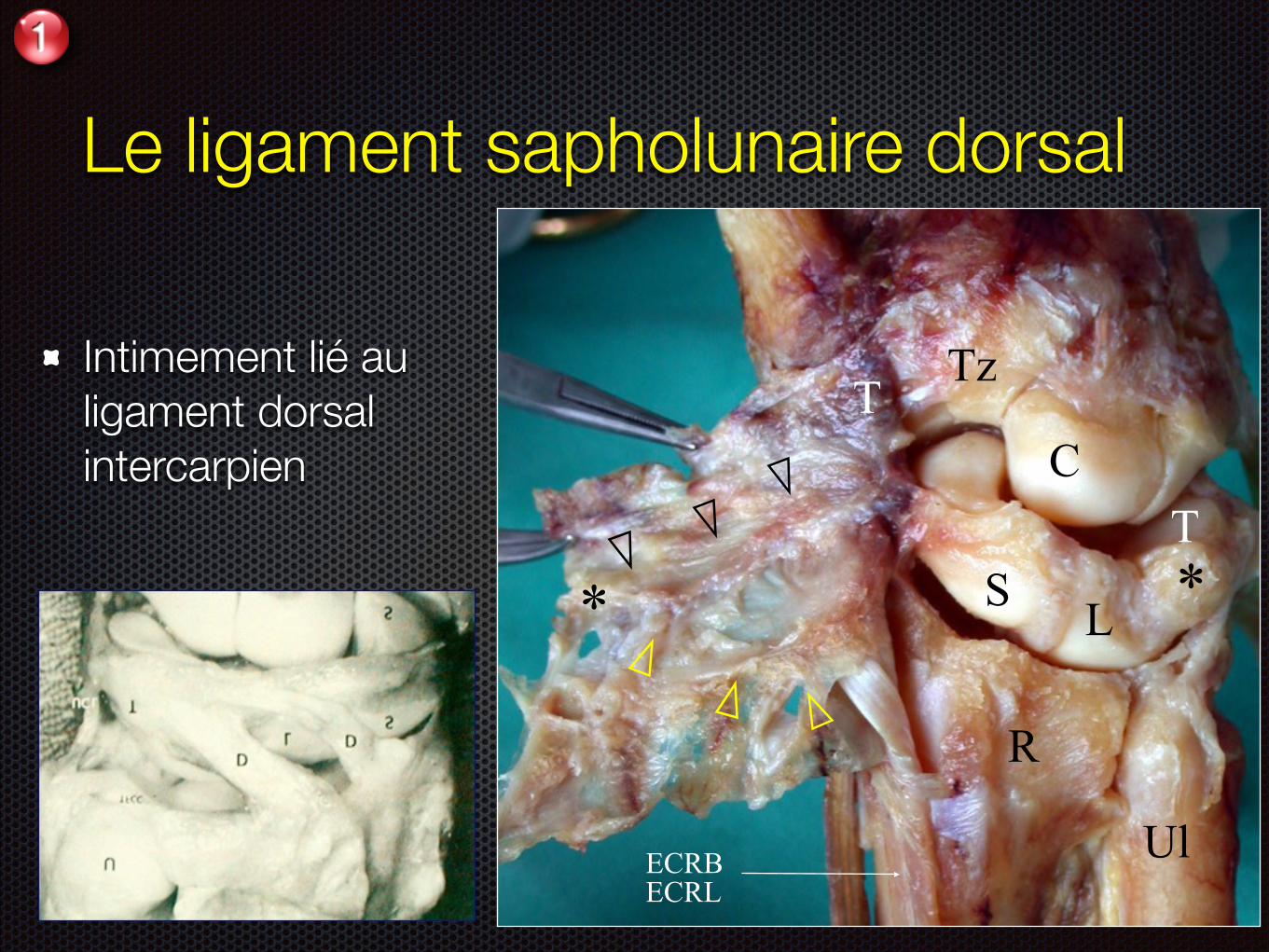
Le ligament sapholunaire dorsal
Intimement lié au ligament dorsal intercarpien
*T
C
TzT
* LS
R
UlECRB ECRL
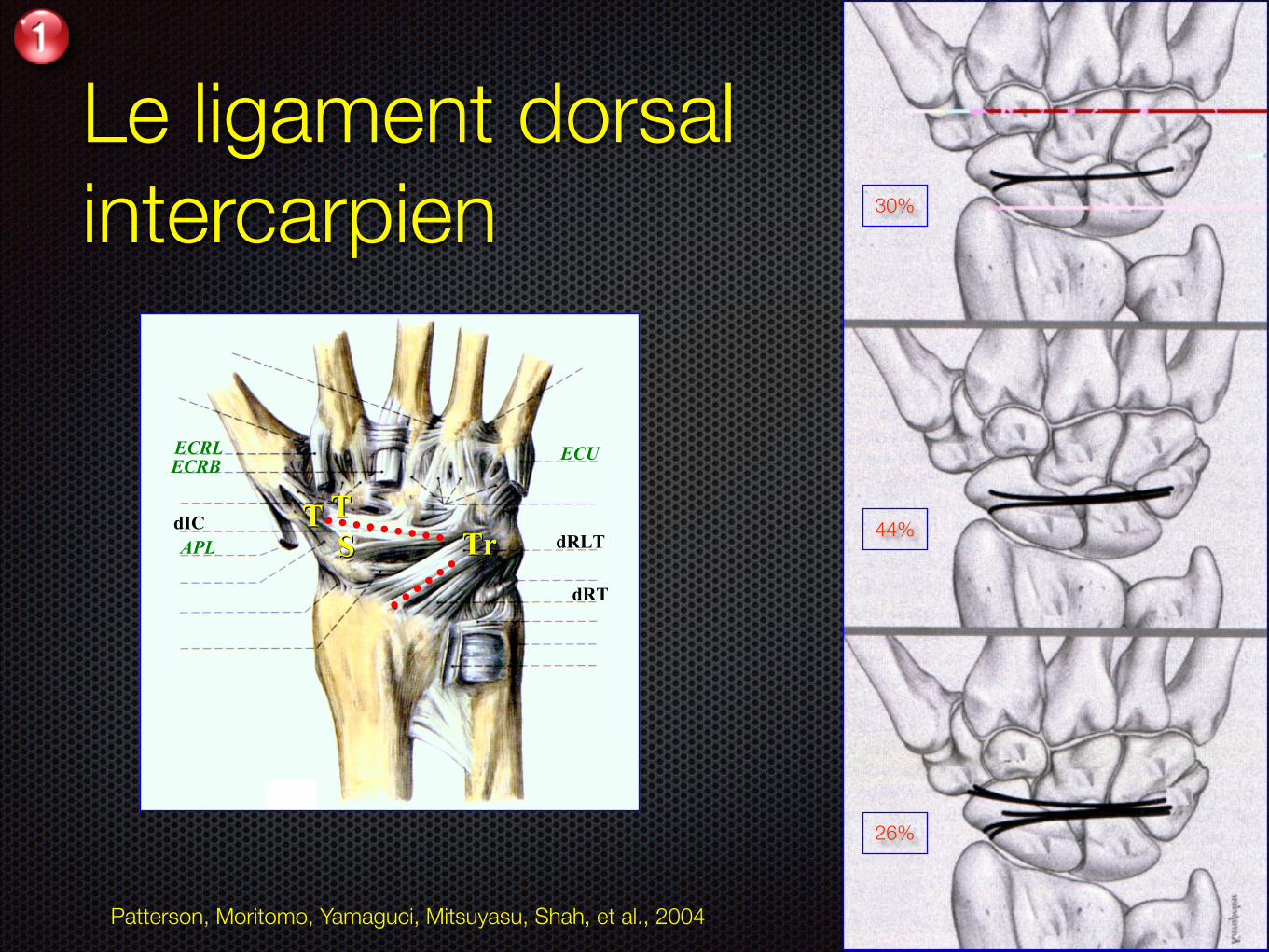
Le ligament dorsal intercarpien 30%
44%
26%
SSTTTT
TrTrdRT
dRLTdIC
ECRLECRB
APL
ECU
Patterson, Moritomo, Yamaguci, Mitsuyasu, Shah, et al., 2004
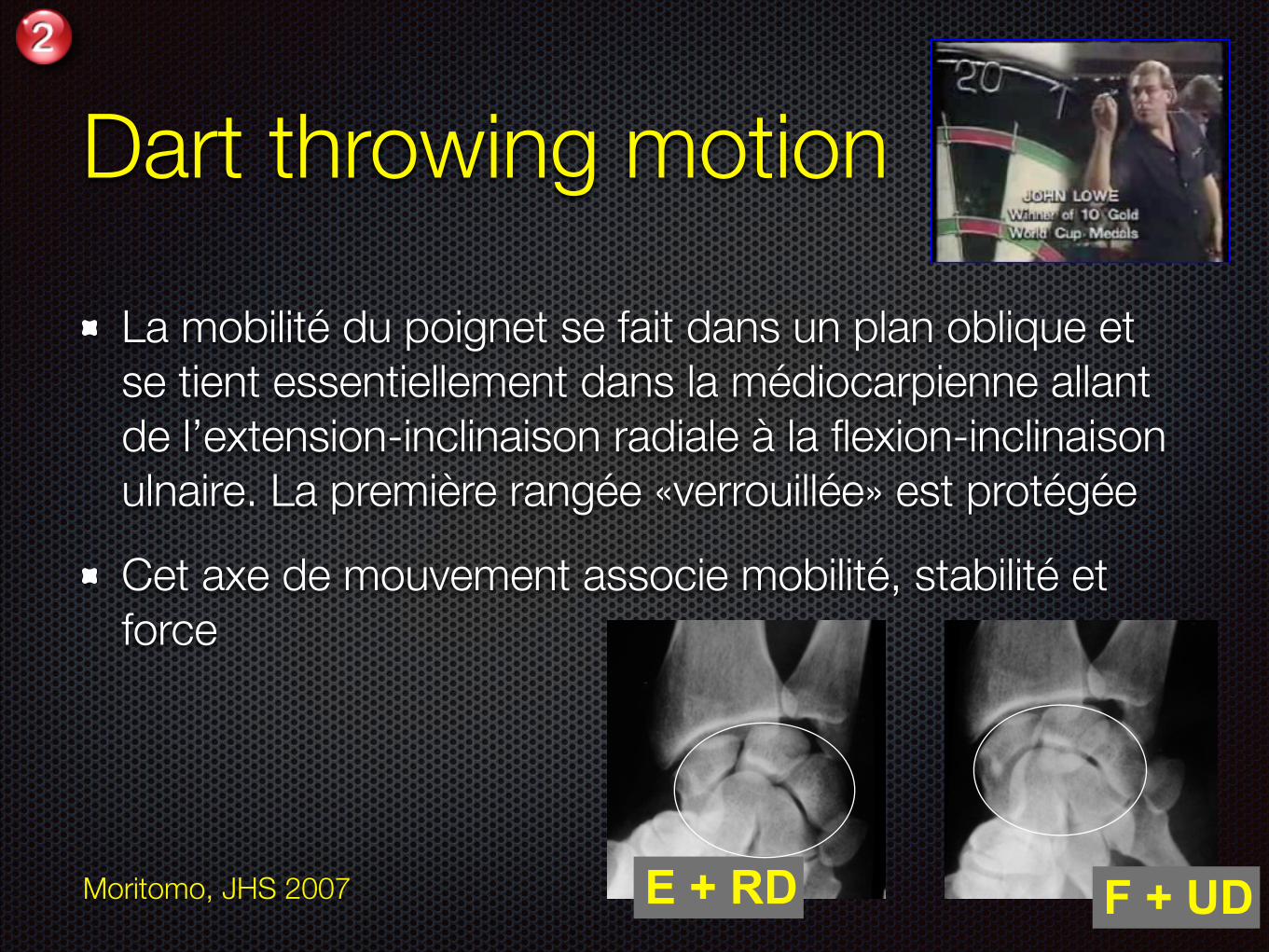
Dart throwing motion
La mobilité du poignet se fait dans un plan oblique et se tient essentiellement dans la médiocarpienne allant de l’extension-inclinaison radiale à la flexion-inclinaison ulnaire. La première rangée «verrouillée» est protégée
Cet axe de mouvement associe mobilité, stabilité et force
Moritomo, JHS 2007 E + RD F + UD
Evolution naturelle ?
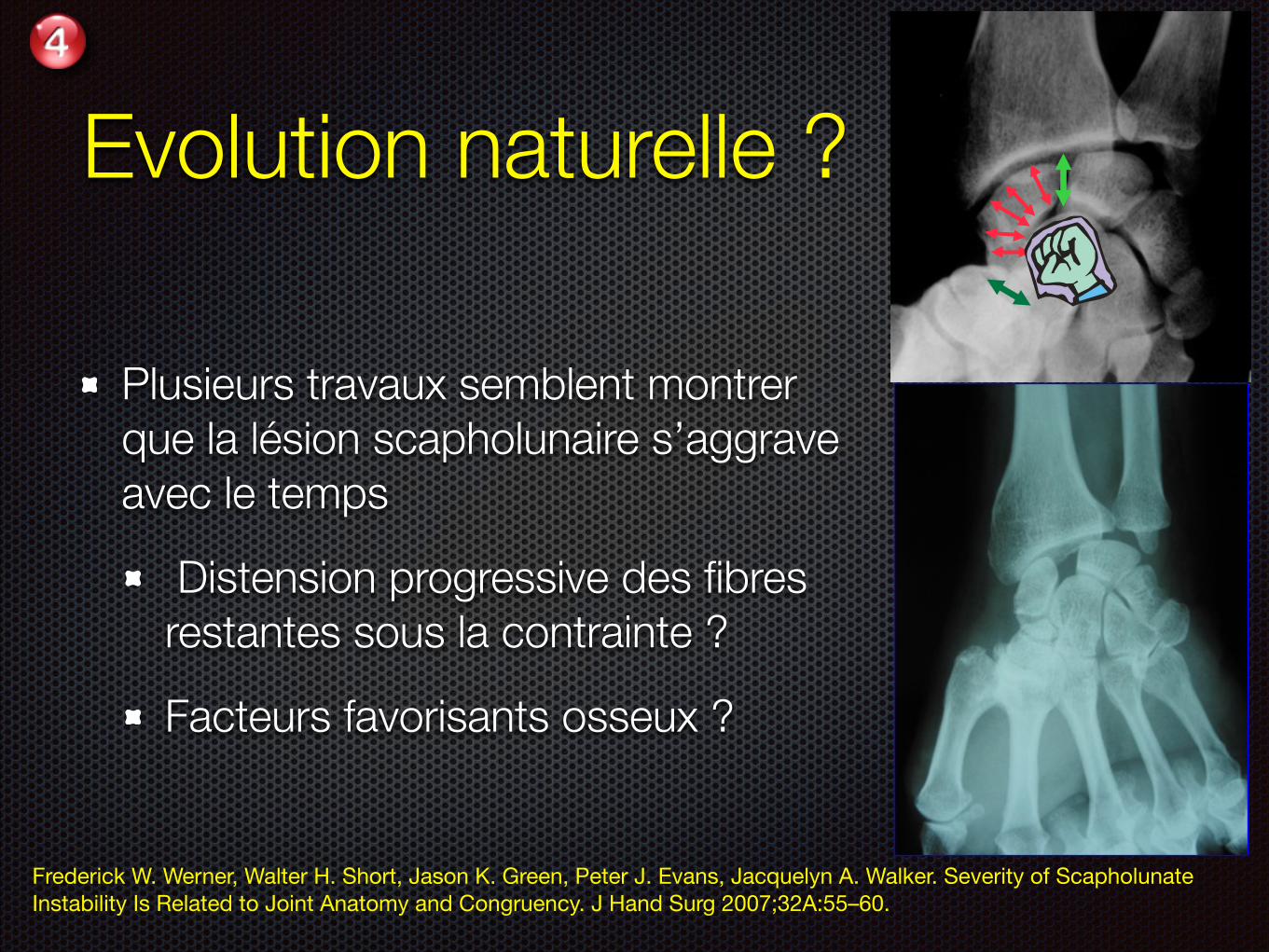
Plusieurs travaux semblent montrer que la lésion scapholunaire s’aggrave avec le temps
Distension progressive des fibres restantes sous la contrainte ?
Facteurs favorisants osseux ?
Frederick W. Werner, Walter H. Short, Jason K. Green, Peter J. Evans, Jacquelyn A. Walker. Severity of Scapholunate Instability Is Related to Joint Anatomy and Congruency. J Hand Surg 2007;32A:55–60.
Evolution naturelle ?
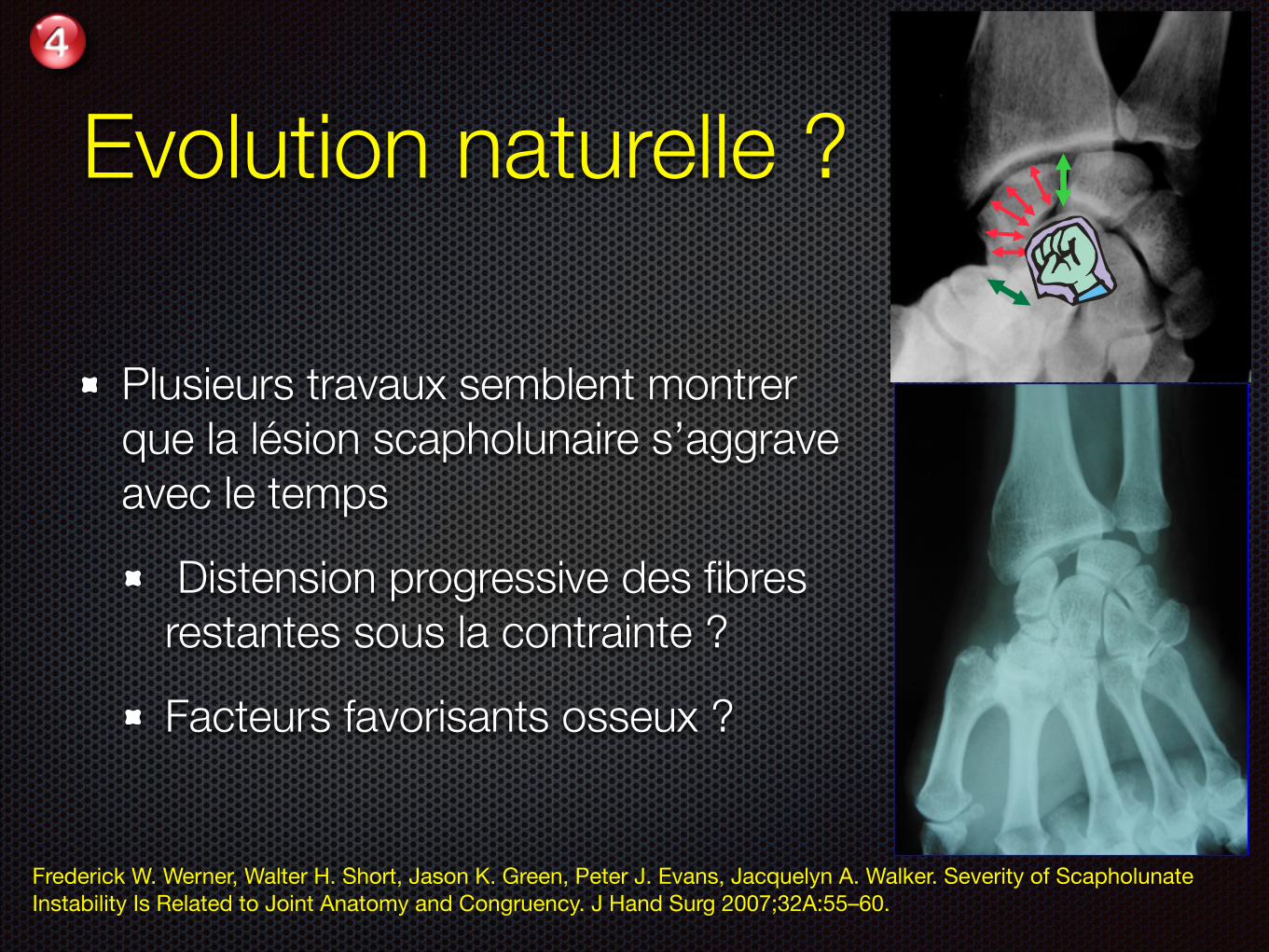
Plusieurs travaux semblent montrer que la lésion scapholunaire s’aggrave avec le temps
Distension progressive des fibres restantes sous la contrainte ?
Facteurs favorisants osseux ?
Frederick W. Werner, Walter H. Short, Jason K. Green, Peter J. Evans, Jacquelyn A. Walker. Severity of Scapholunate Instability Is Related to Joint Anatomy and Congruency. J Hand Surg 2007;32A:55–60.
Evolution naturelle ?
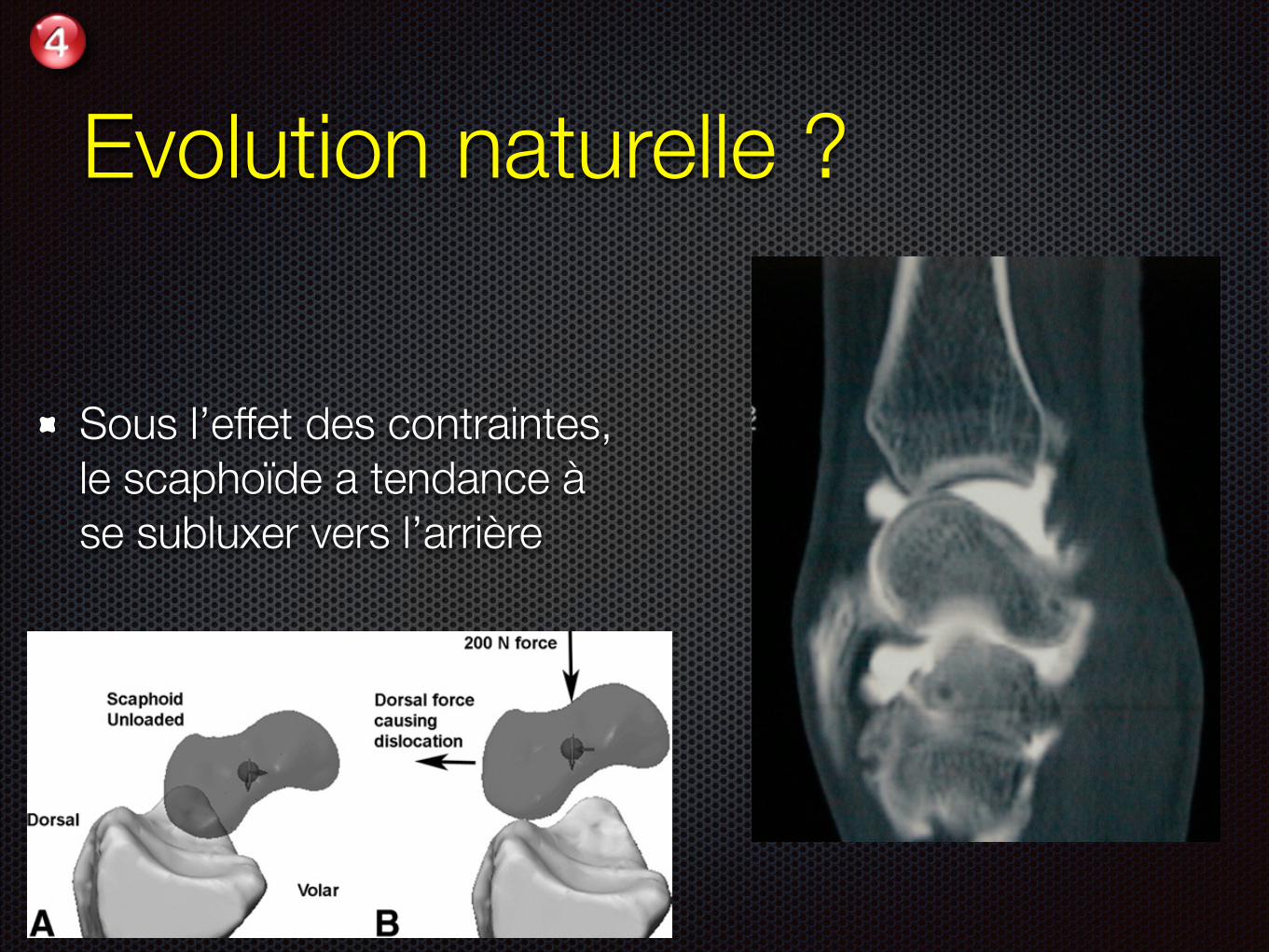
Sous l’effet des contraintes, le scaphoïde a tendance à se subluxer vers l’arrière
ample would be determining the force needed to pulla car tire out of a hole. Because the CT scans of thebones did not include cartilage, the scaphoid waslowered onto the radius until contact was made.Material properties were selected to simulate carti-lage (modulus of elasticity, 0.7 MPa; Poisson’s ratio,0.1; coefficient of friction, 0.01). In this study, onlythe role of the bony architecture in preventing dislo-cation was examined. No soft-tissue constraints wereincluded. First, for each arm, at each wrist position,the dorsally directed force needed to cause a dorsaldislocation of the scaphoid was determined by grad-ually increasing the dorsal force, while a 200 N
compressive and proximally directed force was ap-plied to simulate wrist grip (Fig. 4). Dislocation wasdefined as the position when the scaphoid rose up tothe top of the dorsal rim of the distal radius. Second,the dorsal/volar constraint for each scaphoid wasdetermined by applying a 50 N dorsal force and thena 50 N volar force to the scaphoid, while maintainingthe 200 N axial compressive force (Fig. 5). The sumof the resultant dorsal and volar motions of thescaphoid was measured and defined as the dorsal/volar constraint. In these models, scaphoid motionwas constrained to translations in the sagittal planeand measured for each type of load.
ResultsWith respect to the radiographic measurements(Table 2), after ligamentous sectioning those wristswith a deeper RS fossa and a greater volar tilt have ascaphoid that is less likely to ride up the dorsal rim ofthe distal radius during wrist motion. The amount ofulnar tilt does not seem to be a factor that is relatedto scapholunate instability after ligamentous section-ing.
With respect to the bone geometry measurementsmade from the 3D models of the scaphoid and distalradius (Table 3), after ligamentous sectioning thosewrists with a larger radius of curvature in boththe sagittal and coronal planes for the RS fossa andthe scaphoid seem to be less likely to become unsta-ble than those with smaller curvatures. Visually,these arms were observed to have a smaller SL gapand did not show scaphoid clunk. In all of the fore-arms, the sagittal scaphoid curvature was smaller onthe proximal/volar surface (average, 3.7 mm; SD, 0.7mm), corresponding to when the scaphoid was inflexion as compared with its proximal/dorsal surface(average, 7.6 mm; SD, 2.1 mm), corresponding towhen the scaphoid was in neutral.
The force to cause the scaphoid to dislocate dor-sally out of the RS fossa was computed to be greaterin those wrists that were observed to be minimally
Figure 4. Determination of the dislocation force of thescaphoid. (A) Sagittal view of the radius and scaphoid underno compressive or dorsal loading. (B) Scaphoid has dislo-cated and is sitting on the dorsal rim of the radius. A 200 Ncompressive force was applied to simulate wrist grip.
Figure 5. Determination of the dorsal/volar constraint of thescaphoid. After a 200 N compressive force was applied tosimulate wrist grip, first a 50 N dorsal force and then a 50 Nvolar force was applied. The displacement of the scaphoid asa result of the 50 N dorsal force was summed with thedisplacement of the scaphoid as a result of the 50 N volarforce to compute the dorsal/volar constraint of eachscaphoid.
Table 2. Bone Geometry Measurements FromRadiographs
Level of Instability
Minimal(n ! 3)
Intermediate(n ! 3)
Gross(n ! 2)
Depth of RSfossa, mm (SD) 10.3 (1.2) 9.8 (1.4) 8.6 (0.1)
Volar tilt,° (SD) 17.8 (2.5) 15.3 (1.8) 8.5 (0.7)Ulnar tilt,° (SD) 20.2 (1.4) 19.5 (1.7) 21.5 (3.5)
58 The Journal of Hand Surgery / Vol. 32A No. 1 January 2007
Evolution naturelle ?
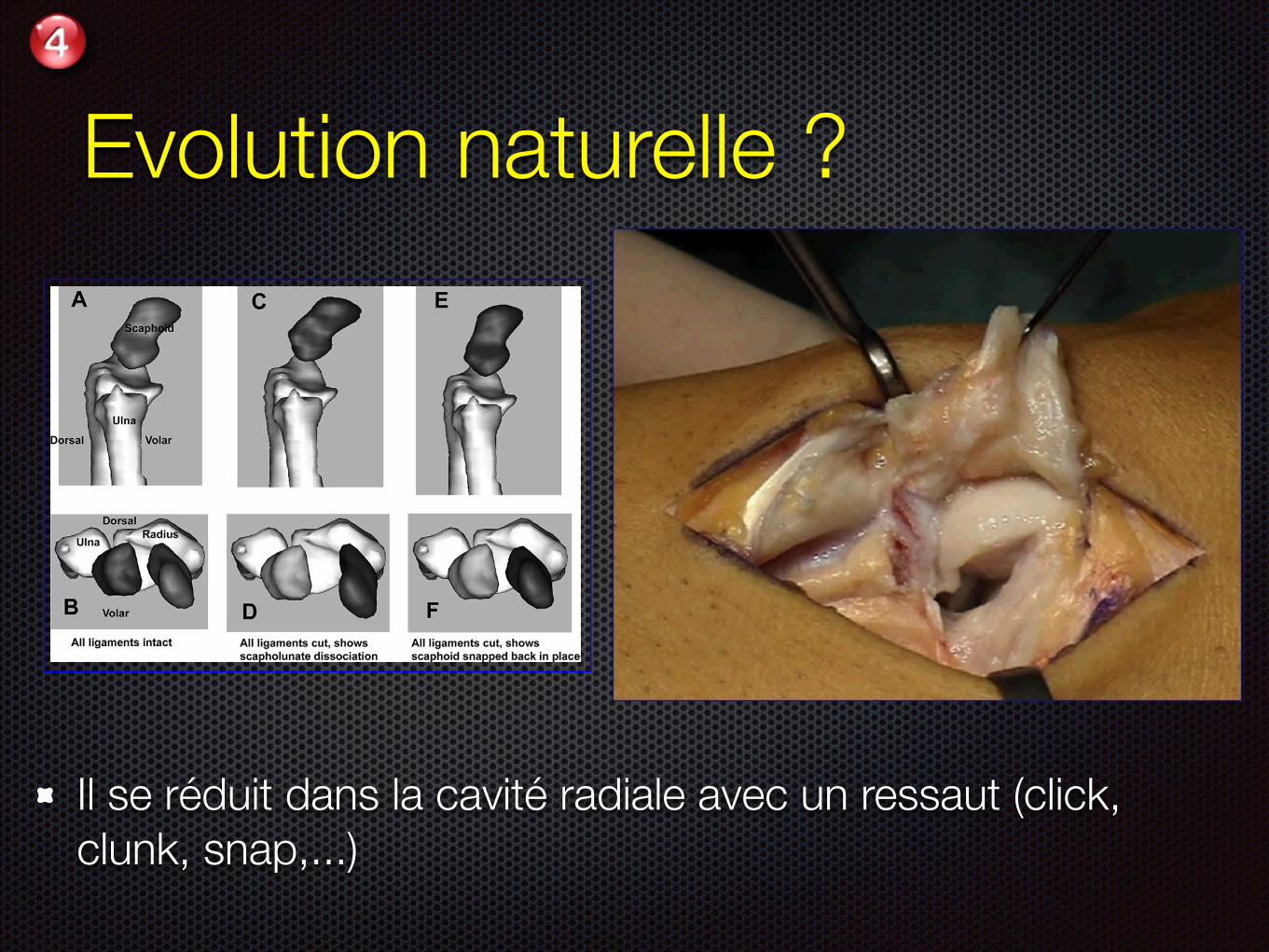
Il se réduit dans la cavité radiale avec un ressaut (click, clunk, snap,...)
while the 3-dimensional (3D) motions of the scaph-oid and lunate were monitored using electromagneticmotion sensors (Fastrak; Polhemus, Colchester,VT).1–4 Carpal kinematic data were acquired withall ligamentous structures intact and after the com-bined sectioning of the SLIL, the radioscaphocapi-tate (RSC) ligament, and the scaphotrapezium (ST)ligament. After ligamentous sectioning, 3 levels ofcarpal instability were defined (Table 1), minimal,intermediate, or gross, based on visual examina-tion of the gap between the scaphoid and lunateand if the scaphoid would clunk back into the RSfossa.
After the 3 ligaments were sectioned, each wristhad a computed tomography (CT) scan. By combin-ing the resultant surface models of the scaphoid andlunate with the corresponding kinematic data, anima-tions of the scaphoid and lunate were made for eachof the 8 arms5 for each of the motions. Dorsal andaxial views of the animations were reviewed to aid inquantifying the SL gap in each arm before and afterligament sectioning. The animations also showedwhether during the motion, after ligamentous sec-tioning, the scaphoid snapped back into the ra-dioscaphoid joint, defined as scaphoid clunk (Fig. 1).The animation models were exported into computer-aided design (CAD) software (Solidworks; Solid-works Corp., Concord, MA) to aid in making bonegeometry measurements. Because of how the CTscans were thresholded, the CAD models do notinclude cartilage.
The bony geometry was quantified by examiningposteroanterior (PA) and lateral radiographs, andfrom the CAD models of the bones. The radiographswere taken with the arm in 90° of elbow flexion, atneutral forearm rotation, and with the wrist in neutralflexion/extension and radioulnar deviation. The beamwas centered over the wrist joint at the junctionbetween the proximal carpal row and the distal ra-
Table 1. Scapholunate Instability: 3 QualitativeLevels
Minimal Little or no SL gap, no scaphoidclunk
Intermediate SL gap present during part of wristmotion, no scaphoid clunk
Gross SL gap present and eitherscaphoid clunk, or scaphoidriding up to and down from thedorsal rim of radius, orscaphoid riding up and stayingon dorsal rim of radius
Figure 1. Scaphoid clunk. (A) Lateral view of the scaphoid at 20° of wrist extension with the wrist moving from neutral toextension, with all ligaments intact. (B) Corresponding transverse plane view of the scaphoid shown in (A). (C) Lateral view ofthe same scaphoid with the wrist at 20° extension, but with the SLIL, RSC, and ST ligaments sectioned. The scaphoid has flexed,moved dorsally, and radially compared to the intact state, and is now on the dorsal rim of the radius. (D) Correspondingtransverse view of the scaphoid shown in (C). As the wrist and scaphoid continue to extend, the scaphoid “snaps” back into theradioscaphoid fossa, approximately 0.04 seconds later in the cadaver wrist motion: (E) lateral view; (F) corresponding transverseview.
56 The Journal of Hand Surgery / Vol. 32A No. 1 January 2007
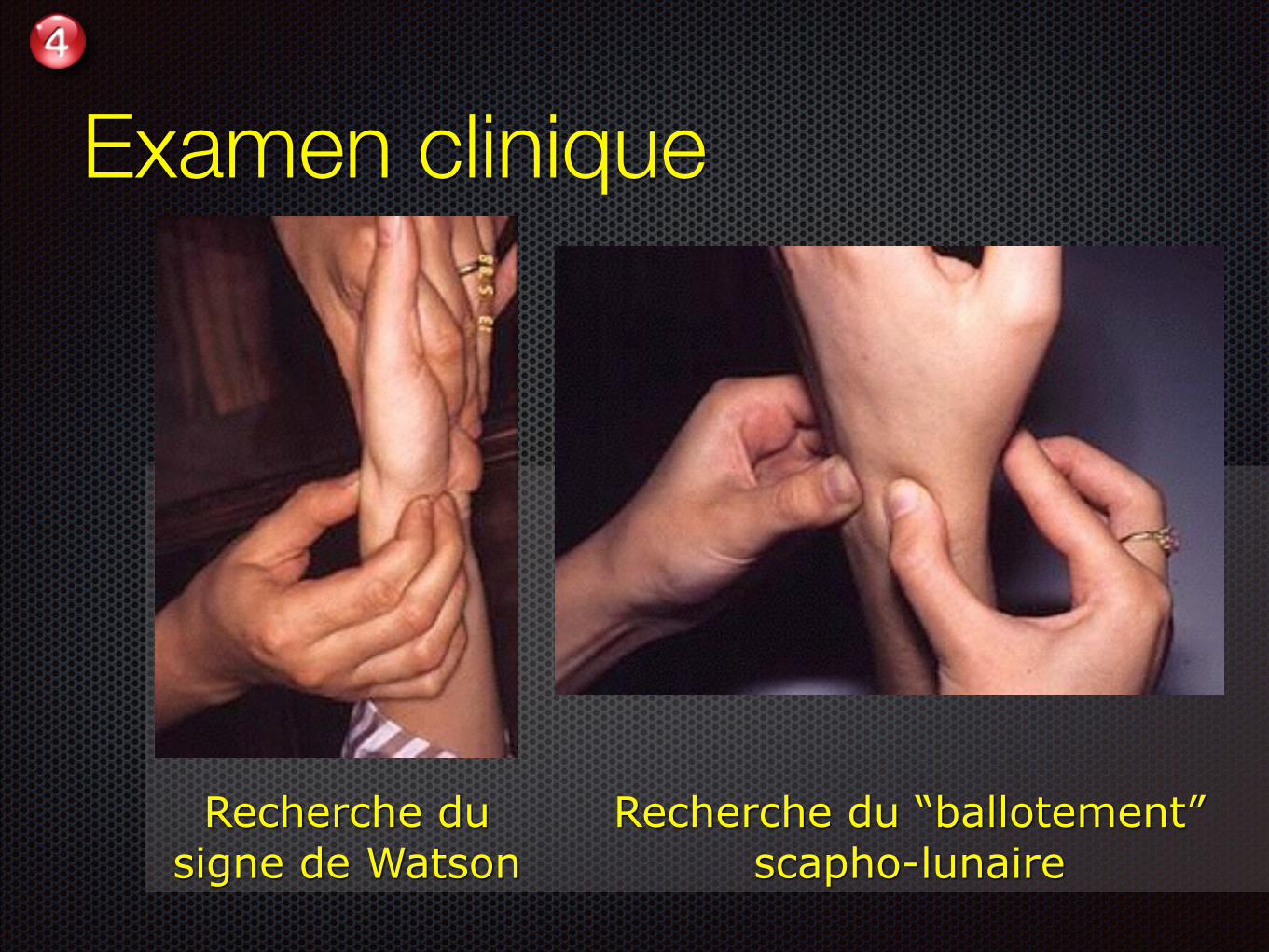
Recherche du signe de Watson
Recherche du “ballotement” scapho-lunaire
Examen clinique
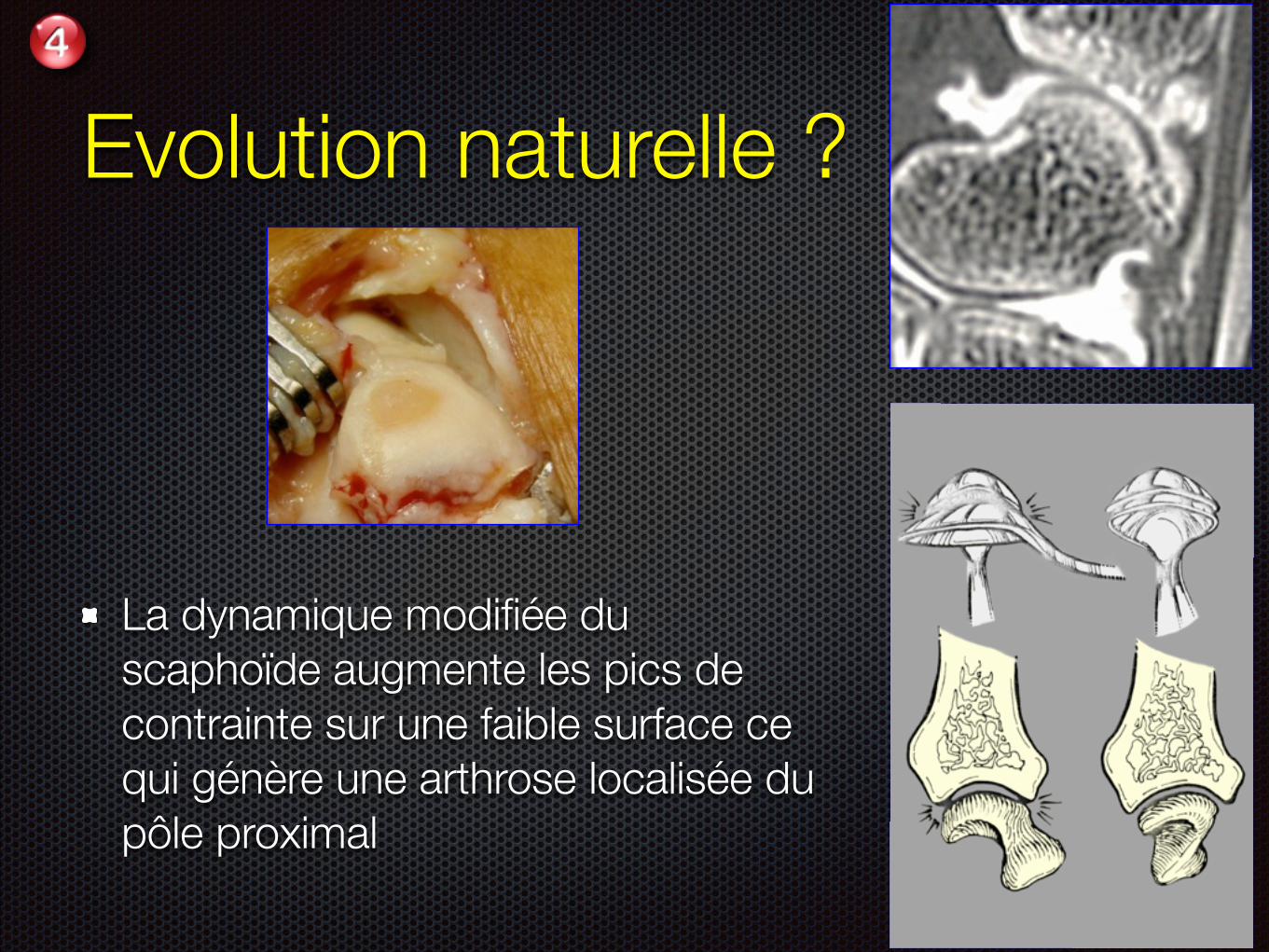
Evolution naturelle ?
La dynamique modifiée du scaphoïde augmente les pics de contrainte sur une faible surface ce qui génère une arthrose localisée du pôle proximal
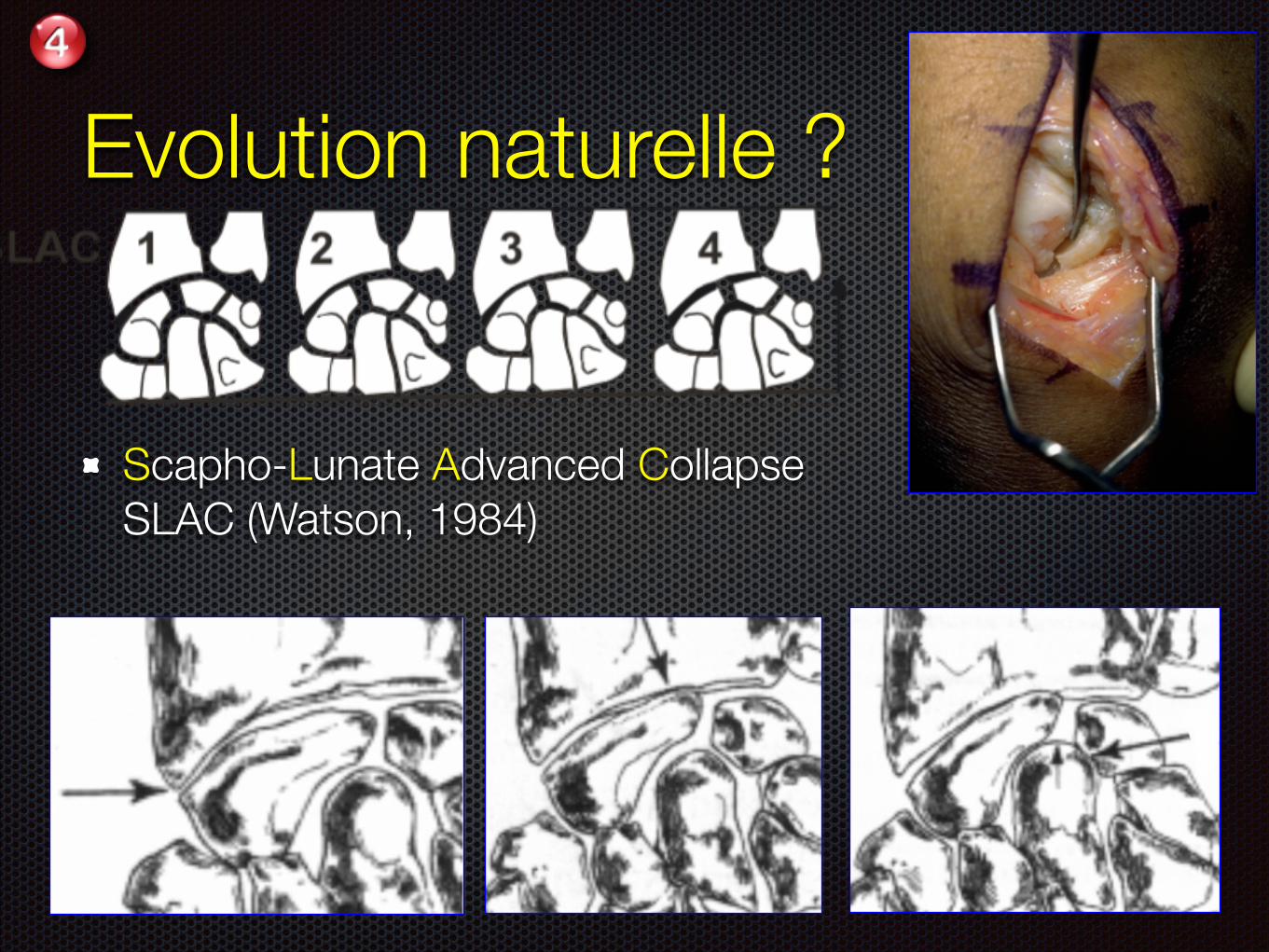
Evolution naturelle ?
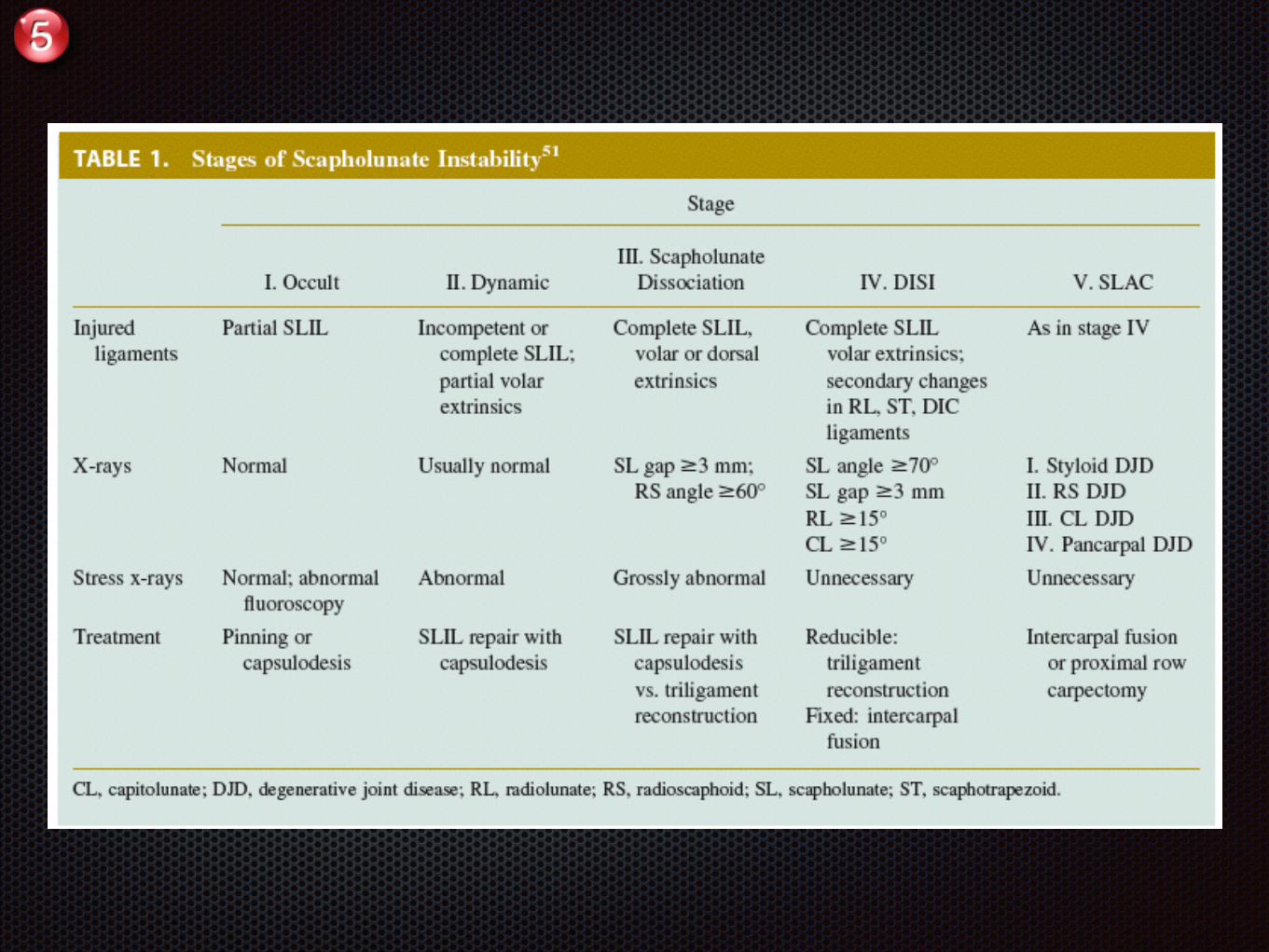
Scapho-Lunate Advanced Collapse SLAC (Watson, 1984)
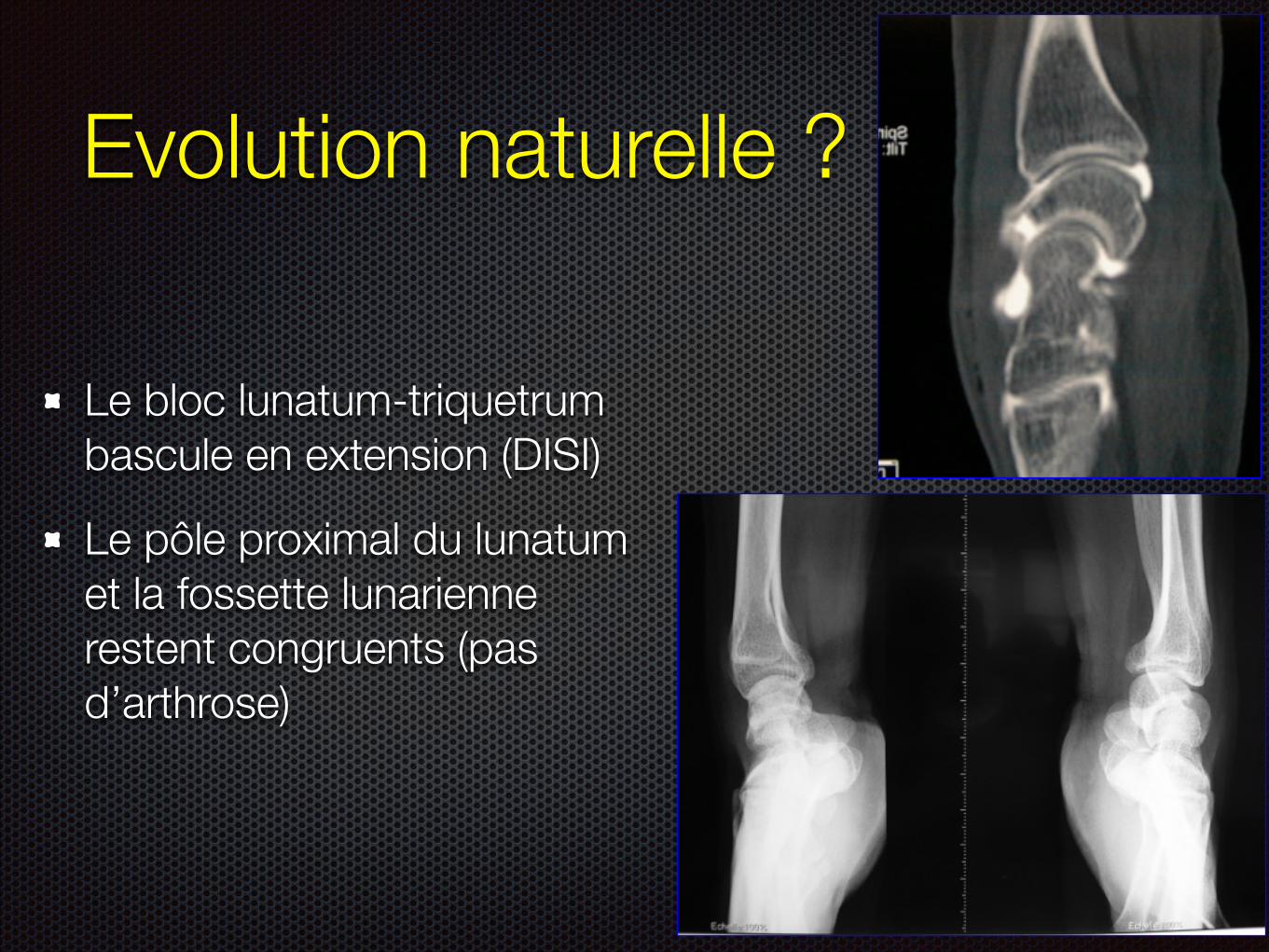
Evolution naturelle ?
Le bloc lunatum-triquetrum bascule en extension (DISI)
Le pôle proximal du lunatum et la fossette lunarienne restent congruents (pas d’arthrose)
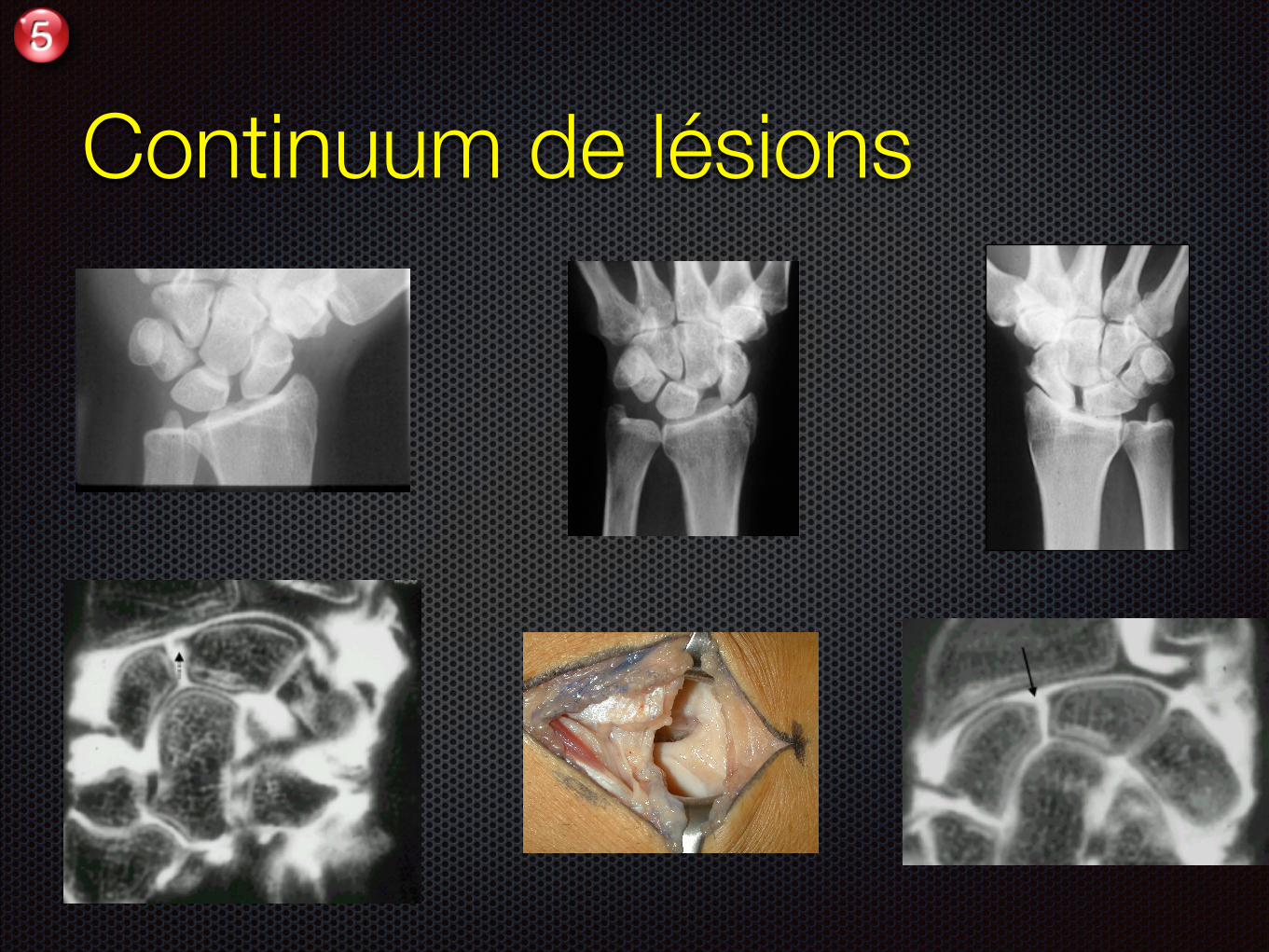
Continuum de lésions
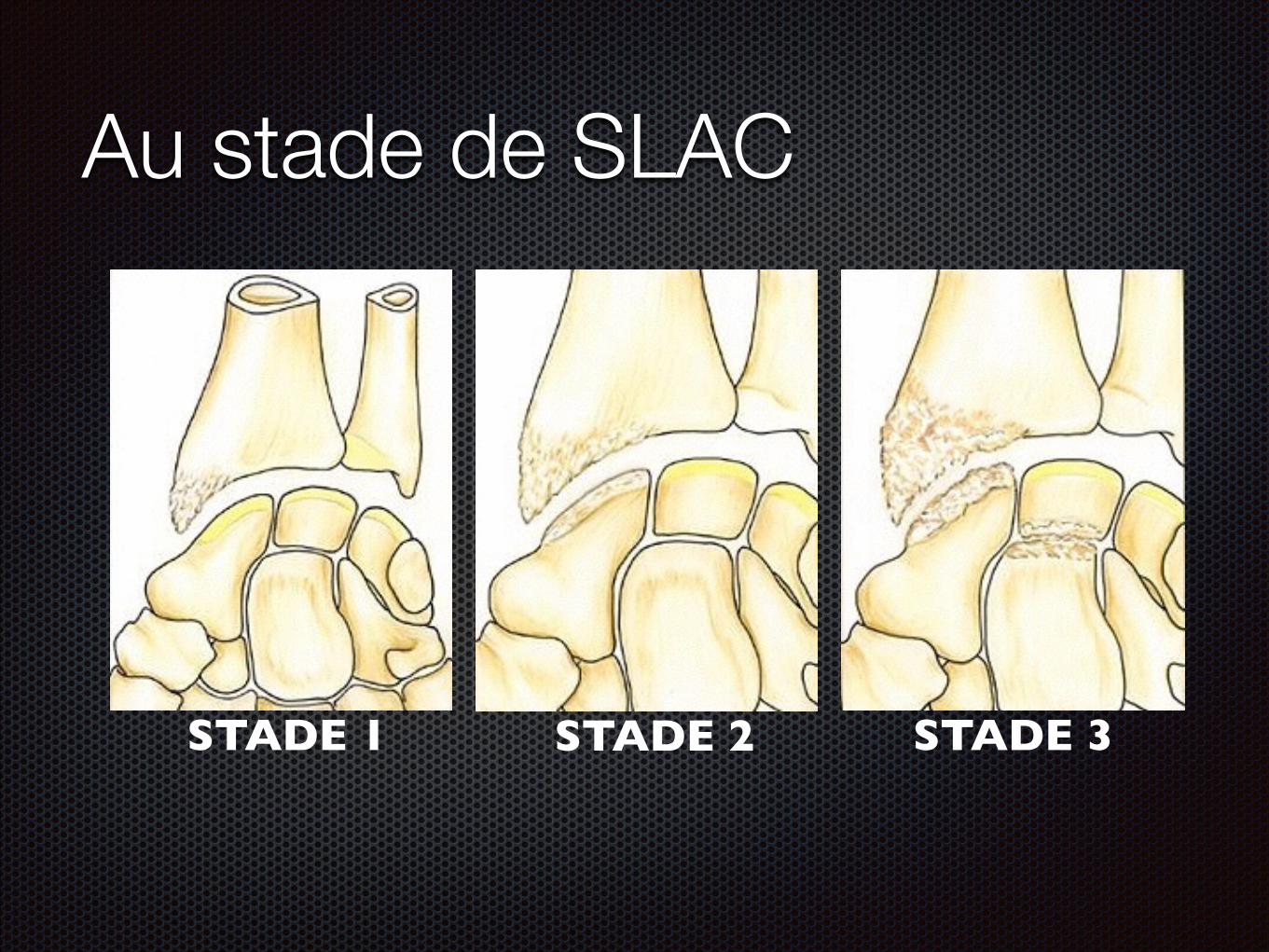
Au stade de SLAC
STADE 1 (
STADE 2 (
STADE 3 (