looped band placed around thighs increases emg of … · looped band placed around thighs increases...
TRANSCRIPT
Looped Band Placed Around ThighsIncreases EMG of Gluteal MusclesWithoutHindering Performance During SquattingKyle F. Spracklin,1 Duane C. Button,1 and Israel Halperin2,3*
Background: There is little information about the effects of placing a resistance band aroundthe outer thighs on the amplitude of performance and electromyography (EMG) of lowerbody muscles during a free barbell back squat (FBBS) activity. This study quantified EMGamplitudes of the gluteus medius, gluteus maximus, vastus lateralis, and biceps femoris dur-ing an FBBS with and without the use of a looped resistance band. In addition, the effects ofthe looped band on the number of repetitions completed on failure in performing FBBS weremeasured at 2 intensities.Methods: In this study, 15 resistance-trained males (age, 23.6 6 3.5 years) completed anFBBS 3 repetition maximum (RM) test on the first testing day to estimate their 1RM. On days2 and 3, participants completed 5 repetitions equal to 80% of their estimated 1RM followed bya repetition to failure test using 60% of estimated 1RM with and without a band placed aroundtheir thighs in a counter-balanced fashion while EMG amplitudes were collected.Results: No differences were found at 60% intensity test between conditions (band: 21.4 66, control: 20.4 6 4.7; P = .171). Similarly, no differences were found between conditions inEMG of the vastus lateralis or biceps femoris at both intensities (effect size [ES] range =0.01–0.4, P ≥ .05). In contrast, other than a few exceptions, gluteus medius and maximusshowed greater EMG activity in the looped-band condition during tests (ES range = 0.28–1.15, P < .05) at both 60% and 80% intensities.Conclusion: Placing a looped resistance band around the thighs can be used as a trainingstrategy to increase the activation of the hip muscles during FBBS using medium to heavyloads without negatively affecting performance.
Keywords: Loop band; squat; resistance training; electromyography
Key Point: Using a looped band around the distal thigh during a barbell squat activityincreases EMG amplitude of the gluteal muscles
*Corresponding Author: ([email protected])1School of Human Kinetics and Recreation, Memorial University of Newfoundland, St. John’s, Newfoundlandand Labrador, Canada.2Discipline of Physiology, Australian Institute of Sport, Canberra, Australian Capital Territory, Australia.3Centre for Exercise and Sport Science Research, School of Medical & Health Sciences, Edith CowanUniversity, Joondalup, Western Australia, Australia.
60
Journal of Performance Health ResearchVolume 1, Issue 1. Pages 60–71DOI: 10.25036/jphr.2017.1.1.sprakin© 2017 Performance Healthwww.performancehealthresearch.com
Orginal Research
OPEN ACCESS
INTRODUCTION
The free barbell back squat (FBBS) is awidely practiced version of the loadedsquat.1,2 It is strongly correlated with varioussport performance measures such as verticaljumps and sprints,3,4 and it is commonly pre-scribed by exercise professionals to enhancesport performance.5,6 Because it is such aneffective exercise, both strength and condi-tioning and rehabilitation professionals arecontinually searching for technical or externalaids to help increase squatting proficiency.One possible training strategy includes theplacement of resistance bands or looped elas-tic tubing modalities around different aspectsof the lower limbs (feet/ankles/distal–lateralthighs).7–10 The looped band can act as pro-prioceptive aid that may influence lower bodyalignment,10,11 electromyography (EMG)amplitudes,7,8 and athletic performance.Hence, given its growing popularity, ease ofuse, low cost, and potential impact on somevariables, investigating its effects is important.
Placing a looped band around the lowerlimbs is hypothesized to act as a propriocep-tive aid, encouraging trainees to abduct thefemur and avoid subsequent medial knee col-lapse.10,11 Recently, it was shown that resist-ance bands placed around the lower body didnot promote “neutral” knee alignment duringsquatting and jumping exercises.7,9 The lackof effects in these studies may stem from thelimited feedback participants received, theirtraining status, or the location and resistancelevel of the bands. Placing an elastic bandaround the lower limbs has been shown toincrease hip muscle EMG amplitudes duringvarious lower body exercises.7,8 Hip adduc-tion and subsequent internal rotation is linkedto patellofemoral pain syndrome12 and non-contact anterior cruciate ligament inju-ries13,14; thus, increasing the contribution ofthe hip external rotators and abductors mayassist in countering these movements.15,16
However, despite the growing body ofresearch, it remains unknown how placing alooped band around the distal thighs will
influence EMG amplitude of lower body mus-cle groups during high-intensity/high-loadexercises. In most studies investigating theeffects of a resistance band placed around thelower body, the outcome measures wereunloaded jumps and low-load/low-intensityexercises.7,8 Furthermore, a looped band mayalso influence performance measures (numberof repetitions). To date, the effects of loopedbands were only investigated in relation toEMG and mechanical alignment.
The purpose of this investigation was2-fold. The first goal was to examine theeffects of placing looped resistance bandsaround the distal–lateral portion of the thigh,on EMG amplitudes of the thigh, and on pos-terior hip muscle groups during high- andmoderate-intensity FBBS among resistance-trained participants. The second goal was toexamine the effect of looped resistance bandson FBBS performance at moderate resistance.
METHODSIn this study 15 male participants (mean
age, 23.7 6 3.5 years; height, 180 6 8.3 cm;weight 86.1 6 10.2 kg) possessing 6.2 6 4.6years of FBBS experience volunteered to par-ticipate in the study. Participants were verballyinformed of all procedures and they signed awritten consent form. The InterdisciplinaryCommittee on Ethics in Human Research ofthe Memorial University of Newfoundlandapproved this study (ICEHR #20141327-HK), and this study was conducted in accord-ance with the Tri-Council Guideline inCanada with full disclosure of potential risksto participants.
Participants were required to visit the labo-ratory on the following 3 occasions: introduc-tory, control, and experimental conditions.All sessions were separated by a minimum of3 days, and a maximum of 7 days. The com-pletion of the experimental and control dayswas counter-balanced and randomized for allparticipants. During the introductory session,participants were given a verbal explanationon what to expect during the study and were
Spracklin et al. J Perform Health Res. 2017. 1(1)
61
given a consent form to read and sign.Participants’ age, height, weight, and years ofexperience doing FBBS were recorded. Anelectronic goniometer was positioned on thelateral axis of the knee to ensure the kneereached a minimum of 90°. Once the 90°squat was determined, variable risers wereplaced to that height as a guide to ensure thatparticipants achieved this depth with eachrepetition. Participants were instructed toonly lightly touch, rather than completely siton, the risers. A metronome set to 50 beats/min was used to control the tempo duringdescent and ascent phases of the squat. Tofind each individuals’ 3 repetition maximum(RM) on the first day, participants wereallowed to warm-up with as much weight andsets as needed to accommodate the trainingstatus of each individual. The 3RM was usedto predict their 1RM, which was then used tocalculate each participant’s 80% and 60% ofpredictive 1RM for subsequent testing days.A tape was placed on the floor, tracing theouter edge of the feet to control for feet posi-tioning and width of stance between sessions(Figure 1). The investigator used verbal com-mands to instruct each participant to descendand ascend in a similar fashion on all testingdays. See Figure 2 for an example of a FBBSperformed during the experiment.
For the control and experimental sessions,participants performed maximum voluntarycontraction (MVC) testing at the beginningof each session to normalize the EMG meas-ures each day. Skin preparation for EMGelectrodes included hair removal, dead epi-thelial cell removal, and cleansing. Indelibleink outlines were traced around the surfaceelectrodes to ensure accurate repeated elec-trode placement between trials. Bipolar sur-face EMG electrodes were used to measureall EMG signals. Two surface EMG record-ing electrodes (disc-shaped, 10 mm in diame-ter; Meditrace Pellet Ag/AgCl electrodes,Graphic Controls Ltd., Buffalo, NY) wereplaced 2 cm apart on the dominant-leg vastuslateralis (VL), biceps femoris (BF), gluteusmedius (GME), and gluteus maximus (GMA)
muscle bellies, with a ground electrode placedon the fibular head. A tape was applied to theelectrodes and leads to ensure optimal surfacecontact for the duration of the testing. AllEMG activity was sampled at 2000 Hz, witha Blackman 61-dB band-pass filter between10 and 500 Hz, amplified (bipolar differential
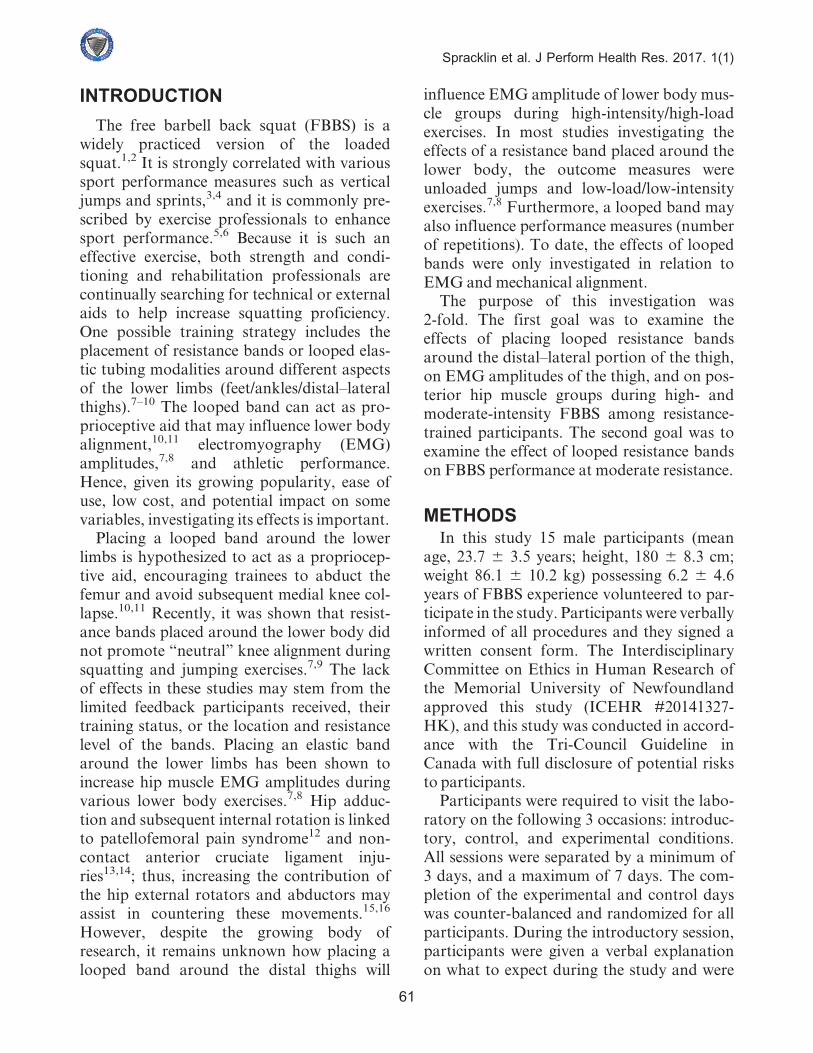
Figure 1. Control for width of stance and fe-mur external rotation. Tape placed at the an-terior and lateral aspects of the foot andmarked for each individual participant.Participants were instructed to adjust theirstance to this angle and width during eachtesting session.
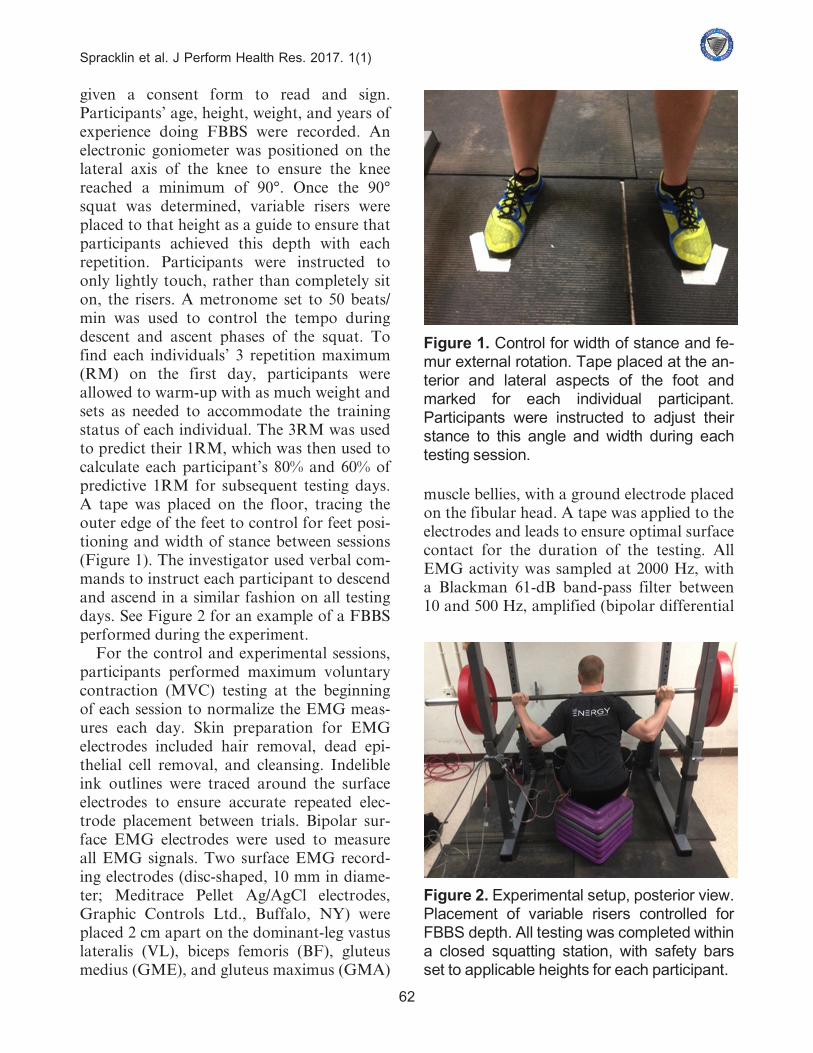
Figure 2. Experimental setup, posterior view.Placement of variable risers controlled forFBBS depth. All testing was completed withina closed squatting station, with safety barsset to applicable heights for each participant.
Spracklin et al. J Perform Health Res. 2017. 1(1)
62
amplifier, input impedance = 2 Mf, commonmode rejection ratio of 110 dB min [50/60 Hz],gain at 1000, and analog-to-digitally con-verted [12 bit]). Raw data were stored on apersonal computer for further analysis (DellInspiron 6000). A commercially availablesoftware program (AcqKnowledge 4.1,Biopac Systems Inc., Holliston, MA) wasused to analyze the digitally converted analogdata.
Participants performed two 3-secondMVCsfor the knee extensors, knee flexors, hip exten-sors and hip abductors to determinemaximumEMG levels for each of the tested musclegroup. For all MVCs, participants wereinstructed to contract the muscles as hard andas fast as possible, and were given strongverbal encouragement. Root mean square(RMS) EMG of all muscles was analyzed overa 1-second duration during theMVCs.
• Knee Extension MVC: Participants wereseated in a specially designed chair(Technical Services, Memorial University,St. John’s, NL, Canada) with the hips andknees secured at 90°. Bilateral shoulderstraps linked with waist and groin strapsensured minimal body translation. Afoam-padded strap was placed around thedominant leg at the ankle. The paddedstrap was secured by a wire connected to ametal brace located on the chair.Participants performed the isometric kneeextension MVC by contracting the limbagainst the strap as hard as possible.
• Knee flexion MVC: From a standing posi-tion, participants stood with their hipsplaced at 0° and the dominant knee flexedto 90°. Participants performed the isomet-ric MVC by pushing their dominant legheel as hard as possible against an immov-able metal bar.
• Hip abduction MVC: Participants werepositioned on a bench, lying on the sidecontralateral to the dominant leg, with thehips and knees placed at 0°. Participantsperformed the isometric MVC by abduct-ing their leg against an unmovable metal
bar. Participants performed the isometrichip abduction as hard as possible.
• Hip extension MVC: From a standingposition, participants stood with their hipsand knees at 0° and performed the isomet-ric MVC by pushing the dominant leg heelagainst a wall. Participants performed theisometric hip extension as hard aspossible.
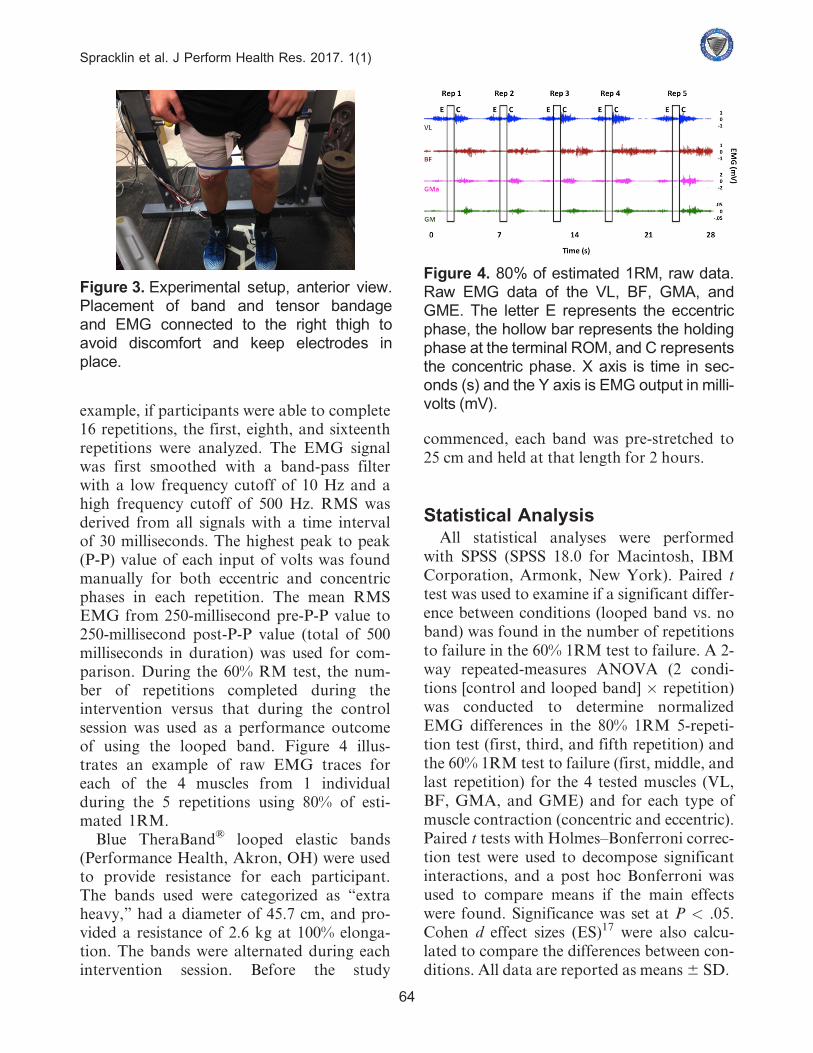
After MVC testing on days 2 and 3, partici-pants then completed a nonspecific, submaxi-mal warm-up on a stationary bike at 70 RPMwith one 1 KP resistance for 5 minutes.Participants then completed an exercise-spe-cific warm-up, consisting of 1 set with a 20-kgbar followed by 2 sets of squats with a self-selected load. The self-selected warm-up com-pleted on the day 1 of the experiment wasrepeated on day 2; thus, the number of sets,the number of repetitions, and the loads usedduring the warm-up were similar between the2 testing sessions. This warm-up strategy waschosen to accommodate the training status ofvarious participants and to increase the exter-nal validity of the study. After completing thelast warm-up set, participants were given 5minutes of rest before completing 5 repeti-tions using 80% of the estimated 1RM, afterwhich they rested for additional 5 minutesand then completed 1 set to failure using 60%of the estimated 1RM (ie, inability to com-plete the next concentric contraction despiteattempting to within the allocated time).Tensor bandages were wrapped around boththighs to ensure that electrodes would stay inplace and ease the discomfort of wearing thelooped band (Figure 3).
EMG amplitudes were measured duringthe squat protocols. Mean RMS of the VL,BF, GME, and GMA was analyzed over awindow of EMG activity, which was thennormalized to the MVCs conducted on thatday. The EMG analysis was conducted forthe first, third and fifth repetition for the 80%1RM 5-repetition test; the first, middle (me-dian), and last repetition were chosen for the60% RM repetition to failure test. For
Spracklin et al. J Perform Health Res. 2017. 1(1)
63
example, if participants were able to complete16 repetitions, the first, eighth, and sixteenthrepetitions were analyzed. The EMG signalwas first smoothed with a band-pass filterwith a low frequency cutoff of 10 Hz and ahigh frequency cutoff of 500 Hz. RMS wasderived from all signals with a time intervalof 30 milliseconds. The highest peak to peak(P-P) value of each input of volts was foundmanually for both eccentric and concentricphases in each repetition. The mean RMSEMG from 250-millisecond pre-P-P value to250-millisecond post-P-P value (total of 500milliseconds in duration) was used for com-parison. During the 60% RM test, the num-ber of repetitions completed during theintervention versus that during the controlsession was used as a performance outcomeof using the looped band. Figure 4 illus-trates an example of raw EMG traces foreach of the 4 muscles from 1 individualduring the 5 repetitions using 80% of esti-mated 1RM.
Blue TheraBand® looped elastic bands(Performance Health, Akron, OH) were usedto provide resistance for each participant.The bands used were categorized as “extraheavy,” had a diameter of 45.7 cm, and pro-vided a resistance of 2.6 kg at 100% elonga-tion. The bands were alternated during eachintervention session. Before the study
commenced, each band was pre-stretched to25 cm and held at that length for 2 hours.
Statistical AnalysisAll statistical analyses were performed
with SPSS (SPSS 18.0 for Macintosh, IBMCorporation, Armonk, New York). Paired ttest was used to examine if a significant differ-ence between conditions (looped band vs. noband) was found in the number of repetitionsto failure in the 60% 1RM test to failure. A 2-way repeated-measures ANOVA (2 condi-tions [control and looped band] � repetition)was conducted to determine normalizedEMG differences in the 80% 1RM 5-repeti-tion test (first, third, and fifth repetition) andthe 60% 1RM test to failure (first, middle, andlast repetition) for the 4 tested muscles (VL,BF, GMA, and GME) and for each type ofmuscle contraction (concentric and eccentric).Paired t tests with Holmes–Bonferroni correc-tion test were used to decompose significantinteractions, and a post hoc Bonferroni wasused to compare means if the main effectswere found. Significance was set at P < .05.Cohen d effect sizes (ES)17 were also calcu-lated to compare the differences between con-ditions. All data are reported as means6 SD.
Figure 3. Experimental setup, anterior view.Placement of band and tensor bandageand EMG connected to the right thigh toavoid discomfort and keep electrodes inplace.
Figure 4. 80% of estimated 1RM, raw data.Raw EMG data of the VL, BF, GMA, andGME. The letter E represents the eccentricphase, the hollow bar represents the holdingphase at the terminal ROM, and C representsthe concentric phase. X axis is time in sec-onds (s) and the Y axis is EMG output in milli-volts (mV).
Spracklin et al. J Perform Health Res. 2017. 1(1)
64
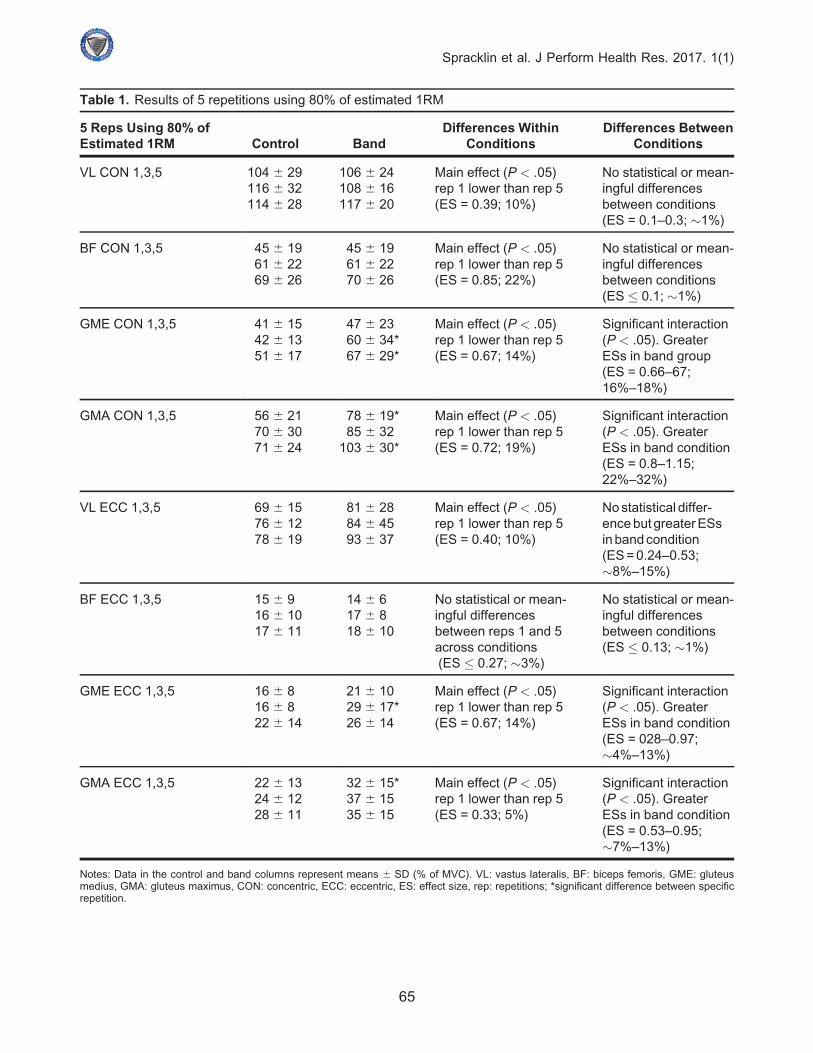
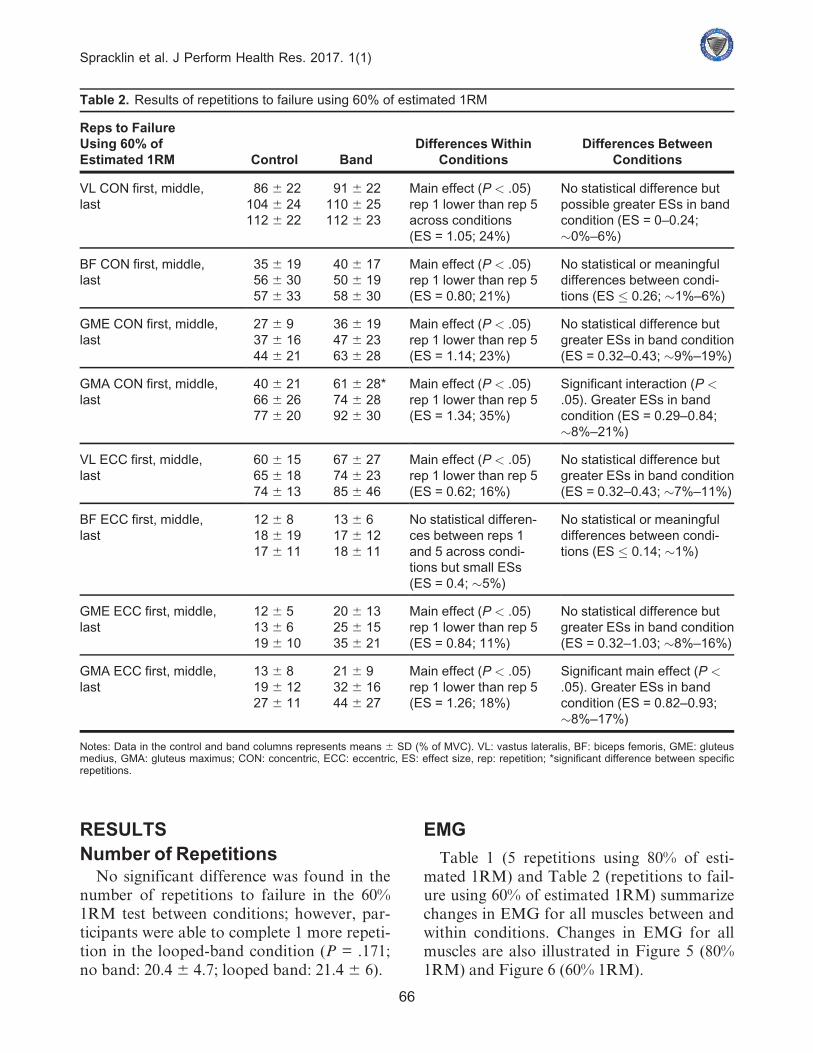
Table 1. Results of 5 repetitions using 80% of estimated 1RM
5 Reps Using 80% ofEstimated 1RM Control Band
Differences WithinConditions
Differences BetweenConditions
VL CON 1,3,5 104 6 29116 6 32114 6 28
106 6 24108 6 16117 6 20
Main effect (P < .05)rep 1 lower than rep 5(ES = 0.39; 10%)
No statistical or mean-ingful differencesbetween conditions(ES = 0.1–0.3; �1%)
BF CON 1,3,5 45 6 1961 6 2269 6 26
45 6 1961 6 2270 6 26
Main effect (P < .05)rep 1 lower than rep 5(ES = 0.85; 22%)
No statistical or mean-ingful differencesbetween conditions(ES � 0.1; �1%)
GME CON 1,3,5 41 6 1542 6 1351 6 17
47 6 2360 6 34*67 6 29*
Main effect (P < .05)rep 1 lower than rep 5(ES = 0.67; 14%)
Significant interaction(P < .05). GreaterESs in band group(ES = 0.66–67;16%–18%)
GMA CON 1,3,5 56 6 2170 6 3071 6 24
78 6 19*85 6 32
103 6 30*
Main effect (P < .05)rep 1 lower than rep 5(ES = 0.72; 19%)
Significant interaction(P < .05). GreaterESs in band condition(ES = 0.8–1.15;22%–32%)
VL ECC 1,3,5 69 6 1576 6 1278 6 19
81 6 2884 6 4593 6 37
Main effect (P < .05)rep 1 lower than rep 5(ES = 0.40; 10%)
Nostatistical differ-encebut greaterESsinbandcondition(ES=0.24–0.53;�8%–15%)
BF ECC 1,3,5 15 6 916 6 1017 6 11
14 6 617 6 818 6 10
No statistical or mean-ingful differencesbetween reps 1 and 5across conditions(ES � 0.27; �3%)
No statistical or mean-ingful differencesbetween conditions(ES � 0.13; �1%)
GME ECC 1,3,5 16 6 816 6 822 6 14
21 6 1029 6 17*26 6 14
Main effect (P < .05)rep 1 lower than rep 5(ES = 0.67; 14%)
Significant interaction(P < .05). GreaterESs in band condition(ES = 028–0.97;�4%–13%)
GMA ECC 1,3,5 22 6 1324 6 1228 6 11
32 6 15*37 6 1535 6 15
Main effect (P < .05)rep 1 lower than rep 5(ES = 0.33; 5%)
Significant interaction(P < .05). GreaterESs in band condition(ES = 0.53–0.95;�7%–13%)
Notes: Data in the control and band columns represent means 6 SD (% of MVC). VL: vastus lateralis, BF: biceps femoris, GME: gluteusmedius, GMA: gluteus maximus, CON: concentric, ECC: eccentric, ES: effect size, rep: repetitions; *significant difference between specificrepetition.
Spracklin et al. J Perform Health Res. 2017. 1(1)
65
RESULTSNumber of Repetitions
No significant difference was found in thenumber of repetitions to failure in the 60%1RM test between conditions; however, par-ticipants were able to complete 1 more repeti-tion in the looped-band condition (P = .171;no band: 20.46 4.7; looped band: 21.4 6 6).
EMG
Table 1 (5 repetitions using 80% of esti-mated 1RM) and Table 2 (repetitions to fail-ure using 60% of estimated 1RM) summarizechanges in EMG for all muscles between andwithin conditions. Changes in EMG for allmuscles are also illustrated in Figure 5 (80%1RM) and Figure 6 (60% 1RM).
Table 2. Results of repetitions to failure using 60% of estimated 1RM
Reps to FailureUsing 60% ofEstimated 1RM Control Band
Differences WithinConditions
Differences BetweenConditions
VL CON first, middle,last
86 6 22104 6 24112 6 22
91 6 22110 6 25112 6 23
Main effect (P < .05)rep 1 lower than rep 5across conditions(ES = 1.05; 24%)
No statistical difference butpossible greater ESs in bandcondition (ES = 0–0.24;�0%–6%)
BF CON first, middle,last
35 6 1956 6 3057 6 33
40 6 1750 6 1958 6 30
Main effect (P < .05)rep 1 lower than rep 5(ES = 0.80; 21%)
No statistical or meaningfuldifferences between condi-tions (ES � 0.26; �1%–6%)
GME CON first, middle,last
27 6 937 6 1644 6 21
36 6 1947 6 2363 6 28
Main effect (P < .05)rep 1 lower than rep 5(ES = 1.14; 23%)
No statistical difference butgreater ESs in band condition(ES = 0.32–0.43; �9%–19%)
GMA CON first, middle,last
40 6 2166 6 2677 6 20
61 6 28*74 6 2892 6 30
Main effect (P < .05)rep 1 lower than rep 5(ES = 1.34; 35%)
Significant interaction (P <.05). Greater ESs in bandcondition (ES = 0.29–0.84;�8%–21%)
VL ECC first, middle,last
60 6 1565 6 1874 6 13
67 6 2774 6 2385 6 46
Main effect (P < .05)rep 1 lower than rep 5(ES = 0.62; 16%)
No statistical difference butgreater ESs in band condition(ES = 0.32–0.43; �7%–11%)
BF ECC first, middle,last
12 6 818 6 1917 6 11
13 6 617 6 1218 6 11
No statistical differen-ces between reps 1and 5 across condi-tions but small ESs(ES = 0.4; �5%)
No statistical or meaningfuldifferences between condi-tions (ES � 0.14; �1%)
GME ECC first, middle,last
12 6 513 6 619 6 10
20 6 1325 6 1535 6 21
Main effect (P < .05)rep 1 lower than rep 5(ES = 0.84; 11%)
No statistical difference butgreater ESs in band condition(ES = 0.32–1.03; �8%–16%)
GMA ECC first, middle,last
13 6 819 6 1227 6 11
21 6 932 6 1644 6 27
Main effect (P < .05)rep 1 lower than rep 5(ES = 1.26; 18%)
Significant main effect (P <.05). Greater ESs in bandcondition (ES = 0.82–0.93;�8%–17%)
Notes: Data in the control and band columns represents means 6 SD (% of MVC). VL: vastus lateralis, BF: biceps femoris, GME: gluteusmedius, GMA: gluteus maximus; CON: concentric, ECC: eccentric, ES: effect size, rep: repetition; *significant difference between specificrepetitions.
Spracklin et al. J Perform Health Res. 2017. 1(1)
66
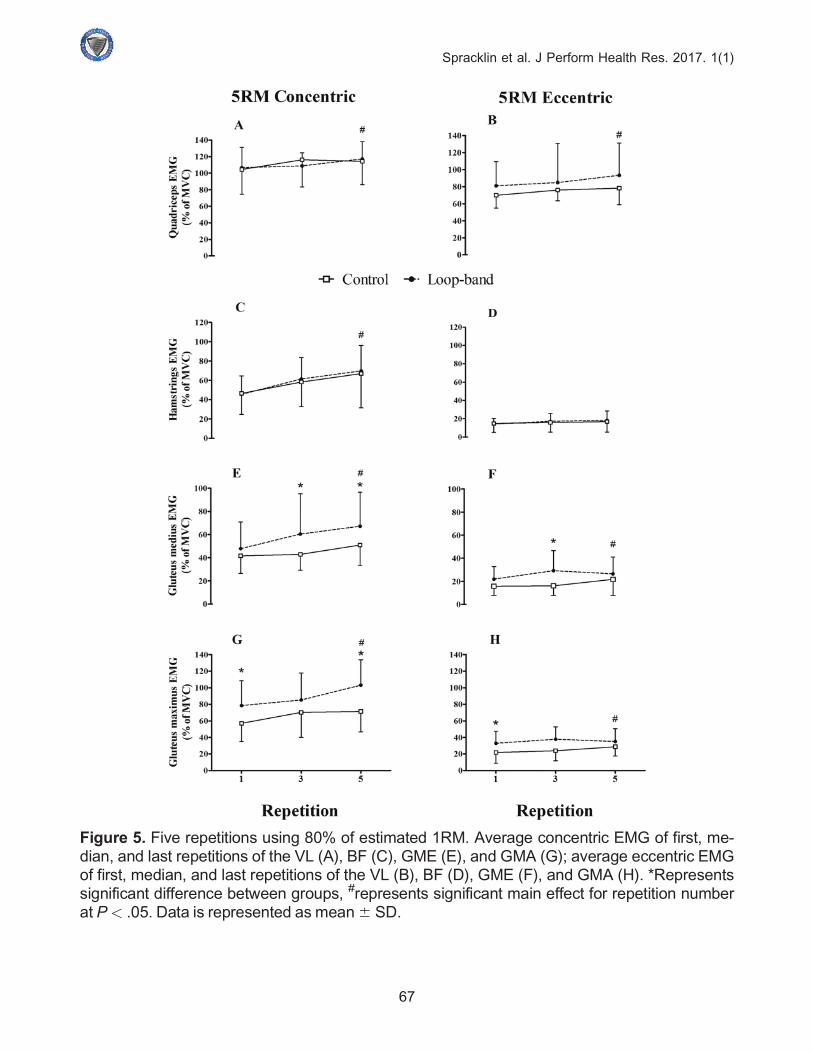
Figure 5. Five repetitions using 80% of estimated 1RM. Average concentric EMG of first, me-dian, and last repetitions of the VL (A), BF (C), GME (E), and GMA (G); average eccentric EMGof first, median, and last repetitions of the VL (B), BF (D), GME (F), and GMA (H). *Representssignificant difference between groups, #represents significant main effect for repetition numberat P< .05. Data is represented as mean6 SD.
Spracklin et al. J Perform Health Res. 2017. 1(1)
67
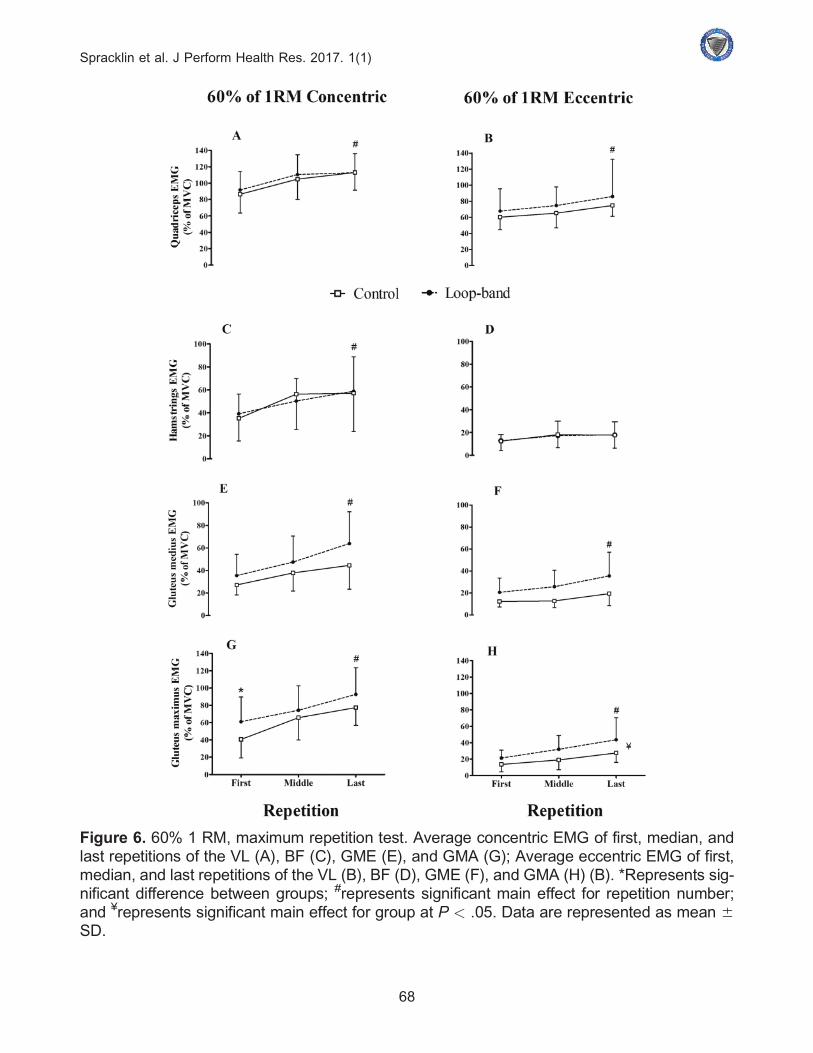
Figure 6. 60% 1 RM, maximum repetition test. Average concentric EMG of first, median, andlast repetitions of the VL (A), BF (C), GME (E), and GMA (G); Average eccentric EMG of first,median, and last repetitions of the VL (B), BF (D), GME (F), and GMA (H) (B). *Represents sig-nificant difference between groups; #represents significant main effect for repetition number;and ¥represents significant main effect for group at P < .05. Data are represented as mean 6SD.
Spracklin et al. J Perform Health Res. 2017. 1(1)
68

DISCUSSIONThe goals of this study were 2-fold. The first
was to investigate how placement of theTheraBand looped bands around the distallateral thighs affects EMG amplitudes of vari-ous lower body muscles during moderate- andhigh-intensity FBBS among resistance-trainedmales. The second goal was to examine howthe looped bands influence performancemeasured by the number of repetitions partic-ipants were able to complete using a submaxi-mal load (60% estimated 1RM).
In agreement with previous literature,7,8
greater EMGamplitudes of the glutealmuscles(both GME and GMA) were detected underthe looped-band condition. We observed thisin both the 5 repetitions at 80% of estimated1RM and the repetitions to failure test at 60%of estimated 1RM during both the concentricand eccentric phases of the squat. The loopedband-induced increase in GME during thesquats may be due to increased stabilization ofthe pelvis and avoiding medial knee col-lapse,2,12 and the increasedGMAmay contrib-ute more to avoiding internal rotation of thehip.2,12 In contrast, the quadriceps and ham-string muscle groups showed no meaningfulchange in EMG amplitudes when the loopedband was applied. The increased EMG ampli-tudes of the gluteal muscles is somewhatexpected given that the hip abductors arerequired to resist the forces created by theloopedband.
Gooyers et al.9 hypothesized that frontalknee plane mechanics remained unchanged intheir study because unpublished findings fromtheir laboratory indicated that the loopedbands may have elicited greater activity in thelateral thigh muscles (VL) during squattingmovements. The results from our study do notsupport this contention in a trained popula-tion, as the quadriceps did not show a signifi-cant change in EMG when the looped bandwas applied.
In general, all muscles showed a commontrend: greater EMG amplitudes from the first,
to the middle, and to the last repetition, exceptfor the eccentric contraction of the hamstringsduring both the 5 repetitions using 80% of esti-mated 1RM and the repetitions to failure testusing 60% of estimated 1RM. The increase inEMG amplitudes with increasing repetitionnumber is typical during submaximal fatiguingcontractions.18,19 It may be that EMG ampli-tudes increased to sustain the required efforts:with each completed repetition, muscle fatiguedevelops for various central and peripheralnervous system reasons. EMG is a crude mea-sure of central drive, as it is also influenced byperipheral factors.20 However, the incrementalincreases in EMG found in this study couldindicate increased central drive to overcomefatigue.18,19
Although the placement of the looped bandconsiderably influencedEMGamplitudes dur-ing the repetitions to failure 60% of estimated1RM test, it did not statistically influence thenumber of repetitions completed.However, onaverage, the number of repetitions completedby participants increased by 1 in the looped-band condition. Although this was not statisti-cally significant, clinicians, coaches, and train-ees in a real-world setting may want toincorporate this method to help athletesincrease their repetition totals. To the best ofour knowledge, this is the first study to investi-gate the effects of a looped band on perform-ance rather than only EMGamplitudes and/orbiomechanical alignment. Given the lack ofnegative, and even the potential positiveeffects, in conjunctionwith the increasedEMGamplitudes, further research investigating theeffects that looped bands have on performanceis aworthwhile and interesting researchavenue.
A number of difficulties were encountered inthis study. First, some participants reportedthat the looped bands in this experiment wereforceful and were apprehensive to use themduring their first practice sets.However, tensorwraps were found to decrease the level of dis-comfort. Second, the placement of the loopedbandproved difficult to standardize on partici-pants, as the looped band would not stay flat-tened against the participant’s thighs, as it
Spracklin et al. J Perform Health Res. 2017. 1(1)
69
would naturally follow the path of least resist-ance on theparticipants’ legs.Developing tech-nical strategies to assist in maintaining thelooped band in a flattened position during asquat iswarranted.
Practical ImplicationsCoaches tend to focus on strengthening the
hips of athletes who are involved in a widerange of athletic endeavors,2 as it is generallybelieved the hip musculature plays an impor-tant role with regard to bettering one’s over-all performance and reducing injuryrates.14,21 Therefore, it is generally agreedthat activating the hips to a greater extent canserve a dual purpose of increasing athleticperformance and correcting dysfunction ofthe lower extremities. Coaches and trainerswho program high-intensity squat trainingcan also use the looped bands to activate thehip musculature to a greater degree knowingthat it should not have a negative effect onperformance.
CONCLUSIONSThe findings suggest that looped bands
around the distal lateral portion of the thighlead to:
• increased EMG amplitude of the glutealmuscle group;
• no change in hamstring or quadricepsEMG amplitude; and
• no change in performance (but may have asmall positive benefit).
Future efforts to examine the impact oflooped bands around the distal thigh shouldfocus on:
• biomechanical change on frontal kneeplane mechanics in a trained populationduring high-intensity squatting; and
• the effect of the looped band on the FBBSat lower intensities in recreationally trainedathletes from both a biomechanical andmuscular perspective.
Recreational athletes could potentially havethe greatest room for improvement in theirsquatting technique, as trained athletes havepracticed and refined the squat to a greaterdegree.
Financial Disclosure: This research wassupported with an unrestricted grant fromPerformance Health. The authors report noconflicts of interest.
REFERENCES1. Gullett JC, et al. A biomechanical comparison
of back and front squats in healthy trained indi-viduals. J Strength Cond Res. 2009;23(1):284–292.
2. Schoenfeld BJ. Squatting kinematics and kineticsand their application to exercise performance. JStrength Cond Res. 2010;24(12):3497–3506.
3. McBride JM, et al. Relationship between maxi-mal squat strength and five, ten, and forty yardsprint times. J Strength Cond Res. 2009;23(6):1633–1636.
4. Wisløff U, et al. Strong correlation of maximalsquat strength with sprint performance and verticaljump height in elite soccer players. Br J Sports Med.2004;38(3):285–288.
5. Chelly MS, et al. Effects of a back squat trainingprogram on leg power, jump, and sprint performan-ces in junior soccer players. J Strength Cond Res.2009;23(8):2241–2249.
6. Comfort P, et al. Are changes in maximal squatstrength during preseason training reflected inchanges in sprint performance in rugby league play-ers? J Strength Cond Res. 2012;26(3):772–776.
7. Dai B, et al. A resistance band increased internal hipabduction moments and gluteus medius activationduring pre-landing and early-landing. J Biomech.2014;47(15):3674–3680.
8. Cambridge ED, et al. Progressive hip rehabilitation:the effects of resistance band placement on glutealactivation during two common exercises. ClinBiomech. 2012;27(7):719–724.
9. Gooyers CE, et al. The influence of resistance bandson frontal plane knee mechanics during body-weightsquat and vertical jump movements. SportsBiomech. 2012;11(3):391–401.
10. Liebenson C. Functional Training Handbook.Lippincott Williams &Wilkins; 2014.
11. Cook G, et al. Reactive neuromuscular training forthe anterior cruciate ligament-deficient knee: a casereport. J Athl Train. 1999;34(2):194–201.
12. Geiser C, et al. Effects of isolated hip abductor fa-tigue on frontal plane knee mechanics. Med SciSports Exerc. 2010:42(3): 535–545.
Spracklin et al. J Perform Health Res. 2017. 1(1)
70
13. Powers CM. The influence of abnormal hipmechanics on knee injury: a biomechanical per-spective. J Orthop Sports Phys Ther. 2010;40(2):42–51.
14. Hewett TE, et al. Anterior cruciate ligament inju-ries in female athletes: Part 1, mechanisms andrisk factors. Am J Sports Med. 2006;34(2):299–311.
15. Padua DA, et al. Neuromuscular characteristics ofindividuals displaying excessive medial knee dis-placement. J Athl Train. 2012;47(5):525–536.
16. Nakagawa TH, et al. The effect of additionalstrengthening of hip abductor and lateral rotatormuscles in patellofemoral pain syndrome: a random-ized controlled pilot study. Clin Rehabil. 2008;22(12):1051–1060.
17. Cohen J. A power primer. Psychol Bull. 1992;112(1):155–159.
18. Walker S, et al. Neuromuscular fatigue duringdynamic maximal strength and hypertrophic resist-ance loadings. J Electromyogr Kinesiol. 2012;22(3):356–362.
19. Smilios I, et al. Power output and electromyo-graphic activity during and after a moderate loadmuscular endurance session. J Strength Cond Res.2010;24(8):2122–2131.
20. Farina D, et al. Decoding the neural drive tomuscles from the surface electromyogram. ClinNeurophysiol. 2010;121(10):1616–1623.
21. Delp SL, et al. Variation of rotation momentarms with hip flexion. J Biomech. 1999;32(5):493–501.
Spracklin et al. J Perform Health Res. 2017. 1(1)
71