lobar atelectasis : typical and atypical radiographic and ... · kyung soo lee, et al: lobar...
TRANSCRIPT

Journ al of the Korean Radiological Society, 1995: 32( 4) : 595-605
Lobar Atelectasis : Typical and Atypical Radiographic and CT Findings1
Kyung 500 Lee, M.D. , Joong Mo Ahn, M.D. ,
Jung-Gi 1m, M.D.2, Nestor L. Müller, M.D. , PhD.3
The characteristic radiographic and CT findings of lobar atelectasis are well known. However, lobar atelectasis is a dynamic process, and atypical presentations may occur due to a number of different causes. Familiarity with the various typical and atypical radiographic findings of lobaratelectasis is important for correct diagnosis. The aim of this manuscript is toillustrate the spectrum of radiographic findings of lobar atelectasis and to correlate the radiographic findings with the CT findings. The review will illustrate examples of typical and atypicallobar atelectasis, including combined lobar atelectasis, peripherallobar atelectasis, migrating lobar atelectasis, rounded atelectasis involving the entire lobeand lobaratelectasis mimicking paravertebral and mediastinal masses.
Index Words: Lung , collapse
Lung , CT Lung , radiography
INTRODUCTION
Volume loss leads to anatomic alterations within the atelectatic lobe as well as compensatory changes in adjacent structures as they attempt to occupy the space left by the atelectatic lobe (1 - 3). Considerable volume loss is required in order to increase the opacity of the lung. More sensitive findings of atelectasis include displacement of the interlobar fissures , hila, mediastinum and bronch i. The presence and conspicuity of the various findings is influenced by the severity of atelectasis, type of atelectasis , condition of the underlying lung , as well as the presence of extrap비 monary abnormal ities such as pleural thickening. Awareness of the various direct and indirect signs of lobar atelectasis and of atypical presentations is important in order to make the
correct diagnosis. The diagnosis of lobar atelectasis can usually be
'DeparlmenlofD iagnoslic Imaging, Samsung Medical Cenler (KSL, JMA) 2DepartmenlolRadiology, CollegeolMedicine, Seoul Nalional Universily (JGI) 3Departmenl 01 Radiology, Universily 01 Brilish Col umbia and Vancouver Hospital and Health Sciences Cenlre (NLM) Recipient 01 a Certilicate 01 Merit award lor a scientilic exhibitatthe1994 RSNA scienlilic assembly and Bronse Medal Award lor a Scienlilic Exhibilatthe 1994 Korean Radiological Sociely Meeling Received March 5, 1995; Accepted April17 , 1995 Address reprinl requesls 10 :Kyung Soo Lee, M.D., Deparlmenl 01 Diagnoslic Imaging , Samsung Medical Cenler , # 50 Irwon-Dong , Kangnam-Ku , Seoul 135-230, Korea. Tel. 82- 2- 341 0- 2511 ,2516 Fax. 82- 2-3410- 2559
made based on findings of the chest radiograph. Computed tomography (CT) can be helpful in the assessment of patients with lobar atelectasis, partic비 arly
when the radiographic findings are atypical (4-7). CT is also often performed in order to determine the underlying cause for the atelectasis.
The aims of this manuscript are to illustrate the vari。us forms of typical and atypical lobar atelectasis on chest radiographs and to correlate the radiographic findings of lobar atelectasis with those seen on CT.
Right Upper Lobar Atelectasis Right upper lobe (RUL) atelectasis results in ove
rinflation of the right middle lobe and shift of the minor fissure superiorly and medially (Table 1). It also results in compensatory overinflation of the right lower lobe (RLL) with shift of the major fissure anteriorly, superiorly and medially (Fig. 1). The Golden ’s S sign denotes a centrally located mass with associated lobar atelectasis. The mass should be large enough to be borderforming with the adjacent hyperexpanded lung (Fig. 1). With complete atelectasis , the RUL is either pancaked medialiy , simulating mediastinal widening or a mediastinal mass (Fig. 2) , or superiorly simulating an apical pleural cap
On the lateral chest radiograph , an ill - defined opacity anterior to the trachea and obliteration 01 the anterior margin olthe ascending aorta may sometimes be the only lindings (1 -3) .
595 -

Journ al of the Korean Radiologica l Society. 1995; 32(4) : 595- 605
The minor fissure changes its position more dramatically than does the major fissure. With elevation of
the minor fissure. the middle lobe shifts up laterally
alongside the atelectatic upper lobe. At CT the middle
and upper lobes can be seen side - by - side anterior to
the major fissure with the superior segment of the
lower lobe posterior to the fissure (Fig. 1). The major
fissure maintains its previous contour . whether str-
aight. concave. or convex (4 -7)
Left Upper Lobar Atelectasis
With LUL atelectasis. the direction of movement is
anterosuperior rather than directly superior as in RUL atelectasis (Table 2). The left p비 monary artery . which
courses over the left main bronchus. restrains the
bronchus and limits the superior migration of the
a Fig. 1. Typical right upper lobar atelectasis
b
a. Chest radiograph shows right upper lung zone opacity marginated laterally by the elevated right minor fissure. b. Conventional (10 mm collimation) CT scan demonstrates atelectatic right upper lobe marginated laterally by right minor fissure (arrowheads) and posteriorly by right m러。r fissure (arrow). Due to central mass. the medial major fissure shows convex border (Golden ’ sSsign)
a b Fig . 2. Right upper lobar atelectasis simulating rightsuper ior mediastinal mass a. Chest radiograph shows semilunar opacity abutting right superior mediastinum b. Conventional (10 mm collimation) enhanced CT scan at level of distal trachea shows atelectatic right upper lobe with mucoid impaction in dilated bronchi. Atelectatic upper lobe is sharply marginated laterally by the minor fissure
% -「J
Kyun g Soo Lee, et al: Lobar Atelectasis
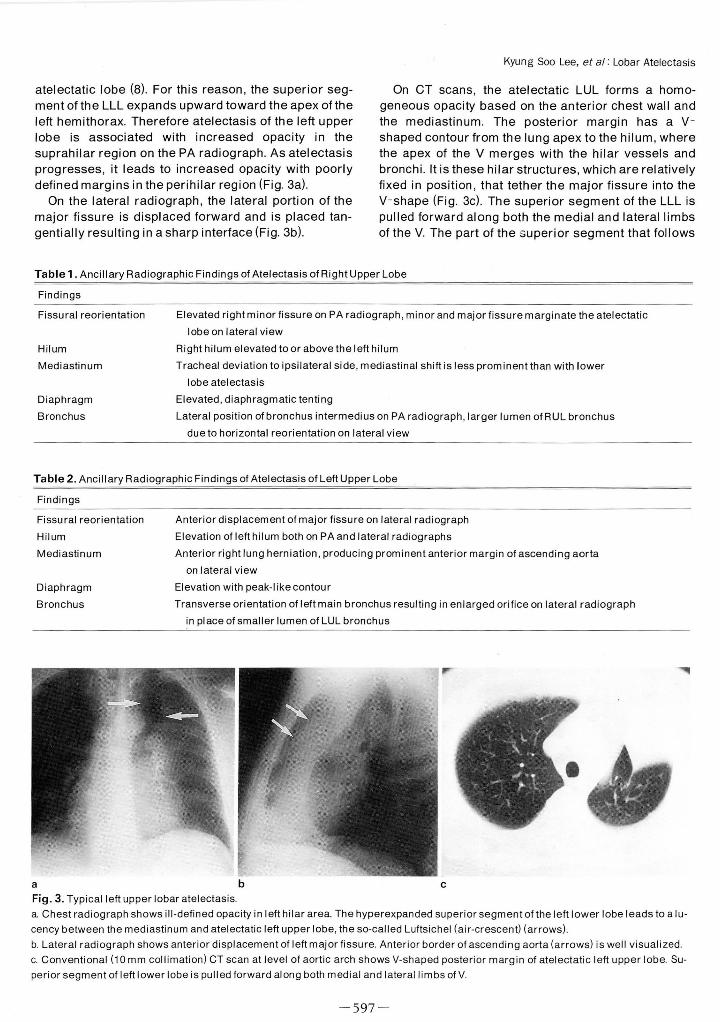
atelectatic lobe (8) . For this reason , the superior seg
ment of the LLL expands upward toward the apex of the
left hemithorax. Therefore atelectasis of the left upper
lobe is associated with increased opacity in the
suprahilar region on the PA radiograph. As atelectasis
progresses , it leads to increased opacity with poorly
defined margins in the perihilar region (Fig. 3a)
On the lateral radiograph , the lateral portion of the
major fissure is displaced forward and is placed tan
gentially resulting in a sharp interface (Fig. 3b)
On OT scans, the atelectatic LUL forms a homo
geneous 이객city based on the anterior chest wall and
the mediastinum. The posterior margin has a V
shaped contour from the lung apex to the hilum , where
the apex of the V merges with the hilar vessels and
bronchi . It is these hilar structures, which are relatively
fixed in position , that tether the major fissure into the
V - shape (Fig. 3c). The superior segment of the LLL is
pulled forward along both the medial and laterallimbs
of the V. The part of the superior segment that follows
Table 1. Ancillary Radiographic Findings of Atelectasis of Right Upper Lobe
Findings
Fissural reorientation
Hilum
Mediastinum
Diaphragm
Bronchus
Elevated right minor fissure on PA radiograph , minor and major fissure marginate the atelectatic
lobe on lateral view
Right hilum elevated to or above the left hilum
Tracheal deviation to ipsilateral side , mediastinal shift is less prominent than with lower
lobe atelectasis
Elevated , diaphragmatic tenting
Lateral position of bronchus intermedius on PA radiograph , larger lumen of RUL bronchus
due to horizontal reorientation on lateral view
Table 2. Ancillary Radiographic Findings of Atelectasis of Left Upper Lobe
Findings
Fissural reorientation
Hilum
Mediastinum
Diaphragm
Bronchus
Anterior displacement of major fissure on lateral radiograph
Elevation of left hilum both on PA and lateral radiographs
Anterior right lung herniation , producing prominent anterior margin of ascending aorta
on lateral view
Elevation with peak-I ike contour
Transverse orientation of left main bronchus resulting in enlarged orifice on lateral radiograph
in place of smaller lumen of LUL bronchus
a b c Fig. 3. Typicalleft upper lobar atelectasis
1 ’
a. Chest radiograph shows ill-defined opacity in left hilar area. The hyperexpanded superior segment ofthe left lower lobe leads to a lu
cency between the mediastinum and atelectatic left upper lobe, the so-called Luftsichel (air-crescent) (arrows)
b. Lateral radiograph shows anterior displacement of left major fissure. Anterior border of ascending aorta (arrows) is well visualized.
c. Conventional (10 mm collimation) CT scan at level of aortic arch shows V-shaped posterior margin of atelectatic left upper lobe. Su
perior segment of left lower lobe is p비 led forward along both medial and laterallimbs of V.
- 597 -

Journal of the Korean Radiological Society, 1995 : 32(4) : 595- 605
the medial limb forms a tongue of lung between the
mediastinum and the atelectatic LUl. This tongue is
visible on PA radiographs and has been called the
Luftsichel (air - crescent) or periaortic lucency (7) (Fig.
3c) . Less commonly , the major fissure may have a
straight border rather than a V - shaped contour (Fig. 4)
a b
a
a b
Occasionally the atelectatic lobe may have sharp
margins on the PA radiograph simulating a hilar mass
(Fig. 4 , 5). With marked LUL atelectasis , the contour of
the major fissure interface may appear continuous with
that of the normal epipericardial fat on the lateral
radiograph (Fig. 5) .
Fig. 4. Complete atelectasis 01 left upper
lobe.
a. Chest radiograph shows mass-like lesion
in left hilar area. b. Thin-section (1.5collimation) CT scan
。btained at level 01 carina shows atelectatic
left upper lobe. Left upper lobe, being re
placed only by dilated bronchi , is marginated posteriorly by maj or lissure
Fig. 5. Complete atelectasis 01 left upper
lobe simulating left hilar mass
a. Chest radiograph shows mass-like lesion in left hilar area. III-delined opacity is als。
shown superior to mass-like I esion. b. Lateral radiograph shows anteriorly dis
placed left major fissure , inlerior aspect 01
which is continuous with normal epicardial lat (arrows)
Fig. 6. Typical right middle lobar atelecta-
515
a. Posteroanterior chest radiograph shows
triangular shaped opacity in right lower
lung zone with obliteration of right lower
cardiac border b. Lateral radiograph shows triangular 。pacity in anterior aspect 01 thorax over
lapped with cardiac silhouette with its apex
toward hilum.
-598 -
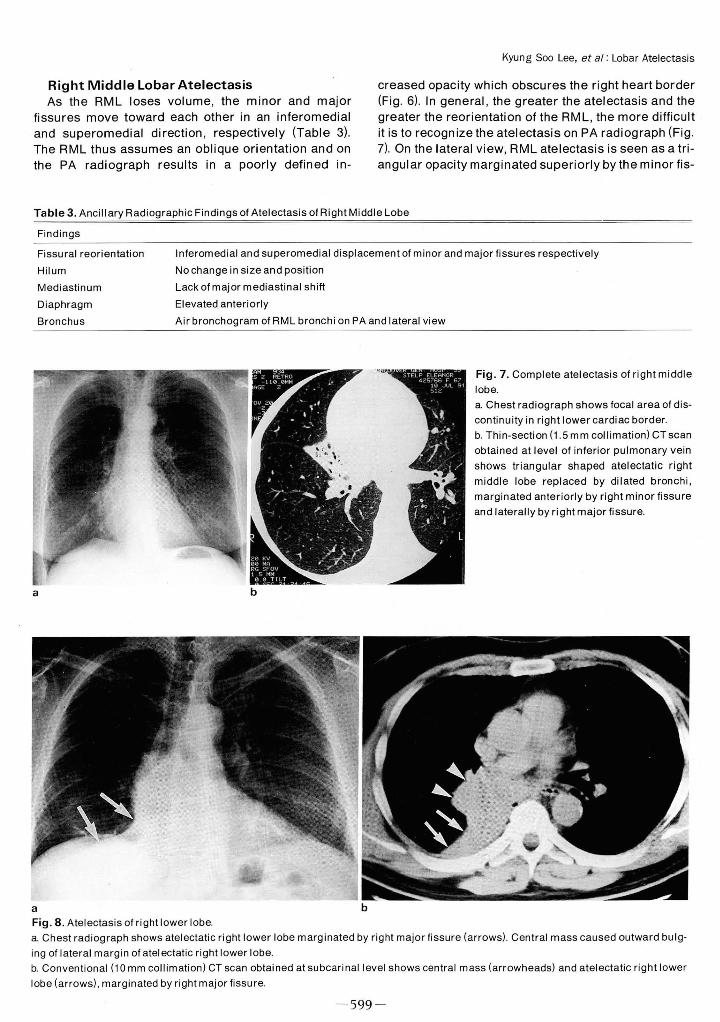
Right Middle Lobar Atelectasis
As the RML loses volume, the minor and major
fissures move toward each other in an inferomedial
and superomedial direction , respectively (Table 3) The RML thus assumes an oblique orientation and on
the PA radiograph results in a poorly defined in-
Kyun g Soo Lee, et al: Lobar Atelectasis
creased opacity which obscures the right heart border
(Fig. 6) . In general , the greater the atelectasis and the
greater the reorientation of the RML, the more difficult
it is to recognize the atelectasis on PA radiograph (Fig.
7). On the lateral view, RML atelectasis is seen as a tri
angular opacity marginated superiorly by the minor fis-
Table 3 . Ancillary Radiographic Findings of Atelectasis of Right Middle Lobe
Findings
Fissural reorientation
Hilum
Inferomedial and superomedial displacement of minor and major fissures respectively
No change in size and position
Mediastinum
Diaphragm
Bronchus
a
Lack of major mediastinal shift
Elevated anteriorly
Air bronchogram of RML bronchi on PA and lateral view
b
a b Fig. 8. Atelectasis of right lower lobe
Fig. 7. Complete atelectasis of right middle
lobe
a. Chest radiograph shows focal area of dis
continuity in right lower cardiac border.
b. Thin-section (1 .5 mm collimation) CTscan
。btained at level of inferior p비 monary vein
shows triangular shaped atelectatic right
middle lobe replaced by dilated bronchi ,
marginated anteriorly by right minor fissure
and laterally by right major fissure‘
a. Chest radiograph shows atelectatic right lower lobe marginated by right major fissure (arrows). Central mass caused outward bulg
ing of lateral margin of atelectatic right lower lobe.
b. Conventional (10 mm collimation) CT scan obtained at subcarinallevel shows central mass (arrowheads) and atelectatic right lower
lobe (arrows) , marginated by right major fissure.
599

Journal of the Korean Radiological Society, 1995 : 32( 4) : 595 - 605
sure and inferiorly by the major fissure (Fig. 6b). The
apex of the triangle is in the hilar area, and the base is
located peripherally.
On CT scans , the RML is triangular or trapezoidal
(Fig. 6 , 7). Its posterior border, demarcated by the
major fissure , is usually well defined because the
major fissure crosses the scan plane almost
perpendicularly. On the other hand, the interface be
tween RML and RUL is often less distinct because of
the dome - shaped contour ofthe minor fissure.
Table 4. Ancillary Radiographic Findings 01 Lower Lobe Atelectasis
Findings
lower lobar Atelectasis
As the lower lobes become atelectatic, the lateral
portion of the major fissure moves posteriorly toward
the costophrenic angle and may be well delineated on
the lateral radiograph (Table 4). The medial portion of
the major fissure relates to the mediastinal wedge of
pulmonary attachment. The wedge is frequently diffi
cult to detect on the lateral radiograph except for a
slight area of increased opacity extending from the
posterior costophrenic angle toward the hilum. On PA
Fissural reorientation
Hilum
Inleroposterior displacement 01 both major and minor lissures
Downward displacement, small size
Mediastinum
Diaphragm
8ronchus
a
Obliteration 01 IVC and descending aorta shadow with RLL and LLL atelectasis respectively,
contact 01 RUL and LUL with anterior mediastinum with each lobar atelectasis
Portions 01 each hemidiaphragm that abuts the atelectatic lower lobe may be obscured
Vertical orientation 01 lower lobar bronchus in PA radiograph , posterior and downward
displacementol ipsilateral upper lobar bronchus on lateral radiograph
Fig. 9. Complete atelectasis 01 ri ght lower lobe a. Chest radiograph shows a line shadow suggesting lateral margin 01 right major lissure in right retrocardiac area. Note oligemic hilar vessels. b. Thin-section (1.0 mm collimation) CT scan obtained at level 01 distal bronchus intermedius shows posteriorly displaced right minor lissure and atelectatic right lower lobe (arrow) marginated by right major lissure. c. CT scan obtained 10 mm distal to (b) shows a branch (arrow) 01 c right m iddl e I obar bronchus , oriented posteriorly and superiorly.
- 600
~
1

radiographs , the lateral margin of the lobe may be ill defined or well defined, depending on whether or not the adjacent hyperexpanded lung has placed the fissural edge of the lower lobe tangential to the X - ray beam (Fig. 8)
On CT scans , the lower lobes lose volume in a posteromedial direction , pulling down the majorfissure (Fig. 8). The lateral portion of this fissllre demonstrates a greater degree of mobility, because the medial portion is fixedto the mediastinum by the hilar structures and the inferior p비 monary ligament.
If marked atelectasis of the RLL has occurred , the triangular - shaped opacity may be difficult to detect
a b
Kyung Soo Lee, et al : Lobar Atelectasis
through the mediastinum because of its small size (Fig. 9). In LLL atelectasis , the involved lobe may appear as a left paraspinal mass instead of the more characteristic triangular shape with the apex atthe hilum and the base at the left hemidiaphragm (Fig. 1 이. The appearance of lower lobar atelectasis as a paraspinal mass is believed to result from incomplete attachment ofthe inferior p비 monary ligamentto the hemidiaphragm (9)
Combined Lobar Atelectasis Combined lobar atelectasis refers to the condition in
which the volumes of two lobes of the lung are decreased simultaneously (1 , 3, 1 이 Because theright
Fig. 10. Atypical atelectasis 01 left lower lobe simulating left paraspinal mass a. Chest radiographs shows left hilar prominence and unusual branching pattern 01 hilar vessels. Margin 01 descending aorta is interrupted distally (arrow), suggesting possible left paraspinal mass. Note shilt 01 upper mediastinum to the lelt. b. Conventional (10 mm collimation) CT scan obtained at ventricular level shows atelectatic left lower lobe, posteriorly in paraspinal area
a b
- 601 -
Fig. 11. Combined atelectasis 01 right middle and lower lobes due to mucus impaction in bronchus intermedius. a. Chest radiograph shows opacity in right lower lung zone obscuring right atrium and right hemidiaphragm. Inlerior displacement 。1 major (arrows) and minor (arrowheads) lissures is presen t. Also note inlerior displacement 01 right hilum and hyperexpan-sion 01 ri ght upper lobe b. Lateral radiograph shows opacilication throughout right lower lung zone obscuring right hemidiaphragm. Upper border 01
opacity is bordered anteriorly by minor lissure and posteriorly by major lissure

Journal of the Korean Radiological Society, 1995; 32(4) : 595-605
a b Fig. 12. Combined atelectasis of right upper and middle lobes due to metastatic endobronchial tumor. a. Chest radiograph shows opacity in right upper and middle lung zones. Cephalad displacement and rotation of hilar vessels are observed. Right hemidiaphragmatic tenting is associated. Also noted are metastatic nodules and mass in left lung. b. Lateral radiograph shows anterior displacement of right major fissure (arrows).
Fig. 13. Combined atelectasis of right upper and lower lobes due to mucus plug. Chest radiograph following general anesthesia shows opacities in right upper and lower lung zones, sharply marginated by elevated right minor fissure (arrowheads) and depressed right major fissure (arrows) respectively. Right middle lobe is overexpanded
lung has three lobes, three combinations of combined atelectasis are possible. The most freq i.J ent combination is that of middle and lower lobar atelectasis caused by obstruction of the bronchus intermedius. Less commonly seen are combined atelectasis of the upper and middle lobes and combined right upper and
- 602
lower lobe atelectasis (1 이.
Combined Atelectasis of the Right Middle and Lower Lobes Because the bronchus intermedius is the common
pathway to the right middle and lower lobes, a single localized lesion involving the bronchus intermedius gives rise to combined atelectasis of these lobes. The bronchial obstruction can be caused by a tumor , a foreign body, a mucous plug, or an inflammatory stricture (10).
On the PA radiograph , the atelectatic RLL obscures the right hemidiaphragm , whereas the atelectatic right middle lobe obscures the right cardiac border (Fig. 11) Depression of boththe major and minor fissures is present, the depression being most marked laterally (Fig. 11 a). Other signs of combined atelectasis of the right middle and lower lobes include a small and depressed right hilum and decreased vascularity of a hyperexpanded RUL compared with the normal left lung. On the lateral view , increased opacity is present throughoutthe lower part ofthe chest.
On CT scans, the atelectatic RML and RLL occupy the lower hemithorax and abut the right cardiac border medially and the right hemidiaphragm inferiorly. The right major and minor fissures border the lateral and anteromedial margins ofthe atelectatic lobes, respectively (Fig. 11). Complete combined RML and RLL atelectasis can be difficult to detect on PA and lateral radiographs. The diagnosis should be suspected in patients with a small right hilum and an apparently 이igemic right lung which represents the hyperex-
panded RUL
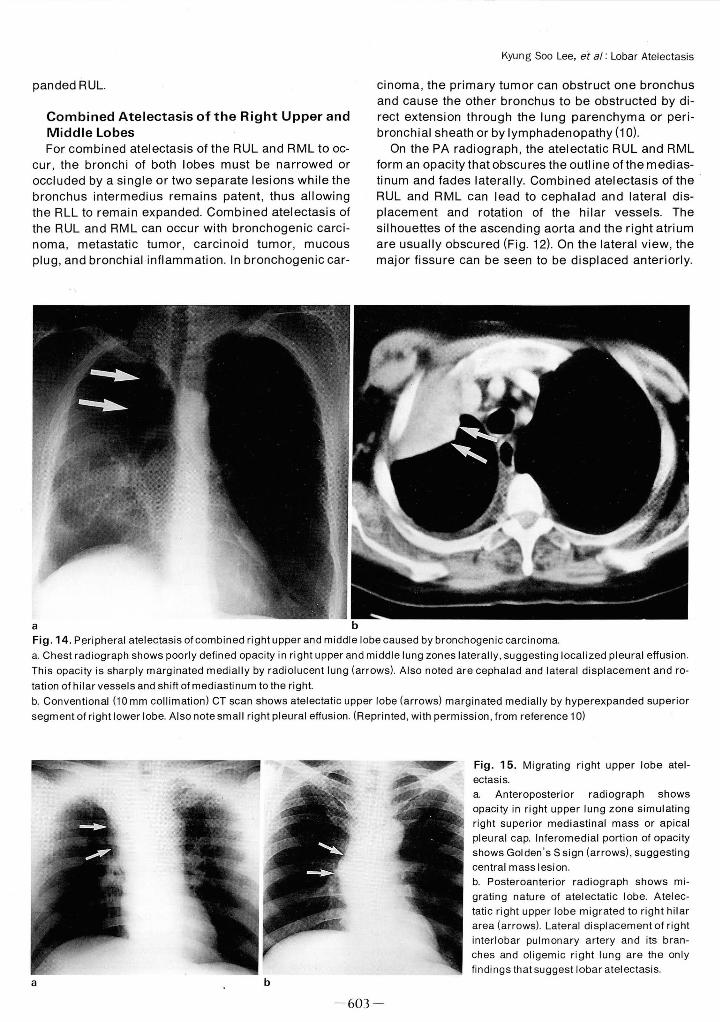
Combined Atelectasis of the Right Upper and
Middle Lobes
For combined atelectasis of the RUL and RML to occur , the bronchi of both lobes must be narrowed or
occluded by a single or two separate lesions while the
bronchus intermedius remains patent , thus allowing
the RLL to remain expanded. Combined atelectasis of
the RUL and RML can occur with bronchogenic carci
noma, metastatic tumor, carcinoid tumor, mucous plug , and bronchialinflammation. In bronchogenic car-
a
Kyun g Soo Lee, et al : Lobar Atelectasis
cinoma , the primary tumor can obstruct one bronchus and cause the other bronchus to be obstructed by di
rect extension through the lung parenchyma or peri
bronchial sheath or by Iymphadenopathy (1 이. On the PA radiograph , the atelectatic RUL and RML
form an opacity that obscures the outline of the mediastinum and fades laterally. Combined atelectasis of the
RUL and RML can lead to cephalad and lateral dis
placement and rotation of the hilar vessels. The
silhouettes of the ascending aorta and the right atrium
are usually obscured (Fig. 12). On the lateral view, the
major fissure can be seen to be displaced anteriorly.
Fig . 14. Peripheral atelectasis of combined right upper and middle lobe caused by bronchogenic carcinoma a. Chest radiograph shows poorly defined opacity in right upper and middle lung zones laterally , suggesting localized pleural effusion This opacity is sharply marginated medially by radiolucent lung (arrows). Also noted are cephalad and lateral displacement and rotation of hilar vessels and shift of mediastinum to the right b. Conventional (10 mm collimation) CT scan shows atelectatic upper lobe (arrows) marginated medially by hyperexpanded superior segment of right lower lobe. Also note small right pleural effusion. (Reprinted, with permission , from reference 1 0)
a b
• 603 -
Fig . 15. Migrating right upper lobe atel ectasis. a. Anteroposterior radiograph shows opacity in right upper lung zone simulating right superior mediastinal mass or apical pleural cap. Inferomedial portion of opacity shows Gol den ’s S sign (arrows) , suggesting central mass lesion‘
b. Posteroanterior radiograph shows migrating nature of atelectatic lobe. Atelectatic right upper lobe migrated to right hilar area (arrows). Lateral displacement of right interlobar p비monary artery and its branches and 이igemic right lung are the only findings that suggest lobar atelectasis
Journal of the Korean Radiologica l Society, 1995 ; 32( 4) : 595- 605
a
The relative proximity 01 the major 1issure to the anterior chest wall is dependent on the degree 01 atelectasis 01 the RUL and RM L. Retrosternal radiolucency , caused by herniation 01 the left lung into the retrosternal space, and the accentuated main pulmonary artery segment also can be seen on the lateral view (Fig. 12). The radiographic 1indings 01 combined atelectasis 01 the RUL and RML are similar to those of LUL atelectasis (1 0)
On CT scan , the atelectatic RUL and RML cause a wedge -shaped area of soft-tissue attenuation abutting the chest wall anteriorly and the ascending aorta and right cardiac border medially. This wedge -shaped opaci1ication extends inferiorly to the level 01 the right atrium. The major 1issure is displaced anteriorly, and the hyperexpanded lower lobe 1ills most of the right hemithorax.
Combined Atelectasis of the Right Upper and Lower Lobes Combined atelectasis of the RUL and RLL is rare. It
may be due to mucous plugs occurring simultaneously in the bronchi of the RUL and RLL. The radiographic 1indings of combined atelectasis of RUL and RLL are similar to those 01 isolated atelectasis 01 either lobe Upper lobe atelectasis leads to elevation of the minor 1issure, whereas lower lobe atelectasis leads to downward and medial shift of the major fissure (Fig. 13). On CT scans , the minor fissure if higher than normal because 01 the atelectasis 01 the RUL and more posterior than normal because of the atelectasis of the RLL. The middle lobe is overin1lated.
Peripheral Lobar Atelectasis Franken and Klatte (11) descri bed the radiographic
1indings of what they called “atypical (peripheral) right upper lobe atelectasis " , mimicking apical pleural e1-fusion. In this type of atelectasis 01 the RUL, the atelectatic lobe continues to lie adjacent to the lateral chest wal l. The dense lateral portion of the atelectatic
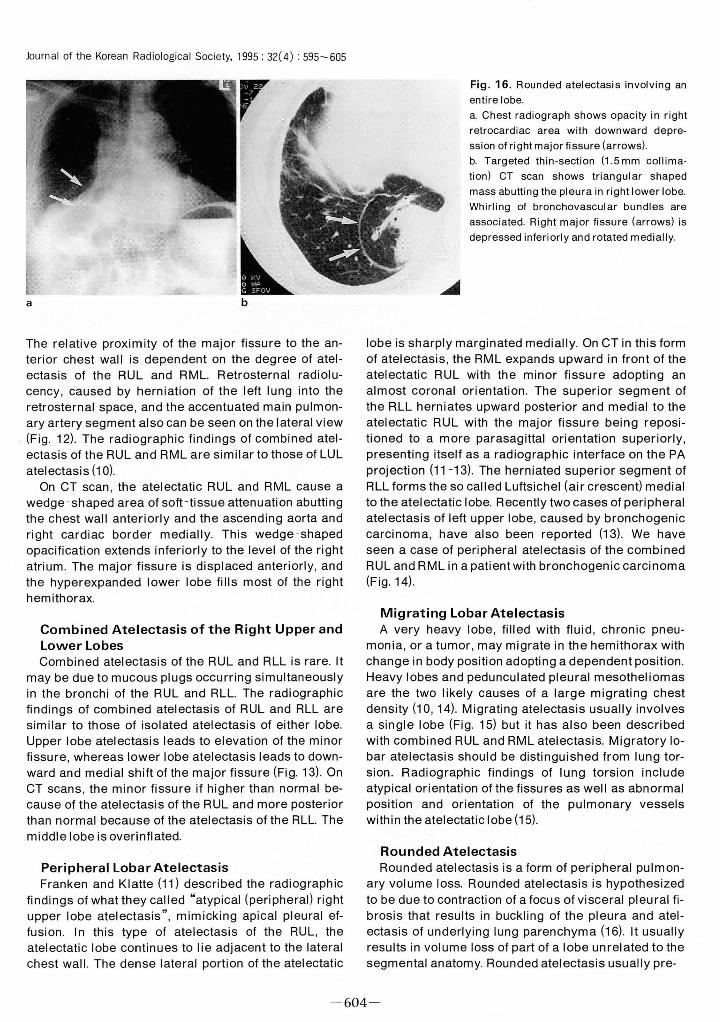
Fig. 16. Rounded atelectasis involving an entire lobe a. Chest radiograph shows opacity in r ight retrocard iac area with downward depression of right major fissure (arrows) b. Targeted thin-section (1.5 mm collimation) CT scan shows triangular shaped mass abutting the pleura in right lower lobe. Whirling of bronchovascular bundles are associated. Right m혀 or fissure (arrows) is depressed infer iorly and rotated medial ly
lobe is sharply marginated medially. On CT in this form 01 atelectasis , the RML expands upward in front 01 the atelectatic RUL with the minor fissure adopting an almost coronal or ientation. The superior segment 01 the RLL herniates upward posterior and medial to the atelectatic RUL with the major fissure being reposi tioned to a more parasagittal orientation superiorly, presenting itsel1 as a radiographic inter1ace on the PA projection (11 -13). The herniated superior segment 01 RLL forms the so called Luftsichel (air crescent) medial to the atelectatic lobe. Recently two cases of peripheral atelectasis 01 left upper lobe, caused by bronchogenic carcinoma, have also been reported (13). We have seen a case 01 peripheral atelectasis of the combined RUL and RML in a patientwith bronchogenic carcinoma (Fig. 14)
Migrating Lobar Atelectasis A very heavy lobe, 1illed with fluid , chronic pneu
monia, or a tumor , may migrate in the hem ithorax with change in body position adopting a dependent position. Heavy lobes and pedunculated pleural mesotheliomas are the two likely causes of a large migrating chest density (10 , 14). Migrating atelectasis usually involves a single lobe (Fig. 15) but it has also been described with combined RUL and RML atelectasis. Migratory 10-bar atelectasis should be distinguished from lung torsion . Radiographic findings 01 lung torsion include atypical orientation of the 1issures as well as abnormal position and orientation of the pulmonary vessels within the atelectatic lobe (15).
Rounded Atelectasis Rounded atelectasis is a form of per ipheral pulmon
ary volume loss. Rounded atelectasis is hypothesized to be due to contraction of a focus of visceral pleural fibrosis that results in buckling of the pleura and atel ectasis of underlying lung parenchyma (16). It usually results in volume loss of part 01 a lobe unrelated to the segmental anatomy. Rounded atelectasis usually pre-
- 604 -

sents as a mass that may sim비 ate a p비 monary neo
plasm on chest radiograph. The CTcriteria for the diag
nosis of rounded atelectasis include (1) a rounded or
oval mass abutting a pleural surface, (2) vessels and
bronchi curving into the mass, and (3) associated
pleural thickening with or without calcification (17)
Although rounded atelectasis is usually confined to a
small portion of lung , occasionally it may involve the
entire lobe and simulate a large mass (Fig. 16).
Kyung $00 Lee, et a/: Lobar Atelectasis
s;st Tomogr 1983 ; 7 : 758-767
6. Naidich DP, Ettinger N, Leitman BS, McCauley DI. CT 01 lobar col
lapse‘ Sem;n Roentgeno/1984 ; 19: 222-235
7. Raasch BN , Heitzman ER, Carsky EW, Lane EJ, Berlow ME, Witwer G. Computed tomographic study 01 bronchopulmonary
collapse. Rad;oGraphics 1984; 4: 195-232
8. Khoury MB, Godwin JD, Halvorsen RA, Putman CE. CT 01 lobar
collapse. Invest Radio/1985 ; 20 : 708-716
9. Glay J, Palayew MJ. Unusual pattern 01 left lower lobe atelecta
sis. Radiology 1981 : 141 : 331-333‘
10. Lee KS, Logan PM , Primack SL, Muller NL. Combined lobar atel-
REFERENCES ectasisofthe rightlung: imaging lindings. AJR 1994 ; 163 : 43-47 11 . Franken EA, Klatte EC. Atypical (peripheral) upper lobe collapse
1. Proto AV, Tocino 1. Radiographic manilestations 01 lobar col- Ann Radio/1977; 20: 87-93
lapse. SeminRoentgeno/1980 ; 15 : 117-173 12. Adler J, Cameron DC. CTcorrelation in peripheral rightupper 10-
2. Mintzer RA, Sakowicz BA, Blonder JA. Lobar collapse. Usual and bar atelectasis. JComput AssistTomogr 1988 ; 12: 51 0-511
unusual lorms. Chest1988; 94 : 615-620 13. Donc C, Desmarais R. Peripheral upper lobe collapse in adults.
3. Lubert M, Krause GR. Further observations on lobar collapse. Radiology 1989 ; 170 : 657-659
RadiolClinNorthAm1963 ;1 :331-346 14. Heitzman ER. The lung:radiologic-pathologic correlation , 2nd
4. Naidich DP , McCauley DI , Khouri NF, Leitman BS, Hulnick DH, ed. St. Lou is: Mosby, 1984 :457-501
Siegelman SS. Computed tomography 01 lobar collapse: 1. 15. Felson B. Lung torsion ‘ radiographic lindings in nine cases
endobronchial obstruction. J Comput Assist Tomogr 1983 ; 7: Radiology 1987 : 162 : 631-638 745-757 16. Menzies R, Fraser R. Rounded atelectasis. Pathologic and
5. Naidich DP , McCauley DI , Khouri NF, Leitman BS, Hulnick DH, pathogenetic leatures. Am J Surg Patho/1987 ; 11 : 674-681
Siegelman SS. Computed tomography 01 lobar collapse : 2. col- 17. McHugh K, Blaquiere RM. CT leatures 01 rounded atelectasis
lapse in the absence olendobronchial obstruction. JComput As- AJR 1989 ; 153: 257-260
대 한 방 사 선 의 학회 지 1995 ; 32( 4) : 595 - 605
대엽성 무기폐:전형적 및 비전형적 단순흉부촬영 및 전산화단층촬영 소견I
1 삼성의료원 진단방사선과 2서울대학교병원 진단방사선과
30epartment of Radiology, University of British Columbia and
Vancouver Hospital and Health Science Center
이경수 · 안중모 · 임정기2 • Nestor l. Müller3
대엽성 무기폐의 단순 흉부촬영 및 전산화단층촬영의 특징적 소견은 잘 알려져 있다. 하지만 무기폐는 역동적 과정이어서
비전형적인 소견이 드물지 않게 나타난다. 다양한 형태의 전형적 또는 비전형적인 무기폐의 방사선학적 소견에 친숙함으로
써 무기폐를 정확히 진단할 수 있다. 이 논문의 목적은 대엽성 무기폐의 다앙한 방사선학적 소견을 기술하고 단순촬영 소견
을 전산화단층촬영 소견과 연관시킨것이다. 즉 전형적인 소견과 연합성 무기폐, 말초형 무기폐, 전이성 무기펴1 , 원형 무기페,
그리고 척추 큰처나 종격동의 종괴 형태로 나타나는 비전형적인 무기폐를 기술한다.
- 605 -
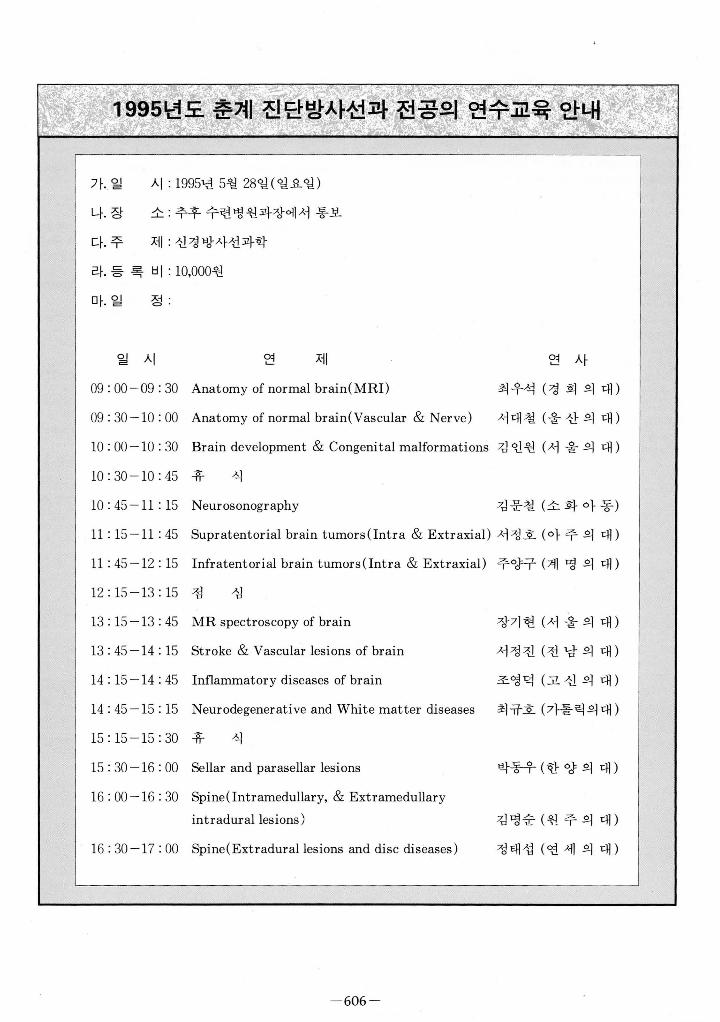
가. 일 시 : 1995년 5월 28일(일요일)
나. 장 소 : 추후 수련병원과장에서 통보
다.주 제 :신경방사선과학
라. 등 록 비 : 10,000원
마.일 정:
일 시 연 제 연 사
09: 00-09 : 30 Anatomy of normal brain(MRI) 최우석 (경 희 의 대 )
09: 30-10: 00 Anatomy of normal brain(Vascular & Nerve) 서대철 (울산의 대)
10: 00-10 : 30 Brain development & Congenital malformations 김 인원 (서 울 의 대 )
10: 30-10: 45 휴 식
10: 45-11 : 15 Neurosonography 검문철 (소화 아동)
11 : 15-11 : 45 Supratentorial brain tumors (Intra & Extraxial) 서정호 (아 주 의 대 )
11 : 45 -12 : 15 Infratentorial brain tumors (Intra & Extraxial) 주양구 (계 명 의 대 )
12 : 15 - 13 : 15 점 λ1 n
13 : 15 -13 : 45 MR spectroscopy of brain
13 : 45 -14 : 15 Stroke & Vascular lesions of brain
장기현 (서 울의 대)
서정진 (전남의 대)
14: 15 -14 : 45 Inflammatory diseases of brain 조영 덕 ( 고 신 의 대 )
14: 45 -15: 15 Neurodegenerative and White matter diseases 최규호 (가톨릭의대 )
15 : 15 -15 : 30 휴 식
15 : 30 -16: 00 Sellar and parasellar lesions
16: 00-16 : 30 Spine (Intramedullary, & Extramedullary
intradurallesions)
16 : 30 -17 : 00 Spine( Extradurallesions and disc diseases)
- 606-
박동우(한양의 대)
김명순 (원 주의 대)
정태섭 (연세 의 대)