liver abscess marc richards morning report september 8th, 2009
Post on 19-Dec-2015
230 views
TRANSCRIPT
LIVER ABSCESS
Marc RichardsMorning Report
September 8th, 2009
CLASSIFICATIONS
• PYOGENIC• Gram Positive• Gram Negative• Anaerobic• (Polymicrobial)
• AMEBIC
• CANDIDA
• TB (rare)
EPIDEMIOLOGY
• Pyogenic Abscesseso Bacterialo Most common o M > F 3:1
• Entamoebao M > F 7:1o 40-50 million amoeba infections/year
worldwideo Age Extremeso Endemic Areas most susceptible
o Country of origin or Travel
RISK FACTORS
• PYOGENIC• DM• Cancer• Liver Transplant
• ENTAMOEBA• Pregnancy• Steroids• Cancer• Endemic area travel (short
or long term)• EtOH?
PATHOPHYS.
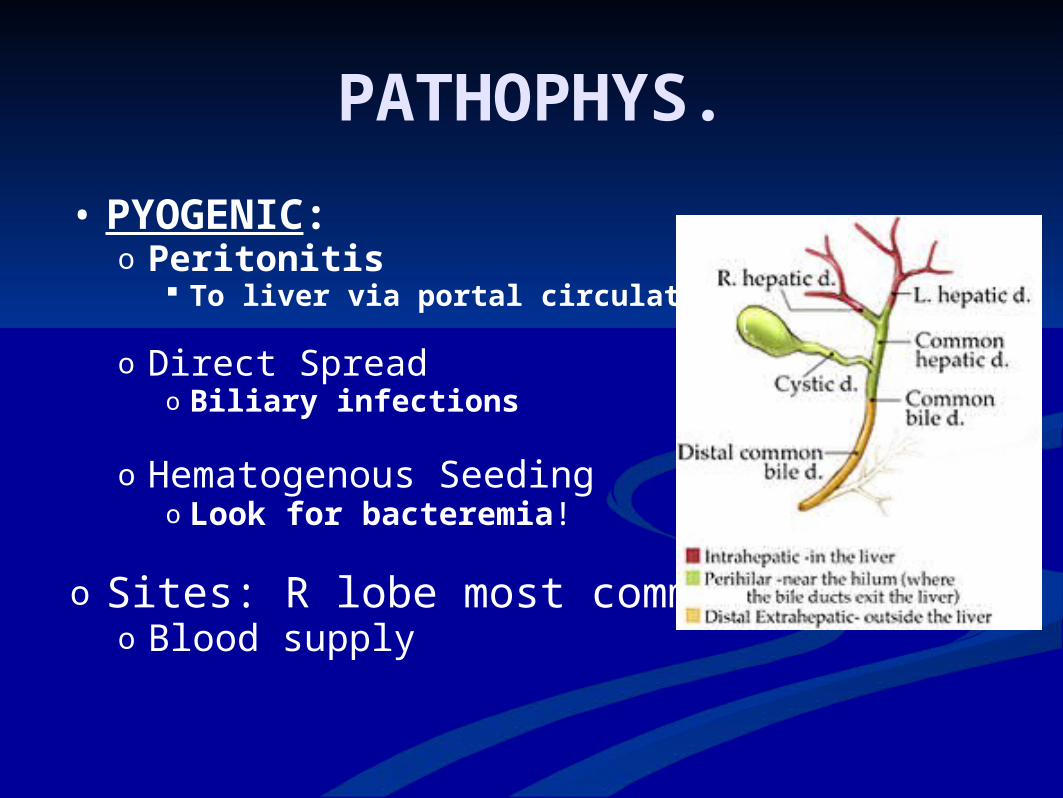
• PYOGENIC:o Peritonitis
To liver via portal circulation
o Direct Spreado Biliary infections
o Hematogenous Seedingo Look for bacteremia!
o Sites: R lobe most commono Blood supply
PATHOPHYS.
• ENTAMOEBA:o Fecal-Oral transmission into GI Tract
To liver via portal circulation
o Can also spread to other extraintestinal siteso Hearto Braino Lungs
CLINICAL MANIFESTATIONS
o SYMPTOMSo Fever (90%)o RUQ pain (50-75%)o Constitutional Sxo Diarrhea (<30%)
o SIGNSo Hepatomegaly (50%)o RUQ tendernesso Jaundiceo Acute abdomen
(<7%)
WORKUP• CBC (leukocytosis)
• LFTs • AlkPhos elevated (67-90%)• AST/ALT elevated (50%)• TBili elevated (50%)
• Blood Cultures• Bacteremia (50%)• E Histolytica Ab• Echinococcus Ab
• Imaging- US, CT, MRI• Can not differentiate types of abscess
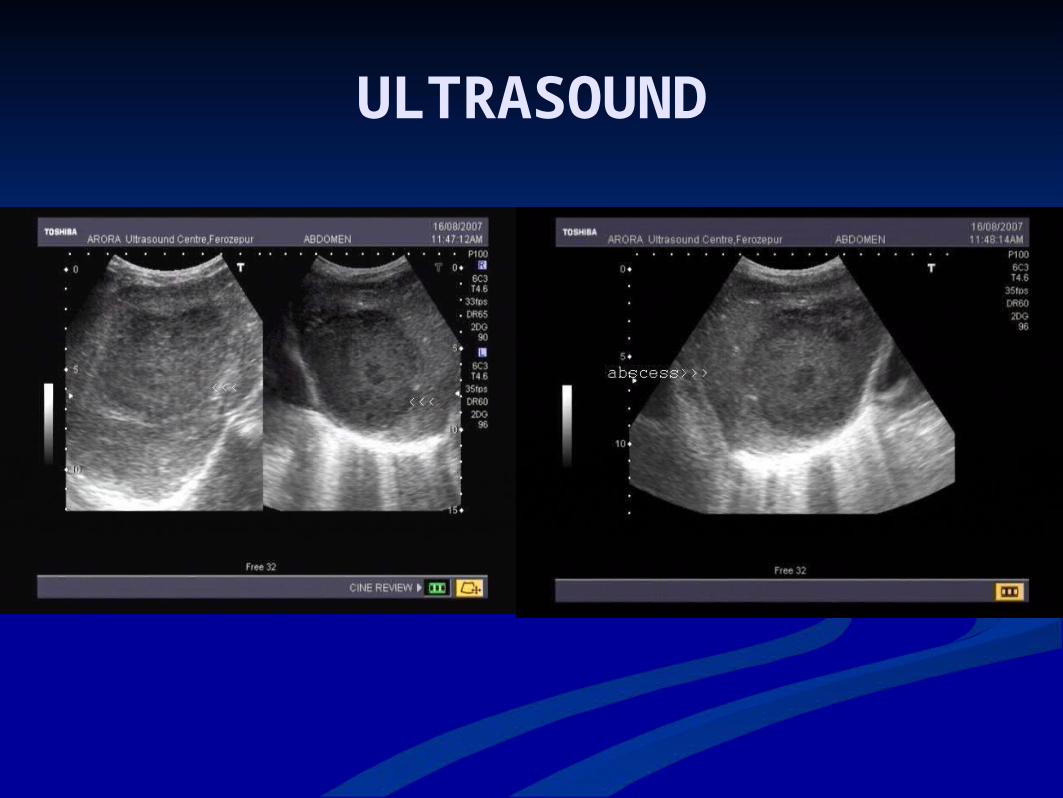
ULTRASOUND
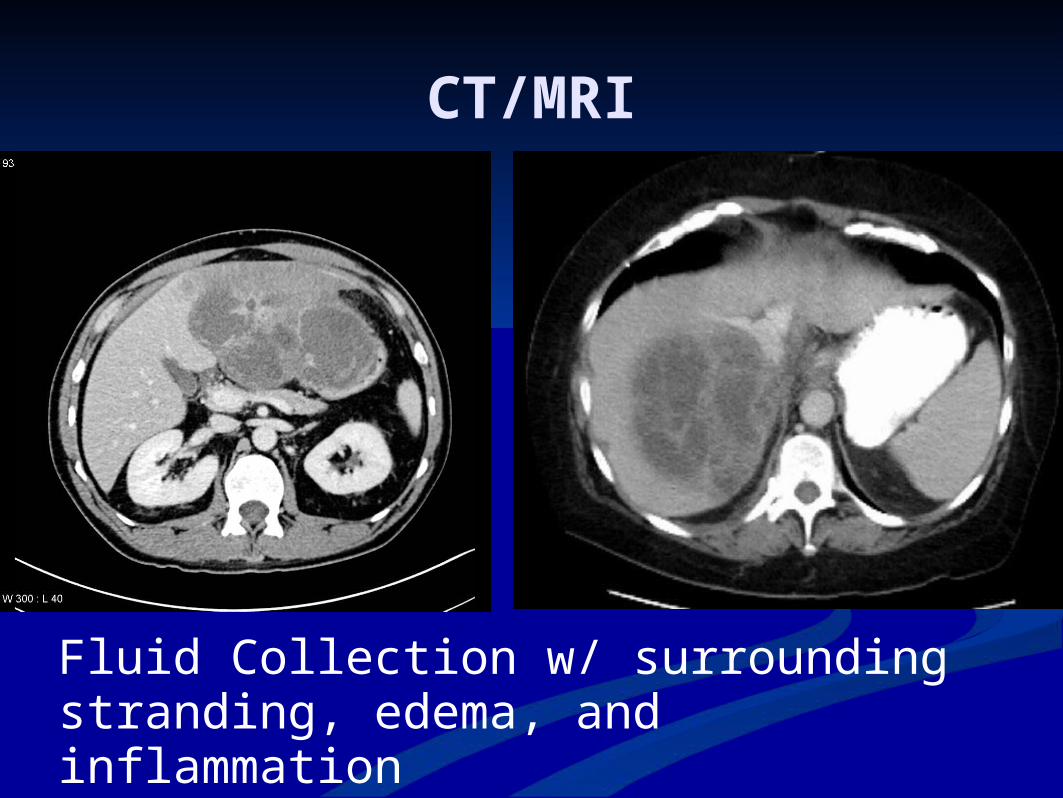
CT/MRI
Fluid Collection w/ surrounding stranding, edema, and inflammation
DIAGNOSTIC PROCEDURE
***IMAGING-GUIDED DRAINAGE***
***SEND FOR CULTURE***
WHAT MAY GROW…• POLYMICROBIAL (including anaerobes)• GRAM NEGATIVES (think gut bugs)• E. Histolytica
• Money is in the serum Ab (95%)• Less yield with wet-mount of abscess or fecal microscopy
(<20%)
• OTHERS• Strep Milleri group• S Aureus (chemoembo) • S Pyogenes (chemoembo)• Candida (s/p chemo)• Klebsiella• TB• Burkholderia
TREATMENT
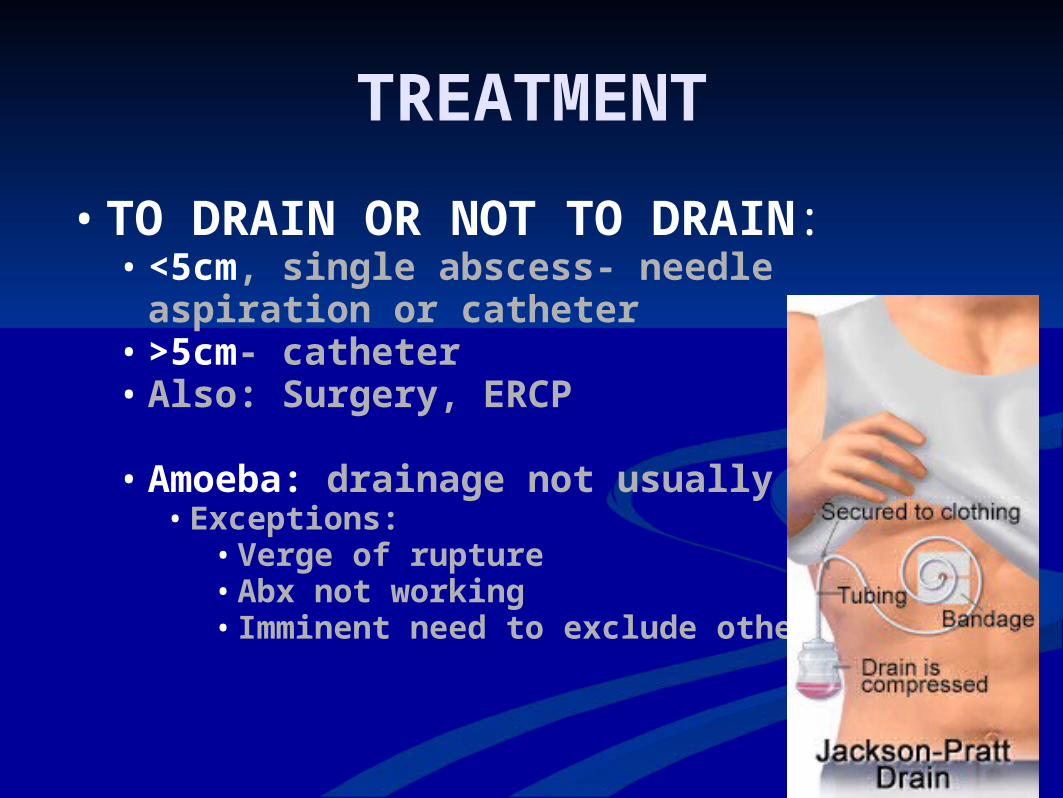
• TO DRAIN OR NOT TO DRAIN:• <5cm, single abscess- needle aspiration or catheter• >5cm- catheter• Also: Surgery, ERCP
• Amoeba: drainage not usually required• Exceptions:
• Verge of rupture• Abx not working• Imminent need to exclude other dx
TREATMENT-ABX
• Pyogenic: Gram Neg + Anaerobe cov.• Unasyn• Zosyn• 3rd gen Ceph (Rocephin) + Flagyl• PCN Allergy: FQ + Flagyl, Carbapenem
• Course: 4-6 weeks• IV duration depends on f/u imaging• Suitable PO Abx: Augmentin OR FQ + Flagyl
• Amoeba: Flagyl 500-750mg TID 7-10days• Then follow with lumenal antiamebic
• Usually Paromomycin TID 10d
PROGNOSIS & NATURAL HISTORY
• Mortality 2-12%• Often due to comorbidities, not necessarily
abscess itself
TAKE HOME MESSAGE
• Think Pyogenic (usually gram neg/anaerobe) or E.Histolytica
• Broad Spectrum Abx at first• Image Image Image• Imaging-Guided Culture +/- JP Drain• Treat for 4-6 weeks
• MIAMI > FLORIDA STATE
REFERENCESeMedicine
Current 2007
UpToDate
Suki