lisinopril versus atenolol in the treatment of patients with mild-to-moderate essential hypertension
TRANSCRIPT
CURRENT THERAPEUTIC RESEARCH VOL. 55, NO. 9, SEPTEMBER 1994
LISINOPRIL VERSUS ATENOLOL IN THE TREATMENT OF PATIENTS WITH MILD-TO-MODERATE
ESSENTIAL HYPERTENSION
L O U I S E. L A P L A N T E F O R T H E C A N A D I A N P R I N I V I L - A T E N O L O L S T U D Y G R O U P
Montreal, Quebec, Canada
A B S T R A C T
The efficacy and safety of lisinopril and atenolol in the treatment of patients with mild-to-moderate hypertension were compared in a mul- ticenter study. Nineteen investigators in Canada participated in this double-blind, placebo-controlled, randomized, parallel study. Follow- ing a 4-week placebo period, eligible patients were randomized to ac- tive treatment for 16 weeks. A total of 176 patients were screened; 90 patients received lisinopril and 83 patients received atenolol, I patient was lost to follow-up, and 2 were excluded because no treatment value were available. Drug dosages were titrated according to blood pressure response. The results of this study show that lisinopril and atenolol both significantly reduced systolic and diastolic blood pressures in both the supine and standing positions. The degree of reduction in systolic and diastolic blood pressures obtained with lisinopril and atenolol were similar to one another. The overall incidence of clinical and laboratory adverse effects was also similar in both groups.
I N T R O D U C T I O N
Hypertension can be classified, according to its severity, as mild, moderate, or severe. Mild-to-moderate cases represent about 80% of all patients with hypertension. 1 In the past, t rea tment of hypertension was determined ac- cording to the severity of the problem and followed a form of therapy known as the "stepped-care" approach. 2 According to this method of treat- ment, patients with the less severe form of hypertension received a diuretic and/or beta-blocker. When the disease was more severe, any one of a num- ber of vasodilator agents was added to the diuretic and/or beta-blocker treatment. With the advent of new drugs such as calcium channel blockers and angiotensin-converting enzyme (ACE) inhibitors, this stepped-care approach was abandoned in favor of more individualized treatment, where clinical and epidemiologic data as well as the presence of target organ involvement would justify the use of one drug over another. 3
Beta-blockers and ACE inhibitors are two types of drugs used in the t rea tment of patients with mild-to-moderate hypertension, either as mono-
Address correspondence to: Dr. Louis E. Laplante, HSpital Maisonneuve-Rosemont, 5415 blvd. L'Assomp- tion, Montreal, Quebec, Canada H1T 2M4. Received for publication on May 16, 1994. Printed in the U.S.A. Reproduction in whole or part is not permitted.
1027 0011-393x/94/$3.50
LISINOPRIL VERSUS ATENOLOL IN ESSENTIAL HYPERTENSION
therapy or in combination with other drugs. Atenolol is a cardioselective beta-blocker that is widely prescribed for the treatment of patients with hypertension. It can be administered once or twice daily. Lisinopril* is a long-acting ACE inhibitor given once daily for the treatment of hyperten- sive patients. The objective of this paper is to report the results of a double- blind, placebo-controlled, randomized, multicenter study comparing these two drugs in the treatment of patients with mild-to-moderate essential hypertension.
P A T I E N T S AND M E T H O D S
Nineteen Canadian investigators screened a total of 176 men and women between the ages of legal consent and 76 years in this double-blind, pla- cebo-controlled, randomized, parallel study of lisinopril versus atenolol. Informed consent was obtained from all patients in accordance with the Declaration of Helsinki.
The study was conducted either in private office settings or in outpa- tient hospital facilities. Newly diagnosed and previously treated ambula- tory patients of either sex who had mild-to-moderate hypertension were included.
Patients were excluded from the study for the following conditions: no response to ACE inhibitors or beta-blockers; secondary hypertension of any etiology; severe, complicated, or malignant hypertension; treatment with nonsteroidal anti-inflammatory drugs (NSAIDs) on a non-constant regimen; myocardial infarction or uncontrolled angina within the past 6 months; treatment with beta-blockers or digitalis post-infarct or for an- gina; congestive heart failure; hemodynamically significant valvular heart disease; atrial-ventricular (A-V) conduction defect (second- or third-degree block); cerebrovascular accident, transient ischemic attack, episode of hy- pertension, or encephalopathy in the past year; confirmed evidence of ac- tive renal disease: aspartate aminotransferase (AST) or alanine ami- notransferase (ALT) levels 100% above the normal range; total serum bilirubin >26 ~mol/L; alkaline phosphatase concentrations 30% above normal; or clinically significant gastrointestinal disorders. Patients receiv- ing drugs in any of the following categories were also excluded: adrenergic psychotropic drugs including monoamine oxidase inhibitors, appetite sup- pressants, lithium, or vasopressor nasal decongestants. Clinically sig- nificant abnormal values of any of the following laboratory parameters were reasons for exclusion: hematocrit, hemoglobin, white blood cells, platelets, and serum potassium levels <3.4 or >5 mmol/L. Severe concur- rent disease such as a neoplasm or collagen disease; poor compliance or mental disability; hypersensitivity to ACE inhibitors or beta-blockers; pa-
* Trademark: Prinivil ® (Merck & Co., Inc./Merck Frosst Canada Inc., R.U., Kirkland, Quebec, Canada).
1028
L.E. LAPLANTE
t ients in whom the use of lisinopril or atenolol was contraindicated; pa- t ients with chronic skin rash or recurrent dermatosis; women of childbear- ing potential; patients at risk during the placebo washout period; patients with a hear t rate below 60 beats/min; patients at risk of hypoglycemia, including patients with non-insul in-dependent diabetes mellitus and un- stable insulin-dependent diabetes mellitus; or any other condition or ther- apy that might pose a risk to the patient or confound the results of this study were also excluded.
Eligible patients entered a 4-week placebo period during which time they took one lisinopril placebo tablet and one atenolol placebo tablet once daily in the morning. After 2 weeks of placebo therapy, any patient whose supine diastolic blood pressure was t>110 mm Hg and ~<115 mm Hg was randomized to study t rea tment immediately. Patients who did not meet this criteria continued to receive placebo for an additional 2 weeks. After 4 weeks of placebo therapy, those patients who had a supine diastolic blood pressure i>95 mm Hg and ~<115 mm Hg then entered the double-blind t rea tment period.
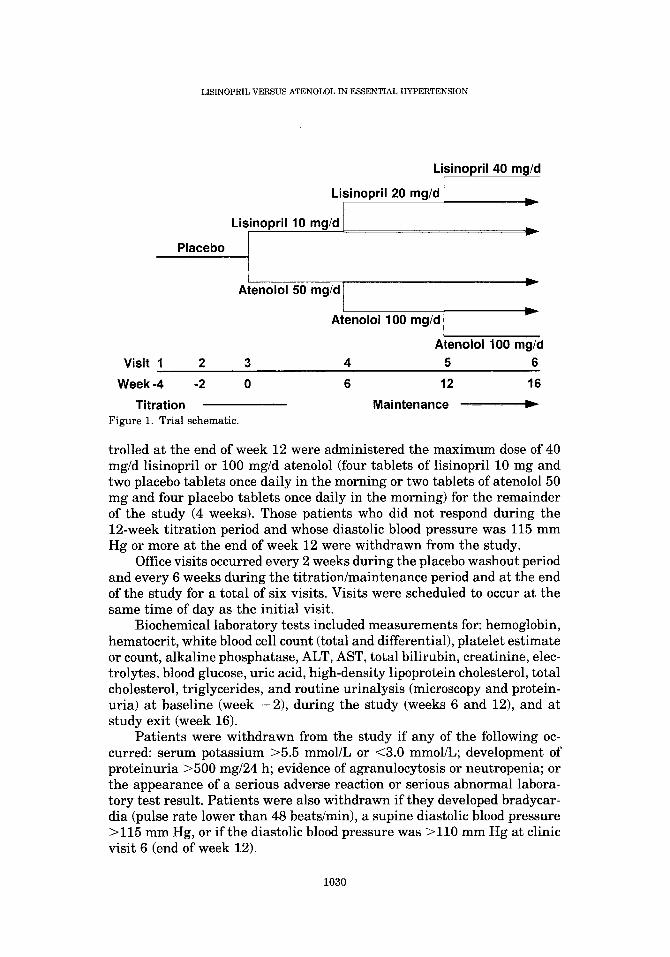
The active t rea tment period, depending on patient response, consisted of a 6- or 12-week t i trat ion period followed by a maintenance period of 4 to 10 weeks. At the beginning of the titration period, patients were randomly assigned to t rea tment with either lisinopril 10-mg tablets or atenolol 50- mg tablets once daily in the morning. At the same time, patients took placebo tablets that matched the comparative agent in appearance. There were three dose levels available in the lisinopril group (10 mg/d, 20 mg/d, and 40 mg/d) and two dose levels in the atenolol group (50 mg/d and 100 mg/d). The maximum daily doses for lisinopril and atenolol were 40 mg and 100 mg, respectively (Figure 1).
For the first 6 weeks of the titration period, patients took one tablet of active medication (lisinopril 10 mg/d or atenolol 50 mg/d) and one tablet of placebo once daily in the morning. Those patients whose blood pressure was controlled at the end of that time (end of week 6) entered the main- tenance period and continued with one tablet of active medication and one tablet of placebo daily for 10 more weeks. Satisfactory blood pressure con- trol was considered to be a supine diastolic blood pressure ~<90 mm Hg.
Those patients whose blood pressure was not controlled at the end of week 6 were then t i t ra ted to 20 mg/d lisinopril or 100 mg/d atenolol (two tablets of lisinopril 10 mg and two placebo tablets once daily in the morn- ing or two tablets of atenolol 50 mg and two placebo tablets once daily in the morning) and returned for a blood pressure measurement after an additional 6 weeks of therapy (end of week 12). Pat ients whose blood pres- sure was controlled (~<90 mm Hg supine diastolic) at the end of week 12 entered the maintenance period and continued to receive 20 mg/d lisinopril or 100 mg/d atenolol once daily in the morning for the remainder of the study (4 weeks). Those patients whose blood pressure was still not con-
1 0 2 9
LISINOPRIL VERSUS ATENOLOL IN ESSENTIAL HYPERTENSION
Visit 1 2
Placebo
Lisinopril 40 mg/d
Lisinopril 20 mg/d I
Lisinopril 10 mg/d I h =
Atenolol 50 mg/d ...
Atenolol 100 mg/d
Atenolol 100 mg/d 3 4 5 6
Week-4 -2 0 6 12 16
Titration Maintenance Figure 1. Trial schematic.
trolled at the end of week 12 were administered the maximum dose of 40 mg/d lisinopril or 100 mg/d atenolol (four tablets of lisinopril 10 mg and two placebo tablets once daily in the morning or two tablets of atenolol 50 mg and four placebo tablets once daily in the morning) for the remainder of the study (4 weeks). Those patients who did not respond during the 12-week ti tration period and whose diastolic blood pressure was 115 mm Hg or more at the end of week 12 were withdrawn from the study.
Office visits occurred every 2 weeks during the placebo washout period and every 6 weeks during the ti tration/maintenance period and at the end of the study for a total of six visits. Visits were scheduled to occur at the same time of day as the initial visit.
Biochemical laboratory tests included measurements for: hemoglobin, hematocrit, white blood cell count (total and differential), platelet estimate or count, alkaline phosphatase, ALT, AST, total bilirubin, creatinine, elec- trolytes, blood glucose, uric acid, high-density lipoprotein cholesterol, total cholesterol, triglycerides, and routine urinalysis (microscopy and protein- uria) at baseline (week -2 ) , during the study (weeks 6 and 12), and at s tudy exit (week 16).
Pat ients were withdrawn from the study if any of the following oc- curred: serum potassium >5.5 mmol/L or <3.0 mmol/L; development of proteinuria >500 mg/24 h; evidence of agranulocytosis or neutropenia; or the appearance of a serious adverse reaction or serious abnormal labora- tory test result. Pat ients were also withdrawn if they developed bradycar- dia (pulse rate lower than 48 beats/min), a supine diastolic blood pressure >115 mm Hg, or if the diastolic blood pressure was >110 mm Hg at clinic visit 6 (end of week 12).
1030
L.E. LAPLANTE
Statistical Analysis
The primary efficacy analysis was performed using the all-patients- t reated approach and included all patients with efficacy data at both base- line and while receiving treatment. Baseline values were defined as the values at visit 3 (week 0) and exit values were defined as the values at visit 6 (week 16). If da ta were missing at week 0 or 16, the last available observations were carried forward and used for the analyses. Pat ient char- acteristics were compared using the Fisher's exact test (for dichotomous variables) or the Wilcoxon test (for ordered variables). Treatment compa- rabili ty of the efficacy variables at baseline was assessed using an analysis of variance (ANOVA) on the ranked values. Within-treatment compari- sons were made using the Wilcoxon signed-rank test; between-treatment comparisons were made using an ANOVA on the ranks of the percent changes from baseline. Categories of blood pressure responses were ana- lyzed using the Fisher's exact test or the Wilcoxon test for categorical variables (in the presence of more than two categories).
Safety analyses were based on the clinical and laboratory adverse experiences, and on laboratory measures. Treatments were compared with respect to the number of patients with an adverse experience after the beginning of the t rea tment period using the Fisher's exact test. Within- t rea tment comparisons of continuous clinical and laboratory measure- ments were made using the Wilcoxon signed-rank test; between-treatment comparisons were made using an ANOVA on the ranks of the absolute changes from baseline.
All statistical comparisons of t reatments were two-sided tests and were declared significant when the observed probability was below ~ = 5%. A lower significance level (~ = 0.25%) was used for the laboratory measurements to compensate for the large number of tests.
RESULTS
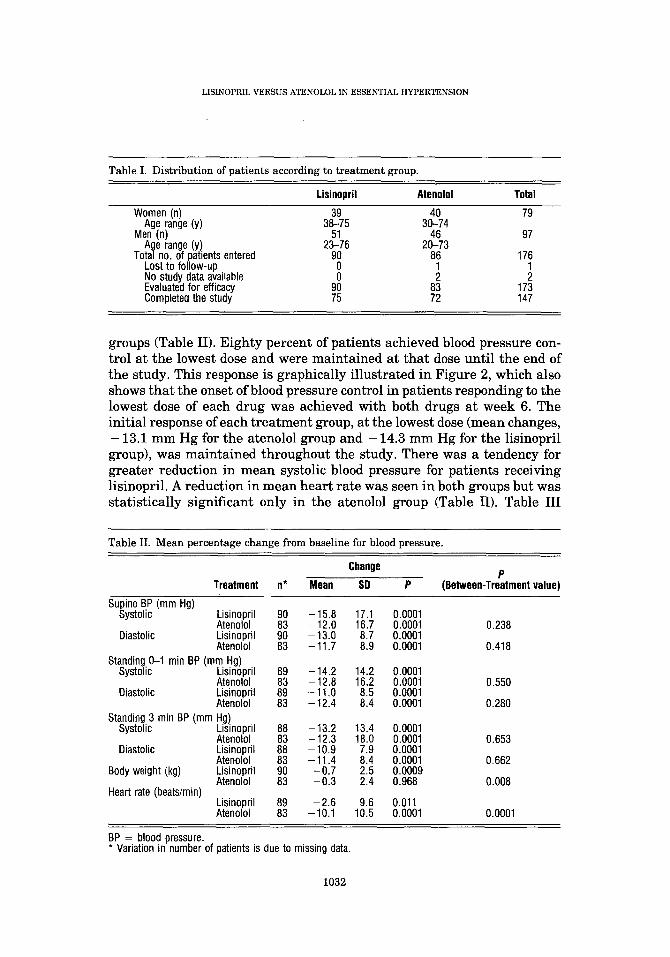
A total of 176 patients (79 women and 97 men) were entered in the study. Of these, 1 was lost to follow-up, 2 were excluded because no t rea tment values were available, 173 were evaluated for efficacy, and 147 completed the study according to the protocol. The distribution of these patients, grouped by treatment , is shown in Table I. Pat ients in both t rea tment groups demonstrated similar characteristics for age, sex, and race (97% white; 3% nonwhite). Fifty-four patients in each t rea tment group had pre- viously received t rea tment for their elevated blood pressure.
Both lisinopril and atenolol significantly reduced systolic and diastolic blood pressures in the supine and standing positions (P = 0.0001). Blood pressure reduction was highly significant at the lowest dose (P = 0.0001). The degree of reduction in blood pressure was similar in patients t reated with either medication (P > 0.05), and there was no difference between
1031
LISINOPRIL VERSUS ATENOLOL IN ESSENTIAL HYPERTENSION
Table I. Distribution of patients according to treatment group.
Lisinopril Atenolol Total
Women (n) 39 40 79 Age range (y) 38-75 30-74
Men (n) 51 46 97 Age range (y) 23-76 20-73
Total no. of patients entered 90 86 176 Lost to follow-up 0 1 1 No study data available 0 2 2 Evaluated for efficacy 90 83 173 Completed the study 75 72 147
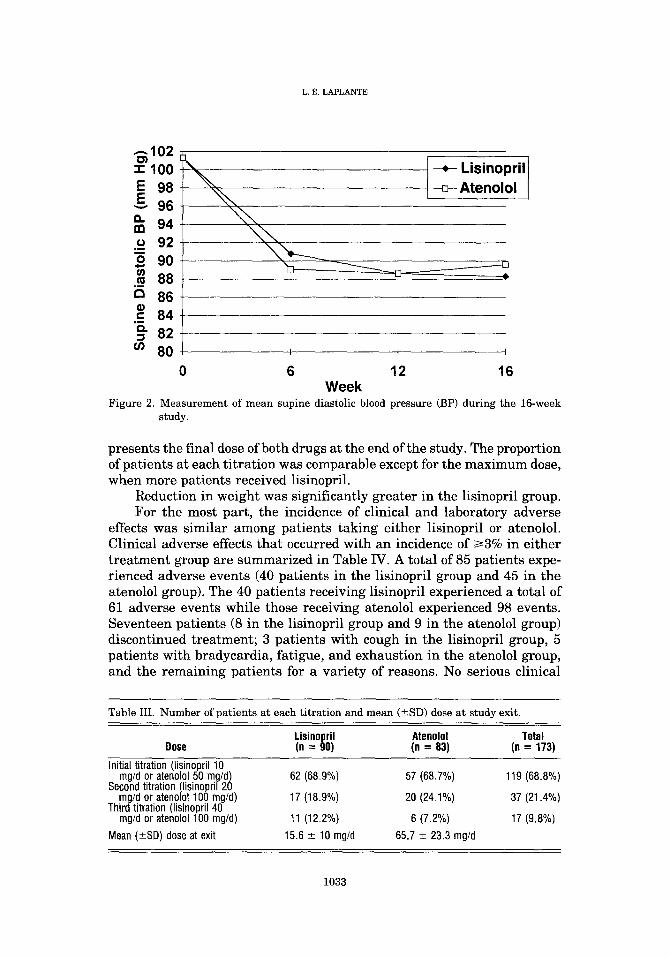
groups (Table II). Eighty percent of patients achieved blood pressure con- trol at the lowest dose and were maintained at that dose until the end of the study. This response is graphically il lustrated in Figure 2, which also shows that the onset of blood pressure control in patients responding to the lowest dose of each drug was achieved with both drugs at week 6. The initial response of each t rea tment group, at the lowest dose (mean changes, - 13.1 mm Hg for the atenolol group and - 14.3 mm Hg for the lisinopril group), was maintained throughout the study. There was a tendency for greater reduction in mean systolic blood pressure for patients receiving lisinopril. A reduction in mean heart rate was seen in both groups but was statistically significant only in the atenolol group (Table II). Table III
Table II. Mean percentage change from baseline for blood pressure.
Change P
Treatment n* Mean SD P (Between-Treatment value)
Supine BP (mm Hg) Systolic Lisinopril 90 - 15.8 17.1 0.0001
Atenolol 83 -12.0 16.7 0.0001 0.238 Diastolic Lisinopril 90 - 13.0 8.7 0.0001
Atenolol 83 - 11.7 8.9 0.0001 0.418 Standing 0-1 rain BP (ram Hg)
Systolic Lisinopril 89 -14.2 14.2 0.0001 Atenolol 83 -12.8 16.2 0.0001 0.550
Diastolic Lisinopril 89 - 11.0 8.5 0.0001 Atenolol 83 - 12.4 8.4 0.0001 0.280
Standing 3 rain BP (ram Hg) Systolic Lisinopril 88 - 13.2 13.4 0.0001
Atenolol 83 -12.3 18.0 0.0001 0.653 Diastolic Lisinopril 88 - 10.9 7.9 0.0001
Atenolol 83 - 11.4 8.4 0.0001 0.662 Body weight (kg) Lisinopril 90 -0 .7 2.5 0.0009
Atenolol 83 - 0.3 2.4 0.968 0.008 Heart rate (beats/min)
Lisinopril 89 - 2.6 9.6 0.011 Atenolol 83 -10.1 10.5 0.0001 0.0001
BP = blood pressure. * Variation in number of patients is due to missing data.
1032
L.E. LAPLANTE
. - -102 ~ 1 0 0
98 96 94
o 92 o 90 u)
88 c~ 86 o~ ," 84 Q. := 82
u) 80
- * - Lisinopri l
Atenolol
I I I
0 6 12 16 Week
Figure 2. Measurement of mean supine diastolic blood pressure (BP) during the 16-week study.
presents the final dose of both drugs at the end of the study. The proportion of patients at each titration was comparable except for the maximum dose, when more patients received lisinopril.
Reduction in weight was significantly greater in the lisinopril group. For the most part, the incidence of clinical and laboratory adverse
effects was similar among patients taking either lisinopril or atenolol. Clinical adverse effects that occurred with an incidence of/>3% in either treatment group are summarized in Table IV. A total of 85 patients expe- rienced adverse events (40 patients in the lisinopril group and 45 in the atenolol group). The 40 patients receiving lisinopril experienced a total of 61 adverse events while those receiving atenolol experienced 98 events. Seventeen patients (8 in the lisinopril group and 9 in the atenolol group) discontinued treatment; 3 patients with cough in the lisinopril group, 5 patients with bradycardia, fatigue, and exhaustion in the atenolol group, and the remaining patients for a variety of reasons. No serious clinical
Table III. Number of patients at each titration and mean (-+SD) dose at study exit.
Lisinopril Atenolol Total Dose (n = 90) (n = 83) (n = 173)
Initial titration (lisinopril 10 mg/d or atenolol 50 rng/d)
Second titration (lisinopril 20 mg/d or atenolol 100 rag/d)
Third titration (lisinopril 40 mg/d or atenolol 100 mg/d)
Mean (+_SD) dose at exit
62 (68.9%) 57 (68.7%) 119 (68.8%)
17 (18.9%) 20 (24.1%) 37 (21.4%)
11 (12.2%) 6 (7.2%) 17 (9.8%)
15.6 --¢- 10 rng/d 65.7 +- 23.3 mg/d
1033

LISINOPRIL VERSUS ATENOLOL IN ESSENTIAL HYPERTENSION
Table IV. Clinical and laboratory adverse effects occurring with an incidence of 3% or more in either t rea tment group.
Lisinopril Atenolol
Headache 10.0% 9.3% Cough 5.6% 3.5% Dizziness 4.4% 7.0% Upper respiratory infections 3.3% 0.0% Cholesterol increased 3.3% 0.0% Cold 0.0% 3.5% Edema 0.0% 5.8% Nausea 0.0% 4.7% Bradycardia 0.0% 3.5% Fatigue 0.0% 5.8%
adverse effects were reported. As for laboratory adverse effects, only one serious adverse effect was reported in the atenolol group; a patient discon- t inued t rea tment because of an elevated ALT level that the investigator concluded was probably not related to the t rea tment drug (elevated ALT level was preexisting but unknown prior to randomization). An increase in cholesterol levels was observed in three patients (3.3%) in the lisinopril group; this side effect was observed in only one patient (1.2%) in the aten- olol group.
DISCUSSION
The approach to the t rea tment of patients with hypertension has under- gone fundamental changes during the last 10 years. In the first hal f of the 1980s, the therapeutic approach to hypertension was one of stepped-care therapy. 2 Diuretics and beta-blockers were the cornerstone of the thera- peutic arsenal for the t rea tment of patients with mild-to-moderate essen- tial hypertension. Vasodilators were then added, as required, in cases of more severe and resistant high blood pressure. With the advent of new families of antihypertensive agents, such as the calcium channel blockers and ACE inhibitors, different pharmacologic mechanisms for blood pres- sure control became available. Moreover, substantial evidence accumu- lated tha t some ant ihypertensive agents (such as diuretics and beta- blockers) have major clinical and metabolic effects 4 that could negate the benefits associated with controlling blood pressure. With a wider choice of therapy, the emphasis is now on a more individualized approach to the management of hypertension, 5 where clinical, epidemiologic, and patho- physiologic factors are more useful in determining the selection of therapy. Sex, age, race, and the presence of a target organ pathology or associated complication are all relevant in this process. The conservation of quality- of-life characteristics are also now taken into account more routinely when a physician is assessing a hypertensive patient. 6'7
Atenolol is a cardioselective, long-acting beta-blocker tha t has been
1034

L.E. LAPLANTE
used extensively in the t rea tment of hypertensive patients over the last 15 years, s Lisinopril, which was introduced more recently, is a long-acting ACE inhibitor that is now advocated in the t rea tment of hypertension.
Antihypertensive drug efficacy of one drug over another is sometimes difficult to compare in the control of mild-to-moderate high blood pressure. Indeed, antihypertensive drugs routinely produce similar significant re- ductions in blood pressure in patients with this condition. Since this ther- apy is chronic, the relative incidence of side effects and impact on quality of life thus become important factors in determining the best drug for each patient. Other considerations, such as risk factors for cardiovascular dis- eases, are also influential in the selection of pharmacologic therapy. In this Canadian mult icenter study, the overall efficacy of lisinopril and atenolol in controlling patients' mild-to-moderate elevations of blood pressure was similar. Other studies have demonstrated a greater decrease in systolic blood pressure in patients t reated with lisinopril than with atenolol; an increase in arterial compliance may explain this observation. 9
In this study, the incidence of most side effects reported for both drugs was similar. Such results were also reported in studies that compared lisinopril with atenolol, or other long-acting ACE inhibitors with cardio- selective beta-blockers. 1°-12 Other comparative clinical studies demon- strated tha t lisinopril had no detrimental effect on left ventricular systolic or diastolic performance while atenolol decreased both systolic and dia- stolic parameters of ventricular performance. 13 Although we observed a nonsignificant increase in cholesterol levels in three patients taking lis- inopril, it has already been extensively shown tha t lisinopril does not affect lipid profiles. 14-~6 There was a greater incidence of bradycardia and fatigue experienced by patients receiving atenolol than lisinopril. These side effects are typical of beta-blockers. 19 The clinical and laboratory side effect events reported for both drugs in this study were similar to those reported in the li terature. 17
CONCLUSIONS
The results of this study indicate that: lisinopril and atenolol significantly reduced systolic and diastolic blood pressures in both the supine and stand- ing positions; the reduction in systolic and diastolic blood pressures ob- tained with lisinopril and atenolol are similar to one another; in patients treated with atenolol and lisinopril, the overall incidence of clinical or laboratory adverse effects is similar, and because there was a statistically significant difference in hear t rate in favor of lisinopril, it may be a pre- ferred agent for the t rea tment of physically active hypertensive patients.
Lisinopril and atenolol when administered for 16 weeks at doses of 10 to 40 mg and 50 to 100 mg, respectively, demonstrated comparable efficacy
1035
LISINOPRIL VERSUS ATENOLOL IN ESSENTIAL HYPERTENSION
in the control of high blood pressure in a sample of Canadian patients with mild-to-moderate essential hypertension. The side-effect profile for both drugs was, for the most part, comparable and no unexpected adverse ex- periences were encountered. As already suggested in the medical litera- ture, both drugs could be given together in the treatment of essential hypertension. Is
Acknowledgments
The following are members of the Canadian Prinivil-Atenolol Study Group: Carl E. Abbott, MD, FRCPC, Halifax, Nova Scotia; Marie-H~l~ne Abboud, MD, CCFP, Hull, Quebec; Laurent B~langer, MD, Longueil, Que- bec; Ellen D. Burgess, MD, FACP, FRCPC, Calgary, Alberta; Matthew Burnstein, MD, Halifax, Nova Scotia; Pierre Cartier, MD, FRCPC, Mon- treal, Quebec; Louise Corneille, MD, Laval, Quebec; Pierre Croteau, MD, Sherbrooke, Quebec; David W. Irving, MD, FACP, FACC, FCCP, FRCPC, Edmonton, Alberta; Peter Jacyk, M.Sc., MD, Toronto, Ontario; Zaheerali Lakhani, MB, MRCP, ABIM, FACC, FRCPC, Edmonton, Alberta; Louis E. Laplante, MD, FRCPC, Montreal, Quebec; Jean R. Shapiro, MD, FRCPC, Vancouver, British Columbia; Chantale Turcotte, MD, Montreal, Quebec; Marvin Waxman, MD, CCFP, Toronto, Ontario; Michael Weinstock, MD, Toronto, Ontario; Ren6 V. Weir, MD, Victoria, British Columbia; Thomas Wilson, MD, FRCPC, Saskatoon, Saskatchewan; and George Zajac, MD, CCFP, Toronto, Ontario, Canada.
References:
1. The Hypertension Detection and Follow-up Program Cooperative Group: A progress re- port. Circ Res. 1977;40(Suppl 1):106-112.
2. Joint National Committee. 1984 Report of the Joint National Committee on the detec- tion, evaluation and treatment of high blood pressure. Arch Intern Med. 1984;144:1045- 1057.
3. Houston MC. New insights and approaches to reduce end-organ damage in the treatment of hypertension: Subsets of hypertension approach. A m Heart J. 1992;23:1337-1367.
4. The MRFIT Research Group. Multiple Risk Factor Intervention Trial. Risk factor changes and mortality results. JAMA. 1982;248:1465-1477.
5. Poulter NR. From stepped care to tailored therapy. J H u m Hypertens. 1991;5(Suppl 2):17-22.
6. Grimm RH, Neaton JD, McDonald M, et al. Beneficial effects from systematic dosage reduction of the diuretic chlorthalidone; a randomized study within a clinical trial. A m Heart J. 1985;109:856-864.
7. Croog SH, Levine S, Testa MA, et al. The effect of antihypertensive therapy on the quality of life. NEJM. 1986;314:1657-1664.
1036
L.E. LAPLANTE
8. Wadworth AN, Murdoch D, Brogden RN. Atenolol. A reappraisal of its pharmacological properties and therapeutic use in cardiovascular disorders. Drugs. 1991;42:468-510.
9. Pannier BE, Garabedian VG, Madonna O, et al. Lisinopril versus atenolol: Decrease in systolic versus diastolic blood pressure with converting enzyme inhibition. Cardiovasc Drugs Ther. 1991;5:775-782.
10. Frimodt-Moeller J, Loldrup Poulsen D, Kornerup HJ, Bech P. Quality of life, side effects and efficacy of lisinopril compared with metoprolol in patients with mild to moderate essential hypertension. J Hum Hypertens. 1991;5(Suppl 2):215-221.
11. The Canadian Enalapril Study Group. Comparison of monotherapy with enalapril and atenolol in mild to moderate hypertension. Can Med Assoc J. 1987;137:803-808.
12. Beevers DG, Blackwood RA, Garnham S, et al. Comparison of lisinopril versus atenolol for mild to moderate essential hypertension. Am J Cardiol. 1991;67:59-62.
13. Zusman RM, Christensen DM, Higgins J, Boucher CA. Comparison of the cardiac and hemodynamic effects oflisinopril and atenotol in patients with hypertension: Therapeutic implications. J Cardiovasc P harmacol. 1992;20:216-222.
14. Shionoiri H, Shin-Ichiro V, Gotoh E, et al. Glucose and lipid metabolism during long-term lisinopril therapy in hypertensive patients. J Cardiovasc Pharmacol. 1990;16:905-909.
15. Cameron HA, Higgins J. Clinical experience with lisinopril. Observations on safety and tolerability. J Hum Hypertens. 1989;3:177-186.
16. Williams LL, Lopez LM, Thorman AD, et al. Plasma lipid profiles and antihypertensive agents; effects of lisinopril, enalapril, nitrendipine, hydralozine and hydrochlorothiazide. Drug Intell Clin Pharm. 1988;22:546-550.
17. Thompson M, Droussin AM, Lama PA. The antihypertensive effect and safety of lisino- pril in patients with mild to moderate essential hypertension. A Belgian multicenter study. Acta Cardiol. 1990;XLV:297-309.
18. Swedish Lisinopril Study Group. Lisinopril combined with atenolol in the treatment of hypertension. J Cardiovasc Pharmacol. 1991;18:457-461.
19. McMahon FG. Management of Essential Hypertension: The New Low Dose Era. 2nd ed. Mount Kisco, NY: Futura Publishing Co., 1984:277-338.
1037