l’innovazione dei trattamenti nel carcinoma dell’ovaio · l’innovazione dei trattamenti nel...
TRANSCRIPT

XVIII Congresso Nazionale Cipomo La Gestione della Complessita’ in
Oncologia Lazise 15-17 Maggio 2014
Complessita’ Clinico Professionali e
l’Innovazione dei Trattamenti nel
Carcinoma dell’Ovaio
Domenica Lorusso Gynecologic Oncologic Unit
National Cancer Institute-Milan

FIGO Annual Report Carcinoma of the Ovary: 5-yr Survival Rates

34
36
38
40
42
44
46
% o
f P
atie
nts
Su
rviv
ing F
ive
Ye
ars
Year of Diagnosis
5-year survival rates
1990-1992 42.5%
1993-1995 43.5%
1996-2003 45%

Carbo = carboplatin; cis = cisplatin; CR = complete response; cyclo = cyclophosphamide; gem = gemcitabine; IP = intraperitoneal; IV = intravenous; pac = paclitaxel; PLD = pegylated liposomal doxorubicin; topo = topotecan
The challenge of going beyond carboplatin/paclitaxel: key trials worldwide
Trial n Regimens compared Outcome
GOG-0162 324 Cis + either 24 h or 96 h pac Efficacy similar
AGO-GINECO 1,282 Carbo/pac vs carbo/pac/epirubicin No benefit of a third agent
MITO-1 273 Carbo/pac x6 topo x4 or surveillance No PFS benefit with topo maintenance
GOG-0172 429 IV cis/IV pac vs IP cis/IP pac IP has better efficacy/worse toxicity and QoL
GCIG 887 Carbo/pac vs carbo/pac/epirubicin No benefit of a third agent
AGO-GINECO 1,308 Carbo/pac topo x4 or surveillance No benefit of topo maintenance
GOG-0178 277 Cis/pac pac x3 vs x12 cycles in patients in CR
PFS improved with pac x12 cycles/no OS difference in a selected patient population
GOG-0182 4,312
Carbo/pac vs carbo/pac/gem (2 regimens) vs carbo/pac/topo vs carbo/pac/PLD
No benefit of a third agent
OV16
819 Carbo/pac x8 vs cis/topo x4 carbo/pac x4
Efficacy similar; tolerability better with carbo/pac
AGO-OVAR9 1,742 Carbo/pac vs carbo/pac/gem No benefit of a third agent
1995
2010

Katsumata et al.(JGOG) Lancet 2009 Dose dense weekly paclitaxel
• Epithelial ovarian cancer FIGO stage II-IV (80% Stage III-IV)
• RT< 1 cm: 45%; Clear Cell 10%
RANDOM
Carboplatino AUC 6
Paclitaxel 180 mg/mq
• 637 patients
Carbo AUC 6 ogni 21
Paclitaxel 80 mg/mq 1, 8, 15
EVERY 21 DAYS



OVARIAN CANCER TREATMENT: PERSPECTIVES
• INDIVIDUALIZE THERAPY
- TOXICITY CRITERIA
- HYSTOTIPE
- GENETIC OR EPIGENETIC MUTATIONS
• CHRONIC DISEASE
- MAINTENANCE THERAPIES
- ARTIFICIAL PROLONGATION OF PLATINUM FREE INTERVAL

A randomized multicentre phase III study comparing weekly vs every 3 weeks carboplatin plus paclitaxel
in patients with advanced ovarian cancer: MITO-7 (Multicentre Italian Trials in Ovarian cancer) – ENGOT-ov-10
(European Network of Gynaecological Oncological Trial Groups) - GCIG (Gynecologic Cancer Intergroup) trial.
Sandro Pignata1,Giovanni Scambia2, Rossella Lauria3, Francesco Raspagliesi4, Pierluigi Benedetti Panici5,
Gennaro Cormio6, Dionyssios Katsaros7, Roberto Sorio8, Giovanna Cavazzini9, Gabriella Ferrandina10,
Enrico Breda11, Viviana Murgia12, Cosimo Sacco13, Nuria Maria Asensio Sierra 14, Carmela Pisano1,
Vanda Salutari2, Beatrice Weber15, Eric Pujade-Lauraine16, Ciro Gallo17, Francesco Perrone1
on behalf of the MITO-7 Investigators
1 National Cancer Institute – “G.Pascale” Foundation, Napoli, Italy; 2 Catholic University of the Sacred Heart, Rome, Italy;
3 Federico II University, Napoli, Italy; 4 Fondazione IRCCS Istituto Nazionale Tumori, Milano, Italy; 5 "Sapienza" University of Rome, Rome, Italy; 6 University of Bari, Bari, Italy; 7 S. Anna Hospital, University of Torino, Italy;
8 National Cancer Institute CRO, Aviano (PN), Italy; 9 “C.Poma” Hospital, Mantova, Italy; 10 Catholic University of the Sacred Heart, Campobasso, Italy; 11 Fatebenefratelli Hospital, Rome, Italy; 12 Santa Chiara Hospital, Trento, Italy; 13 University Hospital "S. Maria della Misericordia", Udine, Italy;
14 Arcispedale “S. Maria Nuova” IRCCS, Reggio Emilia, Italy; 15 Centre Alexis Vautrin, Vandoeuvre-les-Nancy, France;
16 Hôpitaux Universitaires Paris-Centre, site Hôtel-Dieu, AP-HP, Université Paris Descartes, Paris, France; 17 Second University of Napoli, Napoli, Italy.

0 6 12 18 24 30 36 42 48
Months
0.0
0.2
0.4
0.6
0.8
1.0
Pro
bab
ility
of p
rog
ressio
n-f
ree
su
rviv
al
Patients Events
Median PFS
Months (95% CI)
Every 3-week 403 214 16.5 (14.6 – 20.0)
Weekly 405 196 18.8 (17.1 – 22.0)
Log-rank test p = 0.18
Unadjusted HR: 0.88 (0.72 – 1.06)
Analysis: March 2013, median follow-up 19.9 months
Progression-free survival
Patients at risk
Every 3-week 403 354 217 118 72 38 14 1 -
Weekly 405 346 231 124 71 36 20 9 -
Presented by: S.Pignata

0 6 12 18 24 30 36 42 48
Months
0.0
0.2
0.4
0.6
0.8
1.0
Pro
bab
ility
of su
rviv
al
Patients Events
Median OS
Months (95% CI)
Every 3-week 403 76 47.9 (47.9 – n.a.)
Weekly 405 89 n.a. (36.3 – n.a.)
Log-rank test p = 0.24
Unadjusted HR: 1.20 (0.88 – 1.63)
Overall survival
Patients at risk
Every 3-week 403 380 303 193 120 75 31 5 2
Weekly 405 372 294 190 123 68 32 10 -
Presented by: S.Pignata
Analysis: March 2013, median follow-up 19.9 months

FA
CT
-O T
OI
mea
n s
core
40
50
60
70
80
90
QoL: FACT-O TOI, first 9 weeks
Week 0 1 2 3 4 5 6 7 8 9
Pts (weekly) 308 266 254 237 239 238 218 212 223 177
Pts (q3w) 301 229 208 250 209 195 221 193 177 169
Weekly
Every 3-week
** ** **
*
*
* p<0.05 vs. baseline
** p<0.001 vs. baseline
In all scales, higher values represent better outcome.
All tests are adjusted by performance status, stage, residual disease after surgery, age category, and size of the institution
Treatment:time interaction p<0.0001
Presented by: S.Pignata


Ovarian cancer not one disease
8704 patients from 7 randomised trials
Mackay et al. Int J Gynecol Cancer 2010 Adenoca: adenocarcinoma

Mutations typically associated with ovarian carcinoma subtypes
High-grade serous ovarian cancer
• TP53: encodes a protein that regulates the cell cycle
• BRCA1 and BRCA2: encode proteins that are involved in genome protection
Low-grade
serous
BRAF; KRAS
Mucinous
carcinoma
KRAS
Endometrioid
carcinoma
PTEN (low grade);
TP53; BRCA1/2
Clear cell
carcinoma
PTEN; PIK3CA;
ARID1A
Other
subtypes
Romero I et al. Endocrinology 2012;153:1593–1602
TP53, tumour protein 53

mEOC
A multicentre randomised factorial trial
comparing oxaliplatin + capecitabine,
bevacizumab and carboplatin + paclitaxel in
patients with previously untreated mucinous
Epithelial Ovarian Cancer (mEOC)
Cancer Research UK & UCL Cancer Trials Centre
mEOC is an intergroup study with two identical protocols from GOG and NCRI with a single analysis

GCIG Study
RA
ND
OM
IZA
TIO
N
TC
Paclitaxel 175 mg/m2 (d1)
Carboplatin AUC 6 (d1)
Every 3 wk x 6
CPT-11/CDDP
CPT-11 60 mg/m2 (d1, 8, 15)
Cisplatin 60 mg/m2 (d1)
Every 4 wk x 6
International Cooperative Phase III Study
for Clear Cell Carcinoma
-Clear Cell Ca
-Stage I~IV
326 patients in each arm, 652 total for 4.25 years

Randomization
2:1
Stratification
Platinum-Free Interval:
≤6 months vs. > 6 months
Prior Systemic Tx:
1-2 vs. >2
MEK162
45mg BID
Patients with Recurrent or Persistent Low-grade Serous
Carcinomas of the Ovary, Fallopian Tube or Primary
Peritoneum
Must have received prior platinum-containing therapy,
but no more than 3 prior chemotherapies; unlimited
prior hormonal therapy
N=300
Primary endpoint: PFS (Assumed true HR = 0.60, 7 vs 11.67 months)
Key secondary endpoint: OS
Other secondary: ORR, DOR, DCR, Safety, QOL, TR (predictive markers)
FPI planned: May 2013
Sponsor: Array
ENGOT Model: C
Paclitaxel 80 mg/m² d1,8,
15 q 4 wks, or
PLD 40 mg/m² q 4 wks, or
Topotecan 1,25 mg/m²
d1-5 q 3 wks
18
N = 300

High grade serous Muellerian cancer is a disease of homologous recombination dysfunction
TCGA, Nature 2011; Swisher et al, PNAS 2011 in press; Turner, et al NatRevCancer 2004; Weberpals, et al JCO 2008;
Tan et al, JCO 2008; Mendes-Pereira et al, EMBO Mol. Med. 2009
BRCA1 germline
8%
BRCA2 germline
6% BRCA1 somatic
3% BRCA2 somatic
3%
BRCA1 methyl’n
11%
EMSY ampl 6%
PTEN loss 5% other HRD
7%
CCNE1 amp 15%
MMR germline
2%
other 34%
Other HRD 7%: TP53, RAD51C,
PALB2, RAD50,
MRE11A, BARD1,
CHEK2, BRIP1,
FANCD2, ATR, ATM

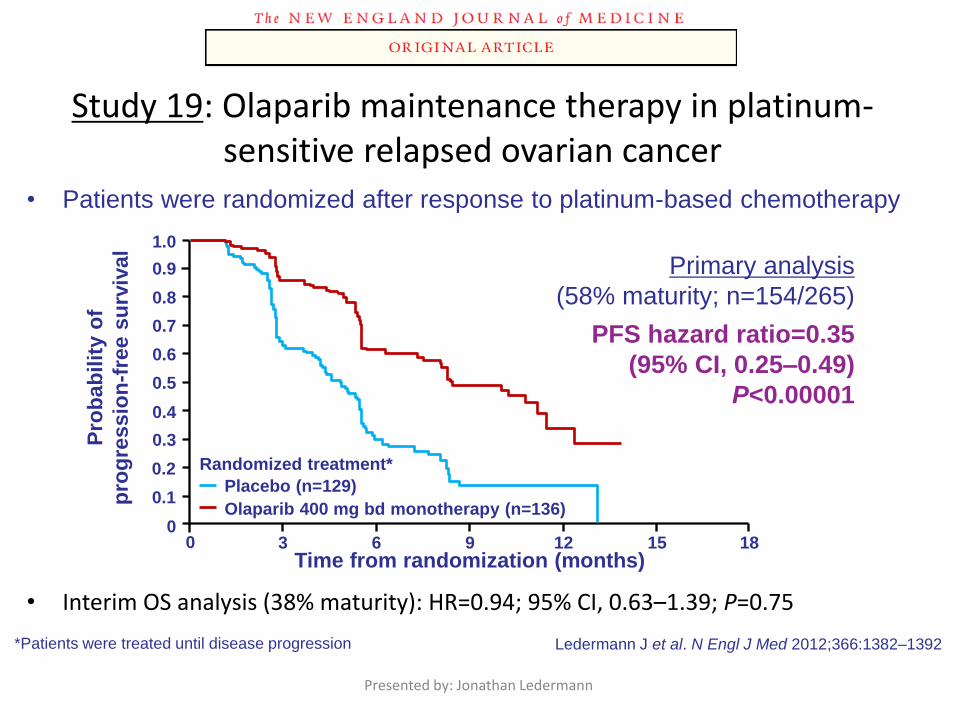
Study 19: Olaparib maintenance therapy in platinum-sensitive relapsed ovarian cancer
• Interim OS analysis (38% maturity): HR=0.94; 95% CI, 0.63–1.39; P=0.75
Presented by: Jonathan Ledermann
0
0.6
0.8
0.9
0
0.1
0.2
0.3
0.4
0.5
0.7
1.0
3 6 9 12 15 18
Pro
ba
bil
ity o
f
pro
gre
ss
ion
-fre
e s
urv
ival
Time from randomization (months)
Primary analysis
(58% maturity; n=154/265)
PFS hazard ratio=0.35
(95% CI, 0.25–0.49)
P<0.00001
Randomized treatment*
Placebo (n=129)
Olaparib 400 mg bd monotherapy (n=136)
Ledermann J et al. N Engl J Med 2012;366:1382–1392 *Patients were treated until disease progression
• Patients were randomized after response to platinum-based chemotherapy

PFS by BRCAm status
Presented by: Jonathan Ledermann
0
Time from randomization (months)
0
1.0
Pro
po
rtio
n o
f p
ati
en
ts
pro
gre
ssio
n-f
ree
3 6 9 12 15
0.9
0.8
0.7
0.6
0.5
0.4
0.3
0.2
0.1
• 82% reduction in risk of disease progression or death with olaparib
Olaparib BRCAm
Placebo BRCAm
Number at risk
Olaparib BRCAm
Placebo BRCAm
74 59 33 14 4 0
62 35 13 2 0 0
BRCAm (n=136)
Olaparib Placebo
Events: total pts (%) 26:74 (35.1) 46:62 (74.2)
Median PFS, months 11.2 4.3
HR=0.18
95% CI (0.11, 0.31);
P<0.00001

Parp inibitori in mantenimento dopo
chemioterapia in pazienti BRCA mutate e
fenotipi BRCAness
• Trial Solo1 Olaparib Prima linea
• Trial Solo2 Olaparib Recidiva platino sensibile
• Trail Tesaro Nova Niraparib Recidiva platino sensibile
• Trail ARIEL 3 Rucaparib Recidiva platino sensibile

The Angiogenic Switch and Antiangiogenic Therapy
Somatic mutation
Small avascular
tumor
Tumor secretion of proangiogenic
factors stimulates angiogenesis
Rapid tumor growth and metastasis
Angiogenic inhibitors may reverse this process

The essential role of VEGF in
ovarian cancer
Moghaddam, et al. Cancer Metastasis Rev 2012

GOG Phase II studies: Response Rates
Tumor Type Dose ORR (PR+CR)
Ovarian Cancer 15mg/kg q3wk 16-21%
Renal Cell 10mg/kg q2wk 10%
Met Breast Cancer 3-20mg/kg q2wk 7%
NHL 10mg/kg q2wk 5%
CRC 10mg/kg q2wk 3%
HRPC 10mg/kg q2wk 0%

Placebo
GOG-0218: Schema
• Stratification variables
– GOG performance status
– Stage/debulking status Bevacizumab 15 mg/kg
15 months
Paclitaxel (P) 175 mg/m2
Carboplatin (C) AUC 6
Carboplatin (C) AUC 6
Paclitaxel (P) 175 mg/m2
Carboplatin (C) AUC 6
Paclitaxel (P) 175 mg/m2
Placebo Front-line: epithelial OV, PP or FT cancer ● Stage III optimal (macroscopic) ● Stage III suboptimal ● Stage IV
N=1873
I
II
III
Arm
1:1:1
OV = ovarian; PP = primary peritoneal FT = fallopian tube; Bev = bevacizumab
R
A
N
D
O
M
I
S
E
(CP)
(CP + Bev)
(CP + Bev Bev)
Bev 15 mg/kg
Burger et al. ASCO 2010

*p value boundary = 0.0116
Data cut-off date: September 29, 2009
GOG 218- Significant PFS improvement, censored for CA-125 events and non-protocol therapy
1.0
0.8
0.6
0.4
0.2
0
0 6 12 18 24 30 36 42 48 PFS (months)
PF
S e
sti
ma
te
CP + Pl Pl
CP + Bev15 Bev15
CP + Pl Pl
(n=625)
CP + Bev15
Bev15
(n=623)
Median PFS (months) 12.0 18.2
Stratified analysis HR
(95% CI)
0.62
(0.52–0.75)
p value one-sided (log rank) <0.0001*
N Engl J Med 365;26,2011

OS benefit is suggested with chemotherapy + Avastin and continued single-agent Avastin in stage IV disease
129 113 95 28 72 42 15 5
142 117 104 30 73 44 15 10
144
149
154 144 130 117 37 83 57 21 10
3
3
3
0
1
0
Time (months)
0 72
1.0
0.8
0.6
0.4
OS
es
tim
ate
12 24 36 48 60
0.2
0.0
CPP
CPB
CPB15
165
165
153
0
0
0
CPP (n=153)
CPB15 (n=165)
CPB15+ (n=165)
CPP CPB CPB15
Deaths, n
(%)
93 (61) 99 (60) 81 (49)
Median
survival
(months)
32.8 32.9 40.6
HR
(95% CI)
0.98
(0.74–1.31)
0.72
(0.53–0.97)
Randall, et al. SGO 2013: Abstract 80 Randall, et al. SGO 2013: Abstract 80

ICON 7 Schema
Stratification variables:
• Stage & extent of debulking (I–III debulked ≤1cm vs I–III debulked >1 cm vs IV and
inoperable stage III)
• Timing of intended treatment start (≤4 vs >4 weeks after surgery)
• GCIG group
Paclitaxel 175 mg/m2
Carboplatin AUC 5 or 6
Carboplatin AUC 5 or 6
Paclitaxel 175 mg/m2
18 cycles (12 months)
R
Bevacizumab 7.5 mg/kg q3w
1:1
OC = epithelial ovarian, primary peritoneal or fallopian tube cancer
• FIGO stage I–IIA
(clear cell or grade 3)
or FIGO stage IIB–IV
• Surgically debulked
histologically
confirmed OC
n=1528
Dec 2006 to Feb 2009
30
Number at risk
Control 254 109 43 24 18 6
Research 248 175 53 32 23 5
1.00
0.75
0.50
0.25
0
Pro
po
rtio
n a
live
with
ou
t p
rog
ressio
n
Time (months)
0 6 12 18 24 30 36 42 48 54 60
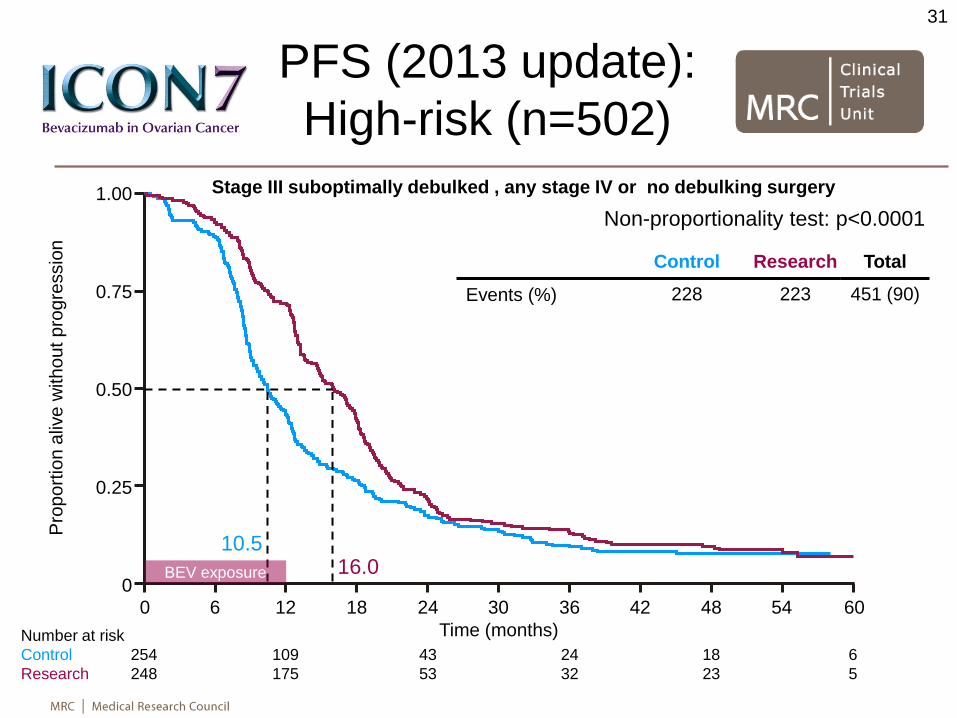
PFS (2013 update):
High-risk (n=502)
Control Research ∆
Events (%) 228 223
Restricted mean, months
15.9 20.0 +4.1
Median, months 10.5 16.0 +5.5
Log-rank test p=0.001
HR (95% CI) 0.73 (0.61–0.88)
Non-proportionality test: p<0.0001
16.0 10.5
31
Stage III suboptimally debulked , any stage IV or no debulking surgery
Total
451 (90)
BEV exposure

Final OS: High-risk
(n=502)
Number at risk
Control 254 208 156 101 82 21
Research 248 224 180 135 95 27
1.00
0.75
0.50
0.25
0
Pro
po
rtio
n a
live
Time (months)
0 6 12 18 24 30 36 42 48 54 60
Control Research ∆
Deaths (%) 174 158 Restricted mean, months
34.5 39.3 +4.8
Median, months 30.3 39.7 +9.4 Log-rank test p=0.03
HR (95% CI) 0.78 (0.63–0.97)
Non-proportionality test:
p=0.0072
Stage III suboptimally debulked , any stage IV or no debulking surgery
39.7 30.3
9.4
32
BEV exposure
Total
332 (66)

Avastin RCP Dicembre 2011:
Avastin, in combinazione con carboplatino e paclitaxel è indicato per il
trattamento in prima linea del carcinoma ovarico epiteliale, del carcinoma
alle tube di Falloppio o del carcinoma peritoneale primario in stadio
avanzato (stadio III B, III C e IV, secondo la classificazione FIGO).
Avastin è somministrato in aggiunta a carboplatino e a paclitaxel fino a 6 cicli di
trattamento, seguiti dalla somministrazione di Avastin in monoterapia da proseguire
fino alla progressione della malattia o per un massimo di 15 mesi o fino a che non compare
tossicità inaccettabile, qualsiasi si manifesti prima.
La dose raccomandata di Avastin è di 15 mg/kg di peso corporeo, da somministrarsi
una volta ogni 3 settimane mediante infusione endovenosa

‘Boost Trial’

Trial Chemotherapy Bevacizumab PFS HR
First line
GOG-02181 (n=1873)
Paclitaxel Carboplatin
Concurrent and maintenance
15 mg/kg q3w (3-arm placebo)
0.72
ICON72
(n=1528) Paclitaxel
Carboplatin
Concurrently only 7.5 mg/kg q3w
(2 arm) 0.81
Second line
Platinum resistant Aurelia3
(n=361)
Caelyx Topotecan Paclitaxel
Concurrent 10 mg/kg q2w
(2 arm) 0.48
Platinum sensitive OCEANS4
(n=484) Gemcitabine Carboplatin
Concurrent 15 mg/kg q3w
(2 arm) 0.48
Bevacizumab in ovarian cancer: four pivotal trials
1. Burger et al. N Engl J Med 2011
2. Perren et al. N Engl J Med 2011
3. Pujade-Laurain et al. J Clin Oncol 2012
4. Aghajanian et al. J Clin Oncol 2012

Subgroup
Restricted mean Median, months
HR (95% CI) Events/n
Research
better
Control
better Control Research Control Research
All patients 27.7 29.2 17.5 19.9 0.93
(0.83–1.05) 1080/1528
Non-high riska 33.8 33.7 26.0 25.0 1.03
(0.88–1.21) 629/1026
High riskb 15.9 20.0 10.5 16.0 0.73
(0.61–0.88) 451/502
Stage I, II, III (0 cm) 37.9 39.3 45.5 38.8 0.97
(0.79–1.18) 378/725
Stage III >0, ≤1 cm 22.7 21.3 13.7 17.7 1.07
(0.83–1.38) 251/301
Stage III >1 cm 17.0 20.8 11.1 17.0 0.75
(0.59–0.96) 260/290
Stage IV 15.5 19.4 10.2 14.9 0.75
(0.55–1.02) 163/182
Inoperable 10.4 15.8 8.4 12.4 0.58
(0.26–1.29) 28/30
Trend
interaction
p=0.014
Interaction
p=0.005
PFS (2013 update)
36
0.2 0.5 1 2 5
HR (95% CI)
aAll stage I and II, stage III ≤1 cm bNo debulking surgery, stage III >1 cm, any stage IV

DISCREPANCY BETWEEN SURGEON AND POST OPERATIVE CT SCAN EVALUATION IN RESIDUAL
TUMOR DETECTION
Author
No patients % discrepancy Site of failure
Chi D 2007 78 48% Perihepatic region, small bowel peritoneum
Lakhman Y 2011 63 49% Perihepatic Region, Upper abdominal lymphnodes
Lorusso D 2013 (submitted)
64 20.3% Perihepatic region, small bowel peritoneum


AURELIA (GINECO)
Stratification variables:
• Chemotherapy regimen
• Previous anti-angiogenic
therapy
• PFI <3 vs 3–6 months
Chemotherapy
to progression
Chemotherapy
to progression
Bevacizumab 10 mg/kg
q2w* to progression
Platinum-
resistant
OC, PP, FTC,
(PFI <6 months)
Prior
bevacizumab
allowed
n=360
(4/2011)
Primary endpoint:
PFS
Secondary
endpoints:
ORR, PFIbio, OS, QoL,
safety
Chemotherapy options (physician’s choice):
• Weekly paclitaxel 80 mg/m2
• Topotecan (4 mg/m2 d1, 8, 15 OR 1.25
mg/m2 d1–5 q3w)
• Pegylated liposomal doxorubicin 40 mg/m2
d1 q4w *15 mg/kg q3w if combined with topotecan q3w
P R O G R E S S I O N
Physician’s
choice: SOC or
bevacizumab 15
mg/kg q3w
SOC (Optional
bevacizumab)


Paclitaxel cohort: OS O
vera
ll surv
ival (%
)
75
50
25
0 0 6 12 18 24 30 36 42
100
CT
BEV + CT
No. at risk:
55 40 32 22 13 3 0
60 52 43 34 19 4 1
Time (months)
CT (N=55)
BEV + CT (N=60)
Events, n (%) 41 (75) 36 (60)
Median OS, months (95% CI)
13.2 (8.2‒19.7)
22.4 (16.7‒26.7)
HR (unadjusted) (95% CI)
0.65 (0.42‒1.02)

OCEANS, a phase III, multicenter, randomized, blinded, placebo-controlled trial of carboplatin and gemcitabine plus bevacizumab in
patients with platinum-sensitive recurrent ovarian, primary peritoneal, or fallopian tube cancer
CG + PL
CG for 6 (up to 10) cycles Stratification variables:
• Platinum-free interval
(6–12 vs >12 months)
• Cytoreductive surgery for
recurrent disease (yes vs no)
Platinum-sensitive
recurrent OCa
•Measurable disease
•ECOG 0/1
•No prior chemo for
recurrent OC
•No prior BV
(n=484)
G 1000 mg/m2, d1 & 8
C AUC 4
PL q3w until progression
C AUC 4
BV 15 mg/kg q3w until progression
G 1000 mg/m2, d1 & 8
CG + BV

242 177 45 11 3 0 CG + PL
OCEANS: Primary analysis of PFS
CG + PL
(n=242)
CG + BV
(n=242)
Events, n (%) 187 (77) 151 (62)
Median PFS,
months (95% CI)
8.4
(8.3–9.7)
12.4
(11.4–12.7)
Stratified analysis
HR (95% CI)
Log-rank p-value
0.484
(0.388–0.605)
<0.0001
Months No. at risk
242 203 92 33 11 0 CG + BV
1.0
0.8
0.6
0.4
0.2
0
Pro
port
ion p
rogre
ssio
n fre
e
0 6 12 18 24 30

MITO-16/MaNGO OV-2: Avastin plus chemotherapy at progression after front-line Avastin plus chemotherapy in platinum sensitive
Principal investigators: Sandro Pignata, Nicoletta Colombo
Stage IIIB–IV EOC, FT or PPC
progressing or recurring at least
6 months after
front-line chemotherapy
plus Avastin
(n≈400)
• Primary endpoint: PFS
• Secondary endpoint: OS
• 60 Italian centres involved and involvement of others European groups (ENGOT –
Italy, Germany, France, Greece, Switzerland) (sponsor: INT Napoli)
1:1
Avastin15mg/kg q3w
PLD or gemcitabine or paclitaxel
Carboplatin
PLD or gemcitabine or paclitaxel
Carboplatin
x 6
– 8
cycle
s
until PD

Target therapies in Ovarian Cancer
Bevacizumab
Pazopanib
Nintedanib
Trebananib
Cediranib

• Phase III randomized, placebo-controlled, double-blind, multicenter
• N=940 patients randomized (1:1) from June 2009 to August 2010
• Pazopanib administered at 800 mg daily for up to 24 months*
ICF
Survival
follow-up
(post-PD)
First-line
surgery and
chemotherapy
(allowed: dose-
dense, IP,
neoadjuvant)
Placebo
24 months
Pazopanib
24 months
R
A
N
D
O
M
I
Z
E
Observation
(to PD)
Study Design
If not PD
+ tumor
< 2 cm
Median 7 months from diagnosis to randomization
*Original design was for 12 months and later amended to 24 months

Pazopanib trial: 1st Endpoint: Progression-free Survival (RECIST)
(months)
Δ= 5.6 months
Median time from
Diagnosis: 7 months
472 332 234 171 91 19
468 318 208 164 88 20 1
Patients
at risk
0
0,5
1
0 6 12 18 24 30 36
HR = 0.766 (95% CI: 0.643-0.911)
Stratified log-rank test: P = 0.0021
Pazopanib: 472 pts. / 237 events
median 17.9 (15.9 - 21.8) mos
Placebo: 468 pts. / 273 events
median 12.3 (11.8 - 17.7) mos

Adverse Events Grade 3-4 per Patient occurring in at least 1% in the Pazopanib Arm
Grade 3/4 adverse events Placebo (N=461)
Pazopanib (N=477)
Δ
Hypertension 26 (6%) 147 (31%) 121 (25%)
• Hypertension (including Grade 2) 80 (17%) 248 (52%) 168 (35%)
Liver-related toxicity 3 (<1%) 45 (9%) 42 (9%)
Neutropenia 7 (2%) 47 (10%) 40 (8%)
Diarrhea 5 (1%) 39 (8%) 34 (7%)
Asthenia / Fatigue 1 (<1%) 13 (3%) 12 (3%)
Thrombocytopenia 3 (<1%) 12 (3%) 9 (2%)
Palmar-plantar erythrodysesthesia 1 (<1%) 9 (2%) 8 (2%)
Headache 3 (<1%) 8 (2%) 5 (1%)
Abdominal pain 5 (1%) 8 (2%) 3 (<1%)
Proteinuria 2 (<1%) 6 (1%) 4 (<1%)
Arthralgia 3 (<1%) 5 (1%) 2 (<1%)

Drug Exposure: Mean Daily Dose
Patient Daily Dose (mg)
Placebo
(N=461)
Pazopanib
(N=477)
Mean 761.0 585.6
Median 800.0 607.4
Patients with any dose reduction 63 (14%) 277 (58%)
weeks

Multicenter, randomised, double-blind, Phase III trial to investigate the
efficacy and safety of Vargatef (BIBF 1120) in combination with standard
treatment of carboplatin and paclitaxel compared to placebo plus carboplatin
and paclitaxelin patients with advanced ovarian cancer
AGO-OVAR12
R
C
T
C
T
C
T
C
T
C
T
C
T
C
T
C
T
C
T
C
T
C
T
C
T
= Vargatef 2 x 200 mg po qd
= Placebo
120 weeks
C = Carboplatin AUC 5-6 d1
T = Paclitaxel 175 mg/m2 (3h) d1
q21d / 6 courses
Vargatef / Placebo :
- no intake on days of chemotherapy
- dose: 200 mg po bid (combi + mono)
- dose adaptation in case of undue toxicity
- max. duration of 120 weeks in non-progressing pts
2
1
S
U
R
G
E
R
Y
n=1300

Nintedanib: Primary Endpoint:
Progression-Free Survival
RECIST 1.1 and CA-125 in conjunction with Clinical MBO Criteria
0
0,5
1
0 6 12 18 24 30 36 42
Time from randomization (months)
455 381 257 168 76 3 0 0
911 761 542 352 160 17 1 0
TC + Nintedanib
(n=911)
TC + Placebo (n=455)
Events, n (%) 486 (53.3) 266 (58.5)
Median, months 17.3 16.6
HR* (95% CI) 0.84 (0.72, 0.98)
p value 0.0239
All patients (N=1366) – Cut-off date: 29 April 2013
*Stratified for macroscopic residual postoperative tumour, FIGO stage and carboplatin dose

Exploratory Subgroup Analysis
“ICON 7 defined low-risk patients subgroup”
(FIGO II or FIGO III and ≤ 1cm residual postoperative tumor)
Patients at risk
Esti
mat
ed p
erce
nta
ge a
live
a
nd
pro
gres
sio
n-f
ree
Time from randomization (months)
Placebo 283 248 186 123 52 2 0
Nintedanib 556 478 380 270 124 9 0
TC + Nintedanib
(n=556)
TC + Placebo (n=283)
Events, n (%) 234(42.1) 149(52.7)
Median, months 27.1 20.8
HR (95% CI) 0.74 (0.61, 0.91)
0
0,5
1
0 6 12 18 24 30 36 42
median PFS difference: + 6.3 months (similar to OVAR 16)

Nintedanib trial: non-haematological AEs
(>15%), all CTCAE Grades
Placebo + chemo
Nintedanib + chemo

Dose intensity – Drug exposure Placebo + chemo
n (%)
Nintedanib + chemo
n (%)
Chemo dose reductions, number of pts 450 902
any dose reduction of chemotherapy 50 (11.1) 190 (21.1)
Carboplatin and Paclitaxel 6 ( 1.3) 40 ( 4.4)
Carboplatin (regardless of Paclitaxel) 24 ( 5.3) 90 ( 9.9)
Paclitaxel (regardless of Carboplatin) 32 ( 7.1) 140 (15.5)
Chemo courses, number of patients 450 902
mean n courses 5.8 5.5
reaching 6 courses 414 (92.0%) 778 (86.3%)
Nintedanib or placebo, number of pts 445 890
Patients without any dose reductions 407 (91.5) 430 (48.3)
One dose reduction 32 ( 7.2) 297 (33.4)
Two dose reductions 6 ( 1.3) 163 (18.3)

TRINOVA-1
Weekly paclitaxel
AMG-386 IV 15 mg/kg qw to
progression
Recurrent partially platinum sensitive or resistant OC, PP, FTC, (PFI <12 months, >6months after the beginning of the first-line platinum-based chemotherapy) Radiographically evaluable disease, documented PD Prev Chemo <3 Toxicity <G3
n=900 Primary endpoint: PFS
Secondary endpoints: OS, ORR, DOR, CA125 response
rate, safety and tolerbality of AMG386, PK of AMG386
Weekly paclitaxel
Placebo IV qw
to progression
ClinicalTrials.gov. Identifier NCT01204749
12 June 2013
Press release
AMGEN announces PFS benefit of
2 months in favour of trebananib
arm
(HR 0.66)

Progression-free Survival
(Primary Analysis) Pac + Placebo
(n = 458)
Pac + Trebananib
(n = 461)
Events, n (%) 361 (79) 310 (67)
Median PFS, months 5.4 7.2
HR = 0.66 (95% CI, 0.57–0.77)
P (stratified log rank) < 0.001
Presented by Monk BJ at European Cancer Congress
European Journal of Cancer 49; suppl 3, Sept 2013 LBA 41

Treatment-emergent AEs in
≥ 25% of Patients
Patient Incidence, n (%)
Paclitaxel +
Placebo
N = 458
Paclitaxel +
Trebananib
N = 461
All Grades Grade ≥ 3 All Grades Grade ≥ 3
Any 434 (96) 244 (54) 446 (97) 258 (56)
Localized edema 116 (26) 4 (1) 264 (57) 24 (5)
Nausea 171 (38) 6 (1) 187 (41) 8 (2)
Alopecia 163 (36) 2 (<1) 154 (33) 0
Diarrhea 122 (27) 13 (3) 136 (30) 11 (2)
Abdominal pain 131 (29) 21 (5) 132 (29) 22 (5)
Asthenia 119 (26) 15 (3) 129 (28) 13 (3)
Fatigue 137 (30) 17 (4) 127 (28) 15 (3)
Vomiting 101 (22) 12 (3) 122 (26) 14 (3)
Constipation 128 (28) 4 (1) 105 (23) 3 (1)
Neutropenia 125 (28) 40 (9) 99 (21) 26 (6) Presented by Monk BJ at European Cancer Congress
European Journal of Cancer 49; suppl 3, Sept 2013 LBA 41

OV6 TRINOVA-2
Pegylated Liposomal Doxorubicin
50 mg/m² IV Q4W
AMG-386 IV 15 mg/kg qw to
progression
Recurrent partially platinum sensitive or resistant OC, PP, FTC, (PFI <12 months, >6months after the beginning of the first-line platinum-based chemotherapy) Radiographically evaluable disease, documented PD Prev Chemo <3 Toxicity <G3
n=380 Primary endpoint: PFS
Secondary endpoints: OS, ORR, DOR, CA125 response
rate, safety and tolerbality of AMG386, PK of AMG386
Pegylated Liposomal Doxorubicin
50 mg/m² IV Q4W
Placebo IV qw
to progression
ClinicalTrials.gov Identifier: NCT01281254

TRINOVA-3/ENGOT-ov2/ BGOG-ov7
TC ± AMG 386 as first-line therapy of stage III–IV
ovarian cancer
Concurrent treatment Maintenance phase
RA
ND
OM
IZA
TIO
N
ARM A:
AMG 386*
Paclitaxel**
Carboplatin**
ARM B:
AMG 386/Placebo*
Paclitaxel**
Carboplatin**
Paclitaxel 175 mg/m2 IV Q3W
Carboplatin AUC 5 or 6 IV Q3W
for
maximum of 6 cycles
Plus
AMG 386 15 mg/kg IV QW or
AMG 386 placebo IV QW
AMG 386
monotherapy
until progression or
18 months
AMG 386 Placebo
monotherapy
Until progression or
18 months
EN
D O
F T
RE
AT
ME
NT
(P
rog
ress
ive
dis
ea
se
or
un
acc
ep
tab
le t
oxic
ity o
r
wit
hd
raw
al o
f co
nsen
t o
r d
eath
Up to 7 days from
randomization to 1st dose Treatment phase
Neoadjuvant chemo +
Interval Debulking
allowed in both arms
After 3 courses
N = 1000
Randomised double-blind phase III
trial of cediranib (AZD 2171) in
relapsed platinum sensitive ovarian
cancer: Results of the ICON6 trial.
An academic sponsored GCIG trial
Ledermann JA, Perren T, Raja FA, Embleton AC, Rustin GJS,
Jayson G, Kaye SB, Swart AM, Vaughan M, Hirte H
on behalf of the ICON 6 Collaborators
(NCRN, NCIC-CTG, ANZGOG, GEICO)

Dec 2007: Trial opened in seven centres in UK and Canada. Cediranib 30 mg
reduced to 20 mg after 30 patients enrolled
Nov 2009: Completed new Stage I (toxicity phase) recruitment at 20 mg dose.
Stage II (efficacy phase) trial expanded
Sept 2011: AZ ceased development of cediranib.
• Trial size reduced
• PFS instead of OS as primary endpoint
• Trial re-designed without Interim Analysis
• Primary comparison: Arm A (Chemo only) vs. Arm C (Maintenance)
• Secondary: OS and Chemo only vs. Concurrent vs. Maintenance, Toxicity, QoL
• 80% power, at 5% alpha, to detect a HR=0.65 would require 176 PFS events (470
patients)
Dec 2011: Trial closed 486 patients (456 at 20 mg dose)
• 176 PFS events occurred around Q4 2012. Analysis delay until ~5% remained on trial
drug
Chronology and Statistical Design – Summary

0.00
0.25
0.50
0.75
1.00
164 148 65 21 7 118 90 24 8 3
.
0 3 6 9 12 15 18 21 24Months
Chemo. Maint.
Chemotherapy
Maintenance
Restricted mean survival time increases by
3.1 months with maintenance treatment
Chemo. Maint.
PFS events, n (%) 112 (94.9) 139 (84.8)
Median, months 8.7 11.1
Log-rank test p=0.00001
HR (95% CI) 0.57 (0.45 – 0.74)
Test for non-proportionality p=0.024
Restricted means, months 9.4 12.5
CEDIRANIB IN RECURRENT PLATINUM SENSITIVE
OC: Progression-free survival – arms A vs. C

0.00
0.25
0.50
0.75
1.00
164 159 139 89 48 2222 118 106 89 46 27 1111
.
0 6 12 18 24 30Months
Chemo. Maint.
OS events, n (%) 63 (53.3) 75 (45.7)
Median, months 20.3 26.3
Log-rank test p=0.042
HR (95% CI) 0.70 (0.51 – 0.99)
Test for non-proportionality p=0.0042
Restricted means, months 17.6 20.3
Restricted mean survival time increases
by 2.7 months with maintenance
treatment (over two years)
CEDIRANIB IN RECURRENT PLATINUM SENSITIVE
OC : Overall survival
Chemo. Maint.
Chemotherapy
Maintenance

CONCLUSIONS
• Treatment according to histotype is the future
• Angiogenesis is the driving pathway in ovarian cancer carcinogenesis
- 4 positive phase III trials in first line treatment
- 2 positive second line trials in platinum resitant disease
- 3 positive second line trials in platinum sensitive disease
…..The pitfalls:
• NO predictive factors of response
• NO idea which phase of disease
• NO idea what schedule and for how long
• NO idea which type of therapy
• NO clear mechanism of resistance that may conditionate the most appropriate sequence of treatment, if any.
• NO comparison data between drugs
……many trials to do, MANY LESSONS TO LEARN……