linfomas intermedios entre linfoma de hodgkin y linfoma ... · linfomas intermedios entre linfoma...
TRANSCRIPT

Linfomas intermedios entre Linfoma de
Hodgkin y Linfoma Mediastínico de
Célula Grande
Juan F. García
XXVI Congreso Nacional de la SEAP-IAP
CURSO DE PATOLOGÍA LINFOIDE
Linfomas de la zona gris

Classical HL : HRS cells + characteristic reactive microenvironment
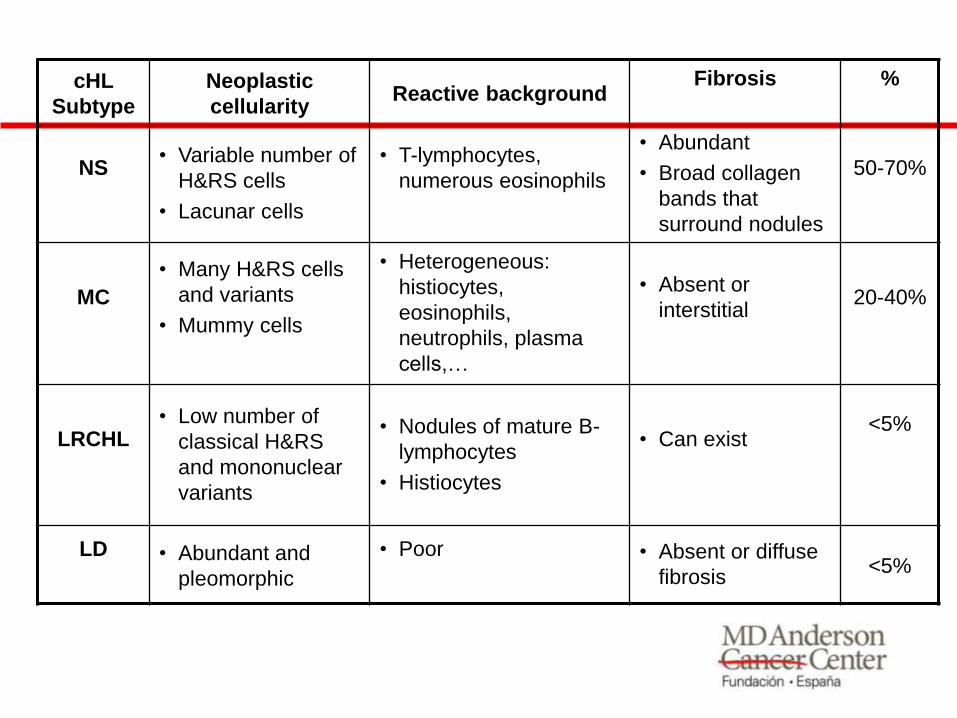
cHL
Subtype
Neoplastic
cellularity Reactive background
Fibrosis
%
NS
• Variable number of
H&RS cells
• Lacunar cells
• T-lymphocytes,
numerous eosinophils
• Abundant
• Broad collagen
bands that
surround nodules
50-70%
MC
• Many H&RS cells
and variants
• Mummy cells
• Heterogeneous:
histiocytes,
eosinophils,
neutrophils, plasma
cells,…
• Absent or
interstitial
20-40%
LRCHL
• Low number of
classical H&RS
and mononuclear
variants
• Nodules of mature B-
lymphocytes
• Histiocytes
• Can exist
<5%
LD
• Abundant and
pleomorphic
• Poor
• Absent or diffuse
fibrosis <5%
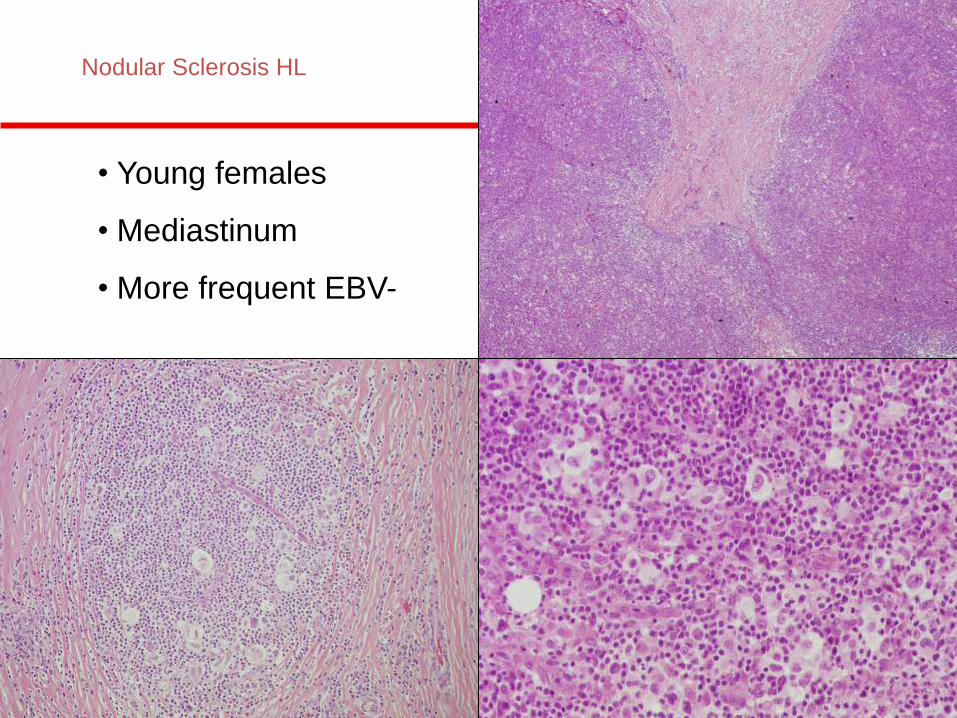
Nodular Sclerosis HL
• Young females
• Mediastinum
• More frequent EBV-
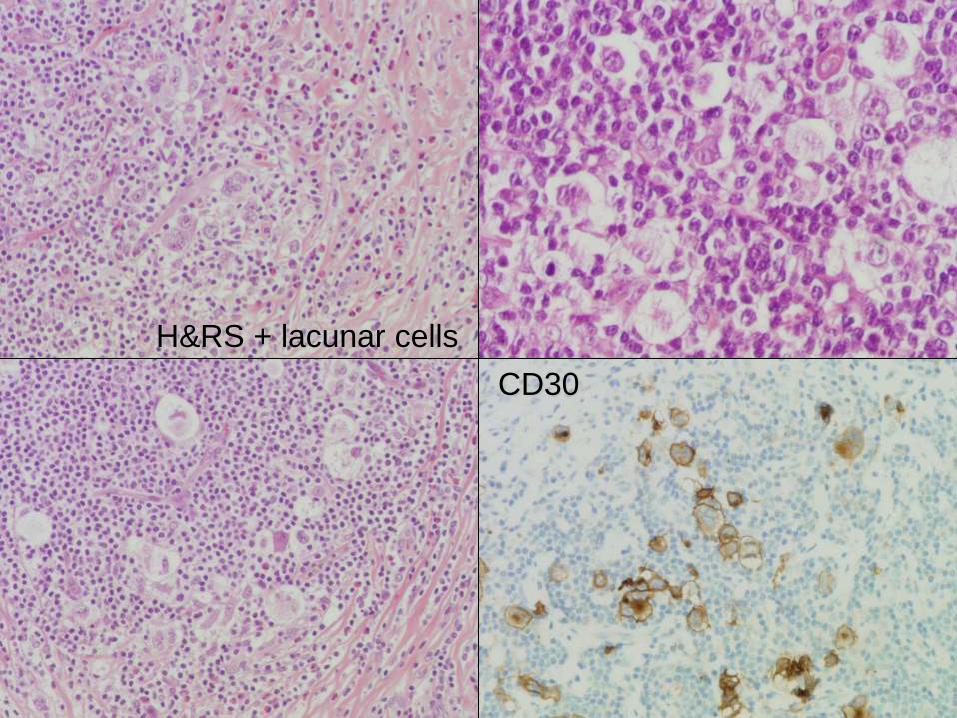
H&RS + lacunar cells
CD30

CD30
> 90%
CD15
70-80%
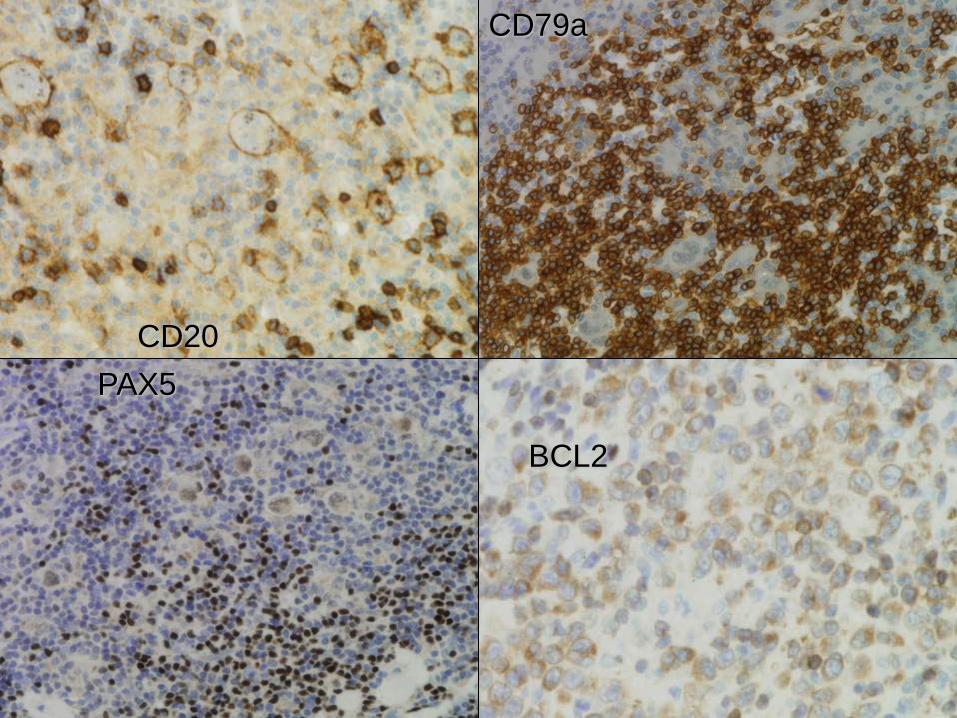
CD20
CD79a
PAX5
BCL2
Diffuse Large B-cell Lymphoma
Morphology: diffuse, with centroblastic, immunoblastic,
plasmablastic, pleomorphic cytology
Immunophenotype: CD20+ CD79a+ OCT2+ Pax5+
Bcl6: 80%
Bcl2: 50-70%.
p53: 10%, poor response to chemotherapy
GC-type: CD10+
ABC: MUM1+
Genotype:
t(14;18) (bcl2-IgH): 20%
t(3q27) (bcl6): 30%
8q24 (c-myc): 10%
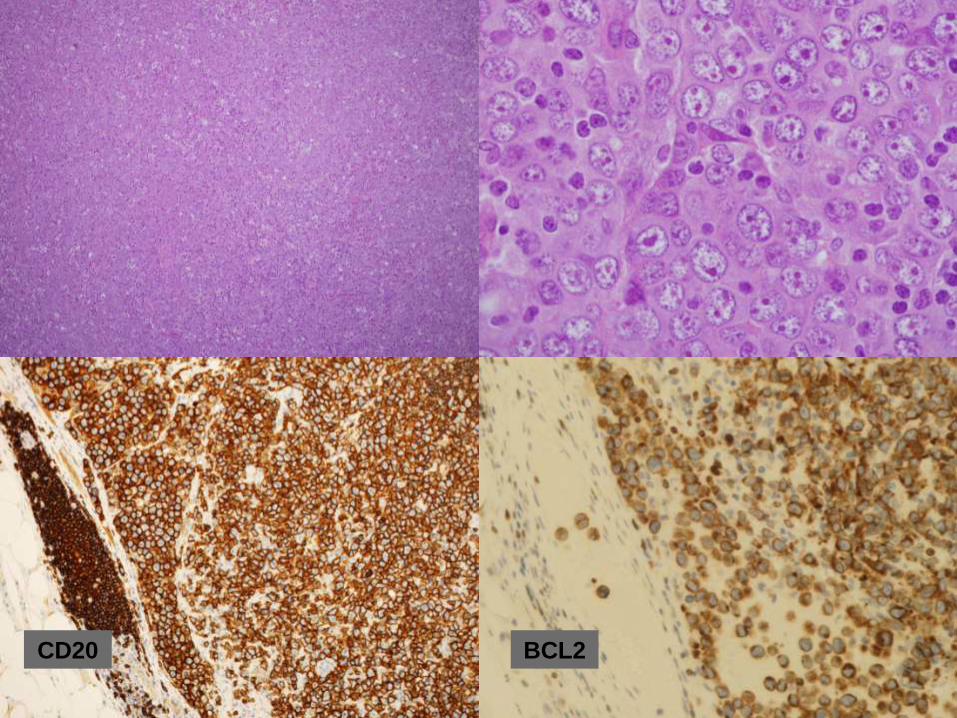
CD20 BCL2
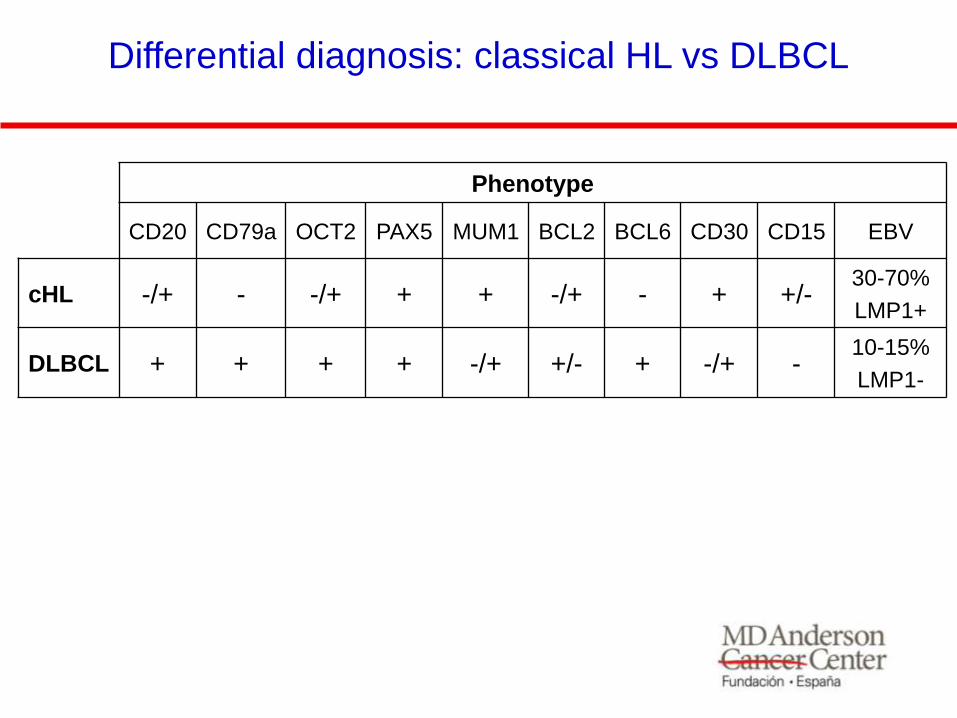
Phenotype
CD20 CD79a OCT2 PAX5 MUM1 BCL2 BCL6 CD30 CD15 EBV
cHL -/+ - -/+ + + -/+ - + +/- 30-70%
LMP1+
DLBCL + + + + -/+ +/- + -/+ - 10-15%
LMP1-
Differential diagnosis: classical HL vs DLBCL

Primary Mediastinal DLBCL
• Young adults (W>M)
• Clinical symptoms, related with the
localization
• Sclerosis surrounding the tumor
cells
• Weak expression of Ig and other B-cell
markers
• HRS-like cells may be present
• Clinical course depending the stage at
diagnosis
• CD23+, CD30+, MAL1+
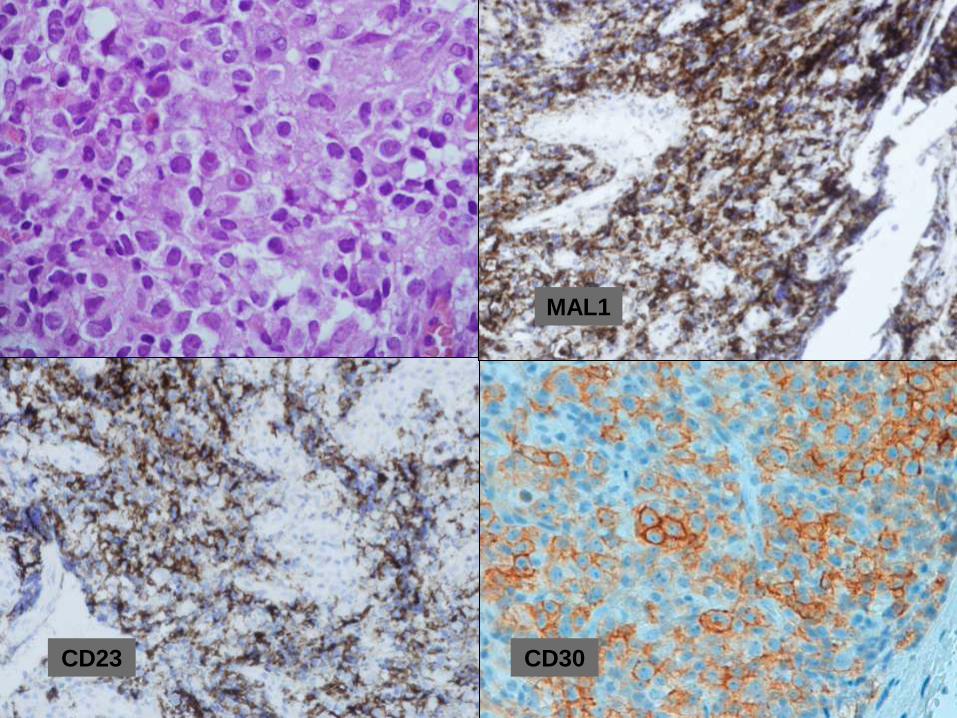
CD23 CD30
MAL1
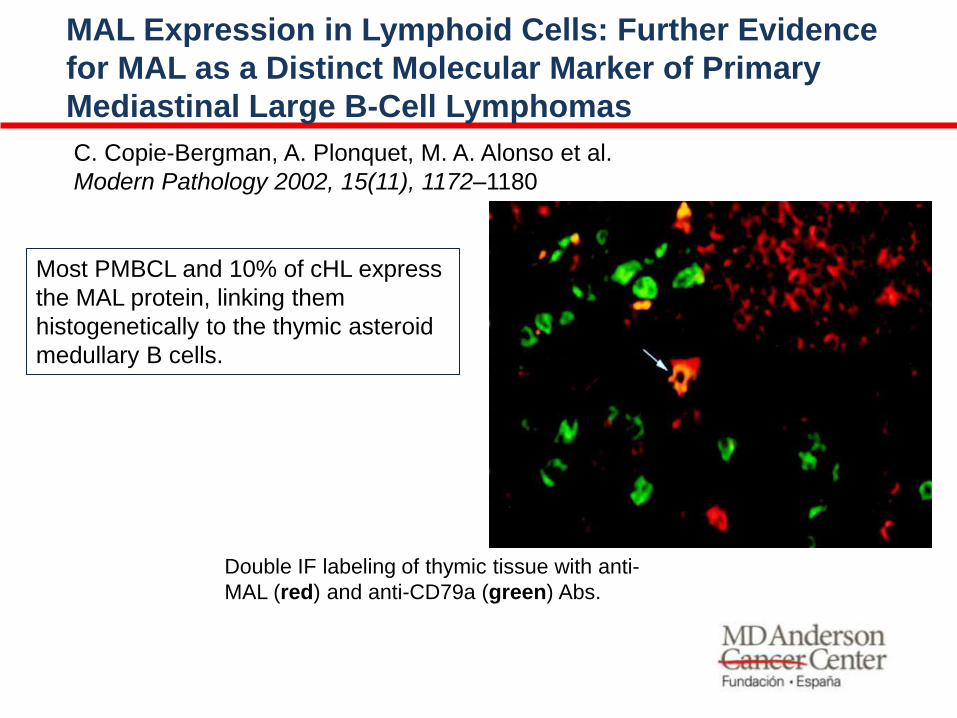
Most PMBCL and 10% of cHL express
the MAL protein, linking them
histogenetically to the thymic asteroid
medullary B cells.
C. Copie-Bergman, A. Plonquet, M. A. Alonso et al.
Modern Pathology 2002, 15(11), 1172–1180
MAL Expression in Lymphoid Cells: Further Evidence
for MAL as a Distinct Molecular Marker of Primary
Mediastinal Large B-Cell Lymphomas
Double IF labeling of thymic tissue with anti-
MAL (red) and anti-CD79a (green) Abs.

Molecular diagnosis of primary mediastinal B cell
lymphoma identifies a clinically favorable subgroup
of diffuse large B cell lymphoma related to Hodgkin
lymphoma.
Rosenwald A, et al. J Exp Med 2003;198(6):851-62.

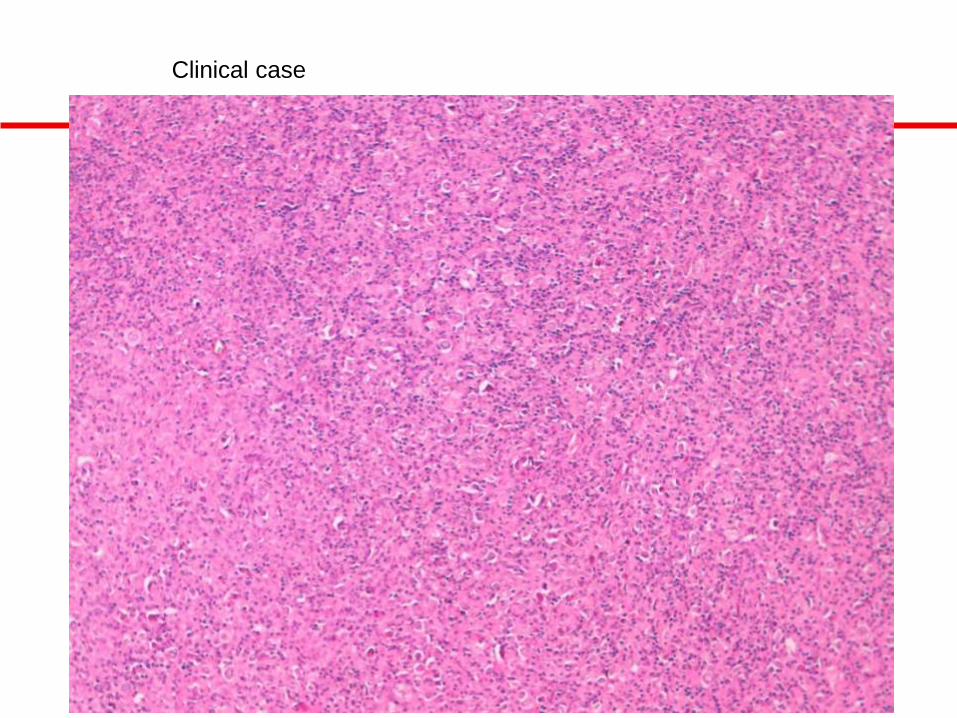
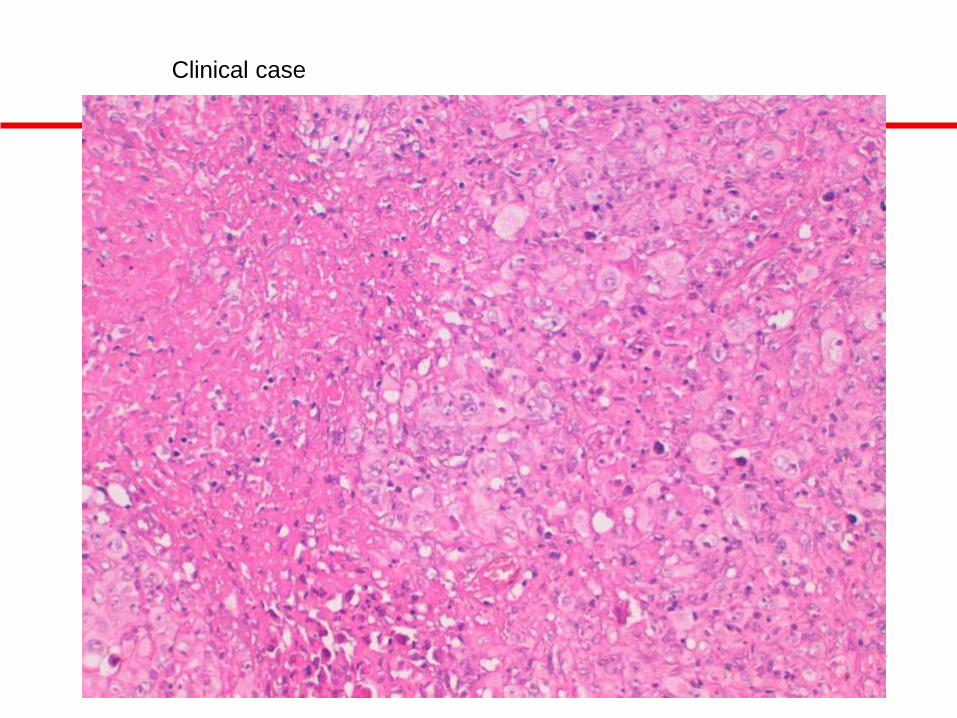
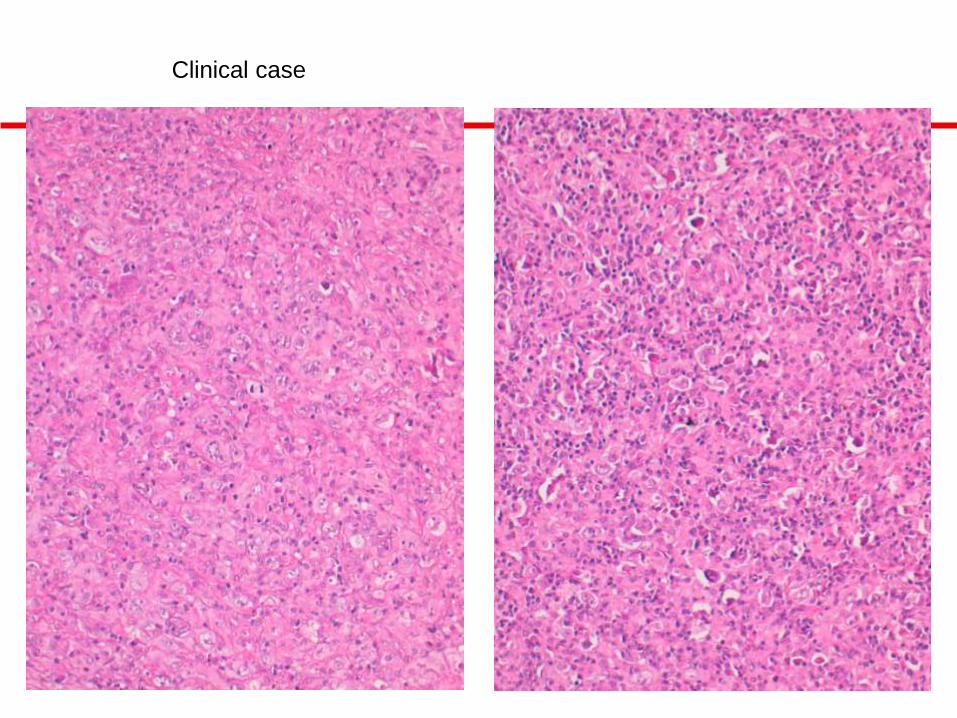
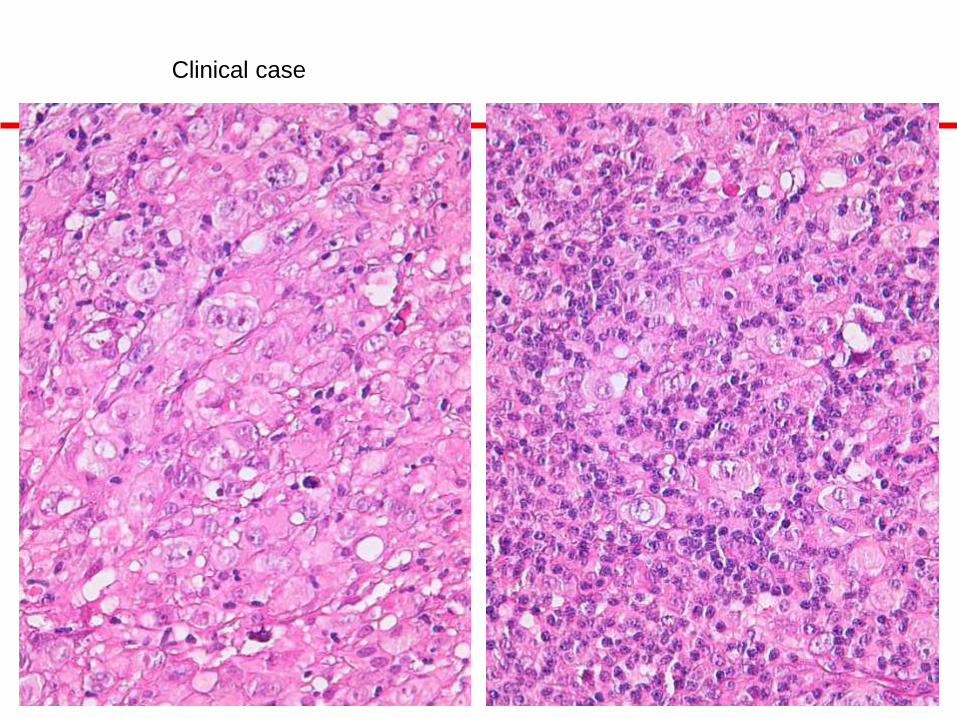
• 47-y old male
• Constitutional syndrome with fever and weight loss (january 2011)
• Mediastinal mass (bulky) and cava syndrome
• FNA: consistent with large-cell lymphoma
• Biopsy (trucut): consistent with Hodgkin lymphoma
• Open biopsy is performed by mediastinoscopy
Clinical case
Clinical case
Clinical case
Clinical case
Clinical case
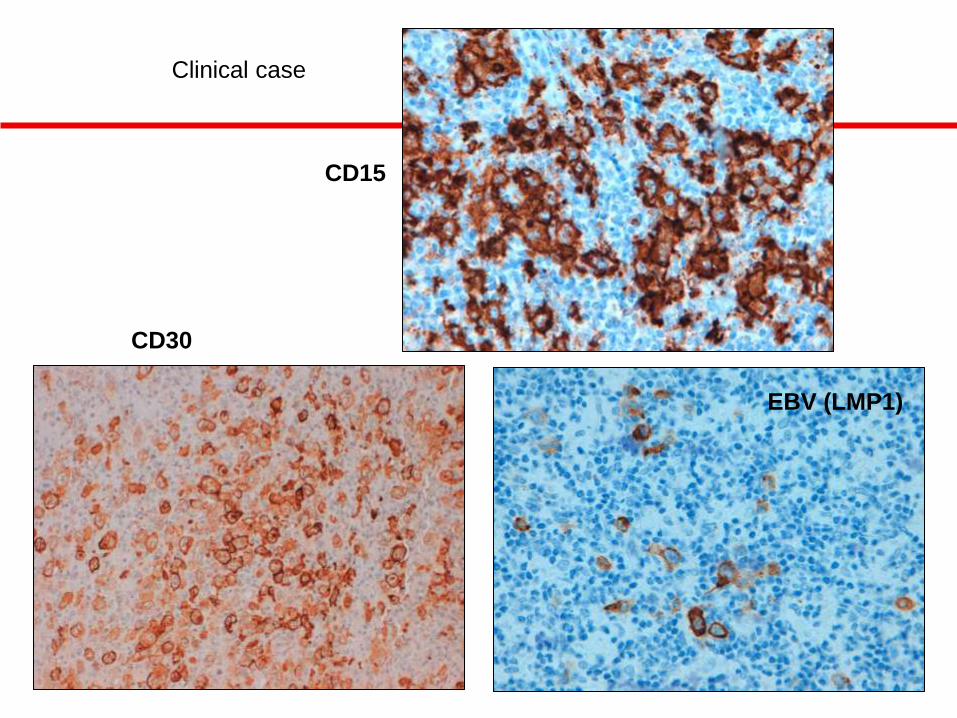
CD15
CD30
EBV (LMP1)
Clinical case

Caso clínico
CD20 CD79a
Clinical case
B-Cell Lymphoma, Unclassifiable, with Features
Intermediate between Diffuse Large B-Cell
Lymphoma and Classical Hodgkin Lymphoma
(BCLu-DLBCL/cHL)
• The patient was treated with intensive chemotherapy:
R-CHOP-21 (x8) + Radiotherapy, with complete
remission
• Follow-up: alive without disease
Clinical case
• Most lymphomas can be accurately classified based on the current
WHO classification of lymphoid neoplasms (clinical information
morphology, immunophenotype, and genetic characteristics).
• Despite technical and scientific progress, some aggressive B-cell
lymphomas with features overlapping between two different types
of lymphomas remain difficult to classify.
• The updated 2008 WHO classification has addressed this problem
by creation of two new provisional categories of B-cell lymphomas,
unclassifiable; one with features intermediate between diffuse large
B-cell lymphoma and classical Hodgkin lymphoma and the second
with features intermediate between diffuse large B-cell lymphoma
and Burkitt lymphoma.
Grey Zone Lymphomas: Lymphomas with Intermediate Features
B-Cell lymphoma, unclassifiable, with features
intermediate between diffuse large B-cell lymphoma
and classical Hodgkin lymphoma (WHO 2008)
• Neoplasms with morphological and immunophenotypic features
intermediate between DLBCL and HL
• Usually young males with mediastinal involvement, diagnosed at
advanced stages
• Tumors with similar morphology and immunophenotype may also
present in extramediastinal locations.

Workshop report on Hodgkin's disease and related diseases
('grey zone' lymphoma).
Rudiger T, Jaffe ES, Delsol G, et al. Ann Oncol. 1998;9 Suppl 5:S31-38.
• Three cases showed features of both
diffuse large B-cell lymphoma and
classical Hodgkin's lymphoma within
the same specimen (composite
lymphomas).
• Additionally, five cases occurring in
the mediastinum showed both
morphological and
immunohistochemical transition
between cHL and DLBCL.
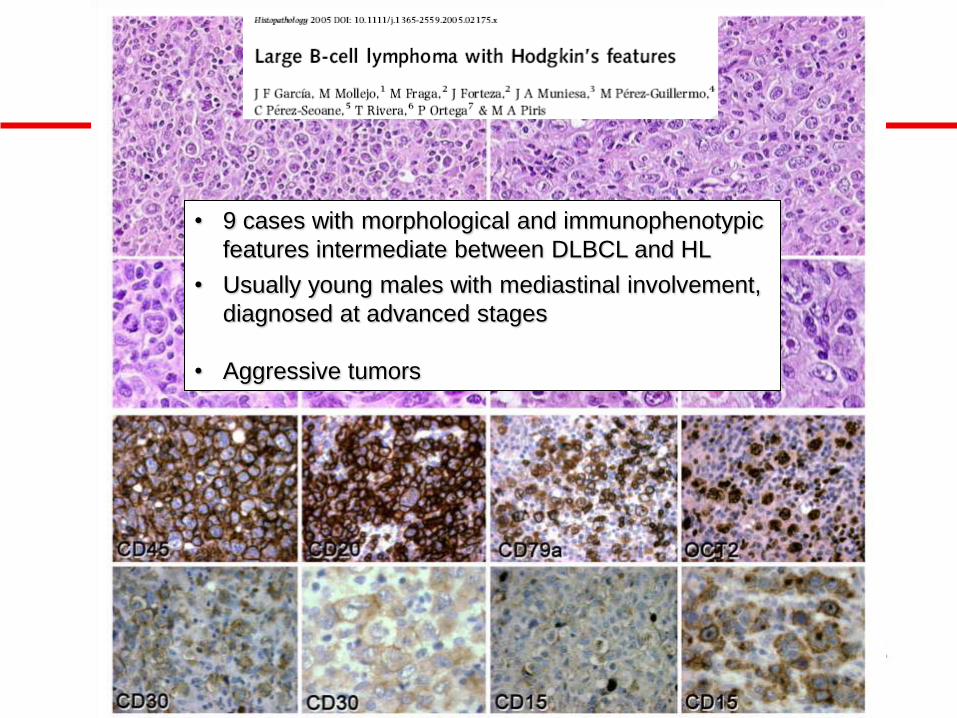
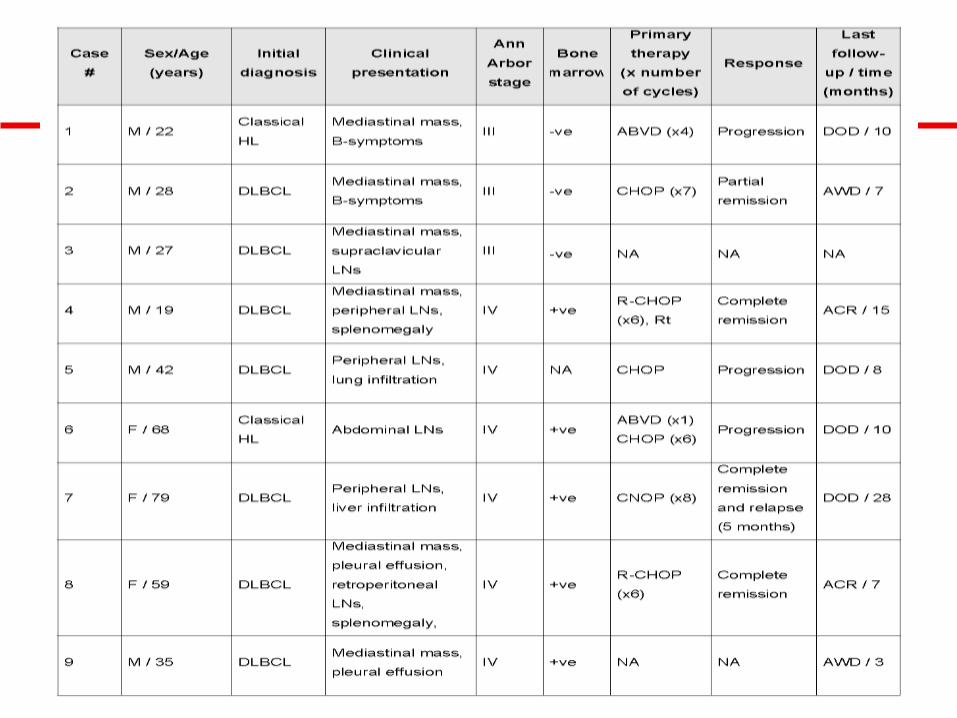
• 9 cases with morphological and immunophenotypic
features intermediate between DLBCL and HL
• Usually young males with mediastinal involvement,
diagnosed at advanced stages
• Aggressive tumors
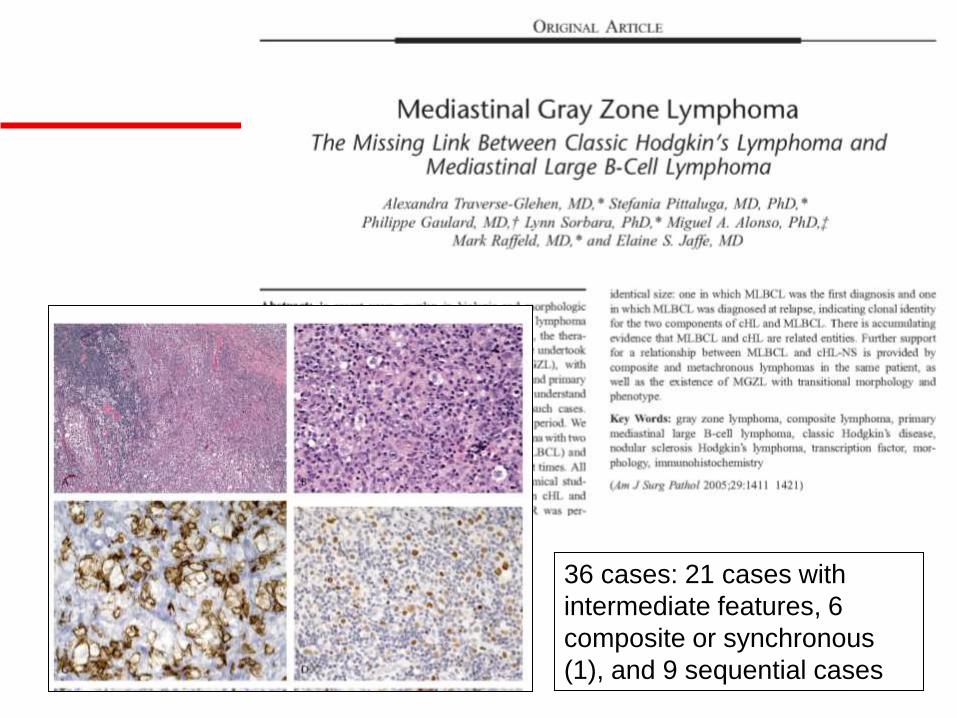
36 cases: 21 cases with
intermediate features, 6
composite or synchronous
(1), and 9 sequential cases

• MAL staining was found in 7 of 10 MGZL, and in at least
one component of 6 of 7 evaluable composite or
sequential MLBCL/cHL cases.
• Two cases of sequential lymphoma showed
rearrangements of the IgH gene of identical size: one in
which MLBCL was the first diagnosis and one in which
MLBCL was diagnosed at relapse, indicating clonal
identity for the two components of cHL and MLBCL.
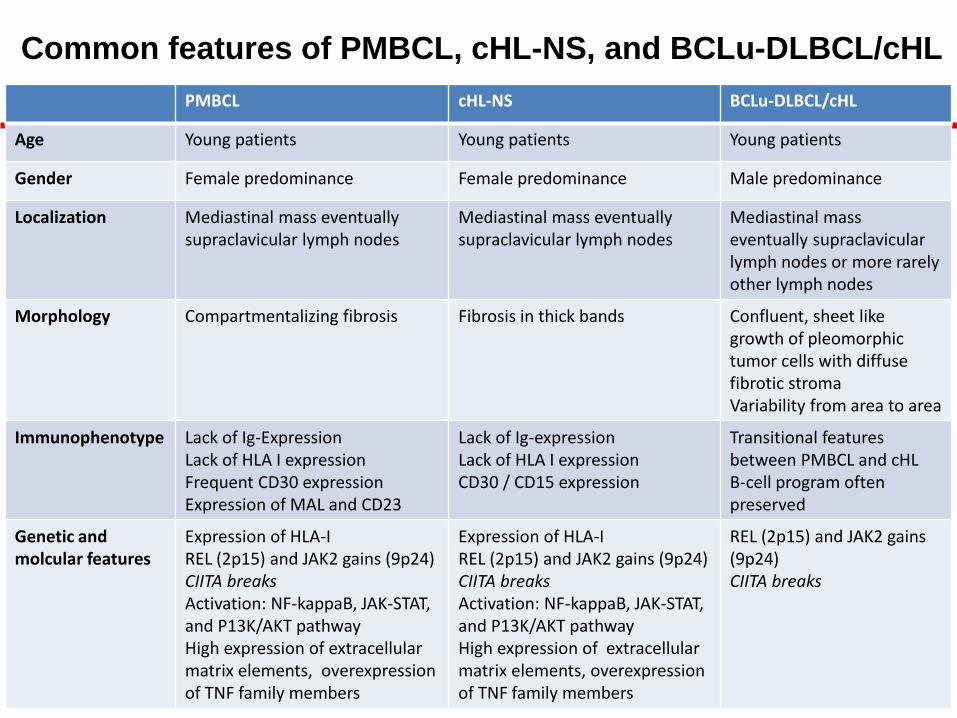
PMBCL cHL-NS BCLu-DLBCL/cHL
Age Young patients Young patients Young patients
Gender Female predominance Female predominance Male predominance
Localization Mediastinal mass eventually supraclavicular lymph nodes
Mediastinal mass eventually supraclavicular lymph nodes
Mediastinal mass eventually supraclavicular lymph nodes or more rarely other lymph nodes
Morphology Compartmentalizing fibrosis Fibrosis in thick bands Confluent, sheet like growth of pleomorphic tumor cells with diffuse fibrotic stroma Variability from area to area
Immunophenotype Lack of Ig-Expression Lack of HLA I expression Frequent CD30 expression Expression of MAL and CD23
Lack of Ig-expression Lack of HLA I expression CD30 / CD15 expression
Transitional features between PMBCL and cHL B-cell program often preserved
Genetic and molcular features
Expression of HLA-I REL (2p15) and JAK2 gains (9p24) CIITA breaks Activation: NF-kappaB, JAK-STAT, and P13K/AKT pathway High expression of extracellular matrix elements, overexpression of TNF family members
Expression of HLA-I REL (2p15) and JAK2 gains (9p24) CIITA breaks Activation: NF-kappaB, JAK-STAT, and P13K/AKT pathway High expression of extracellular matrix elements, overexpression of TNF family members
REL (2p15) and JAK2 gains (9p24) CIITA breaks
Common features of PMBCL, cHL-NS, and BCLu-DLBCL/cHL
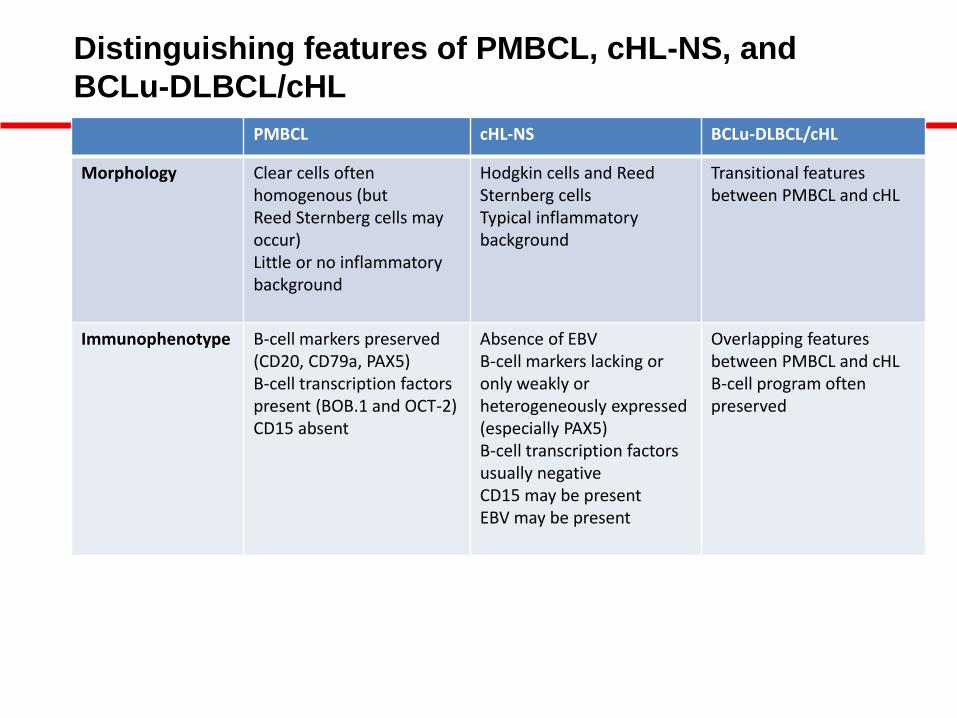
PMBCL cHL-NS BCLu-DLBCL/cHL
Morphology Clear cells often homogenous (but Reed Sternberg cells may occur) Little or no inflammatory background
Hodgkin cells and Reed Sternberg cells Typical inflammatory background
Transitional features between PMBCL and cHL
Immunophenotype B-cell markers preserved (CD20, CD79a, PAX5) B-cell transcription factors present (BOB.1 and OCT-2) CD15 absent
Absence of EBV B-cell markers lacking or only weakly or heterogeneously expressed (especially PAX5) B-cell transcription factors usually negative CD15 may be present EBV may be present
Overlapping features between PMBCL and cHL B-cell program often preserved
Distinguishing features of PMBCL, cHL-NS, and
BCLu-DLBCL/cHL

Molecular diagnosis of primary mediastinal B cell
lymphoma identifies a clinically favorable subgroup
of diffuse large B cell lymphoma related to Hodgkin
lymphoma.
Rosenwald A, et al. J Exp Med 2003;198(6):851-62.
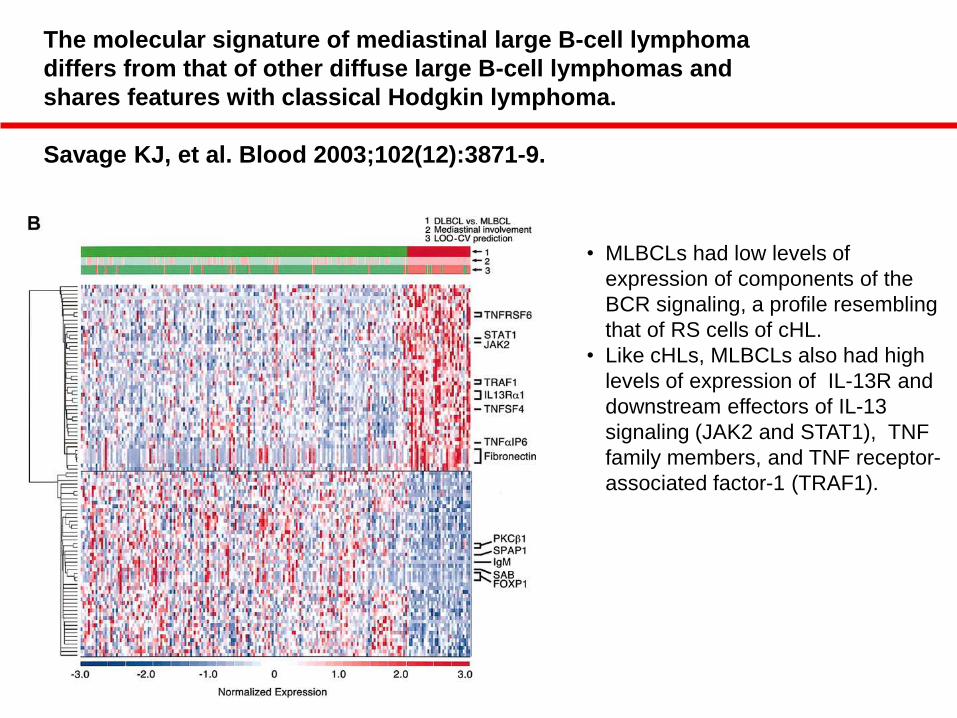
The molecular signature of mediastinal large B-cell lymphoma
differs from that of other diffuse large B-cell lymphomas and
shares features with classical Hodgkin lymphoma.
Savage KJ, et al. Blood 2003;102(12):3871-9.
• MLBCLs had low levels of
expression of components of the
BCR signaling, a profile resembling
that of RS cells of cHL.
• Like cHLs, MLBCLs also had high
levels of expression of IL-13R and
downstream effectors of IL-13
signaling (JAK2 and STAT1), TNF
family members, and TNF receptor-
associated factor-1 (TRAF1).
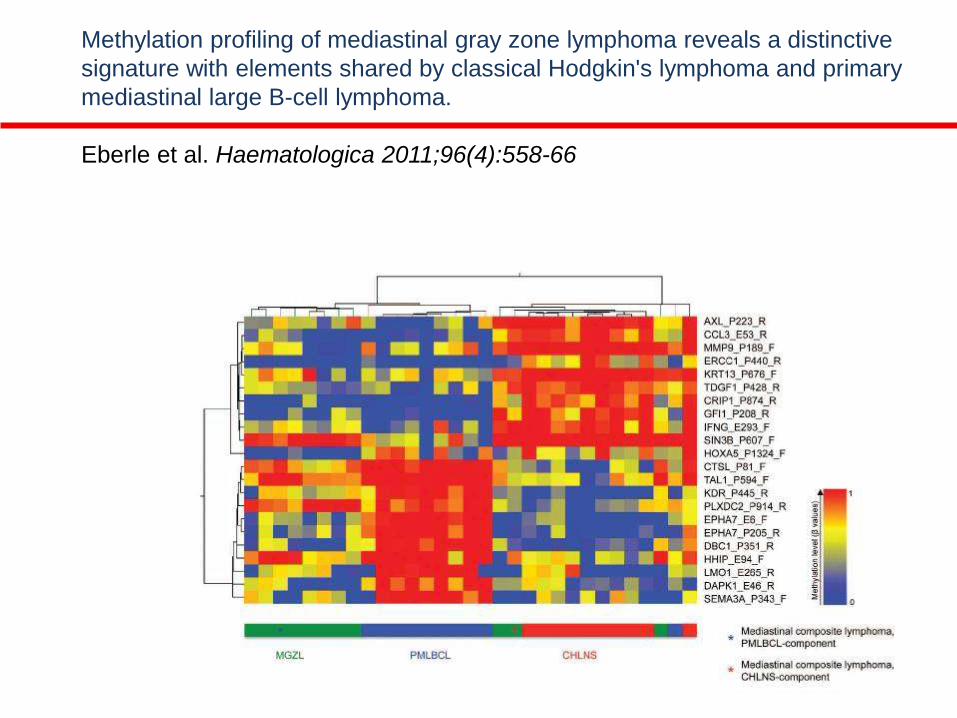
Methylation profiling of mediastinal gray zone lymphoma reveals a distinctive
signature with elements shared by classical Hodgkin's lymphoma and primary
mediastinal large B-cell lymphoma.
Eberle et al. Haematologica 2011;96(4):558-66
Gray zone lymphoma: chromosomal aberrations with immunophenotypic
and clinical correlations
Eberle FC, et al. Mod Pathol 2011;24(12):1586-97
Gray zone lymphoma (n=27), mediastinal composite lymphoma
(n=3) and mediastinal synchronous/metachronous lymphoma (n=3)
• Gains including amplifications in 2p16.1 (REL/BCL11A locus)
were observed in 33% of all patients,
• Gains/amplifications affecting the JAK2/PDL2 locus in 9p24.1
were present in 55%.
• Rearrangement of the CIITA locus at 16p13.13 in 8/30 cases
(27%)
• 7/26 cases (27%) demonstrated gains of 8q24 (MYC).
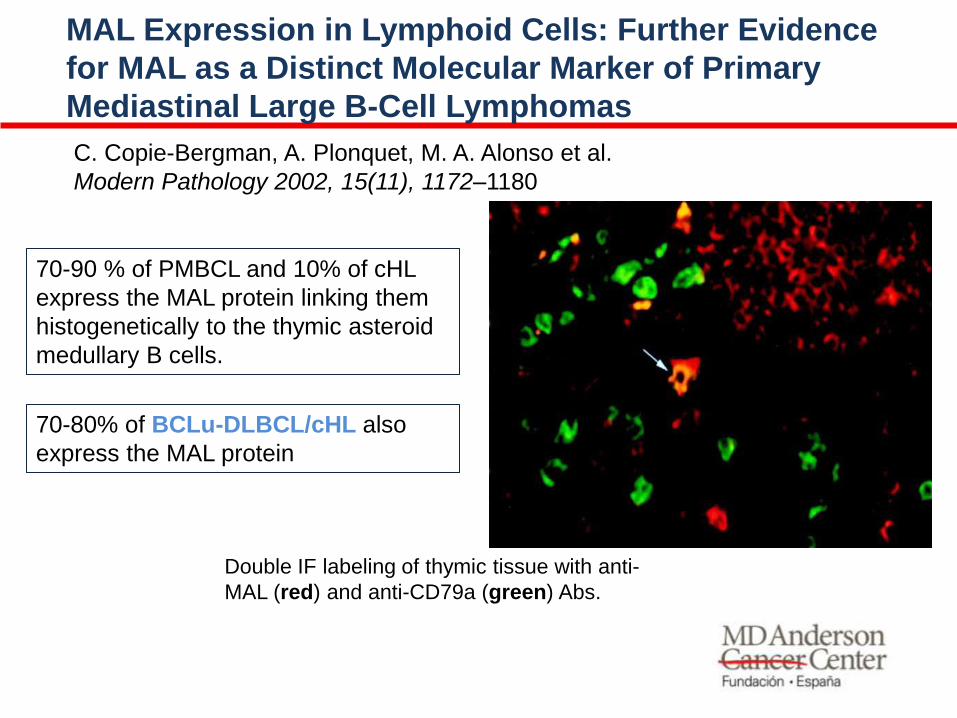
70-90 % of PMBCL and 10% of cHL
express the MAL protein linking them
histogenetically to the thymic asteroid
medullary B cells.
C. Copie-Bergman, A. Plonquet, M. A. Alonso et al.
Modern Pathology 2002, 15(11), 1172–1180
MAL Expression in Lymphoid Cells: Further Evidence
for MAL as a Distinct Molecular Marker of Primary
Mediastinal Large B-Cell Lymphomas
Double IF labeling of thymic tissue with anti-
MAL (red) and anti-CD79a (green) Abs.
70-80% of BCLu-DLBCL/cHL also
express the MAL protein
B-Cell lymphoma, unclassifiable, with features
intermediate between diffuse large B-cell lymphoma
and classical Hodgkin lymphoma (WHO 2008)
• How to treat them?
Gray zone lymphoma: better treated like cHL or PMLBCL?
Dunleavy K, et al. Curr Hematol Malig Rep 2012;7(3):241-7
Grant C, et al. Curr Hematol Malig Rep. 2011;6(3):157-63
• There is a lack of prospective experience in treating GZL
because of the rarity of these tumors.
• Historical data indicate that they have done poorly with
traditional approaches developed for the treatment of
either cHL or diffuse large B-cell lymphoma.
• Preliminary results indicate that 4 of 4 patients treated
with R-CHOP regimen are in complete remission, with 1
patient requiring mediastinal radiation
Traverse-Glehen A, et al. Am J Surg Pathol 2005;29:1411–1421
BCLu-DLBCL/cHL: Diagnostic criteria
• Cases morphologically resembling PMBCL but
with strong expression of CD15, absence of
CD20 or presence of EBV.
• Cases rich in tumor cells resembling cHL, which
are strongly positive for CD20 and other B-cell
markers (CD79a).