lecture 9 chapter 39 antihypertensive drugs. antihypertensive agents hypertension (htn) - an inc. in...
TRANSCRIPT

Lecture 9Chapter 39
Antihypertensive Drugs

AntihypertensiveAgents
• Hypertension (HTN) - An inc. in BP such that systolic is > 140 mm/hg & diastolic > 90 mm/hg on 2 or more occasions after initial screening
• Essential HTN = most common. About 90% of clients.
* Exact Origin - unknown. Contributing Factors - family hx, hyperlipidemia, African American background, diabetes, obesity, aging, stress, excessive ETOH & smoking.
• Secondary HTN is about 10% of HTN, related to endocrine or renal disorders
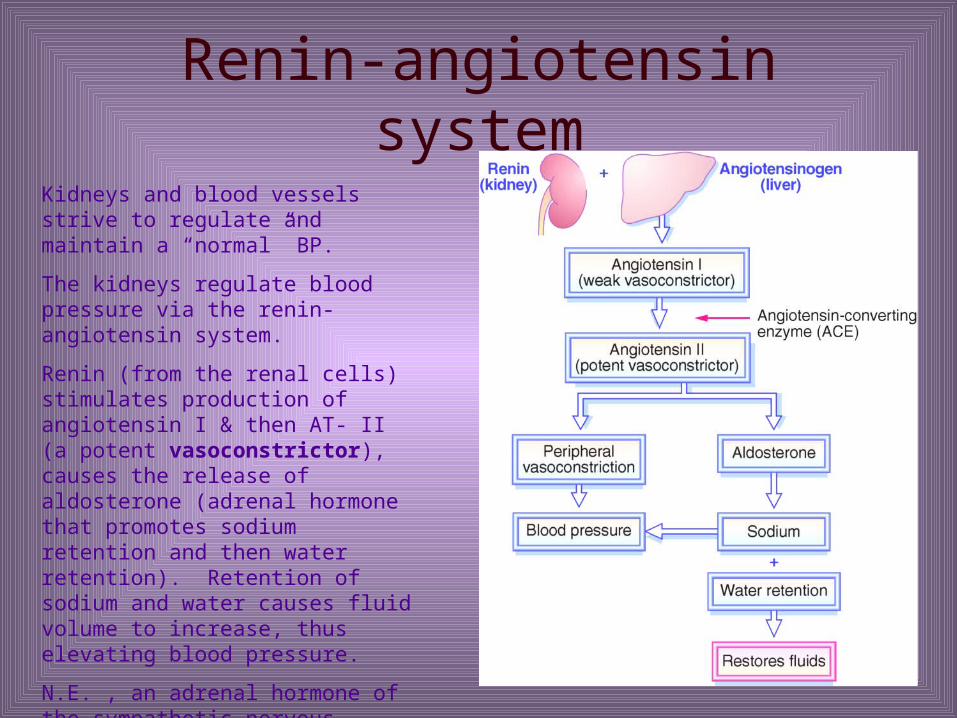
Renin-angiotensin system
Kidneys and blood vessels strive to regulate and maintain a “normal” BP.
The kidneys regulate blood pressure via the renin-angiotensin system.
Renin (from the renal cells) stimulates production of angiotensin I & then AT- II (a potent vasoconstrictor), causes the release of aldosterone (adrenal hormone that promotes sodium retention and then water retention). Retention of sodium and water causes fluid volume to increase, thus elevating blood pressure.
N.E. , an adrenal hormone of the sympathetic nervous system, increases blood pressure.

Hypertension
• Non-Pharmacological - Should be first line of treatment. If successful, no meds. may be needed.
* Stress reduction techniques, exercise, salt restriction, dec. in ETOH intake, no smoking, wt. reduction
• Systolic pressure >140 mm/hg = antihypertensive meds started
• Pt. education & compliance very important as in a good history
Hypertension• Pharmacological therapy - Individualized * Want to start at lowest possible doses of meds. * Reduce risk factors, even while on meds. - lifestyle
changes may allow the client to decrease medications. * suggested after 1 yr. of therapy to dec. dose to determine
if less drug dose possible• Step care hypertensive approach to treatment developed
several years ago - Classified by 4 stages based on BP range. Pg. 695 table 39-1
• Individualized approach is also used - more modified to each client. Pg. 696 - Table 39-3

STEPPED – CARE APPROACHStep 1
Diuretic, Beta Blocker, Calcium blocker, Angiotensin-converting enzyme
Step 2 Diuretic with beta blocker Sympatholytics
Step 3 Direct-acting vasodilator Sympatholytic with diuretic
Step 4 Adrenergic neuron blocker Combinations from steps I, II & III

Antihypertensive Agents
• Drugs used to treat Hypertension:
• Diuretics -
* Promote Na depletion dec. in extra cellular fluid (ECF)
* First line drug for Rx of mild HTN
* Hydrochlorothiazide (HydroDIURIL) most frequently prescribed for first line Rx of mild HTN
* Can be used alone or w/ other antiHTN agents

ANTIHYPERTENSIVE AGENTS
SYMPATHOLYTICS (SYMPATHETIC DEPRESSANTS)
1. BETA-ADRENERGIC
2. CENTRAL ACTING SYMPATHOLYTICS
3. ALPHA-ADRENERGICS
4. ADRENERGIC NEURON BLOCKERS
5. ALPHA & BETA ADRENERGIC BLOCKERS
Antihypertensive Agents
• 1) Beta-Adrenergic Blockers (Beta Blockers)
Atenolol (Tenormin), Metoprolol (Lopressor) - Beta-1 cardio selective
Nadolol (Corgard), Propranolol (Inderal) -
Nonselective Beta-1, Beta-2
- Step 1 or 2 Rx - may be combined w/ a diuretic
- Reduces cardiac output (CO) by diminishing sympathetic nervous system response
Antihypertensive AgentsBeta Blockers
- With continued use the vascular resistance diminished & BP lowered
- Reduces HR & contractility - Reduces renin release from kidneysNonselective = inhibits Beta-1 (heart) & Beta-2 (bronchial)
receptors - HR slows & BP decreases - Bronchoconstriction occursCardio selective - Preferred - acts mainly on Beta-1
receptors & bronchospasms less likely - not absolute protection *Use cautiously in clients w/ pulmonary history*

Antihypertensive Agents
• 2) Centrally Acting Sympatholytics (Adrenergic Blockers) Clonidine HCL (Catapres), Methyldopa (Aldomet) - Stimulate Alpha-2 receptors dec. sympathetic activity
dec. epi., norepi. & dec.renin release dec. peripheral vascular resistance
- Can be used w/ other agents - Clonidine = a new transdermal preparation - provides a 7 day
duration of action- Used w/ diuretics – to prevent NA+ and fluid retention- Do not D/C drug abruptly - HTN crisis possible

Antihypertensive Agents
• 3) Alpha - Adrenergic Blockers
Prazosin HCL (Minipress)
- Blocks alpha adrenergic receptors vasodilatation & a dec. in BP
- Helps maintain renal blood flow
- Useful in clients with lipid abnormalities - decs. VLDL & LDL - responsible for build-up of fatty plaques in arteries & incs. HDL (friendly)
- Can cause Na & H2O retention - diuretics may be added
ANTIHYPERTENSIVE AGENTS
• Safe for diabetics, do not affect respiratory function.
• Used in HTN, refractory CHF, Benign prostatic hypertrophy (BPH)
• Side effects – dizziness, drowsiness, HA, N, V, &D., impotence, vertigo, urinary frequency, tinnitus, dry mouth
• Adverse - Orthostatic hypotension, palpitations, tachycardia
• When taken with ETOH or other antihyper. severe hypotension
Antihypertensive Agents
• 4) Adrenergic Neuron Blockers (Peripherally acting sympatholytics)
* Potent drugs that block norepi. form sympathetic nerve endings a dec. in norepi. dec. in BP
* Decrease in both cardiac output & peripheral vascular resistance
Reserpine (Serpasil) & guanethidine (Ismelin) - Potent - used for severe HTN
* Step IV drugs - alone or with diuretics to dec. peri. edema * Common SE = Orthostatic Hypotension*
Antihypertensive Agents• 5) Alpha-1 & Beta-1 Adrenergic blockers Carteolol (Cartrol), Labetalol (Trandate) - Blocks both alpha-1 & beta-1 receptors - Block alpha-1 = dilation of arterioles & veins -Effect on alpha receptors stronger than on beta receptors so
have a dec. BP & pulse rate - Block beta-1 lead to decreased HR & AV contractility - Large doses could block beta-2 receptors inc. in air way
resistance - Do not give to severe asthmatics. AV blockSE = Orthostatic Hypotension, GI, nervousness, dry
mouth&fatigue
Antihypertensive Agents
• Direct - Acting Arteriolar Vasodilators - potent Hydralazine (Apresoline) - Mod. to severe HTN Sodium Nitroprusside (Nipride) - Very potent - for
hypertensive Emergencies - Act by relaxing smooth muscles of bld. vessels - mainly
arteries vasodilation - Inc. blood flow to brain & kidneys - With vasodilation the BP dec., Na & H2O retained peripheral edema. Diuretics used to counter this SE- SE = numerous - tachycardia, palpitations, edema, dizzy, GI
bleeding
Antihypertensive Agents
• Angiotensin Antagonists - Angiotensin-Converting Enzyme Inhibitors (ACE inhibitors)
Captopril (Capoten), Enalapril (Vasotec), Lisinopril (Zestril)
- Prevents conversion of Angiotensin I to angiotensin II (vasoconstrictor) & blocks release of aldosterone. Aldosterone promotes Na retention & K excretion. Block aldosterone & Na excreted, but H2O & K retained
- Used to treat HTN primarily, - but not a 1st line drug. Also used in heart failure.
- SE = hyperkalemia & 1st dose hypotension (more common with comb. Diuretic & ACE inhibitor.
Antihypertensive Agents
• Angiotensin II receptor Antagonists (Blockers) - A - II Blockers
Losartan (Cozaar)
- Newer drugs similar to ACE inhibitors + prevent release of aldosterone (Na+ retaining hormone)
- Act on renin - angiotensin system - Diff between ACE &AII is A-II blockers block
angiotensin from angiotensin I receptors found in many tissues - blocks at receptor site.
- A-II blockers cause vasodilation & dec. peripheral resistance

ACE inhibitors inhibit the enzyme necessary for the conversion of A-I to A-II
A-II blockers - block angiotensin II from receptors in blood vessels, adrenals, and all other tissues.
AntihypertensiveAgents
• Calcium Channel Blockers Verapamil (Calan), Nifedipine (Procardia),
Diltiazem (Cardizem) - Free calcium muscle contractility, peripheral
resistance & BP . So, Calcium blockers - Dec. calcium levels & promote vasodilation - Drugs can be used w/ clients prone to asthma - SE. Flushing, HA, dizzyness, ankle edema,
bradycardia, AV node block,
Math
A dosage of 200 mg must be prepared from a solution strength of 80 mg. per ml. How many mls. should be given?
80 mg = 200mg Cross multiply 1 ml X ml
80 X = 200 mg Immediately divide by the number
on front of X
200 = Reduce the fraction. 5 80 2
2.5 ml