lecture 4 cataract & glaucoma lecture 4 cataract & glaucoma lecture is delivered by ph. d.,...
TRANSCRIPT

Lecture 4 Lecture 4 CATARACT & GLAUCOMACATARACT & GLAUCOMA
Lecture is delivered byLecture is delivered by
Ph. D., assistant of professor Tabalyuk T.A.Ph. D., assistant of professor Tabalyuk T.A.




Classification of cataracts:Classification of cataracts:
By age: By age: congenital, juvenile, age-related congenital, juvenile, age-related (senile)(senile)
By location opacities in the lens as seen By location opacities in the lens as seen with slit beamwith slit beam:: cortical, nuclear, anterior cortical, nuclear, anterior subcapsular, posterior subcapsularsubcapsular, posterior subcapsular
By maturity: By maturity: early, immature, mature, early, immature, mature, hypermature (Morgagnian cataract)hypermature (Morgagnian cataract)
By pattern: By pattern: cuneiform (typical senile type), cuneiform (typical senile type), zonular, polar, pyramidal (congenital types)zonular, polar, pyramidal (congenital types)







DIFFERENTIAL DIAGNOSISThe same sign is progressive (not acute) painless visual loss
SignCATARACT GLAUCOMA
MACULAR DEGENERATION
Visual acuity
is decreased
Field of vision
is not damaged constriction of nasal visual field, Bjerrum’s scotoma
may be central scotoma
Intraocular pressure
normal,if increased-secondary phakogenic glaucoma
increased normal
Lens opaque transparent,if opaque– complicated cataract
transparent, if opaque– complicated cataract
Fundus If is seen, not damaged.If damaged - complicated cataract
optic disc changes - dislocation of vessels, pale colour, increased cupping
degenerative patches in central area













Artificial lensesArtificial lenses

Artiphakia is a condition of eye with artificial lens (IOL).
Aphakia is a condition of eye without lens. The visual acuity without correction is very poor – 0,02-0,04. Iridodenesis (iris vibration) is typical.Thick plus glasses are needed for vision: for far distance – sph convex 10,0-12,0 Dfor near distance – sph convex 13,0-15,0 D.
Secondary cataract occurs eventually in about 20 % cases after cataract surgery. It is opacity of natural posterior capsule. It can be treated by YAG laser capsulotomy.
Attention! The term «complicated cataract» is used to describe a lens opacity which occurs as a result of some other disease of the eye. Longstanding uveitits, an untreated retinal detachment or an intraocular tumour are all examples of an associated disease.


CONGENITAL CATARACTS :
I degree – visual acuity is 0,3 and more; the size of opacity is less then 1,5 mm; the surgery may be done at the age of 14-16 years.
II degree– visual acuity is 0,05-0,2; the surgery is usually done at the age of 3-4 years.
III degree– visual acuity is less then 0,05; the surgery must be done during first year of life.



Ectopia lentis (displacement of the lens) may be partial (subluxation) or complete (luxation).
Aethiology: trauma, familial ectopia lentis (may be associated with ectopic pupil), associated with other ocular disprders (aniridia and buphtalmos), Marfan’s and Weill-Marchesani syndromes, metabolic (homocystinuria and hyperlysinaemia).
Clinical features: iridodenesis (vibration of iris) and not proportional depth of anterior chamber.
Marfan’s syndrome: tall person with partial displacement of the lens (subluxation), fragile bones and arachnodactyly.


Video – phakoemulsificationVideo – phakoemulsification

The outflow pathways of aqueous humorThe outflow pathways of aqueous humor::1.Main:: posterior chamber - pupil - anterior
chamber - trabecular meshwork - Schlemm’s canal (scleral sinus)- vorticose veins – scleral venous plexus.
Additional::2. Perivascular spaces of iris.2. Perivascular spaces of iris.3. Suprachoroidal space - perivascular spaces – 3. Suprachoroidal space - perivascular spaces –
through sclera into the tenonthrough sclera into the tenon’ s space.4. Perivascular spaces ofPerivascular spaces of central retinal vessels.
The IOP The IOP is maintained by a balance between is maintained by a balance between aqueous inflow and outflow &aqueous inflow and outflow & usually measures usually measures betweenbetween
16-2616-26 mm Hg (using tonometr of mm Hg (using tonometr of MaklakovMaklakov) ) &&
10-2010-20 mm Hg (using tonometr of mm Hg (using tonometr of GoldmanGoldman))



Noncontact pneumatic Noncontact pneumatic autotonometryautotonometry


Not every increasing of IOP is glaucoma. It may be ocular hypertension, caused, for example, by using corticosteroids, intoxication or climax. Typical for ocular hypertension are:
absence of structural and functional changes;
lasting existence without complaints;symmetrical increasing of IOP. So, ocular hypertension is a symptom,
glaucoma is a syndrome. Glaucoma is such increasing of IOP,
which is accompanied by specific visual defects (constriction of nasal visual field, Bjerrum’s scotoma) and specific optic disc changes (dislocation of vessels, increased cupping etc.)

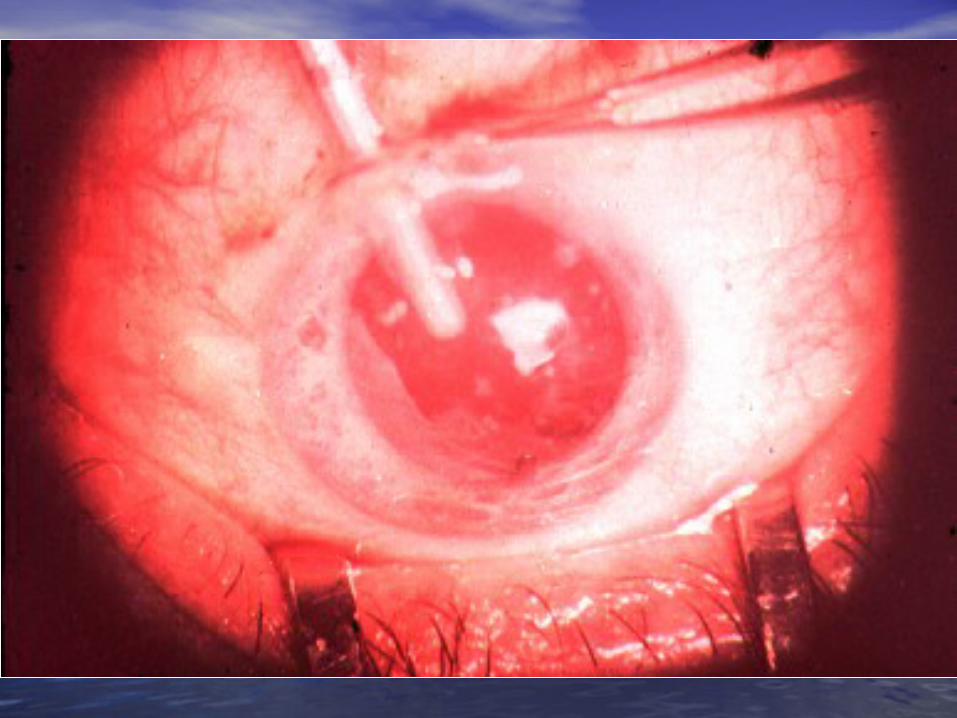
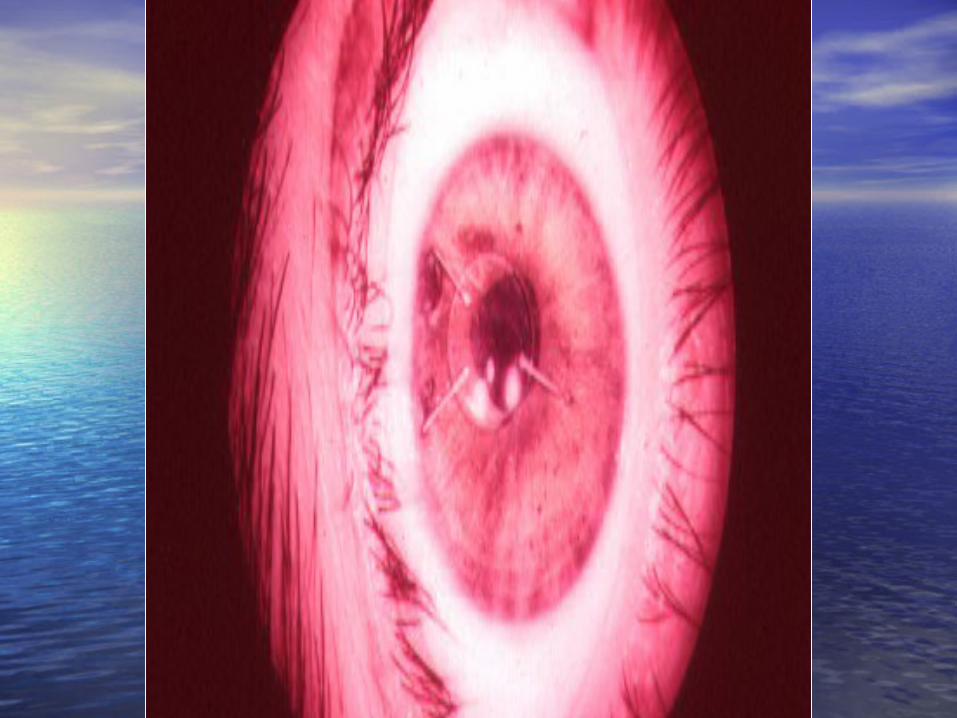
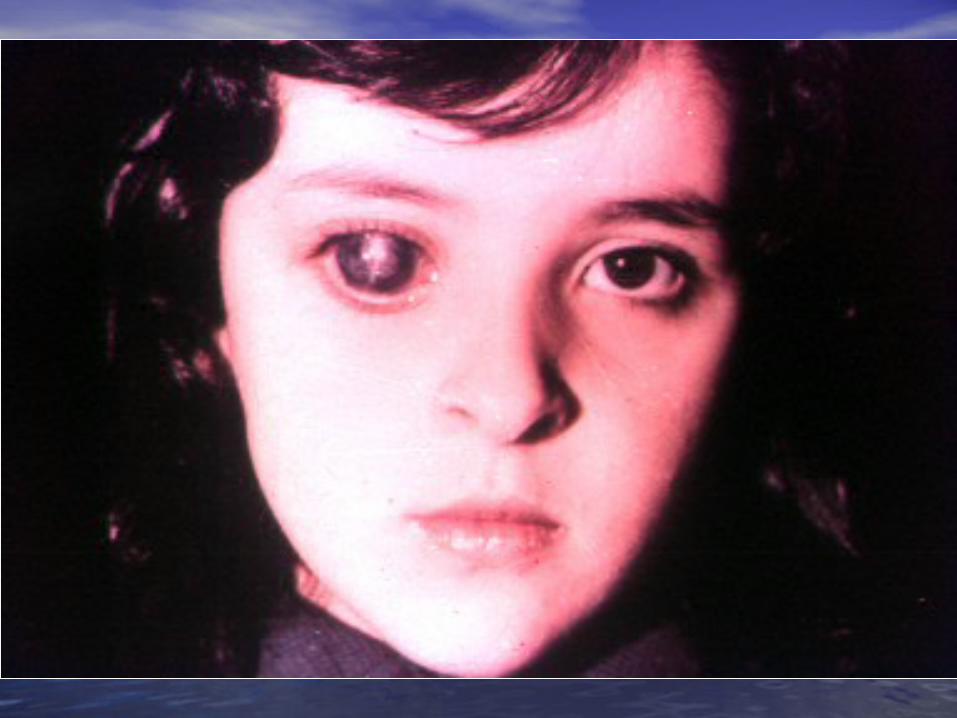
Congenital glaucoma (or hydrophtalmos) is caused by abnormal development of eye drainage system. The accumulation of aqueous in the eye due to elasticity of baby’s external coat causes the increasing of eye size.
There are 2 clinical forms:I. Hydrophtalmos without stasis (megalocornea, stretching
out of limbus, deep anterior chamber, increased eye, loss of vision, increased IOP, typical changes of optic nerve).
II. Hydrophtalmos with stasis (all above mentioned signs + photophobia, blepharospasmus, mixt injection, corneal oedema, which is reliefed by 40 % glucosae).
There are 4 stages:I. Early – D of cornea 12,0-12,5 mm, anterior-posterior distance
of the eye is increased on 1,5-2,0 mm, N fundus.II. Advanced - D of cornea 13,0-14,0 mm, anterior-posterior
distance of the eye is increased on 3,0-4,0, glaucomatous cupping of optic disc ophthalmoscopically.
III. Far advanced - D of cornea is more then 14,0 mm, anterior-posterior distance of the eye is more then 30,0 mm, atrophy of optic disc ophthalmoscopically.
IV. Terminal (or buftalm) – full blidness, scleral staphyloma.




Methods of diagnostic of congenital glaucoma:
General examination, especially of cornea & limbus Biomicroscopy or focal lighting Keratometry Tonometry Ultrasound biometry Ophthalmoscopy
Methods of treatment of congenital glaucoma:Only surgical. Immediatly!
Goniotomy Sinusotrabeculectomy Enucleation in buftalmos

Classification of primary acquired Classification of primary acquired glaucomaglaucoma
Clinical form Stage Level of IOP Dynamics of visual
functions
1.1. Open-Open-angle angle
2.2. Close-Close-angleangle
3.3. MixtMixt
I – earlyI – early
II – II – advancedadvanced
III – far III – far advancedadvanced
IV - terminalIV - terminal
A - compensatedA - compensated
B - B - subcompancatedsubcompancated
C -decompancatedC -decompancated
stabile &stabile &
nonstabilenonstabile

Stages of primary glaucoma (according to visual functions defects):
I – visual field is consticted less then 10 degrees, physiological cupping is increased.
II - visual field is consticted more then 10 degrees, edge excavation.
III – tube visual field (15 degrees from the point of fixation), edge excavation.
IV – visual field or visual acuity is zero, atrophy of optic disc.
Depending on IOP (using tonometr of Maklakov) glaucoma is subdivided:
A (compensated) – IOP is less then 27 mm Hg.B (subcompancated) – IOP is 28-32 mm Hg.C (decompancated) – IOP is 33 mm Hg and more.According to dynamics of visual functions during 6
month:stabile &nonstabile – constriction of visual field on 10 degree and
more;in tube vision – on 2-3 degrees and more;increasing of scotomas size;increasing of size of optic disc cupping

Open-angle glaucomaPathogenesis – constriction or closing of openings in
trabeculae & Schlemm’s canal as a result of endocrine, vascular or general diseases such as atherosclerosis, artery hypertension, diabetus mellitus etc.
Clinical features: usually asymptomatic until significant loss of visual field has occured;
the eye looks usual, only dystrophic iris changes may be revealed biomicroscopically;
open anterior chamber angle on gonioscopy, may be excess pigmentation of trabeculae;
& typical for glaucoma signs (elevated IOP+visual field loss,first of its nasal part +optic nerve damage).
Methods of investigation:A. Functional – visometry, perimetry, campimetry,
adaptometry.B. Objective – general examination, focal lighting,
biomicroscopy, gonioscopy, ophthalmoscopy, tonometry.

Close-angle glaucomaPathogenesis –the closing (blockade) of anterior chamber
angle by iris root as a result of excess anterior position of lens or functional pupil blockade (not organic, i.e. occlusio or seclusio pupille) due to excess near location of lens & iris.
Clinical features: complaints for clouding of vision, haloes around lights in the morning, headache, pain in the eye etc.;
frequent change of eye refraction & glasses prescribtion;
sometimes begins from acute attack;signs of venous stasis – dilated scleral veins;
flat anterior chamber & iris bombee biomicroscopically;narrow or close anterior chamber angle on gonioscopy;& typical for glaucoma signs (elevated IOP+visual field
loss,first of its nasal part +optic nerve damage).
Methods of investigation:A. Functional – visometry, perimetry, campimetry,
adaptonetry.B. Objective – general examination, focal lighting,
biomicroscopy, gonioscopy, ophthalmoscopy, tonometry.




DIFFERENTIAL DIAGNOSISDIFFERENTIAL DIAGNOSIS
SignCATARACT
CHRONIC GLAUCOMA
RETINITIS PIGMENTOSA
Visual acuity
is decreased progressivly
Field of vision
is not damaged constriction of nasal visual field, Bjerrum’s scotoma
concentric visual field narrowing
Intraocular pressure
normal,if increased-secondary phakogenic glaucoma
increased normal
Lens opaque transparent,if opaque– complicated cataract
transparent, if opaque– complicated cataract
Fundus if is seen, not damaged.If damaged - complicated cataract
optic disc changes – nasal dislocation of vessels, glaucomatous cupping
mid-peripheral perivascular “bone-spicule” pigmentation, waxy disc pallor without nasal dislocation of vessels & glaucomatous cupping

Medical treatment of chronic glaucoma:1. Local hypotensive therapy. The antiglaucomatous drops are
divided into two main groups: I. which improve outcome of aqeous humourCholinomimetics - 1 % pilocarpini, carbachol;α, Β – adrenomimetics – dipinefrini, epinefrini;Analogs of prostaglandins F 2 α (which stimulate the uveo-scleral outflow) – latanoprost (xalatan), travoprost (travatan) II. which reduce production of aqeous humourCentral agonists of α2- adrenoreceptors - klonidini;B-adrenoblockers: nonselective - timololi, arutimoli, & selective - betoptic;Carbonic anhydrase inhibitors – Azopt.2. Vasodilatators – acidi nicotinici, cavintoni, trentali, halidori etc.3. Nootrops – piracetami, nootropili, etc.4. Stimulators of nerve conductivity – proserini.5. Tissue therapy, vitamins.Laser treatment of chronic glaucoma:Laser peripheral iridotomies in primary angle-closure glaucoma;Laser trabeculoplasty in primary open-angle glaucoma.Surgery of chronic glaucoma:Filtration surgery in primary open-angle glaucoma, e.g.
trabeculectomy.In primary angle-closure glaucoma radical surgery –
phacoemulsification of cataract with IOL implantation; palliative surgery – iridectomy.



Nonpenetreting filtration surgeryNonpenetreting filtration surgery:: canaloplastycanaloplasty
• Figure 1Figure 1 (left) (left). Introduction of the microcatheter into Schlemm's . Introduction of the microcatheter into Schlemm's canalcanal
• Figure 2Figure 2 (right) (right). A 10-0 polypropylene suture being tied around . A 10-0 polypropylene suture being tied around the end of thethe end of the microcathetermicrocatheter

Nonpenetreting filtration surgeryNonpenetreting filtration surgery::viscocanalostomyviscocanalostomy
The initial steps of The initial steps of viscocanalostomy are similar to viscocanalostomy are similar to those of trabeculectomy. those of trabeculectomy. Specifically, the surgeon creates Specifically, the surgeon creates a one-half– to two-thirds–depth a one-half– to two-thirds–depth superficial scleral flap, within the superficial scleral flap, within the bed of which a deep scleral flap bed of which a deep scleral flap is made. The deep dissection is made. The deep dissection begins 4 to 5 mm posterior to the begins 4 to 5 mm posterior to the limbus and advances toward the limbus and advances toward the limbus in a tissue plane just limbus in a tissue plane just above the suprachoroidal space. above the suprachoroidal space. As the dissection advances As the dissection advances anteriorly, the roof of Schlemm’s anteriorly, the roof of Schlemm’s canal is removed. The surgeon canal is removed. The surgeon then cannulates Schlemm’s canal then cannulates Schlemm’s canal and injects a bolus of viscoelastic and injects a bolus of viscoelastic material into each of the canal’s material into each of the canal’s cut ends (cut ends (as in the pictureas in the picture). This ). This viscodissection is intended to viscodissection is intended to dilate the canal and facilitate the dilate the canal and facilitate the subsequent drainage of aqueous. subsequent drainage of aqueous.
Laser surgery in glaucomaLaser surgery in glaucoma

Differential diagnosis of acute close-angle Differential diagnosis of acute close-angle glaucomaglaucoma
Symptom acute close-angle glaucoma
iridocyclitis
haloes around lights + -
irradiation of pain + -
injection (redness) mixtvenous stasis
pericornealarterial
cornea oedematous
decreased sensitivity
precipitates on endothelium
normal sensitivity
anterior chamber flat normal
pupil mydriasis miosis, posterior synechia
IOP increased normal or decreased

Emergency in acute close-angle glaucoma:
instillation of miotics (pilocarpini 1 or 2 %) every 15 minutes during first hour, every 30 minutes during next hour, then 4 times a day;
analgetics (promedoli 2 % 1,0 ml s/cutaneous);
diuretics (Diacarbi 0,5 or Hipothiasidi 0,1 per os, Lasix 1 % 2,0 ml i/m)
If the attack of acute close-angle glaucoma doesn’t disappear during 12-24 hours,
antiglaucomatous surgery is indicated.

Suspicion of glaucoma may be in such cases:• IOP is 27 mm Hg and more (using tonometr of Maklakov) and 21 mm and more (using tonometr of Goldman);• complaints for clouding of vision, haloes around lights in the morning;• iris bombee, less depth of anterior chamber;• typical changes of optic disc;• the difference in right and left eye IOP is more then 5 mm Hg.
All patients with suspicion of glaucoma must be observed in details in clinics. This diagnosis can exist only one year.
Methods of investigation:A. Functional – visometry, perimetry, adaptonetry, campimetry.B. Objective – general examination, focal lighting, biomicroscopy, gonioscopy, ophthalmoscopy, tonometry.C. Necessary additional – diurnal tonometry, tonography, elastotonometry, provocative test.

Secondary glaucoma is complication or outcome of some other eye diseases. It may be:
1. Uveal glaucoma – as a result of pupil occlusion. Management – treatment of uveitis. In deep anterior chamber– mydriatics. In flat anterior chamber – miotics.2. Phacogenic – prodused by immature cataract or lens dislocation into the anterior chamber. Management – cataract surgery.3. Phacolytic - prodused by hypermature cataract. Management – cataract surgery.4. Vascular glaucoma as a result of central vein occlusion or neovascularization in diabetus mellitus. Management – treatment of main disease.5. Posttraumatic as a result of burns, penetrating or blunt injury of eyeball. Management – miotics.6. Neoplastic – as a result of intraocular tumours. Management–surgery (enucleation).

THANK YOU FOR THANK YOU FOR ATTENTION!ATTENTION!