leap winter 2012
DESCRIPTION
Leap magazine is designed to ensure that as we learn more about cancer, you do, too.TRANSCRIPT
HERBAL CURE? ASK AN EXPERT ABOUT SAW PALMETTO
WHEAT & CHAFF WHAT DO PEOPLE HAVE
AGAINST GLUTEN?
PM#40020055
TRANSFORMINGCANCER
TOP JOB
PUSH PAST PRESSURE Manage your stress
p.40
LOOK CLOSERA trio of donors funds
cutting-edge scanners
BIOBANKS EXPLAINEDHow tissue samples
get to the lab
BEYOND THE BLADE
Surgical oncology impacts cancer care
For an unforgettable six hours this March, join hundreds of women and men as they jump, jive, dance and laugh while raising valuable funds for breast health in Alberta. 1.855.250.MOVE
TODAY ATREGISTER
COMINGEDMONTON MARCH 2013
&CALGARY
For an unforgettable six hours this March, join hundreds of women and men as they jump, jive, dance and laugh while raising
REGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTER
EDMONTON &CALGARY
BUSTAMOVE.CA
000Leap-BustAMove-FP.indd 1 11/6/12 2:02:08 PM
Speech pathologist Anna Sytsanko has
people talking(and eating)
into Alberta’s cancer-free movement WINTER 2012
into Alberta’s cancer-free movement
Leap_Winter12_p52-01.indd 1 11/20/12 4:07:35 PM
10K RUN //5K WALK Fight Cancers Below the Waist
REGISTER TODAYUNCOVERTHECURE.ORGCalgary 403.269.3337 // Edmonton 780.423.2220
Revealing changesCOMING SOON!
Leap_Winter12_p02-03.indd 2 11/20/12 10:29:14 AM
alber tacancer foundat ion.ca winter 2012 3
WINTER 2012 • VOL 3 • No. 3CONTENTS
FEATURES16 TOP JOB
Speech pathologis t Anna Sy t s anko helps patient s eat , t alk and share their e xperiences
30 PLANNED GIVINGJohn Por ter los t the love of his life to cancer. He ha s planned to donate par t of his es tate in her honour
31 WHY I DONATEA trio of donor s funds cut ting- edge equipment
36 MANAGE YOUR CANCERO ne - time cancer patient put s her e xperience to use w ith a diar y to help other s mana ge the journey
38 AT-HOME WORKOUTSIf the weather and circums t ance shut s you in , don’t let it interrupt your workout s
40 RESEARCH ROCKSTAR Meet S am Weis s , direc tor of the Hotchkis s Br ain Ins titute, mount ain lover, and research smar t y
44 PUSH PAST PRESSUREStres s beget s s tres s . Here are some tips to help you mana ge
48 PLAN FOR SUCCESSHow to make the mos t of your fundr aising idea
DEPARTMENTS4 OUR LEAP
A mes s a ge from the Alber t a Cancer Foundation
6 FOREFRONTBet ter pos ture, Top 10 w inter ac tivities , O utdoor pur suit s , Coconut skin b alm , Road r a ge, Fun for veg ans , Veg gie recipe, Hope for myeloma , A caring gif t
12 BODYMINDGet the skinny on herb al treatment s
13 SMART EATSShould you avoid gluten?
14 ASK THE EXPERTSWhy do I need a brea s t ultr a sound? What are the cancer s that are routinely screened for in Alber ta? Are the health benef it s the s ame for mild- to - moder ate e xercise a s they are for moder ate - to - intense? What is s aw palmet to?
19 BEYOND CANCERSur vivor care plans are on the horizon
34 CORPORATE GIVINGION Print Solutions ha s a big hear t
50 MY LEAPMeet a team that boogied and zumb aed it s w ay into the Bus t a Move record books
WINTER SPOTLIGHTTRANSFORMING CANCER
40
36
20
ON THE COVER: Anna SytsankoPHOTO: Curtis Trent
20 BEYOND THE BLADESur gical oncolog y makes inroads into cancer care
24 GREENER DREAMSWe have many tools to cope w ith cancer. Solace can be found in sunshine and g reener y
26 BIOBANK PRIMERHow a tis sue s ample get s from the patient to the lab and w hat you need to know
28 NEW CANCER SCREENSIs a tes t for lung cancer on the horizon?
10K RUN //5K WALK Fight Cancers Below the Waist
REGISTER TODAYUNCOVERTHECURE.ORGCalgary 403.269.3337 // Edmonton 780.423.2220
Revealing changesCOMING SOON!
20 BEYOND THE BLADE
14
16
24
Leap_Winter12_p02-03.indd 3 11/20/12 4:09:00 PM
myleapmagazine.ca4 winter 2012
ALBERTA CANCER FOUNDATIONmessage /
TRUSTEES
John Osler, ChairCalgary
Angela BoehmCalgary
Heather CulbertCalgary
Steven DyckLethbridge
Paul GrundyEdmonton (ex-offi cio)
Katie McLeanCalgary
John J. McDonaldEdmonton
Brent Saik, Vice ChairSherwood Park
Heather WattEdmonton
Vern Yu, Chair Calgary
Over the last few months, you may have noticed a change in the way wetalk about our donor dollars. We have been using phrases like “transfor-mational investments” and “maximum impact” and “outcomes that mat-ter to Albertans.” There is a good reason for this.
The Alberta Cancer Foundation is making some changes. Our donors want to know where their dollars are going and, more importantly, how their funds are making a difference. We want to make sure that the invest-ments we make on behalf of our donors have an even bigger impact in this province. We want to see positive outcomes for Albertans. We want to make sure that the research we fund fi lters directly down to the health-care system and improves the lives of Albertans. To do this, the Alberta Cancer Foundation is embarking on a more focused and active research investment approach aimed at reaching our vision of a cancer-free future. By continuing to focus our resources on high quality, scientifi c research combined with an increased focus on outcomes, clinical impact and col-laboration, we will improve the lives of Albertans facing cancer.
Our donors have played a big role in funding cancer research in this province. They have contributed more than 25 per cent of the $400 mil-lion spent on cancer research in the last decade in Alberta, and we owe it to donors to make sure their investments deliver progress.
We are working closely with our partners, including Alberta Health Services-Cancer Care, universities in Alberta, Calgary and Lethbridge,
donor groups and other funding agencies to deter-mine key opportunities and priorities for investment in research.
We recognize the importance of targeting invest-ments where there is the greatest opportunity to make positive and tangible progress. We also want to build capacity in the cancer research community, encourage collaboration and develop sustainable
infrastructure. We will focus our investments in areas where we can achieve signifi cant outcomes in screening, diagnostics, treatment, pre-vention and survivorship. Most importantly, we want to make it easier to rapidly translate research into practice. Our basic, translational and clini-cal researchers all play a vital role in achieving this impact.
We believe a cancer-free future is attainable. We also believe we’re at a tipping point with cancer research. With the right approach and frame-work, we can accelerate the use of this growing body of knowledge to improve the health of Albertans.
We will keep you updated on our progress as we roll out this new frame-work. If you have any questions, please contact our provincial office at 1-866-412-4222 or 780-643-4400.
Myka Osinchuk, CEO John Osler, ChairAlberta Cancer Foundation Alberta Cancer Foundation
Shift in Focus
We will focus our investments in areas where we can achieve signifi cant outcomes in screen-ing, diagnostics, treatment, prevention and survivorship.
Leap_Winter12_p04-05.indd 4 11/20/12 4:09:36 PM
A l b e r t a ’ s c a n c e r - f r e e m o v e m e n t winter 2012 5
w w w . a l b e r t a c a n c e r . c a
The Alberta Cancer Foundation is more than a charity—it’s a
movement for cancer-free lives, today, tomorrow and forever.
It’s a movement of those who know a cancer-free future is possible and who won’t settle for “some day.”
It’s a movement of Albertans who stand with those who have no choice but to stand up to cancer.
It’s a movement of those who know something can be done and are willing to do it.
For those facing cancer today, in honour of those lost to cancer, and for generations to come,
we promise progress.
WINTER VOL 3 • No. 3
ALBERTA CANCER FOUNDATIONASSOCIATE EDITOR: PHOEBE DEY
EDITORIAL ADVISORY COMMITTEEDR. PAUL GRUNDY,Senior Medical Director, Cancer CareAlberta Health ServicesDR. HEATHER BRYANTVice-President, Cancer ControlCanadian Partnership Against CancerDR. STEVE ROBBINSDirector, Southern Alberta Cancer Research InstituteAssociate Director, Research, Alberta Health Services, Cancer CareCHRISTINE MCIVERCEO, Kids Cancer Care Foundation of Alberta
VENTURE PUBLISHING INC.PUBLISHER: RUTH KELLYASSOCIATE PUBLISHER: JOYCE BYRNEEDITOR: MIFI PURVISASSISTANT EDITOR: MICHELLE LINDSTROMART DIRECTOR: CHARLES BURKEASSISTANT ART DIRECTOR: COLIN SPENCEASSOCIATE ART DIRECTOR: ANDREA DEBOERPRODUCTION COORDINATOR: BETTY-LOU SMITHPRODUCTION TECHNICIAN: BRENT FELZIENDISTRIBUTION: JEN KING
CONTRIBUTING WRITERS: Gisele Aparacio-Hull, Linda Carlson, Janine Giese-Davis, Michael Hingston, Annalise Klingbeil, Cailynn Klingbeil, Michelle Lindstrom, Craille Maguire Gillies, Bobbi Menard, Omar Mouallem, Lisa Ricciotti, Karol Sekulik, Christy Soholt
CONTRIBUTING PHOTOGRAPHERS AND ILLUSTRATORS: Brian Buchsdruecker, Ewan Nicholson, Heff O’Reilly, Curtis Trent, Eugene Uhuad
ABOUT THE ALBERTA CANCER FOUNDATIONThe Alberta Cancer Foundation is Alberta’s own, established to advance cancer research, prevention and care and serve as the charitable foundation for the Cross Cancer Institute, Tom Baker Cancer Centre and Alberta’s 15 other cancer centres. At the Alberta Cancer Foundation, we act on the knowledge that a cancer-free future is achievable. When we get there depends on the focus and energy we put to it today.
Leap is published for the Alberta Cancer Foundation by Venture Publishing Inc., 10259-105 Street, Edmonton, AB T5J 1E3Tel: 780-990-0839, Fax: 780-425-4921, Toll-free: [email protected]
The information in this publication is not meant to be a substitute for professional medical advice. Always seek advice from your physician or other qualifi ed health provider regarding any medical condition or treatment.
Printed in Canada by Transcontinental LGM. Leap is printed on Forest Stewardship Council ® certifi ed paper Publications Agreement #40020055 ISSN #1923-6131Content may not be reprinted or reproduced without permission from Alberta Cancer Foundation.
Leap_Winter12_p04-05.indd 5 11/21/12 11:00:53 AM
myleapmagazine .ca6 winter 2012
forefront / PREVENT, TREAT, CURE
Top 10 Winter Activities
Coconut oil is often used as an alternativeto traditional cooking oil, but some of the tropical fruit’s benefi ts can be obtained by other means. Try applying a small amount of coconut oil to dry skin brought on by winter weather. Coconut oil is easily absorbed into the skin and is packed with antioxidants. Right after your shower or bath, rub a small amount on your damp skin to help retain the skin’s natural moisture balance. Coconut oil is a good choice of moisturizer for people with simple acne, as it contains lauric acid, which has anti-microbial properties.
Balm for Winter Skin
BY CAILYNN KLINGBEIL, BOBBI MENARD, MICHELLE LINDSTROM AND MIFI PURVIS
Yes it’s cold out, but there are plenty of activities to enjoy, even if they require a few extra layers. Embrace active living in all four seasons and you’ll stay fi t, both physically and mentally.
1. NO MOUNTAINS, NO PROBLEM Cross-country skiing, or Nordic skiing, is a great aerobic workout, and less expensive than downhill skiing or snowboarding. There are groomed trails within the city limits in Edmonton and Calgary. The Canmore Nordic Centre and Strathcona Wilderness Centre are also popular spots.
2. KEEP YOUR FEET MOVING Running and walking in minus-20 temperatures requires the right clothing and the right attitude. Layer clothing to ward off chills and wear running shoes with an aggressive tread. For added motivation, check out The Running Room’s Hypothermic Half Marathons, held in Calgary, Edmonton, Lethbridge and Red Deer (events.runningroom.com).
3. YOU TUBE Think of it as tobogganing for grownups as you fl y down a snow-covered hill in an infl atable tube. Mount Norquay has the only snow tube park in the Banff area (banffnorquay.com/tubing), while Edmonton snow tubers can stay in the city and check out Sunridge Ski Area (sunridgeskiarea.com).
4. BOOTS WERE MADE FOR HIKING Jasper National Park’s extensive trail network includes many valley-bottom trails that are open year-round. Trail condition reports are available online (atparckscanada.gc.ca/apps/tcond). Local shops sell and rent ice cleats.
5. A GOOD DOG It’s a winter adventure you won’t soon forget, as a team of sled dogs pulls you across the frozen landscape. Local sled dog tour companies operate in Canmore, Banff, Lake Louise and Jasper.
6. SHOES FOR SNOW Snowshoeing is another inexpensive way to head outside, while beating the crowds on the ski slopes, no special training required. The University of Calgary’s Outdoor Centre offers guided snowshoe tours every weekend.
7. ICE ICE BABY Check out natural ice sculptures on a guided tour of the Rocky Mountain’s frozen river canyons. Several companies offer ice walk tours of Johnson Canyon in Banff, or Maligne Canyon in Jasper.
8. LIKE A KID AGAIN Soaring down a snow-covered hill and then climbing back up it is a classic winter activity. Check out toboggan hills in your city (The City of Edmonton posts current hill conditions on its website). Helmets recommended.
9. PLENTY OF FISH While sitting on a frozen lake waiting for a fi sh might not sound appealing, fans of the sport would argue otherwise. It is a cool experience to see fi sh coming up to the surface from the deep water, and many companies offer tours to introduce people to ice fi shing (with heated shelter, of course).
10. ALPINE DREAMS No, we haven’t forgotten about downhill skiing and snowboarding. Alberta’s ski hills are among the best in the world. Most resorts offer rentals and lessons (skicentral.com/Alberta).
When Henry David Thoreau said, “Nature is genius,” he intuitively recognized the profound role the outdoors plays in the human psyche. Researchers are fi nding more and more reasons to head outside, even for 20 minutes of your day. In a series of 2010 articles in the Journal of Environmental Psychology, researchers found that, “Being outdoors was associated with greater vitality, a relation that was mediated by the presence of natural elements.” What are you waiting for?
Outdoor Pursuits
Leap_Winter12_p06-11.indd 6 11/20/12 4:10:12 PM

Pick upyour copy today!
Find more health in apple magazineMore health
More healthy eating
More family
More wellness
More Alberta
More healthy eating
apple offers you and your family everyday health and wellness information.
Look for apple at 1,800 locations across Alberta.
Visit applemag.ca for moredetails and exclusive stories.
You may fi nd yourself white knuckling it to work because of the combination of winter driving conditions and the bad drivers out there who make your commute dangerous. While you can’t control the weather, you can take steps to make your commute less stressful.
“Road rage is basically aggressive driving,” says Rick Lang, an Edmonton-based manager of personal operations and AMA driver education. We’ve all seen those drivers and know what the warning signs are – tailgating, honking and changing lanes erratically – and Lang says your best defense is predictability. For example, he says, “If you’re in the curb lane, stay in the curb lane unless you have a reason to go into the left lane or vice versa.” The more lane changes you do, the more spontaneous you appear to other drivers, making them wary or frustrated.
Following the basics of road safety also sets drivers up for success. Shoulder checking and signalling will prevent you from cutting anyone off . Keeping your
RAGE in the Machine
headlights on, especially at this time of year when daylight is minimal, makes your car more visible to others.
There will always be drivers who have aggressive habits and it’s best not to make eye contact with them. “That could be like lighting the fuse,” Lang says. He suggests letting the other driver go fi rst and just get to your destination a few seconds later than planned. “I would rather have someone who is driving aggressively in front of me than behind me,” he says. Above all, avoid retaliating with your car horn or with rude gestures. It isn’t worth it.
Leap_Winter12_p06-11.indd 7 11/20/12 4:10:33 PM

myleapmagazine .ca8 winter 2012
The Great Life Cookbook: Whole Food, Vegan, Gluten-Free Meals for Large GatheringsBy Priscilla Timberlake and Lewis Freedman, RD
“Nearly every Friday for the last 17 years, we have hosted locally grown, macrobiotic vegan dinners in our country home in upstate New York,” writes Priscilla
Timberlake. “Our intention with this book is to offer a blueprint so that others can use it to build community around nourishing macrobiotic/vegan meals.”
Macrobiotics, Timberlake goes on to explain, is a philosophy of life, one that translates as “great life.” The blueprint for vegan entertaining in the hefty cookbook offers 12 full meals, one for each month of the year. Recipes serve 20 to 24 people, although you’ll fi nd a handy guide to scaling down recipes at the end of the book. (Timberlake says she often doubles the recipes to serve 40 or 50 guests.)
Before readers start the recipes they’re guided through some history, including how Timberlake met Lewis Freedman (her husband and co-author of the book) and the couples’ experience with a whole-foods, plant-based diet.
For each month, the book shows recipes for eight dishes including soups, grains, vegetables and desserts. It may seem overwhelming to tackle so many recipes and serving upwards of 20 people, but the book has ample pictures and clear instructions. There are also suggestions for alterative ingredients if some of the more exotic ones listed are not available.
Also handy is “The Apprentice’s Guide,” at the back of the cookbook. It introduces 10 less common ingredients Timberlake reccommends, and provides a list of utensils that the authors consider essential. If you’re unfamiliar with sea vegetables (alaria or dulse, anyone?) or a suribachi (a ceramic bowl with ridges used with a wooden pestle to grind various condiments), this section has you covered. A comprehensive index also makes it easy to fi nd the recipe you want, in case an eight course dinner is not your thing.
“Offering healthy, delicious food is a very practical way to benefi t others,” Timberlake writes, “Cooking with mindfulness fosters one’s own inner peace and joy.” She’s hopeful users of this cookbook will feel the joy.
Adapted from the Great Life Cookbook (Coddington Valley Publishing, $26.50)
INGREDIENTS• ¾ pound of asparagus
• 2 medium carrots
• ½ head small caulifl ower
Orange Sesame Dressing:
• Juice of one orange (about 1/3 cup)
• 1 tablespoon tahini
• Pinch of sea salt
• Parsley for garnish
Steamed Vegetables with Orange Sesame Dressing
• Whisk orange juice, tahini and salt together until smooth. If dressing is too thick add a few tablespoons of water to thin.
• Cut asparagus into 5-cm lengths, discard tough ends. Peel and cut carrots into roughly the same size as asparagus. Cut caulifl ower into bite-sized pieces. In a vegetable steamer add the carrots fi rst and steam for fi ve to seven minutes. Add the caulifl ower, steam for another fi ve to seven minutes. Add the asparagus and steam for an additional fi ve minutes or until are vegetables are cooked to desired fi rmness.
• Toss vegetables with Orange Sesame Dressing and serve.
smooth. If dressing is too thick add a few tablespoons
Cut asparagus into 5-cm lengths, discard tough ends.
Vegans Have Fun, Too
Leap_Winter12_p06-11.indd 8 11/20/12 10:32:37 AM
More than 600 Albertans survive cancer each year who would not have survived had they developed cancer 25 years ago.
More than 50 new cancer research projects ranging from investigating cancer mechanisms at a molecular level to increasing pain control for patients were launched last year, in addition to the hundreds receiving ongoing funding from the Alberta Cancer Foundation.
rural Alberta women have access to digital mammography screening through mobile units funded by the Alberta Cancer Foundation.
grants were given to patients and families in fi nancial need during treatment.
Albertans are participating in more than 200 clinical trials across the province, spanning all cancer types.
healthy Albertans will teach us more about cancer by volunteering to participate in the Tomorrow Project research study funded by the Alberta Cancer Foundation.
endowed chairs have been established in Alberta ranging from research on melanoma to palliative care.
Progress…
thanks to donors like you
albertacancer.ca
A common virus that leaves healthy people feeling under the weather could be part of the foundation for a new treatment of multiple myeloma. Naturally-occuring reovirus typically manifests as fl u-like symptoms such as respiratory infection. Alberta researchers are fi nding that the reovirus can kills myeloma cells.
In an Alberta Cancer Foundation-funded study published in the August issue of the journal Clinical Cancer Research, scientists injected the reovirus into animal models containing human multiple myeloma cell lines. Unlike conventional cancer treatments, such as radiation therapy and chemotherapy, which kill both cancerous and healthy cells, researchers found the virus targeted the cancer cells while leaving the normal, healthy cells alone.
Multiple myeloma, which represents about one per cent of all cancers, occurs when an accumulation of abnormal plasma cells in the bone marrow interferes with the production of normal blood cells.
Hope for Multiple Myeloma“We’re not into human trials with this yet but it’s
certainly where we’re heading,” says Dr. Don Morris, lead author of the study, medical oncologist and a member of the University of Calgary’s Southern Alberta Cancer Research Institute.
Morris says the treatment might be used in future in conjunction with other cancer therapies. “We’ve recently found that the combination of reovirus and other new therapies currently used in the treatment of myeloma work better together,” he says.
“Reovirus has the ability to multiply within the cancer cells unlike chemotherapy drugs, which have a dose limitation due to side eff ects to the patient,” says Chandini Thirukkumaran, PhD, fi rst author of the study, research assistant professor in oncology and member of the University of Calgary’s Southern Alberta Cancer Research Institute.
Some experts estimate there will be approximately 2,400 new cases of multiple myeloma in Canada this year − 230 of them in Alberta.
Leap_Winter12_p06-11.indd 9 11/21/12 9:54:22 AM
myleapmagazine .ca10 winter 2012
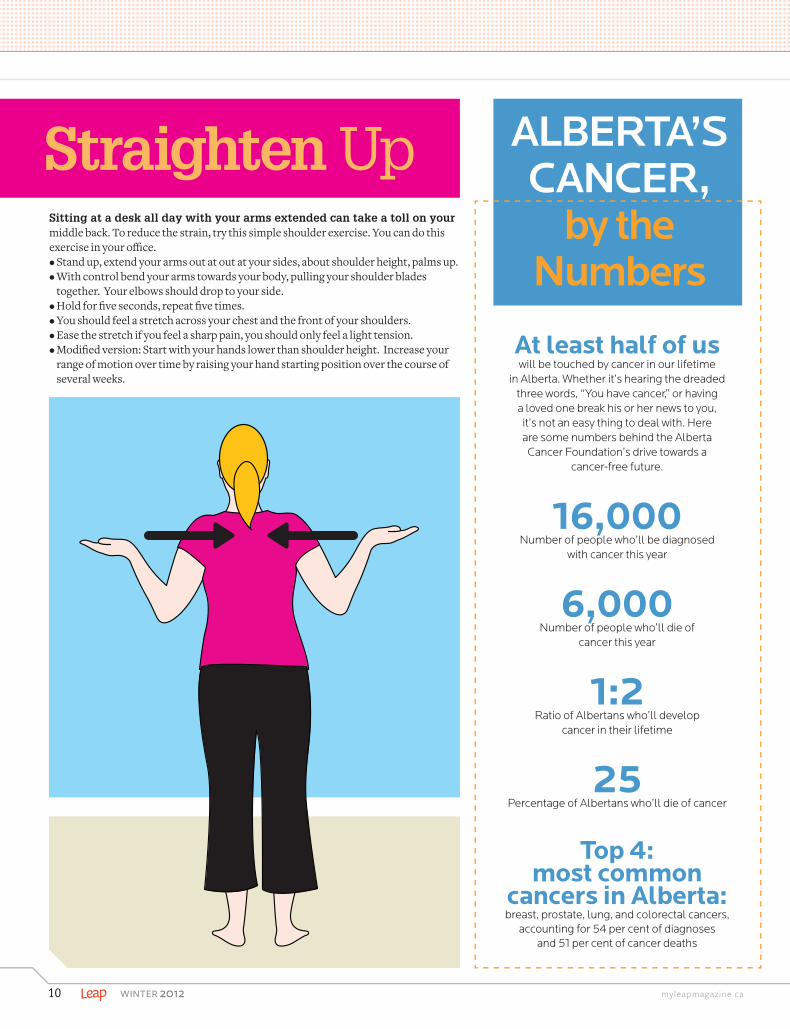
Sitting at a desk all day with your arms extended can take a toll on your middle back. To reduce the strain, try this simple shoulder exercise. You can do this exercise in your offi ce.• Stand up, extend your arms out at out at your sides, about shoulder height, palms up.• With control bend your arms towards your body, pulling your shoulder blades
together. Your elbows should drop to your side.• Hold for fi ve seconds, repeat fi ve times.• You should feel a stretch across your chest and the front of your shoulders.• Ease the stretch if you feel a sharp pain, you should only feel a light tension.• Modifi ed version: Start with your hands lower than shoulder height. Increase your
range of motion over time by raising your hand starting position over the course of several weeks.
Straighten Up
At least half of uswill be touched by cancer in our lifetime
in Alberta. Whether it’s hearing the dreaded three words, “You have cancer,” or having a loved one break his or her news to you, it’s not an easy thing to deal with. Here are some numbers behind the Alberta Cancer Foundation’s drive towards a
cancer-free future.
16,000 Number of people who’ll be diagnosed
with cancer this year
6,000 Number of people who’ll die of
cancer this year
1:2Ratio of Albertans who’ll develop
cancer in their lifetime
25 Percentage of Albertans who’ll die of cancer
Top 4: most common
cancers in Alberta: breast, prostate, lung, and colorectal cancers,
accounting for 54 per cent of diagnoses and 51 per cent of cancer deaths
ALBERTA’S CANCER,
by the Numbers
Leap_Winter12_p06-11.indd 10 11/20/12 10:34:01 AM

A l b e r t a ’s c a n c e r - f r e e m o v e m e n t winter 2012 11
PINK CHAIROne of the most signifi cant legacies of the great, 60-kilometre-walk fundraiser is the funding of Weekend to End Women’s Cancers Chair in Breast Cancer Research. Dr. Christine Friedenreich has fi lled this chair and her expertise and interest make her a perfect fi t.
Dr. Friendenreich is a pioneer in the fi eld of exercise and cancer. Long before the benefi ts of exercise became common knowledge, she was investigating the infl uence of physical activity on cancer control across the spectrum of the cancer journey – from prevention to diagnosis to survivorship.
Stay tuned for more information on the work she has planned to enhance the provincial breast cancer care programs in this province.
Holiday GivingIn your search for the perfect gift this holiday season there are many reasonsto consider giving a donation in lieu of another pair of socks under the tree. You can choose to give because a family member recently had a cancer journey, in memory of a loved one, or in the hope of a new discovery. Often choosing to donate is done in the spirit of shared celebration and the holidays are the perfect time to celebrate the bonds that connect us.
The simplest way to donate in honour of someone is to visit the Alberta Cancer Foundation website albertacancer.ca. When fi lling out the donation form, choose to have a letter sent to the honouree by fi lling in their mailing address and name. The honouree will receive a letter telling them about the donation. However, the amount of the donation is not disclosed.
As the donor you will receive a tax receipt for the donation. Also, as donor you can choose to give to general research or have the donation directed to a favoured program by calling Alberta Cancer Foundation at 1-866-412-4222.
At a black-tie gala on in November, Dr. Gregory Cairncross was awarded a prize for Outstanding Leadership in Alberta Science for his work in brain cancer research. In front of 700 guests he was presented the award from ASTech, the Alberta Science and Technology Foundation, celebrating innovation in science and technology. Cairncross made advances in the treatment of a kind of brain cancer, doubling the lifespan and improving the quality of life of patients.
Also honoured, this time in the team effort category, was Dr. Gino Fallone’s team, which has been creating new vistas for radiotherapy for cancer treatment. The team applied CT-based image guidance for radiotherapy, addressing the limitations of that system. By introducing MRI guidance for radiotherapy, managing to couple an MRI with a Linear Accelerator (LINAC) to produce optimal images and an effective radiation device, they achieved a world fi rst.
ASTech is a not-for-profi t organization funded in part by the Government of Alberta and supported by more than 20 major patrons. Since inception in 1989, the ASTech Foundation has provided more than $1.3 million in awards recognizing Alberta’s science and technology community. The theme of this year’s ASTech Awards show was “Everyday Heroes,” celebrating the heroes behind the homegrown discoveries, breakthroughs and advances that are changing our world for the better.
CongratulationsCongratulationsAre in Order
Leap_Winter12_p06-11.indd 11 11/20/12 4:47:15 PM
MAKING POSITIVE CONNECTIONSbodymind /
of a person’s diet, rather than as supplements. Other NHPs have potential for improving treatment outcomes when combined
with standard therapies. These include Coriolus versicolor mushrooms (also known as PSK and turkey tail), shiitake mushrooms, melatonin (a sleep hormone taken as a pill), and fl ax seed and oil. Others, such as ginseng root, may improve chemotherapy effectiveness, and the mineral strontium may help reduce cancer-related bone pain. The caveat for all of these products is that more research is necessary to pinpoint how much is helpful for which types of cancer, and when to introduce them to the treatment process.
These products aren’t necessarily benign: natural doesn’t always mean safe. There can be interactions with medications you are be taking, contraindications, and the potential for overdose. Check that products have a Health Canada label certifying their contents. Sometimes you may get a product that isn’t what it says, or is contaminated, or has fi llers and different ingredients. Memorial-Sloan Kettering Cancer Centre has a great online database where you can look up products and see what the contraindications and drug interactions are, and to check dosage. Finally, let your doctor and pharmacist know which NHPs you are taking.
These products are not necessarily benign: natural does not always mean safe.
The general public and cancer patients specifi cally have a huge interest in the use of so-called natural health products (NHPs). Of course we want to know if they’re helpful and when we should use them. Beyond that, we want to know which ones to use and how. There’s a lot of information available online, but it can be overwhelming and confusing trying to make sense of what’s what in a world where everyone is trying to make a profi t.
The first thing we should figure out is what they are. NHPs are the most commonly used category of complementary therapies in cancer care, and include vitamins, minerals, food products, food derivatives and some hormones. They’ve been touted as curative and preventive, treating a variety of cancers and other conditions. But what’s the reality? I wanted to fi nd out more, and as I began looking at the scientifi c evidence, I realized there was a lot of really good information out there. I didn’t have the time to find, read and digest it all. So I hired a student, Ngaire King (winner of the Alberta Cancer Foundation’s Linda Singleton Summer Studentship), who spent four months this past summer reviewing the scientific literature on NHPs and making summaries to help me and others get a handle on what the research was saying.
The results were encouraging, and staggering. King carefully reviewed almost 900 scientifi c studies that investigated 72 NHPs. Most of these studies were in the context of cancer prevention, but many patients used NHPs to treat symptoms and side effects of cancer treatments. Some studies investigated NHPs as providing potential survival advantages when combined with conventional therapy. The Top-10 list of most-studied therapies emerged, and some stood out for helping to reduce risk for getting a variety of cancers. These include green tea, garlic, calcium, lycopene (found in tomatoes), Vitamin A, Vitamin C, Vitamin D, soy, folic acid (folate) and beta-carotene (orange vegetables). These seemed to help most in reducing cancer risk when consumed in foods as part
Dr. Linda Carlson (lindacarlson.ca) is the Enbridge Chair in Psychosocial Oncology at the University of Calgary and a clinical psychologist at the Tom Baker Cancer Centre.
myleapmagazine .ca12 winter 2012
BY LINDA E. CARLSON
Naturally Curious
myleapmagazine .ca
Are so-called natural health products benefi cial for your health or just hard on your pocketbook?
FIND OUT MORE! Memorial-Sloan Kettering Cancer Centre’s NHP database is worth a visit: http://www.mskcc.org/mskcc/html/11570.cfm. And we provide seminars on complementary therapies at the Tom Baker Cancer Centre’s auditorium, usually on the third Wednesday afternoon of each month. Call 403-355-3207 to confi rm dates and times.
Leap_Winter12_p12-13.indd 12 11/20/12 10:34:48 AM

SIFTING THE INFORMATIONHow do you sort through all the diet information available on the web, television or magazines in the checkout line at the grocery store? Ask yourself these questions:• Is someone trying to sell you something such as a book, food product or
supplement?• Is there research to support the claims or is it just personal opinion or
testimonial? • Is the research recent and is it documented?• Who is promoting the information? Is it a health professional such as a
doctor, registered dietitian, physiotherapist or pharmacist? • Does it sound too good to be true?
FOOD FOR LIFEcookingsmart /
Everywhere you turn, there’s another food productor cookbook that promotes gluten-free eating. Restaurants offer gluten-free selections. You read about celebrities attributing their weight loss or improved health to a gluten-free diet. Is this a trend or a healthier way to live? What is gluten and why would you need to avoid it?
Gluten is a protein that’s found in many grains – wheat, rye, barley – and in foods made with these grains, such as fl ours, bread products, pasta, breakfast cereals, cakes, cookies and condiments. Oats are naturally gluten-free but may contain gluten when processed in a facility that also processes wheat.
There are groups of people who must avoid gluten. They are people with celiac disease and people with non-celiac gluten sensitivity. Estimates indicate that about one per cent of the western population has celiac disease and it affects more females than males. It’s an autoimmune disorder, meaning the immune system attacks itself. When someone has celiac disease and eats food with gluten, it damages the intestinal wall. The body is then unable to absorb vitamins such as folate and minerals such as calcium and iron. The result is bloating, abdominal pain, diarrhea, constipation, migraines, depression and mouth ulcers. Over time, gluten in the diet of people with celiac disease can lead to osteoporosis, anemia, infertility and even cancer. But following a strict gluten-free diet for life can lead to healthy intestines and freedom from both symptoms and long-term health problems.
Non-celiac gluten sensitivity is a non-allergic and non-autoimmune response to gluten. Between six and nine per cent of the population has gluten sensitivity. Symptoms can vary. The most common is abdominal pain and other symptoms similar to celiac disease. But exposure to gluten does not damage the intestines.
Celebrities have promoted a gluten-free diet as it is a great way to lose weight. But grains without gluten, such as corn, millet, quinoa and rice, are similar in calories to the gluten-containing grains. A gluten-free cookie has a similar nutritional content and calorie count as a similar cookie without gluten, and it’s no more healthful.
Before you go gluten-free, consider a few points. If you think you have celiac disease, see your doctor to be
screened for it before cutting gluten out. Symptoms associated with celiac disease are the same as those of many other things, from overeating to lactose intolerance. Getting properly diagnosed is important.
The best strategy for losing weight and keeping it off is to work with a registered dietitian on an eating plan that fi ts your lifestyle. A dietitian can also help you sort through nutritional information to find solid research behind the recommendations.
So before you head to the grocery store to purchase gluten-free bread or remove all the wheat fl our and gluten-containing products from your cupboards, ask yourself if the drastic change is necessary for a long-term healthy weight and lifestyle. Eating well can be simple, but it’s not easy at fi rst. It takes time and practice preparing and eating foods from each of the food groups as recommended by Canada’s Food Guide.
Karol Sekulic is a registered dietitian with Alberta Health Services who has expertise and interest in the areas of weight management, nutrition and communications.
A l b e r t a ’s c a n c e r - f r e e m o v e m e n t winter 2012 13
BY KAROL SEKULIC
The Wheat from the ChaffSeparating the fads from facts is necessary before you take a step like cutting gluten out of your diet
Leap_Winter12_p12-13.indd 13 11/20/12 10:35:07 AM
myleapmagazine .ca14 winter 2012
BEFORE IT STARTSLeap consults the experts to fi nd answers to your questions about an herbal remedy, screening and exercise for cancer prevention
Both tests are useful in different ways, explains radiologist Maureen Hutson, MD, F.R.C.P., of Edmonton’s Medical Imaging Consultants. While mammography has proven useful in screening for breast cancer, ultrasound has not been established as a routine method to screen for breast cancer, instead it is useful for evaluating breast tissue.
“A mammogram is performed using X-rays to ‘see through’ the breast tissue,” Hutson says. “Usually only two views of each breast are performed, but sometimes the technologist has to perform some extra X-ray views so that the tissue of the breasts can be adequately assessed.”
An ultrasound differs because sound waves are used to create images of tissue instead of X-rays. “Ultrasounds can show differences between solid tissue, including normal tissue and solid nodules, and fl uid-fi lled tissue such as cysts. It can also evaluate breast ducts,” she says.
Hutson says it’s likely the radiologist who read the specifi c mammo-gram in question probably saw a rounded nodule or area of distorted tis-sue in one of the breasts. Other reasons for more testing include when your family physician indicates there is a palpable abnormality in one breast or nipple discharge.
In these situations, as a radiologist, Hutson would want to further assess the area with a breast ultrasound in order to look for a possible solid nodule, fl uid-fi lled cyst or duct abnormality. If once of those three fi ndings appears in an ultrasound, a radiologist may recommend a nee-dle biopsy of the area under the guidance of ultrasound to evaluate for any early signs of breast cancer.
Hutson says it’s important to remember that most patients recalled for further imaging after a mammogram typically have normal or benign fi ndings. “The radiologist is just being very careful to not miss a fi nding which could indicate very early, and therefore, very treatable breast cancer,” she says.
After my mammogram, they called me back in for a breast ultrasound. What’s the difference? What were they looking for?
asktheexpert / A RESOURCE FOR YOU
Alberta Health Services’ (AHS) website “Screening for Life”explains cancer-screening practices in our province. Who should be screened and what type of cancer to search for is determined by age and sex since most tests are done on people who don’t have cancer symptoms. Screening is meant to point out early signs of the disease and abnormal cell changes (not cancerous yet, but could become so over time) because early detection makes treatment more effective.
AHS health promotion specialist Fazilah Shariff, MSW, says current screening programs are restricted to breast, cervical and colorectal cancers because not enough evidence yet shows that screening for other cancer types, across large populations, effec-tively reduces the number of cancer diagnoses or deaths. “However,” Shariff says, “tests for cancers such as prostate, skin or ovarian cancer may still be useful on an individual basis, depending on your personal history.”
Risks to screening include false positives, and Shariff stresses the importance of speaking with your healthcare provider about your concerns to be able to make a better-informed and person-alized plan regarding cancer screening. See screeningforlife.cafor more information.
What are the cancers that are routinely screened for in Alberta? Why?
BY MICHELLE LINDSTROM
Leap_Winter12_p14-15.indd 14 11/20/12 10:35:55 AM

A l b e r t a ’s c a n c e r - f r e e m o v e m e n t winter 2012 15
Saw palmetto is a palm tree found in the West Indies and in coastalregions of the southeastern United States, the berries of which are used in herbal remedies, explains Dr. Linda E. Carlson, Enbridge research chair in psychosocial oncology and associate professor at the University of Calgary.
“Native Americans used the herb to treat problems of the urinary tract, such as trouble urinating or frequent nighttime urination,” she says.
Clinical studies have shown saw palmetto relieves some symp-toms of benign prostatic hyperplasia (BPH), or enlarged prostate, such as diffi cult and frequent urination. To clarify, she says that BPH is not prostate cancer and saw palmetto has not been shown to lower prostate cancer risk – although more research is needed in this area.
Saw palmetto supplements are very popular in Europe where doctors often prescribe them for BPH treatment. Also popular in the U.S. and Canada, they are not approved for use as BPH treatment here. Although uncommon, side effects can include headache, nau-sea, vomiting, upset stomach, dizziness, constipation or diarrhea, trouble sleeping and fatigue. Its long-term effects and safety have not been studied in detail, but many men use it without incident.
“Men who have symptoms that might be caused by BPH, such as diffi cult, frequent or urgent urination, should see a doctor as soon as possible rather than treating themselves with saw palmetto alone,” Carlson says. “These symptoms can also result from prostate cancer or other serious conditions, and self-treatment with saw palmetto alone could delay diagnosis and treatment.”
My husband is taking saw palmetto from the health food store for an enlarged prostate. Is it safe?
Ask our experts questions about general health, cancer prevention and treatment. Please submit them via email to [email protected]. Remember, this advice is never a substitute for talking directly to your family doctor.
“The exact type, dose and timing in life when exercise is most benefi cial for reducing the risk of developing chronic diseases, such as cancer, is not entirely known,” says Dr. Christine Friedenreich of the University of Calgary’s Faculty of Medicine and Faculty of Kinesiology. She says evidence shows that all types of physical activ-ity (e.g., occupational, household and recreational) are benefi cial for reducing risk but sustaining recreational activity for longer durations more benefi cial.
Evidence of the benefits to increasing the frequency and dura-tion – the dose – of an activity has already been found to lower breast cancer risk.
“A moderate-intensity activity reduces breast cancer risk by 15 per cent and vigorous activity by 18 per cent,” Friedenreich says. “With respect to the duration of activity needed to reduce breast cancer risk, there is a clear dose-response effect with an eight per cent risk reduction with two to three hours per week; 14 per cent for three to four hours per week; and 28 per cent for 6.5 hours per week or more.”
At what point in life does physical activity become most associated with cancer risk reduction? Friedenreich says, sustained lifelong activity offers the greatest benefits however, activity later in life is also very benefi cial even if it is preceded by lower levels of activity. “The evidence on physical activity and cancer prevention is particu-larly strong for colon, breast and endometrial cancers,” she says. “There is also considerable evidence that activity may reduce the risk of prostate, ovarian and lung cancers.” It’s never too late to start mov-ing and reduce your risk of cancer.
Are the health benefi ts the same for mild-to-moderate exercise as they are for moderate-to-intense?
Leap_Winter12_p14-15.indd 15 11/20/12 10:36:03 AM

myleapmagazine .ca16 winter 2012
Top Job
Leap_Winter12_p16-19.indd 16 11/20/12 10:37:06 AM
A l b e r t a ’s c a n c e r - f r e e m o v e m e n t winter 2012 17
BY MICHAEL HINGSTON / PHOTOGRAPH BY CURTIS TRENT
Speech pathologist Anna Sytsanko leads a group of cancer patients whose treatment means a new approach to talking and eating
Meals
On a Wednesday afternoon in the fall, a dozen people sit around a boardroom table in Edmonton’s Cross Cancer Institute, talking about bread. A man in his 30s scratches his thinning beard
and says he can’t open his mouth wide enough to eat a Subway sandwich anymore. Several others say they’ve had to give up bread altogether – it’s too thick and dry to swallow. Through it all, Anna Sytsanko sits at the head of the table and off ers tips and advice. She’s the founder of this swallowing therapy support group for cancer patients, and it’s just one of the ways she lets her patients guide their own care.
The fi rst thing Sytsanko does when she meets a new patient is ask what they want to get out of the treatment. She’s a speech-language pathologist, which means it’s her job to help cancer patients who are having trouble swallowing, speaking, or both.
Of andConversation
Leap_Winter12_p16-19.indd 17 11/20/12 10:37:21 AM
18 winter 2012 myleapmagazine .ca
“Working in a group helps patients achieve their goals faster,” Anna Sytsanko says.
Sometimes this is a direct result of their illness, as when the cancer is located in the mouth or throat. And sometimes it’s a side eff ect of radiation or chemotherapy treatment for cancer found elsewhere in the body, which can impair the body’s ability to produce saliva.
Either way, Sytsanko says, it’s important to let the patient take the lead. “If they’re happy with their situation,” she says, “we have to respect that.”
Sytsanko was born and raised in Russia. As an undergraduate, she studied linguistics at Tyumen State University, before she immigrated to Canada in the 1990s. She received a master’s degree from the University of Alberta in 2004. She was drawn to speech-language pathology because of the breadth of work – it’s estimated that one in 10 Canadians over 50 has some type of swallowing disorder – and because it meant she could work in a hospital setting alongside several other related disciplines. She’s been with the Cross Cancer Institute since 2007.
The occasional reluctant patient aside, Sytsanko says that the bulk of her patients are indeed ready and willing to work to improve their situation – and a surprising number of their goals are built around eating and drinking.
“Often they say, ‘I just want to eat a salad again,’ ” Sytsanko says. “Or ‘I just want to have Christmas dinner with my family.’ So that’s what we set as the goal, and then there are little steps we can take to accomplish it.” Those steps can include a regimen of physical and mental exercises, as well as adjustments to their daily routines. If they can’t get back to normal, Sytsanko works with them to fi nd a new normal.
Eating, she says, is a highly ritualized part of our culture. To have any part of that ritual thrown off – whether because you have to use a feeding tube, or simply because it takes you two hours to chew and swallow a meal – can lead to embarrassment and social isolation, and even malnutrition.
In fact, most of Sytsanko’s stories about her patients’ successes involve food. That’s because if you’re struggling to swallow correctly, something as simple as relearning to eat a cookie, or even ice chips, can feel like a major breakthrough. “Speech pathology is very good at encouraging people,” she says.
The importance of food and drink was made particularly clear at the support group meeting. This is an opportunity for several hospital staff – including Sytsanko, a dietitian, and a nurse practitioner – to treat a group of similar patients all at once.
Attendees to these informal sessions take turns discussing how they’ve been feeling that week, along with reports of any new symptoms or concerns. The staff ask questions as needed, while Sytsanko acts as a
kind of moderator. There’s plenty of time for patients to bounce ideas off of one another, too. And by far the most popular topic is food: specifi cally, what items each patient can or can’t eat.
“You should try French toast drenched in maple syrup,” one patient says. “It’s the best way to keep eating bread.” Her husband, who is at the meeting with her, nods his agreement.
Another patient, holding an extra-large Tim Hortons white hot chocolate – everyone carries some kind of beverage to combat dry mouth – says she doesn’t like French toast.
The fi rst woman’s husband replies, “Ah, but you’ve never had my French toast.”
Meeting with patients as a group isn’t simply a matter of effi ciency for the staff . The group setting also provides a huge benefi t to the patients, Sytsanko says. When a cancer patient talks to Sytsanko one-on-one, he may be skeptical or unsure of his ability to ever improve. But it’s completely diff erent when he’s surrounded by a group of peers. “They can provide experience and suggestions to one another,” she says. “It helps patients
achieve their goals faster, and they often work harder.”
In fact, in the four years Sytsanko has run this particular
group, she can only think of one or two patients who didn’t want to come. Despite some language barriers, there’s camaraderie in the air.
One of the attendees this week is Barbara Riddell, a 67-year-old who drives up with her husband from Leduc every Wednesday afternoon. She was diagnosed with tongue cancer in 2011, and began radiation treatment at the Cross Cancer Institute that August. Riddell’s doctors had to replace part of her tongue with skin and muscle grafted from the inside of her left wrist, but she was still having trouble moving food around. That’s when she met Sytsanko.
“I’ve found her to be a warm, caring person,” Riddell says. “And very concerned: if she didn’t have an answer for you, she’d fi nd out and get back to you.” Riddell points out that at the meeting we’ve just stepped out of, Sytsanko had been in and out of her chair fetching headphones, voice recorders, and printed material for the attendees.
Riddell likes to think of her experience with cancer as a journey. “A lot of days it feels like you’re walking on a gravel road in your bare feet. But then, all of a sudden, you get a wonderful day on pavement. You know that there’s still more gravel roads – or sometimes you hit a ditch. But further down the road there’s more pavement.”
And thanks to Sytsanko and the others, Riddell says, “Right now I’m travelling on a lot of pavement.”
treatment for cancer found elsewhere in the body, which can impair the body’s ability to produce saliva.
Either way, Sytsanko says, it’s important to let the patient take the lead. “If they’re happy with their situation,” she says, “we have to respect that.”
Sytsanko was born and raised in Russia. As an undergraduate, she studied linguistics at Tyumen State University, before she immigrated to Canada in the 1990s. She received a master’s degree from the University of Alberta in 2004. She was drawn to speech-language pathology because of the breadth of work – it’s estimated that one in 10 Canadians over 50 has some type of swallowing disorder – and because it meant she could work in a hospital setting alongside several other related disciplines. She’s been with the Cross Cancer Institute since 2007.
The occasional reluctant patient aside, Sytsanko says that the bulk of her patients are indeed ready and willing to work to improve their situation – and a surprising number of their goals are built around eating and drinking.
“Often they say, ‘I just want to eat a salad again,’ ” Sytsanko says. “Or ‘I just want to have Christmas dinner with my family.’ So that’s what we set as the goal, and then there are little steps we can take to accomplish it.” Those steps can include a regimen of physical and mental exercises, as well as adjustments to their daily routines. If they can’t get back to normal, Sytsanko works with them to fi nd a new normal.
Eating, she says, is a highly ritualized part of our culture. To have any part of that ritual thrown off – whether because you have to use a feeding tube, or simply because it takes you two hours to chew and swallow a meal – can lead to embarrassment and social isolation, and even malnutrition.
In fact, most of Sytsanko’s stories about her patients’ successes involve food. That’s because if you’re struggling to swallow correctly, something as simple as relearning to eat a cookie, or even ice chips, can feel like a major breakthrough. “Speech pathology is very good at encouraging people,” she says.
The importance of food and drink was made particularly clear at the support group meeting. This is an opportunity for several hospital staff – including Sytsanko, a dietitian, and a nurse practitioner – to treat a group of similar patients all at once.
Attendees to these informal sessions take turns discussing how they’ve been feeling that week, along with reports of any new symptoms or concerns. The staff ask questions as needed, while Sytsanko acts as a
Top Job
Leap_Winter12_p16-19.indd 18 11/20/12 4:47:40 PM
A l b e r t a ’s c a n c e r - f r e e m o v e m e n t winter 2012 19
STORIES OF SURVIVORSHIPbeyondcancer /
When cancer treatment ends, many survivors aren’t clear about who will provide their care going for-ward and wind up feeling a bit lost as they try to navi-gate their way back to their normal lives. In 2006, the Institute of Medicine published a report titled, “From Cancer Patient to Cancer Survivor: Lost in Transition.” It recommended that all survivors – in conjunction with primary care providers – receive a “survivor care plan” as they leave active treatment. It recommended that each survivor receive information about their diagnosis and treatment, recommended follow-ups, preventive practices, legal protections, and availability of psycho-social services.
In the United States, The American College of Surgeon’s Commission on Cancer intends to mandate that all accredited institutions provide care plans to survivors by 2015. A number of organizations provide access to online care plan templates, so survivors can fi ll out the details of their diagnosis and treatment and receive a printout of recommendations. For example, LIVESTRONG™ has a web-based tool allowing survi-vors to generate care plans. The American Society of Clinical Oncology’s (ASCO) care plan templates inte-grate their recommendations to guide care. Journey Forward’s templates tailor educational materials and resources to the survivor. Our group at CancerBridges reviewed these templates and found that, while they had some great information for survivors, they are ori-ented to the American health system.
In Canada, although we have no similar mandate and no easily accessible web-based templates, most provinces are beginning to facilitate some form of can-cer survivor care plans. In Alberta, CancerBridges was fortunate to receive money through the Canadian Partnership Against Cancer to create and deliver care plans to a pilot group of breast and head-and-neck survivors. Based on the success of the pilot, we’ve pro-posed to extend the delivery of care plans to all survi-vors across the province. (See “Good Planning,” left.)
These individualized care plans would be printed and handed to survivors, faxed to the family physician, and scanned into the oncology record so that each of these people, important in the care of the survivor, is on the same page at the end of active treatment.
Research demonstrates that longer survival, higher quality of life, and faster return to work are possible for
cancer survivors who adhere to treatment and follow-up, commit to lifestyle chang-es such as an active lifestyle, healthy eating and stress reduction, receive psychoso-cial support, and reduce their depression levels and symptom burden.
At CancerBridges we are advocating for survivor care plans and consistent mes-sages to survivors during and following active treatment. We hope to improve com-munication with care plans and to address these changes in recommended pro-grams during this critical post-treatment phase.
BY JANINE GIESE-DAVIS
SURVIVOR CARE PLANSThe case for providing patients with a road map to guide them after active treatment
GOOD PLANNING
In Alberta, we included templates in our care plan for breast and head-and-neck cancer survivors. We found several items that we considered to be cru-cial to the document.• Diagnosis and treatment • A brief medical history including chronic diseases and allergies• A list of current pre-
scribed and over-the-counter medications, vitamins, and other therapies
• Guidelines for survivors’ follow-up care, a list of next follow-up appoint-ments and who will provide surveillance within the health system,
• List of the survivors’ family physician, surgeon, medical and radiation oncologist, nurses, social workers, psychologists, dieticians, and others, along with their locations and phone numbers
• Signs of possible recurrence and cancer spread• Management of physical and psychosocial treatment-related side effects • A list of the survivors’ side effects and treatment plan• An interactive section on coping and adjustment that allows survivors to
indicate their levels of distress so nurses could refer them appropriately• Interactive section on managing health after treatment allowing survivors
to prioritize goals and action plans for physical activity, diet, weight, alco-hol, and smoking
• Interactive section on managing the transition: goals, and action plans for relationships and support, intimacy and sexuality, spirituality, fi nances, employment, and retirement
• A section to highlight other strengths and needs
Leap_Winter12_p16-19.indd 19 11/20/12 10:37:44 AM

myleapmagazine .ca20 winter 2012
The sharpest tool the surgical oncologist has on hand at the operating
table is information
f Terry Fox were diagnosed today, not only would he probably survive the cancer but he might be running without a prosthetic, too.
That’s according to one of Canada’s leading surgical oncologists, Dr. Walley Temple, who came to Calgary’s Tom Baker Cancer Centre in 1983 and has been a major player in the fi eld’s rapid evolution. In those three decades, he watched the centre go from three surgeons dealing with tumours – two gynecologists and himself – to approximately 30. And he’s witnessed treatments and cure rates of specifi c cancers improve at a similar pace.
In the case of the Canadian hero who died at 22 of osteosarcoma, a malignant bone tumour that most commonly aff ects adolescents, systemic chemotherapy could have reduced the size of the leg tumour and the disease might not have spread to his lungs. Not only could it have greatly limited the required surgery, but artifi cial parts could have rebuilt his leg from the inside so that a prosthetic wasn’t necessary.
Temple is the director of Cancer Surgery Alberta. And despite a reputation as a jokester, he is serious in his desire to limit the number of times surgeons reach for the scalpel. “Surgical oncology,” says Temple, “is looking at how you can do less surgery with better results.” So today, a young man diagnosed with osteosarcoma has an 85 per cent chance of recovery – almost double what it was at the time of Fox’s diagnoses – and only a two per cent chance of requiring amputation, when in the 1980s it was 20 per cent.
Other technological advancements to roll into the Tom Baker Centre and Edmonton’s Cross Cancer Institute include robotic surgery tools that allow for precision in constrained areas; tools that cauterize blood vessels automatically;
I
Beyondthe Blade
BY OMAR MOUALLEM / PHOTOS BY EWAN NICHOLSON
Transforming CANCER
Leap_Winter12_p20-23.indd 20 11/20/12 10:38:52 AM

A l b e r t a ’ s c a n c e r - f r e e m o v e m e n t winter 2012 21
MEETING OF MINDS: Dr. Walley Temple, in the glasses, attends a multidisciniplary team meeting aimed at treating the whole patient.
Leap_Winter12_p20-23.indd 21 11/20/12 10:39:01 AM

myleapmagazine .ca22 winter 2012
surgical simulation hand sensors used in training to measure the amount of force used by a resident surgeon; and hot (40˚C) chemotherapy treatments that bathe the abdominal cavity after a tumour is removed multiply the drug’s strength as a cancer killer by 50 to 100 times – a method that Temple and his University of Calgary team pioneered.
At Cancer Surgery Alberta, a body to create and standardize surgical cancer care, Temple helped found a web-based network of surgeons to compare results for improved future outcomes and knowledge translation.
But most of the “phenomenal progress” Temple has witnessed is not the result of anything turbo charged, nor any great leap by a genius scientist working solo in a lab. The great innovation – cancer surgery’s big leap is “a multidisciplinary approach, where we no longer work in silos.” To that end, the greatest advancement he’s seen in cancer medicine is the holistic weaving of all the three modes of cancer treatments – radiation, chemotherapy and surgery. He says, “Surgery is very challenging,
technical and requires the utmost of the entire team.”Dr. Todd McMullen, a Cross Cancer Institute
surgical oncologist specializing in endocrine cancers, says Temple was instrumental in pushing the fi eld in this multidisciplinary direction, and he reserves high praise for him. “He’s one of the key fi gures who established surgical oncology to Canada and pushed it forward as a specialty where it wasn’t just about the surgery but understanding the nature of oncology, tumours, their natural history, their behaviour, and a multidisciplinary approach.”
McMullen is the director and adjunct professor of the department of oncology at the University of Alberta. Like Temple and many other doctors at Alberta’s leading cancer clinics, he holds cross-appointments across institutions. “Surgical oncology is not just the surgery, it’s knowing when to operate so that you integrate what you plan to do with the radiation oncologists and the medical oncologists,” McMullen says. “So the plan is made by a group of physicians instead of just a surgeon saying, ‘OK. You’ve got something that we’re going to try to take out.’ ”
Every week at Alberta’s two major cancer centres, 30-plus oncologists, as well as pathologists, specialized nurses and sometimes psychosocial profes-sionals sit on a tumour board.
At the roundtable meeting, the group closely exam-ines the condition of every newly registered patient so that each expert with something to contribute, does. From beginning to end, the roundtable will abruptly switch gears as many as a dozen times, from a patient with an abdominal tumour to one with a tumour of the
limb to another with gastrointestinal tumours or sarcoma of the lungs. “We go every-where in the body,” says Temple. “It’s become a very intense ‘lookup’ of each patient to make sure we deliver the best possible treatment.”
He adds, “That’s our role: To keep interpreting the new possibilities of other modalities to provide a totally diff erent solution.”
Traditionally, McMullen says, professionals simply presented patients with the numbers – the statistics of survival based on a whole population. “Now we’re tailoring our therapy,” he says. “It’s very nice to give patients detail and say, ‘We’ve done an in-depth analysis and for you we think this is the best treatment,’ instead of, ‘Well this is what works for everyone else.’”
Esther Harris, an 87-year-old writer and retired academic, knows the story all too well.
In 2003, she was living in Vancouver when her gynecologist referred her to a hematologist after fi nding an alarmingly high white blood cell count. “I walked into his offi ce and 10 seconds later he told me I was going to die,” she recalls. The diagnosis was non-Hodgkin’s lymphoma, which can attack any tissue in the immune system. “He said, ‘I don’t think we can give you any of the chemotherapies because, at your age, they will probably kill you.’ ”
This was not the fi rst time she’d been diagnosed with cancer. Fifteen years prior, she
“Surgical oncology,” says Dr. Walley Temple, “is looking at how you can do less surgery
with better results.”
LIGHT HEARTED: Dr. Walley Temple makes humour a part of his stressful job of surgical oncology.
surgical simulation hand sensors used in training to measure the amount of force used by a resident surgeon; and hot (40˚C) chemotherapy treatments that bathe the abdominal cavity after a tumour is removed multiply the drug’s strength as a cancer killer by 50 to
Transforming CANCER
Leap_Winter12_p20-23.indd 22 11/20/12 4:48:24 PM
The tumour group examines the condition of every newly registered
patient so that each expert with something to contribute, does.
developed a tumour close to her eye and had to have her eyelid surgically removed and replaced with a skin graph from behind her ear. Throughout it all, she ploughed through her work, got more articles published, earned another degree and continued teaching. Few things can slow her down but the diagnosis of non-Hodgkin’s lymphoma stopped her in her tracks. She accepted the death sentence and moved to Calgary to be closer to her daughter. There, she registered at the Tom Baker Centre and, to her surprise, got a different story: The oncologists assured her they’d find the right chemo dosage for her situation.
That was just the beginning for Harris. In less than a decade, she has endured three chemotherapies to overcome non-Hodgkin’s lymphoma, plus treatments for two more cancers that she developed and beat.
When she was diagnosed with colorectal cancer in 2008, the oncologist took one look at her medical profile and agreed that, given her age, predisposition to cancer and non-Hodgkin’s lymphoma, he should attend to her right away. Within weeks, surgeons removed the tumour and resectioned her bowel using new robotic technology that allows for precision in very small areas.
Then, three years later, she developed what she says looked like horns on her forehead, the result of
squamous-cell carcinoma, a non-fatal skin cancer that causes protrusions. It took 10 months of radiation to shrink the tumours and surgery to excise the ones dangerously near her eye. On the plus side, Harris says jokingly, “They drew a line of stitches across my hairline and pulled skin over my forehead, so I don’t have an old woman’s forehead. No wrinkles or lines, it’s like a facelift.”
Needless to say, the Calgary cancer centre has come to know her well. “I don’t think I would have survived without them. I’m madly in love with all my doctors, men
and women.”Dr. Temple is pleased, but not surprised,
to hear her praises. “In Alberta, our patients identify that we have a wonderful system,” he says. “Alberta is just way ahead in terms of what we can offer our patients.” Most Albertans, unfortunately, don’t find this out until they’re diagnosed with cancer.
But there’s much that’s still unknown about surgical oncology, says Temple. “It’s a bit like asking how much do we know about the solar system.” As oncologists better understand tumour behaviour, unique genetic receptors and mutations, they’ll better understand the individual and therefore the particular patient’s disease.
“We’re at the very beginning of this phase of personalized medicine,” says McMullen, who is helping the Cross Cancer Institute lead a trial to determine why, if at all, presence of a newly discovered gene mutation requires more aggressive thyroid cancer surgery.
When it comes to surgical technology, McMullen says there’s always going to be incremental innovations – better devices, more advanced robotics that become cheaper and more common. But, if you were to touch base with him on the topic in 2022, “I still think personalized therapy and tailoring my surgical technique to a given patient, and the oncologist being able to pick the right therapy – those changes are where we’d have the most to discuss.”
Leap_Winter12_p20-23.indd 23 11/20/12 10:39:23 AM
Of all the tools we have to cope with cancer, it’s important to stop and smell the roses
usan Carr always took solace in theoutdoors. Never more so than after her diagnosis with cancer.
About eight years ago, Carr began exper-iencing severe abdominal pain. After a year of trying to fi nd answers, she met a gastroenterologist who told her it wasn’t all in her head and ordered a CT scan. Unfortunately, the scan revealed pancreatic cancer. (The pancreas is an organ that releases enzymes into the intestines so they can absorb food and fat.) Early on, there are no symptoms and by the time pain strikes, the disease is often advanced.
But today, she counts herself as lucky. “I had an extraordinary surgeon, Dr. Norman Kneteman, who chose to operate on me when hope was slim,” she says. Doctors found that, despite her pain, Carr’s cancer had not spread to other tissues and organs.
And then Carr recalls her fi rst appointment with her oncologist, Dr. Charles Butts. “He pulled up a chair, bent over to look me squarely in the eyes, and asked me to tell him about myself. When I began to talk about my health, he said, ‘No, tell me about you. Who are you?’ From that moment on, I felt safely enveloped at the Cross Cancer Institute.”
She would end up spending countless hours at the Cross for treatment. Later, when her health was better, she dedicated countless more hours as a volunteer. “Here I am today, alive and well,” she says, “and privileged to chair the 50th Anniversary Committee of the volunteer
SBY MARTIN DOVER
association.” The committee was charged with leaving a legacy to honour the volunteers who, over the past 50 years, have raised $4 million in support of patient care and comfort.
From Carr’s perspective as a patient and as a volunteer, there was one thing missing that might boost the care patients received and the solace their families needed: a garden. “There was no place at the Cross for patients and their families to sit outside, catch a breath of fresh air,” she says, “and for a short period of time, perhaps, be distracted from the reality of a cancer diagnosis.”
Carr says that people who have been on the brink of death understand that nature can have a profound buoying eff ect on the spirit. And she wasn’t alone. A garden of one kind or another at the Cross has long been a goal. At times, it has come close to fruition, but has never panned out. The volunteer association’s 50th anniversary committee also recognized the connection between nature and health, and set about to make it happen. The legacy project, the Healing Garden, was born. “It seemed appropriate,” Carr says, “to serve as a sanctuary for patients and their families – to renew the spirit and comfort the soul.”
Alberta Cancer Foundation funds will help build and maintain the Healing Garden. Jane Weller of the foundation describes the project as “a natural fi t” with her organization’s goals. “We consider the volunteers our valued partners as we both work hand-in-hand to enhance care and ease the journey for patients and
myleapmagazine .ca24 winter 2012
Sharing: FACE CANCER WITH STORIESSharingTransforming CANCER
Leap_Winter12_p24-25.indd 24 11/20/12 4:48:58 PM

their families at the Cross Cancer Institute,” she says. Weller says that though the Healing Garden is the
foundation’s fi rst offi cial partnership with the volunteer association, volunteers are often a patient’s fi rst brush with cancer care in Alberta, and they help set the tone. “When we talk to donors about their motivation, many of them will speak about volunteers and medical staff in the same breath,” she says. Weller adds that the Healing Garden has already captured the interest of donors as a meaningful way to become involved.
In November, Carr was on hand for the sod-turning ceremony. Once the Healing Garden is complete, patients and families can head to the west side of the cancer centre to fi nd it. A $600,000 wheelchair-accessible space, it was created through a partnership that includes the Cross Cancer Institute Volunteer Association, the Alberta Cancer Foundation, Alberta Health Services and Delnor Construction Ltd. It will include two plaza areas, a winding walkway and a small private seating zone surrounded by vegetation and shrubs and it will off er some protection from wind and rain, while still connecting patients to the outdoors. The garden opens in June 2013.
As Susan Carr would tell you, the cancer-busting power of the latest surgical treatments, along with chemotherapy and radiation therapy, are pretty awe-inspiring. But you should never underestimate the healing power of the sun falling through the leaves and the breeze gently caressing your skin.
zone surrounded by vegetation and shrubs and it will off er some protection from wind and rain, while still connecting patients to the outdoors. The garden opens
As Susan Carr would tell you, the cancer-busting power of the latest surgical treatments, along with chemotherapy and radiation therapy, are pretty awe-inspiring. But you should never underestimate the healing power of the sun falling through the leaves and the breeze gently caressing your skin.
A l b e r t a ’s c a n c e r - f r e e m o v e m e n t winter 2012 25
THE GREEN TEAMThe team at work behind the Cross Cancer Institute’s Volunteer Association legacy project, the Healing Garden, encompasses deep commitment and talent. They are: Susan Carr, Eugene Malo, John Jacob, Marg Smith, Minota Dundas, Debbie-Hall Lavoie, Shirley Gaudet, Lynda Harker, Deborah McTaggart-Baird, and Paula Germann. In conjunction with the Cross Cancer Institute’s Volunteer Association, the space is also made possible by support from Alberta Cancer Foundation, Alberta Health Services and Delnor Construction Ltd. To fi nd out how you can help, call the Alberta Cancer Foundation’s Jane Weller at 780-432-8358.
Leap_Winter12_p24-25.indd 25 11/20/12 10:40:49 AM
myleapmagazine .ca26 winter 2012
Transforming cancer
BIOBANK PRIMER By MIFI PURVIS
here is nothing quite as valuable to a researcher as human tissue. No one knows that better than Kathryn Graham, PhD, manager of the CBCF Tumour Bank in Edmonton. (There is
a sister facility in Calgary and the research benefits of both extend through Alberta and beyond.) Graham says that many major medical developments start with a well-crafted research idea that requires multiple tissue samples of a certain type. The biobank of tissue samples that she oversees may be behind tomorrow’s breakthroughs. Here’s how a tissue sample gets from the patient to a researcher’s lab.
T
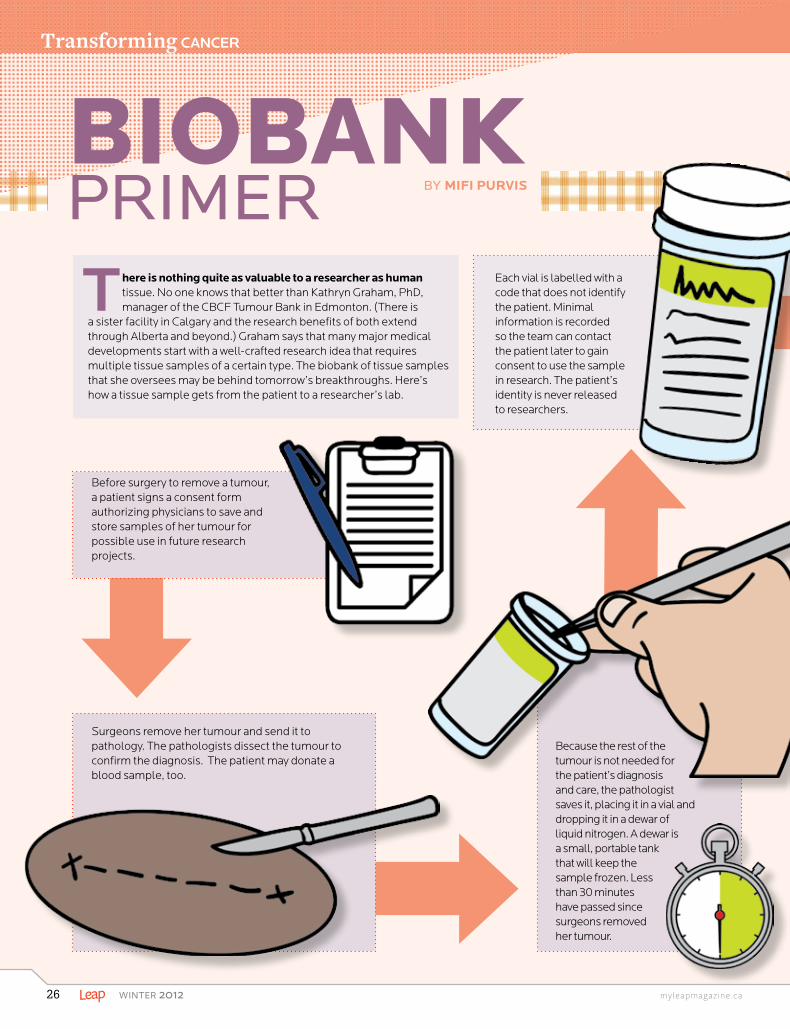
Before surgery to remove a tumour, a patient signs a consent form authorizing physicians to save and store samples of her tumour for possible use in future research projects.
Surgeons remove her tumour and send it to pathology. The pathologists dissect the tumour to confirm the diagnosis. The patient may donate a blood sample, too.
Because the rest of the tumour is not needed for the patient’s diagnosis and care, the pathologist saves it, placing it in a vial and dropping it in a dewar of liquid nitrogen. A dewar is a small, portable tank that will keep the sample frozen. Less than 30 minutes have passed since surgeons removed her tumour.
Each vial is labelled with a code that does not identify the patient. Minimal information is recorded so the team can contact the patient later to gain consent to use the sample in research. The patient’s identity is never released to researchers.
A l b e r t a ’s c a n c e r - f r e e m o v e m e n t winter 2012 27
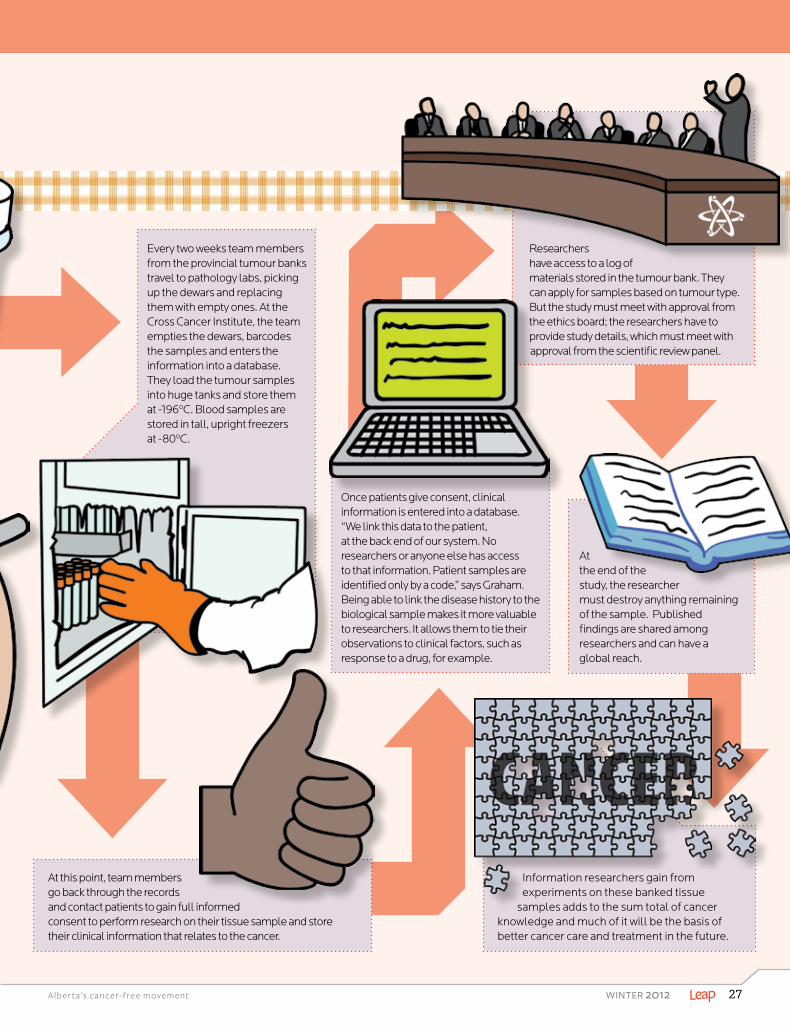
Every two weeks team members from the provincial tumour banks travel to pathology labs, picking up the dewars and replacing them with empty ones. At the Cross Cancer Institute, the team empties the dewars, barcodes the samples and enters the information into a database. They load the tumour samples into huge tanks and store them at -196ºC. Blood samples are stored in tall, upright freezers at -80ºC.
At this point, team members go back through the records and contact patients to gain full informed consent to perform research on their tissue sample and store their clinical information that relates to the cancer.
Once patients give consent, clinical information is entered into a database. “We link this data to the patient, at the back end of our system. No researchers or anyone else has access to that information. Patient samples are identified only by a code,” says Graham. Being able to link the disease history to the biological sample makes it more valuable to researchers. It allows them to tie their observations to clinical factors, such as response to a drug, for example.
Researchers have access to a log of materials stored in the tumour bank. They can apply for samples based on tumour type. But the study must meet with approval from the ethics board; the researchers have to provide study details, which must meet with approval from the scientific review panel.
At the end of the study, the researcher must destroy anything remaining of the sample. Published findings are shared among researchers and can have a global reach.
Information researchers gain from experiments on these banked tissue
samples adds to the sum total of cancer knowledge and much of it will be the basis of better cancer care and treatment in the future.
myleapmagazine .ca28 winter 2012
BY ANNALISE KLINGBEIL
Is screening for lung cancer around the corner?
Transforming CANCER
Is screening for lung cancer around the corner?
t’s the leading cause of cancer-related death in Canada, killing more people than prostate, breast and colon cancer combined. “There are more deaths from lung cancer than any other cancer,” says Dr. Paul MacEachern, a respirologist who
knows fi rsthand how deadly the disease is. Much of the Calgary doctor’s day-to-day work is spent evaluating patients with masses in their lungs. MacEachern sees patients who are referred to him because they’ve had abnormal CT scans or chest X-rays. He frequently diagnoses patients with lung cancer before referring them to the Tom Baker Cancer Centre for treatment.
Leap_Winter12_p28-29.indd 28 11/20/12 10:43:16 AM

A l b e r t a ’s c a n c e r - f r e e m o v e m e n t winter 2012 29
The survival rates for people diagnosed with lung cancer are low, because most people are diagnosed too late. “The majority of people who present with lung cancer, present at a stage where it’s already advanced,” explains MacEachern over the phone from a hotel room in Atlanta where he’s at-tending a lung conference. Because people show symptoms after the cancer has progressed, the early detection and treat-ment of lung cancer is the most promising strategy to reduce mortality from the disease. “It’s very attractive to think, ‘Well if we can just catch these lung cancers early, then we can save lives.’ ” MacEachern says. Unfortunately, it isn’t that easy.
There is currently no screening program for lung cancer in Alberta. Until quite recently, there was no evidence to suggest that screening worked. In the fall of 2011, a U.S. study, the “National Lung Screen-ing Trial,” demon-strated that lung cancer screening with a CT scan had the potential to save lives and reduce mortality for lung cancer. “That was big news because we’ve never had a screening test for lung cancer before,” MacEachern says. While the new study was exciting and seemed promising, it left doctors like MacEach-ern wondering how to move forward with the information without putting a strain on the medical system.
“The reason people aren’t automatically jumping on this is because screening is a process, not just one test,” says MacEachern, adding that resources need to be put into place to properly screen patients for lung cancer. The screening test that would be used, if a lung cancer screening program were to be introduced in the future, is a simple low dose CT scan that aims to minimize radiation exposure. Yet, giving a CT scan to thousands of people is no easy feat. “The magnitude of people that need to be screened is huge in the sense of the workload it could potentially generate,” says MacEachern. If everybody in Alberta who was potentially eligible for screening were to be screened, the workload in terms of the sheer number of CT scans would very quickly overwhelm the health-care system and the surgeons and radiologists who work in it, MacEachern says.
Another problem with blanket screening is that the rate of detection of nodules that turn out to be nothing is high. About 20 per cent of people screened will have an abnormal-ity, usually a nodule in the lung. Of these nodules, more than 95 per cent are benign. Unfortunately the CT scan does not show which nodules will turn out to be cancer, leading to followup testing and investigation of all nodules. This leads to anxiety and worry for people being screened, extra tests such as followup CT scans, and occasionally invasive proce-dures such as biopsies or surgeries and the attendant risk of complications associated with the procedures.
If a screening program were introduced, the ideal can-didates for screening would be those with the highest risk of lung cancer. Factors that increase the risk of lung cancer include age and smoking and, as such, MacEachern says the best candidates would be people aged 55 to 75 with a history of heavy smoking. “If we’re going to implement screen-ing, we have to take our time and make sure it’s done right;
otherwise the potential for harm is greater,” he says. As doctors like MacEachern evaluate how a lung can-
cer screening program should be implemented across the province in a widespread fashion, Canadians across the country are participating in a lung cancer detection study that recognizes the need to create a lung cancer screening program. The Terry Fox Research Institute and the Canadian Partnership Against Cancer are under-taking an early lung cancer detection study. MacEachern notes Calgary is one of seven sites across the country par-ticipating in the study and about 250 Calgarians make up the study’s 2,500 participants. “The main purpose of the study was to try and validate the risk prediction model.
Is there some way we can predict bet-ter who is at risk for lung cancer that would allow us to then hopefully be able to screen fewer people but to catch
most of the lung cancers?” he asks. The study is nearing completion. All participants have had scans and are now in followup stages while data is collected.
The study screened current and former smokers between 50 to 75 years of age at high risk of lung cancer. Through the data gathered, the study aims to track the type of diagnostic tests and treatment, as well as their costs, thus determining the health-care resources re-quired and how much it would cost the public if a lung cancer screening program were to be implemented across the country. A primary objective of the study, which has brought together experts in radiology, respi-ratory medicine, thoracic surgery, pathology, oncology, epidemiology, health economics and health-care policy, is to fi nd an eff ective way to identify lung cancer in its early stages, thus increasing survival rates.
Whether we can implement lung cancer screening across the province, or from coast to coast, is still in question. “It’s exciting in a way because we’ve never had a screening test for lung cancer and it does have the potential to save lives,” MacEachern says, adding: “The excitement is tempered by the fact the magnitude of the problem is huge.” As Canada’s deadliest cancer contin-ues to take lives, MacEachern says it’s imperative that in the future, the right people get screened for lung cancer, in the right fashion. “People get excited about screening and there is reason to get excited. It has signifi cant po-tential,” he says. “I just want to stress that it’s going to take some time before we can implement this. We’d like to try to implement something because there is benefi t to Albertans if we do so, but there are potential harms and we have to make sure we do it right to minimize the harms and maximize the benefi ts.”
Despite the potential risks involved with screen-ing for lung cancer, MacEachern stresses, “A screening program should not be considered a substitute for a tobacco control program. The best way to reduce your chance of getting lung cancer is to quit smoking or never start smoking.”
There is currently no screening program for lung cancer in Alberta. Until quite
recently there was no evidence to suggest that screening worked.
Leap_Winter12_p28-29.indd 29 11/20/12 10:43:24 AM

myleapmagazine .ca30 winter 2012
Married 52 years, 10 days. Together, in total, for 58years and four days. John Porter can tell you exactly how long he and his wife Virginia shared their lives before she died of cancer. He speaks of the days and years he spent with his teenaged sweetheart and “dear partner in life,” now comforted by the many memories. “We were blessed with a happy and satisfying marriage,” says Porter, 90. “We had an extremely full life together.”
After marrying in 1948, they moved from Saskatoon to Calgary, where Porter found work as a geologist. They bought the home where Porter still lives and the couple – who never had children – enjoyed a life of hosting dinner parties, visiting the local theatre and tak-ing road trips. As a homemaker, Virginia found her niche behind the sewing machine making dresses and suits.
Things took a turn in 1986 when she developed uter-ine cancer and spent the next fi ve years receiving treat-ment at the Tom Baker Cancer Centre. Nine years after her treatment, she developed osteosarcoma, the most common type of bone cancer, and she died in 2000. “I still miss her dearly,” says Porter. “I have a lot of mem-ories and a lot of photographs and it sustains me, but it’s rather lonely.”
Unfortunately he’s no stranger to the losses of can-cer, which had already claimed the lives of his father, twin brother and both of Virginia’s parents. Cancer also struck his mother and sister, who lived past the illness. Before Virginia died, the couple decided to make yearly contributions and to commit part of their estate as a gift for the Alberta Cancer Foundation.
During his trips back and forth to the Tom Baker, Porter came to know the facility well and appreciate the high level of care his wife received. And the research projects he learned about impressed him. As a result, his legacy will be distributed evenly across patient care and research.
“I’m so impressed – being a geo-scientist myself – it’s just amazing, the changes and new ideas they’ve come up with,” he says. “I don’t think there’s a magic bullet, but a lot of intelligent people and researchers are work-ing on this. I think we’ll look back in another century and say ‘Boy that was a real renaissance period.’”
Derek Michael, gift planning specialist with the
Alberta Cancer Foundation, says future gifts such as Porter’s are crucial. “Making that commitment for cancer patients down the road means we’ll have funding available for future research and patient care programs,” Michael says. “There can be a long-term vision and plan. People like John benefi t complete strangers they’ll never meet and yet they’re still willing to make that generous commitment.”
There’s a misconception that gift planning is only for the wealthy, Michael adds. He says that any amount is signifi cant. “It can be whatever makes sense for your circum-stances. It adds up quickly.”
After 12 years, Porter says fi nding closure over the loss of his wife is diffi cult. But when it comes to the disease, he has great faith the foundation will use his future gift to help families down the road.
“This gives me some quiet satisfaction.”
BY GISELE APARICIO-HULL
John Porter lost his wife, brother and father to cancer. Now he is leaving behind a gift to help families of the future
IN LOVING MEMORY: John Porter came to know the Tom Baker Cancer Centre and appreciated the level of care his wife received.
LEGACY LOVEplanned giving /WORKING FOR A CAUSE
PLAN AHEADGirish Agrawal, senior executive fi nancial consultant, says most people under-estimate the charitable potentials of their estate. “Once there is a commit-ment, there are ways to enhance that commitment or make it more effi cient.” Future gift options range from a specifi ed amount or asset in a will, a charita-ble remainder trust, a life insurance policy, or setting up a private foundation.The Alberta Cancer Foundation can guide interested donors through the pro-cess. Contact Derek Michael, gift planning specialist, 780-643-4662. “It may not be part of their day-to-day job, but they do have access to the resources you need,” says Agrawal.
OF
Leap_Winter12_p30-33.indd 30 11/20/12 10:44:25 AM
A l b e r t a ’s c a n c e r - f r e e m o v e m e n t winter 2012 31
A pair of PET/CT scanners reduce wait times for diagnosis and testing and improve new treatments for Albertans. Meet some of the donors behind the project
WhereGOES
D r. John Mercer is understandably bullish about the most recent of his department’s gleaming new machines. Cutting-edge PET/CT scanners were installed in Edmonton’s Cross Cancer Institute in 2005 and 2012. The
machines look obviously clinical and a little futuristic. The scanner comprises two parts. The fi rst – the part that contains the machinery to scan the patient – is shaped like a Lifesaver that’s taller than a man and standing on its edge. The second part is a bed on which the patient lies that moves through the ring in the centre of the scanner.
In preparation for the scan, a patient takes a kind of nuclear medicine called a tracer by intravenous injections. The tracer moves through the body localizing in tissues, al-lowing the nuclear medicine physician to visualize healthy and diseased tissue. The scans are used mainly to fi nd and monitor cancer, but can be used for other conditions, such as diseases of the brain and circulatory system. Including preparation and scan, the process takes about half an hour.
STORIES OF GIVINGwhy I donate /
THE MONEY
BY MIFI PURVIS / PHOTOS BY BRIAN BRADY
Leap_Winter12_p30-33.indd 31 11/20/12 4:50:25 PM
myleapmagazine .ca32 winter 2012
stories of givingwhy I donate /
The presence of the machines means that more pa-tients can be scanned in a shorter time more accurately, significantly reducing wait times for cancer screening, arguably the most stressful days or weeks in a patient’s journey. The new PET/CT machines will process three
times as many patients as conventional scanners. But they bring much more than reduced wait times to Alberta.
The machines are the latest additions to what Mercer calls “a fantastic facility, one that in the last 10 years has become a globally recognized leader
in radiopharmaceutical development.” Mercer is the re-search director of the Edmonton PET Centre. Whereas other facilities might use just one or two tracers, the Ed-monton PET Centre at the Cross Cancer Institute main-tains a library of tracers, tailored to find and monitor various cancers.
“The machines operate in two different modalities,” Mercer says, “taking two different types of images at the same time.” The PET modality (positron emission tomography) looks for a specific tumour. “The prob-lem with PET is that there is no anatomical reference point, so we don’t know where a tumour is exactly,” Mercer says. The CT (computed tomography) is like a
three-dimensional X-ray. “It allows us a precise idea of where a tumour is located.” Together, the scans show a transparent, 3-D version of the patient that doctors can manipulate and zoom in on. The tracers light up the tissues doctors are looking for.
Since the PET Centre came online in 2002, Mercer says there have been more than 50 clinical trials in which physicians have use this imaging technology. “The trac-ers allow us to fine tune our choice of therapy for each patient,” he says. “We are trying to tie ourselves to per-sonalized medicine. Having these instruments here lets us get even closer to that.”
Of course there is a pricetag. At $3 million per machine it’s a significant one.
The Alberta Cancer Foundation has funded these machines through the generous support of its donors. By strategically investing its funds, the foundation pro-vides opportunities for donors to invest in research programs, equipment and patient care.
The Muhlenfelds: Making home a better placeReinhard Muhlenfeld knows a good opportunity when he sees it. “We came to Canada in 1975,” the 82-year-old businessman says. Originally from Germany, Muhlen-feld had been living for years in England. His expertise brought him to Alberta to build a feed plant in Sexsmith. “It was a two-year project and we didn’t intend to stay,” he recalls. But after that project was over another opportunity came. “We bought a small mill in Bar-
The machines are the latest additions to what Mercer calls
“a fantastic facility, one that in the last 10 years has become a globally recognized leader
in radiopharmaceutical development.”
Leap_Winter12_p30-33.indd 32 11/20/12 12:20:04 PM

A l b e r t a ’s c a n c e r - f r e e m o v e m e n t winter 2012 33
rhead and hired someone to run it,” he says. Other feed mills followed and Reinhard, his wife Elisabeth and their children Sandra, Angela and Peter, sold the house in England and put down roots in Alberta.
Today, with Elisabeth at his side, he is reminiscing from his book-lined office at his home in Edmonton and it’s clear Muhlenfeld knows a good opportunity when he sees it. On one of his regular trips to visit the feed mills, he came across a bag of pet food. “I took a look at this bag, and I saw it was made in the United States,” he says. “It turned out there was no one manufacturing pet food in Alberta.” In 1985, Muhlenfeld set out to change that. Today, Champion Pet Foods makes high-quality pro-tein-rich dog and cat food mainly from locally-sourced ingredients at its two plants in rural Alberta. It markets its product to 40 countries. “We have two production systems and 225 employees,” Muhlenfeld says. “Our son Peter is the chief salesman.” The business has been prof-itable, and the Muhlenfelds wanted to give back.
“As Reinhard says, we made the money here and it should stay here in Alberta,” says Elisabeth. “We chose to give to hospitals.”
Early in the process, they sat down with Jane Weller from the Alberta Cancer Foundation, who presented some options, among them, the chance to direct funds to a PET/CT scanner. The Muhlenfelds saw this as a good opportunity. They made an initial generous donation and, after a tour of the facility during which they found out what the machine could do, they followed up with a
second donation. “They needed some toys to go with it,” Muhlenfeld says.
EECOL Electric: Employees for a better futureEECOL Electric has had a part in powering Canada since 1919. An employee-owned company, EECOL services the electrical material supply requirements of industry. The company boasts large inventories, qualified personnel, and great service. And, like every organization, EECOL has lost valued colleaugues to cancer.
“We are long-time supporters of the Alberta Cancer Foundation,” says Garry Tansem, EECOL’s regional manager for Northern Alberta. “We’ve been looking for more structure and more significant choice when we di-rect our charitable dollars,” Tansem says. “We wanted to put the funds into the region where we live and work.” To that end, EECOL developed a five-year plan for its cor-porate donations.
Tansem says that he and others from EECOL consult-ed Jane Weller of the Alberta Cancer Foundation and ex-plained the kind of projects the company wanted to fund. “We wanted something specific to Northern Alberta,” he says, “and we wanted to help patients today and into the future.” Weller presented a few options and the EECOL team identified the PET/CT scanners as an investment they could get behind. “People from our region, North-ern Alberta, usually go to the Cross for cancer diagnosis and treatment. We saw the scanner as significantly im-pacting care in our area.”
The Stollery Charitable Foundation: Building a healthier communityIn 1994, after a lifetime of profitable work for PCL Construction Group, Bob Stollery (who died in 2007) along with his wife Shirley, already generous philan-thropists, wanted to create a legacy that would last. They were the driving force behind the Stollery Chil-dren’s Hospital in Edmonton and the wide-reaching Stollery Charitable Foundation. Like the Muhlenfelds, they wanted to give back to the community that had afforded them success.
“The Stollery Charitable Foundation is a private, en-dowed, family foundation,” explains executive director Scott Graham. He says that the foundation’s mandate in-cludes the goal of improving the health of the community in cooperation with other funders. “We heard about the PET/CT scanners in an early inquiry from the Alberta Can-cer Foundation in 2008. We discussed them with Dr. Tony Field, and he made a compelling case for how they would help the community.” Field explained how the scanners would reduce wait times and improve the detection and monitoring of cancer. His enthusiasm and clear explana-tions captured the interest of Graham and Jeff Bryson, director of granting at the Stollery Charitable Foundation.
“We took Dr. Field’s information to the family to see what we might do to help.” Graham adds that part of the attraction was the Alberta Cancer Foundation’s reputa-tion as an organization that uses donor dollars effectively. “We knew that we’d be able to paint with a wide brush,” Graham says, “that the scanners would help a large swath of people in the community.”
Leap_Winter12_p30-33.indd 33 11/20/12 12:21:37 PM
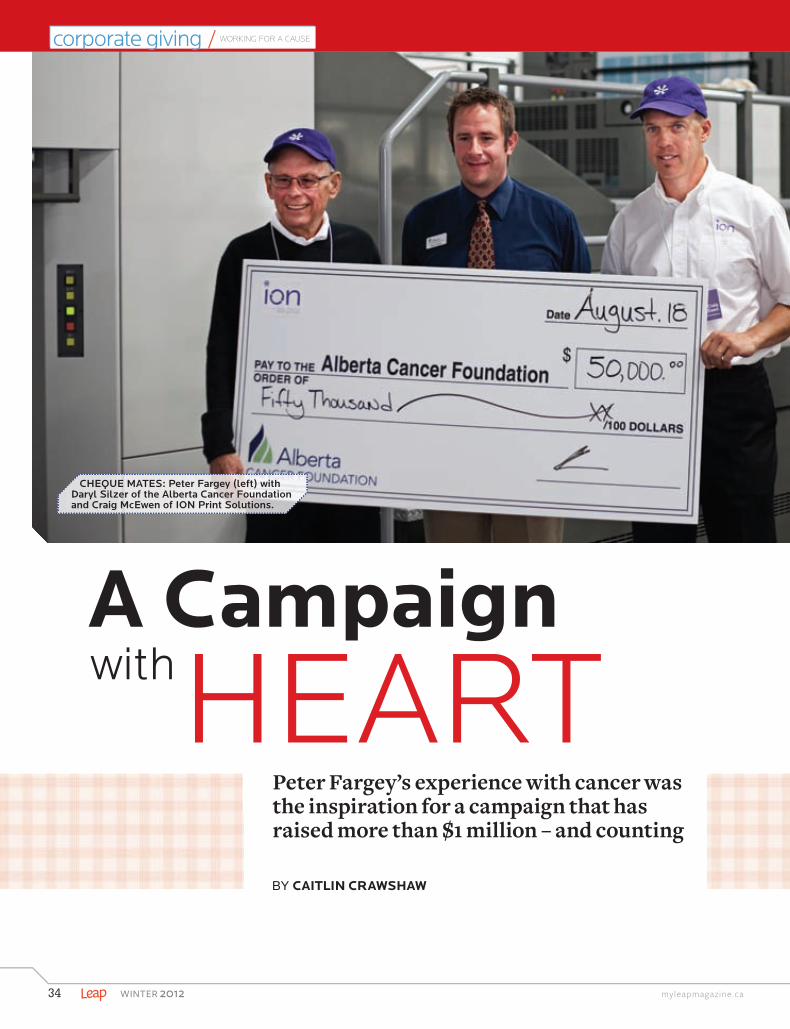
myleapmagazine .ca34 winter 2012
BY CAITLIN CRAWSHAW
Peter Fargey’s experience with cancer was the inspiration for a campaign that has raised more than $1 million – and counting
Friends for LIFE corporate giving / WORKING FOR A CAUSE
A CampaignwithHEART
CHEQUE MATES: Peter Fargey (left) with Daryl Silzer of the Alberta Cancer Foundation and Craig McEwen of ION Print Solutions.
Leap_Winter12_p34-35.indd 34 11/20/12 10:44:23 AM

A l b e r t a ’s c a n c e r - f r e e m o v e m e n t winter 2012 35
for LIFE
McEwen approached his business part-ner to see if he’d be up for telling his
story in a big way. Fargey didn’t hesitate.
hese days, cancer survivor Peter Fargey feels like a million bucks – which is roughly the sum he and his company, ION Print Solutions, have raised for the Alberta Cancer Foundation over the last three years. Since 2010,
the Nisku-based printing company has been involved in a summertime matching gift campaign, matching public donations to the foundation of $50,000 or less.
To put this into perspective: the Alberta Cancer Foundation’s summer campaigns have historically netted $30,000 per year, while the ION Print Solutions campaign has netted an average of $350,000.
The campaign’s success might stem from its source. Back in 2010, Fargey – one of ION’s founders – began suff ering from persistent gut pain that wasn’t eased by the usual remedies, like dietary changes or Tylenol. While he was on holiday, the pain grew worse – severe enough that he had a hunch it wasn’t a normal stomach ache. “We were in the States at the time,” Fargey says, “and when I got home, I went to see the family doctor.”
Fargey’s physician ordered tests that revealed he had cancer. “I think it’s always in the back of your mind, but when they found it, of course, it was a shock to be told all of a sudden that you have cancer,” he says. For that matter, it wasn’t just any cancer, but a rare cancer in his duodenum (the fi rst section of the small intestine). In fact, it puzzled his oncologist, Dr. Michael Sawyer. “It was so rare that he didn’t know how to treat it,” Fargey explains.
Erring on the side of caution, Sawyer chose a treatment that involved surgery (the removal of Fargey’s duodenum, bile duct and half of his pancreas) and an entire year of chemotherapy. “Thankfully, Dr. Sawyer decided to treat it very aggressively and thankfully, it worked,” says Fargey. The staff at the Cross Cancer Institute in Edmonton, where he received his treatments, made the experience much more tolerable, he says: “The people at the Cross were magnifi cent, they really were. Let’s just say they’re very good at what they do.”
At the same time as Fargey was receiving his treatments, ION Print Solutions was greening its operations: “We made equipment invest-ments, building and lighting changes – things to reduce the amount of wa-ter and power we use,” explains managing partner Craig McEwen. Cancer, which is increasingly linked to environmental pollutants, was also on his mind, thanks to Fargey’s experiences. He wondered if perhaps the com-pany could publicize its new environmental initiatives while at the same time, raise money for cancer research, patient care, screening and preven-tion programs. He thought Fargey could be the face of the campaign.
McEwen approached his business partner to see if he’d be up for telling his story in a big way. Fargey didn’t hesitate: “I bought in right away,” he says. “I thought it was a great idea.” ION approached the Alberta Cancer Foundation and together they launched a campaign in the summer of 2010, a few months before Fargey’s chemo ended. Donations began pouring in and it became apparent that the campaign resonated with Albertans.
McEwen thinks the combination of his colleague’s story, the environ-mental message, and the fact that ION was helping the public leverage their donation dollars, appealed to people. “It was incredible how many calls we had from people considering donating to make sure we would match what they donated,” he says.
The third campaign offi cially ended in August 2012, but the company looks forward to doing it again next summer. The fourth year of the campaign will be similar to the look and feel of the fi rst three, but McEwen hopes to recruit other companies to take part, as well.
October 2012 marked two years since Fargey’s last chemo treatment and he’s happy to report that he’s offi cially free of cancer. However,
like anyone who has endured the treatments, he’ll continue to get tested regularly – every six months – for several years. “Everyone hopes to get to fi ve years,” he says, and all signs point to a good long-term
prognosis, especially after his most recent tests. And while Fargey’s been the face of the campaign for three years running, he’s more than happy to keep telling his story. “As long as they think it’ll continue to raise money, why not?”
T
RARE BIRD: Always one to do it his way, Peter Fargey’s cancer was so unusual his doctors weren’t sure of the best treatment approach at fi rst.
Leap_Winter12_p34-35.indd 35 11/20/12 4:50:57 PM
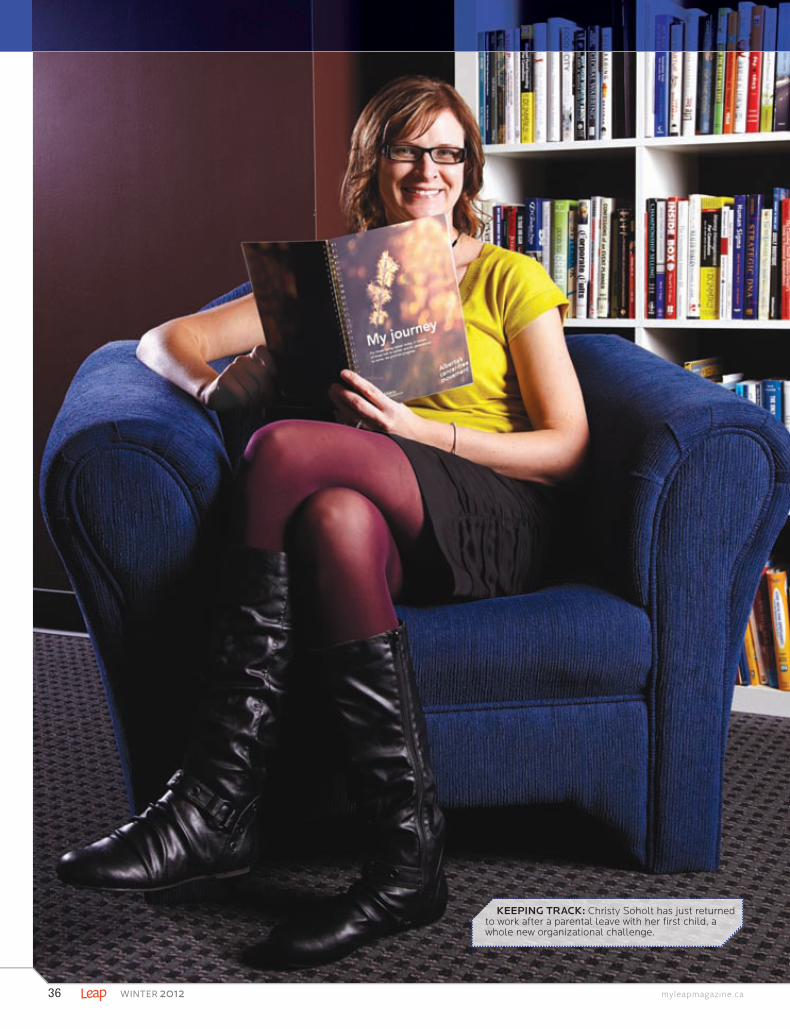
36 winter 2012 myleapmagazine .ca
KEEPING TRACK: Christy Soholt has just returned to work after a parental leave with her fi rst child, a whole new organizational challenge.
Leap_Winter12_p36-37.indd 36 11/20/12 12:24:22 PM
The Alberta Cancer Foundation is updating the journal on a regular basis and your feedback is welcome. Please send suggestions to [email protected]
I was quickly buried under a mountain of information and overwhelmed by an appointment schedule I could
not keep track of.
winter 2012 37A l b e r t a ’s c a n c e r - f r e e m o v e m e n t
A new daily planner, designed by a cancer survivor, is available to help people cope with the process of cancer treatment
’ve always had good intentions to stay organized. I have vowed to be prepared, punctual, and keep my promises. For the most part I’ve been able to live up to my own expectations. Despite having the reputation of being the last to show at a family function, I’ve been
called “the organizational guru” at work. I could rattle off my jammed calendar in mere minutes, and I could fi nd a specifi c piece of information in the blink of eye – well, maybe that last one is a slight exaggeration – but I considered myself fairly on top of it.
Until May 7, 2008 after a visit with my family doctor, I went thinking she would tell me that the biopsy of “my lump” (as I aff ectionately called it) proved to be nothing to worry about. Instead I came home with a stack of literature on breast cancer. Thus began my love-hate relationship with documenting the hundreds of details of my cancer journey.
Shocked at my diagnosis, particularly at my young age of 28, I had a lot of questions. A lot. I had not ever been close to anyone on a cancer journey and I had no idea what to expect. Thankfully my cancer care staff blew me out of the water with answers. All the information I could possibly need and then some; a four-hour explanation of my specifi c diagnosis and treatment plan, supported by a handout with additional information. The fi rst meeting was followed by another appointment with another specialist, and a seminar that would help me with that issue, oh, and a clinical trial that would be perfect, and a support group that would be worth meeting, and so on. In just a few short months, I was buried under a mountain of information and overwhelmed by an appointment schedule I could not keep track of.
Four short months later, my Dad heard the dreaded words “you have cancer” when he was diagnosed with non-Hodgkins lymphoma. Just like that, there were now two cancer journeys in my immediate family of four to keep track of. Being the seasoned expert on the subject that I now was, I accompanied him and Mom as much as possible to his seemingly endless appointments, trying to write down anything that would make sense, remembering to ask the hundreds of questions that had been going through all our minds, and now trying to make sense of a new mountain of handouts. Complete with side-eff ects of treatment, cancer was taking over my life, and my house.
Eventually the handouts and books made their way into a pretty pink box I purchased for that purpose. Now my offi ce desk had a box with the fi tting saying “everything is possible” on it where there was once a stack of papers.
Somehow this small change in organization helped me feel like I was taking control of something that felt out of control before. Mom found her own system for Dad’s records – a very large fi le folder. And while my box was sorted by subject, Mom’s was organized by date. Both systems seemed to help us manage the cancer journey just a little bit better.
Then there was the matter of a slew of new appointments and contacts. From doctor appointments to support group contacts to self-help seminars and treatment dates, being a cancer patient seemed to be a full-time job. I laugh when I think about my naiveté at diagnosis, thinking I was going to continue working through my illness. Bless those who can make that happen, I was lucky to make it to the lab for blood work on time! My solution was low-tech; a quick trip to a stationary store and I was armed with a pocket calendar and a pencil that tucked into my purse. At a quick
glance I now not only knew what the next day and month had in store, but I had my key contacts close at hand. I could jot down my questions as they came to me, and I could take more control of my journey. Mom’s system for Dad was similar and though it’s not
revolutionary, having this sort of system for my personal life was a brand new idea to me.
After treatment, I turned my passion for a cancer-free future into a career by joining the Alberta Cancer Foundation team. Understanding that information, support, contacts, appointments and more is a large component of the cancer journey, we at the Foundation wanted to give patients a gift to help ease this burden. After sorting through my box, reviewing my pocket calendar, and consulting researchers, nurses, volunteers, patient education specialists, nutritionists, and more, the My Journey patient journal and fi le folder gift was born. I am so pleased that the foundation off ers this package to all patients throughout the province, and I hope it will help patients navigate and take control of their journey. Patients can pick up a copy, free of charge at any Alberta Cancer Foundation offi ce.
I would not wish anyone this diffi cult journey. I hope in some small way that my journey and book helps ease others.
IBY CHRISTY SOHOLT / PHOTO BY EUGENE, 3TEN
Leap_Winter12_p36-37.indd 37 11/21/12 11:01:31 AM
Motivation to Move
myleapmagazine .ca38 winter 2012
A
“I like to take on a challenge that frightens me enough and
motivates me to get ready for it,” McLean says.
By Michelle lindstroM
There are no excuses to let your exercise regimen grind to halt in the deep freeze of an Alberta winter
for LIFE
lberta’s outdoor race season is over for the average fair-weather athlete, but training
definitely isn’t … or at least it shouldn’t be.Finding the motivation to exercise in the winter
months can be harder than actually working out. Dark mornings, dark evenings. Comfort clothes, comfort food. But it doesn’t have to be as hard as it sounds.
Katie McLean, an Alberta Cancer Foundation trustee and chair of Joe’s Team Calgary, shares how she pushes past the times she wants to snuggle deeper into her couch and slip into hibernation. “You might know a few people that just look like they’re fit all the time and they never have any issues motivating themselves,” she says. “I guarantee you that without a goal, those people are not that motivated.” What she does, along with many others who never seem to lose their desire to exercise, is set a new goal days or weeks before achieving the current one.
It’s OK to base your goal on fear. “I like to take on a challenge that frightens me enough and motivates me to get ready for it,” McLean says. For example, she plans to do the 2013 Escape from Alcatraz Triathlon in March. “I’m so scared, I actually get nervous just thinking about it – and I’ve done a lot of races.” Fear can be the driver to make trainees head to the gym instead of home and bed. An alternative can be to work out in your home, driven by the knowledge that training is required to cross the finish lines in spring and summer of all race types and distances. Besides, maintenance in the off-season makes for easier spring training.
When you work out at home, you’re amongst loved ones instead of spending hours across town in a gym, meeting your plank and burpee quota. A con is the lack of space in most homes to set up exercise machines. McLean’s answer is a bike trainer, especially if you already have a bike. (A bike trainer lifts one wheel off the floor and turns your road or mountain bike into a stationary one.)
She plunks her trainer in front of her TV. “I’ve watched some great movies,” she says. McLean makes it a social gathering by inviting friends, and their bikes, over to use another trainer she has and off they go – stationary bike buddies. She and her husband trained together in their basement last winter to prep for the 2012 Enbridge Ride to Conquer Cancer – her husband’s first long-distance bike race.
Inside or outside, you should grab a friend. “When someone pushes you further on a lazy day,” McLean says, “your competitive side kicks in. On your own, you’re more likely to say, ‘Ahh, I’m finished. That’s enough.’ ”
When training on your own, discouragement is inevitable – that’s where music comes in. “Get a playlist together that inspires you,” McLean says. Movies are just too hard to
concentrate on when she’s working out really hard. Training for running is more difficult than biking in winter if you don’t have a
treadmill at home, a gym membership or the desire to suit up appropriately and run outside. If you have a room with the space and a high ceiling, McLean suggests skipping to build cardio endurance. Her modification, because she doesn’t have the space, is to jump up and down while making small circles with her arms – all the motions of skipping without the rope.
A person’s existing fitness level and goals will determine the intensity of their winter workout regime. “I love the idea of always maintaining a base level of fitness,” McLean says, “because that means you’re ready for training for almost any sport.” Her definition of “base level of fitness” includes a routine of working out three times a week in, for example, a spin class, yoga or playing some kind of sport. This foundation of fitness makes it much easier to kick things up a notch, take things outside and train for a June event, like her pet project: Joe’s Team Triathalon/Dualthalon, a sprint event to raise funds for the Alberta Cancer Foundation in support of head-and-neck cancers.
Leap_Winter12_p38-39.indd 38 11/20/12 10:35:02 AM
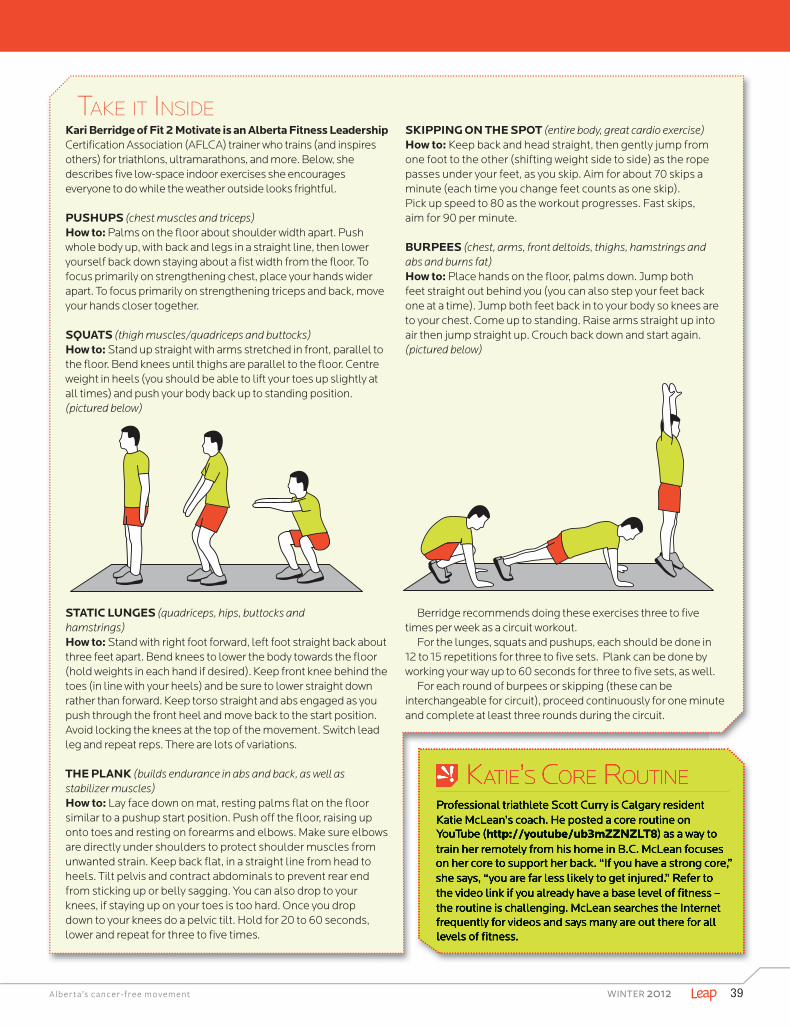
Motivation TO MOVE
KATIE’S CORE ROUTINEProfessional triathlete Scott Curry is Calgary resident Katie McLean’s coach. He posted a core routine on YouTube (http://youtube/ub3mZZNZLT8) as a way to train her remotely from his home in B.C. McLean focuses on her core to support her back. “If you have a strong core,” she says, “you are far less likely to get injured.” Refer to the video link if you already have a base level of fi tness – the routine is challenging. McLean searches the Internet frequently for videos and says many are out there for all levels of fi tness.
A l b e r t a ’s c a n c e r - f r e e m o v e m e n t winter 2012 39
KATIE’S CORE ROUTINEProfessional triathlete Scott Curry is Calgary resident Katie McLean’s coach. He posted a core routine on YouTube (http://youtube/ub3mZZNZLT8) as a way to train her remotely from his home in B.C. McLean focuses on her core to support her back. “If you have a strong core,” she says, “you are far less likely to get injured.” Refer to the video link if you already have a base level of fi tness – the routine is challenging. McLean searches the Internet frequently for videos and says many are out there for all levels of fi tness.
TAKE IT INSIDEKari Berridge of Fit 2 Motivate is an Alberta Fitness Leadership Certifi cation Association (AFLCA) trainer who trains (and inspires others) for triathlons, ultramarathons, and more. Below, she describes fi ve low-space indoor exercises she encourages everyone to do while the weather outside looks frightful.
PUSHUPS (chest muscles and triceps)How to: Palms on the fl oor about shoulder width apart. Push whole body up, with back and legs in a straight line, then lower yourself back down staying about a fi st width from the fl oor. To focus primarily on strengthening chest, place your hands wider apart. To focus primarily on strengthening triceps and back, move your hands closer together.
SQUATS (thigh muscles/quadriceps and buttocks)How to: Stand up straight with arms stretched in front, parallel to the fl oor. Bend knees until thighs are parallel to the fl oor. Centre weight in heels (you should be able to lift your toes up slightly at all times) and push your body back up to standing position. (pictured below)
STATIC LUNGES (quadriceps, hips, buttocks and hamstrings)How to: Stand with right foot forward, left foot straight back about three feet apart. Bend knees to lower the body towards the fl oor (hold weights in each hand if desired). Keep front knee behind the toes (in line with your heels) and be sure to lower straight down rather than forward. Keep torso straight and abs engaged as you push through the front heel and move back to the start position. Avoid locking the knees at the top of the movement. Switch lead leg and repeat reps. There are lots of variations.
THE PLANK (builds endurance in abs and back, as well as stabilizer muscles)How to: Lay face down on mat, resting palms fl at on the fl oor similar to a pushup start position. Push off the fl oor, raising up onto toes and resting on forearms and elbows. Make sure elbows are directly under shoulders to protect shoulder muscles from unwanted strain. Keep back fl at, in a straight line from head to heels. Tilt pelvis and contract abdominals to prevent rear end from sticking up or belly sagging. You can also drop to your knees, if staying up on your toes is too hard. Once you drop down to your knees do a pelvic tilt. Hold for 20 to 60 seconds, lower and repeat for three to fi ve times.
for LIFE SKIPPING ON THE SPOT (entire body, great cardio exercise)How to: Keep back and head straight, then gently jump from one foot to the other (shifting weight side to side) as the rope passes under your feet, as you skip. Aim for about 70 skips a minute (each time you change feet counts as one skip). Pick up speed to 80 as the workout progresses. Fast skips, aim for 90 per minute.
BURPEES (chest, arms, front deltoids, thighs, hamstrings and abs and burns fat)How to: Place hands on the fl oor, palms down. Jump both feet straight out behind you (you can also step your feet back one at a time). Jump both feet back in to your body so knees are to your chest. Come up to standing. Raise arms straight up into air then jump straight up. Crouch back down and start again. (pictured below)
Berridge recommends doing these exercises three to fi ve times per week as a circuit workout.
For the lunges, squats and pushups, each should be done in 12 to 15 repetitions for three to fi ve sets. Plank can be done by working your way up to 60 seconds for three to fi ve sets, as well.
For each round of burpees or skipping (these can be interchangeable for circuit), proceed continuously for one minute and complete at least three rounds during the circuit.
Leap_Winter12_p38-39.indd 39 11/20/12 10:35:14 AM

myleapmagazine .ca40 winter 2012
A sense of humour, a master’s degree and a set of skis will get you far in stem cell research, just ask the director of the Hotchkiss Brain Institute
Research Rockstar
e’s much less Grizzly Adams than you’d expect for a confessed mountain-loving man. “My love of the mountains is the mountains,” Dr. Sam Weiss says. Only when he says it,
there is a big, growly emphasis on the “is.” He gets out of the lab or office, destined for Banff, as often as he can. You’ll find him hiking in the warmer, dryer seasons and cross-country skiing in the colder, snowier seasons. But mostly Weiss looks more the part of a clean-cut, science-loving, stem cell expert.
His many titles in the faculty of medicine at the University of Calgary include professor, department of cell biology and anatomy/pharmacology and therapeutics member, genes and development research group and director of the Hotchkiss Brain Institute. But he keeps his CV simple: “I’m not a physician, I’m just a PhD.”
In 1992, Weiss co-headed a team that found and reported that the adult brain contained neural stem cells. “It was a bit of a serendipitous discovery,” he says, since he was actually studying something else at the time. Stem cells can divide, self-renew and change into specialized cell types, so Weiss’s discovery stirred inquiries throughout
H
Weiss GuyBY MICHELLE LINDSTROM / PHOTOS BY BOOKSTRUCKER PHOTOGRAPHYBOOKSTRUCKER PHOTOGRAPHY
Leap_Winter12_p40-43.indd 40 11/20/12 10:34:01 AM

A l b e r t a ’ s c a n c e r - f r e e m o v e m e n t winter 2012 41
CELLS & SCIENCE: Dr. Sam Weiss is a man of discovery in the lab and the mountains. CELLS & SCIENCE: Dr. Sam Weiss is a man of discovery in the lab and the mountains.
Leap_Winter12_p40-43.indd 41 11/20/12 10:34:13 AM

myleapmagazine .ca42 winter 2012
Research Rockstar
“He has the ability to see the big picture and describe what he’s doing in an exciting way to everybody in the room.”– Dr. Gregory Cairncross
the scientific community, mainly questioning if brain injury and disease (including cancer) could be repaired with the use of neural stem cells.
Weiss’s discovery was big news in 1992. It even appeared in the New York Times. Dr. Gregory Cairncross, a professor in the oncology department at Western University in London, Ontario at the time, read it and started following the work of Professor Weiss at the University of Calgary. The article discussed Weiss’s
thesis: could harnessing stem cells in the brain be used after an injury or stroke by reactivating or rewiring the organ in some way to rebuild it? By that time, Cairncross had already written an article about brain stem cells and how cancers of the brain may arise from those cells.
“His science intersected with my ideas of the origins of brain cancer,” Cairncross says, adding that’s why he remembered Weiss and looked him up years later.
Cairncross was recruited for a position, head of the clinical neurosciences department at the University of Calgary, over a decade ago and specifi cally asked to meet with Weiss when he travelled west for his job interviews – all due to that New York Times article. “He was about the way I thought he would be,” Cairncross says, undaunted by the long wait to meet the scientist. Cairncross knew he had the clinical background and Weiss had science behind him, nudging his suspicions that their knowledge and interests could complement each other. He was right.
They belonged to diff erent departments, maintaining their own research teams for years, until more brain stem cell discoveries around the world triggered Weiss to specialize his studies further, and his connection with Cairncross became closer. Five years ago, Weiss made the decision to direct his entire lab’s focus on studying glioblastoma multiforme (an aggressive malignant brain tumour).
“I work very closely through my lab with four or fi ve other investigators who are very interested in brain tumours,” Weiss says. His investigative connections span the Hotchkiss Brain Institute, the Southern Alberta Cancer Research Institute in the faculty of medicine, at least four labs in Calgary and numerous others throughout Alberta, B.C., Quebec and Ontario. This means that, on any given day, Weiss can be found running between his offi ce and his lab, and the offi ces and labs of his colleagues, and doing all that running around while trying to push forward discov-eries, applications, and improve neurological and mental health.
“If you look up ‘team director’ you’ll probably see my picture there,” he says. “Wisely, I’m denied access to direct experimentation.”
On June 5, an $8.2-million grant was presented to Weiss and Cairncross as the principal members of a fi ve-year project to study glioblastomas and the drugs used to treat these tumours. The grant was funded by a large partnership including the Terry Fox Research Institute, The Terry Fox Foundation, Alberta Innovates – Health Solutions, the Alberta Cancer Foundation, Genome Canada, Genome B.C. and the B.C. Cancer Foundation.
“This grant is about growing brain cancer cells in the laboratory using Sam’s methods and then testing whether they’re sensitive to thousands of diff erent types of drugs,” Cairncross says. The need for the study is because even though brain cancers can look very similar under the microscope, most have diff erent genetic subtypes and require diff erent treatment regimens. Currently, the same drugs are used for all subtypes.
MAGNETIC PERSONALITY: Top students want to be in on Dr. Weiss’s groundbreaking studies.
Leap_Winter12_p40-43.indd 42 11/20/12 10:34:26 AM
A l b e r t a ’ s c a n c e r - f r e e m o v e m e n t winter 2012 43
Today’s treatments control glioblastomas (keep patients’ pain levels down and stall additional cancer growth) for a year or two with drugs; Weiss, Cairncross and their network of clinical investigators would like to increase that to fi ve, if not eight, years with newer and more eff ective drug compounds.
“We have a collective responsibility to do everything in our power to improve the quality of peoples’ lives,” Weiss says. The goal of the newly funded study, he says, is to give patients a longer, more fruitful and enjoyable life with a plethora of available, viable drugs to enable personalized treatment plans.
“I’ve transferred my energies to seeing other people make the next discoveries,” Weiss says. He’s directed his current focus on the bigger picture rather than on individual scientifi c return. “I believe that is the future of science: its impact on community,” he says.
Cairncross is not surprised Weiss is so successful in science and has become a talent magnet. “He has the ability to see the big picture and describe what he’s doing in an exciting way to everybody in the room,” Cairncross says. “Some of the very best students seek out Sam
to work with and many of them have gone on to very successful careers in science after being in Sam’s lab.”
Whether or not his love for science has passed on through his genes is questionable, though. He says, although his almost-18-year-old daughter shares an interest in biology, she’s more inclined to pursue a career in the arts and design. “It’s not up to me to suggest for a moment that she should be like me,” Weiss says. “She could give you a thousand reasons for thinking why she shouldn’t be like me.” He jokes, but he’s worked with enough students to know that people need to determine their own dreams.
Weiss is a lot of things – a mentor, researcher and director of a major medical institution – but a less obvious strength stands out to Cairncross as being Weiss’s best quality. “There are a lot of hardworking people, lots of ambitious people, lots of determined people, lots of people who persevere, but not everyone has that certain quality to notice something important when they trip over it,” Cairncross says.
When other people would just carry on, Weiss turns to get a closer look.
SAM I AM
Why did you become a scientist?My mother tells me that I was extremely inquisitive as a child and defi nitely interested in nature and biology and I liked to ask questions. So I guess there was an inclination. But for a while I was inclined as much to go be a ski bum as I was to be a post-graduate student.
Where did you study?I was an undergraduate in Montreal – I went to McGill University in 1975. I began graduate studies (at the University of Calgary) in 1978 and I had sea-son’s pass at Lake Louise so I was able to effectively balance my personal and professional interests. I graduated with my PhD in ’83. I trained for two years in France, three years in the United States and I returned in ’88 to Calgary, where I’ve been ever since.
Why did you train in France?I believe in international collaboration and co-operation so I felt that this was a great chance to exercise that concept and it was an absolutely fan-tastic experience. I learned all about discovery – I also learned about fi ne wine. I was one of the fi rst post-doctoral fellows funded by the Alberta Heritage Foundation for Medical Research to train abroad.
What would your colleagues say about you?I think their descriptors would focus around ener-
gy and ambition. I think most people would say that my positive energy and passion for my work are probably my greatest strengths.
What would your wife and daughter say about you?If they were talking about my professional per-spectives, they would say, ‘He works too hard’ – although I would argue that I do get out to the mountains enough to counter-balance that – ‘but loves what he does, and mostly has a smile on his face when he goes to work.’
Leap_Winter12_p40-43.indd 43 11/20/12 10:34:38 AM
myleapmagazine .ca44 winter 2012
Push Past
Leap_Winter12_p44-47.indd 44 11/20/12 4:12:15 PM

A l b e r t a ’ s c a n c e r - f r e e m o v e m e n t winter 2012 45
Stress begets stress, so I’ve decided not to wait until my current frantic patch at work is over. I’m making some life adjustments today
t is 2 a.m. and I’m at my computer fi ghting a deadline.Again. I know too much stress is bad for me – who doesn’t? I’ve read how excessive stress sets off fi ght-or-fl ight alarms in my brain (the hypothalamus to be exact), which triggers
my adrenal glands to release fl oods of adrenaline and cortisol. I know this hardwired response creates a burst of emergency energy that I really need right now, but it’s always followed by a crash. And I have scanned the research that shows how continuous stress, and the high cortisol levels that go with it, can cause hypertension, digestive problems, high cholesterol levels and a rundown immune system – all of which increases my risk of serious health problems, including obesity, type-2 diabetes, heart problems and possibly cancer.
None of this is news to me, one of the chronically stressed. I also know the answer isn’t more chocolate, yet another cup of coff ee, or cutting back on sleep in a desperate bid to create more time to get things done.
So why, oh why – when I am well aware of the health hazards – don’t I stop the stress-inducing behaviour? Why do I keep repeating a pattern of bad choices that don’t work? I know what I should do to safeguard my health. It’s simple: eat well, sleep well and exercise. So why don’t I? I asked three experts for some badly needed advice and helpful tips for getting back on track. If I can do it, so can you.
Push Past Pressure
BY LISA RICCIOTTI
Leap_Winter12_p44-47.indd 45 11/20/12 4:12:36 PM

Regain control of your hormone-driven brain by deliberately switching from mindless reactions to a state of
mindfulness. Stop and breathe.
myleapmagazine .ca46 winter 2012
UNDERSTAND THAT FOOD IS MOODEXPERT NO. 2: Robin Anderson, registered dietitian at Revive WellnessINSIGHT: Don’t blame your lack of willpower. There’s a reason you crave cheesecake and chips under stress. Like Mittra, Anderson points out that stress aff ects our brains, increasing our desire for higher-fat and higher-sugar foods. When we’re stressed, the brain’s internal reward pathways tend to shut down, so it desperately looks for a replacement pleasure from foods we perceive as rewards or comfort food. The trick is to know that default is ready to take over when you’re under pressure. “Be pre-emptive and proactive,” says Anderson. “Plan and prepare!”ACTION: You’re less likely to reach for a chocolate bar if temptation isn’t nearby and you have healthy options at hand, Anderson says. Clean out your environment by removing all junk foods that may trigger your desire to comfort yourself with food. Take the time to shop and restock with better options. But you don’t want to add to your stress by investing a lot of time and eff ort preparing a healthy meal.
Keep it simple, Anderson advises. Meals don’t have to be elaborate; eggs, toast and fruit are a quick, nutritious supper option in a time crunch, as is fl avoured tuna with crackers and veggies. (Buy your veggies pre-prepped to save even more time.) Become a batch cooker. Make Sunday night cooking night and prepare a big batch of soup, stew or a large casserole. Then freeze in individual containers for a quick meal. Make a large salad with a simple vinaigrette dressing that keeps well, and even improves over time. For this, use ingredients such as shredded cabbage, grated carrots, lentils and beans. You can serve it over several days, adding tomatoes, crumbled cheese and fresh greens at the last minute. Tape recipes for your favourite “fall-back meals” that use ingredients you always have on hand, inside your cupboard doors for inspiration when you’re too tired to think. If you have kids, enlist their help in preparation.
“My kids were making salads when they were eight, which made the diff erence between whether we had a salad or not,” Anderson says. For more of her tips and recipes, see revivewellness.ca.
MASTER THE MIND-BODY CONNECTIONEXPERT NO. 1: Deepika Mittra, therapist and certifi ed practitioner of mind-body medicine in EdmontonINSIGHT: Smart people do stupid things under stress because we literally stop thinking rationally. Most of the time, our cerebral neocortex is in control, Mittra explains, directing us with rational, logical thoughts. But when we’re stressed, the primitive, instinctive amygdala takes over.
Or, in non-brainy terms, Mittra says we revert to the reactions of a screaming three-year-old. When we most need the support of mind over matter to pull us through, our brains desert us. We want to feel safe, we want comfort and pleasure – and we want it now! This answers the big question of why we make bad choices under stress, and fall back into harmful habits. Seeking instant gratifi cation, we look for the quick fi x, whether that’s overeating, overdrinking, overindulging or over-doing in general. ACTION: Regain control of your hormone-driven brain by deliberately switching from mindless reactions to a state of mindfulness. Stop and breathe. Not the usual shallow, upper-chest breaths that we take, but deep and slow breathing from the abdomen. Concentrate on breathing in, slowly and deeply through your nose, hold for several seconds, then slowly exhale through your mouth. You should see your lower stomach rise and fl atten as you breathe in and out.
There’s real science behind this, Mittra says. This breathing exercise stimulates the vagus nerve, which will lower your heart rate, your blood pressure, and your stress level. Now that your thinking brain is back in
the driver’s seat, you can start thinking like an adult again and make healthy choices. “The beauty of this breathing technique is that you can do it anywhere, anytime, without anyone realizing what you’re doing,” says Mittra. “It can be your secret weapon for slaying the stress monster.”
Mittra also recommends taking mini-mental holidays through visualization by imagining yourself in a favourite place and taking mini-breaks throughout the day to stretch, move and breathe. The tech-minded can download a smartphone app called MyCalmBeat for feedback on personal breathing rates. Also, look for ongoing advice from Mittra. Visit her website, openingspaces.ca, and select Blog.
Leap_Winter12_p44-47.indd 46 11/20/12 4:12:52 PM
Exercise is fantastic for stress relief, with the bonus of mood-boosting
endorphins as a side eff ect.
MOVE YOUR BODY NOW AND OFTENEXPERT NO. 3: Chris Tse, fi tness trainer at Blitz ConditioningINSIGHT: Exercise is fantastic for stress relief, with the bonus of mood-boosting endorphins as a side eff ect. Yet people say they don’t have time to work out. Tse says doing something is always better than nothing, and if you’re making the switch from a sedentary lifestyle to an active one, start by focusing on small gains. “Ignore the Canadian Physical Activity Guidelines that call for 150 minutes of
moderate- to vigorous-intensity aerobic activity per week,” Tse suggests. Moving from non-active to 150 minutes can seem daunting. “Just start, even
if it’s only fi ve minutes a day, or fi ve minutes every couple of hours. You’ll get there, but it’s not going to happen overnight.” ACTION: Choose an activity you enjoy; you’re not going to do daily lanes if you hate swimming. Start where you’re comfortable, and then add progression. Tse fi nds that the diff erence between clients who succeed and those who don’t is motivation. He suggests keeping your motivation strong by using the buddy system. Or, put a modern twist on it and build an online support system by making your goals and progress public on Facebook or Twitter. Aim for functional, overall fi tness rather than concentrating on an isolated part of your body. And ditch the no-time and bad-weather excuses by learning exercises you can do anywhere. Check out the Blitz Conditioning blog (under Workouts) for examples of no-equipment exercises, at-home step routines and simple strength-training lifts at blitzconditioning.com.
From the Alberta Cancer FoundationTHANK YOU!
Thank you to everyone who supported this year’s Cash & Cars and More Lottery.
To date, the Cash & Cars Lottery has raised more than $21.5 million for progress in cancer research, prevention, screening, treatment and support programs for Albertans.
Your support makes this possible. Thank you!
albertacancer.ca
Leap_Winter12_p44-47.indd 47 11/20/12 4:13:05 PM

myleapmagazine .ca48 winter 2012
n 2009, Kim Arseneault found herself makingregular and unwanted trips to Edmonton from her home in Manning, nearly 585 kilometres north of the
capital, in the scenic Peace Country. Her destination was the Cross Cancer Institute where she was receiving treat-ment for ovarian/fallopian tube cancer.
“My fi rst treatment was not pleasant,” she says, “but they made some adjustments to the medicine that made it tolerable.” Fortunately, Arseneault has a daughter in Ed-monton for support. “Treatment wasn’t a walk in the park,” she says, “but it wasn’t as bad as I expected.” It certainly was not as bad as it had been for her mother, who died of cancer in 1988, despite some aggressive treatments.
“When I walked into the Cross, I was damn scared. But I looked around and I saw caring people. There was spiritual care, mind-body care... It was an amazing place.”
The treatment she received made a big impact. Her health is good she says, and there’s been no sign of can-cer in her twice-yearly follow-up tests. She’s grateful for her own physical health. Arseneault says that she was so impressed with all levels of care that she wanted to give something signifi cant back.
“I was talking to a friend from Manning, K.R. Vreel-ing, who took his treatments for multiple myeloma at the same time I was being treated,” she says. Vreeling had sim-ilar experiences and was likewise motivated to help.
Many people experience the urge to give back, but are stymied by inertia, not knowing how to start or letting the moment pass. Arseneault and Vreeling set themselves apart
with a successful fundraiser for the Alberta Cancer Foundation. Here is how their approach netted $80,000 in four hours in one evening in Manning, Alberta, population 1,164.
Arseneault is not without experience, she has been active in the community,raising funds for various things for more than 25 years. Some of the practices she has developed over the years are ones that Joe Garecht espouses. He is the driving force behind the Philadelphia-based company The Fundraising Authority, a consultancy and website he has built that specializes in training people and non-profi t organiza-tions to rev up their fundraisers. The fi rst thing a successful fundraiser needs, according to Garecht, is a fundraising goal. “You need to decide what you want your donation to accomplish,” he says, “and then fi nd out how much it will cost.” The target amount will defi ne the parameters of the event.
For Arseneault, this event hits close to home, and her goal was to raise money ear-marked for patient care. “The fi rst thing we did was to gather a committee,” says Arse-nault. “We set a goal of raising $35,000.” She got on the phone, accessed her network and used her own story to tug at people’s heartstrings – what she describes as key to the event’s success. Committee members booked a hall and started selling tables of eight, either in memory of a person who died of cancer or in support of someone undergoing treatment. “Every table at that hall had people who had been aff ected by cancer at one level or another,” Arseneault says. “We sold out in two weeks, and each table cost $500.”
Arseneault says that it proved more successful to sell whole tables to companies or families than it did to sell single seats. Businesses, such as the local branch of Finning Canada, the mill, and other oil-and-gas industry services companies all bought tables. The group’s fi rst course of action was fundraising, rather than event planning, which Garecht calls a sound approach. “The most common mistake I see is that committees spend too much time on event details and not enough on actual fundraising,” he says.
Garecht says that a fundraiser should have a budget and a written event plan. “It doesn’t need to be long or involved, but it needs to state your goal and also describe how you are go-ing achieve it,” he says. “Half the document should be devoted to the fundraising aims.”
BY MIFI PURVIS
A great fundraising event requires skill and planning. Are you ready for the task?
I
Leap_Winter12_p48-49.indd 48 11/20/12 4:13:47 PM
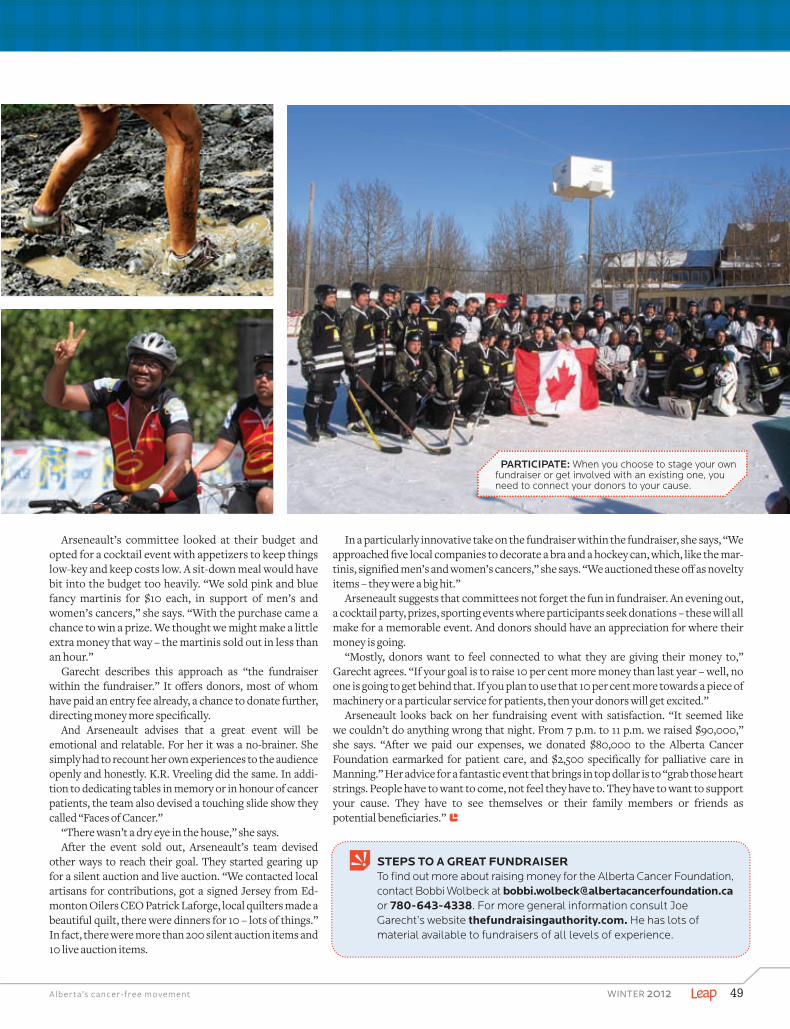
A l b e r t a ’s c a n c e r - f r e e m o v e m e n t winter 2012 49
STEPS TO A GREAT FUNDRAISERTo fi nd out more about raising money for the Alberta Cancer Foundation, contact Bobbi Wolbeck at [email protected] 780-643-4338. For more general information consult Joe Garecht’s website thefundraisingauthority.com. He has lots of material available to fundraisers of all levels of experience.
Arseneault’s committee looked at their budget and opted for a cocktail event with appetizers to keep things low-key and keep costs low. A sit-down meal would have bit into the budget too heavily. “We sold pink and blue fancy martinis for $10 each, in support of men’s and women’s cancers,” she says. “With the purchase came a chance to win a prize. We thought we might make a little extra money that way – the martinis sold out in less than an hour.”
Garecht describes this approach as “the fundraiser within the fundraiser.” It off ers donors, most of whom have paid an entry fee already, a chance to donate further, directing money more specifi cally.
And Arseneault advises that a great event will be emotional and relatable. For her it was a no-brainer. She simply had to recount her own experiences to the audience openly and honestly. K.R. Vreeling did the same. In addi-tion to dedicating tables in memory or in honour of cancer patients, the team also devised a touching slide show they called “Faces of Cancer.”
“There wasn’t a dry eye in the house,” she says.After the event sold out, Arseneault’s team devised
other ways to reach their goal. They started gearing up for a silent auction and live auction. “We contacted local artisans for contributions, got a signed Jersey from Ed-monton Oilers CEO Patrick Laforge, local quilters made a beautiful quilt, there were dinners for 10 – lots of things.” In fact, there were more than 200 silent auction items and 10 live auction items.
In a particularly innovative take on the fundraiser within the fundraiser, she says, “We approached fi ve local companies to decorate a bra and a hockey can, which, like the mar-tinis, signifi ed men’s and women’s cancers,” she says. “We auctioned these off as novelty items – they were a big hit.”
Arseneault suggests that committees not forget the fun in fundraiser. An evening out, a cocktail party, prizes, sporting events where participants seek donations – these will all make for a memorable event. And donors should have an appreciation for where their money is going.
“Mostly, donors want to feel connected to what they are giving their money to,” Garecht agrees. “If your goal is to raise 10 per cent more money than last year – well, no one is going to get behind that. If you plan to use that 10 per cent more towards a piece of machinery or a particular service for patients, then your donors will get excited.”
Arseneault looks back on her fundraising event with satisfaction. “It seemed like we couldn’t do anything wrong that night. From 7 p.m. to 11 p.m. we raised $90,000,” she says. “After we paid our expenses, we donated $80,000 to the Alberta Cancer Foundation earmarked for patient care, and $2,500 specifi cally for palliative care in Manning.” Her advice for a fantastic event that brings in top dollar is to “grab those heart strings. People have to want to come, not feel they have to. They have to want to support your cause. They have to see themselves or their family members or friends as potential benefi ciaries.”
PARTICIPATE: When you choose to stage your own fundraiser or get involved with an existing one, you need to connect your donors to your cause.
Leap_Winter12_p48-49.indd 49 11/20/12 10:32:39 AM

myleapmagazine.ca50 winter 2012
Constructing SuccessWhen Betty Sampson’s daughter Sarah, a nurse who works at the Cross Cancer Institute, brought home an issue of Leap magazine, she encouraged her mom to participate in a new event highlighted on the cover: Bust a Move for Breast Health, or BaM, running in both the Edmonton and Calgary this year.
“She said ‘Hey Mom, you should do this. You’re an exercise nut and this is really cool. I said, ‘Sure, let’s do it together.’ She said ‘No, you do it,’” Sampson recalls with a laugh.
Undeterred, Sampson turned to her colleagues at PCL Constructors Inc., where she has participated in an in-house boot camp for years. “I approached one of my girlfriends in the boot camp and said, ‘Do you feel like doing this with me?’” The answer was yes and soon Sampson had recruited a team of fi ve women and men, including one member whose wife recently went through cancer treatment.
Sampson, who describes her teammates as headstrong and motivated people, says the group began asking friends, family and co-workers for donations. They also adopted a new name – Chesticles. In their one month of fundraising, the Chesticles raised more than $33,000, which was the highest amount raised by a team at Edmonton’s new Bust a Move event.
Next it was time for the actual event, which involved hundreds of people in
outrageous costumes participating in a giant fitness class at Edmonton’s Northlands Expo Centre. “We had no idea it would be so much fun,” she says. “It was hard work but it was such an amaz-ing atmosphere; it was inspiring. We walked away and could not shut up about the event for weeks.”
As for Sampson’s motivation for joining in, aside from a pestering daughter? “I did it because I don’t have a cancer story,” Sampson says. “I don’t want a story; I want to go through life with-out one. I have two daughters at home and I want them to go through life without these stories, too.” – Cailynn Klingbeil
BUSTING OUT SOME MOVES: (Left to right) John Waters, Denis Dubord, Betty Sampson, Danielle Schnurer, Kylene Nauman hold keynote Bust-a-Mover Richard Simmons.
Visit bustamove.ca for more information
myleap / INSPIRING INDIVIDUAL
NATIONAL TITLE SPONSOR
REGISTER TODAY! CONQUERCANCER.CA[888] 624-BIKE [2453]
THE RIDE IS BIGGER AND BETTER IN 2013!
The Enbridge® Ride to Conquer Cancer® benefiting the Alberta Cancer Foundation has a new route, campsite, and a whole new direction to ride in!
Space is limited, so be sure to secure your spot in history today!
JUNE 22-23, 2013
Leap_Winter12_p50-51.indd 50 11/20/12 10:31:45 AM

NATIONAL TITLE SPONSOR
REGISTER TODAY! CONQUERCANCER.CA[888] 624-BIKE [2453]
THE RIDE IS BIGGER AND BETTER IN 2013!
The Enbridge® Ride to Conquer Cancer® benefiting the Alberta Cancer Foundation has a new route, campsite, and a whole new direction to ride in!
Space is limited, so be sure to secure your spot in history today!
JUNE 22-23, 2013
Leap_Winter12_p50-51.indd 51 11/20/12 10:31:57 AM

For an unforgettable six hours this March, join hundreds of women and men as they jump, jive, dance and laugh while raising valuable funds for breast health in Alberta. 1.855.250.MOVE
TODAY ATREGISTER
COMINGEDMONTON MARCH 2013
&CALGARY
For an unforgettable six hours this March, join hundreds of women and men as they jump, jive, dance and laugh while raising
REGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTERREGISTER
EDMONTON &CALGARY
BUSTAMOVE.CA
000Leap-BustAMove-FP.indd 1 11/6/12 2:02:08 PMLeap_Winter12_p52-01.indd 52 11/20/12 10:30:47 AM