leadership: developing your team for icd-10 - … · leadership: developing your team for icd-10...
TRANSCRIPT

Leadership: Developing your Team for ICD-10
WSHIMA-2016 Annual MeetingApril 28, 2016 in Lynnwood, WA
Laura Legg, RHIT, CCS, CDIP
Carole Morris, CCS-P, CHC
Objectives
Discuss Post ICD-10 Leadership strategies for:
• Post implementation challenges
• Motivating staff to keep learning ICD 10, including new codes
• Coding productivity and quality metrics
• Effective auditing post-implementation
• Key Performance Indicators


Challenges of Implementation
What we have learned:
• Coder specialization
• Lack of CDI program to assist with provider education
• Collaboration between CDI and Coding
• Productivity transitions across all patient types
• Increased time for coding and chart review
Coder specialization
• 46% coders code IP or OP
• 54% code other record types regularly or as needed
• Cross training optimal

CDI Challenges
• Lack of CDI program to assist with provider education
• 26% hospitals had no CDI program
• 11.8% CDI programs are new <12 months

Collaboration between CDI and Coding
• 45% CDI and coding both under HIM department
• Strong collaboration=optimal results
• Aggressive programs with high physician involvement

Productivity Transitions
• All patient types
• More time for record review
-Operative reports for PCS
-clinic records for specificity for diagnosis codes instead of signs and symptoms

Key performance indicator Expected increase or decrease Note
Clinical Quality:
Query rate Increase 25% 20-25%
Query response rate N/A No change
Operational:
DNFC Increase 25%-45% Inversely correlated to coding productivity
Coder productivity Decrease 25%-45% Inpatient, 45%; outpatient, 25%; highly dependent on amount of practice dual coding
Coder quality N/A Variable based on education and coder skill
CC/MCC capture rate N/A Focus effort on capturing robust documentation, including MCC/CC
Financial:
Gross AR days Increase 10%-20% Increase expected to last longer than 90-day stabilization period; likely to last nine months or more
Denial rates Increase 100%-200% Still expecting
ICD-10 key performance indicators-Early on
Source: Reprinted with permission from Whittle Advisors, LLC.

Next Steps
• Keep up to date on ICD-10 through education
• Assess your ICD-10 progress to identify potential issues
• Troubleshoot issues identified through your monitoring of KPIs
• Deploy tactics
Keeping up to date through Education
• Thawing of the Code Freeze
• Advanced PCS education
• Advanced anatomy and physiology education
• Pharmacology education
• Motivation to keep learning

Thawing of the Code Freeze
• Partial Code Freeze began October 1, 2011
• October 1, 2016-Regular updates to ICD-10 will begin

PCS updates
• 75,625 valid PCS codes for FY 2017
• 3,651 new codes
• 487 revised code titles
• 97% are cardiovascular system codes
Code changes will be implemented in October 2016 or 2017
New Cardiovascular PCS codes
• Unique device values for multiple intraluminal devices
• Qualifier bifurcation to multiple root operation tables of all artery body part values
• Specific body part values for thoracic aorta
• Specific table values to capture congenital cardiac procedures
• Codes involving placement of an intravascular neurostimulator
Other PCS Changes
• New codes in lower joint body system
• Expanding the body part detail for root operations Removal and Revisions
• Adding unique codes for unicondylar knee replacement
• New codes intracranial administration of substances such as Gliadel chemotherapy wafer using an open approach
Other PCS Changes
• Face transplant
• Hand transplant
• Donor organ perfusion
Now that the code freeze has ended all current and future ICD-10 PCS code proposals will be considered for implementation during the following fiscal year.


ICD 10 CM changes• 1,928 diagnosis codes for fiscal year 2017
Expanded code choices for:
– Atrial fibrillation
– Heart failure
– Diabetes Mellitus, type 2
– Disorders of the breast
– Pulmonary hypertension
– Other

Planning for adoption
• Provide coding education
• Plan for similar to large volume of changes for CPT each year
• Ensure that staff understand the changes and know how to apply the correct codes

Motivation
How do we motivate staff to keep learning in ICD-10?
• New teaching methods and tools
• Avoid training fatigue (death by Power Point!)
• Make it fun!
Building ICD-10 Education
• Use AHA Coding Clinic
• Highlight subtle changes that change a DRG
• Check the literature-websites, blogs, journals
• Tackle the most confusing and controversial issues head-on
• Use real case examples

Creating “Champions”
• "Evaluate your current situation"
• "Paint the bigger picture"
• "Communicate often "
• "Eliminate the mythology"
• "Use technology"
• "Evaluate your program"

Assessing your ICD-10 Progress
Step 1: Assess progress by identifying key performance indicators, establish a baseline for each
-Compare post-transition KPIs to that baseline
Assessing your ICD-10 Progress
Step 2: Address the findings by:
• Developing ways to gather and address feedback
• Check clinical documentation and code selection
• Verify that all system upgrades are installed
• Work with payers to resolve billing issues
Assessing your ICD-10 Progress
Step 3:
• Maintain progress by keeping coding tools and systems updated
• Regularly review ICD-10 general coding guidelines

KPI-Coding Productivity
• Identify productivity in ICD-9 to establish baseline into ICD-10
• Evaluate workflow and identify what is reasonable
• ICD-9 metrics will not cross over to ICD-10
• Identify obstacles
• Conduct a 30 day trial, prior to enforcement of new standards
Coding Productivity
• Solicit coder and administration buy-in for new standards
• Continue to evaluate productivity with willingness to modify
• Monitor AHIMA for publication of new standards

HRG Internal Standards
• NOTE: These productivity expectations may need to be adjusted based on the case-mix, organizational complexity (teaching, rural, community), acuity, and work assignments other than coding.
Inpatient OBS SDS ER Ancillary Clinic
2 3 5 8-10 15-17 8-10

KPI-Coding Accuracy
• Anticipate decrease in accuracy from ICD-9 to ICD-10
• Increase amount of quality assessments to identify knowledge gaps
• Provide focused education
• Work with providers and or leadership on deficiencies in provider documentation

Coding Accuracy
• Provide educational tools and resources
• Balance productivity with accuracy
• Always remember coders take pride in their work and communication method is key

Post-implementation Auditing

Effective Auditing
• You don’t know what you don’t know
• Sufficient volumes
• Account selection
• Feedback specific to ICD 10 Chapters & new codes
• PCS trends

ICD-10 CM auditing
CODE DEFICIENCY CODE ICD-10 Chapter
A Infectious Disease
DX Not adequately documented to code: C Neoplasms
A Disease type specificity D Disease of blood & blood forming organs
B Manifestation E Endocrine & Metabolic
C Chronicity F Mental & Behavioral
D Location/Laterality G Nervous system
E Other H Eye & Ear
I Circulatory system
PX Not adequately documented to determine: J Respiratory system
1 Root Operation K Digestive system
2 Body Part L Skin
3 Approach M Musculoskeletal system
4 Device N Genitourinary system
5 Qualifier O Pregnancy
6 Other S Injury & Poisoning

AUDIT # PHYSICIAN SPECIALTY MR# ACCOUNT # ICD-10 CHAPTER DEFICIENCY CODE PDX/PPX CC/MCC REMARKS
1 Example IM A C 1 strep pathogen not specifically documented
2 IM D A Anemia type not specified (Five codeable diagnoses left off DS list)
3 IM I A (seven codeable diagnoses left off DS list), CHF NOS
4 IM A E 1 Sepsis & pneumonia (possible asp not clarified) no organism documented;
B gastroparesis and DM not linked on DS
5 IM D A Anemia NOS
6 IM
7 IM
DS first listed diagnosis is Bandemia (even though the bandemia resolved 2 days after admission) and the actual diagnosis is aspiration pneumonia. Continued a diagnosis as first-listed in their progress notes even after it is resolved and/or ruled out.
8 IM D A Malnutrition not specified as mild, moderate, or severe
9 IM A A Stomatitis vs Mucositis vs cellulitis of the floor of the mouth
10 IM N C Stage CKD not documented. Stage I-V (IV &V are CC's)
11 IM D AAnemia due to chronic disease can be further specified as due to CKD (Anemia of Chronic Kidney disease) Patient is stage V with need for dialysis
12 IM No Recommendation
13 IM No Recommendation
14 IM L C Lymphadenitis is classified in I10 for both acute and chronic
15 IM No Recommendation
16 IM No Recommendation
17 IM No Recommendation
18 IM K C 1
Cholangitis is classified in ICD10 as primary and chronic nonsupprative destructive, to identify severity. Cholangitis is further classified in I10 with calculus to identify this condition not classified in I9. Current documentation does not identify acuity.
19 IM N C 1
Pyelonephritis is not further specified as acute or chronic in the documentation. ICD10 classifies pyelonephritis associated with ureteral obstruction or stricture, reflex uropathy and hydronephrosis.
20 IM No Recommendation

ICD-10 PCS
PX Not adequately documented to determine:
1 Root Operation
2 Body Part
3 Approach
4 Device
5 Qualifier
6 Other

Butterfly glioblastoma for stereotactic brain biopsy. Change procedure code 00B00ZX, Excision of Brain, Open Approach, Diagnostic to 00B03ZX, Excision of Brain, Percutaneous Approach, Diagnostic. Per Operative report, "The trajectory for plan 1 was locked and the biopsy needle measured to, using the bovie to coagulate the dura was passed and then biopsy specimen was obtained. Per definition of Percutaneous surgical approach is "Entry, by puncture or minor incision [burr hole], of instrumentation through the skin or mucous membrane and any other body layers necessary to reach the site of the procedure." See Coding Clinic, Third Quarter 2015: Page 11 for additional information regarding burr holes.Reviewers note: Burr holes as approach percutaneous vs. open is a contentious subject as it's conceptually borderline and makes a huge change in DRGs. This was a legitimate OR procedure and probably ought to be "open" from an intuitive standpoint but the current references guide using "percutaneous".
PCS Feedback

PCS Feedback
Mini craniotomy with evacuation of hematomaDelete procedure code 009400Z, Drainage of Subdural Space with Drainage Device, Open Approach. Patient had both drainage of liquid hematoma as well as clotted material. Per Coding Clinic, Third Quarter 2015: Page 10, "An acute subdural hematoma is characterized by a solid or gelatinous clot. A chronic subdural hematoma is typically composed of liquid matter rather than solid. If the procedural report only describes evacuation of liquid or fluid, use the root operation "Drainage." The root operation "Extirpation" is used when solid matter is removed. If there is both drainage of liquid and cleaning out of solid matter, code only "Extirpation." When this information is not available, "Extirpation" is the default
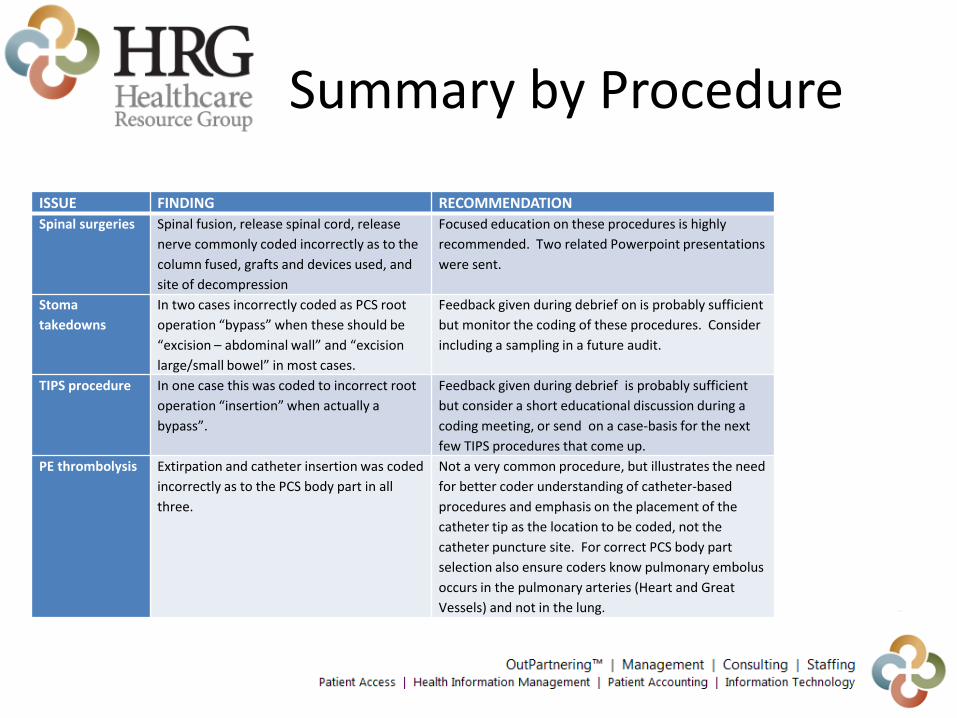
ISSUE FINDING RECOMMENDATION
Spinal surgeries Spinal fusion, release spinal cord, release
nerve commonly coded incorrectly as to the
column fused, grafts and devices used, and
site of decompression
Focused education on these procedures is highly
recommended. Two related Powerpoint presentations
were sent.
Stoma
takedowns
In two cases incorrectly coded as PCS root
operation “bypass” when these should be
“excision – abdominal wall” and “excision
large/small bowel” in most cases.
Feedback given during debrief on is probably sufficient
but monitor the coding of these procedures. Consider
including a sampling in a future audit.
TIPS procedure In one case this was coded to incorrect root
operation “insertion” when actually a
bypass”.
Feedback given during debrief is probably sufficient
but consider a short educational discussion during a
coding meeting, or send on a case-basis for the next
few TIPS procedures that come up.
PE thrombolysis Extirpation and catheter insertion was coded
incorrectly as to the PCS body part in all
three.
Not a very common procedure, but illustrates the need
for better coder understanding of catheter-based
procedures and emphasis on the placement of the
catheter tip as the location to be coded, not the
catheter puncture site. For correct PCS body part
selection also ensure coders know pulmonary embolus
occurs in the pulmonary arteries (Heart and Great
Vessels) and not in the lung.
Summary by Procedure

Key performance indicators
• Coder productivity—number of medical records coded per hour; review by individual coder
• Physician query rate— number of records coders return to clinicians with requests for more documentation to support proper code selection
• Requests for additional information—number of requests from payers for additional information required to process claims

Key Performance Indicators
• Incomplete or missing diagnosis codes—number of incomplete or missing ICD-10 diagnosis codes on orders
• Use of unspecified codes— volume and frequency of unspecified code use
• Medical necessity pass rate— rate of acceptance of claims with medical necessity content

Key performance indicators
• Days to final bill - number of days from date of service until providers generate and submit claim
• Claims acceptance/rejection rates-percentage of claims accepted/rejected during payer front-end edits (before entering the payer’s adjudication system)
• Claims denial rate—percentage of claims accepted into the payer’s adjudication system that are denied
Hospital Inpatient Services
• DNFB—or discharged not final billed, the number or rate of patients who have been discharged without the hospital issuing a final bill; look at the number of claims in DNFB within 30 days of Timely Filing guidelines
• DNFC-Discharged not final coded
• DRG volumes under ICD-9 versus ICD-10

Deploy tactics-Track & Improve
Develop a Feedback System
-Create processes to gather feedback and questions from your staff.
-Create an issues list where staff can document new issues in one location as they arise.
-Track the system or payer with the issue, steps taken to resolve it, and the current status.
Clinical Documentation
• Look at clinical documentation by provider
• Issues with documentation might result from insufficient clinician training on ICD-10 coding concepts and guidelines
• Any lag times in responses to coder questions can further affect related key performance indicators

Check Code Selection
• Understand your processes for selecting diagnosis codes and applying coding guidelines to help identify the sources of issues and to target remediation efforts
• Provide education resources for your clinicians and coders
• Identify a physician champion to act as a liaison and offer best practices

Check System Issues
• Verify your systems have implemented available upgrades.
• Check for technical problems with your systems
• Work with your vendor to resolve any systems issues affecting productivity

Resolve issues with Payers
• The Medicare/Medicaid Provider Contact List can be useful if you are experiencing issues with KPIs that are specific to Medicare Fee-For-Service (FFS) or Medicaid.
• For other issues with KPIs, contact your payer, clearinghouse, or billing service.
Look to the Future
• What will HIM look like in 5 years?
• How will value based health care financing and payment contribute to change?
Questions

Contact information
Carole Morris, CHC, CCS-P
Vice President of Coding Services
Healthcare Resource Group
Phone: 509-209-2049
Laura Legg, RHIT, CCS, CDIP
AHIMA approved ICD-10 CM/PCS Trainer
Healthcare Resource Group
Director of Consulting and Education
Phone: 509-209-2013

References
• Centers for Medicare and Medicaid Services ICD-10 CM Official Guidelines for Coding and Reporting, 20-16. http://www.cdc.gov/nchs/data/icd/10cmguidelines.2016_Finalpdf
• Centers for Medicare and Medicaid Services, ICD-10-PCS Official Guidelines for Coding and Reporting, 2016. https://www.cms.gov/Medicare/Coding/ICD10/Downloads/2016-Official-ICD-10-PCS-Coding-Guidelines.pdf
• American Hospital Association, AHA Central Office Website. http://www.ahacentraloffice.org/
52
5/3/2016