labor and delivery powerpoint 2
DESCRIPTION
laborTRANSCRIPT
Four ’s of Labor
Passenger Power Passageway Psyche
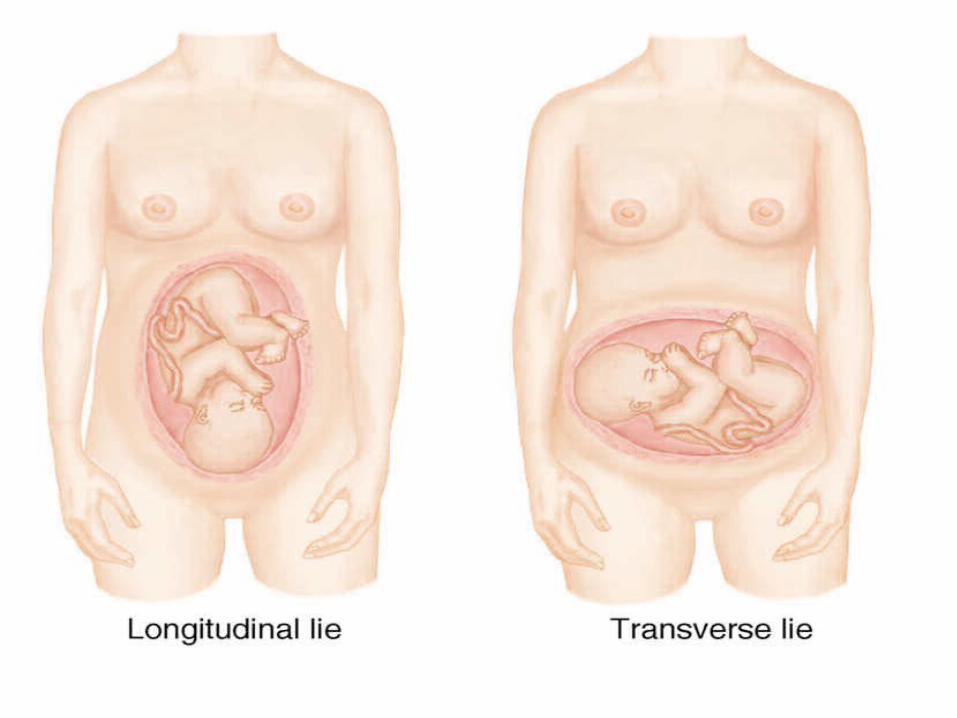
Passenger Lie – Relationship of the longitudinal
axis of the baby to the longitudinal axis of the mother
Longitudinal Transverse Which do you think was intended?
Passenger Issues with Transverse Lie
1)
2)
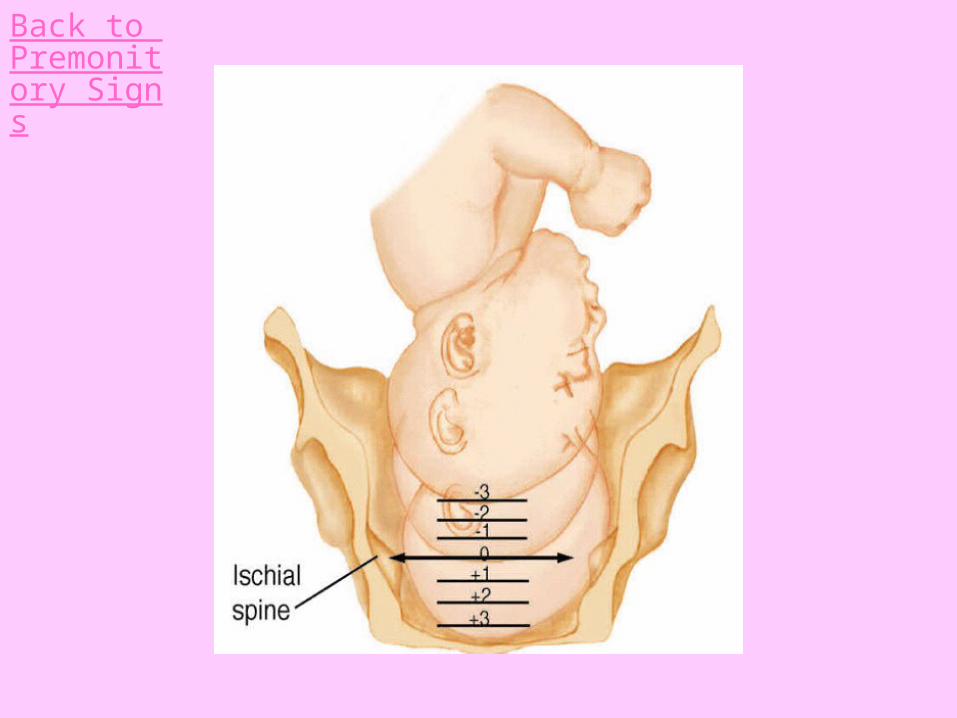
Passenger – Station Relationship of the presenting part
to the ischial spines Engagement – Station 0 or below Minus stations – Above the spines Positive stations – Below the spines
Back to Premonitory Signs
Passenger – Presentation Part of the passenger that
enters the pelvis first Vertex presentation – 95% Breech presentation – 4% Brow, face, shoulder - 1%

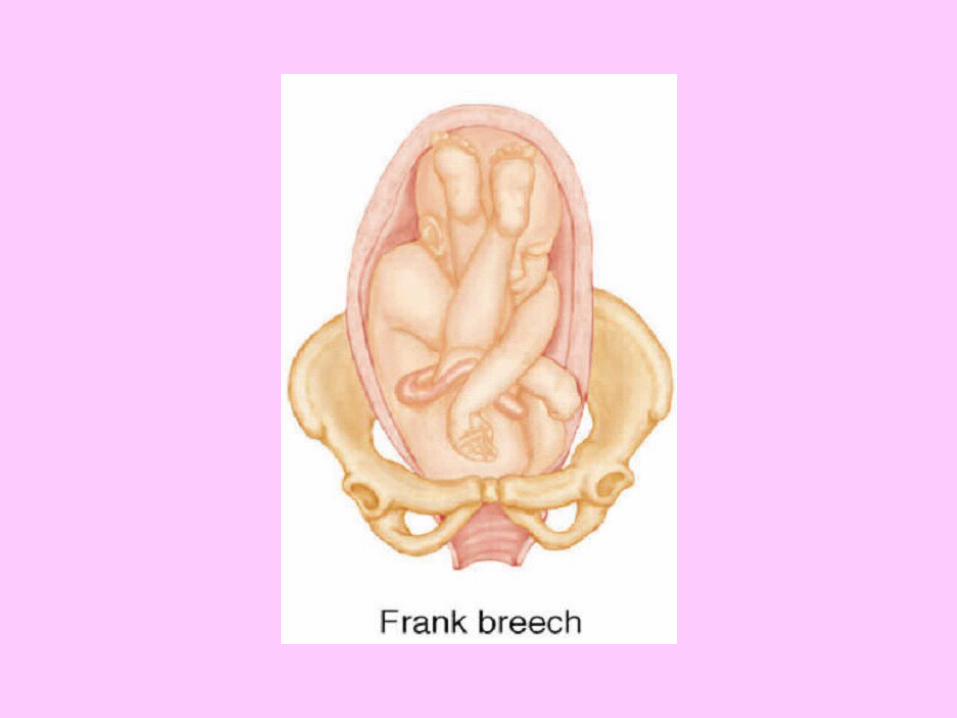
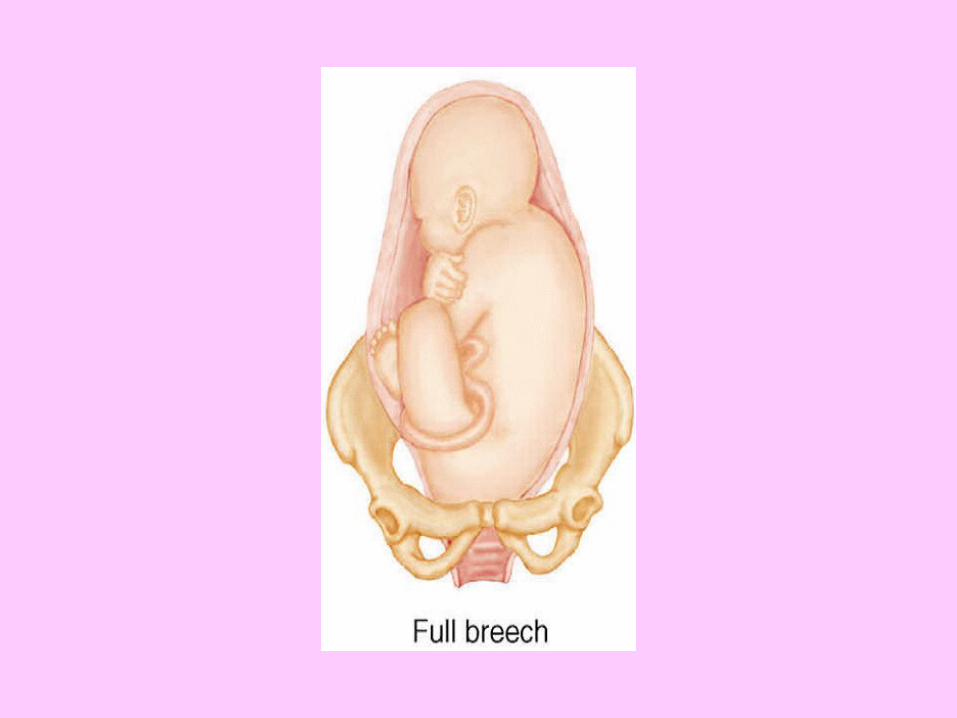
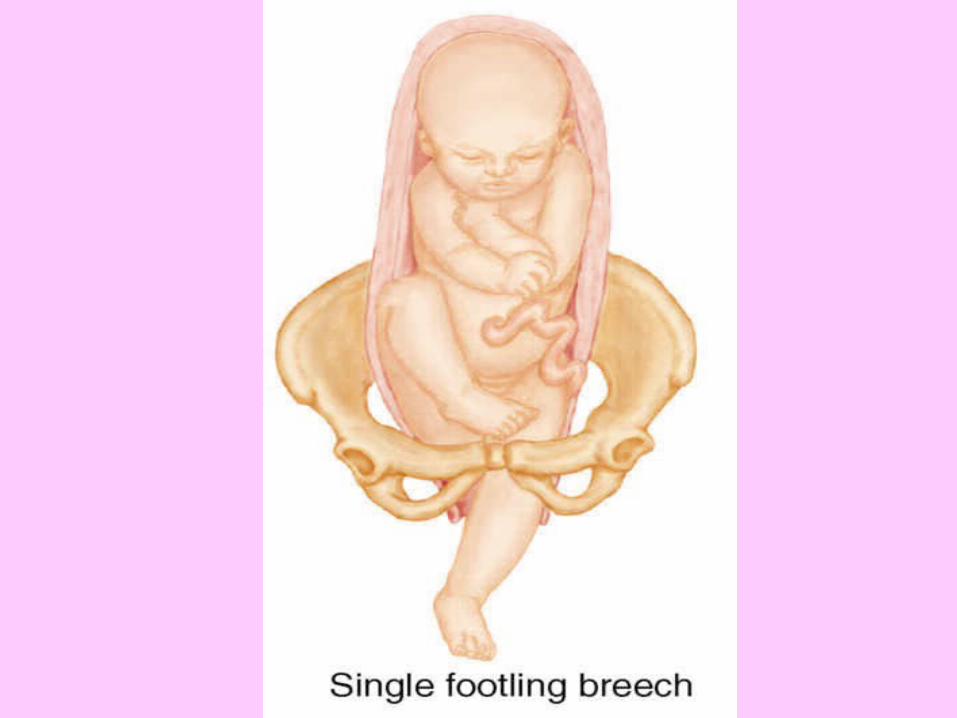
Passenger – Breech Presentation Footling breech– double or single Frank breech Complete breech
Passenger – Risks of Breech Presentation
Prolapsed cord CPD Asphyxia C/S
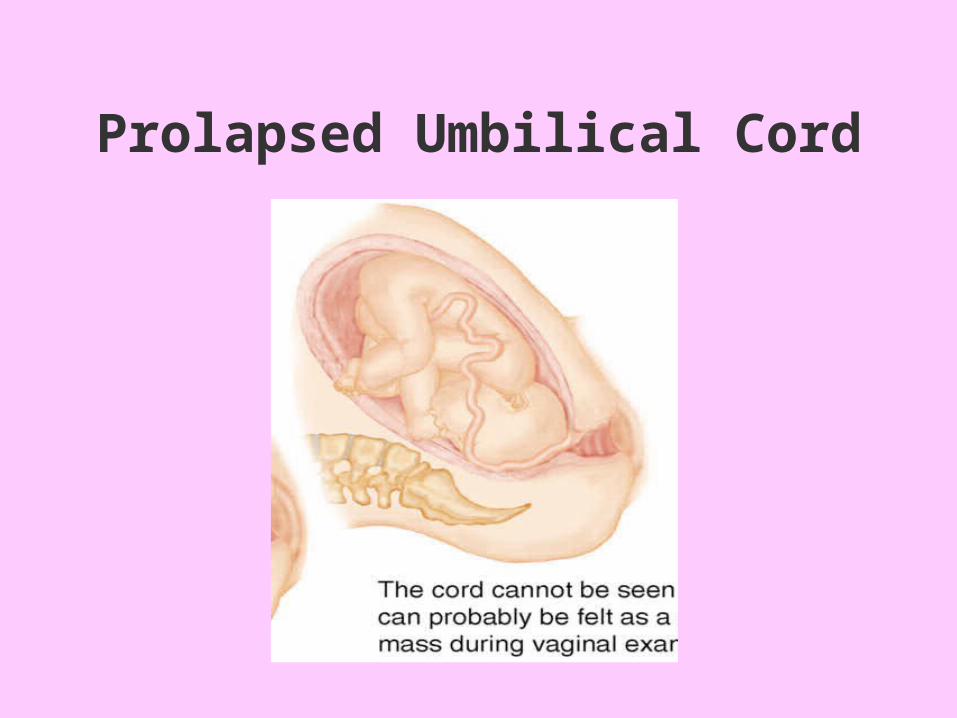
Prolapsed Umbilical Cord
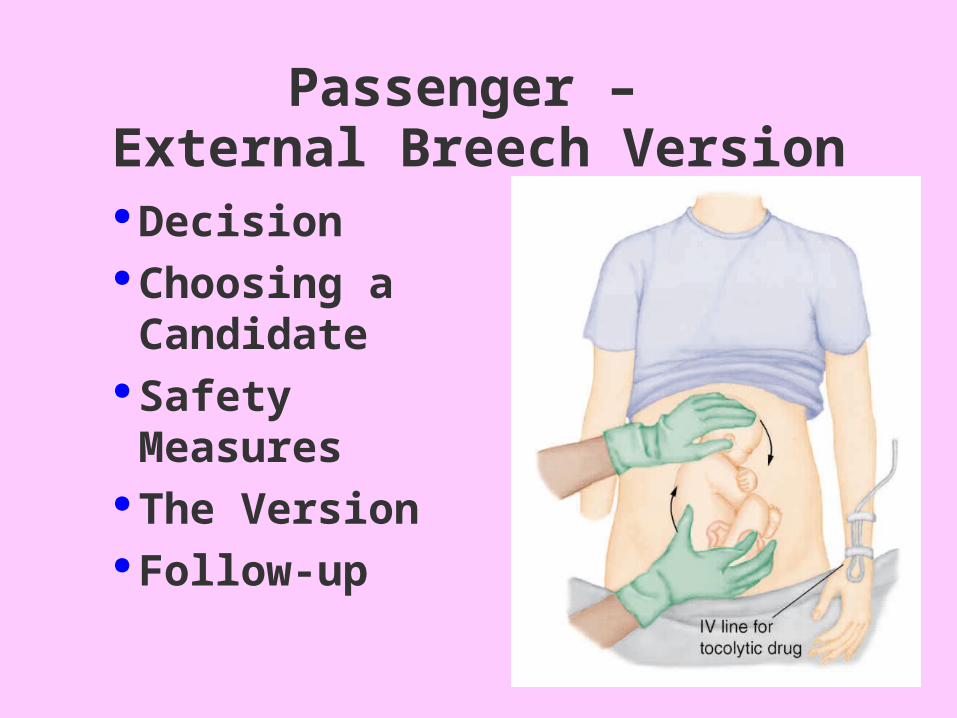
Passenger – External Breech Version
Decision Choosing a
Candidate Safety Measures The Version Follow-up
Increased risks:Preterm labor and birthCesarean DeliveryPostpartum Hemorrhage
Passenger – Multiple Passengers
Passenger – Position Three letters denoting relationship of a
landmark on the baby to the mother’s pelvis
Landmark = Occiput/vertex
Sacrum/breech Ex. LOA = Left occiput anterior (The occiput of the baby is pointing toward
the left front of the mother’s pelvis.)
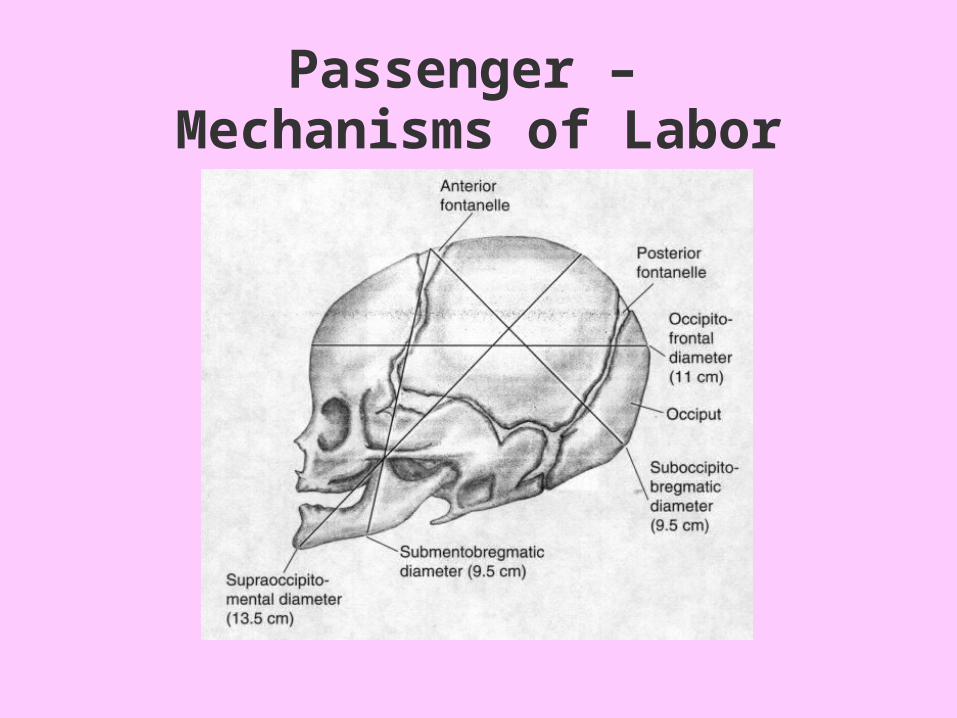
Passenger – Mechanisms of Labor
Movements of the baby through the pelvis during labor/birth. Each is essential to an easy, safe passage.
Engagement/ descent Flexion Internal rotation Extension External rotation/restitution
Passenger – Mechanisms of Labor
Power! Power during labor comes
from strong contraction of the upper uterine segment
2nd stage – adds power of abdominal muscles
Use of DRUGS to augment (“to add to”) or induce (“to begin”) labor, or ripen(“soften and efface”) the cervix
Action: Stimulate uterine contractions Prostaglandins
Prepidil gel
Cervidil vaginal insert
Cytotec vaginal tablet Oxytocin
Power!
Cervical Ripening Agents
ProstaglandinsEvening Primrose OilMechanical dilation using balloon cath.“Stripping” the membranesCastor Oil Sexual Intercourse
Most common reasons for induction:
1)
2) Other reasons: Who would not be a candidate
for induction?
Power!
Power! – Safe Use of Oxytocin Know the Standard of Care! Follow protocols exactly Start slowly and evaluate before
advancing Watch patient, vital signs and fetal
monitor Know side effects When to hold? When to fold?
Collaborate!
Power! – Risks of Oxytocin in a Pregnant Patient
Hyperstimulation Fetal distress Uterine rupture Hypertension
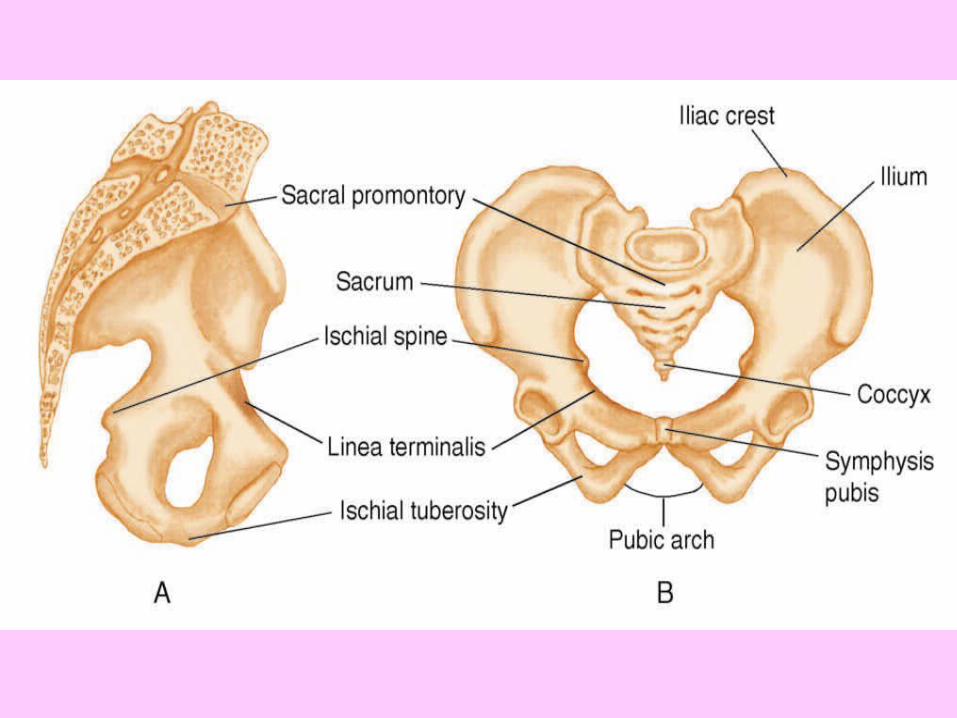
Passageway – Pelvic types
types -
gynecoid
android
anthropoid
platypelloid
Passageway – Pelvic Characteristics
If you were a baby shopping for a great pelvis to be born from, which would you choose? Why?
1)
2)
3)
4)
Passageway – Pelvic Measurements
Diagonal Conjugate – usually about 12.5cm measured vaginally from the symphysis to the sacral promontory
True Conjugate – measurement from the top of the symphysis to the sacral promontory estimated by subtracting 1.5cm from the diagonal conjugate
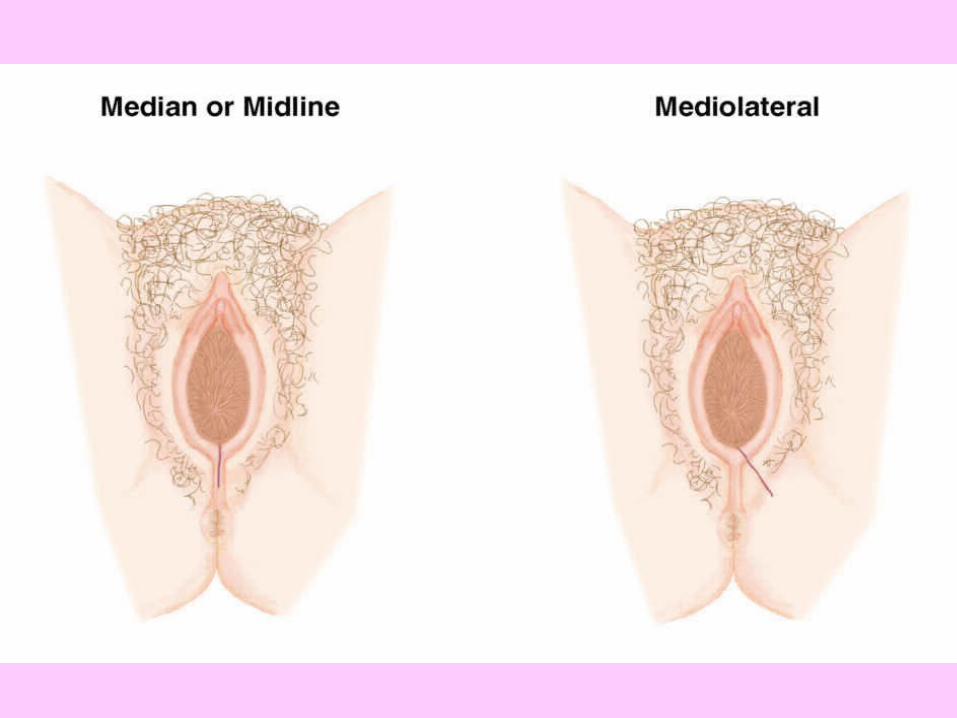
Passageway – Episiotomies & Lacerations
Midline/Median episiotomies are the most common
Cut right before the delivery of the head to minimize blood loss
Midline = Skin and perineal muscle May extend into the anal
sphincter/rectal mucosa if lacerations occur
Passageway – Lacerations1st degree = tearing of perineal skin2nd degree = skin & perineal muscle3rd degree = skin, muscle & anal
sphincter4th degree = skin, muscle, sphincter
& rectal mucosa
Passageway – Life After Lacerations?
Yes! These usually heal quickly and well facilitated by:
1)
2)
3)
4)
5)
Possible Indications for C/S
Cephalopelvic disproportionActive genital herpesNonreassuring fetal heart rate patternsProlapsed umbilical cordFetal malpresentations (breech, transverse lie)Certain prior uterine surgeries (classical
cesarean incision, etc.)Certain maternal diseases where labor not
advisable

Skin Incisions for Cesarean Birth

Uterine Incisionsfor Cesarean Birth
Nursing Care Preparing for C/S
Pre-op teaching (if possible)Touch, eye contact, info. to decrease anxietyNeeds IV line, Foley, shave prep lower abd.Keep NPO- may give antacid like “Bicitra”Notifies pediatrician – Prepare baby itemsPositioning on OR table - displace uterusMonitor FHR until procedure-check one more
time prior to surgery
VBACVaginal Birth After CesareanSuccess rate 70-80%Candidates for VBAC (ACOG): - 1 prior low-transverse C/S
- clinically adequate pelvis
- no other uterine scars or prior uterine rupture
- MD immediately available to perform emerg. C/S
Risks of VBAC: - uterine rupture
- fetal/maternal death
- hysterectomy
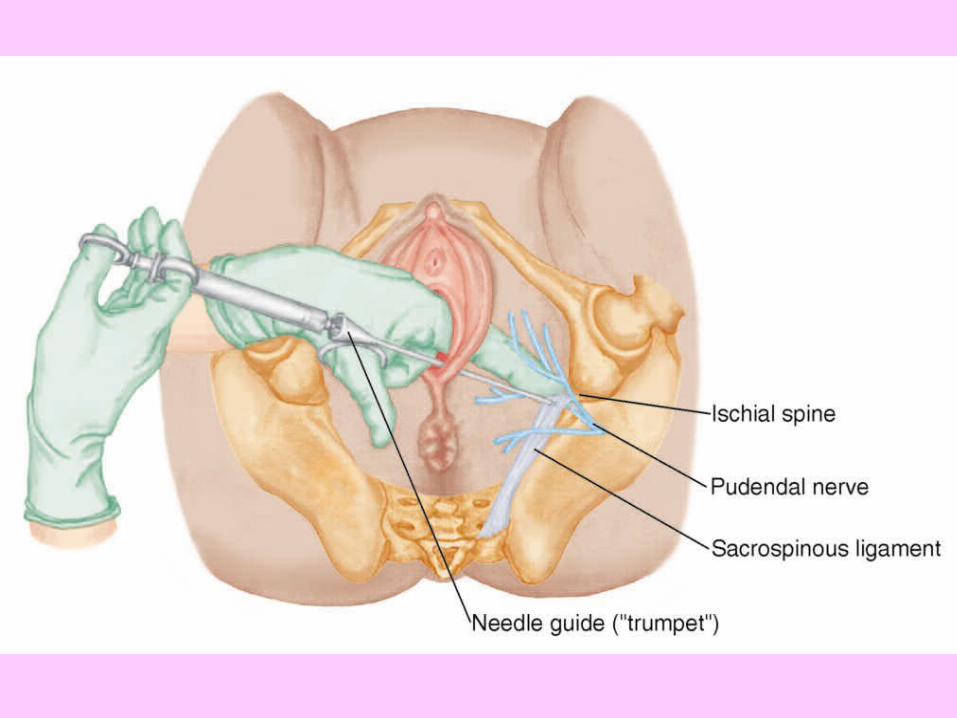
Anesthesia - Local Local infiltration of the Perineum Pudendal Block –
infiltration of the pudendal nerves transvaginally
provides effective perineal anesthesia
performed using an Iowa trumpet late in 2nd stage
very low risk/few side effects
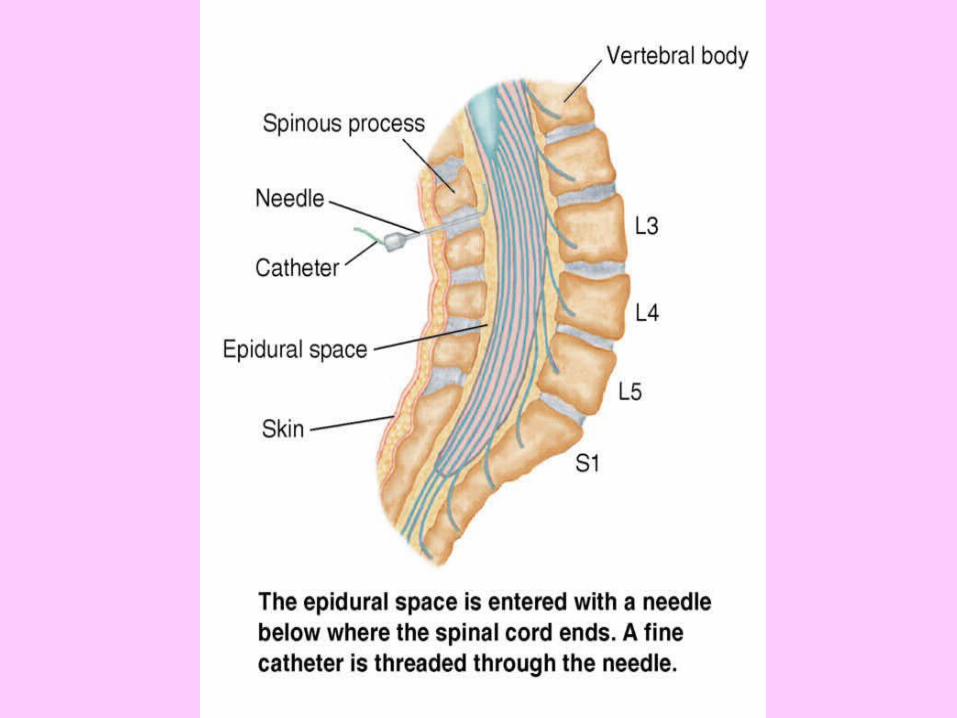
Anesthesia – Regional
Continuous Lumbar Epidural (CLE) - provides relief from contraction pain
during labor/C/S usually given once active labor
established ( but may be given earlier/later depending on situation)
no penetration of dura, so no risk of headache
give fluid bolus to decrease hypotension risk
Anesthesia – RegionalSpinal Block
• Used for cesarean birth, or BTL
• Not used for vaginal delivery
• Penetration of dura may cause post spinal HA
• Hypotension risk also tx. with fluid bolus
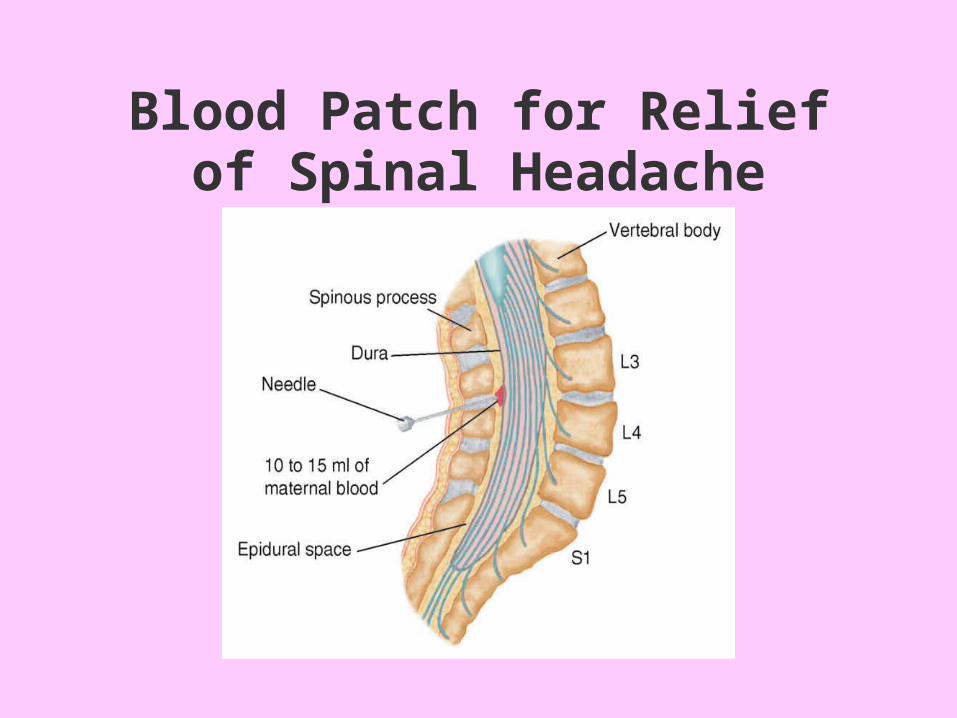
Blood Patch for Relief of Spinal Headache
Anesthesia – RegionalRisks for CLE and Spinal
Hypotension Urinary catheterization Infection Ascending anesthesia
*Need to have informed consent for regional anesthetic!