kenneth d. candido, m.d. chicago, illinois - fsipp · kenneth d. candido, m.d. chicago, illinois...
TRANSCRIPT

227 Page 1
Spinal Injections for the Diagnosis and Treatment of Chronic Pain
Kenneth D. Candido, M.D. Chicago, Illinois
Pain arising from the spine continues to be a challenging and vexing problem in terms of diagnostic assessment and implementation of therapeutic measures designed to modulate it. There are significant economic, social and health impacts of chronic spinal pain. There are multiple distinct potential and diverse pain generators that may be functioning individually or in tandem to produce a unique pain experience in any given individual. The present discussion will be limited due to space constraints to pain emanating from the cervical and lumbar spinal regions. Additionally, the interventions discussed will include the following: cervical interlaminar and transforaminal injections and medial branch blocks; lumbar interlaminar, caudal and transforaminal injections and medial branch blocks; and sacroiliac joint injections. Admittedly, this is merely a concise overview of an extremely complex topic. The interested reader is referred to the reference section for a somewhat more comprehensive bibliography. Nature and Scope of the Problem Chronic pain consists of pain that persists for a minimum of six months following an injury or disease process, extending beyond the typical course of healing of the underlying process, which is associated with chronic pathologic processes that cause continuous or intermittent pain indefinitely, even continuing in the absence of pathology, which may never heal1. Prevalence of chronic pain is 2-40% of adults and the lifetime prevalence of spinal pain is 54-80%. The surgical treatment of spinal pain includes more than 285,000 laminectomy/discectomy and close to 300,000 fusion procedures/year in the USA, at an aggregate cost of approximately 15 billion dollars1. The utilization of non-surgical remedies including injection therapies are also trending upwards according to CMS data, and represent more than one million lumbar epidural and transforaminal injections/year, costing over sixty-five million dollars2. Return to work may be accomplished in many cases by aggressive pain management strategies. This has been demonstrated in a military population exposed to interventional pain management procedures3. Recommendations have been published concerning the work-up and treatment of individuals with chronic spinal pain to enhance patient education and improve patient care in terms of shortening the course of the pain experience4-
6. The decision on selecting candidates for interventional pain management is typically made following a comprehensive history and physical examination and a demonstration of pathological findings of diagnostic imaging7 and electrodiagnostic studies8. Also, most interventions do not stand alone as pain relieving modalities but actually function as one part of a multifaceted treatment regimen9. Evidence from large meta-analyses suggests that spinal pain treatment where radicular pain is present reaches Level I for caudal epidural block; Level II-1 or II-2 for cervical or lumbar facet joint injections for facet joint mediated pain; Level II-1 for cervical interlaminar epidural injections for upper extremity radicular pain; and Level II-1 for lumbar transforaminal (TFESI) epidural injections for radicular pain of the lower extremities using the USPSTF criteria10. Rationale for Lumbar (LESI), Caudal Epidural and Transforaminal Steroid Injections (TFESI) (Figures 1, 2) Lumbar spinal pain may be localized (LBP), facet-joint mediated, emanate from the intervertebral discs, or it may be radicular, among other etiologies. Lumbar approaches to managing radicular pain typically involve interlaminar injections (Figure 1A-B), caudal injections (Figure 1C-D) or transforaminal injections (Figure 2). The disc has a rich innervation primarily in its outer third of the annulus with elements being contributed by the sinuvertebral nerve, gray rami communicantes, and lumbar ventral rami11-14. Nerves in discs contain calcitonen-gene-related peptide (CGRP), vasoactive intestinal peptide (VIP), Substance P, prostaglandins (Phospholipase A2)(PLA2), histamine, lactate and potassium, each of which is characteristic of nociception15-17. Even so, lavage of the epidural space in volunteers suffering with acute radicular pain did not reveal presence of the aforementioned mediators18. However, elevated serum hs-CRP may be an indicator in responsiveness to steroid epidural administration19. Steroids remain the most commonly injected chemicals for radicular pain and include Methylprednisolone acetate (MPA), Triamcinolone and Betamethasone20-25. Clearly, steroid epidural injections do not alter herniated disc (HNP) regression26. However, steroids may modify enzyme activity and may decrease inflammation by stabilizing leukocyte lysosomal membranes; preventing release of destructive acid hydrolases from leukocytes; inhibiting
227 Page 2
2
macrophage accumulation in inflamed areas; reduce leukocyte adhesion to the capillary endothelium; reducing capillary wall permeability and edema formation; decreasing complement components; antagonizing histamine activity and release of kinins; reducing fibroblast proliferation and collagen disposition; and possibly other mechanisms as well27. Alternatives to steroids for radicular pain management include epidural administration of TNF-alpha28-30, Indomethacin31, Autologous Conditioned Serum32, as well as intradiscal administration of steroids33, or hypertonic dextrose 50%34. Spine surgeons do not uniformly refer patients for injection therapy for radicular pain regardless of etiology of the pain35. More procedures are performed in the Southern USA than in the Northeast. Injection rates are positively correlated with lumbar surgery rates36. Lumbar, Caudal and Transforaminal Injections (ESI) for Managing Radicular Leg Pain (Figures 1, 2) Lumbar epidural injections may be accomplished using one of three basic approaches-interlaminar, caudal or transforaminal. Steroid injections may be a simple, cost-effective and minimally invasive treatment for sciatic type pain37. Early meta-analysis data suggested that convincing evidence was lacking for injection therapies in terms of managing low back or radicular pain38. Some studies suggested ESI were inferior to simple saline injection39. A newer meta-analysis suggested that evidence for TFESI use in radicular pain was strong; caudal ESI moderate, and LESI limited or inconclusive40. For degenerative disc disease (DDD) LESI were shown to be beneficial for pain and functional improvement41. For large HNP, surgical discectomy was shown to be superior to LESI for reducing symptoms42. Fluoroscopic guidance enhances delivery of steroid to the target of interest43. LESI seem more effective in the short-term, than for long-term benefit with evidence for short term use being strong for LESI, caudal ESI, and TFESI and moderate for TFESI in long-term pain management44-49. HNP location and grade of nerve root compression as assessed by pre-procedure MRI may determine clinical outcome following LESI50, although spinal canal dimension was found not to be predictive of success or failure of LESI in spinal stenosis51. In a joint clinical practice guideline from the American College of Physicians and American Pain Society, imaging studies were felt only necessary with severe or progressive neurologic deficits or if patients were deemed candidates for LESI52. A typically-quoted duration of action of LESI is 3-months53. LESI done intraoperatively during spinal surgery was shown not to affect outcome in terms of reducing radicular pain54 although they do appear to shorten the duration of hospital stay when performed in recent laminectomy patients55. While some would advocate performing a “series” of LESI for radicular pain, the evidence appears scant to support this practice routinely56, and in fact, the use of opioids may increase in those who receive 3 or more LESI57. When 3 LESI are performed, however, it appears that separating the injections by 10 day intervals provides superior pain relief to performing them every 24 hours58. There appears to be an unresolved conflict in the medical literature concerning the relative efficacy of LESI and other spinal pain treatments, with some authors noting insufficient evidence to support their use in general59,60 and others noting substantial benefit from some, but not all therapies61. Several review articles are available to discuss the relative merits of these treatments62,63.
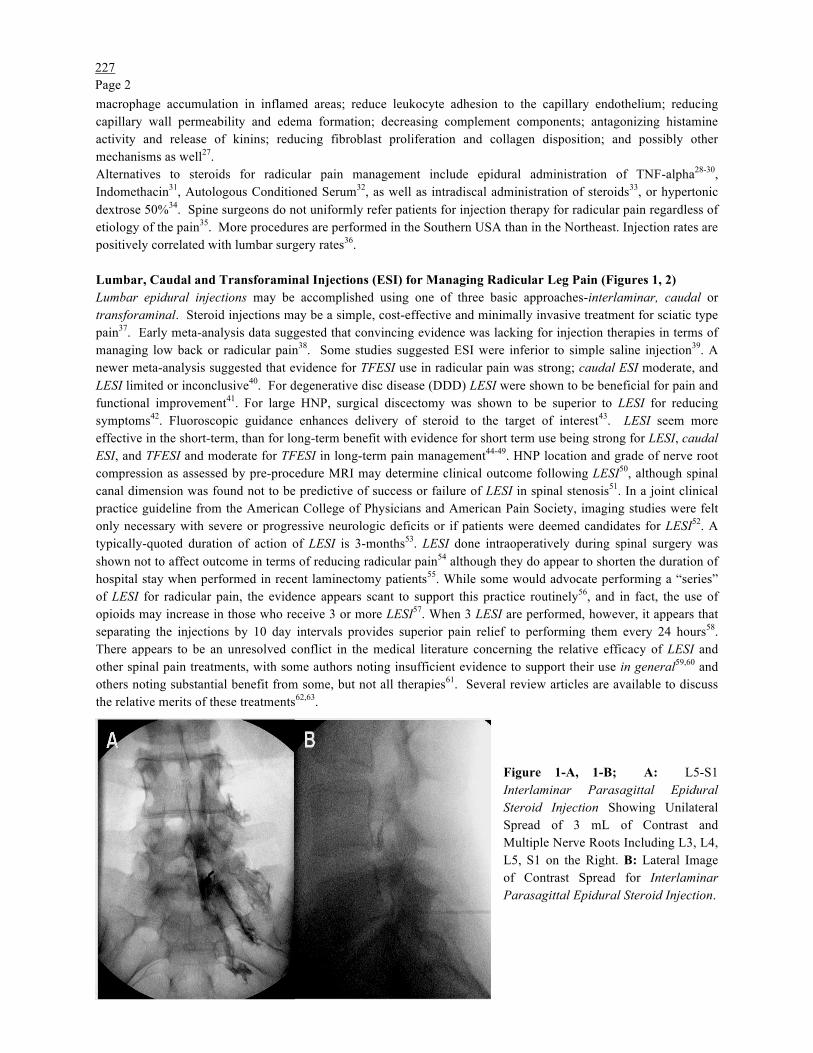
Figure 1-A, 1-B; A: L5-S1 Interlaminar Parasagittal Epidural Steroid Injection Showing Unilateral Spread of 3 mL of Contrast and Multiple Nerve Roots Including L3, L4, L5, S1 on the Right. B: Lateral Image of Contrast Spread for Interlaminar Parasagittal Epidural Steroid Injection.

227 Page 3
3
Caudal Approaches (Figures 1C-1D): The caudal application of local anesthetics for treating sciatic pain dates back to more than 100 years ago63. Steroids in volumes from between 10 mL to 64 mL have been injected through the sacral hiatus, with 10 mL being necessary to attain spread to the L5 segment and 15 mL necessary to reach L464. The caudal approach is certainly a viable alternative to TFESI when attempting to place medication at a target level in patients who have had previous spinal surgery, which obviates the possibility of interlaminar techniques due to the surgical scar. Studies show a reduction in pain, improved physical functioning, and lowering of opioid usage, persisting up to six months in almost 50% of patients receiving between one and three injections for radicular pain65. When compared to targeted steroid placement onto the affected nerve root using spinal endoscopy, caudal ESI using 11 mL volumes proved superior in terms of analgesia66. Caudal ESI is equally effective for HNP at L4-5 or L5-S167, and for bilateral radicular pain due to degenerative lumbar spinal stenosis68. Caudal injection with or without steroids (lidocaine 0.5%) appear effective for LBP (70%)69; radicular pain (up to 91% success for average of 35 weeks)70; failed-spine-surgery-syndrome (FBSS) (pain relief in up to 70% and functional status improvement in 55% of patients)71; lumbar spinal stenosis (SS) (60% success rates)72; with the evidence reaching Level I when caudal ESI is done for HNP or radicular pain and discogenic pain alone, and Level I or II-1 when used for FBSS with adhesiolysis61. Even water-for-injection (WFI) proved effective for treating LBP and sciatic pain following caudal administration73. Some have advocated adding hypertonic saline to local anesthetic and steroid for adhesiolysis in SS patients using a caudal technique. Results include pain relief in ¾ of patients for up to one year74. In a retrospective NASS telephone survey of 216 caudal recipients treated for SS, 87.5% improved with a series of injections75. Up to 50 mL of solution injected extends to mid-lumbar segments in a majority of subjects76.
Figure 1-C and 1-D; C: Caudal Epidural Steroid Injection With Bilateral S1, S2 and S3 Nerve Root Spread of 5 ML of Contrast Through A Catheter. D: Lateral Image of Contrast Spread for Caudal Epidural Steroid Injection.
Transforaminal Approaches (Figures 2-A, 2-B): Transforaminal techniques have become extremely popular over the past decade or so for treating unilateral radicular pain, while improving standing and walking tolerance in degenerative SS77. Prospective studies showed 84% success rates vs. 48% for trigger-point injections (TPI) in LBP with radiculopathy78. TFESI have shown efficacy for FBSS, SS, and L-S radiculopathy for up to one year or more79. While ventral epidural (88%) and nerve root filling (97%) may occur, intravascular injection may complicate the procedure80 which may be missed up to 57% of the time with static fluoroscopy techniques81. TFESI may reduce the requirement for spinal surgical disc decompression82, especially for sciatica symptoms < 6 months in duration83. With injected volumes ≥ 0.5 mL, there is no guarantee that TFESI are “selective” to a single specified nerve root level84. Volumes of ≥ 2 mL attain ventral epidural spread (i.e., “the target for nociception”) between 75-100% of the time85,86. However, interlaminar techniques have been described which are modifications of standard midline approaches that demonstrate attainment of ventral epidural spread in 100% of cases without the 10% incidence of intravascular injection reported for TFESI86,87. Unilateral epidural spread is attained using interlaminar techniques by

227 Page 4
4
placing the needles parasagittally instead of midline88-90. Interpretation of contrast dispersion may be affected by the experience of the observer, however91. In direct comparisons of efficacy of TFESI with interlaminar injections for treating L-S radicular symptoms, some studies have shown superior results from TFESI92,93, while others have shown no difference whatsoever when modifications were undertaken either to the LESI or TFESI component86,94. It is possible that bilateral TFESI may be more effective than single-injection LESI in terms of placing medication into the ventral epidural compartment, provided the LESI is undertaken as a midline, and not parasagittal technique95. A recent, but retrospective analysis suggested that both LESI and TFESI were superior in providing pain relief than caudal ESI for SS or HNP96, results which are in agreement with previous work93 but not with meta-analyses of these techniques61,97,98. Although TFESI may result in surgical sparing in some, selected patients98,99, plasma disc decompression may provide superior pain relief for contained HNP100.
Figure 2-A and 2-B; A: A-P and B: Lateral Images of Fluoroscopically-Guided Lumbar Transforaminal Steroid Injection. A Left-Sided Approach at the L4-L5 Level was undertaken. Three mL of Iodine-Based Water Soluble Contrast Outlines the Left L4 and L5 Nerve Roots and Extends into the Ventral Epidural Space.
Complications of Lumbar Epidural Techniques: Numerous complications from lumbar LESI, TFESI and caudal ESI have been reported and may be procedure-related, medication-related, or patient-related101. Glucocorticoids suppress insulin action and should be used cautiously in diabetics102, and betamethasone injection LESIs by various routes result in elevation in glucose levels in diabetics lasting approximately 2 days103. There is no relationship between cumulative MPA dose and bone mineral density in healthy adults104. A single dose of MPA epidurally can cause Cushing’s Syndrome105and steroid psychosis has been reported106. Rare ocular complications include chorioretinopathy107 and acute retinal necrosis108 and transient blindness109. Air injected during the LOR technique may cause gas embolism110 or pneumocephalus if the dura is entered111-5. Central effects include persistent hiccups116, bilateral 6th nerve palsy117, dysphonia118, and facial flushing119-121. Intradiscal injection occurs following both TFESI and LESI122-3 but occurs 12 times more commonly in the former case than the latter. Dural puncture and subdural injection occur following both LESI and TFESI, but are more common in the former than the latter124. More serious complications include infections including discitis and epidural abscess formation and meningitis125-33; intravascular injections from TFESI134-5; epidural and subdural hematoma formation136-140; cauda equina syndrome141; and paralysis and death, primarily from TFESI141-9. Cervical Transforaminal (CTFESI) and Interlaminar (CESI) Injection (Figures 3-A, 3-B; 4-A, 4-B): Treatment of radicular cervical spinal pain may be accomplished using CTFESI or CESI. The strength of evidence using the USPSTF criteria favoring CESI is II-161, with success rates up to 77%150. Fluoroscopy improves accuracy of needle placement for interlaminar CESI while ventral epidural spread is noted in between 28%-93% of midline CESI151-2. Depth from skin to the cervical epidural space is > in males and at C6-7averages 5.1 ± 0.6 cm; in females it is 4.6 ± 0.6 cm153 with mean width of epidural space of 3 mm (1-4 mm)154. Some fat (1-2 mm) may be found at C7-T1 but not above that level155. At C6-7, 4-6 mL injected will spread up to C-2156. The ligamentum flavum may not fuse midline so a lateral fluoroscopic view is important to obtain157. Performing CESI using minimal to no

227 Page 5
5
sedation may limit subsequent complication development, particularly since cord penetration may be somewhat painless155, 158-60. Injection should be undertaken slowly since rapid injection into constricted areas may lead to neurological complications161 although injection for SS seems to lead to improved outcomes162 and contrast may spread 3.61 ± 0.84 levels 163. It is likely that neurological problems following CESI occur only after MPA use and the hanging drop technique164-7. Vascular uptake may occur during CESI interlaminar injections168-9. While some suggest that the incidence of complications following CESI (0.52%-16.8%) is not different than from CTFESI170, this, as well as the severity of complications after each, is in dispute171. Minor complications include syncope, headache and facial flushing172-3. Other complications include granuloma formation174; subdural injection175; pneumocephalus176; epidural and subdural hematoma177-9; epidural abscess180-1; paralysis182; and stroke183. In summary, it appears that CESI do help resolve pain and provide short-term benefits in a majority of patients with HNP184-6. CTFESI have also been used to treat radicular arm pain. When fluoroscopy is used, intravascular (venous or arterial) injection occurs 63.4% of the time187, representing a > three-fold higher incidence than previously reported188. Digital Subtraction Angiography (DSA) may detect twice as many intravascular injections189. Observational studies suggest that up to 30% of patients receiving CTFESI obtain complete pain relief (CPR) while 30% obtain partial, but lasting relief190. Dural puncture rates are equivalent to interlaminar CESI191. Some studies show relatively low rates of minor and transient complications from CTFESI, ocurring especially with anterior needle placement170,192-3, while cadaveric dissection reveals ascending and deep cervical arterial branches entering the posterior foramen, the classic target site194-6. It appears CTFESI may be more dangerous than previously reported197 and indeed, there have been cases of temporary198 as well as permanent neurological sequelae199-203 and
death204 during particulate steroid203,205 administration. Figure 3-A and 3-B; Cervical Transforaminal Injection: A-P View and Lateral Views. A: Right-Sided Approach at C5-C6 in a Patient With Previous History of Anterior Spinal Discectomy and Fusion Surgery Demonstrates Contrast Spread Along the Right C-6 Nerve Root. Lighter Shading Represents a Previously Performed Right-Sided C-5 Nerve Root Injection Cephalad to the Level Represented in these Images. B: Lateral Oblique View of Right
C-6 Nerve Root Spread. Figure 4-A and 4-B: Cervical Interlaminar Epidural Injection at C6-C7: A-P and Lateral Views. On A-P Imaging the Needle is Seen Entering the Interlaminar Space in the Midline as Defined by the Dorsal Spinous Processes. On Lateral View, The Spread of 3 mL of Contrast Extends Along the Dorsal Epidural Space for Multiple Levels to C3-C4.

227 Page 6
6
Facet Joint Pain: Role of Cervical Medial Branch Blocks (Figures 5A-5B). The strength of evidence using the USPSTF criteria with 5 levels of evidence (range Level I to III with 3 subcategories in Level II) for accuracy of diagnostic facet joint nerve blocks (MBB) is Level I or II-1 in the diagnosis of lumbar (LMBB) and cervical facet joint pain (CMBB) and is Level II-1 or II-2 for therapeutic cervical and lumbar facet joint nerve blocks61. The rationale for performing these blocks is that pain generators include free and encapsulated nerve endings with nerves containing Substance P and CGRP. The facet joint capsule contains low threshold mechanoreceptors, mechanically sensitive nociceptors and silent nociceptors206. Neck pain following trauma is due to facet joint pain in about 20% of patients207-8. Pain is referred and may be mapped out with the C3-4 and C5-6 levels most commonly affected209,210. False positive rates following single-diagnostic blocks may be 45%211. Early meta-analysis suggested that radiofrequency ablation (RFA) of the medial branches was limited for both cervical and lumbar spinal pain212, but was later found to be moderate (Level III)213. Complications occur with greater frequency if fluoroscopy is not used for CMBB214, as even with fluoro guidance, intravascular injection occurs in up to 4%215. Smaller volume blocks using 0.25 mL of LA may improve precision and accuracy216. Steroids added to local anesthetic do not provide superior pain relief to LA alone217 and intraarticular injections are not indicated in the C-Spine218. RFA of CMB may provide 38 weeks of analgesia using continuous energy techniques219-220, and up to 60 weeks when only successes are considered221-2. When RF of the third occipital nerve (TON) is performed for cervicogenic HA, results may last 10 months, while ataxia, numbness and dysesthesias may develop223; for RF of the DRG of C4, C5, C6, duration of analgesia (DOA) may be 6 weeks224. Pulsed RF techniques may provide analgesia by augmenting C-fos225 and MIB-1 activity226.
Figure 5-A and 5-B: Cervical Medial Branch Blocks: Lateral and A-P Views Of Three Needles Placed on the Left Side at C3, C4 and C5 Levels, for Block of the C3-C4 and C4-C5 Facet Joint Innervation. Needles sit on the Trapezoid, Center of the Articular Pillars. Figure 6-A and 6-B: A-P and Lateral Views of Lumbar Medial Branch Blocks: A-P and Lateral Views of Four Needles Placed on the Left at L3, L4, L5 and the Sacral Ala.
227 Page 7
7
Lumbar Medial Branch Techniques (Figures 6A-6B): Lumbar facet joint pain (zygapophyseal or “Z” joint) affects up to 15% of patients with axial LBP227. Literature supporting the use of diagnostic lumbar facet and MB nerve blocks is controversial. Some meta-analyses purport that there is strong evidence in support of diagnostic Lumbar MBB in terms of accuracy of diagnosing facet joint pain48,213,228-230 and determining candidacy for RF procedures231, regardless of how stringent analgesia criteria were between >50% and ≥ 80% pain relief. Others are equally compelling in their determinations that FJ blocks (not MB nerve) are not supported by the preponderance of literature232. Some have advocated pre-procedural CT scan (SPECT) as a diagnostic measure to determine suitability for FJB or MBB233. With careful patient selection, RF of the lumbar MB may provide effective analgesia lasting many months234-241. Cryolesioning offers alternatives to RFA in selected patients, as well242. Sacroiliac Joint Injections (Figures 7A-7B): As a true synovial joint, the sacroiliac joint (SIJ) is a pain-sensitive structure richly innervated by a combination of unmyelinated free nerve endings and the posterior primary rami of L2-S3. Several muscles have their insertion into the SIJ and include the piriformis; biceps femoris; gluteus maximus and minimus; erector spinae; latissimus dorsi; thoracolumbar fascia; and the iliacus, and any of these may be involved in SIJ related pain. Still, the diagnosis of SIJ pain is difficult to make unequivocally243. Intraarticular SIJ injections underestimate the prevalence of SIJ pain due to the influence of extraarticular sources244. Furthermore, single-site, single-depth sacral lateral branch injections are not consistent in providing analgesia of the SIJ245, while multi-site, multi-depth injections are effective in up to 70%246. Double diagnostic SIJ blocks may reduce the false-positive rate of single diagnostic blocks from 20%, but even so, the evidence for short-term and long-term relief from SIJ injections and RF procedures is limited247,248. Recently, SIJ injections have been noted to be effective in cases of spondyloarthropathy249. L4-5 dorsal rami and S1-3 lateral branch, water-cooled RF may be provide superior analgesia vs. placebo250.
Figure 7-A and 7-B: Sacroiliac Joint Injection: Before and After 3 mL of Contrast Administration, Right-Sided; Oblique Fluoroscopy Angle.
References
1) Pain Physician 12:35-70, 2009. 2) Radiology 225:723-9, 2002. 3) Anesthesiology 107:1003-8, 2007. 4) Spine J 10:514-29, 2010. 5) Joint Bone Spine 74:530-5, 2007. 6) Spine 34:1078-93, 2009. 7) Clin J Pain 23:571-5, 2007. 8) J Pain 9:64-70, 2008. 9) Spine 34:985-9, 2009. 10) Pain Physician 12:123-98, 2009. 11) J Anat 132:39-56, 1981. 12) J Pathol 132:95-104, 1980. 13) Am J Anat 188:282-96, 1990. 14) Acta Anat 38:96-113, 1959. 15) Spine 15:383-6, 1990. 16) Spine 10:156-7, 1985. 17) Spine 13:1344-8, 1988. 18) J Spinal Disord Tech 19:266-9, 2006. 19) J Ky Med Assoc 104:295-9, 2006. 20) Pain Pract 3:222-5, 2003. 21) Spine J 4:468-74, 2004. 22) Pain Med 9:227-34, 2008. 23) Singapore Med J 48:241-5, 2007. 24) Anesthesiology 106:331-8, 2007. 25) Skeletal Radiol 38:1077-82, 2009. 26) J Spinal Disord Tech 15:469-76, 2002. 27) Pain Physician 5:182-199, 2002. 28) Swiss Med Wkly 133:170-77, 2003. 29) Curr Med Res Opin 20:1075-85, 2004. 30) Anaesth Intensive Care 35:301-2, 2007. 31) Anesth Analg 96: 463-8, 2003. 32) Spine 32:1803-8, 2007. 33) Spine 29:833-6, 2004. 34) Pain Physician
227 Page 8
8
9:115-121, 2006. 35) PM R 1:329-34, 2009. 36) J Bone Joint Surg Am 90:1730-7, 2008. 37) J Orthop Surg 8:39-44, 2000. 38) Cochrane Database Syst Rev CD001824, 2000. 39) Ann Rheum Dis 62:639-43, 2003. 40) Pain Physician 6:319-34, 2003. 41) Spine J 4:495-505, 2004. 42) J Bone Joint Surg Am 86-A:670-9, 2004. 43) Spine J 5:191-201, 2005. 44) J Bone Joint Surg Br 87:352-5, 2005. 45) Rheumatology 44:1399-1406, 2005. 46) Health Technol Assess 9:1-58, 2005. 47) Pain Physician 8:127-143, 2005. 48) Pain Physician 10:7-111, 2007. 49) Pain Physician 10:185-212, 2007. 50) Korean J Radiol 8:156-63, 2007. 51) J Spinal Disord Tech 20:168-71, 2007. 52) Ann Intern Med 147:478-91, 2007. 53) Neurology 68:723-9, 2007. 54) Ann Saudi Med 27:279-83, 2007. 55) Spine 33:2028-33, 2008. 56) Arch Phys Med Rehabil 89:543-52, 2008. 57) Arch Phys Med Rehabil 89:1011-5, 2008. 58) The Open Orthopaedics Journal 3:121-4, 2009. 59) Cochrane Database Syst Rev CD001824, 2008. 60) Spine 34:49-59, 2009. 61) Pain Physician 12:699-802, 2009. 62) Spine J 8:45-55, 2008. 63) Br J Anaesth 99:461-73, 2007. 64) Pain Physician 5:133-48, 2002. 65) Pain Physician 5:18-29, 2002. 66) Br J Anaesth 94:514-9, 2005. 67) J Spinal Disord Tech 20:49-52, 2007. 68) Pain Physician 10:547-58, 2007. 69) Pain Physician 11:785-800, 2008. 70) Pain Physician 11:801-15, 2008. 71) Pain Physician 11:817-31, 2008. 72) Pain Physician 11:833-48, 2008. 73) Spine 15:1441-7, 2009. 74) Pain Physician 12:341-54, 2009. 75) Skeletal Radiol 39:691-9, 2009. 76) J Korean Med Sci 16: 193-7, 2001. 77) Am J Phys Med Rehab 81:898-905, 2002. 78) Spine 27:11-6, 2002. 79) Pain Physician 5:266-70, 2002. 80) Pain Physician 7:217-23, 2004. 81) Spine 33:205-10, 2008. 82) Chang Gung Med J 29:93-9, 2006. 83) AJR 187:1427-31, 2006. 84) Pain Physician 11:855-61, 2008. 85) Pain Physician 7:211-215, 2004. 86) Anesth Analg 106:638-44, 2008. 87) Pain Pract 9:275-81, 2009. 88) Arch Phys Med Rehabil 89:413-6, 2008. 89) Radiology 243:804-11, 2007. 90) Pain Physician 9:361-6, 2006. 91) PM R 1:55-9, 2009. 92) Pain Physician 9:361-6, 2006. 93) Anesth Analg 104:1217-22, 2007. 94) AJNR 28:204-8, 2006. 95) Clin J Pain 25:206-10, 2009. 96) J Back Musculoskelet Rehabil 22:83-9, 2009. 97) Pain Physician 12:233-51, 2009. 98) PM R 1:657-8, 2009. 99) J Am Acad Orthop Surg 15:228-38, 2007. 100) J Neurosurg Spine 12:357-71, 2010. 101) Anesthesiology 100:98-105, 2004. 102) Rheumatology 41:68-71, 2002. 103) PM R 1:340-5, 2009. 104) Clin Rheumatol 22:12-7, 2003. 105) Endocr Pract 11:408-10, 2005. 106) Pain Physician 11:917-20, 2008. 107) Am J Ophthalmol 132:423-5, 2001. 108) Am J Ophthalmol 136:192-4, 2003. 109) Spine 27:476-7, 2002. 110) Ann Emerg Med 38:592-5, 2001. 111) Headache 45:247-8, 2005. 112) Pain Physician 8:239-41, 2005. 113) Emerg Med J 25:416, 2008. 114) Clin Neurol Neurosurg 111:309-10, 2009. 115) J Neurosurg Spine 5:359-61, 2006. 116) Anesth Analg 100:1834-6, 2005. 117) Can J Anaesth 51:821-3, 2004. 118) Arch Phys Med Rehabil 83:1309-10, 2002. 119) Arch Phys Med Rehabil 81:1045-50, 2000.120) Pain Physician 7:427-9, 2004. 121) Am J Phys Med Rehabil 80:416-24, 2001. 122) Pain Med 9:688-94, 2008. 123) Anesth Analg 110:1464-7, 2010. 124) Pain Physician 10:697-705, 2007. 125) Zentralbl Neurochir 61:111-4, 2000. 126) South Med J 95:772-4, 2002. 127) Spine 28:209-11, 2003. 128) AJNR Am J Neuroradiol 25:642-4, 2004. 129) Mayo Clin Proc 79:682-6, 2004. 130) Pain Physician 7:269-72, 2004. 131) Pain 116:407-110, 2005. 132) Acta Radiol 48:687-9, 2007. 133) Pain Physician 11:693-7, 2008. 134) Spine 25:2628-32, 2000. 135) Spine J 7:79-82, 2007. 136) Anesthesiology 95:1307, 2001. 137) Anesth Analg 95:1691-7, 2002. 138) Anesthesiology 102:701-3, 2005. 139) J Manipulative Physiol Ther 30:536-8, 2007. 140) Spine 34:376-9, 2009. 141) J Manipulative Physiol Ther 29:492, 2006. 142) Anesth Analg 101:1209-11, 2005. 143) RAPM 29:494-5, 2004. 144) Ann Readapt Med Phys 49:242-7, 2006. 145) AJNR Am J Neuroradiol 30:1691-3, 2009. 146) Pain Med 10:1389-94, 2009. 147) Pain Physician 8:309-14, 2005. 148) Eur Radiol 20:181-9, 2010. 149) Pain Physician 13:237-44, 2010. 150) Pain Physician 13:223-36, 2010. 151) Spine 27:509-14, 2002. 152) Anesth Analg 108:1658-61, 2009. 153) RAPM 28:95-7, 2003. 154) J Clin Anesthesia 10:309-13, 1998. 155) Spine 23:2137-42, 1998. 156) Spine 31:1576-9, 2006. 157) Anesthesiology 99:1387-90, 2003. 158) Anaesthesia 55:194, 2000. 159) APSF Newsletter 20:45-60, 2005. 160) RAPM 33:404-15, 2008. 161) Spine J 5:558-63, 2005. 162) Am J Phys Med Rehabil 88:239-46, 2009. 163) Spine 31:1576-9, 2006. 164) Pain Clinic 1:3-7, 1986. 165) Anesthesiology 93:885-8, 2000. 166) Anesthesiology 86:1394-6, 1997. 167) Spine J 5:558-63, 2005. 168) Pain Physician 9:267-72, 2006. 169) Arch Phys Med Rehabil 89:553-8, 2008. 170) Pain Physician 7:445-9, 2004. 171) Spine 32:2144-51, 2007. 172) Arch Phys Med Rehabil 84:627-33, 2003. 173) Pain Pract 9:59-64, 2009. 174) Anesthesiology 100:445-7, 2004. 175) Anaesth Intensive Care 31:570-2, 2003. 176) Anesth Analg 92:1576-7, 2001. 177) J Neurosurg Anesthesiol 13:323-8, 2001. 178) Surg Neurol 57:235-40, 2002. 179) Spine 15:174-6, 2002. 180) J Otolaryngol 34:254-7, 2005. 181) Spine 29:7-9, 2004. 182) Spine J 5:558-63, 2005. 183) Arch Neurol 63:1643-6, 2006. 184) Spine 33:S153-69, 2008. 185) Skeletal Radiol 36:431-6, 2007. 186) J Vasc Interv Radiol 18:1151-5, 2007. 187) Anesth Analg 109:233-9, 2009. 188) Spine 28:21-5, 2003. 189) PM R 1:636-42, 2009. 190) Anesthesiology 100:1595-1600, 2004. 191) Curr Rev Musculoskelet Med 2:30-42, 2009. 192) JBJS 87-A:1025-30, 2005. 193) Arch Phys Med Rehabil 86:277-83, 2005. 194) Spine 34:731-9, 2009. 195) Pain 117:104-11, 2005. 196) RAPM 31:270-4, 2006. 197) Spine 32:1249-56, 2007. 198) Pain Med 5:202-5, 2004. 199) RAPM 31:282-5, 2006. 200) Spine 30:266-8, 2005. 201) J Spinal Cord Med 30:385-8, 2007. 202) RAPM 33:377-9, 2008. 203) Spine J 4:468-74, 2004. 204) Am J Forensic Med Pathol 24:351-5, 2003. 205) Pain Med 9:227-34, 2008. 206) J Bone Joint Surg Am 88:63-7, 2006. 207) Pain 54:213-7, 1993. 208) J Am Acad Orthop Surg 15:596-606,2007. 209) Pain Medicine 8:344-53, 2007. 210) Med J Aust 19:174-6, 2001. 211) J Spinal Disord Tech 20:539-45, 2007. 212) RAPM 26:394-400, 2001. 213) Pain Physician 10:229-53, 2007. 214) Clin Neurol Neurosurg 108:709-11, 2006. 215) Spine 33:174-7,

227 Page 9
9
2008. 216) Anesthesiology 112:144052, 2010. 217) Pain Physician 9:333-46, 2006. 218) Pain Pract 10:112-23, 2010. 219) NEJM 335:1721-6, 1996. 220) Pain 6:282-6, 2005. 221) Neurosurg 45:61-8, 1999. 222) Pain Physician 12:323-44, 2009. 223) J Neurol Neurosurg Psych 74:88-93, 2003. 224) Pain 52:49-53, 1993. 225) Neurosurg 50:850-6, 2002. 226) Eur J Pain 5:169-74, 2001. 227) Anesthesiology 106:591-614, 2007. 228) Pain Physician 110:213-28, 2007. 229) Pain Physician 11:121-32, 2008. 230) Pain Physician 12:71-121, 2009. 231) Spine J 8:498-504, 2008. 232) Spine 34:1078-93, 2009. 233) South Med J 101:931-4, 2008. 234) Arch Phys Med Rehabil 90:201-5, 2009. 235) J Spinal Disord Tech Jan 2010 (ahead of print). 236) Appl Neurophysiol 39:80-6, 1977. 237) Appl Neurophysiol 39:87-96, 1977. 238) Pain 57:7-83, 1994. 239) Stereotact Funct Neurosurg 68:212-7, 1997. 240) Spine 24:1937-42, 1999. 241) Spine 26:1411-7, 2001. 242) Int Orthopaedics 31:525-30, 2007. 243) Eur Spine J 16:1539-50, 2007. 244) Arch Phys Med Rehabil 89:2048-56, 2008. 245) Pain Med 9:844-50, 2008. 246) Pain Med 10:679-88, 2009. 247) Pain Physician 12:399-418, 2009. 248) Skeletal Radiol 39:5-9, 2010. 249) Spine J 9:690-703, 2009. 250) Anesthesiology 109:279-88, 2008.