kearns–sayre syndrome, abnormal corneal endothelium and normal tension glaucoma
TRANSCRIPT

Letters to the Editor
Visual recovery of the amblyopic eye in an adult patient
after loss of the dominant eye
Kai Kaarniranta and Matti Kontkanen
North Karelia Central Hospital, Joensuu, Finland
Sir,
T reatment of amblyopia is thoughtto be most effective during early
childhood, while treatment benefitdeclines with increasing age (Epelbaumet al. 1993). However, in some circum-stances, permanent visual improvementof anamblyopic eyehasbeendocumentedeven during adulthood (Wick et al. 1992;El Mallah et al. 2000; Jakobsson et al.2002; Rahi et al. 2002a, 2002b).
We report a case of full visual improve-ment from 0.3 to 1.0 in an amblyopic eyeafter enucleation of the leading eye.
In 1985, a 19-year-old man wasinvolved in a car accident that causedbrain contusion and bulbus rupture ofhis leading eye. The dominant right eyewas enucleated 1 day after the trauma.The surgeon performing the enuclea-tion was unaware that the non-dominant left eye was amblyopic dueto hypermetropic anisometropia. Occlu-sion treatment during early childhoodhad not improved the subject’s bestcorrected visual acuity (VA) in theamblyopic eye, which was still only 0.3in 1985. Both eyes were hypermetropic,with the right eye being þ2.25 (VA 1.0)and the left þ6.0 (VA 0.3) before theaccident. Despite the hyperopia, thesubject did not wear spectacles. Thepatient’s sister also suffered from an-isometropic amblyopia.
Two months after the right eye wasenucleated, VA in the left eye wasimproved by two lines; after 1 year VAwas almost normal and after 2 years it
had achieved a normal level (Table 1).At the age of 36 years, after 17 years offollow-up, the patient did not acceptfull hyperopic correction (Table 1).
This case shows that VA in an adultin an eye with anisometropic amblyopiais able to recover to normal spontan-eously after the loss of the dominanteye. In this particular case, attemptshad been made to treat the amblyopiaduring childhood, but with little suc-cess. Many amblyopic children do notshow any improvement in VA becauseof poor parental co-operation (Campos1995); this was probably the reason forfailure in this case.
The present accommodative ampli-tude might be explained by a develop-mental change due to the hyperopicanisometropia, rather than as congeni-tal sequelae (Milder & Rubin 2000).The patient had accommodated con-tinuously as a child and he had thusdeveloped excessive accommodativeamplitude, particularly as he had notworn spectacles before the accident.On the other hand, his excessive accom-modative amplitude may be a normalvariant. Accommodative capacity var-ies widely, although the amplitude ofaccommodation decreases with passingyears (Milder & Rubin 2000).
In conclusion, the loss of an eye is adramatic experience for a patient; evenmore difficult to accept is enucleationof the better eye. In contrast to mostearlier findings, which show poor prog-
noses in the treatment of amblyopiaafter 7 years of age, we report that fullvisual recovery of an amblyopic eye cantake place in an adult patient after theloss of the leading eye when centralfoveal fixation is present.
ReferencesCampos E (1995): Amblyopia. Surv Ophthal-
mol 40: 23–39.
El Mallah MK, Chakravarthy U & Hart PM
(2000): Amblyopia: is visual loss permanent?
Br J Ophthalmol 84: 952–956.
Epelbaum M, Milleret C, Buisseret P &
Dufier JL (1993): The sensitive period for
strabismic amblyopia in humans. Ophthal-
mology 100: 613–614.
Jakobsson P, Kvarnstrom G, AbrahamssonM,
Bjernbrink-Hornblad E & Sunnqvist B
(2002): The frequency of amblyopia among
visually impaired persons. Acta Ophthalmol
Scand 80: 44–46.
Milder B & Rubin ML (2000): In: Milder B &
Rubin ML (eds). The Fine Art Prescribing
Glasses. 2nd edn. Gainesville: Triad Publishing
Co. 10�55, 217–253.
Rahi JS, Logan S, Borja MC, Timms C,
Russell-Eggitt I & Taylor D (2002a): Predic-
tion of improved vision in the amblyopic eye
after visual loss in the non-amblyopic eye.
Lancet 360: 621–622.
Rahi JS, Logan S, Timms C, Russell-Eggitt I &
Taylor D (2002b): Risk, causes and out-
comes of visual impairment after loss of
vision in the non-amblyopic eye: a popula-
tion-based study. Lancet 360: 597–602.
Wick B, Wingard M, Cotter S & Scheiman M
(1992): Anisometric amblyopia: is the patient
ever tooold to treat?OptomVisSci69: 866–878.
Correspondence:
Matti Kontkanen MD, PhD
Department of Ophthalmology
North Karelia Central Hospital
Tikkamaentie 16
80210 Joensuu
Finland
Tel:þ358 13 17 12 067
Fax:þ 358 13 17 13 515
Email: [email protected]
Table 1. Remodelling of visual acuity. Best corrected visual acuity.
Month/Year BCVA Subjective refraction Cycloplegic refraction
1978 0.3 – þ 6.0
6/85 0.4 þ 2.0 cylþ 1.0 ax 135 þ 5.5 cylþ 0.75 ax 125
8/85 0.5 þ 2.25 cylþ 1.0 ax 150 –
6/86 0.8 þ 2.25 cylþ 0.75 ax 130 –
8/87 1.0 þ 2.25 cylþ 0.75 ax 130 –
7/02 1.0 þ 2.25 cylþ 1.25 ax 85 þ 4.75 cylþ 1.25 ax 85
ACTA OPHTHALMOLOGICA SCANDINAVICA 2003
539

Neovascular glaucoma treated by intravitreal
triamcinolone acetonide
Jost B. Jonas, Ingrid Kreissig and Robert F. Degenring
Department of Ophthalmology and Eye Hospital, Faculty for Clinical Medicine
Mannheim, Ruprecht-Karls-University, Heidelberg, Germany
Sir,
T riamcinolone acetonide injectedintravitreally has recently been
used in pilot studies for treatment ofvarious oedematous, inflammatory orneovascular diseases of the eye, suchas diffuse diabetic macular oedema,exudative age-related macular degen-eration, persistent pseudophakiccystoid macular oedema, macularoedema due to retinal central or branchvein occlusion, and uveitic cystoidmacular oedema (Machemer et al.1979; Gillies et al. 2003). These clinicalstudies were based on clinical andexperimental investigations in whichthe intraocular tolerability of triamci-nolone acetonide had been examined,and in which an angiostatic effect oftriamcinolone acetonide had beenshown (Antoszyk et al. 1993; Tanoet al. 1980; Penfold et al. 1995; Daniset al. 1996). As neovascular glaucoma iscaused by pathological neovasculariza-tion, it was therefore the purpose of thepresent study to evaluate whether intra-vitreal triamcinolone acetonide mightbe helpful in the treatment of neovas-cular glaucoma.
Our clinical, interventional, caseseries study included five eyes of fivepatients who received an intravitrealinjection of 25mg of triamcinoloneacetonide for treatment of neovas-cular glaucoma. No additional retinaldestructive procedure was carriedout. The five patients included in thepresent study represent a groupof patients other than those on whomwe have already reported (Jonas et al.2001). Their mean age was68.1� 6.2 years. Mean refractive errorwas �0.42� 0.72 dioptres. All patientswere fully informed about the experi-mental nature of the treatment and allsigned informed consent documents.The Ethics Committee of the universityapproved the procedure and it was per-formed in accordance with the ethicalstandards laid down in the 1964
Declaration of Helsinki. All patientsshowed neovascular glaucoma, eitherwith neovascularization of the iris sec-ondary to proliferative diabetic retino-pathy (three patients) or with ischaemiccentral retinal vein occlusion (twopatients). Upon gonioscopy, the anter-ior chamber angle was found to bepartially or completely covered withneovascular tissue. Mean visual acuity(VA) was 0.05� 0.05. Mean intraocularpressure (IOP) was 31.8� 12.7mmHg.The extent of iris neovascularizationwas graded using a scale ranging from0�4, where 0¼ no rubeotic iris vesselsand 4¼maximal iris neovasculariza-tion (Bandello et al. 1993). The meangrade of iris neovascularization was2.5� 1.0. Mean follow-up time was7.3� 2.1months (mean�SD; median7.0months; range 5.2–10.7months). Intwo patients, the intravitreal injectionwas combined with phacoemulsifica-tion and posterior chamber lensimplantation. The intravitreal injectionwas carried in a standardized manneras has been described in detail pre-viously (Jonas et al. 2001).
Intraocular pressure was signifi-cantly (p¼0.003) reduced from31.8� 12.7mmHg preoperatively to24.4� 9.6mmHg postoperatively. Bestpostoperative VA (0.11� 0.16) wasslightly, but not statistically signifi-cantly, better than preoperative values(0.05� 0.05). The degree of rubeosisiridis decreased significantly (p ¼0.02)from 2.5� 1.0 relative units to 0.8� 1.5relative units. All patients demon-strated a regression of iris neovascular-ization.
In an attempt to reduce retinalischaemia and the production of vaso-proliferative factors, neovascular glau-coma has usually been treated byretinal ablative procedures such as pan-retinal argon laser coagulation andanterior retinal exocryocoagulation(Sivak-Callcott et al. 2001). The retinal
destructive procedures were often com-bined with antiglaucomatous interven-tions such as cryocoagulation of theciliary body or implantation of glau-coma drainage systems. In an effort toreduce the angiogenetic influence of anischaemic retina on the formation ofnew vessels on the iris and in the anter-ior chamber angle, we injected triam-cinolone acetonide intravitreally in thepatients in the present study. Previousexperimental investigations as well asclinical pilot studies have suggestedthat intraocular triamcinolone aceto-nide has an anti-angiogenic effect(Tano et al. 1980; Antoszyk et al.1993; Penfold et al. 1995; Danis et al.1996; Jonas et al. 2001). The postopera-tive decrease in iris neovascularizationand the reduction in IOP may implythat the intravitreal injection of triam-cinolone acetonide had an anti-angio-genic effect, thereby explaining thedecrease in iris neovascularization.There are, however, limitations to thepresent study. One of them concernsthe fact that two (40%) patients add-itionally underwent phacoemulsifica-tion with posterior chamber lensimplantation, which as a procedure byitself usually leads to an increase in irisneovascularization in patients withischaemic proliferative retinopathiesand might have worsened the post-operative situation for patients in thestudy group. It may serve, therefore,to support the conclusion drawn fromthe results of the present case seriesstudy, which suggest that intravitrealtriamcinolone acetonide appears tohave an anti-angiogenic effect andmay represent an additional resourcefor treatment of neovascular glaucoma.
ReferencesAntoszyk AN, Gottlieb JL, Machemer R &
Hatchell DL (1993): The effects of intravi-
treal triamcinolone acetonide on experi-
ACTA OPHTHALMOLOGICA SCANDINAVICA 2003
540
mental pre-retinal neovascularization.
Graefes Arch Clin Exp Ophthalmol 231:
34–40.
Bandello F, Brancato R, Lattanzio R,
Falcomata B & Malegori A (1993): Bio-
microscopy versus fluorescein angiography
of the iris in the detection of diabetic irido-
pathy. Graefes Arch Clin Exp Ophthalmol
231: 444–448.
Danis RP, Bingaman DP, Yang Y & Ladd B
(1996): Inhibition of preretinal and optic
nerve head neovascularization in pigs by
intravitreal triamcinolone acetonide.
Ophthalmology 103: 2099–2104.
Gillies MC, Simpson JM, Luo W, Penfold P,
Hunyor AB, Chua W, Mitchell P & Billson
F (2003): A randomized clinical trial of a
single dose of intravitreal triamcinolone
acetonide for neovascular age-related
macular degeneration: 1-year results. Arch
Ophthalmol 121: 667–673.
Jonas JB, Hayler JK, Sofker A & Panda-Jonas
S (2001): Regression of neovascular iris ves-
sels by intravitreal injection of crystalline
cortisone. J Glaucoma 10: 284–287.
Machemer R, Sugita G & Tano Y (1979):
Treatment of intraocular proliferations with
intravitreal steroids. Trans Am Ophthalmol
Soc 77: 171–180.
Sivak-Callcott JA, O’Day DM, Gass JDM &
Tsai JC (2001): Evidence-based recommen-
dations for the diagnosis and treatment of
neovascular glaucoma. Ophthalmology 108:
1767–1776.
Tano Y, Sugita G, Abrams G & Machemer R
(1980): Inhibition of intraocular prolifera-
tion with intravitreal corticosteroid. Am J
Ophthalmol 89: 131–136.
Correspondence:
Dr J. Jonas
Universitats-Augenklinik
Theodor-Kutzer-Ufer 1–3
68167 Mannheim
Germany
Tel:þ 49 621 383 2242
Fax:þ 49 621 383 3803
Email: [email protected] heidelberg.de
Nummular infiltrates in Acanthamoeba keratitis
Thomas Reinhard,1 Gisbert Schilgen,2 Michael Steinert,3 Jorg Hacker3 and Rainer
Sundmacher2
1Eye Hospital, Albert-Ludwig University, Freiburg, Germany2Eye Hospital, Heinrich-Heine University, Dusseldorf, Germany3Institute for Molecular Biology of Infectious Diseases, University Wurzburg,
Wurzburg, Germany
Sir,
R adial keratoneuritis (Mooreet al. 1986) and ring-shaped
infiltrates (Illingworth & Cook 1998)are regarded as typical clinical featuresin Acanthamoeba keratitis. Epithelialirregularities (Cohen et al. 1987; Baconet al. 1993) and stromal infiltrates(Illingworth & Cook 1998) are common,but less typical. Dense subepithelial infil-trates were described by Holland et al.(1991). Here, we present a patient with
Acanthamoeba keratitis showing sub-epithelial infiltrates similar to nummularinfiltrates in adenoviral keratitis.
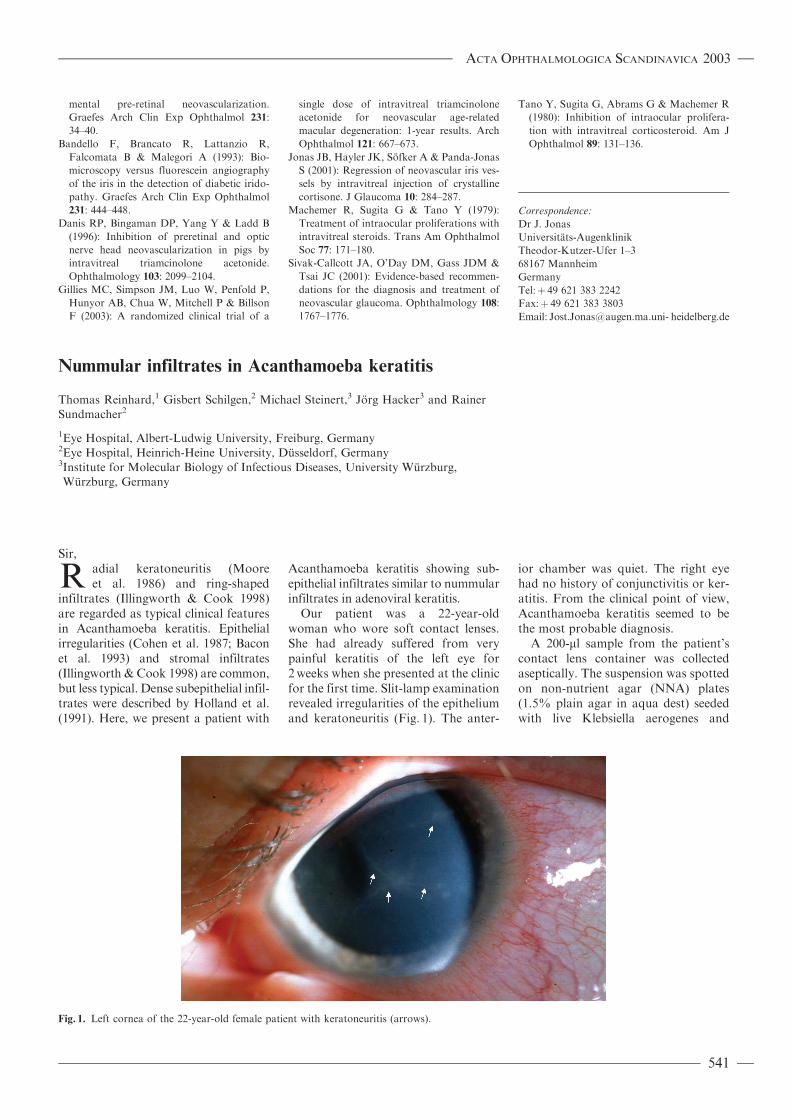
Our patient was a 22-year-oldwoman who wore soft contact lenses.She had already suffered from verypainful keratitis of the left eye for2weeks when she presented at the clinicfor the first time. Slit-lamp examinationrevealed irregularities of the epitheliumand keratoneuritis (Fig. 1). The anter-
ior chamber was quiet. The right eyehad no history of conjunctivitis or ker-atitis. From the clinical point of view,Acanthamoeba keratitis seemed to bethe most probable diagnosis.
A 200-ml sample from the patient’scontact lens container was collectedaseptically. The suspension was spottedon non-nutrient agar (NNA) plates(1.5% plain agar in aqua dest) seededwith live Klebsiella aerogenes and
Fig. 1. Left cornea of the 22-year-old female patient with keratoneuritis (arrows).
ACTA OPHTHALMOLOGICA SCANDINAVICA 2003
541
incubated at 20 �C. The NNA plateswere examined daily for trophozoitesand cysts. Amoebic isolates were iden-tified by morphological criteria and by18S rRNA in situ hybridization. The insitu hybridization was performed withan Acanthamoeba genus-specific oligo-nuceleotide probe as described pre-viously (Stothard et al. 1999; Grimmet al. 2001). Furthermore, materialharvested from the corneal surface wasanalysed in the same way.
Isolation and microscopic analysis ofprotozoa revealed that Acanthamoebatrophozoites and cysts were present inthe liquid in the contact lens container.The positive in situ hybridization sig-nals confirmed the prior identificationby morphological criteria. The optimalhybridization signals were obtainedwith 25% formamid. Using these strin-
gent conditions, the probe specificallyhybridized the Acanthamoeba isolatesas well as Acanthamoeba referencestrains (Grimm et al. 2001). We wereunable, however, to detect Acantha-moeba species in the material harvestedfrom the cornea.
Kanamycin sulfate (0.65%; AlconPharma, Freiburg, Germany), polyhex-amethylene biguanide (0.02%; ownpharmacy) and propamidine isethio-nate (0.1%; May & Baker Ltd, Dagen-ham, Essex, UK) eyedrops wereadministered every 15min for the next10 days. Thereafter, these eyedropswere tapered slowly. Topical predniso-lone 1% acetate application (Pharm-Allergan GmbH, Ettlingen, Germany)was started 6 days after referral to theclinic, with a daily dose of two drops.After 1month, all drugs (kanamycin
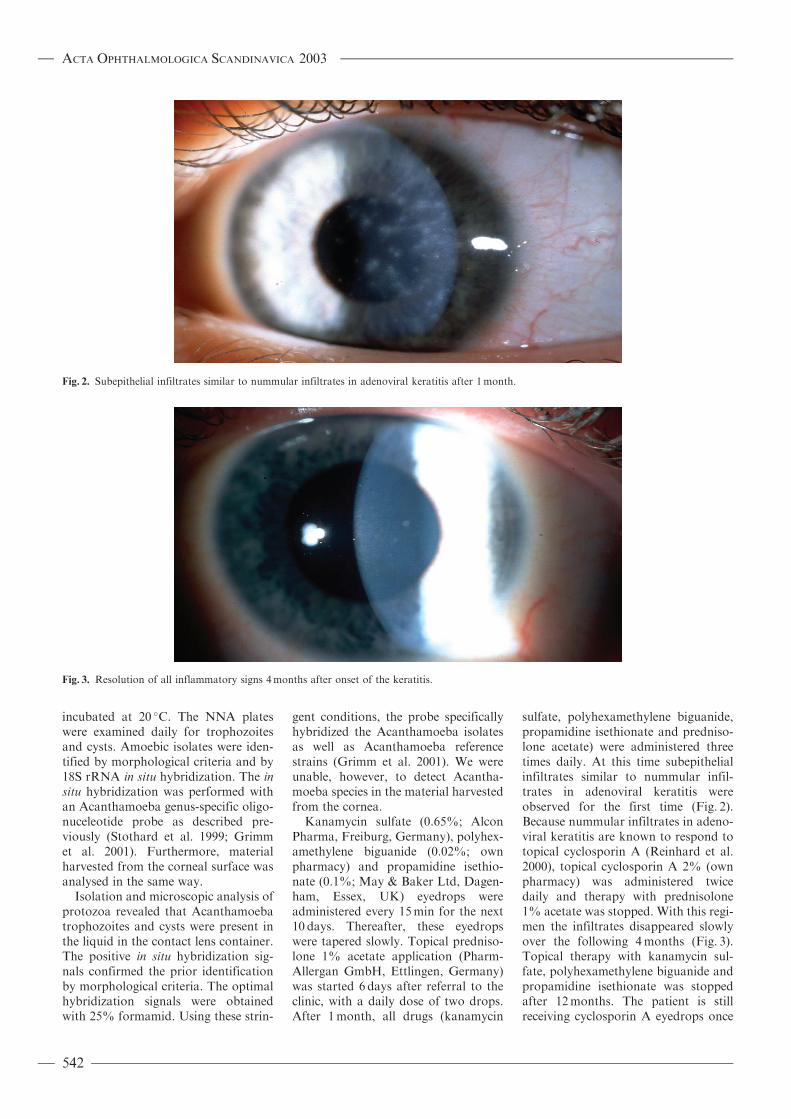
sulfate, polyhexamethylene biguanide,propamidine isethionate and predniso-lone acetate) were administered threetimes daily. At this time subepithelialinfiltrates similar to nummular infil-trates in adenoviral keratitis wereobserved for the first time (Fig. 2).Because nummular infiltrates in adeno-viral keratitis are known to respond totopical cyclosporin A (Reinhard et al.2000), topical cyclosporin A 2% (ownpharmacy) was administered twicedaily and therapy with prednisolone1% acetate was stopped. With this regi-men the infiltrates disappeared slowlyover the following 4months (Fig. 3).Topical therapy with kanamycin sul-fate, polyhexamethylene biguanide andpropamidine isethionate was stoppedafter 12months. The patient is stillreceiving cyclosporin A eyedrops once
Fig. 2. Subepithelial infiltrates similar to nummular infiltrates in adenoviral keratitis after 1month.
Fig. 3. Resolution of all inflammatory signs 4months after onset of the keratitis.
ACTA OPHTHALMOLOGICA SCANDINAVICA 2003
542

daily 12months after onset of the ker-atitis without any sign of recurrence.
In this case, the diagnosis ofAcanthamoeba keratitis was made viaa typical history (soft contact lenswearer, very painful keratitis), detec-tion of keratoneuritis at the slit-lampand detection of Acanthamoeba speciesvia immuno-genetic examination of thesoft contact lens container. Subepi-thelial infiltrates were observed for thefirst time after 4weeks. They were lessdense than those described by Hollandet al. (1991) and resembled nummularinfiltrates in adenoviral keratitis. Thesubepithelial infiltrates described byHolland et al. (1991) in six patientsoccurred up to 18months after onsetof Acanthamoeba keratitis, mostlywhen the patients were still receivingtopical corticosteroids. In our case, theinfiltrates disappeared when topicalcyclosporin A was administered. Mostprobably, the infiltrates were causedby an immunological reaction againstAcanthamoeba antigen in the anteriorcorneal stroma.
This is the first report of subepithe-lial infiltrates similar to nummular infil-trates in adenoviral keratitis in apatient with Acanthamoeba keratitis.The infiltrates disappeared with com-bined therapy of topical anti-amoebicagents and cyclosporin A.
ReferencesBacon AS, Frazer DG, Dart JKG,MathesonM,
Ficker LA & Wright P (1993): A review of 72
consecutive cases of Acanthamoeba keratitis,
1984–92. Eye 7: 719–725.
Cohen EJ, Parlato CJ, Arentsen JJ, Genvert
GI, Eagle RC, Wieland MR & Laibson PR
(1987): Medical and surgical treatment of
Acanthamoeba keratitis. Am J Ophthalmol
103: 615–625.
Grimm D, Ludwig W, Brandt BC, Michel R,
Schleifer KH, Hacker J & Steinert M (2001):
Development of 18S rRNA-targeted oligo-
nucleotide probes for specific detection of
Hartmannella and Naegleria in Legionella-
positive environmental samples. Syst Appl
Microbiol 24: 76–82.
Holland EJ, Alul IH, Meisler DM, Epstein RJ,
Rotkis WM, Nathenson AL & Liesegang TJ
(1991): Subepithelial infiltrates in Acantha-
moeba keratitis. Am J Ophthalmol 112:
414–418.
Illingworth CD & Cook SD (1998): Acantha-
moeba keratitis. Survey Ophthalmol 42:
493–508.
Moore MB, McCulley JP, Kaufman HE &
Robin JP (1986): Radial keratoneuritis as a
presenting sign in Acanthamoeba keratitis.
Ophthalmology 104: 1310–1315.
Reinhard T, Pfahl HG, Godehardt E & Sund-
macher R (2000): Topical cyclosporin A in
nummular infiltrates after adenoviral kera-
toconjunctivitis. A pilot study. Ophthalmo-
loge 97: 764–768.
Stothard DR, Hay J, Schroeder-Dietrich JM,
Seal DV & Byers TJ (1999): Fluorescent oli-
gonucleotide probes for clinical and environ-
mental detection of Acanthamoeba and the
T4, 18S rRNA gene sequence type. J Clin
Microbiol 37: 2687–2693.
Correspondence:
Thomas Reinhard MD
79085 Freiburg
Germany
Tel:þ 49 761 270 4005
Fax:þ 49 761 270 4063
Email: [email protected]
Kearns–Sayre syndrome, abnormal corneal endothelium
and normal tension glaucoma
Tomasz Zarnowski,1 Michaela Jaksch,2 Robert Rejdak1 and Zbigniew Zagorski1
1Tadeusz Krwawicz Chair of Ophthalmology and 1st Eye Hospital, University School
of Medicine, Lublin, Poland2Metabolic Disease Centre Munich-Schwabing, Munich, Germany
Sir,
W e present a rare coincidence ofKearns–Sayre syndrome, low
corneal endothelial density and normaltension glaucoma. In Kearns–Sayresyndrome (KSS), the triad of externalophthalmoplegia, heart block and ret-inal pigmentary changes remains thecornerstone of diagnosis, althoughnumerous additional signs have beenrecognized (Kearns & Sayre 1958). Asignificant proportion of patients showdeletions of the mitochondrial DNA(mtDNA) (Moraes et al. 1989).
Our patient was a 34-year-oldwoman with a history of bilateraldrooping eyelids accompanied by pro-gressive bilateral ophthalmoplegia. Atthe age of 29 years, glaucoma was diag-nosed. There was no familial history of
neurological disease or glaucoma andno patient history of vascular risk fac-tors (high or low blood pressure, coldhands and feet). At the same age, car-diac arrhythmias caused by conductionblock of the His bundle was diagnosed.
Four years later, ophthalmic exami-nation disclosed visual acuity (VA) of0.5 (þ 1.5D) in the right eye (RE) and0.3 (þ 1.5D) in the left eye (LE), withnormal pupils. The patient had no orminimal upgaze and downgaze in eithereye and minimal horizontal ductions. Aslightly asymmetric ptosis was diag-nosed, with a third of the upper marginof the pupil covered by the eyelid in theRE (moderate ptosis of 3mm) and halfthe upper margin of the pupil coveredby the eyelid in the LE (moderate ptosis
of 3.5mm). Moreover, a characteristicbilateral facial weakness (facies myo-pathica) was present. Anterior segmentexamination was unremarkable. Appla-nation pressures measured at differenttimes during the day ranged from13mmHg to 20mmHg. On gonioscopy,angles were wide open over 360 degreeswith no evidence of atypical pigmenta-tion. In the RE, Humphrey 30–2 visualfields demonstrated an almost completeupper hemifield defect correspondingto the disc changes. The LE visualfield was borderline. Both discs showedcontour cupping that was broader anddeeper on the right with markedbilateral peripapillary atrophy. In theRE the vertical C/D ratio was 0.9,with a marked neuro-retinal rim notch
ACTA OPHTHALMOLOGICA SCANDINAVICA 2003
543
in the infero-temporal pale pole; in theLE the vertical C/D ratio was 0.8. Bothmaculae and the midperiphery showedmoderate pigmental clumping.
Specular microscopy revealed 1499cells/mm2 in the RE (below the normalrange) and 1895 cells/mm2 in the LE(below the normal range). Cornealendothelial cells revealed features ofsevere pleomorphism and polymegath-ism. Axial lengths were 21.80mm in theRE and 21.84mm in the LE.
All laboratory tests were unremark-able. Both brain CT and MRI scanswere normal. Electromyography wasnormal. Echocardiography revealed aminor mitral valve insufficiency, butwas otherwise normal. Repeated elec-trocardiography showed signs of heartblock, which increased over the next
4 years. Recently, a bifascicular blockof the His bundle was diagnosed.
A muscle biopsy was performed toconfirm the clinical diagnosis ofKearns–Sayre syndrome. Molecularanalysis of the mtDNA revealed a sig-nificant deletion of about 6–7 kb inlength, with a heteroplasmic rate ofabout 50%. Histological and biochem-ical (respiratory chain) examinationsrevealed no abnormalities. Deletionsin KSS range from 1.5 kb to > 7.0 kband are not localized to a specificregion of the mitochondrial genome.The proportion of mutated genomes inKSS patients ranges from 45% to 75%of total mtDNA. There are no correla-tions between the size or site of thedeletion, biochemical abnormality ofmitochondrial enzymes and clinical
severity (Zeviani et al. 1988). Consis-tently with this, histological and bio-chemical examination revealed noabnormalities in our patient, who washarbouring 50% deleted mtDNA mol-ecules in her skeletal muscle.
The development of glaucomatousdamage in our patient could not beexplained by family history, systemicrisk factors or high intraocular pressure.In fact, the association of KSS and glau-coma seems to be very rare. Kalenak &Kolker (1989) described familial primaryopen-angle glaucoma in a 40-year-oldwoman with KSS. While glaucomaseems to be rarely associated with KSS,in another mtDNA mediated disorder,Leber’s optic neuropathy, normal tensionglaucoma appears to be present moreoften (Opial et al. 2001). Decreased cor-neal endothelial density, polymegathismand pleomorphism in both eyes are otherfindings associated with KSS (Ohkoshiet al. 1989). The fact that abnormal mito-chondrial dysfunction preferentiallyaffects cells with high energy demands(retinal pigment epithelium, cornealendothelium and extraocular muscles)may explain increased apoptosis in thesecells (Chang et al. 1993). In addition,recent studies suggest that excessiveapoptosis due to mtDNA abnormalitiesmay be an important mechanism in thepathogenesis of Fuchs’ endothelial dys-trophy (Borboli & Colby 2002).
As there is neither histological norgenetic evidence for the existence of anassociation between KSS and normaltension glaucoma, it seems that merecoincidence of symptoms is more likelyto explain this case.
ReferencesBorboli S & Colby K (2002): Mechanism of
disease: Fuchs’ endothelial dystrophy.
Ophthalmol Clin North Am 15: 17–25.
Chang TS, Johns DR, Walker D, de la Cruz Z,
Maumenee IH & Green WR (1993): Ocular
clinicopathologic study of the mitochondrial
encephalomyopathy overlap syndromes.
Arch Ophthalmol 111: 1254–1262.
Kalenak JW & Kolker AE (1989): Kearns–
Sayre syndrome and primary open-angle
glaucoma. Am J Ophthalmol 108: 335–336.
Kearns TP&SayreGP (1958): Retinitis pigmen-
tosa, external ophthalmoplegia and complete
heartblock. Arch Ophthalmol 60: 280–287.
Moraes CT,DiMauro S, ZevianiM et al. (1989):
Mitochondrial DNA deletions in progressive
external ophthalmoplegia and Kearns–Sayre
syndrome. N Engl J Med 320: 1293–1299.
A
B
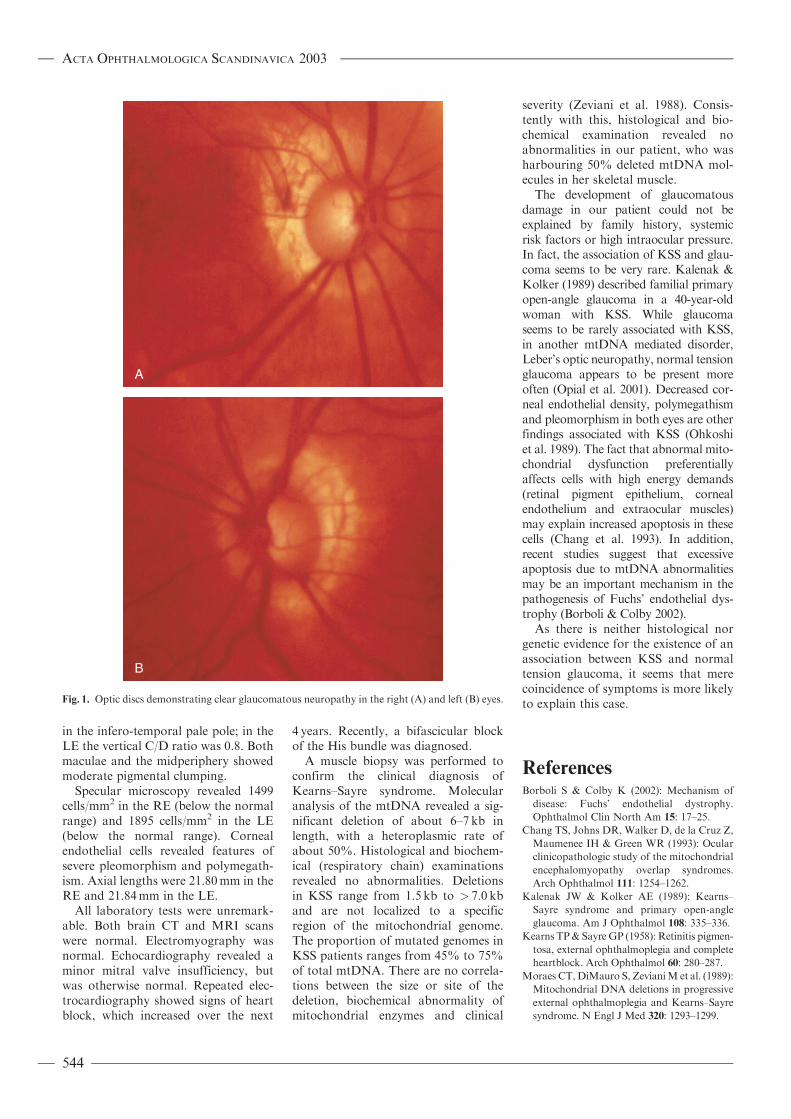
Fig. 1. Optic discs demonstrating clear glaucomatous neuropathy in the right (A) and left (B) eyes.
ACTA OPHTHALMOLOGICA SCANDINAVICA 2003
544

Ohkoshi K, Ishida N, Yamaguchi T & Kanki
K (1989): Corneal endothelium in a case of
mitochondrial encephalopathy (Kearns–
Sayre syndrome). Cornea 8: 210–214.
Opial D, Boehnke M, Tadesse S, Lietz-Partzsch
A, Flammer J, Hirano M, Fluckinger F &
Mojon DS (2001): Leber’s hereditary optic
neuropathy mitochondrial mutations in nor-
mal tension glaucoma. Graefes Arch Clin
Exp Ophthalmol 239: 437–440.
Zeviani M, Moraes CT, DiMauro S, Nakase
H, Bonilla E, Schon EA & Rowland LP
(1988): Deletions of mitochondrial DNA in
Kearns–Sayre syndrome. Neurology 38:
1339–1346.
Correspondence:
Dr Tomasz Zarnowski
Tadeusz Krwawicz Chair of Ophthalmology
1st Eye Hospital
University School of Medicine
Chmielna 1
20-079 Lublin
Poland
Tel:þ 48 81 53 49 843
Fax:þ 48 81 53 24 827
Email: [email protected]
The disposable contact lens is maintained in high osmotic
pressure fluid
Masaru Yoshii,1 Shigekuni Okisaka1 and Kenji Yanashima2
1Department of Ophthalmology, National Defence Medical College, Saitama, Japan2Eye Clinic, National Rehabilitation Centre Hospital for the Disabled, Saitama, Japan
Sir,
N ot a few of our patients complainof a smarting sensation when
they wear new, disposable, soft contactlenses. This occurs even when the dispo-sable contact lens is cleaned in fresh,physiological salt solution just beforeinsertion and despite normal findingsat the anterior part of the eye. We inves-tigated the properties of the fluid usedfor shipping disposable contact lenses interms of pH and osmotic pressure. Toour knowledge, there has been no paperinvestigating the osmotic pressure of dis-posable contact lens shipping fluid.
Several serial lots of disposable contactlenses (1-Day AcuvueTM; Johnson andJohnson Vision Care Inc., Jacksonville,FL, USA) made in the past 2 years wererandomly selected. The osmotic pressureand pH of the shipping fluid were meas-ured using HOSM-1 (TOA ElectronicsLtd, Tokyo, Japan). The osmotic pres-sure was measured using a freezingpoint lowering method; pH was meas-
ured using a glass electrode method.Two different concentrations of physio-logical salt fluids (0.85w/v%, 0.95w/v%)were alsomeasured for comparison in thesame way. Three kinds of standard solu-tions (100mOsm/kg, 900mOsm/kg,0.9% Nacl) were used for the osmoticpressure calibration. Two types of stand-ard solutions (pH¼ 4.01, pH¼ 6.86)were used for the pH calibration.
The osmotic pressure of the shippingfluid proved to be significantly higherthan that of the control physiological saltfluid, as shown in Table 1. It is probablethat the shape of a disposable contact lenschanges when the new lens is removedfrom the shipping fluid, which has a highlevel of osmotic pressure, to be washed infresh, physiological salt fluid, which has amuch lower osmotic pressure. The pHmeasurement values showed neutralityand the variance was slight.
We saw 6274 patients in our disposablecontact lens clinic last year and used
18353 contact lenses. We usually washthe disposable contact lens with physiolo-gical salt solution just after removing itfrom the package. After the patientapplies the disposable contact lenses tohis/her eyes, an ophthalmologist alwaysperforms a slit-lamp examination tocheck the fitting condition of the lenses.The slit-lamp examination is repeatedevery 4months. Thus far, none of ourpatients have suffered from disposablecontact lens disturbance.
The smarting sensationmay be relatedto the difference in the osmotic pressuresof the shipping fluid of the disposablecontact lens and the physiological saltsolution used for cleaning. Nonetheless,contact lens-induced disturbance canbe prevented in most, if not all, casesthrough appropriate, routine follow-upcare (White & Scott 1999) for disposablecontact lenses provided by trained andlicensed ophthalmologists.
ReferencesWhite P & Scott C (1999): Contact lenses. In:
Yanoff M & Duker JS (eds). Ophthalmol-
ogy. London: Mosby 11.1–11.8.
Correspondence:
Masaru Yoshii MD
Department of Ophthalmology
National Defence Medical College
3–2 Namiki
Tokorozawa-shi
Saitama-ken 359-8513
Japan
Tel:þ 81 42 995 1211
Fax:þ 81 42 993 5332
Email: [email protected]
Table 1. Osmotic pressures of shipping fluid and control physiological salt fluid.
Lot No. pH Osmotic
pressure
(mOsm/kg)
1300260156 7.22 459
1000310151 7.23 453
2255310811 7.28 434
2259810522 7.25 424
2859930620 7.26 424
3152540622 7.21 420
1902850809 7.39 422
Control (Nacl)
0.85 w/v% 283
0.95 w/v% 302
ACTA OPHTHALMOLOGICA SCANDINAVICA 2003
545