journal supplement: rethink atherectomy: expert insights ... · reprints of articles are available....
TRANSCRIPT
LLCan HMP Communications Holdings Company
,™
September 2013Volume 25/ Supplement B
www.invasivecardiology.com
The Official Journal of the International Andreas Gruentzig Society
Print ISSN 1042-3931 / Electronic ISSN 1557-2501
Rethink Atherectomy:Expert Insights Into Clinical Application and Use of the
JETSTREAM System
Copyright© 2013 HMP Communications, LLC. All rights reserved. Opinions expressed by authors are their own and not necessar-ily those of HMP Communications, the editorial staff, or any member of the editorial advisory board. This material was submitted as a supplement and was not reviewed by the journal editor or the editorial advisory board. Reprints of articles are available. Contact HMP Communications for information (www.invasivecardiology.com)
Cover_BayerSupplement_0913.indd 1 8/20/13 8:25 AM

2B The Journal of Invasive Cardiology®
Optimizing Strategy in Peripheral Vascular Interventions: The Role of JETSTREAM® Atherectomy
Nicolas W. Shammas, MD, EJD, MS, FACC, FSCAI, FICA
Over the past several years, major advancements have been made in the treatment of infrainguinal disease. The “tool box” has expanded with several manu-
facturers bringing to the market multiple balloons, wires, stents, atherectomy devices, CTO catheters, and so forth. Endovascular specialists are left to choose the right device for the right lesion based on their experience and understand-ing of how these devices operate and where they are most effective. In general, high-level evidence comparing effec-tiveness and safety of these devices is generally lacking with available data mostly derived from small, randomized trials or observational registries. Given the lack of clear recom-mendations about when certain devices are best applied for the most effective and safe results, a general guiding strat-egy to approach infrainguinal disease may be necessary. The “leave nothing strategy” appears to have gained momentum and reflects on our desire to keep the vessel free of stents. Despite randomized data indicating stenting can improve patency over balloon angioplasty, stents continue to have several problems in infrainguinal interventions with reduced patency on long-term follow-up, fractures, re-occlusion by a restenotic-thrombotic process, and possible interference with surgical options and emerging anti-restenotic technolo-gies such as drug-coated balloons or drug-coated stents.
Changing vessel compliance to reduce dissections, bail out stenting and vessel barotrauma, protecting the outflow vessels, and reducing smooth muscle cell proliferation have been the main anchors of a guiding strategy in our labo-ratory when approaching infrainguinal disease. Recently published or presented randomized trials have shown that atherectomy can accomplish the task of reducing dissections
and bail out stenting. Embolic filter protection and em-bolic capture balloon technology have added a level of pro-tection to the outflow vessels, and now with drug-coated balloons, restenosis, and target lesion revascularization can be improved upon.
In this supplement to the Journal of Invasive Cardiology, I discuss the multiple challenges operators encounter when treating infrainguinal disease with a focus on the importance of atherectomy in addressing the issue of changing vessel compliance, reducing dissection, and stenting. The impor-tance of protecting the outflow vessels during atherectomy is also presented. Dr. Ramaiah presents the JETSTREAM device and its distinguishing features from existing atherec-tomy devices on the market including active aspiration, front cutting rotational design, and expandable blade technology. Dr. Davis explores key tips and tricks with the use of the JETSTREAM device including introducers and wire selec-tion, the importance of audible and tactile feel during the operation of the device, the technique of catheter advance-ment and pullback, the use of the blades-up and blades-down feature, and how to avoid distal embolization. Finally, Dr. Shimshak presents 2 case reports with the JETSTREAM system illustrating its strengths in treating severe calcified lesions. Intravascular ultrasound assessment of the lesion before and after treatment is also presented and shows the ability of the device to effectively remove calcium.
Nicolas W. Shammas, MD, MS, FACC, FSCAIPresident and Research Director, Midwest Cardiovascular Research FoundationDavenport, IA
From the Midwest Cardiovascular Research Foundation, Davenport, IA.Disclosure: The author has no commercial, proprietary, or financial interest in any products described in this article. Dr Shammas received related research and educational
grants to the Midwest Cardiovascular Research Foundation from Covidien, Spectranetics, Bayer HealthCare, Medtronic, Boston Scientific, Abbott, and CSI. Supported in part by the Nicolas and Gail Shammas Research Fund at MCRF. Full disclosure at www.mcrfmd.com.
Address for correspondence: Nicolas W. Shammas, MD, MS, FACC, FSCAI, FICA, President and Research Director, Midwest Cardiovascular Research Foundation, 1622 E Lombard Street, Davenport, IA 52803. Email: [email protected]
Editorial-Shammas_0913.indd 2 8/20/13 8:25 AM

Vol. 25, Supplement B, 2013 3B
Addressing Challenges in the Treatment of Infrainguinal Arterial Disease: an Endovascular Specialist’s Perspective
Nicolas W. Shammas, MD, EJD, MS, FACC, FSCAI, FICA
ABSTRACT: Infrainguinal interventions remain challenging to endovascular specialists. Treatment of the femoropopliteal (FP) ar-tery represents approximately 40% of all infrainguinal interventions. The FP artery is subject to multiple external forces. The use of self-expanding nitinol stents in this vessel modestly improves patency but is associated with several potential problems including stent fracture, in-stent restenotic-thrombotic re-occlusions and continued low pa-tency rate on long-term follow-up. Also, infrapopliteal (IP) vessels are generally small in diameter and tend to be calcified with long segments of disease and occlusions. IP vessels are therefore likely to have a high rate of dissection with balloon angioplasty as a primary treatment. Stenting the IP vessels with current stent technology is a suboptimal strategy that should generally be avoided. Literature review supports a strategy based on a triad of improving vessel com-pliance and reducing barotrauma and dissection, minimizing distal embolization and applying anti-restenotic measures to improve pa-tency and reduce target lesion revascularization. We review current literature and tools available to the endovascular specialist to achieve these goals.
Key words: femoropopliteal artery, restenosis, atherectomy, drug coated balloon, in-stent restenosis, distal embolization, tibial runoff, stent fracture, patency, target lesion revascularization, tibial artery,
peroneal artery
Peripheral artery disease (PAD) is an endemic problem, predominantly apparent in elderly, diabetics, and smokers. Currently 12%-14% of people in the United States have PAD. The severity of PAD is a strong predictor of cardiovascular mortality. Therefore, treatment needs to focus on aggressive risk factor modification in addition to revascularization strat-egies to improve symptoms of claudication, reduce amputa-tion, and improve survival.1
Endovascular treatment of infrainguinal disease (FP and IP) has remained a challenge particularly in advanced type C and D lesions as defined by The Trans-Atlantic Inter-Society Consen-sus Document on the Management of Peripheral Arterial Dis-ease (TASC II).2 With the advent of multiple tools to treat these complex lesions, endovascular specialists are now approaching these lesions non-surgically. Despite a relatively high initial procedural success with catheter-based therapies, the long-term outcomes have been less than encouraging with an overall lower patency and high repeat target lesion revascularization (TLR).
We describe our approach in treating infrainguinal disease with a focus on improving compliance and minimizing dissec-tion and bailout stenting, preserving distal runoff and applying anti-restenotic therapies for more durable long-term results.
Treatment of the Femoropopliteal ArteryDe novo lesionsThere is little debate that TASC II A and B lesions are
best suited for endovascular therapies. Although the TASC II committee recommends surgical therapy for TASC C and D lesions, these are now increasingly being handled using an en-dovascular approach. There is no consensus to the best endo-vascular approach in treating de novo lesions in the FP artery. Both primary and provisional stenting of the FP segment are strategies practiced widely. Balloon angioplasty (PTA) alone leads to a higher rate of dissection and need for bailout stent-ing.13 In one study, predictors of bailout stenting included TASC D lesions, moderate (versus mild or none) calcification and primary use of PTA (versus initial debulking prior to ad-junctive PTA).4
We have previously proposed a strategy based on the triad of improving vessel compliance and reducing bailout stenting (mechanical), preserving the outflow vessels (procedural), and reducing restenosis (biological) in approaching the treatment of FP segments.5
Several trials have evaluated the value of stenting in FP disease. Data suggest that stenting of the superficial femoral artery (SFA) reduces the rate of restenosis when compared to PTA. In 104 patients randomized to primary stenting versus PTA of the SFA (mean lesion length in the stent group 11.2 cm), Schillinger et al6 noted that the 6-month rate of resteno-sis on angiography was 24% in the stent group and 43% in the PTA group (P=0.05). At 2-year follow-up, restenosis rates were 45.7% vs 69.2%, respectively, by an intention-to-treat analysis (P=0.031) and 49.2% vs 74.3% (P=0.028), respec-tively, by actual treatment received.7 In a recent randomized trial, Laird et al8 reported freedom from TLR at 12 months to be 87.3% for the Lifestent (Bard Peripheral Vascular) com-pared with 45.1% for PTA as a primary therapy in treating short FP lesions (mean lesion length 7.1 cm in the stented group) (P<0.0001). Duplex ultrasound-derived primary pa-tency at 12 months was better for the stent group (81.3% vs 36.7%; P<0.0001). At 3-year follow-up freedom from TLR was significantly better in the stent group (75.5% vs 41.8%, P<0.0001).9 In contrast, Krankenberg et al10 randomized 244 patients with SFA disease (mean lesion length 4.5 cm) to the Bard Luminexx 3 stent vs PTA. There was no difference in restenosis rates between the stent (31.7 %) and the PTA (38.6%) arms at 1 year. TLR rates at 1 year were 18.3% and 14.9% (non-significant), respectively. Differences in stent
From the Midwest Cardiovascular Research Foundation, Davenport, IA.Disclosure: The author has no commercial, proprietary, or financial interest in any
products described in this article. Dr Shammas received related research and educa-tional grants to the Midwest Cardiovascular Research Foundation from Covidien, Spectranetics, Bayer HealthCare, Medtronic, Boston Scientific, Abbott, and CSI. Supported in part by the Nicolas and Gail Shammas Research Fund at MCRF. Full disclosure at www.mcrfmd.com
Address for correspondence: Nicolas W. Shammas, MD, MS, FACC, FSCAI, FICA, President and Research Director, Midwest Cardiovascular Research Founda-tion, 1622 E Lombard Street, Davenport, IA 52803. Email: [email protected]
Shammas_0913.indd 3 8/22/13 8:48 AM

4B The Journal of Invasive Cardiology®
SHAMMAS
design may have been one factor that accounted for the lack of improvement in patency and TLR in this study.
Irrespective of the stent used, there were continued sig-nificant high TLR rates at one and 2 years in patients who re-ceived stenting of the FP artery.6-11 Stenting reduces restenosis by preventing negative remodeling and recoil rather than re-ducing neointimal proliferation.12 Cryoplasty has been used to improve on stent results. Cryoplasty does reduce neointimal proliferation using cell apoptosis.13 Adjunctive cryoplasty after stenting of the FP segment did show a reduction in restenosis in diabetics. In the COBRA (cryoplasty therapy or conven-tional balloon post-dilation of nitinol stents for revascular-ization of peripheral arterial segments) randomized trial, FP binary restenosis after adjunctive cryoplasty was significantly reduced compared to PTA (29.3% vs 55.8%, p=0.01).14 Re-cently the Zilver PTX,15 a paclitaxel-coated self-expanding stent, was approved in the US. In the Zilver PTX random-ized trial, the ZilverPTX stent (Cook Medical) had a superior 12-month event-free survival (90.4% vs 82.6%; P=0.004) and primary patency (83.1% vs 32.8%; P<0.001) when compared with PTA.
Stents in the FP segment can fracture over time because they are subject to repetitive external forces, including flex-ion, torsion, and compression. Low grade stent fracture is less likely to cause restenosis but high grade fractures were associ-ated with higher rate of restenosis.16,17 Furthermore, stent total re-occlusion is a restenotic-thrombotic process generally more difficult to treat and carries a higher rate of procedural com-plications, recurrent restenosis, and re-stenting.18,19 In addi-tion, it is unclear how a stented FP segment interferes with the effectiveness of emerging anti-restenotic technologies such as drug-coated balloons or drug-coated stents. Finally, stents in-volving the popliteal or common femoral arteries may reduce future surgical options and are best avoided in these locations except in bailout situation.
Atherectomy has emerged as an alternative option to pri-mary stenting of the FP artery. Using directional cutting of FP de novo lesions, SilverHawk atherectomy (Covidien) improved vessel compliance and reduced dissection and bailout stenting compared to PTA alone.3 In the COMPLIANCE 360 trial,20 differential sanding using the Diamondback 360° of calcified FP lesions improved lesion compliance and resulted in reduc-tion in bailout stenting. In addition to debulking with dif-ferential cutting or sanding, plaque modification with cutting balloon may improve compliance and reduce dissection. In short, in de novo SFA lesions (<5 cm), CB had less restenosis than PTA (13% vs 36%; P=0.049) at 12-month follow-up.21 However, this was not consistent across studies.
Amighi et al22 showed no reduction in restenosis post-CB treatment of short de novo FP lesions compared to PTA (32% PTA vs 62% CB at 6 months, respectively; P=0.048). The impact of ablative treatment using excimer laser (Spectranet-ics) or cutting with rotational atherectomy and aspiration with the JETSTREAM device (Bayer HealthCare) on vessel compliance and bailout stenting is unknown. In the CELLO trial (Clirpath Excimer Laser System to Enlarge Lumen Open-ings) patency of FP de novo lesions were 59% and 54% at 6
and 12 months, respectively.23 Furthermore, in observational studies, bailout stenting of the FP segment after excimer la-ser was variable, ranging from 23% to 50% but these stud-ies did not assess vessel compliance and had no comparative PTA arm.19,24 Zeller et al25 reported a 99% device success rate in the multicenter Pathway Peripheral Vascular disease trial (using the JETSTREAM Atherectomy System, Bayer Health-Care) in infrainguinal disease (including non-stent restenotic lesions). In this study, clinically driven TLR rates at 6 and 12 months were 15% and 26%, respectively and the 1-year reste-nosis rate was 38.2% based on duplex imaging. Currently the ongoing JET multicenter prospective registry is evaluating the JETSTREAM rotational and aspiration catheter on TLR at 1 year, acute procedural results, distal embolization and bailout stenting in claudicants with de novo or non-stent restenotic FP lesions.26 At present, there are no randomized data comparing atherectomy with adjunctive drug-coated balloon (DCB) vs atherectomy alone or stenting alone or stenting with adjunc-tive DCB. A small non-randomized study from Italy suggest-ed that atherectomy with DCB yielded better patency rates and improved TLR compared to atherectomy alone.27
Paclitaxel-coated angioplasty balloons have reduced reste-nosis in the FP arteries. In the multicenter Thunder (local Taxan with short time exposure for reduction of restenosis in distal arteries) trial,28 TLR was 37% at 6 months and 52% at 24 months in the control group and 4% and 15% in the paclitaxel-coated balloon group (P<0.001), respectively. In ad-dition, Werk et al29 reported a TLR rate of 33% in control and 6.7% in the paclitaxel-coated balloon (P<0.002) at 6 months. DCB are likely to be a game changing technology in the treat-ment of FP disease.
We have adopted the strategy of atherectomy with low pressure adjunctive PTA as the initial preferred therapy in our laboratory with a significant reduction in dissection rates and need for bailout stenting. The ongoing XL-PAD, a multicenter prospective registry, is currently collecting data on FP treat-ment to evaluate 6-month and 1-year outcomes using various treatment modalities and comparing them to stenting.30
In-stent restenotic lesionsTreatment of in-stent restenosis (ISR) is challenging, par-
ticularly when re-occlusion has occurred. These re-occlusions are typically thrombotic-restenotic lesions with high distal embolic potential and may require additional stenting over existing stents.18,19 In patients with a previously placed stent, smooth muscle cell proliferation accounts for restenosis as recoil and negative remodeling are not likely. Re-stenting of the FP artery is generally not recommended. The short- and long-term outcomes of more than one layer of stent in the FP segment are unknown.
PTA has very high rate of restenosis and debulking has been attempted as a way to reduce or delay TLR. Zeller et al31 reported on 43 patients with FP ISR (mean lesion length of 131 mm) treated with SilverHawk atherectomy. Patency rate was 54% at 1-year. Using excimer laser and the Viabahn (WL Gore and Associates) stent, Laird et al32 reported a primary patency at 12 months of 48% in the SALVAGE trial. In the
Shammas_0913.indd 4 8/20/13 8:26 AM

Vol. 25, Supplement B, 2013 5B
Addressing Challenges in the Treatment of Infrainguinal Arterial Disease
PATENT (Photo-Ablation Using the Turbo-Booster and Ex-cimer Laser for In-Stent Restenosis Treatment) study,33 a pro-spective registry evaluating laser atherectomy for treating FP ISR, Zeller et al reported 82% and 52% freedom from TLR at 6 and 12 months, respectively. Similarly, Shammas et al34 reported a TLR of 48.7% at 1 year in 40 patients treated with the excimer laser for FP ISR with mean lesion length of 201.4 mm. Finally, Beschorner et al35 reported their data on 40 in-frainguinal ISR lesions treated with the Pathway PV ather-ectomy system. Primary patency was 33% after 12 months and 25% after 24 months. The ongoing JETSTREAM ISR registry36 is currently evaluating rotational atherectomy with aspiration in treating FP ISR lesions. In addition to its ability to remove de novo and restenotic tissue, the JETSTREAM is also a thrombectomy device, an added advantage in treating totally occluded FP ISR lesions. The ongoing EXCITE-ISR (Randomized Study of Laser and Balloon Angioplasty Versus Balloon Angioplasty to Treat Peripheral In-stent Restenosis) trial is a superiority study evaluating debulking with the ex-cimer laser on ISR compared to PTA.37
Debulking is emerging as an important tool in treating FP ISR. The value of debulking is mostly delaying TLR in the intermediate follow-up phase, which may reduce the need for early reintervention compared to PTA alone. Almost half the patients will return for reintervention at 1 year. Therefore de-bulking may need to be coupled with anti-restenotic measures to have a significant clinical impact on altering the course of FP ISR. Also it is unclear whether debulking in FP ISR would add a significant improvement in patency to DCB alone. Ex-cimer laser followed by a paclitaxel-coated angioplasty balloon (PTX PTA) is currently being compared in Europe to PTX PTA alone in the treatment of FP ISR lesions.
Treatment of Infrapopliteal ArteryThe treatment of IP lesions is mostly reserved for critical
limb ischemia patients with the goal of limb salvage or in se-vere claudicants with only severe outflow obstructive disease. Stenting of IP vessels is currently not recommended except as a bailout strategy when other non-stent modalities have failed. Although some operators have used drug-eluting stents to treat tibial vessels, use for IP vessels is off-label in the United States. Improving vessel compliance, avoiding flow limiting dissection, and minimizing distal embolization are primary intraprocedural goals when treating the IP vessels.
A clear dichotomy exists between patency, need for TLR, and limb salvage in the treatment of IP lesions.38 Restenosis is typically high in treating IP vessels but limb salvage rates are in the upper 80% to low 90% at 1 year irrespective of what modality has been used to treat these vessels. TLR is also less likely to be needed after the wound has healed and despite loss of patency. This is likely attributable to the fact that a limb with an active wound requires significantly more blood flow for healing than a limb with no ulceration.38
A large percentage of IP vessels have moderate to severe calcification. PTA is likely to result in significant dissection in IP vessels. Debulking prior to adjunctive low pressure PTA may improve compliance and reduce dissection rates. This
hypothesis was validated in the Calcium 360 trial.39 In this multicenter randomized study of adjunctive balloon angio-plasty following orbital atherectomy (CSI) of moderate to severely calcified IP vessels in patients with predominantly critical limb ischemia, debulking yielded an improvement in vessel compliance, less flow limiting dissection, and less bail-out stenting when compared to PTA alone. Of interest in the Calcium 360 trial, the presence of a high residual narrowing post-PTA correlated with increased major adverse events on follow up, a finding that needs to be reproduced in larger clin-ical trials. Furthermore, Zeller et al40 reported their experience with directional atherectomy using the SilverHawk catheter (Covidien) in the treatment of IP disease. Only 4% of lesions required bailout stenting. In 98% of lesions treated, residual narrowing was <30%. Primary and secondary patency rates were 67% and 91% after 1 year and 60% and 80% after 24 months, respectively.
The main advantage of atherectomy over PTA in treatment of IP vessels is the reduction of dissection and bailout stenting. Although cryoplasty had favorable results in treating critical limb ischemia,41 two small, randomized trials suggested that cryoplasty using the PolarCath (Boston Scientific) does not significantly reduce dissection rate and need for stenting in the FP artery but randomized data in the IP vessels is lacking.42,43 Atherectomy with or without adjunctive balloon angioplasty will likely remain an important first line therapy of IP vessels.
Distal embolizationThe treatment of FP or IP lesions carries the risk of distal
embolization (DE),44-47 which requires treatment in 2%-3% of unselected infrainguinal interventions.44 Predictors of DE include thrombotic occlusion, long lesions, TASC D lesions, heavy calcification, mechanical thrombectomy, and atherec-tomy.3,46-48 DE is associated with limb loss,48 longer procedure times, higher contrast use, and increased radiation exposure.49 Also, compromised distal runoff post-procedure may be a pre-dictor for early restenosis/re-occlusion after FP PTA.50
Embolic protection devices in treating the lower extrem-ity vessels have recently been approved by the FDA: Spider Filter (Covidien) and Proteus balloon (Angioslide).51-53 Em-bolic protection adds significant cost to the procedure and is currently not reimbursed. The JETSTREAM System (Bayer HealthCare) is a rotational atherectomy device with simulta-neous aspiration, a unique feature among all existing atherec-tomy devices and with a theoretical advantage of minimizing DE and possibly the need for routine embolic filter use. Both the JET and JETSTREAM ISR registries are evaluating oc-currence of DE with the use of the JETSTREAM catheter in treating FP lesions.
ConclusionA strategy of improving vessel compliance with debulk-
ing, minimizing flow limiting dissection, and bailout stenting coupled with adjunctive low pressure balloon inflation using a paclitaxel-coated balloon is likely to emerge as an effective strategy in treating infrainguinal PAD. The use of embolic pro-tection devices to protect the outflow vessels will be important
Shammas_0913.indd 5 8/22/13 8:48 AM
6B The Journal of Invasive Cardiology®
SHAMMAS
particularly with excimer or SilverHawk atherectomy. Rotation-al atherectomy with simultaneous aspiration (JETSTREAM) or orbital atherectomy may reduce clinically significant DE and the need for routine embolic protection devices.
References1. Shammas NW. Epidemiology, classification and modifiable risk factors of peripheral arte-
rial disease. Vasc Health Risk Man. 2007;3:229-234.2. Norgren L, Hiatt WR, Dormandy JA, et al. Inter-Society Consensus for the Manage-
ment of Peripheral Arterial Disease (TASC II). Eur J Vasc Endovasc Surg. 2007;33(Sup-pl 1):S1-75.
3. Shammas NW, Coiner D, Shammas GA, et al. Percutaneous lower-extremity arterial inter-ventions with primary balloon angioplasty versus Silverhawk atherectomy and adjunctive balloon angioplasty: randomized trial. J Vasc Interv Radiol. 2011;22:1223-1228.
4. Shammas NW, Coiner D, Shammas G, et al. Predictors of provisional stenting in patients undergoing lower extremity arterial interventions. Int J Angiol. 2011 ;20:95-100.
5. Shammas NW. An overview of optimal endovascular strategy in treating the femoropopli-teal artery: mechanical, biological, and procedural factors. Int J Angiol. 2013;22:001-008.
6. Schillinger M, Sabeti S, Loewe C, et al. Balloon angioplasty versus implantation of nitinol stents in the superficial femoral artery. N Engl J Med. 2006;354:1879-1888.
7. Schillinger M, Sabeti S, Dick P, et al. Sustained benefit at 2 years of primary femoropop-liteal stenting compared with balloon angioplasty with optional stenting. Circulation. 2007;115:2745-2749.
8. Laird JR, Katzen BT, Scheinert D, et al. Nitinol stent implantation versus balloon angioplasty for lesions in the superficial femoral artery and proximal popliteal artery: twelve-month results from the RESILIENT randomized trial. Circ Cardiovasc Interv. 2010;3:267-276.
9. Laird JR, Katzen BT, Scheinert D, et al; for the RESILIENT Investigators. Nitinol stent implantation vs. balloon angioplasty for lesions in the superficial femoral and proximal popliteal arteries of patients with claudication: three-year follow-up from the RESILIENT randomized trial. J Endovasc Ther. 2012;19:1-9.
10. Krankenberg H, Schlüter M, Steinkamp HJ, et al. Nitinol stent implantation versus percu-taneous transluminal angioplasty in superficial femoral artery lesions up to 10 cm in length: the femoral artery stenting trial (FAST). Circulation. 2007;116:285-292.
11. Bosiers M, Deloose K, Callaert J, et al. Results of the Protege EverFlex 200-mm-long niti-nol stent (ev3) in TASC C and D femoropopliteal lesions. J Vasc Surg. 2011;54:1042-1050.
12. Capek P, McLean GK, Berkowitz HD. Femoropopliteal angioplasty. Factors influencing long-term success. Circulation. 1991;83(2 Suppl):I70-80.
13. Yiu WK, Cheng SW, Sumpio BE. Vascular smooth muscle cell apoptosis induced by “su-percooling” and rewarming. J Vasc Interv Radiol. 2006;17:1971-1977.
14. Banerjee S, Das T, Abu-Fadel MS, et al. Pilot trial of cryoplasty or conventional balloon post-dilation of nitinol stents for revascularization of peripheral arterial segments: The CO-BRA Trial. J Am Coll Cardiol. 2012;60:1352-1359.
15. Dake MD, Ansel GM, Jaff MR, et al. Paclitaxel-eluting stents show superiority to balloon angioplasty and bare metal stents in femoropopliteal disease: twelve-month Zilver PTX randomized study results. Circ Cardiovasc Interv. 2011;4:495-504.
16. Schlager O, Dick P, Sabeti S, et al. Long-segment SFA stenting — The dark sides: In-stent restenosis, clinical deterioration, and stent fractures. J Endovasc Ther. 2005;12:676-684.
17. Scheinert D, Scheinert S, Sax J, et al. Prevalence and clinical impact of stent fractures after femoropopliteal stenting. J Am Coll Cardiol. 2005;45:312-315.
18. Shammas NW, Dippel EJ, Shammas G, et al. Dethrombosis of the lower extremity arteries using the power-pulse spray technique in patients with recent onset thrombotic occlusions: results of the DETHROMBOSIS Registry. J Endovasc Ther. 2008;15(5):570-579.
19. Shammas NW, Weissman NJ, Coiner D, et al. Treatment of subacute and chronic throm-botic occlusions of lower extremity peripheral arteries with the excimer laser: a feasibility study. Cardiovasc Revasc Med. 2012;13:211-214.
20. Dattilo R. COMPLIANCE 360° 12-month data. American College of Cardiology 61st Annual Scientific Session. Abstract Presentation #1123-37.
21. Cotroneo AR, Pascali D, Iezzi R. Cutting balloon versus conventional balloon angioplasty in short femoropopliteal arterial stenoses. J Endovasc Ther. 2008;15:283-291.
22. Amighi J, Schillinger M, Dick P, et al. De novo superficial femoropopliteal artery lesions: peripheral cutting balloon angioplasty and restenosis rates--randomized controlled trial. Radiology. 2008;248:297-302.
23. Dave RM, Patlola R, Kollmeyer K, et al; for the CELLO Investigators. Excimer laser re-canalization of femoropopliteal lesions and 1-year patency: results of the CELLO registry. J Endovasc Ther. 2009;16:665-675.
24. Shammas NW, Coiner D, Shammas GA, et al; Distal embolic event protection using ex-cimer laser ablation in peripheral vascular interventions: results of the DEEP EMBOLI registry. J Endovasc Ther. 2009;16:197-202.
25. Zeller T, Krankenberg H, Steinkamp H, et al. One-year outcome of percutaneous rota-tional atherectomy with aspiration in infrainguinal peripheral arterial occlusive disease: the multicenter pathway PVD trial. J Endovasc Ther. 2009;16:653-662.
26. JETSTREAM NAVITUS™ System Endovascular Therapy Post-market Registry (JET).
http://clinicaltrials.gov/ct2/show/NCT0143643527. Cioppa A, Stabile E, Popusoi G, et al. Combined treatment of heavy calcified femoro-
popliteal lesions using directional atherectomy and a paclitaxel coated balloon: One-year single centre clinical results. Cardiovasc Revasc Med. 2012;13:219-223.
28. Tepe G, Zeller T, Albrecht T, et al. Local delivery of paclitaxel to inhibit restenosis during angioplasty of the leg. N Engl J Med. 2008;358:689-699.
29. Werk M, Langner S, Reinkensmeier B, et al. Inhibition of restenosis in femoropopliteal ar-teries: paclitaxel-coated versus uncoated balloon: femoral paclitaxel randomized pilot trial. Circulation. 2008;118:1358-1365.
30. Banerjee S, et al. Multi-Center Registry For Peripheral Arterial Disease Interventions and Outcomes. http://xlpad.org/study.html
31. Zeller T, Rastan A, Sixt S, et al. Long-term results after directional atherectomy of femoro-popliteal lesions. J Am Coll Cardiol. 2006;48:1573-1578.
32. Laird JR Jr, Yeo KK, Rocha-Singh K, et al. Excimer laser with adjunctive balloon angio-plasty and heparin-coated self-expanding stent grafts for the treatment of femoropopliteal artery in-stent restenosis: twelve-month results from the SALVAGE study. Catheter Cardio-vasc Interv. 2012;80(5):852-859.
33. PATENT trial. Photo-Ablation Using the Turbo-Booster and Excimer Laser for In-Stent Restenosis Treatment study. Presented at LINC 2012 at the Leipzig Interventional Course, in Leipzig, Germany. Article online in Endovascular Today. http://www.bmctoday.net/evto-day/2012/01/article.asp?f=interim-results-presented-for-spectranetics-patent-study
34. Shammas NW, Shammas GA, Hafez A, et al. Safety and One-Year revascularization outcome of excimer laser ablation therapy in treating in-stent restenosis of femoro-popliteal arteries: A retrospective review from a single center. Cardiovasc Revasc Med. 2012;13:341-344.
35. Beschorner U, Krankenberg H, Scheinert D, et al. Rotational and aspiration atherectomy for infrainguinal in-stent restenosis. Vasa. 2013;42:127-133.
36. Shammas NW. Safety and Effectiveness of JETSTREAM (JS) Atherectomy in Femoro-popliteal In-Stent Restenotic Lesions: A Prospective Registry. http://clinicaltrials.gov/ct2/show/NCT01722877
37. Dippel EJ. Randomized Study of Laser and Balloon Angioplasty Versus Balloon Angio-plasty to Treat Peripheral In-stent Restenosis (EXCITE ISR). http://www.clinicaltrials.gov/ct2/show/NCT01330628
38. Jaffery Z, Grant AG, White CJ. Critical limb ischemia: does long-term patency matter? Vasc Med. 2010;15:439-441.
39. Shammas NW, Lam R, Mustapha J, et al. Comparison of orbital atherectomy plus balloon angioplasty vs. balloon angioplasty alone in patients with critical limb ischemia: results of the CALCIUM 360 randomized pilot trial. J Endovasc Ther. 2012;19:480-488.
40. Zeller T, Sixt S, Schwarzwälder U, et al. Two-year results after directional atherectomy of infrapopliteal arteries with the SilverHawk device. J Endovasc Ther. 2007;14:232-240.
41. Das TS, McNamara T, Gray B, et al. Primary cryoplasty therapy provides durable support for limb salvage in critical limb ischemia patients with infrapopliteal lesions: 12-month follow-up results from the BTK Chill Trial. J Endovasc Ther. 2009;16(2 Suppl 2):II19-30.
42. Spiliopoulos S, Katsanos K, Karnabatidis D, et al. Cryoplasty versus conventional bal-loon angioplasty of the femoropopliteal artery in diabetic patients: long-term results from a prospective randomized single-center controlled trial. Cardiovasc Intervent Radiol. 2010;33:929-938.
43. Shammas NW, Coiner D, Shammas G et al. Percutaneous lower extremity arterial in-terventions using primary balloon angioplasty versus cryoplasty: a randomized pilot trial. Cardiovasc Revasc Med. 2012;13:172-176.
44. Shammas NW, Shammas GA, Dippel EJ, et al. Predictors of distal embolization in periph-eral percutaneous interventions: a report from a large peripheral vascular registry. J Invasive Cardiol. 2009;21(12):628-631.
45. Siablis D, Karnabatidis D, Katsanos K, et al. Outflow protection filters during percuta-neous recanalization of lower extremities’ arterial occlusions: a pilot study. Eur J Radiol. 2005;55:243-249.
46. Suri R, Wholey MH, Postoak D, et al. Distal embolic protection during femoropopliteal atherectomy. Catheter Cardiovasc Interv. 2006;67:417-422.
47. Shammas NW, Dippel EJ, Coiner D, et al. Preventing lower extremity distal emboliza-tion using embolic filter protection: results of the PROTECT registry. J Endovasc Ther. 2008;15:270-276.
48. Lam RC, Shah S, Faries PL, et al. Incidence and clinical significance of distal emboliza-tion during percutaneous interventions involving the superficial femoral artery. J Vasc Surg. 2007;46:1155-1159.
49. Shammas NW, Shammas GA, Dippel EJ, Jerin M. Intraprocedural outcomes following distal lower extremity embolization in patients undergoing peripheral percutaneous inter-ventions. Vasc Dis Manage. 2009;6:58-61.
50. Salapura V, Blinc A, Kozak M, et al. Infrapopliteal run-off and the outcome of femoropop-liteal percutaneous transluminal angioplasty. Vasa. 2010;39:159-168.
51. Covidien’s SpiderFX Embolic Protection Device Approved for Use in Lower Extremities. Endovascular Today. http://bmctoday.net/evtoday/2011/11/article.asp?f=covidiens-spider-fx-embolic-protection-device-approved-for-use-in-lower-extremities.
52. Zankar A, Brilakis ES, Banerjee S. Embolic capture angioplasty of lower extremity lesion following distal embolization. Cardiovasc Revasc Med. 2011;12:337-340.
53. Shammas NW. Commentary: balloon angioplasty with built-in embolic protection mech-anism: the dual role of the proteus balloon. J Endovasc Ther. 2012;19:617-619.
Shammas_0913.indd 6 8/20/13 8:26 AM
Vol. 25, Supplement B, 2013 7B
The JETSTREAM Atherectomy System: Addressing The Clinical Challenges
Venkatesh G. Ramaiah, MD, FACS
Peripheral arterial disease (PAD) is a major cause of mor-bidity in the United States, currently affecting 8 to 12 mil-lion Americans.1 During the last 10 years, there has been a paradigm shift away from open surgery toward endovascular therapy. In the United States, the rate of endovascular lower extremity interventions has quadrupled for critical limb isch-emia and doubled for claudicants. This has been accompanied by a reduction in the rate of major amputations and length of hospital stay, despite an increase in the burden of patient comorbidities.2
Endovascular therapy continues to have significant limi-tations. Balloon angioplasty of complex lesions and chronic total occlusions (CTOs) is associated with dissection, perfora-tion, and distal embolization. Stents must be able to with-stand significant biomechanical forces including compression, flexion, and stretching, which may lead to stent fractures, in-stent stenosis, and stent occlusion.3 Atherectomy may provide a viable alternative to the more established treatment strate-gies as we strive to employ a “leave nothing behind strategy.” Atherectomy offers the ability to debulk atherosclerotic plaque with minimal change in vessel diameter4 and reduce the need for subsequent stent placement.5
JETSTREAM TechnologyThe JETSTREAM Atherectomy System (Bayer Health-
Care) is a novel technology indicated for both atherectomy and thrombectomy. The JETSTREAM System’s unique rota-tional design allows it to debulk and evacuate the liberated debris through continuous aspiration. The JETSTREAM System consists of 2 primary components: the console that mounts to a standard IV pole and a sterile, single-use catheter and control pod unit.
ConsoleThe electrically driven console consists of two peristaltic
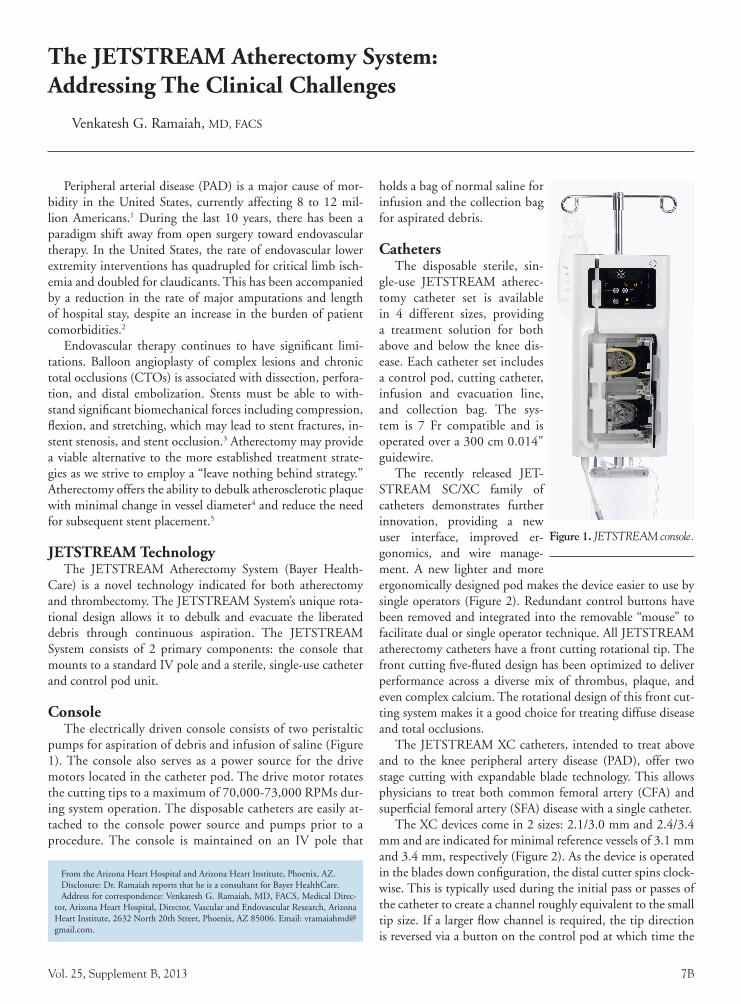
pumps for aspiration of debris and infusion of saline (Figure 1). The console also serves as a power source for the drive motors located in the catheter pod. The drive motor rotates the cutting tips to a maximum of 70,000-73,000 RPMs dur-ing system operation. The disposable catheters are easily at-tached to the console power source and pumps prior to a procedure. The console is maintained on an IV pole that
holds a bag of normal saline for infusion and the collection bag for aspirated debris.
CathetersThe disposable sterile, sin-
gle-use JETSTREAM atherec-tomy catheter set is available in 4 different sizes, providing a treatment solution for both above and below the knee dis-ease. Each catheter set includes a control pod, cutting catheter, infusion and evacuation line, and collection bag. The sys-tem is 7 Fr compatible and is operated over a 300 cm 0.014" guidewire.
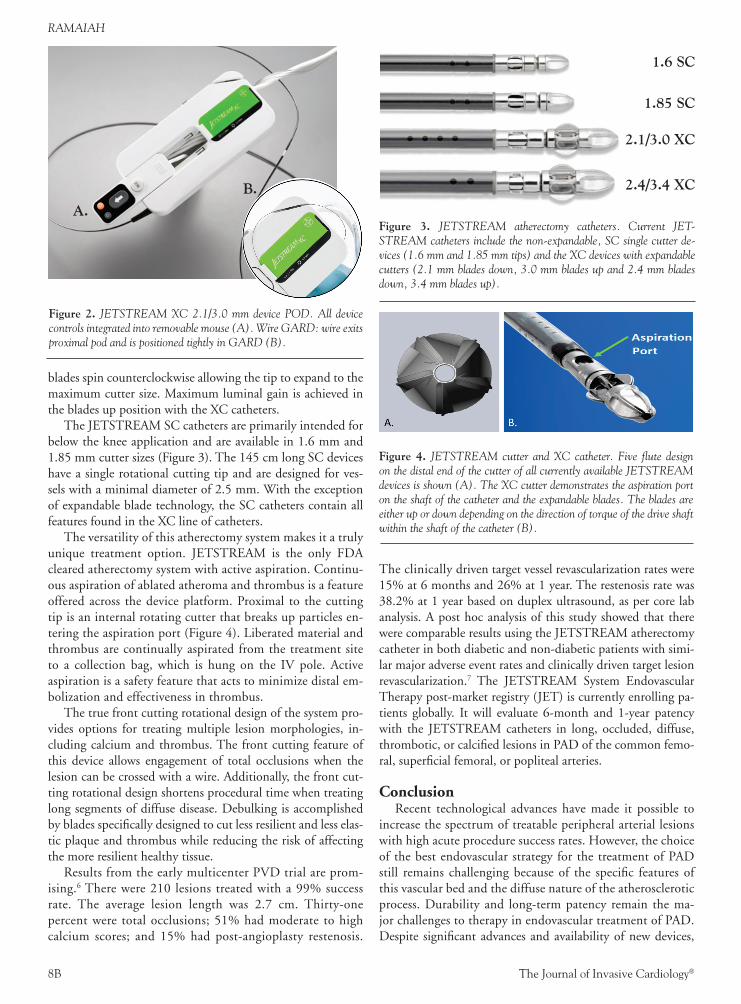
The recently released JET-STREAM SC/XC family of catheters demonstrates further innovation, providing a new user interface, improved er-gonomics, and wire manage-ment. A new lighter and more ergonomically designed pod makes the device easier to use by single operators (Figure 2). Redundant control buttons have been removed and integrated into the removable “mouse” to facilitate dual or single operator technique. All JETSTREAM atherectomy catheters have a front cutting rotational tip. The front cutting five-fluted design has been optimized to deliver performance across a diverse mix of thrombus, plaque, and even complex calcium. The rotational design of this front cut-ting system makes it a good choice for treating diffuse disease and total occlusions.
The JETSTREAM XC catheters, intended to treat above and to the knee peripheral artery disease (PAD), offer two stage cutting with expandable blade technology. This allows physicians to treat both common femoral artery (CFA) and superficial femoral artery (SFA) disease with a single catheter.
The XC devices come in 2 sizes: 2.1/3.0 mm and 2.4/3.4 mm and are indicated for minimal reference vessels of 3.1 mm and 3.4 mm, respectively (Figure 2). As the device is operated in the blades down configuration, the distal cutter spins clock-wise. This is typically used during the initial pass or passes of the catheter to create a channel roughly equivalent to the small tip size. If a larger flow channel is required, the tip direction is reversed via a button on the control pod at which time the
From the Arizona Heart Hospital and Arizona Heart Institute, Phoenix, AZ.Disclosure: Dr. Ramaiah reports that he is a consultant for Bayer HealthCare.Address for correspondence: Venkatesh G. Ramaiah, MD, FACS, Medical Direc-
tor, Arizona Heart Hospital, Director, Vascular and Endovascular Research, Arizona Heart Institute, 2632 North 20th Street, Phoenix, AZ 85006. Email: [email protected].
Figure 1. JETSTREAM console.
Ramaiah_0913.indd 7 8/22/13 8:49 AM
8B The Journal of Invasive Cardiology®
RAMAIAH
blades spin counterclockwise allowing the tip to expand to the maximum cutter size. Maximum luminal gain is achieved in the blades up position with the XC catheters.
The JETSTREAM SC catheters are primarily intended for below the knee application and are available in 1.6 mm and 1.85 mm cutter sizes (Figure 3). The 145 cm long SC devices have a single rotational cutting tip and are designed for ves-sels with a minimal diameter of 2.5 mm. With the exception of expandable blade technology, the SC catheters contain all features found in the XC line of catheters.
The versatility of this atherectomy system makes it a truly unique treatment option. JETSTREAM is the only FDA cleared atherectomy system with active aspiration. Continu-ous aspiration of ablated atheroma and thrombus is a feature offered across the device platform. Proximal to the cutting tip is an internal rotating cutter that breaks up particles en-tering the aspiration port (Figure 4). Liberated material and thrombus are continually aspirated from the treatment site to a collection bag, which is hung on the IV pole. Active aspiration is a safety feature that acts to minimize distal em-bolization and effectiveness in thrombus.
The true front cutting rotational design of the system pro-vides options for treating multiple lesion morphologies, in-cluding calcium and thrombus. The front cutting feature of this device allows engagement of total occlusions when the lesion can be crossed with a wire. Additionally, the front cut-ting rotational design shortens procedural time when treating long segments of diffuse disease. Debulking is accomplished by blades specifically designed to cut less resilient and less elas-tic plaque and thrombus while reducing the risk of affecting the more resilient healthy tissue.
Results from the early multicenter PVD trial are prom-ising.6 There were 210 lesions treated with a 99% success rate. The average lesion length was 2.7 cm. Thirty-one percent were total occlusions; 51% had moderate to high calcium scores; and 15% had post-angioplasty restenosis.
The clinically driven target vessel revascularization rates were 15% at 6 months and 26% at 1 year. The restenosis rate was 38.2% at 1 year based on duplex ultrasound, as per core lab analysis. A post hoc analysis of this study showed that there were comparable results using the JETSTREAM atherectomy catheter in both diabetic and non-diabetic patients with simi-lar major adverse event rates and clinically driven target lesion revascularization.7 The JETSTREAM System Endovascular Therapy post-market registry (JET) is currently enrolling pa-tients globally. It will evaluate 6-month and 1-year patency with the JETSTREAM catheters in long, occluded, diffuse, thrombotic, or calcified lesions in PAD of the common femo-ral, superficial femoral, or popliteal arteries.
ConclusionRecent technological advances have made it possible to
increase the spectrum of treatable peripheral arterial lesions with high acute procedure success rates. However, the choice of the best endovascular strategy for the treatment of PAD still remains challenging because of the specific features of this vascular bed and the diffuse nature of the atherosclerotic process. Durability and long-term patency remain the ma-jor challenges to therapy in endovascular treatment of PAD. Despite significant advances and availability of new devices,
Figure 2. JETSTREAM XC 2.1/3.0 mm device POD. All device controls integrated into removable mouse (A). Wire GARD: wire exits proximal pod and is positioned tightly in GARD (B).
A.
B.
Figure 3. JETSTREAM atherectomy catheters. Current JET-STREAM catheters include the non-expandable, SC single cutter de-vices (1.6 mm and 1.85 mm tips) and the XC devices with expandable cutters (2.1 mm blades down, 3.0 mm blades up and 2.4 mm blades down, 3.4 mm blades up).
1.6 SC
1.85 SC
2.1/3.0 XC
2.4/3.4 XC
Figure 4. JETSTREAM cutter and XC catheter. Five flute design on the distal end of the cutter of all currently available JETSTREAM devices is shown (A). The XC cutter demonstrates the aspiration port on the shaft of the catheter and the expandable blades. The blades are either up or down depending on the direction of torque of the drive shaft within the shaft of the catheter (B).
Ramaiah_0913.indd 8 8/20/13 9:20 AM

Vol. 25, Supplement B, 2013 9B
The JETSTREAM Atherectomy System: Addressing The Clinical Challenges
the principal failure continues to be recurrent restenosis. The role of atherectomy may be to overcome the limitation of bal-loon angioplasty and stent placement. A number of debulking modalities and devices are now available with good procedural results. Long-term outcomes need to be addressed by large, randomized trials.
The JETSTREAM System is an innovative peripheral revascularization platform designed to restore flow through many types of plaque morphologies encountered in PAD. Of-fering a range of sizes to treat vessels above and below the knee, this unique technology offers features that provide effective atherectomy in difficult arterial obstructions while preserving options for further treatment. The JETSTREAM System gives physicians a powerful tool to help fight PAD.
References1. Fowkes FG, Murray GD, Butcher I, et al. Ankle brachial index combined with Framing-
ham Risk Score to predict cardiovascular events and mortality: a meta-analysis. JAMA. 2008;300(2):197-208.
2. Egorova NN, Guillerme S, Gelijns A, et al. An analysis of the outcomes of a decade of experience with lower extremity revascularization including limb salvage, lengths of stay, and safety. J Vasc Surg. 2010;51(4):878-885.
3. Scheinert D, Scheinert S, Sax J, et al. Prevalence and clinical impact of stent fractures after femoropopliteal stenting. J Am Coll Cardiol. 2005;45(2):312-315.
4. Hassan AH, Ako J, Waseda K, et al. Mechanism of lumen gain with a novel rotational aspiration atherectomy system for peripheral arterial disease: examination by intravascular ultrasound. Cardiovasc Revasc Med. 2010;11(3):155-158.
5. Shammas NW, Coiner D, Shammas GA, Dippel EJ, Christensen L, Jerin M. Percutaneous lower-extremity arterial interventions with primary balloon angioplasty versus SilverHawk atherectomy and adjunctive balloon angioplasty: randomized trial. J Vasc Interv Radiol. 2011;22(9):1223-1228.
6. Zeller T, Krankenberg H, Steinkamp H, et al. One-year outcome of percutaneous rota-tional atherectomy with aspiration in infrainguinal peripheral arterial occlusive disease: the multicenter pathway PVD trial. J Endovasc Ther. 2009;16(6):653-662.
Ramaiah_0913.indd 9 8/22/13 8:50 AM

10B The Journal of Invasive Cardiology®
Tips for Success with JETSTREAM Atherectomy System
Thomas Davis, MD
PAD is a complex and challenging disease state. As tools continue to improve, we are able to treat increasingly complex disease. As interventionalists, our objectives are to restore flow, improve symptoms, and ultimately save limbs. My objective is to accomplish all of the above with hopes to preserve my future treatment options with my PAD patients. Therefore, we reserve stent use as a bailout strategy to keep all future treatment options open at my institution. We employ debulk-ing PAD with atherectomy as a front line treatment strategy to accomplish this endpoint.
The JETSTREAM Atherectomy System (Bayer Health-Care) has rapidly evolved into a versatile tool in our treat-ment armamentarium for PAD. In 2008, the FDA cleared the first generation JETSTREAM device for atherectomy of peripheral vasculature and in 2009, an indication for throm-bectomy of upper and lower extremity peripheral arteries was added. Since the initial product clearance, rapid evolu-tion of the technology has resulted in seven new product introductions, the most recent being the JETSTREAM SC/XC family. The new catheters have a lighter control POD, simplified user interface, and a removable control mouse, which potentially reduces radiation exposure. Additionally, the new wire management GARD simplifies wire manage-ment during the case.
Clinical Sweet SpotsIn our laboratory we use all commercially available ather-
ectomy devices as we believe each have their own unique strengths and no single device is right for every case. The strengths of JETSTREAM technology are in its ability to manage mixed morphology lesions. The JETSTREAM Sys-tem is our product of choice for total occlusions and dif-fuse disease from the common femoral artery through the popliteal because it allows front cutting and active aspira-tion. Total occlusions are typically composed of mixed mor-phology of disease (thrombus, calcium, and plaque) and the ability to both debulk and remove the liberated material is very important. Particulate matter (mobile plaque elements) within the target vessel have significant thromboembolic risk. Aspiration of these mobile elements has implicit value, and technique management should help mitigate the risks associated with JETSTREAM usage. The only prerequisite
to using this device is being able to cross the lesion with a 0.014" wire. Typically I will cross with a crossing assist de-vice to avoid sub-adventitial areas, which allows the device to make direct contact with the plaque rather than through a sub-adventitial space.
We also typically use JETSTREAM Atherectomy in long segments of diffuse disease. The rotational front cutting technology effectively prepares lesions for definitive therapy and minimizes fluoroscopy and procedural times. As dem-onstrated in the Calcium Study, JETSTREAM atherectomy remodels luminal irregularities and delivers a statistically sig-nificant improvement in luminal symmetry.1 The improved luminal symmetry better facilitates balloon angioplasty as balloon-to-vessel wall apposition is markedly improved when the luminal space is symmetric.
WiresJETSTREAM is an over-the-wire system and requires a
300 cm 0.014" guidewire for delivery. Because the mecha-nism of action is high speed rotation (70,000-73,000 RPM), this device should only be used over approved wires. The JETSTREAM JETWIRE (Bayer HealthCare) was specifically manufactured for use with the JETSTREAM Atherectomy System and performs quite well. In addition to the JETWIRE, a list of compatible wires is included in the device instructions for use. A supportive wire is needed to allow lesion engage-ment with the front cutting technology. Never attempt to in-sert or operate the device over a bent or kinked wire because it causes poor tracking over the wire and can lead to loss of distal
From the division of Cardiovascular Disease, Department of Internal Medicine, St. John Hospital and Medical Center, Detroit, MI.
Disclosure: Dr. Davis reports that he owns stock in Avinger. He is also on the advisory board for Bayer HealthCare and Bard.
Address for correspondence: Thomas Davis, MD, Director of the Cardiac Cath-eterization Lab and Director of Peripheral Interventions and Disease, St. John Hospi-tal and Medical Center, 22101 Moross Road, Detroit, MI 48236. Email: [email protected].
Figure 1. Wire in GARD with tight loop.
Davis_0913.indd 10 8/20/13 9:24 AM
Vol. 25, Supplement B, 2013 11B
Tips for Success with JETSTREAM Atherectomy System
wire placement when taking the device out after use. It is bet-ter to replace a compromised wire at the beginning of the pro-cedure rather than struggling to re-cross after the initial passes.
Wire Management Wire management during the case is an important and of-
ten overlooked operator responsibility. The device has a wire GARD that prevents the wire from rotating during operation. Once the lesion has been wired, the device is front loaded onto the wire. The wire exits the POD on the back end and should be inserted into the wire GARD forming a tight loop (Figure 1). As the device operates over the wire, the wire loop should grow if the guidewire is effectively anchored distally. If the loop fails to grow you can assume the wire is moving distally with the device. Distal wire movement is the result of inad-equate wire parking. You should always strive to position your wire in the deepest possible distal position.
JETSTREAM ProcedureProcedural technique is the most important driver of suc-
cess with the JETSTREAM atherectomy catheters. Main-taining discipline in the catheter advancement speed is im-perative. The recommendation is 1 mm/second. Initially you may want to use radiopaque tape to help gauge your speed. We found that slow forward advancement followed by subtle pullback improves both the cutting and aspiration efficiency. Not to be confused with a pecking motion, the desired tech-nique is analogous with one step forward—two steps back. Adhering to this technique allows the device to aspirate the liberated debris. This technique is equally important despite the lesion morphology (ie, thrombus, soft plaque, fibrous tis-sue, or calcium). It is common to advance the catheter too fast, but doing so may overwhelm the aspiration capability or stall the catheter.
In addition to the high-level guidance of 1 mm/second, the most important information you should use to guide cath-eter advancement is the auditory and tactile feedback from the
device. The auditory feedback comes from the device motor and the objective is to maintain constant or near constant mo-tor sounds. As the device engages lesion composed of calcium and hard plaque, you will typically hear the motor slow as it manages through the disease. This is less true with soft plaque and thrombus so in these morphology types the 1 mm/second advancement speed is imperative. Tactile feedback is transmit-ted through the catheter as it is advanced across the lesion. In more stubborn disease (hard plaque/calcium), the disease typically will not allow you to go too quickly. Table 1 provides a list of catheter advancement tips.
Blades up or Blades downThe JETSTREAM XC catheters have expandable blades al-
lowing treatment of multilevel disease with one device. The ini-tial passes across a lesion should be down in the “blades-down” or minimum tip configuration. Two blades down passes are recommended. Verbal and auditory feedback from the system will indicate when the lesion is prepped for blades up con-figuration. “Blades-up” should be performed from proximal to distal across the lesion. Generally, two passes will adequately debulk the lesion. Similar to the blades down configuration, the auditory and tactile feedback will indicate when debulking is complete.
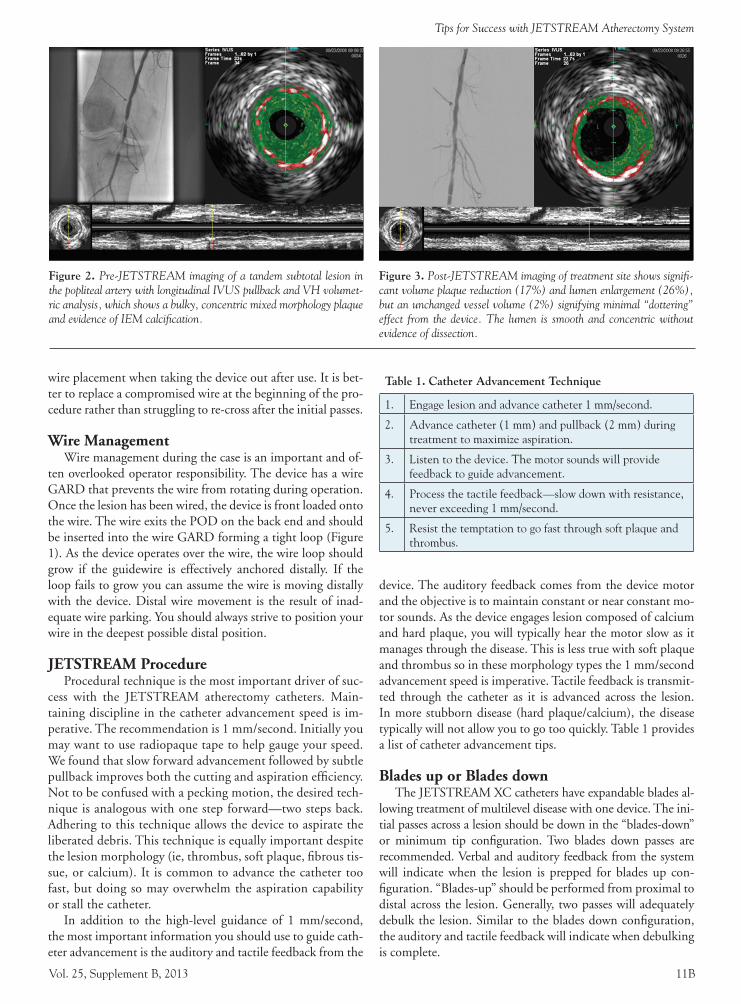
Figure 2. Pre-JETSTREAM imaging of a tandem subtotal lesion in the popliteal artery with longitudinal IVUS pullback and VH volumet-ric analysis, which shows a bulky, concentric mixed morphology plaque and evidence of IEM calcification.
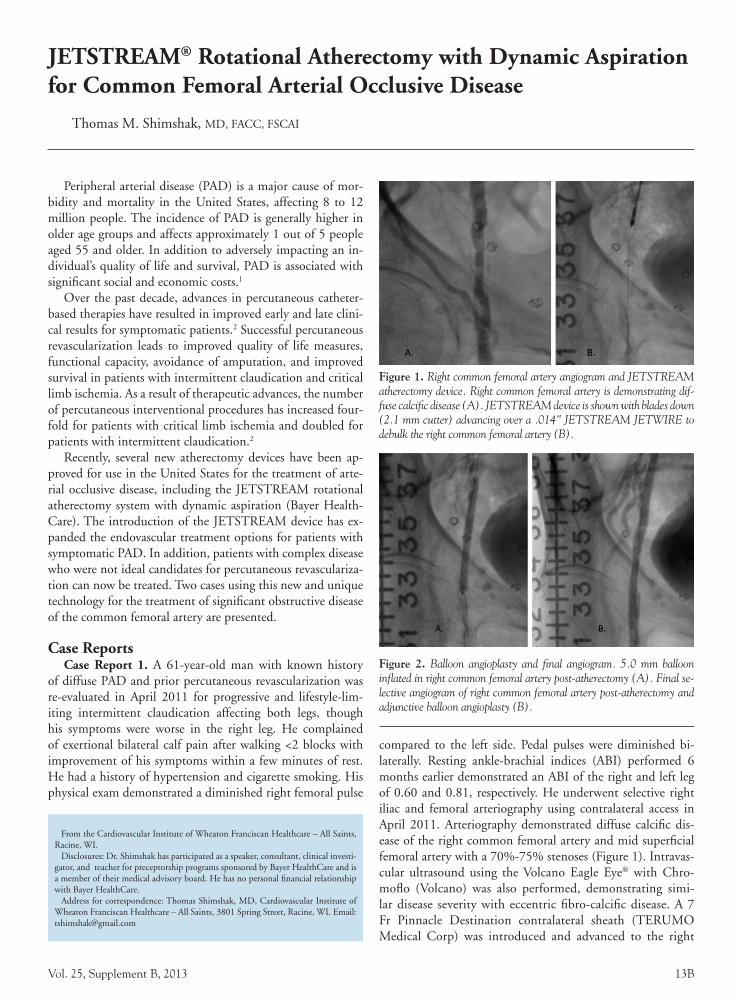
Figure 3. Post-JETSTREAM imaging of treatment site shows signifi-cant volume plaque reduction (17%) and lumen enlargement (26%), but an unchanged vessel volume (2%) signifying minimal “dottering” effect from the device. The lumen is smooth and concentric without evidence of dissection.
Table 1. Catheter Advancement Technique
1. Engage lesion and advance catheter 1 mm/second.
2. Advance catheter (1 mm) and pullback (2 mm) during treatment to maximize aspiration.
3. Listen to the device. The motor sounds will provide feedback to guide advancement.
4. Process the tactile feedback—slow down with resistance, never exceeding 1 mm/second.
5. Resist the temptation to go fast through soft plaque and thrombus.
Davis_0913.indd 11 8/22/13 8:50 AM

12B The Journal of Invasive Cardiology®
DAVIS
AspirationThe unique active aspiration feature on the JETSTREAM
family of products makes this product a great choice in total occlusions and mixed morphology lesions. On rare occasion the device may lose aspiration, which is most typically the result of overwhelming the aspiration and quick advancement during ac-tive treatment. It is also important to note that aspiration works, albeit not at as high a flow, during REX mode too.
The following tips will optimize aspiration performance: Long segments of diffuse disease, total occlusions, and heavy thrombotic lesions may pose a challenge to the aspiration ca-pability of the device, which may be mitigated by operator technique. Catheter advance technique is again paramount to the discussion. To allow the aspiration to remove the in-fused saline and debris, the operator must use 1 mm/second of forward movement with slight pullback following each step forward. Remember the auditory feedback will be limited in this setting as soft plaque and thrombus will have minimal impact on the device’s motor speed. In this setting you must be disciplined and allow the device time to work.
EmbolizationEmbolization is a potential risk in all interventional pro-
cedures. The published literature and our personal experience do not suggest the risk is any higher with this device than other competitive technologies. As discussed in this manu-script optimal performance of this device is contingent upon proper user technique. Though not guaranteed, risk of distal embolization with this atherectomy device can be comparable to other interventional procedures if you are disciplined with regard to technique.
SummaryAtherectomy is evolving as an acceptable treatment option
for peripheral arterial disease. While the newest entrant to the field, the JETSTREAM System has quickly evolved into a useful tool in the battle against this debilitating disease. The set of features on this product uniquely differentiates it from competitive devices and fills a clinical void. Though the device necessitates a specific technique, it is well worth developing. As technology and techniques continue to evolve so will the results we are able to deliver.
Davis_0913.indd 12 8/20/13 9:24 AM
Vol. 25, Supplement B, 2013 13B
JETSTREAM® Rotational Atherectomy with Dynamic Aspiration for Common Femoral Arterial Occlusive Disease
Thomas M. Shimshak, MD, FACC, FSCAI
Peripheral arterial disease (PAD) is a major cause of mor-bidity and mortality in the United States, affecting 8 to 12 million people. The incidence of PAD is generally higher in older age groups and affects approximately 1 out of 5 people aged 55 and older. In addition to adversely impacting an in-dividual’s quality of life and survival, PAD is associated with significant social and economic costs.1
Over the past decade, advances in percutaneous catheter-based therapies have resulted in improved early and late clini-cal results for symptomatic patients.2 Successful percutaneous revascularization leads to improved quality of life measures, functional capacity, avoidance of amputation, and improved survival in patients with intermittent claudication and critical limb ischemia. As a result of therapeutic advances, the number of percutaneous interventional procedures has increased four-fold for patients with critical limb ischemia and doubled for patients with intermittent claudication.2
Recently, several new atherectomy devices have been ap-proved for use in the United States for the treatment of arte-rial occlusive disease, including the JETSTREAM rotational atherectomy system with dynamic aspiration (Bayer Health-Care). The introduction of the JETSTREAM device has ex-panded the endovascular treatment options for patients with symptomatic PAD. In addition, patients with complex disease who were not ideal candidates for percutaneous revasculariza-tion can now be treated. Two cases using this new and unique technology for the treatment of significant obstructive disease of the common femoral artery are presented.
Case ReportsCase Report 1. A 61-year-old man with known history
of diffuse PAD and prior percutaneous revascularization was re-evaluated in April 2011 for progressive and lifestyle-lim-iting intermittent claudication affecting both legs, though his symptoms were worse in the right leg. He complained of exertional bilateral calf pain after walking <2 blocks with improvement of his symptoms within a few minutes of rest. He had a history of hypertension and cigarette smoking. His physical exam demonstrated a diminished right femoral pulse
compared to the left side. Pedal pulses were diminished bi-laterally. Resting ankle-brachial indices (ABI) performed 6 months earlier demonstrated an ABI of the right and left leg of 0.60 and 0.81, respectively. He underwent selective right iliac and femoral arteriography using contralateral access in April 2011. Arteriography demonstrated diffuse calcific dis-ease of the right common femoral artery and mid superficial femoral artery with a 70%-75% stenoses (Figure 1). Intravas-cular ultrasound using the Volcano Eagle Eye® with Chro-moflo (Volcano) was also performed, demonstrating simi-lar disease severity with eccentric fibro-calcific disease. A 7 Fr Pinnacle Destination contralateral sheath (TERUMO Medical Corp) was introduced and advanced to the right
From the Cardiovascular Institute of Wheaton Franciscan Healthcare – All Saints, Racine, WI.
Disclosures: Dr. Shimshak has participated as a speaker, consultant, clinical investi-gator, and teacher for preceptorship programs sponsored by Bayer HealthCare and is a member of their medical advisory board. He has no personal financial relationship with Bayer HealthCare.
Address for correspondence: Thomas Shimshak, MD, Cardiovascular Institute of Wheaton Franciscan Healthcare – All Saints, 3801 Spring Street, Racine, WI. Email: [email protected]
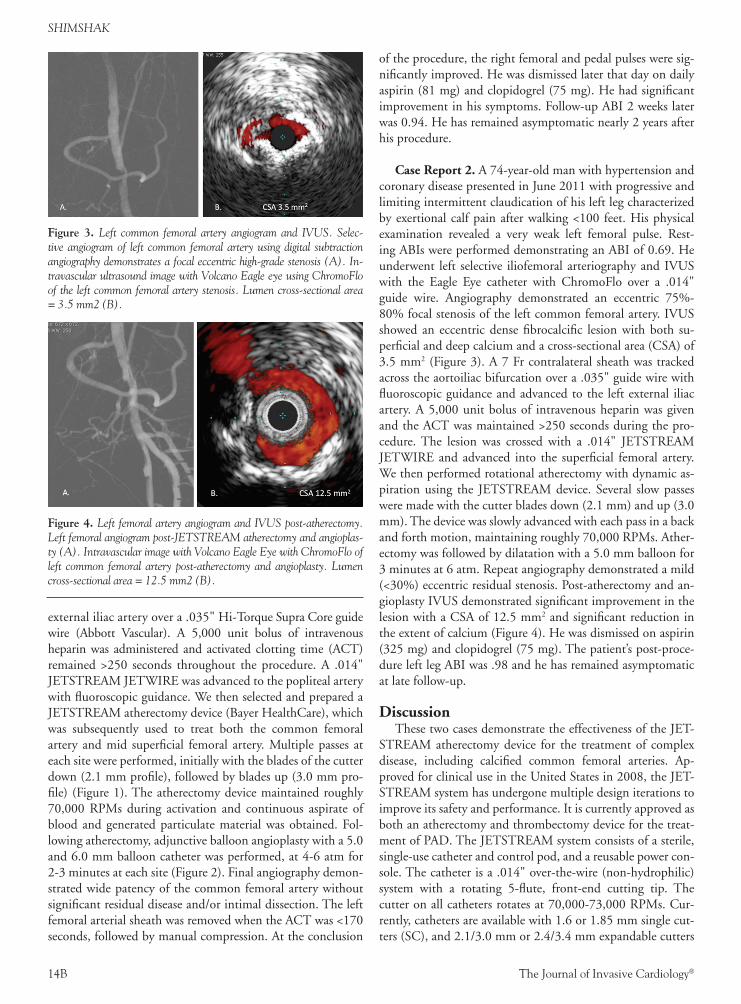
Figure 1. Right common femoral artery angiogram and JETSTREAM atherectomy device. Right common femoral artery is demonstrating dif-fuse calcific disease (A). JETSTREAM device is shown with blades down (2.1 mm cutter) advancing over a .014" JETSTREAM JETWIRE to debulk the right common femoral artery (B).
Figure 2. Balloon angioplasty and final angiogram. 5.0 mm balloon inflated in right common femoral artery post-atherectomy (A). Final se-lective angiogram of right common femoral artery post-atherectomy and adjunctive balloon angioplasty (B).
Shimshak_0913.indd 13 8/22/13 8:51 AM
14B The Journal of Invasive Cardiology®
SHIMSHAK
external iliac artery over a .035" Hi-Torque Supra Core guide wire (Abbott Vascular). A 5,000 unit bolus of intravenous heparin was administered and activated clotting time (ACT) remained >250 seconds throughout the procedure. A .014" JETSTREAM JETWIRE was advanced to the popliteal artery with fluoroscopic guidance. We then selected and prepared a JETSTREAM atherectomy device (Bayer HealthCare), which was subsequently used to treat both the common femoral artery and mid superficial femoral artery. Multiple passes at each site were performed, initially with the blades of the cutter down (2.1 mm profile), followed by blades up (3.0 mm pro-file) (Figure 1). The atherectomy device maintained roughly 70,000 RPMs during activation and continuous aspirate of blood and generated particulate material was obtained. Fol-lowing atherectomy, adjunctive balloon angioplasty with a 5.0 and 6.0 mm balloon catheter was performed, at 4-6 atm for 2-3 minutes at each site (Figure 2). Final angiography demon-strated wide patency of the common femoral artery without significant residual disease and/or intimal dissection. The left femoral arterial sheath was removed when the ACT was <170 seconds, followed by manual compression. At the conclusion
of the procedure, the right femoral and pedal pulses were sig-nificantly improved. He was dismissed later that day on daily aspirin (81 mg) and clopidogrel (75 mg). He had significant improvement in his symptoms. Follow-up ABI 2 weeks later was 0.94. He has remained asymptomatic nearly 2 years after his procedure.
Case Report 2. A 74-year-old man with hypertension and coronary disease presented in June 2011 with progressive and limiting intermittent claudication of his left leg characterized by exertional calf pain after walking <100 feet. His physical examination revealed a very weak left femoral pulse. Rest-ing ABIs were performed demonstrating an ABI of 0.69. He underwent left selective iliofemoral arteriography and IVUS with the Eagle Eye catheter with ChromoFlo over a .014" guide wire. Angiography demonstrated an eccentric 75%-80% focal stenosis of the left common femoral artery. IVUS showed an eccentric dense fibrocalcific lesion with both su-perficial and deep calcium and a cross-sectional area (CSA) of 3.5 mm2 (Figure 3). A 7 Fr contralateral sheath was tracked across the aortoiliac bifurcation over a .035" guide wire with fluoroscopic guidance and advanced to the left external iliac artery. A 5,000 unit bolus of intravenous heparin was given and the ACT was maintained >250 seconds during the pro-cedure. The lesion was crossed with a .014" JETSTREAM JETWIRE and advanced into the superficial femoral artery. We then performed rotational atherectomy with dynamic as-piration using the JETSTREAM device. Several slow passes were made with the cutter blades down (2.1 mm) and up (3.0 mm). The device was slowly advanced with each pass in a back and forth motion, maintaining roughly 70,000 RPMs. Ather-ectomy was followed by dilatation with a 5.0 mm balloon for 3 minutes at 6 atm. Repeat angiography demonstrated a mild (<30%) eccentric residual stenosis. Post-atherectomy and an-gioplasty IVUS demonstrated significant improvement in the lesion with a CSA of 12.5 mm2 and significant reduction in the extent of calcium (Figure 4). He was dismissed on aspirin (325 mg) and clopidogrel (75 mg). The patient’s post-proce-dure left leg ABI was .98 and he has remained asymptomatic at late follow-up.
Discussion These two cases demonstrate the effectiveness of the JET-
STREAM atherectomy device for the treatment of complex disease, including calcified common femoral arteries. Ap-proved for clinical use in the United States in 2008, the JET-STREAM system has undergone multiple design iterations to improve its safety and performance. It is currently approved as both an atherectomy and thrombectomy device for the treat-ment of PAD. The JETSTREAM system consists of a sterile, single-use catheter and control pod, and a reusable power con-sole. The catheter is a .014" over-the-wire (non-hydrophilic) system with a rotating 5-flute, front-end cutting tip. The cutter on all catheters rotates at 70,000-73,000 RPMs. Cur-rently, catheters are available with 1.6 or 1.85 mm single cut-ters (SC), and 2.1/3.0 mm or 2.4/3.4 mm expandable cutters
Figure 3. Left common femoral artery angiogram and IVUS. Selec-tive angiogram of left common femoral artery using digital subtraction angiography demonstrates a focal eccentric high-grade stenosis (A). In-travascular ultrasound image with Volcano Eagle eye using ChromoFlo of the left common femoral artery stenosis. Lumen cross-sectional area = 3.5 mm2 (B).
Figure 4. Left femoral artery angiogram and IVUS post-atherectomy. Left femoral angiogram post-JETSTREAM atherectomy and angioplas-ty (A). Intravascular image with Volcano Eagle Eye with ChromoFlo of left common femoral artery post-atherectomy and angioplasty. Lumen cross-sectional area = 12.5 mm2 (B).
Shimshak_0913.indd 14 8/20/13 8:30 AM

Vol. 25, Supplement B, 2013 15B
Rotational Atherectomy for CFA Occlusive Disease
(XC). All catheters are compatible with a 7 Fr sheath (Figures 5 and 6). The shaft length is either 120 cm or 135 cm for the XC catheters or 145 cm for the SC small vessel catheters. The device is effective in treating a variety of lesion morphologies including soft, fibrotic, calcified, and/or thrombus. By virtue of its property of differential cutting, the JETSTREAM device preferentially cuts atheromatous disease, while sparing normal tissue. It also incorporates dynamic and continuous aspiration of particulate debris and thrombus, a feature that reduces dis-tal emboli and improves device and procedural safety.
The two case presentations highlight the performance at-tributes of this unique atherectomy device in complex calci-fied common femoral artery disease. Historically, endovas-cular therapy for common femoral artery disease has been controversial and technically challenging due to its location and potentially excessive, rigid associated calcium. The in-troduction of this device and other atherectomy devices have enhanced endovascular procedural safety and efficacy for complex lesion and vessel subset.3,4,5 In the two cases pre-sented, the JETSTREAM device combined with IVUS and adjunctive balloon angioplasty allowed us to effectively treat two heavily calcified common femoral arteries. In the second case, IVUS demonstrated an increase in CSA from 3.5 mm2
pre-intervention to 12.5 mm2 post-intervention. This final CSA is much larger than the predicted result from the cutter alone (7.07 mm2) and represents the combined effect of the rotational cutter and plaque atherectomy, dynamic aspiration, and final balloon dilatation. IVUS demonstrated significant removal of calcium as well.
Similar results have recently been reported from the JET-STREAM Calcium Removal Study.6 In this prospective, single-arm, multicenter study, the JETSTREAM device was evaluated for its effectiveness in removing moderate and se-vere calcium in the peripheral arteries based on IVUS criteria. Lesion location was either the common or superficial femoral arteries in 81% of cases, of which 33% had moderate calcifica-tion and 67% had severe calcification by angiography. Based on IVUS evaluation, total lesion length was 44±35 mm; max-imum arc of calcium was 149±82°. Area stenosis decreased from 61.8±19.7% to 38.5±19.6% (p<0.0002), minimum lumen area increased from 6.6±3.7 mm2 to 10.0±3.6 mm2 (p=0.0001). Calcium reduction resulted in a 78±27% increase in lumen area. Although the arc of superficial calcium did not change significantly in this small series, the arc of reverbera-tion did increase significantly (21±20° to 69±71°, p=0.0006), indicating favorable device-related alteration in lesion cal-cium. These changes in lesion characteristics using the JET-STREAM device occurred without any adverse clinical events.
Although the JETSTREAM System has proven efficacy as an atherectomy and thrombectomy device in infra-inguinal PAD, its role as either stand alone or in combination with other therapies (including angioplasty, stenting, and/or drug-eluting balloons) remains to be determined. Future clinical trials in this country and outside of the US will help clarify how this technology will be integrated into the endovascular therapeutic armamentarium.
References1. Fowkes FG, Murray GD, Butcher I, et al. Ankle brachial index combined with
Framingham Risk Score to predict cardiovascular events and mortality: a meta-analysis. JAMA. 2008;300:197-208.
2. Egorova NN, Guillerme S, Gelijns A, et al. An analysis of the outcomes of a decade of experience with lower extremity revascularization including limb salvage, lengths of stay, and safety. J Vasc Surg. 2010;51:878-885.
3. Hassan AH, Ako J, Waseda K, et al. Mechanism of lumen gain with a novel atherec-tomy system for peripheral arterial disease: examination by intravascular ultrasound. Cardiovasc Revasc Med. 2010;11:155-158.
4. Garcia L, Zeller T, McKinsey J, et al. Determination of Effectiveness of Silver-Hawk™/TurboHawk™ Peripheral Plaque Excision System for the Treatment of Infrainguinal Vessels/Lower Extremities Study. Presented at 10th Annual Vascular Interventional Advances (VIVA), October 9-12, 2012.
5. Zeller T, Krankenberg H, Steinkamp H, et al. One-year outcome of percutaneous rotational atherectomy with aspiration in infrainguinal peripheral arterial occlusive disease: the multicenter Pathway PVD Trial. J Endovasc Ther. 2009;16:653-662.
6. JETSTREAM Atherectomy System Can Remove Superficial Calcium in Severely Calcified Peripheral Arteries. Maehara A, Mintz G, Shimshak T, et al. Presented as abstract at 25th ISET. Miami Beach, FL. January 18-23, 2013.
Figure 5. JETSTREAM cutter and XC catheter. Five-flute design on the distal end of the cutter of all currently available JETSTREAM de-vices is shown (A). The XC cutter demonstrates the aspiration port on the shaft of the catheter and the expandable blades. The blades are either up or down depending on the direction of torque of the drive shaft within the shaft of the catheter (B).
Figure 6. JETSTREAM atherectomy catheters. Current JET-STREAM catheters include the fixed, single cutter, small vessel devices (1.6 mm and 1.85 mm cutter), and the expandable XC devices (2.1 mm blades down; 3.0 mm blades up or 2.4 mm blades down;3.4 mm blades up).
Shimshak_0913.indd 15 8/22/13 8:51 AM

LLCan HMP Communications Holdings Company
,™
Copyright © 2013All Rights Reserved.
83 General Warren Blvd. • Suite 100 • Malvern, PA 19355Phone (610) 560-0500 • Fax (610) 560-0501
JETSTREAM® Atherectomy SystemsThe JETSTREAM System is intended for use in atherectomy of the peripheral vasculature and to break apart and remove thrombus from upper and lower extremity peripheral arteries. It is not intended for use in coronary, carotid, iliac or renal vasculature. See prod-uct Information for Use for specific and complete prescribing information.Indications, operating specifications and availability may vary by country. Check with local product representation and country-specific Information For Use for your country. Bayer, JETSTREAM, and JETWIRE are trademarks of the Bayer group of companies. Bayer © 2013
All other trademarks are property of their respective companies.
BackPage_BayerSupplement_0913.indd 1 8/20/13 8:30 AM