journal of cutaneous medicine pyoderma vegetans · case reports pyoderma vegetans anthony j....
TRANSCRIPT

C a s e R e p o r t s
Pyoderma Vegetans
Anthony J. Papadopoulos,1 Robert A. Schwartz,1,2
Rajendra Kapila,3 Joseph A. Samady,1 Zbigniew Ruszczak,1
Babar K. Rao,1 and W. Clark Lambert1,2
Abstract
Background: Pyoderma vegetans is a rare condition that is clinically characterized bylarge verrucous plaques with elevated borders and multiple pustules. The etiology of thisdisorder remains unknown.
Objectives: We describe a 24-year-old woman with rapidly evolving pyoderma veg-etans. Our patient had the unique additional findings of a highly elevated serum IgE leveland a history of hidradenitis suppurativa.
Conclusions: Pyoderma vegetans is diagnosed on clinical and histological criteria. Dif-ferentiation must be made from disorders such as pyoderma gangrenosum, Sweet’s syn-drome, and deep fungal infections. We illustrate a case of pyoderma vegetans and reviewthe literature on this rare disorder. Clinical and histological criteria for diagnosis arepresented, as well as differentiation from some mimicking disorders.
Sommaire
Antecedents: Le pyoderma vegetans est une affection rare qui se caracterise sur le planclinique par de grandes plaques verruqueuses limitees par un bourrelet et de nombreusespustules. L’etiologie de cette affection demeure inconnue.
Objectifs: Decrire le cas d’une jeune femme de 24 ans atteinte de pyoderma vegetansa evolution rapide. La patiente presentait en outre comme signes tout particuliers unenette elevation du taux serique d’IgE et une hidrosadenite axillaire.
Conclusion: Le pyoderma vegetans est diagnostique selon des criteres cliniques ethistologiques. Il doit etre differencie d’affections telles que le pyoderma gangrenosum, lesyndrome de Sweet et les mycoses profondes. Nous presentons ici un cas de pyodermavegetans et procedons a la revue de la litterature portant sur cette affection rare. Lescriteres diagnostiques cliniques et histologiques sont indiques de meme que les caracter-istiques permettant de differencier le pyoderma vegetans de certaines affections qui luiressemblent.
Pyoderma vegetans is a clinically striking eruption ofmultiple pustular ulcerations; it is of possible bacterial
etiology, similar to chancriform pyoderma.1–4 This veg-etating reaction is believed to be due to an immune sys-tem dysfunction or immunosuppressive state. Ulcerative
colitis,5 diffuse T-cell lymphoma,6 and HIV infection7
have all been linked to this condition.
Case Report
A 24-year-old female production supervisor was seen inOctober 1997 complaining of bilateral, ulcerated, pustu-lar lesions on the lower extremities that had been presentfor one year. She was put on a course of ciprofloxacin. Shereturned three weeks later with no improvement and wasadmitted. Wound cultures revealed Pseudomonas aeurogi-nosa; the patient was empirically treated with IV imi-penem-cilastatin and vancomycin. She responded well totherapy and was discharged following a six-day hospital
1Dermatology, New Jersey Medical School, Newark, New Jersey2 Pathology , New Jersey Medical School, Newark, New Jersey3Infectious Diseases, New Jersey Medical School, Newark, New Jersey
Online publication: 17 May 2001
Correspondence to: R. A. Schwartz, MD, Department of Dermatology, NewJersey Medical School, 185 South Orange Avenue, Newark, NJ07103-2714 USA. E-mail: [email protected]
Journal ofCutaneous Medicine
and SurgeryIncorporating Medical and Surgical Dermatology
DOI: 10.1007/s102270000023J Cutan Med Surg 2001; 223–227
223
stay. The patient was then lost to followup. In November1999, she returned complaining of painful pustular andoozing plaques on her left lower extremity of severalweeks’ duration. She was put on a course of ciprofloxacinand amoxocillin clavulanate but did not respond. Pastmedical history included hidradenitis suppurativa andpseudotumor cerebri treated with bilateral optic nervedecompression.
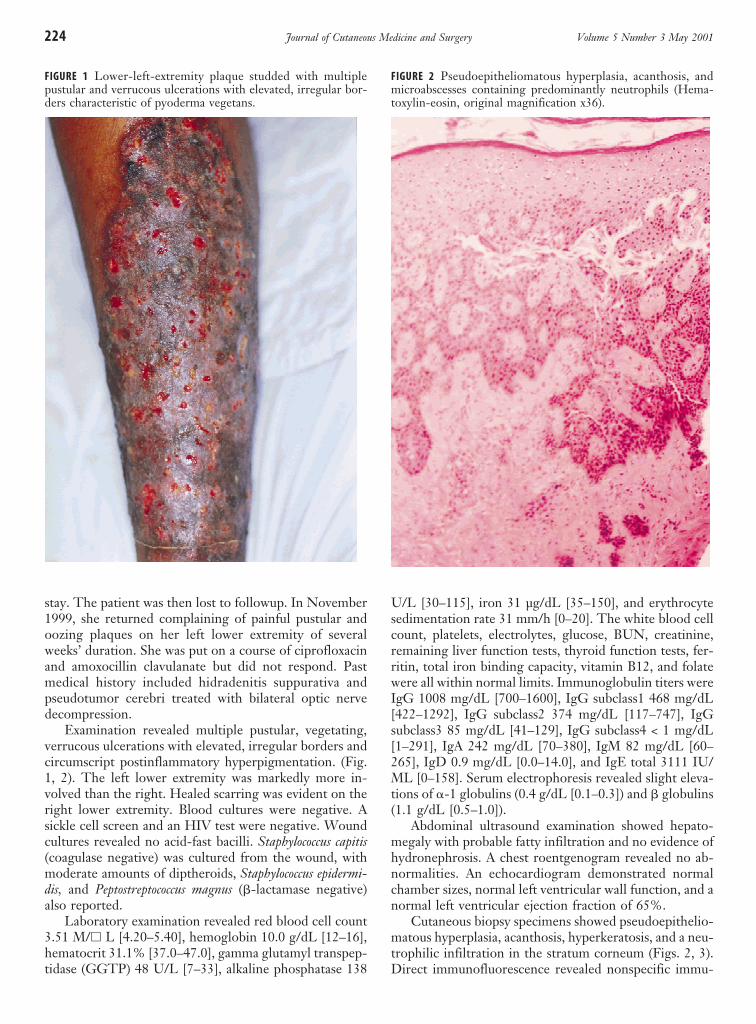
Examination revealed multiple pustular, vegetating,verrucous ulcerations with elevated, irregular borders andcircumscript postinflammatory hyperpigmentation. (Fig.1, 2). The left lower extremity was markedly more in-volved than the right. Healed scarring was evident on theright lower extremity. Blood cultures were negative. Asickle cell screen and an HIV test were negative. Woundcultures revealed no acid-fast bacilli. Staphylococcus capitis(coagulase negative) was cultured from the wound, withmoderate amounts of diptheroids, Staphylococcus epidermi-dis, and Peptostreptococcus magnus (b-lactamase negative)also reported.
Laboratory examination revealed red blood cell count3.51 M/h L [4.20–5.40], hemoglobin 10.0 g/dL [12–16],hematocrit 31.1% [37.0–47.0], gamma glutamyl transpep-tidase (GGTP) 48 U/L [7–33], alkaline phosphatase 138
U/L [30–115], iron 31 µg/dL [35–150], and erythrocytesedimentation rate 31 mm/h [0–20]. The white blood cellcount, platelets, electrolytes, glucose, BUN, creatinine,remaining liver function tests, thyroid function tests, fer-ritin, total iron binding capacity, vitamin B12, and folatewere all within normal limits. Immunoglobulin titers wereIgG 1008 mg/dL [700–1600], IgG subclass1 468 mg/dL[422–1292], IgG subclass2 374 mg/dL [117–747], IgGsubclass3 85 mg/dL [41–129], IgG subclass4 < 1 mg/dL[1–291], IgA 242 mg/dL [70–380], IgM 82 mg/dL [60–265], IgD 0.9 mg/dL [0.0–14.0], and IgE total 3111 IU/ML [0–158]. Serum electrophoresis revealed slight eleva-tions of a-1 globulins (0.4 g/dL [0.1–0.3]) and b globulins(1.1 g/dL [0.5–1.0]).
Abdominal ultrasound examination showed hepato-megaly with probable fatty infiltration and no evidence ofhydronephrosis. A chest roentgenogram revealed no ab-normalities. An echocardiogram demonstrated normalchamber sizes, normal left ventricular wall function, and anormal left ventricular ejection fraction of 65%.
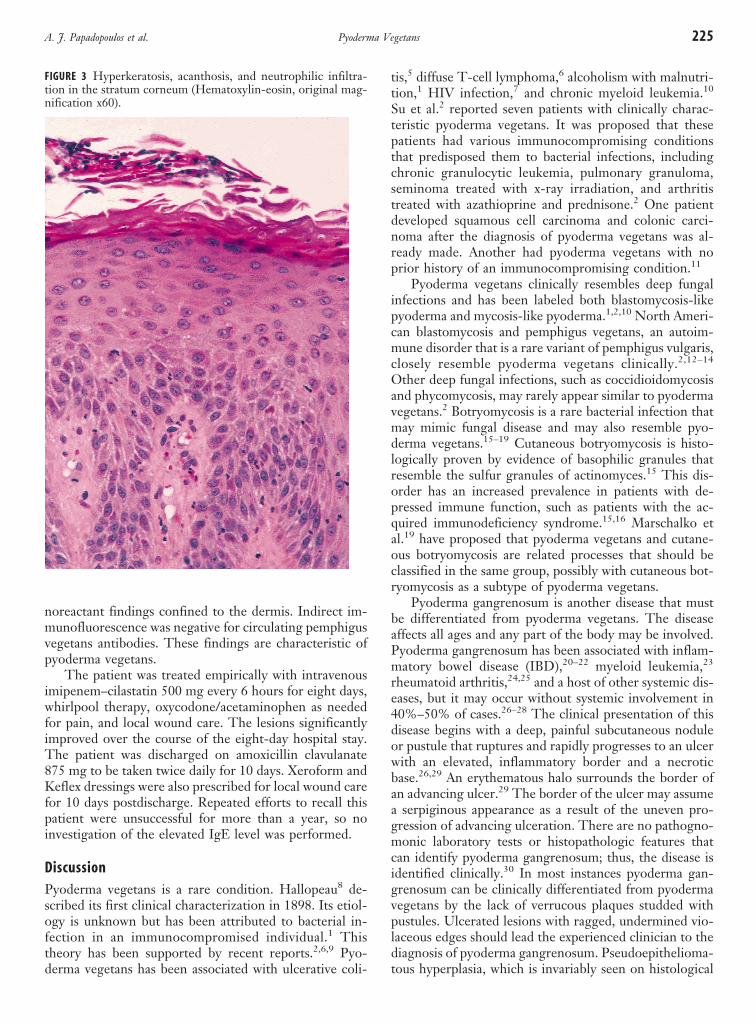
Cutaneous biopsy specimens showed pseudoepithelio-matous hyperplasia, acanthosis, hyperkeratosis, and a neu-trophilic infiltration in the stratum corneum (Figs. 2, 3).Direct immunofluorescence revealed nonspecific immu-
FIGURE 1 Lower-left-extremity plaque studded with multiplepustular and verrucous ulcerations with elevated, irregular bor-ders characteristic of pyoderma vegetans.
FIGURE 2 Pseudoepitheliomatous hyperplasia, acanthosis, andmicroabscesses containing predominantly neutrophils (Hema-toxylin-eosin, original magnification x36).
224 Journal of Cutaneous Medicine and Surgery Volume 5 Number 3 May 2001
noreactant findings confined to the dermis. Indirect im-munofluorescence was negative for circulating pemphigusvegetans antibodies. These findings are characteristic ofpyoderma vegetans.
The patient was treated empirically with intravenousimipenem–cilastatin 500 mg every 6 hours for eight days,whirlpool therapy, oxycodone/acetaminophen as neededfor pain, and local wound care. The lesions significantlyimproved over the course of the eight-day hospital stay.The patient was discharged on amoxicillin clavulanate875 mg to be taken twice daily for 10 days. Xeroform andKeflex dressings were also prescribed for local wound carefor 10 days postdischarge. Repeated efforts to recall thispatient were unsuccessful for more than a year, so noinvestigation of the elevated IgE level was performed.
DiscussionPyoderma vegetans is a rare condition. Hallopeau8 de-scribed its first clinical characterization in 1898. Its etiol-ogy is unknown but has been attributed to bacterial in-fection in an immunocompromised individual.1 Thistheory has been supported by recent reports.2,6,9 Pyo-derma vegetans has been associated with ulcerative coli-
tis,5 diffuse T-cell lymphoma,6 alcoholism with malnutri-tion,1 HIV infection,7 and chronic myeloid leukemia.10
Su et al.2 reported seven patients with clinically charac-teristic pyoderma vegetans. It was proposed that thesepatients had various immunocompromising conditionsthat predisposed them to bacterial infections, includingchronic granulocytic leukemia, pulmonary granuloma,seminoma treated with x-ray irradiation, and arthritistreated with azathioprine and prednisone.2 One patientdeveloped squamous cell carcinoma and colonic carci-noma after the diagnosis of pyoderma vegetans was al-ready made. Another had pyoderma vegetans with noprior history of an immunocompromising condition.11
Pyoderma vegetans clinically resembles deep fungalinfections and has been labeled both blastomycosis-likepyoderma and mycosis-like pyoderma.1,2,10 North Ameri-can blastomycosis and pemphigus vegetans, an autoim-mune disorder that is a rare variant of pemphigus vulgaris,closely resemble pyoderma vegetans clinically.2,12–14
Other deep fungal infections, such as coccidioidomycosisand phycomycosis, may rarely appear similar to pyodermavegetans.2 Botryomycosis is a rare bacterial infection thatmay mimic fungal disease and may also resemble pyo-derma vegetans.15–19 Cutaneous botryomycosis is histo-logically proven by evidence of basophilic granules thatresemble the sulfur granules of actinomyces.15 This dis-order has an increased prevalence in patients with de-pressed immune function, such as patients with the ac-quired immunodeficiency syndrome.15,16 Marschalko etal.19 have proposed that pyoderma vegetans and cutane-ous botryomycosis are related processes that should beclassified in the same group, possibly with cutaneous bot-ryomycosis as a subtype of pyoderma vegetans.
Pyoderma gangrenosum is another disease that mustbe differentiated from pyoderma vegetans. The diseaseaffects all ages and any part of the body may be involved.Pyoderma gangrenosum has been associated with inflam-matory bowel disease (IBD),20–22 myeloid leukemia,23
rheumatoid arthritis,24,25 and a host of other systemic dis-eases, but it may occur without systemic involvement in40%–50% of cases.26–28 The clinical presentation of thisdisease begins with a deep, painful subcutaneous noduleor pustule that ruptures and rapidly progresses to an ulcerwith an elevated, inflammatory border and a necroticbase.26,29 An erythematous halo surrounds the border ofan advancing ulcer.29 The border of the ulcer may assumea serpiginous appearance as a result of the uneven pro-gression of advancing ulceration. There are no pathogno-monic laboratory tests or histopathologic features thatcan identify pyoderma gangrenosum; thus, the disease isidentified clinically.30 In most instances pyoderma gan-grenosum can be clinically differentiated from pyodermavegetans by the lack of verrucous plaques studded withpustules. Ulcerated lesions with ragged, undermined vio-laceous edges should lead the experienced clinician to thediagnosis of pyoderma gangrenosum. Pseudoepithelioma-tous hyperplasia, which is invariably seen on histological
FIGURE 3 Hyperkeratosis, acanthosis, and neutrophilic infiltra-tion in the stratum corneum (Hematoxylin-eosin, original mag-nification x60).
225Pyoderma VegetansA. J. Papadopoulos et al.

examination of pyoderma vegetans, may or may not bepresent in pyoderma gangrenosum.2 A variant of pyo-derma gangrenosum, labeled superficial granulomatouspyoderma, presents as a verrucous, vegetative lesion orulcer, usually as solitary lesions on the back.31 This rarevariant may be confused with pyoderma vegetans. Ab-scess/granuloma formation and plasmacytosis are twomain histological features of this rare variant of pyodermagangrenosum.31 Culture of the lesions for bacteria, my-cobacteria, and fungi are negative, an important distin-guishing factor from pyoderma vegetans in which positivewound cultures are present.2,31
Acute febrile neutrophilic dematosis, or Sweet’s syn-drome, must also be differentiated from pyoderma veg-etans. There is no known etiology for Sweet’s syndrome.An association with malignancy has been established;roughly 1 in 5 cases of Sweet’s syndrome occur in patientswith an underlying malignancy.32,33 Eighty-five percentof malignancies are hematologic in origin, with acute my-eloid leukemia being the most common associated malig-nancy.32,34 The distribution of the lesions is most com-monly on the face, neck and upper extremities. This dis-ease is characterized by an abrupt onset of painful bluish-red papules or nodules that coalesce and form irregularplaques.33,35–37 The lesions tend to enlarge over a periodof weeks, with eventual resolution and healing withoutscarring. Recurrence of lesions is common, with abouthalf of the patients experiencing recurrences, most oftenin previously involved sites.32,33,35,36 Cutaneous eruptionsare frequently accompanied by fever and leukocytosis.32,37
Peripheral leukocytosis with neutrophilia and an elevatedwhite blood cell count are common laboratory findings,although not all patients with Sweet’s syndrome showthese findings.32,33,37 Histological features of this diseaseinclude edema of the dermal papillae and a dense infiltrateof neutrophils in the dermis without evidence of leuko-cytoclastic vasculitis.32–35,38 Fragmented neutrophil nu-clei are also commonly seen.32,33,35,38 Clinical differentia-tion from pyoderma vegetans is based on the lack of ver-rucous plaques with elevated borders. Histologically,Sweet’s syndrome lacks the characteristic pseudoepithe-liomatous hyperplasia seen in pyoderma vegetans; instead,a diffuse dermal neutrophilic infiltrate with edema of thepapillary dermis is seen.32–35,38
Bromoderma, mycobacterial infections, squamous cellcarcinoma, and giant keratoacanthomas are also includedin the differential diagnosis.2
The diagnosis of pyoderma vegetans is based on clini-cal and histological findings.2 Large verrucous plaqueswith elevated borders and multiple pustules are seen clini-cally. Histologic examination demonstrates pseudoepithe-liomatous hyerplasia. Wound cultures also demonstrategrowth of at least one pathogenic bacteria, such as Staph-ylococcus aureus or Pseudomonas aeuroginosa. Cultures forfungi and mycobacteria must be evaluated. Direct andindirect immunofluorescence can distinguish betweenpyoderma vegetans and pemphigus vegetans.12,13 Our pa-
tient met the clinical and histological criteria for the di-agnosis of pyoderma vegetans. Our patient had a historyof hidradenitis suppurativa, similar to a patient reportedby Boyd and Zemtsov.13 They proposed that hidradenitissuppurativa may have caused an immune complex depo-sition in the skin which precipitated the pyoderma veg-etans reaction; the nonspecific immunoreactant deposi-tion by direct immunofluorescence in our patient may beinterpreted as in support of their theory.13 Our patienthad no evident underlying immunocompromising condi-tion. She has been lost to followup for more than one yearand could not be investigated for the abnormally high IgElevel on serum electrophoresis.
Su et al.2 reported significant improvement and clear-ing of pyoderma vegetans in five of seven patients treatedwith intravenous antibiotics and topical wound care withcopper sulfate or aluminum subacetate dressings. A pa-tient treated with intravenous ceftriaxone and topical alu-minum acetate soaks had moderate clearing of lesions.13
Intralesional injection of corticosteroids and zinc oxideapplication completely cleared lesions on the perianal areaover a course of two months in one patient.12 Anotherpatient had complete clearing of a vegetating lesion onthe dorsum of the hand with 2 g of ampicillin daily forfour weeks accompanied by x-ray irradiation.19 Curettageor laser debridement complementing antibiotic therapyhas also been reported to be beneficial in clearing le-sions.39 Topical application of disodium chromoglycate,which has been used in the management of chronic legulcers40 and pyoderma gangrenosum41, healed one pa-tient’s lesions which were refractory to antibiotictherapy.9 Thus, the treatment of pyoderma vegetans hasnot yet been standardized although antibiotic treatmenthas produced variable results.
References
1. Brown CS, Kligman AM. Mycosis-like pyoderma. Arch Dermatol1957; 75:123–125.
2. Su WP, Duncan SC, Perry HO. Blastomycosis-like pyoderma. ArchDermatol 1979; 115:170–173.
3. Zilberberg B. Piodermite vegetante de Hallopeau e Penfigo veg-etante: Pesquisas experimetais sobre a etiologia da Piodermite veg-etante de Hallopeau. Sao Paulo: Empresa Grafica da “Revista DosTribunais” S.A., 1960, pp 1–180.
4. Wozniacka A, Sysa-Jedrzejowska A, Schwartz RA Recurrent chan-criform pyoderma. Chron Dermantol (Roma) (in press).
5. Brunsting LA, Underwood LJ. Pyoderma vegetans in associationwith chronic ulcerative colitis. Arch Dermatol 1949; 60:161–172.
6. Welch KJ, Burke WA, Park HK. Pyoderma vegetans: associationwith diffuse T cell lymphoma (large cell type). J Am Acad Dermatol1989; 20:691–693.
7. Potekaev NS, Iurin OG, Gorbacheva ZS, et al. Pyoderma vegetansas an early sign of HIV infection. Ter Arkh 1991; 63:78–80.
8. Hallopeau H. Pyodermite vegetante, ihre Beziehungen zur Derma-titis Herpetiformis and dem Pemphigus vegetans. Archt DermatolSyph (Wien) 1898; 43:289–306.
9. Rongioletti F, Semino M, Drago F, et al. Blastomycosis-like pyo-derma (pyoderma vegetans) responding to antibiotics and topicaldisodium chromoglycate. Int J Dermatol 1996; 35:828–830.
10. Dutta TK, James J, Baruah MC, et al. Blastomycosis-like pyodermain a case of chronic myeloid leukaemia. Postgrad Med J 1992;68:363–365.
226 Journal of Cutaneous Medicine and Surgery Volume 5 Number 3 May 2001

11. Ishibashi A, Kimura K. A case of pyoderma vegetans (pyo-rhino-blepharo-stomatitis vegetans). Nippon Hifuka Gakkai Zasshi 1986;96:1649–1653.
12. Fujita M, Okamoto S. A case of pyoderma vegetans associated withacne conglobata. J Dermatol (Tokyo) 1990; 17:429–434.
13. Boyd AS, Zemtsov A. A case of pyoderma vegetans and the follicularocclusion triad. J Dermatol (Tokyo) 1992; 19:61–63.
14. Ichimiya M, Yamamoto K, Muto M. Successful treatment of pem-phigus vegetans by addition of etretinate to systemic steroids. ClinExp Dermatol 1998; 23:178–180.
15. Ahdoot D, Rickman LS, Haghighi P. Botryomycosis in the acquiredimmunodeficiency syndrome. Cutis 1995; 55:149–152.
16. Salvemini JN, Baldwin HE. Botryomycosis in a patient with ac-quired immunodeficiency syndrome. Cutis 1995; 56:158–160.
17. Mehregan DA, Su WP, Anhalt JP. Cutaneous botryomycosis. J AmAcad Dermatol 1991; 24:393–396.
18. Follows GA, Mathew J, Lucas S, et al. Cutaneous botryomycosis ina patient with lupus nephritis. Nephrol Dial Transplant 1998;13:3200–3201.
19. Marshalko M, Preisz K, Harsing J, et al. Pyoderma vegetans. Reporton a case and review of data on pyoderma vegetans and cutaneousbotryomycosis. Acta Derm Venereol APA (Ljubljana) 1995; 4:55–59.
20. Levitt MD, Ritchie JK, Lennard-Jones JE, et al. Pyoderma gan-grenosum in inflammatory bowel disease. Br J Surg 1991; 78:676–678.
21. Greenstein AJ, Janowitz HD, Sachar DB. The extra-intestinal com-plications of Crohn’s disease and ulcerative colitis: a study of 700patients. Medicine (Baltimore) 1976; 55:401–412.
22. Basler RS. Ulcerative colitis and the skin. Med Clin North Am1980; 64:941–954.
23. De Keyser F, Verhoef GE, Dewyspelaere J, et al. Pyoderma gan-grenosum in a patient with chronic myeloid leukemia. Acta ClinBelg 1990; 45:340–342.
24. Stolman LP, Rosenthal D, Yaworsky R, et al. Pyoderma gangreno-sum and rheumatoid arthritis. Arch Dermatol 1975; 111:1020–1023.
25. Powell FC, Schroeter AL, Su WP, et al. Pyoderma gangrenosum: areview of 86 patients. Q J Med 1985; 55:173–186.
26. Bennett ML, Jackson JM, Jorizzo JL, et al. Pyoderma gangrenosum.A comparison of typical and atypical forms with an emphasis on time
to remission. Case review of 86 patients from 2 institutions. Medi-cine (Baltimore) 2000; 79:37–46.
27. Powell FC, Su WP, Perry HO. Pyoderma gangrenosum: classifica-tion and management. J Am Acad Dermatol 1996; 34:395–412.
28. Hickman JG, Lazarus GS. Pyoderma gangrenosum: a reappraisal ofassociated systemic diseases. Br J Dermatol 1980; 102:235–237.
29. Dourmishev AL, Miteva I, Schwartz RA. Pyoderma gangrenosum inchildhood. Cutis 1996; 58:257–262.
30. Hurwitz RM, Haseman JH. The evolution of pyoderma gangreno-sum. A clinicopathologic correlation. Am J Dermatopathol 1993;15:28–33.
31. Wilson–Jones E, Winkelmann RK. Superficial granulomatous pyo-derma: a localized vegetative form of pyoderma gangrenosum. J AmAcad Dermatol 1988; 18:511–521.
32. Cohen PR, Kurzrock R. Sweet’s syndrome and cancer. Clin Der-matol 1993; 11:149–157.
33. Fitzgerald RL, McBurney EI, Nesbitt Jr. LT. Sweet’s syndrome. IntJ Dermatol 1996; 35:9–15.
34. Cohen PR, Talpaz M, Kurzrock R. Malignancy-associated Sweet’ssyndrome: review of the world literature. J Clin Oncol 1988;6:1887–1897.
35. Kemmett D, Hunter JA. Sweet’s syndrome: a clinicopathologic re-view of twenty-nine cases. J Am Acad Dermatol 1990; 23:503–507.
36. Sharma PK, Schwartz RA, Janniger CK, et al. Sweet’s syndromewith acute leukemia. Cutis 1991; 47:249–252.
37. Brodkin RH, Schwartz RA. Sweet’s syndrome with myelofibrosisand leukemia: partial response to interferon. Dermatology 1995;190:160–163.
38. Cohen PR, Holder WR, Tucker SB, et al. Sweet syndrome in pa-tients with solid tumors. Cancer 1993; 72:2723–2731.
39. Sawchuk WS, Heald PW. Blastomycosis-like pyoderma—report ofa case responsive to combination therapy utilizing minocycline andcarbon dioxide laser debridement. J Dermatol Surg Oncol 1986;12:1041–1044.
40. Lip P. Sodium chromoglycate (Intal) in the management of chronicleg ulcers. Med J Austral 1978; 2:32.
41. Massone L, Borghi S, Pestarino A, et al. Topical disodium chro-moglycate in the management of pyoderma gangrenosum. Cutis1988; 42:459–462.
227Pyoderma VegetansA. J. Papadopoulos et al.