joint external evaluation tool - extranet.who.int · international ealt reulations 2005 7 - joint...
TRANSCRIPT

JOINT EXTERNAL EVALUATION TOOL
SECOND EDITION - January 2018
TECHNICAL FRAMEWORK IN SUPPORT TO IHR (2005) MONITORING AND EVALUATION
INTERNATIONAL HEALTH REGULATIONS (2005)


JOINT EXTERNAL EVALUATION TOOL
SECOND EDITION - January 2018
TECHNICAL FRAMEWORK IN SUPPORT TO IHR (2005) MONITORING AND EVALUATION

© World Health Organization 2018
Some rights reserved. This work is available under the Creative Commons Attribution-NonCommer-cial-ShareAlike 3.0 IGO licence (CC BY-NC-SA 3.0 IGO; https://creativecommons.org/licenses/by-nc-sa/3.0/igo).
Under the terms of this licence, you may copy, redistribute and adapt the work for non-commercial purposes, provided the work is appropriately cited, as indicated below. In any use of this work, there should be no suggestion that WHO endorses any specific organization, products or services. The use of the WHO logo is not permitted. If you adapt the work, then you must license your work under the same or equivalent Creative Commons licence. If you create a translation of this work, you should add the following disclaimer along with the suggested citation: “This translation was not created by the World Health Organization (WHO). WHO is not responsible for the content or accuracy of this translation. The original English edition shall be the binding and authentic edition”.
Any mediation relating to disputes arising under the licence shall be conducted in accordance with the mediation rules of the World Intellectual Property Organization.
Suggested citation. Joint external evaluation tool: International Health Regulations (2005), second edition. Geneva: World Health Organization; 2018. Licence: CC BY-NC-SA 3.0 IGO
Cataloguing-in-Publication (CIP) data. CIP data are available at http://apps.who.int/iris.
Sales, rights and licensing. To purchase WHO publications, see http://apps.who.int/bookorders. To submit requests for commercial use and queries on rights and licensing, see http://www.who.int/about/licensing.
Third-party materials. If you wish to reuse material from this work that is attributed to a third party, such as tables, figures or images, it is your responsibility to determine whether permission is needed for that reuse and to obtain permission from the copyright holder. The risk of claims resulting from infringement of any third-party-owned component in the work rests solely with the user.
General disclaimers. The designations employed and the presentation of the material in this publica-tion do not imply the expression of any opinion whatsoever on the part of WHO concerning the legal status of any country, territory, city or area or of its authorities, or concerning the delimitation of its frontiers or boundaries. Dotted and dashed lines on maps represent approximate border lines for which there may not yet be full agreement.
The mention of specific companies or of certain manufacturers’ products does not imply that they are endorsed or recommended by WHO in preference to others of a similar nature that are not men-tioned. Errors and omissions excepted, the names of proprietary products are distinguished by initial capital letters.
All reasonable precautions have been taken by WHO to verify the information contained in this pu-blication. However, the published material is being distributed without warranty of any kind, either expressed or implied. The responsibility for the interpretation and use of the material lies with the reader. In no event shall WHO be liable for damages arising from its use.
Design: crayonbleu - France
Joint external evaluation tool: International Health Regulations (2005), second editionISBN 978-92-4-155022-2

CONTENTSAbbreviations 6Background 7
International Health Regulations (2005) 7The IHR Review Committee on Second Extensions 7Technical Framework for IHR Monitoring and Evaluation post 2016 7Voluntary Joint External Evaluation (JEE) 7Revision of the JEE tool 8Purpose of the JEE 9The JEE process 9The JEE format 10Colour scoring system 10Contextual questions 10Technical questions 10
COUNTRY EVALUATION TOOL 11 PREVENT 13
National legislation, policy and financing 13IHR coordination, communication and advocacy 19Antimicrobial resistance 22Zoonotic disease 30Food safety 34Biosafety and biosecurity 38Immunization 45
DETECT 49 National laboratory system 49Surveillance 56Reporting 60Human resources 63
RESPOND 70 Emergency preparedness 70Emergency response operations 75Linking public health and security authorities 80Medical countermeasures and personnel deployment 85Risk communication 88
IHR RELATED HAZARDS AND POINTS OF ENTRY 95 Points of entry 95Chemical events 99Radiation emergencies 104
Appendix 1: Glossary 109Appendix 2: Summary of changes between JEE tool first and second editions 114

INTERNATIONAL HEALTH REGULATIONS (2005)
6 - Joint External Evaluation Tool - Second edition
AMR Antimicrobial resistanceBTWC Biological and Toxin Weapons ConventionCLSI Clinical and Laboratory Standards InstituteCPE Continuing Professional EducationEBS Event-based surveillanceEMT Emergency Medical TeamEOC Emergency Operations CentreEQA External Quality AssessmentEUCAST European Committee on Antimicrobial Susceptibility TestingFAO Food and Agriculture OrganizationFETP Field Epidemiology Training ProgrammeGAP Global Action PlanGHSA Global Health Security AgendaGLASS Global Antimicrobial Resistance Surveillance SystemGOARN Global Outbreak Alert and Response NetworkHAI Healthcare-associated infectionsHIV Human Immunodeficiency VirusIAEA International Atomic Energy Agency IBS Indicator-based surveillanceIHR International Health RegulationsINFOSAN International Food Safety Authorities NetworkINTERPOL International Criminal Police OrganizationISO International Organization for StandardizationIT Information TechnologyJEE Joint External EvaluationMCV Measles-containing vaccineMoU Memorandum of understandingNAPHS National Action Plan for Health Security NCC National Coordinating CentreNGO Non-governmental OrganizationNSHSP National Strategic Health Sector PlanOIE World Organisation for Animal HealthOPCW Organisation for the Prohibition of Chemical WeaponsPCR Polymerase Chain ReactionPHEIC Public Health Emergency of International ConcernPoE Points of EntryPVS Performance of Veterinary ServicesQMS Quality Management SystemSAICM Strategic Approach to International Chemicals Management SOP Standard Operating ProcedureVPDs Vaccine-preventable diseasesWAHIS World Animal Health Information SystemWASH water, sanitation and hygieneWHA World Health AssemblyWHO World Health Organization
ABBREVIATIONS

INTERNATIONAL HEALTH REGULATIONS (2005)
7 - Joint External Evaluation Tool - Second edition
BACKGROUNDwas further echoed by the Review Committee on the Role of the IHR in the Ebola Outbreak and Res-ponse in its fifth recommendation to “introduce and promote external assessment of core capacities”.
TECHNICAL FRAMEWORK FOR IHR MONITORING AND EVALUATION POST 2016 Based on IHR Review committee recommen-dations, WHO developed a concept note for monitoring and evaluation framework comprising of the existing one mandatory component (States Parties Annual Reporting) and three new voluntary components (after action review, simulation exercises and external evaluation) in 2015. A second technical consultation in Lyon in October 2015, led to the development of the joint external evaluation (JEE) tool based on existing WHO tools and various regional strategies and other initiatives, such as the Global Health Security Agenda (GHSA), World Organisation for Animal Health Performance of Veterinary Services (OIE PVS) Pathway. The JEE was published in February 2016. In addition to evaluating the capacities required under the IHR, the JEE and NAPHS also contributes to the implementation of the Sendai Framework for Disaster Risk Reduction that recognises the importance of implementation of the International Health Regulations (2005) and the building of resilient health systems.
VOLUNTARY JOINT EXTERNAL EVALUATION (JEE)The technical areas covered in this voluntary com-ponent of the technical framework are, grouped into four core areas: – prevent, detect, respond, and IHR related hazards and points of entry. The JEE in this respect considers:• preventing and reducing the likelihood of out-
breaks and other public health hazards and events defined by IHR is essential;
• detecting threats early can save lives;• rapid and effective response requires multisec-
toral, national and international coordination and communication; and
• IHR capacities are required at points of entry, and during chemical events and radiation emergencies.
THE INTERNATIONAL HEALTH REGULATIONS (2005) In May 2005, the Fifty-eighth World Health As-sembly (WHA) adopted the International Health Regulations (IHR (2005); hereinafter “IHR” or “the Regulations”), which subsequently entered into force on 15 June 2007. All States Parties are re-quired by the IHR to develop certain minimum core public health capacities. IHR capacity requi-rements are defined as “the capacity to detect, assess, notify and report events” in Article 5; and “the capacity to respond to promptly and effectively to public health risks and public health emergen-cies of international concern” in Article 13.IHR (2005) (Article 54 and Resolution WHA61.2) requires State Parties and the WHO Director-General to report annually to the World Health Assembly on the implementation of the Regulations as decided by the Health Assembly. The IHR Core Capacity Monitoring Framework was developed by the Secretariat, with a checklist and indicators to monitor progress in the development of the core capacities. Between 2010 and 2016, 195 State Parties have reported to WHO at least once using IHR monitoring questionnaires; averaging 73% of MS reporting annually.
THE IHR REVIEW COMMITTEE ON SECOND EXTENSIONSThe IHR Review Committee on Second Extensions for establishing national public health capacities and on IHR implementation (WHA68/22 Add.1) in 2014 recommended that with a longer term vision the Secretariat “should develop options to move from exclusive self-evaluation to approaches that combine self-evaluation, peer review and volunta-ry external evaluations involving a combination of domestic and independent experts. These additio-nal approaches should consider, amongst other things, strategic and operational aspects of the IHR, such as the need for high-level political com-mitment, and whole of government/multisectoral engagement. Any new monitoring and evaluation scheme should be developed with the active invol-vement of WHO regional offices and subsequently proposed to all States Parties through the WHO governing bodies’ process”. This recommendation
1 - Checklist and indicators for monitoring progress in the development of IHR core capacities in States Parties. WHO/HSE/GCR/2013.2. Geneva: World Health Organization; 2013 (http://apps.who.int/iris/bitstream/10665/84933/1/WHO_HSE_GCR_2013.2_eng.pdf?ua=1, accessed 19 December 2017).

INTERNATIONAL HEALTH REGULATIONS (2005)
8 - Joint External Evaluation Tool - Second edition
REVISION OF THE JEE TOOLThe first edition of the tool was made available in February 2016, and by the end of December 2017 67 countries had requested a JEE to WHO and completed the voluntary evaluation using this tool. In late 2016, the JEE Secretariat began the process of systematically collecting sug-gestions and comments on improving the first edition of the JEE tool from WHO Regional Of-fices, technical area leads in WHO headquarters and external experts who had participated in one or more JEE missions and Member States who had conducted a JEE or were preparing for a JEE. The suggested improvements and com-ments were collated into an annotated version of the JEE tool and in April 2017, WHO convened a global meeting with over 90 global technical experts and all WHO ROs to discuss the sug-gested improvements and recommend changes. These changes were incorporated into a revised version of the JEE tool and finalized in mid-2017. This is the second edition of the JEE tool2.
SUMMARY OF CHANGES INCORPORATED INTO THE SECOND ETIDION OF THE JEE TOOLThe main changes within the second edition of the JEE tool is the inclusion of two financing indicators, the merging of two indicators under legislation into a single one and the renaming of three technical areas (Real time surveillance is now Surveillance, Workforce development is now Human resources and Preparedness is now Emergency preparedness). The tool now has 49 indicators (increase of one indicator from the previous 48), within the 19 technical areas. The second edition of the tool helps clarify issues in the interpretation of various indicators, attri-butes and questionnaires, with more footnotes. It also clarifies the discrepancy found in national capacities between the human and animal sec-tors and recommends animal and human health scores for the indicators are given; the lower score of the two is to be considered, rather than the average. The technical areas of IHR coordination, commu-nication and advocacy, Biosafety and biosecu-rity, Immunization, National laboratory system, Reporting, Emergency preparedness, Medical countermeasures and personnel deployment,
Linking public health and security authorities, Risk communication, Points of entry, Chemical events and Radiation emergencies, have minor changes for the purpose of clarity and interpre-tation.
CHANGES IN INDICATORSTwo indicators of National legislation, policy and finance are combined and two additional indicators for finance added. Two indicators on Antimicrobial resistance (AMR) are combined and a new indicator on effective coordination added to align with the global action plan for AMR. For Zoonotic disease, an indicator on workforce is incorporated in the Human resources technical area and the rest of the indicators are updated to better reflect output and outcome. The food safety technical area is split into two to reflect detection and response capacities, respectively. The surveillance technical area now has three indicators where the indicators for event-based, indicator-based and syndromic surveillance are combined as “surveillance systems”. The rest of the indicators of Surveillance remain the same with a few changes that reflect output and out- come of the system. The human resources tech-nical area presently consists of four indicators with the addition of a new indicator on in-ser-vice training capacities, which incorporates veterinary workforce from Zoonotic disease and is linked to the multisectoral workforce as required for IHR implementation. The Emer-gency response operations technical area now has three indicators as one of the indicators on case management was moved to Medical coun-termeasures and personnel deployment. Two indicators on “capacity to activate” and “opera-tional procedures for emergency operations” are combined as “emergency operations centre” and an additional indicator on “emergency response coordination” is added.Details of the changes incorporated into the second edition of the JEE tool are available in Appendix 2.
PURPOSE OF THE JEE The JEE is one of the three voluntary process available for MS to request as needed to evaluate country capacity to prevent, detect and rapidly respond to public health threats independently
2 - Countries that have already started self-evaluation using the first edition of the JEE tool will be evaluated using the same tool. However, countries that are starting self-evaluation from January 2018 onwards will use the second edition of the JEE tool for self-evaluation and external evaluation.

INTERNATIONAL HEALTH REGULATIONS (2005)
9 - Joint External Evaluation Tool - Second edition
3 - Operational readiness” concept was derived from the ‘readiness’ definition of United Nations General Assembly, 2017 (see definitions) and enables countries to fast track the development of certain capacities in order to be ready to respond to emergencies, including imminent high risks, while system-wide capacity development is ongoing.4 - International Health Regulations (IHR): joint external evaluation. Country implementation guide. WHO/WHE/CPI/2017.62. Geneva: World Health Organization; 2017 (http://apps.who.int/iris/bitstream/10665/259605/1/WHO-WHE-CPI-2017.62-eng.pdf, accessed 17 December 2017). 5 - International Health Regulations (IHR): joint external evaluation. Roster of experts process and overview. WHO/WHE/CPI/2017.63. Geneva: World Health Organization; 2017 (http://apps.who.int/iris/bitstream/10665/259604/1/WHO-WHE-CPI-2017.63-eng.pdf, accessed 17 December 2017).6 - International Health Regulations (IHR): joint external evaluation: Mission reports. [website] http://www.who.int/ihr/procedures/mission-reports/en/, accessed on 30 December 2017) 7 - In the WHO African Region, IHR implementation is within the context of Integrated Disease Surveillance and Response Strategy and in the Asia Pacific (South-East Asia Region and Western Pacific Region), IHR implementation is in the context of the Asia-Pacific Strategy for Emerging Diseases.
of whether they are naturally occurring, delibe-rate or accidental. The purpose of the external evaluation is to measure country-specific sta-tus and progress in achieving the targets. This will require a sustainable and flexible process to allow for additional countries to participate and for regular evaluation visits. The first external evaluation will establish a baseline measure-ment of the country’s capacity and capabilities, and subsequent evaluations will identify the progress made and ensure that improvements in capacity are sustainable.JEEs have a number of important features inclu-ding: voluntary country participation; a multisec-toral approach by both the external teams and the host countries; transparency and openness of data and information sharing; and the public release of reports. In the joint process during an external evaluation (envisioned to take place ap-proximately once every four to five years), a team of national experts first completes a self-eva-luation using the JEE tool that is submitted to the external team prior to the country visit. The external team uses the same tool for their inde-pendent evaluation, working together with the national team in interactive sessions.The external evaluation creates a common plat-form for country information and data. This al-lows countries to identify the most urgent needs within their health security system, to prioritize opportunities for enhanced preparedness, res-ponse and action, and to engage with current and prospective donors as well as partners to target resources effectively. Transparency is an important element for attracting and directing resources to where they are needed the most. In addition, JEE priorities and the development of a multiyear national action plan can help ensure operational readiness in countries with urgent needs (such as highly vulnerable, low resource settings).The JEE tool was developed to provide an exter-nal mechanism to evaluate a country’s IHR ca-pacity for ensuring health security and use the
expertise of global experts to provide recommen-dations across the 19 technical areas assessed. The JEE tool draws on the original IHR core ca-pacities and incorporates valuable content and lessons learned from tested external assess-ment tools and processes of several other mul-tilateral and multisectoral initiatives that sup-ported the building of capacity to prevent, detect and respond to infectious disease threats.
PROCESS FOR VOLONTARY JEEThe first stage of the process is a self-evaluation using the JEE tool and country implementation guide,4 completed by the country with multisec-toral engagement. This information is then given to the JEE team consisting of international sub-ject matter experts5. Review of this self-evalua-tion data provides the team members with an understanding of the country’s baseline health security capabilities. The JEE team consisting of international subject matter experts then vi-sit the country for facilitated in-depth discus-sions of the self-reported data and participate in structured site visits and meetings organized by the host country. The evaluation team uses fin-dings from various relevant evaluations and as-sessments, such as the OIE PVS Pathway, moni-toring and evaluation of disaster risk reduction and others.After conducting the evaluation, the JEE team drafts a report to identify status levels for each indicator and presents an analysis of the country’s capabilities, gaps, opportunities and challenges. The draft report is shared with the host country. After the host country concurs with the findings, the final report is published on the WHO website6. This approach facilitates international support of country implementation efforts, encourages sharing of best practices and lessons learned, promotes international ac-countability, engages stakeholders, and informs and guides IHR implementation both in the host country and internationally.7

INTERNATIONAL HEALTH REGULATIONS (2005)
10 - Joint External Evaluation Tool - Second edition
THE JEE FORMATEach indicator in the JEE tool has attributes that reflect various levels of capacity. These are identified with scores ranging from “1” (indicating that implementation has not occurred) to “5” (indicating that implementation has occurred, is tested, reviewed and exercised, and that the country has a sustainable level of capability for the indicator). For each indicator, a country receives a single score based on their current capacity. The “technical area questions” help the evaluators determine the appropriate score. Most of the measures are descriptive and qualitative. Countries are asked to provide documentation for relevant items in addition to the responses. The documentation and responses are reviewed by the evaluators and discussed with host country experts using a peer-to-peer, consensus based approach. The final report includes scores as well as a narrative that document existing capacities, gaps and challenges. The key findings are presented as three to five priority actions for each of the 19 technical areas.
COLOUR SCORING SYSTEMWhile there is overlap among the capacity sections of the tool, each capacity is considered separately in the evaluation exercise. The implementation status of each core capacity is indicated by a score, which reflects the country’s level of advancement, its capacity to institutionalize technical area competencies, and ensure that they are sustainable. The following describes the level of advancement or scoring with colour coding. 1. No capacity: Attributes of a capacity are not
in place.Colour code: Red
2. Limited capacity: Attributes of a capacity are in development stage (implementation has started with some attributes achieved and others commenced).
Colour code: Yellow
3. Developed capacity: Attributes of a capacity are in place; however, sustainability has not been ensured (such as through inclusion in the operational plan of the national health sector plan with a secure funding source).
Colour code: Yellow
CONTEXTUAL QUESTIONSThese are questions on or relating to circumstances that form the backdrop for the given technical areas.
TECHNICAL QUESTIONSThese are questions directly related to technical area indicators and attributes, which enable the country and external team to evaluate achievements against specific attributes.
DOCUMENTATION OR EVIDENCE FOR LEVEL OF CAPABILITYSome responses to contextual and technical questions require documentation, which provides evidence to evaluate the level of achievement in specific indicators and technical areas. Note: In some technical areas indicator specific documentation is requested.
4. Demonstrated capacity: Attributes are in place and sustainable for a few years, and can be measured by the inclusion of attributes or IHR core capacities in the national health sector plan and a secure funding source.
Colour code: Green
5. Sustainable capacity: All attributes are functional and sustainable, and the country is supporting one or more other countries in their implementation. This is the highest level of the achievement of implementation of IHR core capacities.
Colour code: Green
1. A country can advance to the next adjacent level only when it has achieved ALL the attributes of its current capacity levels. For example, in order to reach “demonstrated” capacity, it has to meet all the attributes of “developed” and “demonstrated” capacity.2. All responses must be supported by documentable evidence.

INTERNATIONAL HEALTH REGULATIONS (2005)
11 - Joint External Evaluation Tool - Second edition
COU
NTR
Y EV
ALU
ATIO
N T
OO
L

INTERNATIONAL HEALTH REGULATIONS (2005)
12 - Joint External Evaluation Tool - Second edition
PR
EV
EN
T
INTERNATIONAL HEALTH REGULATIONS (2005)
13 - Joint External Evaluation Tool - Second edition
PREV
ENT
NAT
ION
AL L
EGIS
LATI
ON
1 , PO
LICY
AN
D F
INAN
CIN
G
Targ
ets:
Ade
quat
e le
gal f
ram
ewor
k fo
r Sta
tes
Part
ies
to s
uppo
rt a
nd e
nabl
e th
e im
plem
enta
tion
of a
ll th
eir o
blig
atio
ns a
nd ri
ghts
mad
e by
the
IHR.
Dev
elop
men
t of
new
or m
odifi
ed le
gisl
atio
n in
som
e St
ates
Par
ties
for t
he im
plem
enta
tion
of th
e Re
gula
tions
. Whe
re n
ew o
r rev
ised
legi
slat
ion
may
not
be
spec
ifica
lly re
quire
d un
der a
Sta
te P
arty
’s le
gal s
yste
m, t
he S
tate
may
revi
se s
ome
legi
slat
ion,
regu
latio
ns o
r oth
er in
stru
men
ts in
ord
er to
faci
litat
e th
eir i
mpl
emen
tatio
n in
a m
ore
effic
ient
, effe
ctiv
e or
ben
efici
al m
anne
r. St
ates
Par
ties
ensu
re p
rovi
sion
of
adeq
uate
fun
ding
for
IH
R im
plem
enta
tion
thro
ugh
the
natio
nal
budg
et o
r ot
her
mec
hani
sms.
Cou
ntry
has
acc
ess
to fi
nanc
ial r
esou
rces
for t
he im
plem
enta
tion
of IH
R ca
paci
ties2 .
Fina
ncin
g th
at c
an b
e ac
cess
ed o
n tim
e an
d di
strib
uted
in
resp
onse
to p
ublic
hea
lth e
mer
genc
ies,
is a
vaila
ble.
As m
easu
red
by: (
1) C
urre
nt le
gisl
atio
n in
clud
ing
law
s, re
gula
tions
, adm
inis
trat
ive
requ
irem
ents
, pol
icie
s or
oth
er g
over
nmen
t ins
trum
ents
, pro
ven
to b
e ad
equa
te
in a
ll re
leva
nt s
ecto
rs to
sup
port
IHR
impl
emen
tatio
n. (2
) Ade
quat
e fin
ance
s av
aila
ble
to e
nabl
e ef
ficie
nt a
nd e
ffect
ive
IHR
impl
emen
tatio
n an
d re
spon
se to
all
publ
ic h
ealth
em
erge
ncie
s.
Desi
red
impa
ct: L
egis
latio
n an
d fin
anci
ng in
pla
ce in
all
rele
vant
sec
tors
3 to
supp
ort I
HR
impl
emen
tatio
n in
clud
ing
core
cap
acity
dev
elop
men
t and
mai
nten
ance
1 -
The
term
“le
gisl
atio
n” re
fers
to th
e br
oad
rang
e of
lega
l, re
gula
tory
, adm
inis
trat
ive
or o
ther
gov
ernm
enta
l ins
trum
ents
whi
ch m
ay b
e av
aila
ble
for S
tate
s Pa
rtie
s to
impl
emen
t the
IHR
and
whi
ch a
re n
ot n
eces
saril
y lim
ited
to
inst
rum
ents
ado
pted
by
the
legi
slat
ure.
Ref
er to
the
WH
O g
uida
nce
on IH
R im
plem
enta
tion
in n
atio
nal l
egis
latio
n (h
ttp:
//w
ww
.who
.int/
ihr/
lega
l_is
sues
/leg
isla
tion/
en/,
acce
ssed
24
Nov
embe
r 201
7).
2 -
IHR
capa
citie
s re
fers
to th
e ca
paci
ty to
pre
vent
, det
ect,
asse
ss, n
otify
and
resp
ond
to a
cute
pub
lic h
ealth
eve
nts,
and
incl
udes
dev
elop
ing
and
mai
ntai
ning
all
esse
ntia
l pub
lic h
ealth
func
tions
that
are
nee
ded
to a
pply
and
com
ply
with
the
IHR.
3 -
Rele
vant
sec
tors
incl
ude
priv
ate
and
publ
ic s
ecto
rs, s
uch
as: a
ll le
vels
of t
he h
ealth
car
e sy
stem
(nat
iona
l, su
bnat
iona
l and
com
mun
ity/p
rimar
y pu
blic
hea
lth);
nong
over
nmen
tal o
rgan
izat
ions
(NG
Os)
; div
isio
ns/a
ctiv
ities
of o
ther
se
ctor
s w
hich
affe
ct p
ublic
hea
lth, s
uch
as m
inis
trie
s of
agr
icul
ture
(qua
rant
ine
and
mov
emen
t con
trol
aut
horit
y, im
port
/exp
ort r
egul
atio
ns, d
isea
se d
iagn
osis
and
con
trol
fina
ncin
g, z
oono
sis,
vet
erin
ary
labo
rato
ry e
tc.),
tran
spor
t (t
rans
port
pol
icy,
civi
l avi
atio
n, p
orts
and
mar
itim
e tr
ansp
ort)
, tra
de a
nd/o
r in
dust
ry (f
ood
safe
ty a
nd q
ualit
y co
ntro
l), fo
reig
n tr
ade
(con
sum
er p
rote
ctio
n, c
ontr
ol o
f com
puls
ory
stan
dard
enf
orce
men
t), c
omm
unic
atio
n, d
efen
ce,
trea
sury
or fi
nanc
e (c
usto
ms)
, env
ironm
ent,
inte
rior,
heal
th, t
ouris
m; t
he h
ome
offic
e; m
edia
; and
regu
lato
ry b
odie
s.
PR
EV
EN
T

INTERNATIONAL HEALTH REGULATIONS (2005)
14 - Joint External Evaluation Tool - Second edition
Scor
e
Indi
cato
rs: N
atio
nal l
egis
latio
n, p
olic
y an
d fin
anci
ngP.
1.1
The
Stat
e ha
s as
sess
ed, a
djus
ted
and
alig
ned
its d
omes
tic le
gisl
atio
n, p
olic
ies
and
adm
inis
trat
ive
arra
ngem
ents
in a
ll re
leva
nt
sect
ors,
4,5 t
o en
able
com
plia
nce
with
the
IHR
P.1.
2 Fi
nanc
ing6 i
s av
aila
ble
for t
he
impl
emen
tatio
n of
IHR
capa
citie
sP.
1.3
A fin
anci
ng m
echa
nism
and
fund
s ar
e av
aila
ble
for t
imel
y re
spon
se to
pub
lic h
ealth
em
erge
ncie
s8
No
capa
city
- 1
Asse
ssm
ent
of r
elev
ant
legi
slat
ion,
reg
ulat
ions
, ad
min
istr
ativ
e re
quire
men
ts a
nd o
ther
gov
ernm
ent
inst
rum
ents
not
und
erta
ken
for t
he im
plem
enta
tion
of IH
R
Ther
e is
no
bu
dget
lin
e or
bu
dget
ary
allo
catio
n9 ava
ilabl
e to
fina
nce
the
impl
emen
tatio
n of
IHR
capa
citie
s, a
nd fi
nanc
ing
for i
mpl
emen
tatio
n of
IH
R ca
paci
ties
is
hand
led
thro
ugh
extr
a-bu
dget
ary
mea
ns10
Fina
ncin
g fo
r re
spon
ding
to
pu
blic
he
alth
em
erge
ncie
s is
no
t id
entifi
ed
and
fund
s ar
e al
loca
ted
and
dist
ribut
ed i
n an
ad
hoc
man
ner
durin
g a
publ
ic h
ealth
em
erge
ncy
Lim
ited
ca
paci
ty -
2
Asse
ssm
ent
of r
elev
ant
legi
slat
ion,
reg
ulat
ions
, ad
min
istr
ativ
e re
quire
men
ts a
nd o
ther
gov
ernm
ent
inst
rum
ents
fo
r IH
R im
plem
enta
tion
has
been
ca
rrie
d ou
t an
d re
quire
d ad
just
men
ts h
ave
been
id
entifi
ed
A bu
dget
ary
allo
catio
n or
su
bsta
ntia
l ex
tern
al
finan
cing
11
is
mad
e fo
r so
me
of
the
rele
vant
se
ctor
s12 a
nd th
eir r
espe
ctiv
e m
inis
trie
s to
sup
port
th
e im
plem
enta
tion
of IH
R ca
paci
ties
for b
iolo
gica
l ha
zard
s14 a
t the
nat
iona
l lev
el
An e
mer
genc
y pu
blic
fina
ncin
g m
echa
nism
exi
sts15
th
at a
llow
s fo
r st
ruct
ured
rec
eptio
n an
d ra
pid
dist
ribut
ion
of fu
nds
for r
espo
ndin
g to
pub
lic h
ealth
em
erge
ncie
s
Deve
lope
d ca
paci
ty -
3
The
coun
try
can
dem
onst
rate
the
exi
sten
ce a
nd
use
of r
elev
ant
legi
slat
ion
in a
ll re
leva
nt s
ecto
rs
invo
lved
in th
e im
plem
enta
tion
of th
e IH
R16
A bu
dget
ary
allo
catio
n or
su
bsta
ntia
l ex
tern
al
finan
cing
is
mad
e fo
r hu
man
hea
lth,
vete
rinar
y pu
blic
hea
lth,
agric
ultu
re,
and
all
othe
r re
leva
nt
min
istr
ies
or s
ecto
rs, t
o su
ppor
t the
impl
emen
tatio
n of
all17
IHR
capa
citie
s at
the
natio
nal l
evel
Fina
ncin
g fo
r res
pons
e is
iden
tified
18 fo
r im
med
iate
m
obili
zatio
n w
hen
need
ed, a
t th
e na
tiona
l, st
ate,
pr
ovin
ce a
nd r
egio
nal
leve
ls f
or a
ll th
e re
leva
nt
sect
ors19
in a
dvan
ce o
f a p
ublic
hea
lth e
mer
genc
y
Dem
onst
rate
d ca
paci
ty -
4
The
coun
try
has
legi
slat
ion
refe
renc
es
and/
or
adm
inis
trat
ive
requ
irem
ents
fo
r sp
ecifi
c ar
eas
(suc
h as
cu
rren
t le
gisl
atio
n th
at
spec
ifica
lly
addr
esse
s N
atio
nal
IHR
Foca
l Po
int
desi
gnat
ion
and
oper
atio
ns)
A su
ffici
ent
budg
et20
is
al
loca
ted
with
tim
ely
dist
ribut
ion21
at
th
e na
tiona
l an
d su
bnat
iona
l le
vel(s
) in
all
rele
vant
min
istr
ies
or s
ecto
rs fo
r th
e im
plem
enta
tion
of a
ll IH
R ca
paci
ties
The
emer
genc
y pu
blic
fina
ncin
g m
echa
nism
in
plac
e al
low
s fo
r th
e tim
ely
exec
utio
n22 o
f fu
nds23
by
all
rele
vant
sec
tors
, du
ring
a pu
blic
hea
lth
emer
genc
y
Sust
aina
ble
capa
city
– 5
The
coun
try
has
legi
slat
ion
refe
renc
es
and/
or
adm
inis
trat
ive
requ
irem
ents
for a
ll ar
eas
rela
ted
to
IHR
impl
emen
tatio
n
A su
ffici
ent
budg
et t
hat
is d
istr
ibut
ed in
a t
imel
y m
anne
r at
the
nat
iona
l and
sub
natio
nal l
evel
(s) i
n al
l rel
evan
t min
istr
ies
or s
ecto
rs is
wel
l coo
rdin
ated
in
its
exec
utio
n24, f
or th
e im
plem
enta
tion
of a
ll IH
R ca
paci
ties
Fina
ncin
g ca
n be
exe
cute
d an
d m
onito
red25
in
a tim
ely
and
coor
dina
ted
man
ner a
t all
leve
ls a
nd fo
r al
l rel
evan
t sec
tors
, with
an
emer
genc
y co
ntin
genc
y fu
nd26
in
plac
e, f
or r
espo
nse
to a
n ac
ute
publ
ic
heal
th e
mer
genc
y
PR
EV
EN
T
4 -
Food
saf
ety
legi
slat
ion
shou
ld id
eally
incl
ude
all r
oles
and
resp
onsi
bilit
ies
nece
ssar
y to
mee
t the
obj
ectiv
es a
nd e
nfor
ce th
e va
rious
ele
men
ts o
f foo
d co
ntro
l to
prev
ent f
oodb
orne
dis
ease
s an
d fo
od c
onta
min
atio
n.5
-Tw
o cr
itica
l com
pete
ncie
s on
legi
slat
ion
in th
e PV
S to
ol a
re: C
ritic
al C
ompe
tenc
y (C
C) IV
-1: P
repa
ratio
n of
legi
slat
ion
and
regu
latio
ns; a
nd C
C IV
-2: I
mpl
emen
tatio
n of
legi
slat
ion,
regu
latio
ns a
nd c
ompl
ianc
e. T
he P
VS P
athw
ay
mis
sion
repo
rts
are
a go
od s
ourc
e of
info
rmat
ion
on th
e st
ate
of v
eter
inar
y le
gisl
atio
n in
the
coun
try.
6
- Fi
nanc
ing
refe
rs to
fund
s an
d re
sour
ces
iden
tified
, allo
cate
d, d
istr
ibut
ed a
nd e
xecu
ted
on a
ctiv
ities
and
inte
rven
tions
. It d
oes
not t
ake
into
acc
ount
cos
ting
or id
entif
ying
how
man
y re
sour
ces
or fu
nds
are
nece
ssar
y fo
r th
e im
plem
enta
tion
of a
ctiv
ities
or i
nter
vent
ions
.7
-Fun
ding
and
a fi
nanc
ing
mec
hani
sm fo
r res
pond
ing
to p
ublic
hea
lth e
mer
genc
ies,
that
focu
ses
on p
rovi
ding
reso
urce
s to
faci
litat
e th
e su
rge
capa
city
of t
he h
ealth
sys
tem
and
the
depl
oym
ent o
f int
erve
ntio
ns th
at g
o be
yond
the
rout
ine
stru
ctur
e of
the
heal
th s
yste
m. T
his
coul
d in
clud
e le
gisl
atio
n in
pla
ce, s
uch
as a
pub
lic h
ealth
act
and
sta
te e
mer
genc
y ac
t.8
-As
defin
ed b
y th
e co
untr
y th
roug
h a
set o
f trig
gers
that
dec
lare
a s
ituat
ion
as a
pub
lic h
ealth
em
erge
ncy.
9 -A
bud
get l
ine
exis
ts a
nd a
bud
get i
s al
loca
ted
(the
bud
get l
ine
is fu
nded
).10
-Ac
coun
ts h
eld
by g
over
nmen
t bo
dies
, but
not
incl
uded
in t
he g
over
nmen
t bu
dget
. 11
-Fin
anci
ng f
rom
non
-dom
estic
sou
rces
tow
ards
the
impl
emen
tatio
n of
IHR
capa
citie
s th
at u
ses
the
maj
ority
of
natio
nal fi
nanc
ing
for
emer
genc
y pr
epar
edne
ss, d
etec
tion
and
resp
onse
.

INTERNATIONAL HEALTH REGULATIONS (2005)
15 - Joint External Evaluation Tool - Second edition
12 -
Agric
ultu
re, a
nim
al h
ealth
and
hum
an h
ealth
sec
tors
, as
wel
l as
othe
r sec
tors
, who
se a
ctiv
ities
con
trib
ute
to th
e im
plem
enta
tion
of IH
R ca
paci
ties.
The
re is
a c
ruci
al c
ompe
tenc
y on
ope
ratio
nal f
undi
ng in
the
PVS
tool
CC
I-8.
13
-A
gove
rnm
ent b
ody,
mai
nly
min
istr
ies
at th
e na
tiona
l lev
el, b
ut c
ould
incl
ude
othe
r spe
ndin
g ag
enci
es th
at h
ave
spec
ific
year
ly p
ublic
app
ropr
iatio
ns o
r bud
gets
, whi
ch in
clud
e lin
e ite
m e
xpen
ses.
14 -
Com
pris
e in
fect
ious
dis
ease
eve
nts,
incl
udin
g zo
onot
ic d
isea
ses
and
food
saf
ety
even
ts.
15 -
Ther
e is
a s
peci
al s
et o
f pro
cess
es o
r cha
nnel
s in
pla
ce th
at: a
ctiv
ates
a s
peci
al e
mer
genc
y pu
blic
fina
ncin
g m
echa
nism
, allo
ws
for r
apid
rece
ptio
n an
d di
strib
utio
n of
fund
s, a
nd c
ircum
vent
s th
e va
rious
che
cks
and
bala
nces
of
the
norm
al p
ublic
fina
ncin
g m
echa
nism
. 16
- Em
erge
ncy
resp
onse
fina
ncin
g fr
om n
atio
nal/
regi
onal
con
tinge
ncy
fund
s, th
e W
orld
Ban
ks’s
Pan
dem
ic E
mer
genc
y Fi
nanc
ing
Faci
lity,
othe
r mul
tilat
eral
em
erge
ncy
resp
onse
fund
s,
or o
ther
ext
erna
l sou
rces
, are
iden
tified
and
list
ed b
y N
atio
nal I
HR
Foca
l Poi
nts,
and
con
tact
with
foca
l poi
nts
in c
harg
e of
thes
e fu
nds
or e
xter
nal s
ourc
es a
re m
ade
to p
ut in
pla
ce a
ll th
e ne
cess
ary
form
aliti
es in
adv
ance
of p
ublic
he
alth
em
erge
ncie
s.17
- F
or th
e an
imal
hea
lth s
ecto
r, th
is in
form
atio
n ca
n be
foun
d in
the
coun
try
PVS
eval
uatio
n re
port
, CC
IV-1
: Pre
para
tion
of le
gisl
atio
n an
d re
gula
tions
; and
CC
IV-2
: Im
plem
enta
tion
of le
gisl
atio
n an
d re
gula
tions
and
com
plia
nce
ther
eof.
18 -
IHR
capa
citie
s fo
r all
IHR
rela
ted
haza
rds
(che
mic
al, r
adia
tion
and
biol
ogic
al h
azar
ds).
19 -
Diff
eren
t haz
ards
or p
ublic
em
erge
ncie
s in
volv
e di
ffere
nt s
ecto
rs (e
.g. a
vian
influ
enza
invo
lves
min
istr
ies
of a
gric
ultu
re, h
ealth
and
hom
e). T
hose
sec
tors
iden
tified
as
rele
vant
in th
e em
erge
ncy
resp
onse
pla
ns fo
r eac
h ty
pe o
f ha
zard
hav
e bu
dget
line
s in
pla
ce to
rece
ive
and
exec
ute
emer
genc
y fu
ndin
g. T
here
is c
ritic
al c
ompe
tenc
y on
em
erge
ncy
fund
ing
in th
e PV
S to
ol C
C I-
9.20
- T
his
refe
rs to
acc
ess
to fu
nds
by re
leva
nt m
inis
trie
s or
gov
ernm
ent b
odie
s fo
r the
impl
emen
tatio
n of
all
IHR
capa
citie
s. S
uffic
ienc
y is
mea
sure
d, w
here
pos
sibl
e, b
y co
mpa
ring
budg
et a
lloca
tions
am
ount
s to
reso
urce
nee
ds
iden
tified
in n
atio
nal p
lans
rela
ted
to IH
R an
d/or
hea
lth s
ecur
ity.
21 -
A re
leas
e of
ann
ual a
ppro
pria
tion
of fi
nanc
ing,
usu
ally
on
a qu
arte
rly o
r mon
thly
bas
is, f
or th
e m
eetin
g of
fina
ncia
l obl
igat
ions
.22
- T
he re
spon
se to
pub
lic h
ealth
em
erge
ncie
s in
clud
es a
ser
ies
of in
terv
entio
ns, s
uch
as s
uppl
y an
d eq
uipm
ent p
rocu
rem
ent,
hum
an re
sour
ce c
ontr
actin
g an
d de
ploy
men
t, an
d lo
gist
ical
arr
ange
men
ts, a
nd in
volv
e ac
tors
not
us
ually
invo
lved
with
pub
lic s
ecto
r se
rvic
es, s
uch
as N
GO
s an
d th
e pr
ivat
e se
ctor
, whi
ch u
nder
nor
mal
circ
umst
ance
s ca
n ta
ke a
fair
amou
nt o
f wor
k an
d tim
e, a
nd m
ay n
ot e
ven
be p
ossi
ble.
Mec
hani
sms,
incl
udin
g fa
st-t
rack
ex
ecut
ion
proc
edur
es a
nd le
tter
s of
und
erst
andi
ng w
ith n
on-s
tate
act
ors,
nee
d to
be
in p
lace
bef
ore
an e
mer
genc
y oc
curs
, to
allo
w fo
r exp
edite
d sp
endi
ng o
f fun
ds in
suc
h as
pect
s th
at a
re c
ruci
al to
em
erge
ncy
resp
onse
.23
- In
clud
e do
mes
tic fu
ndin
g an
d fu
ndin
g fr
om e
xter
nal s
ourc
es, a
s ap
plic
able
.24
- A
nat
iona
l aut
horit
y ha
s co
ordi
nate
d th
e al
loca
tion
and
exec
utio
n of
fina
ncin
g fo
r act
iviti
es a
nd in
terv
entio
ns to
impl
emen
t IH
R ca
paci
ties.
25 -
To
assu
re a
ccou
ntab
ility
and
gua
rant
ee th
e di
strib
utio
n of
reso
urce
s to
whe
re th
ey a
re m
ost n
eede
d, a
feed
back
mec
hani
sm is
in p
lace
to c
aptu
re a
nd re
port
cha
ngin
g ne
eds
and
prio
ritie
s.26
- A
n em
erge
ncy
cont
inge
ncy
fund
exi
sts
at th
e na
tiona
l, re
gion
al o
r int
erna
tiona
l lev
el, w
ith w
hich
a n
atio
nal a
utho
rity
can
coor
dina
te th
e re
cept
ion
and
dist
ribut
ion
of fu
nds.
PR
EV
EN
T
Cont
extu
al q
uest
ions
:
1.
How
are
the
legi
slat
ion
and
regu
latio
ns d
evel
oped
, rev
iew
ed a
nd o
pera
tiona
lized
in th
e co
untr
y?2.
D
oes
the
vete
rinar
y se
ctor
hav
e le
gisl
atio
n in
pla
ce t
hat
give
s th
em a
utho
rity
to im
pose
qua
rant
ine,
sto
p an
imal
mov
emen
t, eu
than
ize
and
reim
burs
e ow
ners
for t
he v
alue
of a
nim
als/
poul
try
that
are
sac
rifice
d in
ord
er to
con
trol
/era
dica
te a
dis
ease
?3.
W
hat p
roce
sses
and
mec
hani
sms
are
in p
lace
to g
athe
r and
cha
nnel
fina
ncin
g in
resp
onse
to p
ublic
hea
lth e
mer
genc
ies?
4.
Doe
s th
e co
untr
y de
pend
on
outs
ide
sour
ces
of fi
nanc
ing
and
othe
r res
ourc
es fo
r res
pond
ing
to p
ublic
hea
lth e
mer
genc
ies?
5.
Is th
ere
dom
estic
fina
ncin
g in
the
natio
nal b
udge
t for
recu
rren
t or p
redi
ctab
le p
ublic
hea
lth e
mer
genc
ies?
6.
Wha
t is
the
pro
port
ion
of t
he n
atio
nal h
ealth
bud
get
allo
cate
d fo
r pu
blic
hea
lth, f
or IH
R fu
nctio
ns o
r he
alth
sec
urity
rel
ated
act
iviti
es (
i.e. p
reve
ntio
n,
dete
ctio
n an
d re
spon
se)?
7.
Is th
ere
an e
xist
ing
natio
nal p
lan
to s
tren
gthe
n IH
R ca
paci
ties
(nat
iona
l hea
lth s
ecur
ity p
lan,
oth
er),
and
has
this
pla
n be
en fi
nanc
ed?
8.
Is th
ere
a pl
an to
coo
rdin
ate
the
func
tions
and
ope
ratio
ns o
f the
nat
iona
l IH
R w
ith th
e co
untr
y’s
rele
vant
env
ironm
ent a
nd a
gric
ultu
re re
spon
ders
?9.
Is
ther
e co
nsis
tent
and
tim
ely
dist
ribut
ion
of fu
nds
for r
ecur
rent
act
iviti
es th
at a
re p
art o
f an
exis
ting
natio
nal p
lan?
10
. H
ow a
re s
ubna
tiona
l lev
el a
ctiv
ities
fund
ed?
11.
Is th
ere
a fin
anci
al im
plem
enta
tion
mon
itorin
g m
echa
nism
in p
lace
?12
. W
hat m
echa
nism
s ex
ist t
o en
gage
fund
ing
from
the
priv
ate
sect
or?

INTERNATIONAL HEALTH REGULATIONS (2005)
16 - Joint External Evaluation Tool - Second edition
27 -
The
se q
uest
ions
sho
uld
be a
nsw
ered
by
lega
l or l
egis
lativ
e ad
vise
rs, o
r exp
erts
at t
he h
ealth
min
istr
y or
oth
er re
leva
nt g
over
nmen
t offi
ces/
Nat
iona
l IH
R Fo
cal P
oint
s. P
leas
e as
k to
see
the
rele
vant
doc
umen
ts.
28 -
Leg
isla
tion:
sta
te c
onst
itutio
ns, l
aws,
dec
rees
, ord
inan
ces
or s
imila
r leg
al in
stru
men
ts.
PR
EV
EN
T
Tech
nica
l que
stio
ns:
P.1.
1 T
he S
tate
can
dem
onst
rate
that
it h
as a
sses
sed,
adj
uste
d an
d al
igne
d its
dom
estic
legi
slat
ion27
, pol
icie
s an
d ad
min
istr
ativ
e ar
rang
emen
ts in
all
rele
vant
sec
tors
to e
nabl
e co
mpl
ianc
e w
ith th
e IH
R
1.
Is th
ere
legi
slat
ion
or a
re th
ere
regu
latio
ns o
r adm
inis
trat
ive
requ
irem
ents
, or o
ther
gov
ernm
enta
l ins
trum
ents
28 g
over
ning
pub
lic h
ealth
sur
veill
ance
and
re
spon
se?
2.
Do
polic
ies
or re
gula
tions
exi
st fo
r the
use
of d
rugs
and
che
mic
als
that
can
be
part
of p
ublic
hea
lth im
port
ance
, suc
h as
AM
R, in
sect
icid
es?
3.
Has
an
asse
ssm
ent o
f rel
evan
t leg
isla
tions
, reg
ulat
ions
or a
dmin
istr
ativ
e re
quire
men
ts, a
nd o
ther
gov
ernm
enta
l ins
trum
ents
bee
n ca
rrie
d ou
t (to
det
erm
ine
if th
ey fa
cilit
ate
full
impl
emen
tatio
n of
the
IHR)
?4.
D
oes
the
asse
ssm
ent a
lso
iden
tify
area
s fo
r adj
ustm
ent f
or re
leva
nt le
gisl
atio
n, re
gula
tions
, adm
inis
trat
ive
requ
irem
ents
and
oth
er g
over
nmen
t ins
trum
ents
fo
r IH
R im
plem
enta
tion?
5 Is
ther
e ev
iden
ce o
f usi
ng re
leva
nt le
gisl
atio
n an
d po
licie
s in
var
ious
sec
tors
invo
lved
in th
e im
plem
enta
tion
of IH
R? G
ive
exam
ples
of h
ow ri
ghts
cre
ated
by
the
IHR
are
exer
cise
d an
d ho
w IH
R ob
ligat
ions
are
com
plie
d w
ith.
6.
Doe
s th
e co
untr
y’s
legi
slat
ion
or a
ny re
fere
nces
add
ress
add
ition
al s
peci
fic a
reas
oth
er th
an th
e N
atio
nal I
HR
Foca
l Poi
nt fu
nctio
n (d
esig
natio
n an
d its
op
erat
ion)
; if y
es, w
hat a
re th
ose
area
s?7.
W
hat a
re th
e ad
min
istr
ativ
e re
quire
men
ts th
e co
untr
y ha
s id
entifi
ed to
impl
emen
t the
se le
gisl
atio
n an
d/or
regu
latio
ns?
8.
How
doe
s th
e co
untr
y en
sure
the
coor
dina
tion
of le
gal a
nd re
gula
tory
fram
ewor
ks b
etw
een
sect
ors?
(Sho
w e
vide
nce.
)
P.1.
2 Fi
nanc
ing29
is a
vaila
ble
for t
he im
plem
enta
tion
of IH
R ca
paci
ties
1.
Who
is re
spon
sibl
e fo
r fina
ncia
l pla
nnin
g of
ess
entia
l pub
lic h
ealth
func
tions
for h
ealth
sec
urity
incl
udin
g di
seas
e co
ntro
l?2.
Is
ther
e a
budg
et li
ne w
ithin
a m
inis
try
(suc
h as
hea
lth, a
gric
ultu
re, d
efen
ce) a
t the
nat
iona
l lev
el fo
r act
iviti
es re
late
d to
str
engt
heni
ng IH
R co
re c
apac
ities
? If
not,
how
is IH
R im
plem
enta
tion
fund
ed?
3.
Doe
s th
e N
atio
nal S
trat
egic
Hea
lth S
ecto
r Pla
n (N
SHSP
) or o
ther
spe
cific
pla
ns (s
uch
as th
e N
atio
nal A
ctio
n Pl
an fo
r Hea
lth S
ecur
ity, (
NAP
HS)
, or H
ealth
Em
erge
ncy
Prep
ared
ness
Pla
n) in
clud
e th
e pu
blic
hea
lth fu
nctio
ns n
eede
d to
app
ly a
nd c
ompl
y w
ith th
e IH
R?
4.
Are
ther
e an
y m
emor
anda
of u
nder
stan
ding
(MoU
s) o
r oth
er a
gree
men
t(s)
with
par
tner
s to
fina
nce
IHR
core
cap
aciti
es?
If ye
s, w
hat i
s th
e pr
opor
tion
of
finan
cing
from
par
tner
s fo
r IH
R re
late
d fu
nctio
ns?
5.
Is th
ere
a bu
dget
ava
ilabl
e fo
r all
rele
vant
min
istr
ies
for a
ctiv
ities
rela
ted
to s
tren
gthe
ning
and
mai
ntai
ning
IHR
capa
citie
s fo
r all
IHR-
rele
vant
haz
ards
?6.
If
yes,
whi
ch o
f the
min
istr
ies
have
fully
allo
cate
d bu
dget
s, a
nd w
hat a
re th
e po
ssib
le fu
ndin
g lim
itatio
ns?

INTERNATIONAL HEALTH REGULATIONS (2005)
17 - Joint External Evaluation Tool - Second edition
7.
Is e
xter
nal fi
nanc
ing
for t
he im
plem
enta
tion
of IH
R ca
paci
ties
larg
er th
an th
e su
m o
f dom
estic
fina
ncin
g fo
r the
se?
8.
Is th
ere
timel
y di
strib
utio
n of
fund
s fo
r the
exe
cutio
n of
nat
iona
l act
iviti
es to
str
engt
hen
and
mai
ntai
n IH
R ca
paci
ties?
Are
ther
e de
lays
in re
ceiv
ing
fund
s fo
r act
iviti
es to
str
engt
hen
IHR
capa
citie
s?9.
Is
ther
e tim
ely
dist
ribut
ion
of fu
nds
for a
ll m
inis
trie
s or
sec
tors
at a
ll le
vels
of t
he s
yste
m (n
atio
nal a
nd s
ubna
tiona
l)?10
. D
o th
ese
fund
s en
sure
full
impl
emen
tatio
n of
IHR
capa
citie
s?
11.
How
doe
s th
e co
untr
y en
sure
coo
rdin
atio
n of
bud
get p
lann
ing
and
deve
lopm
ent,
amon
g di
ffere
nt m
inis
trie
s an
d re
leva
nt d
epar
tmen
ts?
Doe
s a
natio
nal
auth
ority
coo
rdin
ate
diffe
rent
sec
tors
in th
e im
plem
enta
tion
of IH
R-re
late
d ac
tiviti
es, a
nd th
e di
strib
utio
n an
d ex
ecut
ion
of th
eir fi
nanc
es?
P.1.
3 Fi
nanc
ing
mec
hani
sm a
nd fu
nds
are
avai
labl
e fo
r tim
ely
resp
onse
30 to
pub
lic h
ealth
em
erge
ncie
s
1.
How
are
reso
urce
s m
anag
ed b
y th
e pu
blic
sec
tor
whe
n a
publ
ic h
ealth
em
erge
ncy
occu
rs?
How
are
reso
urce
s co
ntrib
uted
by
exte
rnal
or
priv
ate
acto
rs
gath
ered
and
dis
sem
inat
ed?
2.
Doe
s a
mec
hani
sm w
hich
allo
ws
for
reso
urce
s to
be
dist
ribut
ed fo
r re
spon
ding
to a
pub
lic h
ealth
em
erge
ncy
in a
rap
id m
anne
r, su
pers
edin
g th
e pu
blic
fin
anci
ng m
echa
nism
s, a
nd h
andl
es th
e al
loca
tion
and
dist
ribut
ion
of p
ublic
fund
s fo
r all
non-
emer
genc
y ca
ses,
exi
st?
3.
Whe
n a
publ
ic h
ealth
em
erge
ncy
occu
rs, d
oes
the
coun
try
know
whe
re it
can
imm
edia
tely
acc
ess
mos
t of t
he fi
nanc
ing
need
ed to
resp
ond
to th
e em
erge
ncy?
4.
D
oes
the
coun
try
have
an
agre
emen
t set
up
with
the
Wor
ld B
ank
Pand
emic
Fin
anci
ng F
acili
ty o
r oth
er m
ultil
ater
al e
mer
genc
y fu
ndin
g m
echa
nism
s?5.
Is
the
re a
pub
lic e
ntity
with
res
ourc
e-ra
isin
g re
spon
sibi
litie
s fo
r w
hen
a pu
blic
hea
lth e
mer
genc
y oc
curs
? H
ow d
oes
this
ent
ity r
aise
and
coo
rdin
ate
exte
rnal
ly d
onat
ed fi
nanc
es a
nd re
sour
ces?
Des
crib
e th
e la
st ti
me
this
hap
pene
d.6.
D
oes
each
rele
vant
min
istr
y or
pub
lic e
ntity
hav
e a
budg
et li
ne in
pla
ce fo
r act
iviti
es re
late
d to
resp
ondi
ng to
pub
lic h
ealth
em
erge
ncie
s?
7.
Are
ther
e sp
ecia
l mec
hani
sms
in p
lace
that
allo
w fo
r the
rapi
d ex
ecut
ion
of fu
nds
allo
cate
d fo
r pub
lic h
ealth
em
erge
ncie
s, m
akin
g it
poss
ible
to q
uick
ly
cont
ract
hum
an re
sour
ces,
pro
cure
equ
ipm
ent,
supp
lies
and
com
mod
ities
, mob
ilize
the
dist
ribut
ion
of b
oth
hum
an re
sour
ces
and
com
mod
ities
, am
ong
othe
r nec
essa
ry e
mer
genc
y re
spon
se in
terv
entio
ns, w
ithou
t hav
ing
to g
o th
roug
h th
e st
anda
rd, t
ime-
cons
umin
g pr
oced
ures
that
thes
e no
rmal
ly re
quire
? 8.
Ar
e th
ere
spec
ial m
echa
nism
s in
pla
ce th
at a
llow
for e
xecu
tion
of fu
nds
to g
o to
priv
ate
sect
or o
r non
gove
rnm
enta
l act
ors,
whe
re th
ese
norm
ally
requ
ire
spec
ial p
roce
dure
s or
are
exc
lude
d fr
om th
e pu
blic
pro
visi
on o
f ser
vice
s?9.
H
ow d
oes
the
coun
try
ensu
re c
oord
inat
ion
of fu
ndin
g re
late
d to
resp
onse
to p
ublic
hea
lth e
mer
genc
ies?
Is th
ere
a na
tiona
l aut
horit
y th
at p
rovi
des
over
sigh
t re
gard
ing
the
allo
catio
n an
d ex
ecut
ion
of fi
nanc
ing
in r
espo
nse
to a
pub
lic h
ealth
em
erge
ncy,
coor
dina
tes
the
inte
rven
tions
of
sect
ors
invo
lved
in t
he
resp
onse
, and
exe
cute
s fu
nds
rela
ted
to th
ese?
29 -
Fin
anci
ng re
fers
to fu
nds
and
reso
urce
s id
entifi
ed, a
lloca
ted,
dis
trib
uted
and
exe
cute
d on
act
iviti
es a
nd in
terv
entio
ns. I
t doe
s no
t tak
e in
to a
ccou
nt c
ostin
g or
iden
tifyi
ng h
ow m
any
reso
urce
s or
fund
s ar
e ne
cess
ary
for t
he
impl
emen
tatio
n of
act
iviti
es o
r int
erve
ntio
ns
PR
EV
EN
T

INTERNATIONAL HEALTH REGULATIONS (2005)
18 - Joint External Evaluation Tool - Second edition
10.
Is re
al-t
ime
mon
itorin
g ca
rrie
d ou
t dur
ing
the
resp
onse
to a
pub
lic h
ealth
em
erge
ncy
that
com
mun
icat
es th
e ch
angi
ng re
sour
ce n
eeds
for t
he re
spon
se to
th
e en
titie
s th
at c
oord
inat
e th
e di
strib
utio
n of
fina
nces
bet
wee
n se
ctor
s, le
vels
and
geo
grap
hica
l are
as o
f the
cou
ntry
?11
. Ar
e pr
oced
ures
in p
lace
that
allo
w fo
r rap
id re
-dis
trib
utio
n of
fund
s an
d re
sour
ces
betw
een
sect
ors,
leve
ls o
r geo
grap
hica
l are
as o
f the
cou
ntry
, with
cha
nge
in re
quire
men
ts fo
r res
pond
ing
to a
pub
lic h
ealth
em
erge
ncy
over
tim
e?
Doc
umen
tatio
n or
evi
denc
e fo
r lev
el o
f cap
abili
ty:
l
Leg
isla
tion,
regu
latio
ns, p
olic
ies
and
finan
cial
pla
ns re
late
d to
dis
ease
con
trol
, IH
R, e
tc.
l
Asse
ssm
ent o
r eva
luat
ion
repo
rts
of le
gisl
atio
n, re
gula
tions
pol
icie
s or
pla
nsl
Any
othe
r leg
isla
tion,
regu
latio
ns a
nd/o
r pol
icie
s pe
rtin
ent t
o bi
olog
ical
, che
mic
al a
nd ra
diol
ogic
al h
azar
ds fr
om re
leva
nt s
ecto
rs
30 -
Fun
ding
and
a fi
nanc
ing
mec
hani
sm fo
r res
pond
ing
to p
ublic
hea
lth e
mer
genc
ies,
whi
ch fo
cuse
s on
pro
vidi
ng re
sour
ces
to fa
cilit
ate
the
surg
e ca
paci
ty o
f the
hea
lth s
yste
m a
nd th
e de
ploy
men
t of i
nter
vent
ions
that
go
beyo
nd
the
rout
ine
stru
ctur
e of
the
heal
th s
yste
m. T
his
coul
d in
clud
e le
gisl
atio
n in
pla
ce, s
uch
as a
pub
lic h
ealth
act
and
sta
te e
mer
genc
y ac
t.
PR
EV
EN
T

INTERNATIONAL HEALTH REGULATIONS (2005)
19 - Joint External Evaluation Tool - Second edition
IHR
COO
RDIN
ATIO
N, C
OM
MU
NIC
ATIO
N A
ND
ADV
OCA
CYTa
rget
s: M
ultis
ecto
ral/
mul
tidis
cipl
inar
y ap
proa
ches
thro
ugh
natio
nal p
artn
ersh
ips
that
allo
w e
ffici
ent,
aler
t and
resp
onse
sys
tem
s fo
r effe
ctiv
e im
plem
enta
tion
of th
e IH
R. C
oord
inat
e na
tionw
ide
reso
urce
s, in
clud
ing
sust
aina
ble
func
tioni
ng o
f a N
atio
nal I
HR
Foca
l Poi
nt –
a n
atio
nal c
entr
e fo
r IH
R co
mm
unic
atio
ns w
hich
is
a k
ey o
blig
atio
n of
the
IHR
– th
at is
acc
essi
ble
at a
ll tim
es. S
tate
s Pa
rtie
s pr
ovid
e W
HO
with
con
tact
det
ails
of N
atio
nal I
HR
Foca
l Poi
nts,
con
tinuo
usly
upd
ate
and
annu
ally
con
firm
them
.
As m
easu
red
by: (
1) E
stab
lishm
ent o
f a fu
nctio
nal m
ultis
ecto
ral a
nd m
ultid
isci
plin
ary
mec
hani
sm fo
r the
coo
rdin
atio
n an
d in
tegr
atio
n of
rele
vant
sec
tors
in th
e im
plem
enta
tion
of IH
R an
d to
res
pond
to
any
publ
ic h
ealth
eve
nts.
(2)
Reg
ular
tes
ting
of t
he m
echa
nism
thr
ough
exe
rcis
es a
nd s
ubse
quen
t im
prov
emen
t of
ar
rang
emen
ts a
nd p
roce
dure
s.
Desi
red
impa
ct: A
mec
hani
sm f
or m
ultis
ecto
ral/
mul
tidis
cipl
inar
y co
ordi
natio
n, c
omm
unic
atio
n an
d pa
rtne
rshi
ps t
o de
tect
, ass
ess
and
resp
ond
to a
ny p
ublic
he
alth
eve
nt o
r ris
k. A
Nat
iona
l IH
R Fo
cal P
oint
that
is a
cces
sibl
e at
all
times
to c
omm
unic
ate
with
the
WH
O IH
R Re
gion
al C
onta
ct P
oint
s an
d w
ith a
ll re
leva
nt
sect
ors
and
othe
r sta
keho
lder
s in
the
coun
try.
1 -
Refe
r to
the
Nat
iona
l IH
R Fo
cal P
oint
Gui
de (h
ttp:
//w
ww
.who
.int/
ihr/
publ
icat
ions
/nfp
/en/
, acc
esse
d 20
Nov
embe
r 201
7).
PR
EV
EN
T

INTERNATIONAL HEALTH REGULATIONS (2005)
20 - Joint External Evaluation Tool - Second edition
Scor
eIn
dica
tors
: IH
R co
ordi
natio
n, c
omm
unic
atio
n an
d ad
voca
cy2
P.2.
1 A
func
tiona
l mec
hani
sm e
stab
lishe
d fo
r the
coo
rdin
atio
n an
d in
tegr
atio
n of
rele
vant
sec
tors
in th
e im
plem
enta
tion
of IH
RN
o ca
paci
ty -
1Co
ordi
natio
n m
echa
nism
with
in a
nd b
etw
een
rele
vant
min
istr
ies,
incl
udin
g go
vern
men
t age
ncie
s, is
not
in p
lace
Lim
ited
ca
paci
ty -
2Co
ordi
natio
n m
echa
nism
with
in a
nd b
etw
een
rele
vant
min
istr
ies
is in
pla
ceN
atio
nal s
tand
ard
oper
atin
g pr
oced
ures
(SO
Ps) o
r equ
ival
ent e
xist
s fo
r coo
rdin
atio
n be
twee
n th
e N
atio
nal I
HR
Foca
l Poi
nt a
nd re
leva
nt s
ecto
rsDe
velo
ped
capa
city
- 3
A m
ultis
ecto
ral,
mul
tidis
cipl
inar
y bo
dy, c
omm
ittee
or
task
forc
e ad
dres
sing
IH
R re
quire
men
ts f
or p
ublic
hea
lth e
mer
genc
ies
of n
atio
nal a
nd in
tern
atio
nal
conc
ern
is in
pla
ce a
nd h
as p
artic
ipat
ed in
the
late
st e
vent
or s
imul
atio
n ex
erci
se
Dem
onst
rate
d ca
paci
ty -
4
Mul
tisec
tora
l and
mul
tidis
cipl
inar
y co
ordi
natio
n an
d co
mm
unic
atio
n m
echa
nism
s3 are
in p
lace
, tes
ted
and
upda
ted
regu
larly
thro
ugh
exer
cise
s or
aft
er-a
ctio
n re
view
s ba
sed
on th
e oc
curr
ence
of a
n ac
tual
eve
ntAc
tion
plan
dev
elop
ed to
inco
rpor
ate
less
ons
lear
nt fr
om m
ultis
ecto
ral a
nd m
ultid
isci
plin
ary
coor
dina
tion
and
com
mun
icat
ion
mec
hani
sms
Sust
aina
ble
capa
city
– 5
An
nual
upd
ates
on
the
stat
us o
f IH
R im
plem
enta
tion
to s
take
hold
ers
(incl
udin
g W
HO
and
oth
er IH
R St
ates
Par
ties
acro
ss a
ll re
leva
nt s
ecto
rs) a
re c
ondu
cted
an
d co
nfirm
the
effic
ienc
y an
d ef
fect
iven
ess
of th
e co
ordi
natio
n, c
omm
unic
atio
n an
d ad
voca
cy a
rran
gem
ents
acr
oss
all r
elev
ant s
ecto
rs
Cont
extu
al q
uest
ions
:
1.
How
doe
s th
e co
untr
y co
ordi
nate
with
diff
eren
t min
istr
ies,
incl
udin
g go
vern
men
t age
ncie
s an
d ot
her r
elev
ant s
ecto
rs fo
r hea
lth e
mer
genc
ies
(bef
ore,
dur
ing
and
afte
r an
emer
genc
y)?
Tech
nica
l que
stio
ns:
P.2.
1. A
func
tiona
l mec
hani
sm e
stab
lishe
d fo
r the
coo
rdin
atio
n an
d in
tegr
atio
n of
rele
vant
sec
tors
in th
e im
plem
enta
tion
of IH
R
1.
Are
key
mem
bers
of t
he N
atio
nal I
HR
Foca
l Poi
nt a
ble
to c
omm
unic
ate
effe
ctiv
ely,
in w
ritin
g an
d ve
rbal
ly, w
ith W
HO
and
oth
er in
tern
atio
nal e
xper
ts fo
r re
port
ing
purp
oses
? 2.
Is
ther
e an
upd
ated
con
tact
dire
ctor
y in
clud
ing
all m
embe
rs o
f the
Nat
iona
l IH
R Fo
cal P
oint
?3.
Is
this
mec
hani
sm p
lace
d at
a h
igh
enou
gh le
vel w
ithin
the
gove
rnm
ent s
o th
at a
who
le-o
f-go
vern
men
t app
roac
h ca
n be
take
n?4.
Ar
e th
ere
exam
ples
of
effe
ctiv
e co
ordi
natio
n w
ithin
the
rel
evan
t m
inis
trie
s on
eve
nts
that
may
con
stitu
te a
pub
lic h
ealth
eve
nt o
r ris
k of
nat
iona
l or
inte
rnat
iona
l con
cern
?
2 -
Addi
tiona
l inf
orm
atio
n ca
n be
use
d fr
om th
e fo
llow
ing
indi
cato
rs:
• D.3
.1 S
yste
m fo
r effi
cien
t rep
ortin
g to
Foo
d an
d Ag
ricul
ture
Org
aniz
atio
n (F
AO),
OIE
and
WH
O• D
.3.2
Rep
ortin
g ne
twor
k an
d pr
otoc
ols
with
in th
e co
untr
y• R
.3.1
Pub
lic h
ealth
and
sec
urity
aut
horit
ies
(suc
h as
law
enf
orce
men
t, bo
rder
con
trol
and
cus
tom
s ar
e lin
ked
durin
g a
susp
ect o
r con
firm
ed b
iolo
gica
l eve
nt)
• Rel
evan
t sec
tors
incl
ude
priv
ate
and
publ
ic s
ecto
rs, s
uch
as: a
ll le
vels
of t
he h
ealth
car
e sy
stem
(nat
iona
l, su
bnat
iona
l and
com
mun
ity/p
rimar
y pu
blic
hea
lth);
NG
Os;
div
isio
ns/a
ctiv
ities
of o
ther
sec
tors
whi
ch a
ffect
pub
lic
heal
th, s
uch
as m
inis
trie
s of
agr
icul
ture
(qua
rant
ine
and
mov
emen
t con
trol
aut
horit
y, im
port
/exp
ort r
egul
atio
ns, d
isea
se d
iagn
osis
and
con
trol
fina
ncin
g, z
oono
sis,
vet
erin
ary
labo
rato
ry e
tc.),
tran
spor
t (tr
ansp
ort p
olic
y, ci
vil
avia
tion,
por
ts a
nd m
ariti
me
tran
spor
t), t
rade
and
/or i
ndus
try
(food
saf
ety
and
qual
ity c
ontr
ol),
fore
ign
trad
e (c
onsu
mer
pro
tect
ion,
con
trol
of c
ompu
lsor
y st
anda
rd e
nfor
cem
ent)
, com
mun
icat
ion,
def
ence
, tre
asur
y or
fina
nce
(cus
tom
s), e
nviro
nmen
t, in
terio
r, he
alth
, tou
rism
; hea
lth, t
ouris
m; t
he h
ome
offic
e; m
edia
; and
regu
lato
ry b
odie
s.3
- Th
ere
is c
ritic
al c
ompe
tenc
y on
com
mun
icat
ion
in th
e PV
S to
ol C
C III
-1.
PR
EV
EN
T

INTERNATIONAL HEALTH REGULATIONS (2005)
21 - Joint External Evaluation Tool - Second edition
5.
Are
SOPs
or g
uide
lines
ava
ilabl
e fo
r coo
rdin
atio
n be
twee
n th
e N
atio
nal I
HR
Foca
l Poi
nt a
nd o
ther
rele
vant
act
ors?
6.
Hav
e fu
nctio
nal m
echa
nism
s fo
r m
ultis
ecto
ral c
olla
bora
tion
that
incl
ude
clin
ical
ser
vice
s, a
nim
al a
nd h
uman
hea
lth s
urve
illan
ce u
nits
, com
mun
icat
ion
units
and
labo
rato
ries
been
est
ablis
hed?
7.
Is t
here
tim
ely
and
syst
emat
ic in
form
atio
n ex
chan
ge b
etw
een
Dis
tric
t/Pr
ovin
cial
Hea
lth O
ffice
s, a
nim
al s
urve
illan
ce u
nits
, lab
orat
orie
s, h
uman
hea
lth
surv
eilla
nce
units
and
oth
er re
leva
nt s
ecto
rs re
gard
ing
pote
ntia
l zoo
notic
risk
s an
d ur
gent
/em
ergi
ng z
oono
tic e
vent
s?8.
Is
ther
e a
func
tiona
l mec
hani
sm fo
r mul
tisec
tora
l col
labo
ratio
n w
ith o
ther
rele
vant
sec
tors
for o
ther
IHR
rela
ted
haza
rds,
suc
h as
che
mic
al a
nd ra
diat
ion
sect
ors?
9.
Is th
ere
a co
ordi
natio
n m
echa
nism
for d
etec
ting
and
resp
ondi
ng to
del
iber
ate
and/
or a
ccid
enta
l eve
nts
occu
rrin
g fo
r exa
mpl
e in
mas
s ga
ther
ings
?10
. Is
a m
ultis
ecto
ral,
mul
tidis
cipl
inar
y co
ordi
natio
n an
d co
mm
unic
atio
n m
echa
nism
upd
ated
and
test
ed re
gula
rly?
11.
Are
actio
n pl
ans
deve
lope
d to
inco
rpor
ate
less
ons
lear
nt fr
om m
ultis
ecto
ral/
mul
tidis
cipl
inar
y co
ordi
natio
n an
d co
mm
unic
atio
n m
echa
nism
s?12
. Ar
e th
e up
date
s of
IHR
impl
emen
tatio
n sh
ared
with
oth
er re
leva
nt s
ecto
rs?
13.
Hav
e th
e fu
nctio
ns o
f the
Nat
iona
l IH
R Fo
cal P
oint
bee
n ev
alua
ted
for e
ffect
iven
ess?
Doc
umen
tatio
n or
evi
denc
e fo
r lev
el o
f cap
abili
ty:
l
OIE
PVS
Pat
hway
repo
rts
l
Rep
orts
to W
HO
gov
erni
ng b
odie
s on
IHR
impl
emen
tatio
n (s
uch
as E
xecu
tive
Boar
d an
d W
orld
Hea
lth A
ssem
bly)
l
Leg
isla
tion,
pro
toco
ls o
r oth
er p
olic
ies
rela
ted
to re
port
ing
to W
HO
l
Any
pla
ns th
at h
ave
been
dra
fted
or o
ther
evi
denc
e th
at c
over
s re
spon
se to
pos
sibl
e bi
olog
ical
, che
mic
al a
nd ra
diol
ogic
al e
vent
s
PR
EV
EN
T

INTERNATIONAL HEALTH REGULATIONS (2005)
22 - Joint External Evaluation Tool - Second edition
ANTI
MIC
ROBI
AL R
ESIS
TAN
CETa
rget
: A fu
nctio
nal s
yste
m in
pla
ce fo
r the
nat
iona
l res
pons
e to
com
bat a
ntim
icro
bial
resi
stan
ce (A
MR)
with
a O
ne-H
ealth
app
roac
h, in
clud
ing:
a)
Mul
tisec
tora
l wor
k sp
anni
ng h
uman
, ani
mal
, cro
ps, f
ood
safe
ty a
nd e
nviro
nmen
tal a
spec
ts. T
his
com
pris
es d
evel
opin
g an
d im
plem
entin
g a
natio
nal
actio
n pl
an to
com
bat A
MR,
con
sist
ent w
ith th
e G
loba
l Act
ion
Plan
(GAP
) on
AMR.
b)
Sur
veill
ance
cap
acity
for A
MR
and
antim
icro
bial
use
at t
he n
atio
nal l
evel
, fol
low
ing
and
usin
g in
tern
atio
nally
agr
eed
syst
ems
such
as
the
WH
O G
loba
l An
timic
robi
al R
esis
tanc
e Su
rvei
llanc
e Sy
stem
(GLA
SS) a
nd th
e O
IE g
loba
l dat
abas
e on
use
of a
ntim
icro
bial
age
nts
in a
nim
als.
c)
Pre
vent
ion
of A
MR
in h
ealth
car
e fa
cilit
ies,
food
pro
duct
ion
and
the
com
mun
ity, t
hrou
gh in
fect
ion
prev
entio
n an
d co
ntro
l mea
sure
s.
d) E
nsur
ing
appr
opria
te u
se o
f an
timic
robi
als,
inc
ludi
ng a
ssur
ing
qual
ity o
f av
aila
ble
med
icin
es, c
onse
rvat
ion
of e
xist
ing
trea
tmen
ts a
nd a
cces
s to
ap
prop
riate
ant
imic
robi
als
whe
n ne
eded
, whi
le re
duci
ng in
appr
opria
te u
se.
The
JEE
tool
sho
uld
also
revi
ew a
nd v
alid
ate
the
coun
try’
s se
lf-as
sess
ed re
spon
se to
the
glob
al m
onito
ring
surv
ey o
n AM
R.
As m
easu
red
by: (
1) M
ultis
ecto
ral n
atio
nal a
ctio
n pl
an to
com
bat A
MR
has
been
pro
duce
d an
d m
ade
publ
ic. (
2) Im
plem
enta
tion
of th
e na
tiona
l act
ion
plan
/sec
tor
plan
s on
AM
R, w
ith m
onito
ring
and
year
ly re
port
ing
on p
rogr
ess
(incl
udin
g re
port
ing
to th
e in
tern
atio
nal l
evel
).
Desi
red
impa
ct: D
ecis
ive
and
com
preh
ensi
ve a
ctio
n to
pre
vent
the
em
erge
nce
and
spre
ad o
f AM
R, w
hich
pos
es a
sub
stan
tial a
nd e
volv
ing
thre
at t
o di
seas
e co
ntro
l and
hea
lth s
ecur
ity. C
ount
ries
will
(in
line
with
the
GAP
) in
crea
se a
war
enes
s of
AM
R ris
ks a
nd h
ow t
o re
spon
d to
the
m; s
tren
gthe
n su
rvei
llanc
e an
d la
bora
tory
cap
acity
; enh
ance
infe
ctio
n pr
even
tion
and
cont
rol a
ctiv
ities
; ens
ure
unin
terr
upte
d ac
cess
to e
ssen
tial a
ntim
icro
bial
s of
ass
ured
qua
lity;
regu
late
and
pr
omot
e th
e ap
prop
riate
use
of a
ntim
icro
bial
s in
hum
an m
edic
ine,
vet
erin
ary
med
icin
e, fo
od p
rodu
ctio
n an
d ot
her fi
elds
as
appr
opria
te; a
nd s
uppo
rt in
itiat
ives
to
fost
er th
e de
velo
pmen
t and
app
ropr
iate
use
of n
ew a
ntim
icro
bial
age
nts,
vac
cine
s an
d di
agno
stic
tool
s.
PR
EV
EN
T

INTERNATIONAL HEALTH REGULATIONS (2005)
23 - Joint External Evaluation Tool - Second edition
Scor
e1
Indi
cato
rs: A
ntim
icro
bial
resi
stan
ce (A
MR)
2 P.
3.1
Effe
ctiv
e
mul
tisec
tora
l3 coo
rdin
atio
n on
AM
RP.
3.2
Surv
eilla
nce
of A
MR4
P.3.
3 In
fect
ion
prev
entio
n an
d co
ntro
l5,6
P.3.
4 O
ptim
ize
use
of a
ntim
icro
bial
m
edic
ines
in h
uman
and
ani
mal
he
alth
and
agr
icul
ture
No
capa
city
- 1
No
natio
nal a
ctio
n pl
an fo
r AM
RN
o la
bora
torie
s tha
t con
duct
antib
iotic
su
scep
tibili
ty t
estin
g ar
e ge
nera
ting
data
(an
tibio
tic s
usce
ptib
ility
tes
ting
and
acco
mpa
nyin
g cl
inic
al
and
epid
emio
logi
cal
data
) an
d re
port
ing
on A
MR
No
syst
emat
ic
effo
rts,
na
tiona
l pr
ogra
mm
e, o
r re
spon
sibl
e pe
rson
s fo
r in
fect
ion
prev
entio
n an
d co
ntro
l in
hu
man
he
alth
ca
re
faci
litie
s/to
pr
omot
e in
fect
ion
prev
entio
n an
d pr
even
t tr
ansm
issi
on
of
resi
stan
t ba
cter
ia in
the
anim
al fo
od p
rodu
ctio
n se
ctor
No
or w
eak
polic
y an
d re
gula
tions
on
app
ropr
iate
use
, av
aila
bilit
y an
d qu
ality
of a
ntim
icro
bial
s
Lim
ited
ca
paci
ty -
2
Nat
iona
l AM
R ac
tion
plan
un
der
deve
lopm
ent
or p
lan
invo
lves
onl
y on
e se
ctor
or m
inis
try
Mul
tisec
tora
l co
ordi
natio
n m
echa
-ni
sm h
as b
een
esta
blis
hed,
with
go-
vern
men
t lea
ders
hip
Som
e clin
ical
or r
efer
ence
labo
rato
ries
can
prod
uce
AMR
data
loc
ally
but
na
tiona
l co
ordi
natio
n an
d/or
qua
lity
man
agem
ent d
o no
t yet
exi
st
Nat
iona
l w
ater
, sa
nita
tion
and
hygi
ene
(WAS
H)
and
envi
ronm
enta
l he
alth
sta
ndar
ds e
xist
but
are
not
fu
lly im
plem
ente
dN
atio
nal p
olic
y an
d pl
an a
re a
vaila
ble
for
infe
ctio
n pr
even
tion
and
cont
rol
(IPC)
in
anim
al h
ealth
car
e th
roug
h im
prov
ing
bios
ecur
ity7 ,
anim
al
vacc
inat
ion
and
anim
al h
usba
ndry
Nat
iona
l po
licy
for
anti-
mic
robi
al
gove
rnan
ce a
nd re
gula
tion
deve
lope
d,
that
add
ress
es u
se,
avai
labi
lity
and
qual
ity o
f ant
imic
robi
als
Deve
lope
d ca
paci
ty -
3
Nat
iona
l AM
R ac
tion
plan
dev
elop
ed
that
add
ress
es a
t lea
st h
uman
hea
lth
and
anim
al fo
od p
rodu
ctio
n se
ctor
sM
ultis
ecto
ral c
oord
inat
ion
is fu
nctio
-na
l with
regu
lar m
eetin
gs
Nat
iona
l AM
R su
rvei
llanc
e ac
tiviti
es
are
perf
orm
ed a
ccor
ding
to
natio
nal
stan
dard
s, w
ith a
fun
ctio
nal n
atio
nal
AMR
refe
renc
e la
bora
tory
th
at
part
icip
ates
in
ex
tern
al
qual
ity
assu
ranc
e an
d co
nduc
ts c
onfir
mat
ory
or a
dditi
onal
test
ing
Coun
try
prio
rity
path
ogen
s ha
ve b
een
iden
tified
for s
urve
illan
ce8
Nat
iona
l gu
idel
ines
fo
r IP
C in
an
imal
pro
duct
ion
are
avai
labl
e an
d di
ssem
inat
edSe
lect
ed h
ealth
car
e fa
cilit
ies/
farm
s ar
e im
plem
entin
g th
e gu
idel
ines
, with
m
onito
ring
and
feed
back
in p
lace
All
refe
rral
ho
spita
ls
have
W
ASH
fa
cilit
ies
that
are
fun
ctio
nal,
in l
ine
with
nat
iona
l sta
ndar
ds
Prac
tices
to
assu
re a
ppro
pria
te u
se
are
impl
emen
ted
in s
ome
heal
th c
are
faci
litie
s6,9
Legi
slat
ion
and
regu
latio
ns a
ppro
ved
on i
mpo
rt,
mar
ketin
g au
thor
izat
ion,
pr
oduc
tion
and
use
of a
ntim
icro
bial
sG
uide
lines
fo
r ap
prop
riate
us
e of
an
timic
robi
als
are
avai
labl
e
PR
EV
EN
T
1 -
Sinc
e AM
R ne
eds
to b
e ad
dres
sed
as a
mul
tisec
tora
l iss
ue, t
he fi
rst a
ttrib
ute
(3.1
) ask
s ab
out p
rogr
ess
with
mul
tisec
tora
l coo
rdin
atio
n, in
clud
ing
deve
lopi
ng a
nd im
plem
entin
g a
natio
nal A
MR
actio
n pl
an. I
n or
der
to m
ake
the
asse
ssm
ent a
nd ra
ting
man
agea
ble,
the
attr
ibut
es fo
r sco
ring
are
focu
sing
on
sele
cted
asp
ects
of t
he re
spon
se to
AM
R: s
urve
illan
ce o
f res
ista
nce
(P3.
2), i
nfec
tion
prev
entio
n in
hea
lth c
are
faci
litie
s an
d on
farm
s (P
3.3)
, and
op
timiz
ing
the
use
of a
ntim
icro
bial
s (P
3.4)
, foc
usin
g on
hum
an a
nd a
nim
al h
ealth
sec
tors
onl
y. T
he a
sses
smen
t of c
apac
ities
for A
MR
cont
rol s
houl
d be
com
plet
ed tw
ice
for a
ttrib
utes
3.2
to 3
.4, a
s ca
paci
ties
shou
ld b
e se
para
tely
ev
alua
ted
in th
e hu
man
hea
lth s
ecto
r and
for a
nim
al fo
od p
rodu
ctio
n se
ctor
(ter
rest
rial a
nd a
quat
ic).
Prog
ress
on
addr
essi
ng o
ther
asp
ects
of t
he re
spon
se to
AM
R (in
clud
ing
othe
r sec
tors
) may
als
o be
con
side
red
durin
g th
e JE
E,
but t
hese
asp
ects
are
not
exp
licitl
y ra
ted.
Whe
re th
ere
are
seve
ral c
riter
ia fo
r a s
core
, the
cou
ntry
is e
xpec
ted
to m
eet a
ll th
ese
crite
ria, a
s w
ell a
s th
e cr
iteria
for l
ower
sco
res.
The
fina
l sco
re s
houl
d be
bas
ed o
n th
e lo
wer
of t
he
scor
es fo
r the
hum
an a
nd a
nim
al h
ealth
sec
tors
.2
- In
the
hum
an h
ealth
sec
tor,
the
asse
ssm
ent
shou
ld r
evie
w b
acte
rial r
esis
tanc
e to
ant
ibio
tics.
Vira
l, ot
her
non-
bact
eria
l pat
hoge
n an
d ve
ctor
res
ista
nce
are
out
of s
cope
, unl
ess
inte
grat
ed in
nat
iona
l pol
icie
s, s
tand
ards
or
guid
elin
es. S
yste
ms
for t
rack
ing
hum
an tu
berc
ulos
is re
sist
ance
are
man
aged
thro
ugh
tube
rcul
osis
pro
gram
mes
. For
food
pro
duct
ion
aspe
cts,
all
antim
icro
bial
s ar
e in
clud
ed.

INTERNATIONAL HEALTH REGULATIONS (2005)
24 - Joint External Evaluation Tool - Second edition
Dem
onst
rate
d ca
paci
ty -
4
Mul
tisec
tora
l AM
R ac
tion
plan
ap
prov
ed a
nd re
flect
s G
AP o
bjec
tives
, w
ith
an
oper
atio
nal
plan
an
d m
onito
ring
arra
ngem
ents
Cent
rally
coo
rdin
ated
nat
iona
l AM
R se
ntin
el
surv
eilla
nce
syst
em
that
pr
oduc
es
regu
lar
repo
rts
on
AMR
resi
stan
ce le
vels
Sent
inel
labo
rato
ries
supp
ortin
g AM
R su
rvei
llanc
e th
at f
ollo
w q
ualit
y as
-su
ranc
e pr
oces
ses
and
dem
onst
rate
go
od p
erfo
rman
ce-t
estin
g
Nat
ionw
ide
impl
emen
tatio
n of
IP
C pl
ans
and
guid
elin
es i
n pu
blic
and
pr
ivat
e se
ctor
sAl
l hea
lth ca
re fa
cilit
ies h
ave a
suita
ble
func
tiona
l en
viro
nmen
t (in
clud
ing
wat
er a
nd s
anita
tion
faci
litie
s),
and
nece
ssar
y m
ater
ials
and
equ
ipm
ent
to p
erfo
rm IP
C pe
r nat
iona
l sta
ndar
ds
Prac
tices
to
enab
le a
ppro
pria
te u
se
are
impl
emen
ted
in h
ealth
fac
ilitie
s na
tionw
ide,
for a
ll an
tibio
tics10
Pr
actic
es
on
appr
opria
te
use
in
anim
als
and
crop
s in
line
with
Cod
ex
and
OIE
sta
ndar
ds a
re a
vaila
ble
and
impl
emen
ted
natio
nwid
eRe
leva
nt
legi
slat
ion
has
been
re
view
ed
for
cohe
renc
e;
gaps
/ov
erla
ps/
inco
nsis
tenc
ies
have
bee
n id
entifi
edU
se
of
antim
icro
bial
s fo
r an
imal
gr
owth
pro
mot
ion
has
been
pha
sed
out
Sust
aina
ble
capa
city
– 5
Mul
tisec
tora
l AM
R ac
tion
plan
has
id
entifi
ed f
undi
ng s
ourc
es,
is b
eing
im
plem
ente
d an
d ha
s m
onito
ring
in
plac
e
The
natio
nal
AMR
surv
eilla
nce
sys-
tem
inte
grat
es s
urve
illan
ce o
f AM
R in
pa
thog
ens
of c
once
rn t
o hu
man
and
an
imal
hea
lth a
nd a
gric
ultu
re,
and
gene
rate
s re
gula
r rep
orts
Repo
rts
prov
ide
data
tha
t is
rep
re-
sent
ativ
e of
the
gene
ral p
opul
atio
n
PC is
in p
lace
and
func
tioni
ng a
t na-
tiona
l and
hea
lth fa
cilit
y le
vels
In
fect
ion
prev
entio
n ef
fect
iven
ess
is
regu
larly
eva
luat
ed, w
ith r
esul
ts p
u-bl
ishe
d Pl
ans
and
guid
ance
are
upd
ated
in
resp
onse
to m
onito
ring
Rele
vant
legi
slat
ion
has
been
revi
sed
and
a co
here
nt fr
amew
ork
is in
pla
ce
and
fully
fun
ctio
nal,
so t
hat
only
li-
cens
ed a
nd p
rove
n qu
ality
dru
gs a
re
in u
se
PR
EV
EN
T
3 -
Mul
tisec
tora
l ind
icat
es a
One
Hea
lth (r
efer
to g
loss
ary)
app
roac
h re
pres
enta
tive
of, a
t lea
st, h
uman
, ani
mal
, cro
ps a
nd fo
od s
afet
y as
pect
s.4
- Th
is a
sses
smen
t foc
uses
on
surv
eilla
nce
of A
MR
leve
ls in
hum
an h
ealth
and
ani
mal
food
pro
duct
ion
sect
ors.
Sur
veill
ance
/mon
itorin
g of
ant
imic
robi
al u
se in
hum
ans
and
anim
als
is a
noth
er im
port
ant e
lem
ent o
f nat
iona
l AM
R ac
tion
plan
s, a
nd th
e pl
ans
may
als
o in
clud
e ot
her t
ypes
of s
urve
illan
ce; h
owev
er, w
hile
thes
e m
ay b
e di
scus
sed
durin
g th
e JE
E, th
ey a
re n
ot p
art o
f the
ratin
g.5
- Fo
r th
e hu
man
hea
lth s
ecto
r, at
trib
ute
P3.3
foc
uses
on
infe
ctio
n pr
even
tion
and
cont
rol (
IPC)
in h
ealth
car
e fa
cilit
ies,
whi
le r
ecog
nizi
ng t
hat
prev
entio
n of
infe
ctio
n in
the
com
mun
ity is
als
o cr
itica
l, th
roug
h pu
blic
hea
lth
mec
hani
sms
incl
udin
g im
prov
ing
wat
er a
nd s
anita
tion,
and
incr
easi
ng v
acci
natio
n co
vera
ge. I
PC p
rogr
amm
es in
the
heal
th s
ecto
r ar
e re
com
men
ded
to in
clud
e: d
evel
opm
ent a
nd im
plem
enta
tion
of e
vide
nce-
base
d gu
idel
ines
; ed
ucat
ion
and
trai
ning
of h
ealth
car
e w
orke
rs; s
urve
illan
ce o
f hea
lth c
are
asso
ciat
ed in
fect
ions
; mul
timod
al im
plem
enta
tion
stra
tegi
es; r
egul
ar m
onito
ring,
aud
it an
d fe
edba
ck o
f pra
ctic
es a
t the
faci
lity
leve
l and
nat
iona
l mon
itorin
g w
ith h
and
hygi
ene
as a
key
per
form
ance
indi
cato
r; an
ena
blin
g en
viro
nmen
t inc
ludi
ng b
ed o
ccup
ancy
not
exc
eedi
ng th
e ca
paci
ty o
f the
faci
lity;
hea
lth w
orke
r sta
ffing
acc
ordi
ng to
pat
ient
wor
kloa
d; a
hyg
ieni
c en
viro
nmen
t inc
ludi
ng
wat
er, s
anita
tion
and
hygi
ene
(WAS
H) i
nfra
stru
ctur
e; a
nd a
vaila
bilit
y of
IPC
mat
eria
ls a
nd e
quip
men
t. (S
ee IP
C Co
re C
ompo
nent
s, 2
016
(htt
p://
ww
w.w
ho.in
t/gp
sc/c
ore-
com
pone
nts.
pdf,
acce
ssed
23
Nov
embe
r 201
7).
6 -
For t
he a
nim
al fo
od p
rodu
ctio
n se
ctor
s, th
e fo
cus
of a
ttrib
ute
P3.3
is o
n in
fect
ion
prev
entio
n th
at p
rom
otes
goo
d an
imal
hus
band
ry a
nd a
ims
to re
duce
the
use
of a
ntim
icro
bial
s in
farm
ed a
nim
als
and
food
pro
duct
ion.
Infe
ctio
n pr
even
tion/
good
ani
mal
hus
band
ry p
lans
in th
e an
imal
food
pro
duct
ion
sect
ors
tend
to in
clud
e pr
omot
ion
of fa
rm h
ygie
ne, a
vac
cina
tion
prog
ram
me,
bio
secu
rity
mea
sure
s, a
ppro
pria
te fe
edin
g an
d cl
ean
wat
er, a
nd h
andl
ing
of
sick
ani
mal
s, to
pre
vent
the
tran
smis
sion
of r
esis
tant
bac
teria
to h
uman
s an
d ot
her a
nim
als.
7 -
Bio
secu
rity
in th
e co
ntex
t of A
MR
rela
tes
to th
e pr
even
tion
of d
isea
se tr
ansm
issi
on in
ani
mal
s. It
refe
rs to
a s
et o
f man
agem
ent a
nd
phys
ical
mea
sure
s de
sign
ed to
redu
ce th
e ris
k of
intr
oduc
tion,
est
ablis
hmen
t and
spr
ead
of a
nim
al in
fect
ions
to, f
rom
and
with
in a
n an
imal
pop
ulat
ion
(OIE
Ter
rest
rial A
nim
al H
ealth
Cod
e).
8 - P
riorit
y pa
thog
ens
for s
urve
illan
ce in
hum
an h
ealth
may
incl
ude
som
e, a
ll or
mor
e th
an th
e ei
ght p
atho
gens
(and
bug
-dru
g co
mbi
natio
ns) s
elec
ted
by th
e W
orld
Hea
lth O
rgan
izat
ion
for g
loba
l rep
ortin
g at
the
early
impl
emen
tatio
n st
age
of G
LASS
(Aci
neto
bact
er b
aum
anni
i, Es
cher
ichi
a co
li, K
lebs
iella
pne
umon
ia, S
taph
yloc
occu
s au
reus
, Str
epto
cocc
us p
neum
onia
e, S
alm
onel
la s
pp.,
Shig
ella
spp
, Nei
sser
ia g
onor
rhea
e). P
riorit
y pa
thog
ens
for a
nim
al h
ealth
and
fo
od s
afet
y w
ill b
e de
fined
at t
he g
loba
l lev
el in
201
7. S
urve
illan
ce is
exp
ecte
d to
incl
ude
Salm
onel
la s
pp. O
ther
prio
rity
path
ogen
s m
ay b
e ad
ded
by n
atio
nal a
utho
ritie
s ba
sed
on c
ount
ry n
eeds
.9
- Pr
actic
es m
ay in
clud
e: u
nint
erru
pted
acc
ess
to h
igh-
qual
ity m
edic
ines
to tr
eat b
acte
rial i
nfec
tions
; mea
sure
men
ts o
f ant
imic
robi
al u
se; a
vaila
bilit
y of
cul
ture
s an
d an
tibio
gram
s fo
r clin
ical
dec
isio
n m
akin
g; re
gula
r upd
ates
to
loca
l ant
ibio
gram
s an
d ge
netic
ana
lyse
s to
info
rm tr
eatm
ent d
ecis
ions
; and
aud
it w
ith fe
edba
ck to
pre
scrib
ers
of a
ntib
iotic
s to
enc
oura
ge a
ppro
pria
te u
se. I
n he
alth
car
e, th
ese
are
ofte
n re
ferr
ed to
as
antim
icro
bial
ste
war
dshi
p pr
ogra
mm
es.
10 -
For
the
ani
mal
sec
tor,
avai
labl
e O
IE P
VS P
athw
ay r
epor
ts s
houl
d be
tak
en in
to a
ccou
nt. C
ount
ries
shou
ld a
lso
give
con
side
ratio
n to
the
mos
t re
cent
res
pons
e to
the
trip
artit
e gl
obal
AM
R m
onito
ring
ques
tionn
aire
whe
n un
dert
akin
g th
is a
sses
smen
t. Th
ere
is a
rele
vant
crit
ical
com
pete
ncy
in th
e PV
S to
ol C
C II-
9: V
eter
inar
y m
edic
ines
and
bio
logi
cals
.

INTERNATIONAL HEALTH REGULATIONS (2005)
25 - Joint External Evaluation Tool - Second edition
Cont
extu
al q
uest
ions
: N/A
Tech
nica
l que
stio
ns:
P3.1
Effe
ctiv
e m
ultis
ecto
ral c
oord
inat
ion
on A
MR
and
the
natio
nal a
ctio
n pl
an
1.
How
is m
ultis
ecto
ral w
ork
on A
MR
orga
nize
d? Is
the
re a
n in
ters
ecto
ral c
oord
inat
ion
com
mitt
ee o
r w
orki
ng g
roup
with
defi
ned
term
s of
ref
eren
ce a
nd
repo
rtin
g/ac
coun
tabi
lity
mec
hani
sms?
How
oft
en h
as it
met
and
who
att
ends
the
mee
tings
? 2.
W
hat i
s th
e st
atus
of t
he n
atio
nal a
ctio
n pl
an o
n AM
R? H
as it
bee
n ap
prov
ed fo
rmal
ly?
Are
ther
e se
vera
l pla
ns o
r one
inte
grat
ed p
lan?
Are
food
, agr
icul
ture
an
d en
viro
nmen
t rep
rese
nted
in a
dditi
on to
hum
an a
nd a
nim
al h
ealth
?3.
D
oes
the
natio
nal a
ctio
n pl
an c
onsi
der
the
mai
n ar
eas
iden
tified
in t
he g
loba
l act
ion
plan
on
AMR
– p
artic
ular
ly r
aisi
ng a
war
enes
s, t
rain
ing/
educ
atio
n on
AM
R, s
urve
illan
ce o
f res
ista
nce
and
use,
pre
vent
ion
of in
fect
ions
and
opt
imiz
ing
the
use
of a
ntim
icro
bial
s in
bot
h hu
man
and
vet
erin
ary/
agric
ultu
re
sect
ors?
4.
Is
ther
e an
ope
ratio
nal p
lan
and
budg
et fo
r im
plem
enta
tion
of th
e na
tiona
l act
ion
plan
? H
ow is
fund
ing
for p
lann
ed a
ctiv
ities
org
aniz
ed?
Is th
ere
adeq
uate
in
vest
men
t/fu
ndin
g av
aila
ble
to s
uppo
rt im
plem
enta
tion?
5.
H
as p
rogr
ess
tow
ards
the
obje
ctiv
es/g
oals
laid
out
in th
e pl
an b
een
mon
itore
d ye
t? H
as th
ere
been
pro
gres
s to
war
ds im
plem
enta
tion?
Hav
e an
y ba
rrie
rs
and/
or c
halle
nges
to im
plem
entin
g th
e na
tiona
l act
ion
plan
bee
n id
entifi
ed?
6.
How
doe
s th
e pl
an re
cogn
ize
the
role
s an
d re
spon
sibi
litie
s of
mul
tiple
juris
dict
ions
and
leve
ls o
f gov
ernm
ent?
P.3.
2 An
timic
robi
al re
sist
ance
(AM
R) s
urve
illan
ce
1.
Wha
t is
the
labo
rato
ry c
apac
ity to
det
ect,
isol
ate
and
iden
tify
antim
icro
bial
-res
ista
nt o
rgan
ism
s fr
om h
uman
s, a
nim
als,
food
and
the
envi
ronm
ent?
2.
Is th
ere
a na
tiona
l pla
n/sy
stem
for s
urve
illan
ce o
f inf
ectio
ns c
ause
d by
ant
imic
robi
al-r
esis
tant
pat
hoge
ns?
Is th
ere
mon
itorin
g of
the
surv
eilla
nce
syst
em
to in
form
regu
lar p
lan
revi
ews
and
upda
tes?
3.
H
ow m
any
hosp
itals
(per
cent
age
of to
tal n
umbe
r of h
ospi
tals
) are
(will
be)
site
s fo
r sur
veill
ance
of i
nfec
tions
cau
sed
by a
ntim
icro
bial
-res
ista
nt p
atho
gens
am
ong
hum
ans?
Whi
ch s
peci
men
s, p
atho
gens
and
ant
imic
robi
als
do/w
ill th
ey c
over
? H
ow d
oes
this
com
pare
with
the
plan
for e
nhan
cing
sur
veill
ance
in
hosp
itals
? Ar
e de
nom
inat
or d
ata
(suc
h as
num
ber o
f pat
ient
s w
ith a
spe
cific
dis
ease
or s
yndr
ome,
num
ber o
f pat
ient
s w
ith s
ampl
es ta
ken)
col
lect
ed?
4.
How
will
sur
veill
ance
be
esta
blis
hed/
wha
t is
in p
lace
in th
e co
mm
unity
and
in o
utpa
tient
set
tings
? 5.
H
ow m
any
farm
s (p
erce
ntag
e of
tota
l num
ber
of fa
rms)
with
live
stoc
k ar
e (w
ill b
e) s
entin
el s
ites
for
surv
eilla
nce
of in
fect
ions
cau
sed
by a
ntim
icro
bial
-re
sist
ant p
atho
gens
in li
vest
ock?
a.
Wha
t ani
mal
spe
cies
are
cov
ered
by
AMR
surv
eilla
nce?
b. W
hat z
oono
tic b
acte
rial s
peci
es a
re c
over
ed b
y AM
R su
rvei
llanc
e?c.
Wha
t vet
erin
ary
path
ogen
s ar
e co
vere
d by
AM
R su
rvei
llanc
e?
PR
EV
EN
T

INTERNATIONAL HEALTH REGULATIONS (2005)
26 - Joint External Evaluation Tool - Second edition
d. W
here
is A
MR
surv
eilla
nce
cond
ucte
d in
the
food
cha
in?
On-
farm
, sla
ught
ered
ani
mal
s, re
tail
mea
t?e.
Des
crib
e th
e sa
mpl
ing
sche
me.
i.
Num
ber o
f sam
pled
site
s an
d ho
w th
ey a
re c
hose
n, s
uch
as n
umbe
r of f
arm
s (r
ando
mly
sel
ecte
d, p
urpo
sive
ly s
elec
ted,
con
veni
ence
sam
ple,
cen
sus)
; nu
mbe
r of a
batt
oirs
(how
are
thes
e se
lect
ed?)
; num
ber o
f ret
ail e
stab
lishm
ents
; num
ber/
type
of p
artic
ipat
ing
clin
ical
labo
rato
ries.
ii. H
ow w
ere
the
num
ber a
nd ty
pes
of is
olat
es d
eter
min
ed?
6.
Is t
here
at
leas
t on
e na
tiona
l ref
eren
ce la
bora
tory
11 f
or A
MR?
How
wel
l is
it (a
re t
hey)
fun
ctio
ning
and
sup
port
ing
surv
eilla
nce
site
s? D
oes
it ro
utin
ely
cond
uct c
onfir
mat
ory
or a
dditi
onal
test
ing
on re
ferr
ed is
olat
es?
7.
Does
the
nat
iona
l ref
eren
ce la
bora
tory
rec
eive
sam
ples
from
clin
ics,
hos
pita
ls, v
eter
inar
y di
agno
stic
labo
rato
ries
and
envi
ronm
enta
l sou
rces
(i.e
. wat
er, s
oil,
efflu
ents
)?8.
W
hat
repo
rts
are
avai
labl
e on
leve
ls o
f res
ista
nce
in p
atho
gens
rel
evan
t to
ani
mal
food
pro
duct
ion
and
hum
ans?
Are
the
re n
atio
nal r
epor
ts o
n im
pact
/bu
rden
of A
MR
avai
labl
e? If
rout
ine
repo
rts
are
not a
vaila
ble,
wha
t stu
dies
hav
e be
en d
one
or a
re u
nder
way
? 9.
Is
ther
e a
natio
nal c
oord
inat
ing
cent
re11
est
ablis
hed
that
is p
rodu
cing
repo
rts
on re
sist
ance
leve
ls?
10.
Wha
t typ
es o
f rep
orts
are
gen
erat
ed?
Who
rece
ives
thes
e re
port
s? A
re re
port
s se
nt to
GLA
SS?
Are
repo
rts
acce
ssib
le to
oth
er s
take
hold
ers
(suc
h as
FAO
, OIE
)?11
. D
oes
surv
eilla
nce
of A
MR
inte
grat
e da
ta fr
om b
oth
hum
an a
nd a
nim
al h
ealth
sou
rces
? 12
. H
ow re
pres
enta
tive
is th
e re
port
ed A
MR
data
of t
he c
omm
unity
and
acr
oss
geog
raph
ic a
reas
and
set
tings
? 13
. H
ow h
as th
e da
ta fr
om A
MR
surv
eilla
nce
been
use
d? H
as it
bee
n co
nsid
ered
by
natio
nal p
olic
y m
aker
s? H
ave
loca
l or n
atio
nal t
reat
men
t gui
delin
es b
een
adap
ted?
Hav
e an
y vo
lunt
ary
or le
gisl
ativ
e po
licie
s be
en p
ut in
to p
lace
bas
ed o
n th
e su
rvei
llanc
e da
ta?
14.
Is a
ntim
icro
bial
use
and
/or c
onsu
mpt
ion
mon
itore
d fo
r hum
ans,
ani
mal
s, a
nd fo
od c
rops
? If
yes,
how
?15
. D
oes
the
coun
try
prov
ide
data
to th
e O
IE’s
glo
bal d
atab
ase
on a
ntim
icro
bial
age
nts
used
in a
nim
als?
16.
Is t
here
sur
veill
ance
of
resi
stan
t pa
thog
ens
cont
amin
atio
n oc
curr
ing
via
efflu
ent
disc
harg
es?
At w
hat
leve
ls (
phar
mac
eutic
al in
dust
ry s
ourc
es, h
ealth
cl
inic
s, in
tens
ive
anim
al fe
edin
g or
live
stoc
k si
tes)
are
effl
uent
s m
onito
red?
17
. Is
the
phar
mac
eutic
als
prod
uctio
n in
dust
ry a
ddre
ssed
in th
e na
tiona
l act
ion
plan
? If
yes,
how
?
11 -
Nat
iona
l Ref
eren
ce L
abor
ator
y: th
e pr
imar
y fu
nctio
n w
ithin
the
AMR
surv
eilla
nce
syst
em is
to p
rom
ote
good
mic
robi
olog
ical
labo
rato
ry p
ract
ices
, inc
ludi
ng a
dapt
ing
and
diss
emin
atin
g m
icro
biol
ogic
al m
etho
ds, s
tand
ards
and
pr
otoc
ols
and
to fa
cilit
ate
colla
bora
tion
on a
ll la
bora
tory
mat
ters
rela
ting
to A
MR.
For
sam
ple
term
s of
refe
renc
e se
e G
LASS
gui
de (G
loba
l Ant
imic
robi
al R
esis
tanc
e Su
rvei
llanc
e Sy
stem
(GLA
SS):
guid
e to
upl
oadi
ng a
ggre
gate
d an
timic
robi
al re
sist
ance
dat
a. G
enev
a: W
orld
Hea
lth O
rgan
izat
ion;
201
6 ht
tp:/
/app
s.w
ho.in
t/iri
s/bi
tstr
eam
/106
65/2
5174
0/1/
WH
O-D
GO
-AM
R-20
16.7
-eng
, acc
esse
d 19
Dec
embe
r 201
7).
12 -
Nat
iona
l Coo
rdin
atin
g Ce
ntre
(NCC
) for
AM
R: a
n in
stitu
tion
that
has
bee
n de
sign
ated
by
the
natio
nal a
utho
ritie
s to
ove
rsee
the
dev
elop
men
t an
d fu
nctio
ning
of t
he n
atio
nal A
MR
surv
eilla
nce
syst
em. T
he N
CC w
ill n
eed
a st
ruct
ure
for s
urve
illan
ce c
oord
inat
ion
and
data
man
agem
ent,
and
colla
bora
te c
lose
ly w
ith b
oth
the
Nat
iona
l Ref
eren
ce L
abor
ator
y an
d su
rvei
llanc
e si
tes.
See
GLA
SS g
uide
(Glo
bal A
ntim
icro
bial
Res
ista
nce
Surv
eilla
nce
Syst
em
(GLA
SS):
guid
e to
upl
oadi
ng a
ggre
gate
d an
timic
robi
al re
sist
ance
dat
a. G
enev
a: W
orld
Hea
lth O
rgan
izat
ion;
201
6 ht
tp:/
/app
s.w
ho.in
t/iri
s/bi
tstr
eam
/106
65/2
5174
0/1/
WH
O-D
GO
-AM
R-20
16.7
-eng
, acc
esse
d 19
Dec
embe
r 201
7).
PR
EV
EN
T

INTERNATIONAL HEALTH REGULATIONS (2005)
27 - Joint External Evaluation Tool - Second edition
P.3.
3 In
fect
ion
prev
entio
n an
d co
ntro
l
Hum
an h
ealth
1.
Is th
ere
a na
tiona
l IPC
pro
gram
me
for h
uman
hea
lth, i
nclu
ding
a re
spon
sibl
e pe
rson
and
defi
ned
goal
s an
d st
rate
gies
at t
he n
atio
nal l
evel
?2.
Is
ther
e a
natio
nal p
lan
for I
PC in
hea
lth c
are
sett
ings
? H
ow o
ften
is th
e pl
an u
pdat
ed a
nd re
view
ed?
3.
How
man
y he
alth
car
e fa
cilit
ies
have
dev
elop
ed lo
cal I
PC p
lans
? 4.
W
hich
cor
e co
mpo
nent
s of
IPC
prog
ram
mes
are
par
t of n
atio
nal a
nd h
ealth
car
e fa
cilit
y le
vel I
PC p
lans
? a.
Do
IPC
plan
s in
clud
e gu
idel
ines
and
pro
cedu
res
for a
irbor
ne tr
ansm
issi
on b
ased
pre
caut
ions
? If
not,
whe
re a
re th
ey a
ddre
ssed
? 5.
D
o al
l hos
pita
ls h
ave
IPC
guid
elin
es in
pla
ce in
clud
ing
rout
ine
mon
itorin
g an
d pr
ovis
ion
of fe
edba
ck o
n he
alth
car
e pr
actic
es a
ccor
ding
to IP
C st
anda
rds?
Ar
e th
ere
func
tioni
ng IP
C co
mm
ittee
s at
faci
lity
leve
l?
6.
Are
ther
e de
sign
ated
trai
ned
IPC
prof
essi
onal
s in
eac
h ac
ute
care
faci
lity?
7.
Is
ther
e a
natio
nal o
r sub
natio
nal p
rogr
amm
e on
con
tinui
ng p
rofe
ssio
nal t
rain
ing
for h
ealth
wor
kers
that
incl
udes
key
gui
ding
prin
cipl
es o
f IPC
and
WAS
H?
8.
Is h
and
hygi
ene
com
plia
nce
mea
sure
d an
d fe
edba
ck p
rovi
ded
rout
inel
y at
the
natio
nal l
evel
? Is
ther
e m
onito
ring
to e
nsur
e su
pplie
s of
pre
vent
ive
equi
pmen
t an
d al
coho
l bas
ed h
and
rub?
9.
How
muc
h pr
ogre
ss h
as b
een
mad
e on
ens
urin
g sa
fe w
ater
, san
itatio
n an
d hy
gien
e fa
cilit
ies
in h
ealth
car
e fa
cilit
ies
and
com
mun
ities
? 10
. Is
the
asse
ssm
ent o
f WAS
H in
clud
ed in
ass
essm
ents
of t
he s
afet
y an
d fu
nctio
nalit
y of
hea
lth fa
cilit
ies
for e
mer
genc
ies?
11.
Wha
t sys
tem
s ar
e in
pla
ce a
t nat
iona
l or s
ubna
tiona
l lev
els
to re
gula
rly m
onito
r hea
lth c
are
prac
tices
acc
ordi
ng to
IPC
stan
dard
mea
sure
s, a
nd to
pub
lish
the
resu
lts?
12.
Is th
ere
a na
tiona
l sur
veill
ance
pro
gram
me
for h
ealth
care
-ass
ocia
ted
infe
ctio
ns (H
AI) i
n pl
ace?
How
doe
s H
AI d
ata
info
rm p
olic
y fo
r AM
R pr
even
tion?
Anim
al h
ealth
12.
Is t
here
a n
atio
nal p
lan
for
prev
entin
g in
fect
ious
dis
ease
s in
ani
mal
s? W
hat
mea
sure
s ar
e in
clud
ed (
such
as
bios
ecur
ity, v
acci
ne u
se a
nd c
over
age,
po
stva
ccin
atio
n m
onito
ring,
mar
ket
hygi
ene
SOPs
, far
m id
entifi
catio
n an
d re
gist
ries,
far
m lo
gs, n
atio
nal s
erol
ogic
al s
urve
illan
ce p
lans
, out
brea
k/ev
ent
repo
rtin
g to
nat
iona
l aut
horit
ies/
OIE
)?13
. W
hat s
yste
ms
are
in p
lace
to s
uppo
rt th
e im
plem
enta
tion
of g
ood
anim
al h
usba
ndry
pra
ctic
es, b
iose
curit
y an
d va
ccin
e st
rate
gies
in a
nim
al p
rodu
ctio
n sy
stem
s? A
re t
here
nat
iona
l pla
ns fo
r va
ccin
atio
n in
ani
mal
s (t
erre
stria
l or
aqua
tic)?
Is t
here
a s
yste
m in
pla
ce t
o re
port
ani
mal
dis
ease
s to
vet
erin
ary
serv
ices
? 14
. W
hat i
s th
e ex
tent
of e
xten
sion
ser
vice
s to
farm
ers,
fish
erm
en, l
ives
tock
ow
ners
and
coo
pera
tives
?15
. W
hat s
yste
ms
are
in p
lace
to re
gula
rly e
valu
ate
the
effe
ctiv
enes
s of
infe
ctio
n co
ntro
l mea
sure
s an
d pu
blis
h re
sults
in a
nim
al h
ealth
(suc
h as
use
of t
he O
IE
PVS
tool
)?
PR
EV
EN
T

INTERNATIONAL HEALTH REGULATIONS (2005)
28 - Joint External Evaluation Tool - Second edition
16.
Wha
t alte
rnat
ive
stra
tegi
es a
nd te
chno
logi
es a
re p
ropo
sed
to s
uppo
rt th
e re
duct
ion
of a
ntim
icro
bial
use
in a
nim
al p
rodu
ctio
n sy
stem
s (s
uch
as n
utrit
iona
l st
rate
gies
)?17
. Ar
e th
ere
food
hyg
iene
pra
ctic
es fo
r har
vest
ing
and
proc
essi
ng o
f foo
ds in
pla
ce a
nd fu
nctio
nal?
18.
Is th
ere
a w
aste
wat
er m
anag
emen
t pla
n in
pla
ce a
nd b
eing
impl
emen
ted?
P.3.
4 O
ptim
ize
use
of a
ntim
icro
bial
med
icin
es in
hum
an a
nd a
nim
al h
ealth
and
agr
icul
ture
1.
Wha
t are
the
natio
nal p
olic
ies
and
regu
latio
ns re
latin
g to
app
ropr
iate
use
, ava
ilabi
lity
and
qual
ity o
f ant
imic
robi
als
for h
uman
and
ani
mal
use
? 2.
Is
ther
e na
tiona
l gui
danc
e on
app
ropr
iate
use
of a
ntib
iotic
s in
hum
ans?
a.
Has
the
appr
opria
tene
ss o
f ant
ibio
tic u
se b
een
stud
ied?
Are
stu
dies
pla
nned
, suc
h as
on
qual
ity o
f pre
scrib
ing?
b. I
s th
ere
a na
tiona
l sel
ectio
n m
echa
nism
or c
omm
ittee
for r
ecom
men
ded
antib
iotic
s?
c. A
re th
ere
antib
iotic
gui
delin
es b
ased
on
natio
nal/
loca
l ant
ibio
gram
s? G
ive
exam
ples
. d.
How
man
y ce
ntre
s m
onito
r or a
udit
adhe
renc
e to
nat
iona
l gui
danc
e on
app
ropr
iate
ant
ibio
tic u
se?
e. A
re th
e la
test
gui
delin
es in
tegr
ated
in p
re-s
ervi
ce tr
aini
ng a
nd in
con
tinui
ng e
duca
tion
cour
ses?
3.
Is
a p
resc
riptio
n re
quire
d fo
r ant
ibio
tic u
se in
hum
ans?
Wha
t evi
denc
e is
ther
e th
at th
is a
pplie
s in
pra
ctic
e in
pub
lic a
nd p
rivat
e se
ctor
s?
4.
Doe
s a
natio
nal p
lan
for a
ntim
icro
bial
ste
war
dshi
p ex
ist i
n th
e ho
spita
l sec
tor?
How
far h
as it
bee
n im
plem
ente
d?5.
W
hat m
easu
res
(e.g
. act
ion
on s
tock
-out
s) a
re in
pla
ce to
ass
ure
acce
ss to
ant
imic
robi
als
for t
hose
hum
ans/
anim
als
who
nee
d th
em?
6.
Is a
pre
scrip
tion
requ
ired
for
antim
icro
bial
use
in a
nim
als
(ter
rest
rial,
aqua
tic, f
eed
indu
stry
)? W
hen
is a
pre
scrip
tion
not
requ
ired?
Wha
t ha
ppen
s in
pr
actic
e? D
o fa
rmer
s ha
ve a
cces
s to
vet
erin
aria
ns a
nd o
ther
pro
fess
iona
ls w
ho c
an a
dvis
e/au
thor
ize
an a
ntim
icro
bial
?7.
Is
ther
e a
plan
to s
tren
gthe
n pr
uden
t use
or s
tew
ards
hip
in a
nim
als?
If y
es, w
ho p
artic
ipat
es a
nd h
ow is
it m
onito
red?
Is it
con
sist
ent w
ith C
odex
and
OIE
gu
idel
ines
? H
ave
guid
elin
es o
n pr
uden
t use
bee
n de
velo
ped?
8.
Wha
t is
the
natio
nal p
olic
y on
use
of a
ntim
icro
bial
s fo
r ani
mal
gro
wth
pro
mot
ion?
Wha
t are
the
next
ste
ps p
lann
ed o
n th
ose?
9.
Is
tes
ting
of a
ntim
icro
bial
qua
lity
in p
lace
? Is
the
re a
mec
hani
sm o
r ar
e th
ere
activ
ities
to
iden
tify
subs
tand
ard,
spu
rious
, fal
sely
labe
lled,
fal
sifie
d an
d co
unte
rfei
t ant
imic
robi
als?
Are
ther
e pe
nalti
es fo
r cou
nter
feit/
subs
tand
ard
prod
ucts
and
are
thes
e en
forc
ed?
Doc
umen
tatio
n or
evi
denc
e fo
r lev
el o
f cap
abili
ty:
l
Nat
iona
l ac
tion
plan
for
AM
R an
d/or
pla
ns f
or A
MR
dete
ctio
n/re
port
ing,
sur
veill
ance
of
AMR,
mon
itorin
g an
timic
robi
al c
onsu
mpt
ion
and
use,
IPC
pr
ogra
mm
es in
hum
an h
ealth
faci
litie
s, in
fect
ion
prev
entio
n an
d im
prov
ed h
usba
ndry
in li
vest
ock/
food
pro
duct
ion,
and
pla
ns to
impr
ove
use
and
qual
ity o
f an
timic
robi
als
(suc
h as
ant
imic
robi
al s
tew
ards
hip
prog
ram
mes
).
PR
EV
EN
T

INTERNATIONAL HEALTH REGULATIONS (2005)
29 - Joint External Evaluation Tool - Second edition
l
Mon
itorin
g re
view
s of
pro
gres
s w
ith im
plem
enta
tion
of n
atio
nal a
ctio
n pl
an(s
) and
rela
ted
plan
s.l
Cou
ntry
resp
onse
to th
e gl
obal
mon
itorin
g su
rvey
on
AMR.
l
Ava
ilabl
e O
IE P
VS P
athw
ay re
port
s.l
Min
utes
from
mee
tings
or o
utpu
ts o
f the
mul
tisec
tora
l coo
rdin
atio
n co
mm
ittee
or g
roup
.l
Cop
y of
repo
rts
mea
surin
g:
• pro
port
ion
of A
MR
path
ogen
s am
ong
spec
imen
s or
isol
ates
;
• res
ults
from
par
ticip
atio
n in
inte
rnat
iona
l ext
erna
l qua
lity
asse
ssm
ent (
EQA)
roun
ds o
f the
nat
iona
l ref
eren
ce la
bora
tory
;
• inc
iden
ce o
f inf
ectio
ns c
ause
d by
AM
R pa
thog
ens
at s
entin
el s
ites
(com
mun
ity a
nd h
ospi
tal a
cqui
red)
;
• ant
imic
robi
al c
onsu
mpt
ion
leve
ls o
r sur
veys
of u
se (h
uman
and
ani
mal
incl
udin
g m
edic
ated
ani
mal
feed
– te
rres
tria
l and
aqu
atic
);
• pro
port
ion
of fa
cilit
ies
adhe
ring
to b
est p
ract
ices
for I
PC in
clud
ing
hand
hyg
iene
(if k
now
n);
• m
anda
tory
farm
qua
lity
assu
ranc
e pr
ogra
mm
es th
at in
clud
e an
timic
robi
al u
se s
urve
illan
ce a
nd s
tew
ards
hip
info
rmat
ion;
• a
vaila
bilit
y of
ant
imic
robi
als
(or s
tock
-out
s), h
ygie
ne s
uppl
ies
and
WAS
H in
hea
lth fa
cilit
ies;
and
• p
erce
ntag
e of
ant
ibio
tics
adm
inis
tere
d ap
prop
riate
ly (i
f sur
veye
d).
l
Doc
umen
tatio
n of
the
revi
ew p
roce
ss, i
nclu
ding
par
ticip
atin
g ag
enci
es o
r sec
tors
.
Refe
renc
es:
l
Shar
ing
FAO
too
ls f
or v
eter
inar
y la
bora
tory
ass
essm
ent.
Food
and
Agr
icul
ture
Org
aniz
atio
n [w
ebsi
te] h
ttp:
//w
ww
.fao.
org/
ag/a
gain
fo/p
rogr
amm
es/e
n/em
pres
/new
s_23
1216
b.ht
ml,
acce
ssed
28
Dec
embe
r 201
7)l
Nat
iona
l ant
imic
robi
al re
sist
ance
sur
veill
ance
sys
tem
s an
d pa
rtic
ipat
ion
in th
e G
loba
l Ant
imic
robi
al R
esis
tanc
e Su
rvei
llanc
e Sy
stem
(GLA
SS):
A gu
ide
to
plan
ning
, im
plem
enta
tion
and
mon
itorin
g an
d ev
alua
tion.
Wor
ld H
ealth
Org
aniz
atio
n; 2
016
(htt
p://
apps
.who
.int/
iris/
bits
trea
m/1
0665
/251
554/
1/W
HO
-D
GO
-AM
R-20
16.4
-eng
, acc
esse
d 23
Nov
embe
r 201
7).
l
OIE
dat
a co
llect
ion
tem
plat
e. P
aris
: Wor
ld O
rgan
isat
ion
for
Anim
al H
ealth
; 201
7 (h
ttp:
//w
ww
.oie
.int/
filea
dmin
/Hom
e/en
g/O
ur_s
cien
tific_
expe
rtis
e/do
cs/
pdf/
AMR/
A_AM
Use
_Tem
plat
e_Fi
nal_
2017
.xls
, acc
esse
d 25
Dec
embe
r 201
7).
l
OIE
sta
ndar
ds a
nd r
ecom
men
datio
ns [
fact
shee
t]. P
aris
: W
orld
Org
anis
atio
n fo
r An
imal
Hea
lth;
2016
(ht
tp:/
/ww
w.o
ie.in
t/fil
eadm
in/h
ome/
eng/
Med
ia_
Cent
er/d
ocs/
pdf/
Fact
_she
ets/
EN_N
orm
es.p
df, a
cces
sed
19 D
ecem
ber 2
017)
.l
WH
O
Glo
bal
actio
n pl
an
on
antim
icro
bial
re
sist
ance
. G
enev
a:
Wor
ld
Hea
lth
Org
aniz
atio
n;
2015
(h
ttp:
//ap
ps.w
ho.in
t/iri
s/bi
tstr
eam
/106
65/1
9373
6/1/
9789
2415
0976
3_en
g.pd
f, ac
cess
ed 1
7 D
ecem
ber 2
017)
.l
Gui
delin
es o
n co
re c
ompo
nent
s of
infe
ctio
n pr
even
tion
and
cont
rol p
rogr
amm
es a
t th
e na
tiona
l and
acu
te h
ealth
car
e fa
cilit
y. G
enev
a: W
orld
Hea
lth
Org
aniz
atio
n; 2
016
(htt
p://
ww
w.w
ho.in
t/gp
sc/c
ore-
com
pone
nts.
pdf,
acce
ssed
23
Nov
embe
r 201
7).
PR
EV
EN
T

INTERNATIONAL HEALTH REGULATIONS (2005)
30 - Joint External Evaluation Tool - Second edition
ZOO
NO
TIC
DIS
EASE
Targ
et: F
unct
iona
l mul
tisec
tora
l, m
ultid
isci
plin
ary
mec
hani
sms,
pol
icie
s, s
yste
ms
and
prac
tices
are
in p
lace
to m
inim
ize
the
tran
smis
sion
of z
oono
tic d
isea
ses
from
ani
mal
s to
hum
an p
opul
atio
ns.
As m
easu
red
by: (
1) A
gree
men
t by
the
anim
al h
ealth
and
pub
lic h
ealth
sec
tors
on
a co
mm
on li
st o
f zoo
notic
dis
ease
s/pa
thog
ens
of g
reat
est n
atio
nal p
ublic
hea
lth
conc
ern.
(2) E
xist
ence
of f
unct
iona
l cap
aciti
es in
the
anim
al h
ealth
and
pub
lic h
ealth
sec
tors
and
of c
olla
bora
tion,
coo
rdin
atio
n an
d co
mm
unic
atio
n be
twee
n th
em fo
r pre
pare
dnes
s, d
etec
tion,
ass
essm
ent a
nd re
spon
se to
zoo
notic
dis
ease
s.
Desi
red
impa
ct:
Func
tiona
l an
imal
hea
lth a
nd p
ublic
hea
lth s
yste
ms
wor
k in
divi
dual
ly a
nd c
olla
bora
tivel
y to
geth
er t
hrou
gh d
ocum
ente
d m
echa
nism
s an
d op
erat
iona
l fra
mew
orks
, usi
ng a
One
Hea
lth a
ppro
ach
and
base
d on
inte
rnat
iona
l sta
ndar
ds, g
uida
nce
and
best
pra
ctic
es, t
o m
inim
ize
the
tran
smis
sion
of
zoon
otic
dis
ease
s to
hum
an p
opul
atio
ns.
PR
EV
EN
T

INTERNATIONAL HEALTH REGULATIONS (2005)
31 - Joint External Evaluation Tool - Second edition
Scor
e1
Zoon
otic
dis
ease
2,3
P.4.
1 Co
ordi
nate
d su
rvei
llanc
e4 sy
stem
s in
pla
ce i
n th
e an
imal
hea
lth a
nd
publ
ic h
ealth
sec
tors
for
zoo
notic
dis
ease
s/pa
thog
ens
iden
tified
as
join
t pr
iorit
ies5
P.4.
2 M
echa
nism
s fo
r re
spon
ding
to
infe
ctio
us a
nd p
oten
tial
zoon
otic
di
seas
es e
stab
lishe
d an
d fu
nctio
nal
No
capa
city
- 1
Som
e ca
paci
ties
for
surv
eilla
nce
of z
oono
tic d
isea
ses
exis
t bu
t ar
e no
t or
gani
zed
betw
een
the
anim
al h
ealth
or p
ublic
hea
lth s
yste
mD
espi
te s
ome
mec
hani
sms
for s
peci
fic d
isea
ses/
path
ogen
s, n
o co
ordi
nate
d re
spon
se m
echa
nism
for z
oono
tic d
isea
ses
is in
pla
ce
Lim
ited
ca
paci
ty -
2
Coun
try
has
a lis
t of fi
ve p
riorit
y zo
onot
ic d
isea
ses/
path
ogen
s ag
reed
am
ong
sect
ors
to b
e of
gre
ates
t nat
iona
l pub
lic h
ealth
con
cern
but
doe
s no
t hav
e a
spec
ific
syst
em fo
r the
ir su
rvei
llanc
e in
pla
ce
Doc
umen
ted
mul
tisec
tora
l nat
iona
l pol
icy,
stra
tegy
and
/or p
lan
for r
espo
nse
to z
oono
tic e
vent
s ha
ve b
een
elab
orat
ed
Deve
lope
d ca
paci
ty -
3
Zoon
otic
sur
veill
ance
sys
tem
s in
pla
ce f
or o
ne t
o fo
ur z
oono
tic d
isea
ses/
path
ogen
s of
gre
ates
t pub
lic h
ealth
con
cern
An e
stab
lishe
d m
ultis
ecto
ral
oper
atio
nal
mec
hani
sm f
or c
oord
inat
ed r
es-
pons
e to
out
brea
ks o
f zoo
notic
dis
ease
s by
hum
an, a
nim
al a
nd w
ildlif
e se
c-to
rs is
in p
lace
Dem
onst
rate
d ca
paci
ty -
4
Zoon
otic
sur
veill
ance
sys
tem
s in
pla
ce f
or fi
ve o
r m
ore
prio
rity
zoon
otic
di
seas
es/p
atho
gens
of g
reat
est p
ublic
hea
lth c
once
rnSe
vera
l exp
erie
nces
of r
espo
nse
to z
oono
tic e
vent
s co
nfirm
“tim
elin
ess”
6 an
d ef
ficie
ncy
of t
he m
ultis
ecto
ral
oper
atio
nal
mec
hani
sm, i
nclu
ding
sys
tem
a-tic
info
rmat
ion
exch
ange
bet
wee
n an
imal
/wild
life
surv
eilla
nce
units
, hum
an
heal
th s
urve
illan
ce u
nits
and
oth
er re
leva
nt s
ecto
rs7,
8
Sust
aina
ble
capa
city
- 5
Rout
ine
shar
ing
of i
nfor
mat
ion
betw
een
the
sect
ors
ensu
res
a co
nfirm
ed
surv
eilla
nce
syst
em fo
r zoo
notic
dis
ease
s of
prio
rity
and/
or o
ther
sTh
e m
ultis
ecto
ral o
pera
tiona
l mec
hani
sm fo
r the
resp
onse
to z
oono
tic e
vent
s an
d em
ergi
ng d
isea
ses
is re
gula
rly te
sted
for c
ontin
uous
impr
ovem
ent
1 -
For f
ull s
core
s, c
apab
ilitie
s sh
ould
be
sepa
rate
ly e
valu
ated
bot
h in
the
hum
an a
nd a
nim
al (l
ives
tock
, com
pani
on a
nim
al a
nd w
ildlif
e) h
ealth
sec
tors
and
mec
hani
sms
for r
egul
ar jo
int p
lann
ing,
sha
ring
of in
form
atio
n, c
olla
bora
tion,
co
mm
unic
atio
n an
d jo
int p
olic
y-de
velo
pmen
t in
a O
ne H
ealth
app
roac
h sh
ould
be
in p
lace
. The
fina
l sco
re s
houl
d be
bas
ed o
n th
e lo
wer
of t
he s
core
s fo
r the
hum
an a
nd a
nim
al h
ealth
sec
tors
.2
- Zo
onot
ic d
isea
ses
is a
n in
fect
ion
or d
isea
ses
that
is tr
ansm
issi
ble
betw
een
anim
als
and
hum
ans.
3 -
Also
see
sec
tion
on F
ood
safe
ty in
dica
tors
for f
urth
er in
form
atio
n.4
- Su
rvei
llanc
e re
fers
to d
isea
ses
on th
e ag
reed
list
of p
riorit
y zo
onos
es. I
f the
re is
no
list,
it re
fers
to s
urve
illan
ce fo
r dis
ease
s on
the
list o
f prio
rity
zoon
oses
of t
he p
ublic
hea
lth s
ecto
r.5
- Th
e in
dica
tor r
efer
s to
the
natio
nal c
apac
ity to
det
ect,
asse
ss a
nd re
spon
d to
zoo
notic
dis
ease
s, a
nd in
clud
es c
onsi
dera
tion
of th
e an
imal
hea
lth a
nd h
uman
hea
lth s
ecto
r cap
acity
, as
wel
l as
the
colla
bora
tive
mec
hani
sm b
etw
een
them
.6
- Ti
mel
ines
s is
judg
ed a
nd d
eter
min
ed b
y ea
ch c
ount
ry a
nd is
refe
rred
to h
ere
as th
e tim
e be
twee
n de
tect
ion
and
resp
onse
.7
- Re
leva
nt s
ecto
rs: A
t min
imum
, the
min
istr
ies
or a
genc
ies
that
are
key
to th
e te
chni
cal a
rea
and
may
incl
ude
hum
an h
ealth
, ani
mal
hea
lth, e
nviro
nmen
t, fo
od s
afet
y, fin
ance
, tra
de/p
orts
of e
ntry
, che
mic
al s
afet
y, ra
diat
ion
safe
ty,
secu
rity,
defe
nce,
priv
ate
sect
or, r
egul
ator
y bo
dies
, med
ia a
mon
g ot
hers
. Civ
il as
soci
atio
ns, s
uch
as p
rivat
e st
akeh
olde
rs (f
rom
indu
stry
, med
ical
ass
ocia
tions
, far
mer
s as
soci
atio
ns) a
nd a
cade
mia
resp
onsi
ble
for a
spec
ts o
f the
te
chni
cal a
rea
(but
not
key
) may
be
incl
uded
as
need
ed.
8 -
Link
ages
bet
wee
n m
inis
trie
s of
hea
lth a
nd a
gric
ultu
re, a
nd w
ildlif
e sp
ecia
lists
to p
rom
ote
the
shar
ing
of in
form
atio
n an
d da
ta s
houl
d be
effi
cien
t and
als
o ex
ist a
t the
regi
onal
and
loca
l lev
els.
Cont
extu
al q
uest
ions
:1.
Fo
r whi
ch o
f the
zoo
notic
dis
ease
s of
gre
ates
t pub
lic h
ealth
con
cern
with
in th
e co
untr
y is
it a
ssum
ed th
at th
e pr
iorit
ized
list
of z
oono
tic d
isea
ses
for t
he
coun
try
is b
ased
on
an in
ters
ecto
ral d
ecis
ion
mak
ing
proc
ess?
a. W
hat p
roce
ss w
as u
sed
to d
evel
op th
e lis
t of z
oono
tic d
isea
ses
of g
reat
est p
ublic
hea
lth c
once
rn?
Did
the
proc
ess
incl
ude
anim
al h
ealth
, as
wel
l as
envi
ronm
enta
l and
oth
er re
leva
nt s
ecto
rs?
2.
Is th
ere
a fo
rmal
mul
tisec
tora
l pol
icy
for c
olla
bora
tion
on z
oono
tic d
isea
ses
in th
e co
untr
y? If
so,
how
is it
org
aniz
ed/l
ed/g
over
ned?
PR
EV
EN
T

INTERNATIONAL HEALTH REGULATIONS (2005)
32 - Joint External Evaluation Tool - Second edition
9 -
In th
is in
dica
tor,
agric
ultu
re m
inis
try
refe
rs to
that
min
istr
y or
age
ncy
resp
onsi
ble
for a
nim
al h
ealth
and
pro
duct
ion.
The
agr
icul
ture
min
istr
y (o
r oth
er re
leva
nt a
genc
y) c
an p
rovi
de a
n ac
cura
te d
escr
iptio
n of
ani
mal
dem
ogra
phic
s w
ithin
the
coun
try
and
with
in e
ach
adm
inis
trat
ive
unit.
3.
Is th
ere
a na
tiona
l mul
tisec
tora
l coo
rdin
atio
n co
mm
ittee
for
one
or m
ore
zoon
otic
dis
ease
s ho
ldin
g re
gula
r m
eetin
gs c
urre
ntly
? If
so, w
hich
is th
e le
ad
agen
cy?
4.
Is th
ere
a m
echa
nism
for j
oint
risk
ass
essm
ent f
or z
oono
tic d
isea
se e
vent
s?5.
W
ithin
the
past
two
year
s, h
as a
n ex
erci
se b
een
cond
ucte
d or
a re
al e
vent
occ
urre
d in
volv
ing
the
min
istr
ies
of h
ealth
and
agr
icul
ture
to p
ract
ice
and
test
th
e sk
ills
of p
ublic
hea
lth w
orke
rs in
bot
h hu
man
and
ani
mal
sec
tors
to in
vest
igat
e an
d re
spon
d to
a z
oono
tic e
vent
? a.
Des
crib
e th
e ex
erci
se o
r rea
l eve
nt th
at o
ccur
red.
b. W
hat w
ere
the
mos
t sig
nific
ant l
esso
ns le
arne
d fr
om th
e ex
erci
se/r
eal e
vent
? 6.
Li
st th
e zo
onot
ic d
isea
ses
for w
hich
con
trol
pol
icie
s ex
ist w
ith th
e pu
rpos
e of
redu
cing
thei
r spr
ead
into
hum
an p
opul
atio
ns?
a. D
escr
ibe
the
prog
ress
in im
plem
entin
g th
ese
polic
ies.
b. I
s th
ere
a pl
an in
pla
ce to
enc
oura
ge re
port
ing
of a
nim
al d
isea
se (m
ay in
clud
e in
dem
nitie
s pa
id)?
c. I
s th
ere
a pl
an in
pla
ce to
add
ress
fact
ors
that
may
pre
vent
farm
ers/
owne
rs fr
om re
port
ing
anim
al d
isea
se (m
ay in
clud
e la
ck o
f fam
iliar
ity w
ith re
port
ing
proc
ess,
lack
of i
ndem
nity
, soc
ial s
tigm
a)?
7.
Has
ther
e be
en a
n O
IE P
VS e
valu
atio
n m
issi
on o
r PVS
Gap
Ana
lysi
s? If
so,
wha
t yea
r(s)
was
it h
eld?
8.
H
as th
ere
been
an
IHR-
PVS
Nat
iona
l Brid
ging
Wor
ksho
p or
oth
er “O
ne H
ealth
” rel
ated
wor
ksho
ps fo
r rel
evan
t min
istr
ies?
If s
o, m
entio
n w
hich
one
(s).
Tech
nica
l que
stio
ns:
P.4.
1 Su
rvei
llanc
e sy
stem
s in
pla
ce fo
r prio
rity
zoon
otic
dis
ease
s/pa
thog
ens
1.
Des
crib
e th
e sy
stem
/mec
hani
sm b
y w
hich
sur
veill
ance
act
iviti
es a
re p
lann
ed a
nd im
plem
ente
d co
ncur
rent
ly b
y th
e an
imal
hea
lth a
nd h
uman
hea
lth s
ecto
rs.
2.
Doe
s th
e co
untr
y ha
ve a
n ag
reed
list
of p
riorit
y zo
onot
ic d
isea
ses?
3.
Doe
s th
e co
untr
y ha
ve a
sur
veill
ance
sys
tem
in p
lace
on
rele
vant
ani
mal
pop
ulat
ions
for t
hese
prio
rity
zoon
otic
dis
ease
s?
4.
Doe
s th
e co
untr
y ha
ve a
hum
an s
urve
illan
ce s
yste
m in
pla
ce fo
r the
se d
isea
ses?
5.
Des
crib
e pa
rtne
rshi
ps b
etw
een
the
min
istr
ies
of h
ealth
and
agr
icul
ture
9 an
d ot
her
rele
vant
age
ncie
s in
clud
ing
biol
ogic
al s
peci
alis
ts, a
cade
mia
, wild
life
spec
ialis
ts a
nd e
nviro
nmen
tal g
roup
s as
they
rela
te to
zoo
notic
dis
ease
det
ectio
n an
d re
spon
se.
a. A
re s
ituat
iona
l aw
aren
ess
repo
rts
or re
port
s of
pot
entia
l dis
ease
out
brea
ks s
hare
d be
twee
n th
e ag
enci
es?
6.
Do
publ
ic h
ealth
labo
rato
ries
and
anim
al h
ealth
labo
rato
ries
com
mun
icat
e w
ith e
ach
othe
r?
a. I
s th
ere
a pr
oces
s fo
r sha
ring
uniq
ue o
r ser
ious
isol
ates
bet
wee
n pu
blic
hea
lth a
nd a
nim
al h
ealth
labo
rato
ries?
b. I
s th
ere
a pr
oces
s fo
r sha
ring
biol
ogic
al s
peci
men
s be
twee
n pu
blic
hea
lth a
nd a
nim
al h
ealth
labo
rato
ries?
c. I
s th
ere
a pr
oces
s fo
r sha
ring
labo
rato
ry re
port
s or
ale
rts
betw
een
publ
ic h
ealth
and
ani
mal
hea
lth la
bora
torie
s?d.
Are
thes
e re
port
s sh
ared
on
a re
gula
r bas
is, o
r onl
y w
hen
zoon
otic
dis
ease
s ar
e di
scov
ered
or s
uspe
cted
?
PR
EV
EN
T

INTERNATIONAL HEALTH REGULATIONS (2005)
33 - Joint External Evaluation Tool - Second edition
7. D
escr
ibe
the
exch
ange
of e
pide
mio
logi
cal r
epor
ts.
a. H
ow o
rgan
ized
is th
e ex
chan
ge o
f epi
dem
iolo
gica
l rep
orts
on
zoon
otic
dis
ease
s?b.
How
are
ani
mal
sur
veill
ance
sys
tem
s lin
ked
to s
urve
illan
ce s
yste
ms
used
for h
uman
pat
hoge
ns?
c. I
s th
ere
a pr
oces
s fo
r sha
ring
surv
eilla
nce
repo
rts
betw
een
publ
ic h
ealth
and
ani
mal
hea
lth la
bora
torie
s?
P.4.
2 M
echa
nism
s fo
r res
pond
ing
to in
fect
ious
and
pot
entia
l zoo
notic
dis
ease
s es
tabl
ishe
d an
d fu
nctio
nal
1. D
escr
ibe
the
polic
y, st
rate
gy o
r pla
n fo
r res
pond
ing
to z
oono
tic e
vent
s in
the
coun
try
in th
e an
imal
hea
lth a
nd p
ublic
hea
lth s
ecto
rs.
a. I
s th
ere
a jo
int p
lan
or s
trat
egy
that
exi
sts
betw
een
hum
an h
ealth
and
ani
mal
hea
lth (i
nclu
ding
wild
life)
sec
tors
?b.
Is
ther
e an
y M
oU b
etw
een
the
sect
ors
for t
he m
anag
emen
t of z
oono
tic e
vent
s?2.
D
escr
ibe
how
the
late
st z
oono
tic e
vent
s w
ere
man
aged
, for
exa
mpl
e:a.
How
was
the
info
rmat
ion
shar
ed b
etw
een
sect
ors?
b. H
ow o
ften
did
the
sect
ors
mee
t at t
he te
chni
cal l
evel
? c.
Are
ther
e ou
tbre
ak in
vest
igat
ion
and
resp
onse
repo
rts
on th
e la
test
zoo
notic
eve
nts?
3.
Are
ther
e an
y m
echa
nism
s fo
r est
ablis
hing
inte
rage
ncy
resp
onse
team
s in
the
even
t of a
sus
pect
ed z
oono
tic o
utbr
eak?
4.
Des
crib
e th
e ro
les
and
resp
onsi
bilit
ies
of h
uman
hea
lth a
nd a
nim
al h
ealth
(inc
ludi
ng w
ildlif
e) s
ecto
rs o
n th
ese
rece
nt z
oono
tic e
vent
s.5.
D
oes
the
coun
try
have
cap
acity
to re
spon
d to
mor
e th
an 8
0% o
f zoo
notic
eve
nts
on ti
me?
Wha
t is
the
timel
ines
s at
pre
sent
?6.
D
oes
the
coun
try
have
a p
repa
redn
ess
plan
for h
andl
ing
emer
ging
or r
e-em
ergi
ng z
oono
tic d
isea
ses
with
ver
ifica
tion?
Doc
umen
tatio
n or
evi
denc
e fo
r lev
el o
f cap
abili
ty:
l
Agr
eed
list o
f zoo
notic
prio
rity
path
ogen
s in
pub
lic h
ealth
l
Des
crip
tions
of e
xist
ing
zoon
otic
sur
veill
ance
sys
tem
sl
OIE
cou
ntry
PVS
Pat
hway
mis
sion
repo
rt
Refe
renc
es:
l
OIE
PVS
Pat
hway
mis
sion
repo
rts.
Wor
ld O
rgan
isat
ion
for A
nim
al H
ealth
[web
site
] (ht
tp:/
/ww
w.o
ie.in
t/su
ppor
t-to
-oie
-mem
bers
/pvs
-pat
hway
/, ac
cess
ed
23 N
ovem
ber 2
017)
.l
Han
dboo
k fo
r th
e as
sess
men
t of
cap
aciti
es a
t th
e hu
man
–an
imal
inte
rfac
e. G
enev
a: W
orld
Hea
lth O
rgan
izat
ion;
201
7 (h
ttp:
//ap
ps.w
ho.in
t/iri
s/bi
tstr
eam
/106
65/2
5455
2/1/
9789
2415
1188
9-en
g.pd
f?ua
=1, a
cces
sed
27 D
ecem
ber 2
017)
.l
Pub
licat
ions
on
food
saf
ety
and
rela
ted
area
s. W
orld
Hea
lth O
rgan
izat
ion
[web
site
] (ht
tp:/
/ww
w.w
ho.in
t/fo
odsa
fety
/pub
licat
ions
/all/
en/,
acce
ssed
23
Nov
embe
r 201
7).
PR
EV
EN
T

INTERNATIONAL HEALTH REGULATIONS (2005)
34 - Joint External Evaluation Tool - Second edition
FOO
D S
AFET
YTa
rget
: Fun
ctio
naf s
yste
m is
in p
lace
for s
urve
illan
ce a
nd re
spon
se c
apac
ity o
f Sta
tes
Part
ies
for f
oodb
orne
dis
ease
and
food
con
tam
inat
ion
risks
or e
vent
s w
ith
effe
ctiv
e co
mm
unic
atio
n an
d co
llabo
ratio
n am
ong
the
sect
ors
resp
onsi
ble
for f
ood
safe
ty.
As m
easu
red
by: (
1) E
xist
ence
of i
ndic
ator
-bas
ed d
isea
se s
urve
illan
ce (I
BS)
or e
vent
-bas
ed d
isea
se s
urve
illan
ce (E
BS)
and
supp
ortin
g la
bora
tory
ana
lysi
s to
de
tect
and
ass
ign
aetio
logy
for f
oodb
orne
dis
ease
s or
orig
in o
f con
tam
inat
ion
even
t, an
d in
vest
igat
ion
of h
azar
ds in
food
s lin
ked
to c
ases
, out
brea
ks o
r eve
nts.
(2)
Exis
tenc
e of
a n
atio
nal f
ood
safe
ty e
mer
genc
y pl
an. (
3) E
xist
ence
of a
des
igna
ted
Inte
rnat
iona
l Foo
d Sa
fety
Aut
horit
ies
Net
wor
k (IN
FOSA
N) E
mer
genc
y Co
ntac
t Po
int,
and
the
OIE
Foc
al P
oint
on
Anim
al P
rodu
ctio
n Fo
od S
afet
y w
ith a
cen
tral
coo
rdin
atio
n m
echa
nism
in p
lace
.
Desi
red
impa
ct: T
imel
y de
tect
ion
and
effe
ctiv
e re
spon
se o
f pot
entia
l foo
d-re
late
d ev
ents
in c
olla
bora
tion
with
oth
er s
ecto
rs re
spon
sibl
e fo
r foo
d sa
fety
.
PR
EV
EN
T

INTERNATIONAL HEALTH REGULATIONS (2005)
35 - Joint External Evaluation Tool - Second edition
Scor
eIn
dica
tors
: Foo
d sa
fety
1 P.
5.1
Surv
eilla
nce
syst
ems
in p
lace
for
the
det
ectio
n an
d m
onito
ring
of
food
born
e di
seas
es a
nd fo
od c
onta
min
atio
nP.
5.2
Mec
hani
sms
are
esta
blis
hed
and
func
tioni
ng f
or t
he r
espo
nse
and
man
agem
ent o
f foo
d sa
fety
em
erge
ncie
s
No
capa
city
- 1
No
or v
ery
limite
d su
rvei
llanc
e sy
stem
in p
lace
for f
oodb
orne
dis
ease
s or
for
food
con
tam
inat
ion
(che
mic
al a
nd m
icro
biol
ogic
al) m
onito
ring
No
or v
ery
limite
d m
echa
nism
in p
lace
Lim
ited
ca
paci
ty -
2Co
untr
y ha
s IB
S or
EBS
and
mon
itorin
g sy
stem
s in
pla
ce t
o m
onito
r tr
ends
an
d de
tect
food
born
e ev
ents
(out
brea
k or
con
tam
inat
ion)
Coun
try
has
a na
tiona
l fo
od
safe
ty
emer
genc
y pl
an
with
fo
od
safe
ty
emer
genc
ies
defin
ed to
ser
ve a
s a
trig
ger f
or e
scal
atin
g ap
prop
riate
resp
onse
Deve
lope
d ca
paci
ty -
3
IBS
or E
BS s
yste
m i
nclu
des
labo
rato
ry a
naly
sis
to a
ssig
n ae
tiolo
gy f
or
food
born
e di
seas
es o
r orig
in o
f con
tam
inat
ion
even
t, an
d in
vest
igat
e ha
zard
s in
food
s lin
ked
to c
ases
, out
brea
ks o
r eve
nts
Coun
try
has
a na
tiona
l foo
d sa
fety
em
erge
ncy
plan
and
a d
esig
nate
d IN
FOSA
N
Emer
genc
y Co
ntac
t Po
int,
with
a c
entr
al c
oord
inat
ion
mec
hani
sm in
pla
ce
that
incl
udes
all
rele
vant
sec
tors
with
fun
ctio
nal a
rran
gem
ents
in p
lace
for
im
plem
enta
tion
of re
spon
se in
the
even
t of a
food
saf
ety
emer
genc
yDe
mon
stra
ted
capa
city
– 4
Coun
try
has
capa
city
to u
nder
take
rapi
d ris
k as
sess
men
ts o
f acu
te fo
odbo
rne
even
ts a
t the
nat
iona
l and
sub
natio
nal l
evel
sSt
rate
gies
and
gui
danc
e fo
r co
mm
unic
atin
g w
ith p
artn
ers,
sta
keho
lder
s,
gene
ral p
ublic
and
inte
rnat
iona
l org
aniz
atio
ns a
re in
pla
ce
Sust
aina
ble
capa
city
– 5
Coun
try
has
a su
rvei
llanc
e sy
stem
in p
lace
that
inte
grat
es in
form
atio
n fr
om
the
entir
e fo
od c
hain
incl
udin
g tim
ely
and
syst
emat
ic in
form
atio
n ex
chan
ge,
to e
nabl
e a
bett
er u
nder
stan
ding
of r
isk
and
miti
gatio
n po
ssib
ilitie
s
The
food
saf
ety
emer
genc
y re
spon
se p
lan,
bas
ed o
n th
e ris
k an
alys
is
fram
ewor
k, is
pre
test
ed a
nd re
view
ed a
fter
an
emer
genc
y ha
s oc
curr
ed
Not
es:
The
PVS
tool
has
thre
e cr
itica
l com
pete
ncie
s on
food
saf
ety
of w
hich
CC
II-8
B (A
nte
and
post
mor
tem
insp
ectio
n at
aba
ttoi
rs a
nd a
ssoc
iate
d pr
emis
es) a
nd
CC II
-8 C
(Ins
pect
ion
of c
olle
ctio
n, p
roce
ssin
g an
d di
strib
utio
n of
pro
duct
s of
ani
mal
orig
in)
can
prov
ide
rele
vant
info
rmat
ion
on c
ount
ry c
apac
ity t
o co
nduc
t su
rvei
llanc
e on
food
born
e pa
thog
ens.
Cont
extu
al q
uest
ions
: N/A
Tech
nica
l que
stio
ns:
P.5.
1 Su
rvei
llanc
e sy
stem
s in
pla
ce fo
r the
det
ectio
n an
d m
onito
ring
of fo
odbo
rne
dise
ases
and
food
con
tam
inat
ion
1.
Doe
s th
e co
untr
y ha
ve a
sur
veill
ance
and
mon
itorin
g sy
stem
in p
lace
that
incl
udes
prio
rity
food
born
e di
seas
es a
s w
ell a
s pr
iorit
y ha
zard
s (c
hem
ical
and
m
icro
biol
ogic
al)?
2.
Doe
s th
e co
untr
y ha
ve c
ase
defin
ition
s fo
r eac
h of
the
notifi
able
food
born
e di
seas
es?
3.
Are
heal
th c
are
wor
kers
and
san
itary
/foo
d in
spec
tors
trai
ned
on re
port
ing
food
born
e ev
ents
(dis
ease
out
brea
ks o
r con
tam
inat
ion
even
ts)?
4.
Is th
ere
a te
am a
t the
nat
iona
l and
sub
natio
nal l
evel
who
can
rapi
dly
asse
ss fo
odbo
rne
even
ts?
5.
Are
peop
le id
entifi
ed to
take
par
t in
the
outb
reak
or e
vent
resp
onse
team
s tr
aine
d to
und
erta
ke o
utbr
eak
inve
stig
atio
ns o
f foo
dbor
ne d
isea
ses?
1 -
Refe
r to
the
rele
vant
tech
nica
l are
a w
here
ther
e is
an
over
lap
betw
een
one
or m
ore
tech
nica
l are
as (s
uch
as F
ood
safe
ty a
nd Z
oono
tic d
isea
se).
PR
EV
EN
T

INTERNATIONAL HEALTH REGULATIONS (2005)
36 - Joint External Evaluation Tool - Second edition
6.
Are
outb
reak
resp
onse
team
s tra
ined
to c
olle
ct a
nd tr
ansp
ort a
ppro
pria
te s
peci
men
s to
a la
bora
tory
dur
ing
food
born
e ou
tbre
aks
to id
entif
y th
e ae
tiolo
gica
l age
nt?
7.
Doe
s th
e co
untr
y ha
ve a
n up
date
d lis
t of l
abor
ator
ies
that
can
per
form
the
nece
ssar
y te
stin
g du
ring
food
born
e ou
tbre
aks
or c
onta
min
atio
n ev
ents
?8.
Ar
e re
pres
enta
tives
from
food
saf
ety
and
othe
r lab
orat
orie
s (a
nd a
nim
al h
ealth
, whe
re a
pplic
able
) rou
tinel
y pa
rt o
f the
out
brea
k re
spon
se te
am?
9.
Do
surv
eilla
nce
and
resp
onse
sta
ff kn
ow th
e fo
cal p
oint
s fo
r foo
d sa
fety
, ani
mal
hea
lth a
nd th
e ke
y la
bora
torie
s th
at w
ould
be
requ
ired
to te
st c
linic
al a
nd/o
r fo
od s
ampl
es c
olle
cted
dur
ing
an e
vent
?10
. Is
ther
e an
effe
ctiv
e (fo
rmal
or i
nfor
mal
) mec
hani
sm fo
r rap
id in
form
atio
n ex
chan
ge d
urin
g su
spec
ted
food
born
e di
seas
e ou
tbre
ak o
r eve
nt in
vest
igat
ions
be
twee
n al
l the
sta
keho
lder
s/re
leva
nt s
ecto
rs?
P.5.
2 M
echa
nism
s ar
e es
tabl
ishe
d an
d fu
nctio
ning
for t
he re
spon
se a
nd m
anag
emen
t of f
ood
safe
ty e
mer
genc
ies
1.
Doe
s th
e co
untr
y ha
ve a
pla
n th
at d
ocum
ents
resp
onse
pro
cedu
res
to a
ddre
ss fo
od s
afet
y em
erge
ncie
s?a.
Doe
s it
incl
ude
defin
ition
of t
rigge
rs?
b. D
oes
it re
fer t
o na
tiona
l (ce
ntra
l) co
ordi
natio
n?c.
Are
cle
ar ro
les
and
resp
onsi
bilit
ies
esta
blis
hed?
d. A
re p
roce
dure
s fo
r com
mun
icat
ions
est
ablis
hed?
2.
Was
the
plan
dev
elop
ed in
a p
artic
ipat
ory
way
?3.
Ar
e al
l key
par
tner
s an
d in
volv
ed s
take
hold
ers
prop
erly
aw
are
of th
eir r
oles
and
of t
he re
spon
se p
roce
dure
s re
quire
d of
them
in th
e ev
ent o
f a fo
od s
afet
y cr
isis
/em
erge
ncy?
4.
Are
all i
mpo
rtan
t sta
keho
lder
s (in
clud
ing
thei
r dec
isio
n m
aker
s, le
ader
s, a
nd w
orki
ng te
ams)
fully
brie
fed
on re
spon
se p
roce
dure
s?5.
Is
the
re a
nat
iona
l mec
hani
sm in
pla
ce e
nsur
ing
the
gath
erin
g an
d sh
arin
g of
rel
evan
t in
form
atio
n fo
r co
llect
ive
eval
uatio
n (s
uch
as n
atio
nal o
r re
gion
al
info
rmat
ion
shar
ing
netw
orks
)?6.
Is
ther
e an
act
ive
INFO
SAN
Em
erge
ncy
Cont
act P
oint
? Ar
e th
ere
activ
e IN
FOSA
N F
ocal
Poi
nts?
Are
ther
e ac
tive
OIE
Nat
iona
l Foc
al P
oint
s on
Ani
mal
Pro
duct
ion
Food
Saf
ety?
7.
Is th
ere
a co
ordi
natio
n m
echa
nism
in p
lace
(suc
h as
a m
ultia
genc
y co
ordi
natio
n te
am) w
ith c
lear
term
s of
refe
renc
e to
faci
litat
e co
mm
unic
atio
n be
twee
n ce
ntra
l and
loca
l lev
els?
a. D
oes
this
invo
lve
sect
ors
from
pub
lic h
ealth
, foo
d in
spec
tion,
vet
erin
ary,
offic
ial l
abor
ator
y, cu
stom
s an
d qu
aran
tine,
and
agr
icul
ture
?b.
Doe
s th
is in
volv
e ot
her r
elev
ant s
ecto
rs, s
uch
as to
uris
m, n
atio
nal s
ecur
ity d
epar
tmen
t, en
viro
nmen
tal s
ervi
ces?
c. A
re c
lear
role
s an
d re
spon
sibi
litie
s as
sign
ed to
all
part
ners
of t
he c
oord
inat
ion
team
?8.
Ar
e ke
y st
akeh
olde
rs a
war
e of
the
prin
cipl
es a
nd p
ract
ices
of c
omm
unic
atio
n an
d co
ntro
l sys
tem
s in
the
even
t of a
food
saf
ety
cris
is o
r em
erge
ncy?
9.
Is th
ere
a lis
t of a
ll ne
cess
ary
cont
act d
etai
ls fo
r com
mun
icat
ing
with
par
tner
s re
adily
ava
ilabl
e an
d up
date
d (lo
cal a
nd fo
reig
n go
vern
men
ts, i
nter
natio
nal
orga
niza
tions
, ind
ustr
y)?
10.
Doe
s th
e co
untr
y un
dert
ake
regu
lar a
ctiv
ities
aim
ed a
t pre
parin
g ef
fect
ive
com
mun
icat
ions
for f
ood
safe
ty e
mer
genc
y re
spon
ses?
11.
Are
ther
e pe
riodi
c si
mul
atio
n ex
erci
ses
to p
re-t
est t
he e
mer
genc
y re
spon
se p
lan?
12.
Are
ther
e re
cord
s of
feed
back
s fro
m p
ast e
mer
genc
y re
view
s, c
onsi
derin
g:a.
app
ropr
iate
ness
of r
espo
nse
activ
ities
;
PR
EV
EN
T

INTERNATIONAL HEALTH REGULATIONS (2005)
37 - Joint External Evaluation Tool - Second edition
b. e
ffect
iven
ess
of w
ithdr
awal
or r
ecal
ls im
plem
ente
d;c.
reg
ulat
ory
proc
edur
es a
vaila
ble
to in
spec
tors
to ta
ke a
ctio
n (p
reve
nt p
rodu
ctio
n an
d di
strib
utio
n of
food
pro
duct
s);
d. c
apac
ity o
f ana
lytic
al s
ervi
ces;
e. g
loba
l cap
acity
of i
nspe
ctio
n se
rvic
es a
nd la
bora
torie
s to
repo
rt to
the
cent
ral c
oord
inat
ion
mec
hani
sm;
f. m
eans
of c
omm
unic
atio
ns; a
ndg.
suf
ficie
nt re
sour
ces
(sta
ff, a
naly
tical
, etc
.) an
d ca
paci
ties
(add
ition
al n
eeds
for t
rain
ing)
?
Doc
umen
tatio
n or
evi
denc
e fo
r lev
el o
f cap
abili
tyl
List
of p
riorit
y fo
odbo
rne
dise
ases
and
prio
rity
food
born
e ha
zard
s (c
hem
ical
and
mic
robi
olog
ical
)l
Gui
danc
e on
prio
rity
food
born
e di
seas
es a
nd th
eir c
ase
defin
ition
sl
Nat
iona
l lev
el re
port
bas
ed o
n co
llate
d lo
cal r
epor
ts fo
r rap
id ri
sk a
sses
smen
tl
Trai
ning
mat
eria
l, re
port
s an
d ce
rtifi
cate
sl
Inte
rvie
ws
with
san
itary
/foo
d in
spec
tors
l
Prot
ocol
s fo
r col
lect
ing/
test
ing
clin
ical
spe
cim
ens
and
food
sam
ples
for a
ll pr
iorit
y fo
odbo
rne
dise
ases
and
food
born
e ha
zard
sl
Dat
a re
port
ing
prot
ocol
s fo
r all
prio
rity
food
born
e di
seas
es a
nd fo
odbo
rne
haza
rds
l
List
of c
onta
ct la
bora
torie
sl
Que
stio
nnai
res
for p
riorit
y fo
odbo
rne
path
ogen
s an
d fo
odbo
rne
haza
rds
l
Inte
grat
ed fo
od c
hain
sur
veill
ance
dat
abas
el
Dat
a an
alys
is re
port
sl
Copi
es o
f reg
ular
sur
veill
ance
bul
letin
sl
Doc
umen
tatio
n pr
esen
ting
the
defin
ition
of a
nat
iona
l foo
d sa
fety
em
erge
ncy
l
Inte
rvie
w o
f key
par
tner
s/st
akeh
olde
rs re
gard
ing
thei
r kno
wle
dge
of th
eir r
oles
and
of r
espo
nse
proc
edur
esl
Reco
rds
of in
form
atio
n ex
chan
ge a
nd c
omm
unic
atio
n w
ith re
leva
nt in
tern
atio
nal,
regi
onal
and
nat
iona
l net
wor
ksl
Upd
ated
list
of p
artn
ers’
con
tact
sl
Doc
umen
ted
and
upda
ted
lists
of p
ossi
ble
exte
rnal
reso
urce
s (e
xper
ts, c
ompe
tenc
ies,
or s
peci
alis
t gro
upin
gs)
l
Any
docu
men
tatio
n, re
port
or r
ecor
d on
the
esta
blis
hmen
t, im
plem
enta
tion
and
ongo
ing
wor
k of
the
coor
dina
tion
mec
hani
sms
l
List
of a
ll ne
cess
ary
cont
act d
etai
ls (l
ocal
and
fore
ign
gove
rnm
ents
, int
erna
tiona
l org
aniz
atio
ns, i
ndus
try)
l
Tem
plat
es fo
r not
ifica
tions
of i
ncid
ents
l
Mod
el p
ress
rele
ases
l
Reca
ll an
d w
ithdr
awal
not
ices
l
Prep
ared
que
stio
ns a
nd a
nsw
ers
l
Repo
rts
on s
imul
atio
n ex
erci
ses
to p
re-t
est t
he re
spon
se e
mer
genc
y pl
anl
Reco
rd o
f fee
dbac
ks fr
om p
ast e
mer
genc
y re
view
s
PR
EV
EN
T

INTERNATIONAL HEALTH REGULATIONS (2005)
38 - Joint External Evaluation Tool - Second edition
BIO
SAFE
TY A
ND
BIO
SECU
RITY
Targ
et: F
A w
hole
-of-
gove
rnm
ent m
ultis
ecto
ral n
atio
nal b
iosa
fety
1 and
bio
secu
rity2 s
yste
m w
ith d
ange
rous
pat
hoge
ns3 i
dent
ified
, hel
d, s
ecur
ed a
nd m
onito
red
in
a m
inim
al n
umbe
r of f
acili
ties
acco
rdin
g to
bes
t pra
ctic
es4 ;
biol
ogic
al ri
sk m
anag
emen
t tra
inin
g an
d ed
ucat
iona
l out
reac
h co
nduc
ted
to p
rom
ote
a sh
ared
cul
ture
of
resp
onsi
bilit
y5 , re
duce
dua
l-us
e ris
ks, m
itiga
te b
iolo
gica
l pro
lifer
atio
n an
d de
liber
ate
use
thre
ats,
and
ens
ure
safe
tran
sfer
of b
iolo
gica
l age
nts;
and
cou
ntry
-sp
ecifi
c bi
osaf
ety
and
bios
ecur
ity le
gisl
atio
n, la
bora
tory
lice
nsin
g an
d pa
thog
en c
ontr
ol m
easu
res
in p
lace
as
appr
opria
te.
As m
easu
red
by:
(1)
Exis
tenc
e of
a n
atio
nal
fram
ewor
k fo
r pa
thog
en b
iosa
fety
and
bio
secu
rity,
stra
in c
olle
ctio
ns, c
onta
inm
ent
labo
rato
ries,
tha
t in
clud
es
iden
tifica
tion
and
stor
age
of n
atio
nal s
trai
n co
llect
ions
in a
min
imal
num
ber o
f fac
ilitie
s fr
om a
ll se
ctor
s. (2
) Exi
sten
ce o
f com
preh
ensi
ve o
vers
ight
and
mon
itorin
g sy
stem
s.
Desi
red
impa
ct: I
mpl
emen
tatio
n of
a c
ompr
ehen
sive
, sus
tain
able
and
lega
lly e
mbe
dded
nat
iona
l ove
rsig
ht p
rogr
amm
e fo
r bio
safe
ty a
nd b
iose
curit
y, in
clud
ing
the
safe
and
sec
ure
use,
sto
rage
, dis
posa
l and
con
tain
men
t of p
atho
gens
foun
d in
labo
rato
ries
and
a m
inim
al n
umbe
r of h
oldi
ngs
acro
ss th
e co
untr
y, an
d in
volv
ing
rese
arch
, dia
gnos
tic a
nd b
iote
chno
logy
fac
ilitie
s w
ithin
all
sect
ors6 .
A ca
dre
of b
iolo
gica
l ris
k m
anag
emen
t ex
pert
s po
sses
sing
the
ski
llset
to
trai
n ot
hers
is
esta
blis
hed
with
in t
heir
resp
ectiv
e in
stitu
tions
. Str
engt
hene
d, s
usta
inab
le b
iolo
gica
l ris
k m
anag
emen
t be
st p
ract
ices
are
in p
lace
usi
ng c
omm
on e
duca
tiona
l m
ater
ials
. Rap
id a
nd c
ultu
re-f
ree
diag
nost
ics
are
prom
oted
as
a fa
cet o
f bio
logi
cal r
isk
man
agem
ent.
Safe
and
com
plia
nt tr
ansp
ort o
f inf
ectio
us s
ubst
ance
s is
al
so ta
ken
into
acc
ount
acc
ordi
ng to
nat
iona
l and
inte
rnat
iona
l reg
ulat
ions
as
appr
opria
te.
1 -
Labo
rato
ry b
iosa
fety
des
crib
es th
e co
ntai
nmen
t prin
cipl
es, t
echn
olog
ies
and
prac
tices
that
are
impl
emen
ted
to p
reve
nt u
nint
entio
nal e
xpos
ure
to p
atho
gens
and
toxi
ns, o
r the
ir ac
cide
ntal
rele
ase.
2 -
Labo
rato
ry b
iose
curit
y de
scrib
es th
e pr
otec
tion,
con
trol
and
acc
ount
abili
ty fo
r val
uabl
e bi
olog
ical
mat
eria
ls w
ithin
labo
rato
ries
as w
ell a
s in
form
atio
n re
late
d to
thes
e m
ater
ials
and
dua
l-us
e re
sear
ch, i
n or
der t
o pr
even
t the
ir un
auth
oriz
ed a
cces
s, lo
ss, t
heft
, mis
use,
div
ersi
on o
r int
entio
nal r
elea
se.
3 -
Dan
gero
us p
atho
gens
and
toxi
ns –
The
info
rmal
Aus
tral
ia G
roup
pro
vide
s a
List
of h
uman
and
ani
mal
pat
hoge
ns a
nd to
xins
for e
xpor
t con
trol
(htt
p://
ww
w.a
ustr
alia
grou
p.ne
t/en
/hum
an_a
nim
al_p
atho
gens
.htm
l, ac
cess
ed 2
3 N
ovem
ber 2
017)
.4
- It
is s
ugge
sted
that
min
imal
/bes
t pra
ctic
e w
ould
follo
w th
e W
HO
Lab
orat
ory
bios
afet
y m
anua
l?5
- Res
pons
ible
life
sci
ence
s re
sear
ch fo
r glo
bal h
ealth
sec
urity
: a g
uida
nce
docu
men
t. W
HO
/HSE
/GAR
/BD
P/20
10.2
. Gen
eva:
Wor
ld H
ealth
org
aniz
atio
n; 2
010
(htt
p://
ww
w.w
ho.in
t/cs
r/re
sour
ces/
publ
icat
ions
/HSE
_GAR
_BD
P_20
10_2
/en
/ (a
cces
sed
21 N
ovem
ber 2
017)
.6
- W
ithin
bot
h hu
man
and
ani
mal
hea
lth s
ecto
rs.
PR
EV
EN
T

INTERNATIONAL HEALTH REGULATIONS (2005)
39 - Joint External Evaluation Tool - Second edition
Scor
eIn
dica
tors
: Bio
safe
ty a
nd b
iose
curit
yP.
6.1
Who
le-o
f-go
vern
men
t bio
safe
ty a
nd b
iose
curit
y sy
stem
in p
lace
for a
ll se
ctor
s (in
clud
ing
hum
an, a
nim
al a
nd a
gric
ultu
re fa
cilit
ies)
P.6.
2 Bi
osaf
ety
and
bios
ecur
ity tr
aini
ng a
nd p
ract
ices
in a
ll re
leva
nt s
ecto
rs7
(incl
udin
g hu
man
, ani
mal
and
agr
icul
ture
)
No
capa
city
- 1
Elem
ents
of a
com
preh
ensi
ve n
atio
nal b
iosa
fety
and
bio
secu
rity
syst
em, s
uch
as p
olic
y in
stru
men
ts a
nd p
rope
r fina
ncin
g8, a
re n
ot in
pla
ceN
o bi
olog
ical
bio
safe
ty a
nd b
iose
curit
y tr
aini
ng o
r pla
ns a
re in
pla
ce
Lim
ited
ca
paci
ty -
2
Som
e, b
ut n
ot a
ll, e
lem
ents
of
a co
mpr
ehen
sive
bio
safe
ty a
nd b
iose
curit
y sy
stem
are
in p
lace
. The
cou
ntry
is:
Star
ting
the
proc
ess
to m
onito
r and
dev
elop
an
upda
ted
reco
rd a
nd in
vent
ory
of p
atho
gens
with
in fa
cilit
ies
that
sto
re o
r pro
cess
dan
gero
us p
atho
gens
and
to
xins
and
wha
t the
y ho
use
Dev
elop
ing,
but
has
not
fina
lized
, co
mpr
ehen
sive
nat
iona
l bi
osaf
ety
and
bios
ecur
ity re
gula
tory
fram
ewor
kD
evel
opin
g la
bora
tory
lice
nsin
g
Coun
try
has
cond
ucte
d a
trai
ning
nee
ds a
sses
smen
t an
d id
entifi
ed g
aps
in
bios
afet
y an
d bi
osec
urity
trai
ning
but
has
not
yet i
mpl
emen
ted
com
preh
ensi
ve
trai
ning
Gen
eral
lack
of
awar
enes
s am
ong
the
labo
rato
ry w
orkf
orce
of
inte
rnat
iona
l bi
osaf
ety
and
bios
ecur
ity b
est
prac
tices
for
saf
e, s
ecur
e an
d re
spon
sibl
e co
nduc
tCo
untr
y do
es n
ot y
et h
ave
sust
aine
d ac
adem
ic t
rain
ing
in i
nstit
utio
ns
prop
ortio
nate
to th
e as
sess
ed ri
sks,
incl
udin
g tr
aini
ng th
ose
who
mai
ntai
n or
w
ork
with
dan
gero
us p
atho
gens
and
toxi
ns
Deve
lope
d ca
paci
ty -
3
Com
preh
ensi
ve n
atio
nal b
iosa
fety
and
bio
secu
rity
syst
em is
bei
ng d
evel
oped
. Th
e co
untr
y is
:Fi
naliz
ing
the
proc
ess
to s
uppo
rt a
ctiv
e m
onito
ring
and
mai
ntai
ning
of u
p-to
-da
te re
cord
s an
d pa
thog
en in
vent
orie
s w
ithin
faci
litie
s th
at s
tore
or p
roce
ss
dang
erou
s pa
thog
ens
and
toxi
nsFi
naliz
ing
the
deve
lopm
ent
and
impl
emen
tatio
n of
com
preh
ensi
ve n
atio
nal
bios
afet
y an
d bi
osec
urity
regu
lato
ry fr
amew
ork
incl
udin
g lic
ensi
ngFi
naliz
ing
the
deve
lopm
ent a
nd im
plem
enta
tion
of p
atho
gen
cont
rol m
easu
res,
op
erat
iona
l han
dlin
g an
d co
ntai
nmen
t fai
lure
repo
rtin
g sy
stem
sSt
artin
g th
e co
nsol
idat
ion
of d
ange
rous
pat
hoge
ns a
nd to
xins
into
a m
inim
um
num
ber o
f fac
ilitie
sSt
artin
g to
put
into
pla
ce t
ools
and
res
ourc
es t
o su
ppor
t di
agno
stic
s th
at
prec
lude
cul
turin
g da
nger
ous
path
ogen
sSt
artin
g to
put
in p
lace
inci
dent
and
em
erge
ncy
and
resp
onse
pro
gram
mes
Coun
try
has
trai
ning
pro
gram
mes
in
plac
e pr
opor
tiona
te t
o th
e as
sess
ed
risks
and
has
beg
un im
plem
enta
tion
Coun
try
has
spec
ific
trai
ning
pro
gram
mes
in p
lace
at m
ost f
acili
ties
hous
ing
or w
orki
ng w
ith d
ange
rous
pat
hoge
ns a
nd to
xins
Trai
ning
on
bios
afet
y an
d bi
osec
urity
has
bee
n pr
ovid
ed to
sta
ff at
som
e, b
ut
not a
ll, fa
cilit
ies
that
mai
ntai
n or
wor
k w
ith d
ange
rous
pat
hoge
ns a
nd to
xins
Coun
try
is d
evel
opin
g su
stai
ned
acad
emic
tra
inin
g pr
opor
tiona
te t
o th
e as
sess
ed r
isks
, in
clud
ing
the
one
for
thos
e w
ho m
aint
ain
or w
ork
with
da
nger
ous
path
ogen
s an
d to
xins
7 -
Rele
vant
sec
tors
incl
ude,
at m
inim
um, t
he m
inis
trie
s or
age
ncie
s th
at a
re k
ey to
this
tech
nica
l are
a, s
uch
as h
uman
hea
lth, a
nim
al h
ealth
, env
ironm
ent,
food
saf
ety,
defe
nce,
priv
ate
sect
or.
8 -
Such
a c
ompr
ehen
sive
bio
safe
ty a
nd b
iose
curit
y sy
stem
wou
ld c
over
legi
slat
ion,
regu
latio
ns, r
equi
rem
ents
and
fina
ncin
g.
PR
EV
EN
T

INTERNATIONAL HEALTH REGULATIONS (2005)
40 - Joint External Evaluation Tool - Second edition
Dem
onst
rate
d ca
paci
ty –
4
Bios
afet
y an
d bi
osec
urity
sys
tem
is
deve
lope
d, b
ut n
ot s
usta
inab
le.
The
coun
try
is:
Activ
ely
mon
itorin
g an
d m
aint
aini
ng a
n up
date
d re
cord
and
inv
ento
ry o
f pa
thog
ens
with
in f
acili
ties
that
sto
re o
r pr
oces
s da
nger
ous
path
ogen
s an
d to
xins
Impl
emen
ting
enac
ted
com
preh
ensi
ve n
atio
nal
bios
afet
y an
d bi
osec
urity
re
gula
tory
fram
ewor
kIm
plem
entin
g la
bora
tory
lice
nsin
gIm
plem
entin
g pa
thog
en
cont
rol
mea
sure
s,
oper
atio
nal
hand
ling
and
cont
ainm
ent f
ailu
re re
port
ing
syst
ems
Com
plet
ing
the
cons
olid
atio
n of
dan
gero
us p
atho
gens
and
tox
ins
into
a
min
imum
num
ber o
f fac
ilitie
sEm
ploy
ing
diag
nost
ics
that
pre
clud
e cu
lturin
g da
nger
ous
path
ogen
sO
pera
ting
inci
dent
and
em
erge
ncy
and
resp
onse
pro
gram
mes
Coun
try
has
trai
ning
pro
gram
mes
in p
lace
Co
untr
y ha
s tr
aini
ng p
rogr
amm
es in
pla
ce a
t al
l fac
ilitie
s an
d st
aff
trai
ned
prop
ortio
nate
to th
e as
sess
ed ri
sks,
incl
udin
g th
ose
that
hou
se o
r wor
k w
ith
dang
erou
s pa
thog
ens
and
toxi
nsCo
untr
y ha
s in
pla
ce a
cade
mic
trai
ning
pro
port
iona
te to
the
asse
ssed
risk
s,
incl
udin
g in
stitu
tions
that
trai
n th
ose
who
mai
ntai
n or
wor
k w
ith d
ange
rous
pa
thog
ens
and
toxi
nsCo
untr
y ha
s lim
ited
abili
ty to
sel
f-su
stai
n al
l of t
he a
bove
Sust
aina
ble
capa
city
– 5
Sust
aina
ble
mul
tisec
tora
l bio
safe
ty a
nd b
iose
curit
y sy
stem
is in
pla
ceM
inis
trie
s ha
ve m
ade
avai
labl
e ad
equa
te f
undi
ng a
nd p
oliti
cal
supp
ort
for
a co
mpr
ehen
sive
nat
iona
l bi
osaf
ety
and
bios
ecur
ity s
yste
m, i
nclu
ding
m
aint
enan
ce o
f fac
ilitie
s an
d eq
uipm
ent
Coun
try
has
sust
aina
ble
trai
ning
pro
gram
mes
incl
uded
into
uni
vers
ity/c
olle
ge
curr
icul
a of
pre
-ser
vice
trai
ning
and
into
con
tinui
ng e
duca
tion
prog
ram
mes
. St
aff c
ompe
tenc
e is
ass
esse
d an
d ex
erci
ses
are
cond
ucte
d pe
riodi
cally
Coun
try
has
fund
ing
and
capa
city
to s
usta
in a
ll of
the
abov
eRe
view
of t
rain
ing
need
s as
sess
men
t is
cond
ucte
d pe
riodi
cally
and
refr
eshe
r tr
aini
ng o
n ne
eds
area
s ar
e co
nduc
ted
perio
dica
llyTr
aini
ng o
n em
erge
ncy
resp
onse
pro
cedu
res
are
prov
ided
per
iodi
cally
Cont
extu
al q
uest
ions
: N/A
Tech
nica
l que
stio
ns:
P.6.
1 W
hole
-of-
gove
rnm
ent b
iosa
fety
and
bio
secu
rity
syst
em in
pla
ce fo
r all
sect
ors
(incl
udin
g hu
man
, ani
mal
and
agr
icul
ture
faci
litie
s)1.
Is
ther
e ac
tive
mon
itorin
g an
d de
velo
pmen
t of a
n up
date
d re
cord
and
inve
ntor
y of
pat
hoge
ns w
ithin
faci
litie
s th
at s
tore
or p
roce
ss d
ange
rous
pat
hoge
ns a
nd
toxi
ns?
a. D
oes
the
coun
try
have
in p
lace
an
upda
ted
reco
rd o
f whe
re a
nd in
whi
ch fa
cilit
ies
dang
erou
s pa
thog
ens
and
toxi
ns a
re h
ouse
d?i.
Hav
e co
llect
ions
of p
atho
gens
and
toxi
ns b
een
iden
tified
?ii.
Wha
t gui
danc
e is
to b
e pr
ovid
ed to
cou
ntrie
s w
hich
do
not h
ave
supp
ortin
g sy
stem
s an
d le
gisl
atio
n al
read
y in
pla
ce to
ena
ble
them
to re
quire
inve
ntor
y re
cord
s of
“dan
gero
us p
atho
gens
and
toxi
ns” k
ept b
y fa
cilit
ies?
PR
EV
EN
T

INTERNATIONAL HEALTH REGULATIONS (2005)
41 - Joint External Evaluation Tool - Second edition
iii.
Is th
ere
an a
gree
d lis
t of “
dang
erou
s pa
thog
ens
and
toxi
ns” t
o w
hich
this
que
stio
n ap
plie
s?
iv.
How
oft
en a
re fa
cilit
ies
expe
cted
to u
pdat
e su
ch re
cord
s?
2.
Is th
ere
a co
mpr
ehen
sive
nat
iona
l bio
safe
ty a
nd b
iose
curit
y re
gula
tory
fram
ewor
k be
ing
enac
ted?
a. D
oes
the
coun
try
have
bio
secu
rity
legi
slat
ion
and/
or re
gula
tions
in p
lace
? Ar
e th
ey b
eing
impl
emen
ted?
b. D
oes
the
coun
try
have
bio
safe
ty le
gisl
atio
n an
d/or
regu
latio
ns in
pla
ce?
Are
they
bei
ng im
plem
ente
d?c.
Des
crib
e th
e fo
llow
ing
from
the
cou
ntry
’s n
atio
nal b
iose
curit
y le
gisl
atio
n, r
egul
atio
ns o
r fr
amew
orks
, and
cou
ntry
’s n
atio
nal b
iosa
fety
legi
slat
ion,
re
gula
tions
or f
ram
ewor
ks.
i. H
ow is
this
info
rmat
ion
shar
ed w
ith la
bora
torie
s at
sub
natio
nal l
evel
s w
ithin
the
coun
try?
ii. A
re re
gula
tions
and
/or g
uide
lines
for b
iose
curit
y fo
llow
ed b
y la
bora
torie
s w
ithin
the
coun
try?
Wha
t abo
ut fo
r bio
safe
ty?
iii. D
escr
ibe
bios
ecur
ity m
onito
ring
activ
ities
. Des
crib
e bi
osaf
ety
mon
itorin
g ac
tiviti
es.
iv. H
as a
third
par
ty a
sses
sed
bios
ecur
ity a
t nat
iona
l lab
orat
ory
faci
litie
s? W
as a
bio
safe
ty a
sses
smen
t als
o do
ne?
1.
Whe
n w
as th
e as
sess
men
t don
e?
2.
Hav
e th
e re
com
men
datio
ns fr
om th
ose
bios
ecur
ity a
nd b
iosa
fety
ass
essm
ents
bee
n pu
t int
o pl
ace?
v.
W
hat t
ype
of la
bora
tory
requ
ires
a lic
ence
in th
e co
untr
y?
vi.
Are
ther
e co
mm
on li
cenc
e co
nditi
ons/
safe
ty a
nd s
ecur
ity re
quire
men
ts fo
r all
licen
sed
labo
rato
ries?
If s
o, w
hat a
re th
ey?
vii.
How
is c
ompl
ianc
e w
ith li
cens
ing
requ
irem
ents
mon
itore
d?vi
ii. Is
ther
e ad
equa
te a
vaila
bilit
y of
fund
ing
to s
uppo
rt b
iosa
fety
and
bio
secu
rity
prog
ram
mes
/ini
tiativ
es a
nd th
eir
over
sigh
t and
enf
orce
men
t at t
he
min
istr
y le
vel?
ix
. Is th
ere
a m
echa
nism
for b
iose
curit
y ov
ersi
ght o
f dua
l-us
e re
sear
ch a
nd re
spon
sibl
e co
de o
f con
duct
for s
cien
tists
?3.
Ar
e th
e la
bora
tory
lice
nsin
g an
d pa
thog
en c
ontr
ol m
easu
res,
incl
udin
g re
quire
men
ts fo
r phy
sica
l con
tain
men
t and
ope
ratio
nal p
ract
ices
, and
con
tain
men
t an
d fa
ilure
repo
rtin
g sy
stem
s be
ing
impl
emen
ted?
a. P
hysi
cal s
ecur
ityi.
Are
appr
opria
te s
ecur
ity m
easu
res
in p
lace
to m
inim
ize
pote
ntia
l ina
ppro
pria
te re
mov
al o
r rel
ease
of b
iolo
gica
l age
nts
(suc
h as
thef
t, ea
rthq
uake
, flo
od)?
b. I
nfor
mat
ion
secu
rity
i. Is
acc
ess
to s
ensi
tive
info
rmat
ion
(suc
h as
inve
ntor
y of
age
nts
and
toxi
ns) c
ontr
olle
d by
ade
quat
e po
licie
s an
d pr
oced
ures
?c.
Tra
nspo
rtat
ion
secu
rity
i. Ar
e pr
oced
ures
for a
saf
e an
d se
cure
tran
spor
t of c
ultu
re, s
peci
men
s, s
ampl
es a
nd o
ther
con
tam
inat
ed m
ater
ials
est
ablis
hed
and
follo
wed
? ii.
Is
ther
e na
tiona
l leg
isla
tion
for t
he tr
ansp
orta
tion
of d
ange
rous
goo
ds, i
nclu
ding
pat
hoge
ns?
d. P
erso
nnel
sec
urity
i.
Is th
ere
a m
echa
nism
to d
eter
min
e w
hich
per
sonn
el a
re a
utho
rized
to a
cces
s pa
thog
ens
of s
ecur
ity c
once
rn?
ii.
Is th
ere
evid
ence
that
this
mec
hani
sm to
aut
horiz
e pe
rson
nel i
s be
ing
impl
emen
ted
corr
ectly
?
PR
EV
EN
T

INTERNATIONAL HEALTH REGULATIONS (2005)
42 - Joint External Evaluation Tool - Second edition
e. B
iosa
fety
and
bio
secu
rity
prac
tices
at f
acili
ties
hous
ing
or w
orki
ng w
ith d
ange
rous
pat
hoge
nsi.
Are
site
-spe
cific
bio
safe
ty a
nd b
iose
curit
y m
anag
emen
t pro
gram
mes
and
sup
port
ing
docu
men
ts (m
anua
ls, S
OPs
, job
aid
es, r
ecor
ds) a
vaila
ble
to
incl
ude
bios
afet
y, bi
osec
urity
, inc
iden
t res
pons
e an
d em
erge
ncy
plan
s (s
uch
as fo
r exp
losi
on, fi
re, f
lood
, wor
ker e
xpos
ure,
acc
iden
t or i
llnes
s, m
ajor
sp
illag
e)?
ii.
Are
role
s an
d re
spon
sibi
litie
s re
late
d to
bio
safe
ty a
nd b
iose
curit
y m
anag
emen
t defi
ned
and
docu
men
ted
(bio
safe
ty o
ffice
r, se
curit
y m
anag
er)?
iii.
Hav
e th
e bi
osaf
ety
and
bios
ecur
ity ri
sks
been
ass
esse
d an
d ca
tego
rized
?iv
. Ar
e bi
osaf
ety
and
bios
ecur
ity c
ontr
ol m
easu
res
desc
ribed
in a
n ac
tion
plan
? v.
Ar
e th
ere
mec
hani
sms
to e
nsur
e th
at p
erso
nnel
: are
sui
tabl
e an
d co
mpe
tent
(e.g
. bes
t pra
ctic
es) i
n hu
man
reso
urce
s m
anag
emen
t (e.
g. v
erifi
catio
n of
prio
r edu
catio
n an
d em
ploy
men
t, pe
riodi
c pe
rfor
man
ce re
view
s), h
ave
succ
essf
ully
com
plet
ed tr
aini
ng/m
ento
rshi
p pr
ogra
mm
es, a
nd h
ave
the
abili
ty to
wor
k un
supe
rvis
ed?
f. I
s th
ere
a sy
stem
in p
lace
to c
ondu
ct a
udits
of l
abor
ator
y fa
cilit
ies?
i.
If so
, are
aud
its p
erfo
rmed
regu
larly
? ii.
W
hat o
rgan
izat
ion
cond
ucts
thes
e au
dits
? Ar
e th
ese
with
in th
e go
vern
men
t or e
xter
nal?
iii
. Ar
e au
dits
con
duct
ed b
y th
e na
tiona
l aut
horit
y (s
uch
as In
stitu
tiona
l Bio
safe
ty C
omm
ittee
) or b
y th
e lo
cal B
iolo
gica
l Saf
ety
Offi
cer?
iv.
Whi
ch ty
pes
of la
bora
torie
s ar
e su
bjec
t to
thes
e au
dits
? g.
Do
labo
rato
ries
ensu
re th
at b
est p
ract
ices
for b
iosa
fety
and
bio
secu
rity
are
in p
lace
? If
yes,
how
?h.
Do
any
of th
e na
tiona
l lab
orat
orie
s ha
ve o
ther
rele
vant
cla
ssifi
catio
ns (i
.e. F
AO/O
IE/W
HO
Col
labo
ratin
g Ce
ntre
s/Re
fere
nce
Labo
rato
ries)
?4.
Ar
e da
nger
ous
path
ogen
s an
d to
xins
con
solid
ated
into
a m
inim
um n
umbe
r of f
acili
ties?
a. H
as th
e co
untr
y co
nsid
ered
con
solid
atin
g th
e lo
catio
ns fo
r dan
gero
us p
atho
gens
and
toxi
ns?
i. If
not,
will
con
solid
atio
n be
con
side
red?
b. H
ave
colle
ctio
ns o
f dan
gero
us p
atho
gens
bee
n co
nsol
idat
ed in
to a
min
imum
num
ber o
f fac
ilitie
s?
5.
Are
they
em
ploy
ing
diag
nost
ics
that
pre
clud
e cu
lturin
g da
nger
ous
path
ogen
s?a.
Doe
s th
e co
untr
y ut
ilize
dia
gnos
tic te
sts
that
elim
inat
e th
e ne
ed fo
r cul
turin
g da
nger
ous
path
ogen
s?6.
Ar
e th
ey im
plem
entin
g ov
ersi
ght
and
enfo
rcem
ent
mec
hani
sms,
and
hav
e m
inis
trie
s m
ade
avai
labl
e ad
equa
te f
undi
ng t
o su
ppor
t th
e co
mpr
ehen
sive
na
tiona
l bio
safe
ty a
nd b
iose
curit
y sy
stem
?a.
Are
ther
e m
echa
nism
s fo
r ove
rsig
ht, e
nfor
cem
ent a
nd a
ttrib
utio
n fo
r bio
safe
ty a
nd b
iose
curit
y le
gisl
atio
n, re
gula
tions
and
/or g
uide
lines
? b.
Doe
s th
e co
untr
y ha
ve fu
ndin
g fo
r the
se a
ctiv
ities
? Is
the
fund
ing
sour
ce s
usta
inab
le?
7.
Are
the
new
faci
litie
s pl
anne
d w
ith lo
ng-t
erm
com
mitm
ent o
f res
ourc
es fo
r ope
ratio
n an
d m
aint
enan
ce a
nd fo
rmal
ly c
omm
issi
oned
bef
ore
open
ing?
8.
Can
the
bios
afet
y ca
bine
ts b
e se
rvic
ed lo
cally
?9.
Ar
e th
ere
suffi
cien
t nat
iona
l res
ourc
es (b
udge
t and
hum
an) t
o en
sure
pro
per a
nd ti
mel
y m
aint
enan
ce o
f fac
ilitie
s an
d eq
uipm
ent?
10.
Is th
ere
an a
ppro
pria
te w
aste
man
agem
ent p
olic
y at
the
natio
nal l
evel
and
is it
bei
ng im
plem
ente
d lo
cally
?
PR
EV
EN
T

INTERNATIONAL HEALTH REGULATIONS (2005)
43 - Joint External Evaluation Tool - Second edition
11.
Doe
s ea
ch fa
cilit
y ha
ve s
uffic
ient
per
sona
l pro
tect
ive
equi
pmen
t bas
ed o
n lo
cal r
isk
asse
ssm
ent?
12.
Is th
ere
a fr
amew
ork
to d
ocum
ent,
repo
rt, i
nves
tigat
e an
d ad
dres
s an
y in
cide
nts
and
acci
dent
s at
the
faci
lity
and
natio
nal l
evel
s?13
. Ar
e na
tiona
l reg
ulat
ions
in p
lace
and
up-
to-d
ate
for t
he tr
ansp
ort o
f inf
ectio
us s
ubst
ance
s (C
ateg
orie
s A
and
B)?
a. If
yes
, do
loca
l car
riers
ens
ure
the
tran
spor
t of i
nfec
tious
sub
stan
ces
acco
rdin
g to
nat
iona
l reg
ulat
ions
? b.
Do
the
peop
le re
spon
sibl
e fo
r the
shi
pmen
t of s
peci
men
s ha
ve a
cces
s to
trai
ning
on
infe
ctio
us s
ubst
ance
tran
spor
t?i.
If ye
s, a
re th
ese
trai
ning
s in
line
with
Uni
ted
Nat
ions
regu
latio
ns o
n th
e tr
ansp
ort o
f inf
ectio
us s
ubst
ance
s?14
. D
o la
bora
tory
per
sonn
el h
ave
equa
l acc
ess
to o
ccup
atio
nal/w
orke
r hea
lth s
ervi
ces
in a
ll fa
cilit
ies?
15.
Is th
ere
a sp
ecifi
c va
ccin
atio
n po
licy
(pre
-exp
osur
e pr
ophy
laxi
s) fo
r lab
orat
ory
pers
onne
l (he
patit
is B
and
oth
er re
leva
nt d
isea
ses)
?16
. Is
pos
t-ex
posu
re p
roph
ylax
is tr
eatm
ent p
rovi
ded
to la
bora
tory
wor
kers
in a
ll fa
cilit
ies?
17
. Ar
e la
bora
tory
-acq
uire
d in
fect
ions
and
oth
er in
cide
nts
repo
rted
? a.
Who
doe
s it
get r
epor
ted
to?
b. I
s th
ere
a na
tiona
l sna
psho
t as
to w
hat i
s ha
ppen
ing
acro
ss th
e co
untr
y?
P.6.
2 B
iosa
fety
and
bio
secu
rity
trai
ning
and
pra
ctic
es in
all
rele
vant
sec
tors
(inc
ludi
ng h
uman
, ani
mal
and
agr
icul
ture
)1.
D
oes
the
coun
try
have
trai
ning
pro
gram
mes
in p
lace
at a
ll fa
cilit
ies,
incl
udin
g th
ose
that
hou
se o
r wor
k w
ith d
ange
rous
pat
hoge
ns a
nd to
xins
?a.
Is b
iosa
fety
and
bio
secu
rity
trai
ning
in p
lace
acr
oss
all f
acili
ties,
incl
udin
g th
ose
that
hou
se o
r w
ork
with
dan
gero
us p
atho
gens
? W
hat
abou
t bi
osaf
ety
trai
ning
? 2.
H
as tr
aini
ng o
n bi
osaf
ety
and
bios
ecur
ity b
een
prov
ided
to s
taff
at a
ll fa
cilit
ies,
incl
udin
g th
ose
that
mai
ntai
n or
wor
k w
ith d
ange
rous
pat
hoge
ns a
nd to
xins
?a.
Doe
s th
e co
untr
y co
nduc
t nee
ds a
sses
smen
ts fo
r bio
safe
ty a
nd b
iose
curit
y tr
aini
ngs?
If s
o, h
ow o
ften
?b.
How
oft
en a
re s
taff
trai
ned
on b
iosa
fety
pro
cedu
res?
Wha
t abo
ut fo
r bio
secu
rity
proc
edur
es?
c. H
ow o
ften
are
sta
ff te
sted
or e
xerc
ised
on
bios
afet
y pr
oced
ures
? W
hat a
bout
for b
iose
curit
y pr
oced
ures
? d.
How
are
thes
e ex
erci
ses
mon
itore
d an
d as
sess
ed?
e. D
o th
ese
exer
cise
s in
clud
e a
proc
ess
to d
ocum
ent s
ucce
sses
and
are
as fo
r im
prov
emen
t?f.
Are
ther
e co
rrec
tive
actio
n pl
ans
in p
lace
?3.
D
oes
the
coun
try
have
in p
lace
sus
tain
ed a
cade
mic
trai
ning
in in
stitu
tions
, inc
ludi
ng th
ose
that
trai
n th
ose
who
mai
ntai
n or
wor
k w
ith d
ange
rous
pat
hoge
ns
and
toxi
ns?
a. D
o ac
adem
ic in
stitu
tions
in th
e co
untr
y ha
ve b
iosa
fety
trai
ning
pro
gram
mes
in p
lace
, inc
ludi
ng th
ose
trai
ning
to w
ork
with
dan
gero
us p
atho
gens
?4.
D
oes
the
coun
try
have
the
fund
ing
and
capa
city
to s
usta
in b
iosa
fety
and
bio
secu
rity
trai
ning
?5.
H
ow d
oes
the
natio
nal s
yste
m e
nsur
e ac
cess
to tr
ansp
ort p
rovi
ders
for n
atio
nal a
nd in
tern
atio
nal t
rans
port
atio
n of
“inf
ectio
us s
ubst
ance
s”?
6.
Is th
ere
indu
ctio
n an
d re
fresh
er tr
aini
ng fo
r all
labo
rato
ry s
taff
on b
iosa
fety
and
bio
secu
rity?
7.
Is th
ere
a m
echa
nism
to e
nsur
e an
d m
onito
r sta
ff co
mpe
tenc
e an
d st
anda
rds
of tr
aini
ng a
t all
labo
rato
ries?
PR
EV
EN
T

INTERNATIONAL HEALTH REGULATIONS (2005)
44 - Joint External Evaluation Tool - Second edition
Doc
umen
tatio
n or
evi
denc
e fo
r lev
el o
f cap
abili
tyl
Doc
umen
tatio
n of
dan
gero
us p
atho
gen
colle
ctio
ns h
ouse
d in
the
coun
try
l
Esta
blis
hmen
t, en
actm
ent a
nd e
nfor
cem
ent o
f any
rele
vant
nat
iona
l leg
isla
tion
on b
iosa
fety
and
bio
secu
rity
l
Bios
afet
y of
ficer
s tr
aine
d, re
ceiv
ing
ongo
ing
trai
ning
and
sta
tione
d at
all
labo
rato
ries
that
hav
e th
e po
tent
ial t
o ha
ndle
dan
gero
us p
atho
gens
and
hig
h ris
k ex
perim
ents
l
Polic
y do
cum
ent f
or b
ioris
k or
bio
safe
ty m
anag
emen
t in
a fa
cilit
y is
a w
ritte
n po
licy
stat
emen
t tha
t is
sign
ed a
nd re
view
ed a
nnua
llyl
OIE
cou
ntry
PVS
Eva
luat
ion
mis
sion
repo
rt (a
lso
see
sect
ion
“Pre
vent
– Z
oono
tic d
isea
se”)
l
OIE
cou
ntry
PVS
Gap
Ana
lysi
s re
port
(als
o se
e se
ctio
n “P
reve
nt –
Zoo
notic
dis
ease
”)l
OIE
cou
ntry
PVS
Lab
orat
ory
mis
sion
repo
rt
PR
EV
EN
T

INTERNATIONAL HEALTH REGULATIONS (2005)
45 - Joint External Evaluation Tool - Second edition
IMM
UN
IZAT
ION
Targ
et: A
nat
iona
l vac
cine
del
iver
y sy
stem
– w
ith n
atio
nwid
e re
ach,
effe
ctiv
e di
strib
utio
n, e
asy
acce
ss fo
r m
argi
naliz
ed p
opul
atio
ns, a
dequ
ate
cold
cha
in a
nd
ongo
ing
qual
ity c
ontr
ol –
that
is a
ble
to re
spon
d to
new
dis
ease
thre
ats.
As m
easu
red
by: 9
0–95
% c
over
age
of th
e co
untr
y’s
12-m
onth
-old
pop
ulat
ion
with
at l
east
one
dos
e of
mea
sles
-con
tain
ing
vacc
ine
(MCV
), as
dem
onst
rate
d by
co
vera
ge s
urve
ys o
r adm
inis
trat
ive
data
.
Desi
red
impa
ct: E
ffect
ive
prot
ectio
n th
roug
h ac
hiev
emen
t an
d m
aint
enan
ce o
f im
mun
izat
ion
agai
nst
mea
sles
and
oth
er e
pide
mic
-pro
ne v
acci
ne-p
reve
ntab
le
dise
ases
(VPD
s). M
easl
es im
mun
izat
ion
is e
mph
asiz
ed b
ecau
se it
is w
idel
y re
cogn
ized
as
a pr
oxy
indi
cato
r for
ove
rall
imm
uniz
atio
n ag
ains
t VPD
s. C
ount
ries
will
als
o id
entif
y an
d ta
rget
imm
uniz
atio
n to
pop
ulat
ions
at r
isk
of o
ther
epi
dem
ic-p
rone
VPD
s of
nat
iona
l im
port
ance
(suc
h as
cho
lera
, Jap
anes
e en
ceph
aliti
s,
men
ingo
cocc
al d
isea
se, t
ypho
id a
nd y
ello
w fe
ver)
. Dis
ease
s th
at a
re tr
ansf
erab
le fr
om c
attle
to h
uman
s, s
uch
as a
nthr
ax a
nd ra
bies
, are
als
o in
clud
ed.
PR
EV
EN
T

INTERNATIONAL HEALTH REGULATIONS (2005)
46 - Joint External Evaluation Tool - Second edition
Scor
eIn
dica
tors
: Im
mun
izat
ion
P.7.
1 Va
ccin
e co
vera
ge (m
easl
es) a
s pa
rt o
f nat
iona
l pro
gram
me
P.7.
2 N
atio
nal v
acci
ne a
cces
s an
d de
liver
y
No
capa
city
- 1
Less
than
50%
of t
he c
ount
ry’s
12-
mon
th-o
ld p
opul
atio
n ha
s re
ceiv
ed a
t lea
st
one
dose
of M
CV, a
s de
mon
stra
ted
by c
over
age
surv
eys
or a
dmin
istr
ativ
e da
taPl
an is
in p
lace
to
impr
ove
cove
rage
, inc
ludi
ng s
uppl
emen
tal i
mm
uniz
atio
n ac
tiviti
es
No
plan
is
in p
lace
for
nat
ionw
ide
vacc
ine
deliv
ery,
nor
have
pla
ns b
een
draf
ted
to p
rovi
de v
acci
nes
thro
ugho
ut th
e co
untr
y to
targ
et p
opul
atio
ns b
ut
not i
mpl
emen
ted
Inad
equa
te v
acci
ne p
rocu
rem
ent a
nd fo
reca
stin
g le
ad to
regu
lar
stoc
k-ou
ts
at th
e ce
ntra
l and
dis
tric
t lev
els
Lim
ited
ca
paci
ty -
2
50–
69%
of t
he c
ount
ry’s
12-
mon
th-o
ld p
opul
atio
n ha
s re
ceiv
ed a
t lea
st o
ne
dose
of M
CV, a
s de
mon
stra
ted
by c
over
age
surv
eys
or a
dmin
istr
ativ
e da
taPl
an is
in p
lace
to a
chie
ve 9
0% c
over
age
with
in th
e ne
xt fi
ve y
ears
and
incl
ude
supp
lem
enta
l im
mun
izat
ion
activ
ities
Impl
emen
tatio
n ha
s be
gun
to m
aint
ain
a co
ld c
hain
for v
acci
ne d
eliv
ery,
but
is a
vaila
ble
in fe
wer
than
40%
of d
istr
icts
in th
e co
untr
y, or
vac
cine
del
iver
y (m
aint
aini
ng c
old
chai
n) is
ava
ilabl
e to
less
than
40%
of t
he ta
rget
pop
ulat
ion
in th
e co
untr
yIn
adeq
uate
vac
cine
pro
cure
men
t an
d fo
reca
stin
g le
ad t
o oc
casi
onal
sto
ck-
outs
at c
entr
al a
nd d
istr
ict l
evel
s
Deve
lope
d ca
paci
ty -
3
70–
89%
of t
he c
ount
ry’s
12-
mon
th-o
ld p
opul
atio
n ha
s re
ceiv
ed a
t lea
st o
ne
dose
of M
CV, a
s de
mon
stra
ted
by c
over
age
surv
eys
or a
dmin
istr
ativ
e da
taPl
an is
in p
lace
to a
chie
ve 9
5% c
over
age
with
in th
e ne
xt th
ree
year
s
Vacc
ine
deliv
ery
(mai
ntai
ning
col
d ch
ain)
is a
vaila
ble
in 4
0–59
% o
f dis
tric
ts
with
in th
e co
untr
y, or
vac
cine
del
iver
y (m
aint
aini
ng c
old
chai
n) is
ava
ilabl
e to
40
–59
% o
f the
targ
et p
opul
atio
n in
the
coun
try
Vacc
ine
proc
urem
ent
and
fore
cast
ing
lead
to
no s
tock
-out
s of
vac
cine
s at
ce
ntra
l lev
el a
nd o
ccas
iona
l sto
ck-o
uts
at d
istr
ict l
evel
Dem
onst
rate
d ca
paci
ty -
4
90%
of t
he c
ount
ry’s
12-
mon
th-o
ld p
opul
atio
n ha
s re
ceiv
ed a
t lea
st o
ne d
ose
of M
CV a
nd t
he t
raje
ctor
y of
pro
gres
s, p
lans
and
cap
aciti
es a
re in
pla
ce t
o ac
hiev
e 95
% c
over
age
by 2
0201
Mor
e th
an 9
0% o
f al
l su
bnat
iona
l (d
istr
icts
/pro
vinc
es o
r st
ates
) un
its a
re
cove
red
Vacc
ine
deliv
ery
(mai
ntai
ning
col
d ch
ain)
is a
vaila
ble
in 6
0–79
% o
f dis
tric
ts
with
in th
e co
untr
y or
vac
cine
del
iver
y (m
aint
aini
ng c
old
chai
n) is
ava
ilabl
e in
60
–79
% o
f the
targ
et p
opul
atio
n in
the
coun
try
Func
tiona
l va
ccin
e pr
ocur
emen
t an
d fo
reca
stin
g, t
ake
into
acc
ount
glo
bal
stoc
ks, l
ead
to n
o st
ock-
outs
at t
he c
entr
al le
vel a
nd r
are
stoc
k-ou
ts a
t the
di
stric
t lev
el th
at a
re w
ithin
thei
r con
trol
Sust
aina
ble
capa
city
- 5
95%
of t
he c
ount
ry’s
12-
mon
th-o
ld p
opul
atio
n ha
s re
ceiv
ed a
t lea
st o
ne d
ose
of M
CV, a
s de
mon
stra
ted
by c
over
age
surv
eys
or a
dmin
istr
ativ
e da
ta; o
r 90%
of
the
cou
ntry
’s 1
2-m
onth
-old
pop
ulat
ion
has
rece
ived
at
leas
t on
e do
se
of M
CV a
nd t
he t
raje
ctor
y of
pro
gres
s, p
lans
and
cap
aciti
es a
re in
pla
ce t
o ac
hiev
e 95
% c
over
age
by 2
020
Vacc
ine
deliv
ery
(mai
ntai
ning
col
d ch
ain)
is a
vaila
ble
in g
reat
er th
an 8
0% o
f di
stric
ts w
ithin
the
cou
ntry
or
vacc
ine
deliv
ery
(mai
ntai
ning
col
d ch
ain)
is
avai
labl
e to
mor
e th
an 8
0% o
f the
nat
iona
l tar
get p
opul
atio
nSy
stem
s to
rea
ch m
argi
naliz
ed p
opul
atio
ns u
sing
cul
tura
lly a
ppro
pria
te
prac
tices
are
in p
lace
Vacc
ine
deliv
ery
has
been
test
ed th
roug
h a
natio
nwid
e va
ccin
e ca
mpa
ign
or
func
tiona
l exe
rcis
eFu
nctio
nal p
rocu
rem
ent a
nd v
acci
ne fo
reca
stin
g re
sults
in n
o st
ock-
outs
1 -
Glo
bal M
easl
es a
nd R
ubel
la: S
trat
egic
Pla
n 20
12–
2020
(htt
p://
apps
.who
.int/
iris/
bits
trea
m/1
0665
/448
55/1
/978
9241
5033
96_e
ng.p
df, a
cces
sed
23 N
ovem
ber 2
017)
.
PR
EV
EN
T

INTERNATIONAL HEALTH REGULATIONS (2005)
47 - Joint External Evaluation Tool
Cont
extu
al q
uest
ions
:
1.
Des
crib
e if
ther
e ar
e ot
her n
atio
nally
impo
rtan
t im
mun
izat
ions
out
side
the
scop
e of
the
WH
O G
loba
l Vac
cine
Act
ion
Plan
(suc
h as
cho
lera
, Jap
anes
e en
ceph
aliti
s,
men
ingo
cocc
al d
isea
se, t
ypho
id a
nd y
ello
w fe
ver)
.2.
Is
pub
lic p
erce
ptio
n on
the
topi
c of
imm
uniz
atio
n m
onito
red?
Do
vacc
inat
ion
cam
paig
ns a
ddre
ss p
erce
ptio
n is
sues
?
Tech
nica
l que
stio
ns:
P.7.
1 Va
ccin
e co
vera
ge (m
easl
es) a
s pa
rt o
f nat
iona
l pro
gram
me
1.
Doe
s th
e co
untr
y ha
ve a
nat
iona
l-le
vel i
mm
uniz
atio
n pr
ogra
mm
e or
pla
n?
a. W
hat v
acci
ne-p
reve
ntab
le d
isea
ses
are
cove
red
by th
is p
rogr
amm
e or
pla
n?b.
Lis
t the
targ
et ra
tes
for c
over
age
for e
ach
of th
ese
vacc
ines
.c.
Is
the
coun
try’
s na
tiona
l vac
cine
act
ion
plan
alig
ned
with
the
WH
O G
loba
l Vac
cine
Act
ion
Plan
?d.
Doe
s th
e co
untr
y’s
plan
take
into
acc
ount
zoo
notic
dis
ease
s of
nat
iona
l con
cern
?e.
Is
imm
uniz
atio
n m
anda
tory
or v
olun
tary
?2.
W
hat p
rogr
amm
es o
r inc
entiv
es a
re in
pla
ce to
enc
oura
ge/s
uppo
rt ro
utin
e va
ccin
atio
n?
3.
Wha
t fac
tors
dis
cour
age/
hind
er ro
utin
e va
ccin
atio
n?4.
D
escr
ibe
the
syst
ems
used
to m
onito
r vac
cine
cov
erag
e.a.
Is
the
perc
enta
ge o
f cov
erag
e w
ith m
easl
es-c
onta
inin
g an
tigen
vac
cine
and
dip
hthe
ria te
tanu
s pe
rtus
sis
trac
ked
for t
he p
opul
atio
n?b.
Whi
ch o
ffice
s or
age
ncie
s ar
e in
volv
ed in
mon
itorin
g va
ccin
e co
vera
ge fo
r the
cou
ntry
?c.
How
oft
en is
vac
cine
cov
erag
e m
easu
red?
d.
Wha
t is
the
sour
ce a
nd q
ualit
y of
the
data
use
d as
den
omin
ator
in c
over
age
estim
ates
?e.
Whi
ch s
yste
ms
are
in p
lace
to m
onito
r the
qua
lity
of c
over
age
data
? 5.
Is
ther
e sp
ecifi
c su
ppor
t (m
onet
ary
and
staf
fing)
for d
ata
gath
erin
g/re
port
ing?
P.7.
2 N
atio
nal v
acci
ne a
cces
s an
d de
liver
y1.
D
escr
ibe
how
nat
iona
l sys
tem
s en
sure
con
tinuo
us c
old
chai
ns a
s ne
cess
ary
for v
acci
ne d
eliv
ery
thro
ugho
ut th
e co
untr
y.2.
W
hat s
truc
ture
and
mec
hani
sms
are
in p
lace
to e
nsur
e a
sust
aina
ble
supp
ly to
ena
ble
a su
cces
sful
pro
gram
me?
3.
Confi
rm th
at g
loba
l vac
cine
sto
ck le
vels
are
take
n in
to a
ccou
nt w
hen
revi
ewin
g do
mes
tic s
tock
leve
ls.
4.
Des
crib
e th
e m
ost r
ecen
t nat
iona
l vac
cine
cam
paig
n(s)
or a
ny re
cent
func
tiona
l exe
rcis
es g
eare
d to
war
ds v
acci
ne d
istr
ibut
ion
and/
or a
dmin
istr
atio
n in
the
coun
try.
5.
Is th
ere
spec
ific
supp
ort (
mon
etar
y an
d st
affin
g) fo
r im
mun
izat
ion
deliv
ery?
PR
EV
EN
T

INTERNATIONAL HEALTH REGULATIONS (2005)
48 - Joint External Evaluation Tool
Refe
renc
es:
l
The
Expa
nded
Pro
gram
me
on Im
mun
izat
ion.
Wor
ld H
ealth
Org
aniz
atio
n [w
ebsi
te] (
http
://w
ww
.who
.int/
imm
uniz
atio
n/pr
ogra
mm
es_s
yste
ms/
supp
ly_c
hain
/be
nefit
s_of
_im
mun
izat
ion/
en/,
acce
ssed
23
Nov
embe
r 201
7).
l
WH
O m
easl
es a
nd p
olio
era
dica
tion
prog
ram
mes
.l
Glo
bal V
acci
ne A
ctio
n Pl
an 2
011–
2020
. Wor
ld H
ealth
Org
aniz
atio
n [w
ebsi
te] (
http
://w
ww
.who
.int/
imm
uniz
atio
n/gl
obal
_vac
cine
_act
ion_
plan
/en/
, acc
esse
d 23
Nov
embe
r 201
7).
l
Glo
bal M
easl
es a
nd R
ubel
la –
Str
ateg
ic P
lan
2012
–20
20.
Gen
eva:
Wor
ld H
ealth
Org
aniz
atio
n; 2
012
(http
://ap
ps.w
ho.in
t/iri
s/bi
tstre
am/1
0665
/448
55/1
/ 97
8924
1503
396_
eng.
pdf?
ua=1
, acc
esse
d 23
Nov
embe
r 201
7).
PR
EV
EN
T

INTERNATIONAL HEALTH REGULATIONS (2005)
49 - Joint External Evaluation Tool - Second edition
DETE
CTN
ATIO
NAL
LAB
ORA
TORY
SYS
TEM
1 Ta
rget
: A S
urve
illan
ce w
ith a
nat
iona
l lab
orat
ory
syst
em, in
clud
ing
all r
elev
ant s
ecto
rs2 ,
part
icul
arly
hum
an a
nd a
nim
al h
ealth
, and
effe
ctiv
e m
oder
n3 poi
nt-o
f-ca
re
and
labo
rato
ry-b
ased
dia
gnos
tics.
As m
easu
red
by: (
1) A
nat
ionw
ide
labo
rato
ry s
yste
m a
ble
to re
liabl
y co
nduc
t at l
east
five
of t
he 1
0 co
re te
sts4 o
n ap
prop
riate
ly id
entifi
ed a
nd c
olle
cted
out
brea
k sp
ecim
ens
tran
spor
ted
safe
ly a
nd s
ecur
ely
to a
ccre
dite
d la
bora
torie
s fr
om a
t lea
st 8
0% o
f int
erm
edia
te le
vels
/dis
tric
ts in
the
coun
try.
(2) E
xist
ence
of n
atio
nal
qual
ity la
bora
tory
sta
ndar
ds a
nd s
yste
m fo
r lic
enci
ng la
bora
torie
s.
Desi
red
impa
ct: E
ffect
ive
use
of a
nat
ionw
ide
labo
rato
ry s
yste
m, i
nclu
ding
all
rele
vant
sec
tors
, cap
able
of s
afel
y an
d ac
cura
tely
det
ectin
g an
d ch
arac
teriz
ing
path
ogen
s ca
usin
g ep
idem
ic d
isea
se in
clud
ing
both
kno
wn
and
unkn
own
thre
ats
from
all
part
s of
the
coun
try.
Exp
ande
d de
ploy
men
t, ut
iliza
tion
and
sust
ainm
ent
of m
oder
n, s
afe,
sec
ure,
affo
rdab
le a
nd a
ppro
pria
te d
iagn
ostic
test
s or
dev
ices
est
ablis
hed.
1 -
The
Nat
iona
l Lab
orat
ory
Syst
em is
a c
olla
bora
tive
com
mun
ity o
f clin
ical
labo
rato
ries,
pub
lic h
ealth
labo
rato
ries,
and
man
y in
divi
dual
par
tner
s w
ho in
itiat
e te
sts
and/
or u
se te
st re
sults
(htt
ps:/
/ww
w.n
cbi.n
lm.n
ih.g
ov/p
mc/
2 -
Rele
vant
sec
tors
incl
ude
priv
ate
and
publ
ic s
ecto
rs, s
uch
as: a
ll le
vels
of t
he h
ealth
car
e sy
stem
(nat
iona
l, su
bnat
iona
l and
com
mun
ity/p
rimar
y pu
blic
hea
lth);
NG
Os;
div
isio
ns/a
ctiv
ities
of o
ther
sec
tors
whi
ch a
ffect
pub
lic h
ealth
, su
ch a
s m
inis
trie
s of
agr
icul
ture
(qu
aran
tine
and
mov
emen
t co
ntro
l aut
horit
y, im
port
/exp
ort
regu
latio
ns, d
isea
se d
iagn
osis
and
con
trol
fina
ncin
g, z
oono
sis,
vet
erin
ary
labo
rato
ry e
tc.),
tra
nspo
rt (
tran
spor
t po
licy,
civi
l avi
atio
n,
port
s an
d m
ariti
me
tran
spor
t), t
rade
and
/or
indu
stry
(foo
d sa
fety
and
qua
lity
cont
rol),
fore
ign
trad
e (c
onsu
mer
pro
tect
ion,
con
trol
of c
ompu
lsor
y st
anda
rd e
nfor
cem
ent)
, com
mun
icat
ion,
def
ence
, tre
asur
y or
fina
nce
(cus
tom
s),
envi
ronm
ent,
inte
rior,
heal
th, t
ouris
m; h
ealth
, tou
rism
; the
hom
e of
fice;
med
ia; a
nd re
gula
tory
bod
ies.
3 -
Mod
ern
mea
ns n
ovel
mol
ecul
ar a
nd c
ellu
lar m
etho
ds c
apab
le o
f pro
mpt
and
acc
urat
e id
entifi
catio
n of
pat
hoge
ns in
a ti
mes
avin
g an
d co
st-e
ffect
ive
man
ner.
4 -
10 c
ore
test
s: A
list
in e
ach
coun
try
incl
udes
six
test
ing
met
hods
sel
ecte
d ac
cord
ing
to th
e IH
R’s
imm
edia
tely
not
ifiab
le li
st a
nd th
e W
HO
top
10 c
ause
s of
dea
th in
low
-inc
ome
coun
trie
s: p
olym
eras
e ch
ain
reac
tion
test
ing
for
influ
enza
viru
s; v
irus
cultu
re fo
r po
liovi
rus;
ser
olog
y fo
r H
IV; m
icro
scop
y fo
r M
ycob
acte
rium
tube
rcul
osis
; rap
id d
iagn
ostic
test
ing
for
Plas
mod
ium
spp
.; an
d ba
cter
ial c
ultu
re fo
r Sa
lmon
ella
ent
eriti
dis
sero
type
typh
i. Th
ese
six
met
hods
are
crit
ical
to th
e de
tect
ion
of e
pide
mic
-pro
ne e
mer
ging
dis
ease
s. C
ompe
tenc
y in
thes
e m
etho
ds is
indi
cate
d by
suc
cess
ful t
estin
g fo
r the
spe
cific
pat
hoge
ns li
sted
. The
rem
aini
ng fo
ur te
sts
shou
ld b
e se
lect
ed b
y th
e co
untr
y on
the
basi
s of
maj
or n
atio
nal p
ublic
hea
lth c
once
rns.
DE
TE
CT

INTERNATIONAL HEALTH REGULATIONS (2005)
50 - Joint External Evaluation Tool - Second edition
Scor
e5
Indi
cato
rs: N
atio
nal l
abor
ator
y sy
stem
6,7,
8 D.
1.1
Labo
rato
ry te
stin
g3 for
de
tect
ion
of p
riorit
y di
seas
es10
D.
1.2
Spec
imen
refe
rral
and
tr
ansp
ort s
yste
m11
D.
1.3
Effe
ctiv
e na
tiona
l dia
gnos
tic n
etw
ork12
D.
1.4
Labo
rato
ry q
ualit
y sy
stem
13
No
capa
city
- 1
Coun
try
has
not t
aken
a ri
sk-b
ased
ap
proa
ch t
o de
term
ine
at le
ast
10
prio
rity
dise
ases
for c
ore
test
ing14
No
syst
em15
in p
lace
for
tra
nspo
r-tin
g sp
ecim
ens
from
int
erm
edia
te
leve
ls/d
istr
icts
to
natio
nal
labo
ra-
torie
s; o
nly
ad h
oc tr
ansp
orta
tion16
is
ava
ilabl
e
No
evid
ence
of u
se o
f rap
id a
nd a
ccur
ate
poin
t-of
-car
e/17
farm
-bas
ed d
iagn
ostic
s18 a
nd la
bo-
rato
ry-b
ased
dia
gnos
tics,
and
no
tier-
spec
ific
diag
nost
ic te
stin
g st
rate
gies
are
doc
umen
ted
Ther
e ar
e no
nat
iona
l la
bo-r
ator
y qu
ality
sta
ndar
ds
Lim
ited
ca
paci
ty –
2
Coun
try
has
defin
ed 1
0 co
re t
ests
an
d th
e na
tiona
l lab
orat
ory
syst
em
is c
ondu
ctin
g on
e to
two
core
test
s an
d qu
ality
ass
uran
ce p
roce
ss is
in
plac
e
Syst
em i
s in
pla
ce t
o tr
ansp
ort
spec
imen
s to
nat
iona
l lab
orat
orie
s fr
om le
ss th
an 5
0% o
f int
erm
edia
te
leve
ls/d
istr
icts
in
the
coun
try
for
adva
nced
dia
gnos
tics
Min
imal
, la
bora
tory
di
agno
stic
ca
pabi
lity
exis
ts w
ithin
the
cou
ntry
, but
no
tier-
spec
ific
diag
nost
ic te
stin
g st
rate
gies
are
doc
umen
ted.
Po
int-
of-c
are/
farm
-bas
ed
diag
nost
ics
are
bein
g us
ed fo
r cou
ntry
prio
rity
dise
ases
19
Nat
iona
l qu
ality
st
anda
rds
have
be
en d
evel
oped
but
ther
e is
no
sys-
tem
for v
erify
ing
thei
r im
plem
enta
-tio
n
Deve
lope
d ca
paci
ty –
3
Nat
iona
l la
bora
tory
sy
stem
is
co
nduc
ting
thre
e to
four
cor
e te
sts;
su
scep
tibili
ty t
estin
g an
d qu
ality
as
sura
nce
proc
ess
are
in p
lace
Syst
em i
s in
pla
ce t
o tr
ansp
ort
spec
imen
s to
nat
iona
l lab
orat
orie
s fr
om 5
0–80
% o
f in
term
edia
te l
e-ve
ls/d
istr
icts
with
in th
e co
untr
y fo
r ad
vanc
ed d
iagn
ostic
s
Tier
-spe
cific
di
agno
stic
te
stin
g st
rate
gies
ar
e do
cum
ente
d, b
ut n
ot f
ully
im
plem
ente
d.
Coun
try
is p
rofic
ient
in
clas
sica
l di
agno
stic
te
chni
ques
in
clud
ing
bact
erio
logy
, se
rolo
gy
and
PCR
in s
elec
t lab
orat
orie
s bu
t has
lim
ited
refe
rral
and
con
firm
ator
y pr
oces
ses.
Cou
ntry
is
usi
ng p
oint
-of-
care
dia
gnos
tics
for
coun
try
prio
rity
dise
ases
A sy
stem
of
licen
sing
of
labo
rato
-rie
s th
at i
nclu
des
conf
orm
ity t
o a
natio
nal q
ualit
y st
anda
rd e
xist
s bu
t it
is v
olun
tary
or
is n
ot a
req
uire
-m
ent f
or a
ll la
bora
torie
s
5 -
For f
ull s
core
s, c
apab
ilitie
s sh
ould
be
sepa
rate
ly e
valu
ated
bot
h in
the
hum
an a
nd a
nim
al (l
ives
tock
, com
pani
on a
nim
al a
nd w
ildlif
e) h
ealth
sec
tors
and
mec
hani
sms
for r
egul
ar jo
int p
lann
ing,
sha
ring
of in
form
atio
n, c
olla
bora
tion,
co
mm
unic
atio
n, a
nd jo
int p
olic
y-de
velo
pmen
t in
a O
ne H
ealth
app
roac
h sh
ould
be
in p
lace
. The
fina
l sco
re s
houl
d be
bas
ed o
n th
e lo
wer
of t
he s
core
s fo
r the
hum
an a
nd a
nim
al h
ealth
sec
tors
.6
- Th
e in
dica
tors
refe
r to
the
natio
nal l
abor
ator
y ca
paci
ty fo
r the
cou
ntry
.7
- Li
nk th
is te
chni
cal a
rea
with
oth
er te
chni
cal a
reas
that
requ
ire la
bora
tory
test
ing
capa
city
(suc
h as
sur
veill
ance
, zoo
nosi
s, fo
od s
afet
y, AM
R)8
- Th
e na
tiona
l lab
orat
ory
syst
em s
houl
d in
clud
e:
• Abi
lity
to c
ondu
ct a
t lea
st fi
ve o
f the
10
core
test
s (s
ee fo
otno
te 4
).• A
bilit
y to
tran
spor
t spe
cim
ens
safe
ly a
nd q
uick
ly fr
om 8
0% o
r mor
e of
inte
rmed
iate
leve
ls/d
istr
icts
to n
atio
nal l
abor
ator
y fa
cilit
ies
for a
dvan
ced
diag
nost
ics.
• Abi
lity
to c
ondu
ct h
igh-
leve
l dia
gnos
tic te
stin
g at
nat
iona
l lab
orat
orie
s or
hav
e ag
reem
ents
with
regi
onal
net
wor
ks to
ens
ure
test
ing
is a
vaila
ble.
• Abi
lity
to te
st fo
r ant
imic
robi
al s
usce
ptib
ility
for p
riorit
y pa
thog
ens
in h
uman
hea
lth a
nd in
ani
mal
food
pro
duct
ion.
9 -
Rapi
d di
agno
stic
test
per
form
ed a
nd re
sult
obta
ined
with
in 1
2–48
hou
rs o
r in
a tim
ely
man
ner f
or tr
igge
ring
and
guid
ing
cont
rol m
easu
res.
10 -
Prio
rity
dise
ases
– b
ased
on
the
loca
l epi
dem
iolo
gy a
nd a
s de
fined
in n
atio
nal s
urve
illan
ce g
uide
lines
for p
riorit
y di
seas
es a
nd/o
r not
ifiab
le d
isea
ses
(ref
er to
Glo
ssar
y an
d fo
otno
te 4
). 11
- T
rans
port
“sys
tem
”: Ac
cura
tely
col
lect
and
mai
ntai
n sp
ecim
en in
tegr
ity a
nd a
s w
ritte
n in
the
SOP.
12 -
The
re is
crit
ical
com
pete
ncy
in th
e PV
S to
ol C
C II-
1: V
eter
inar
y la
bora
tory
dia
gnos
is. T
he O
IE c
ondu
cts
PVS
labo
rato
ry m
issi
ons
whe
re th
e ne
twor
k as
pect
s ar
e ev
alua
ted.
13 -
The
re is
crit
ical
com
pete
ncy
in th
e PV
S to
ol C
C II-
2: L
abor
ator
y qu
ality
ass
uran
ce.
14 -
Cor
e te
sts
can
incl
ude
loca
l prio
rity
test
s de
term
ined
by
coun
try-
sele
cted
indi
cato
r pat
hoge
ns o
n th
e ba
sis
of m
ajor
nat
iona
l pub
lic h
ealth
con
cern
. For
the
anim
al h
ealth
sec
tor,
core
test
s m
ean
the
abili
ty to
test
for a
ll di
seas
es
on th
e ag
reed
list
of p
riorit
y zo
onot
ic d
isea
ses.
If th
ere
is n
o su
ch li
st, t
hen
it is
the
abili
ty to
test
for d
isea
ses
on th
e lis
t of p
riorit
y zo
onot
ic d
isea
ses
of th
e pu
blic
hea
lth s
ecto
r.15
- A
n or
gani
zed
or e
stab
lishe
d pr
oced
ure
in th
e co
untr
y or
out
side
. Som
e is
land
cou
ntrie
s m
ay n
ot re
quire
a s
yste
m in
pla
ce a
t the
cou
ntry
leve
l and
can
hav
e ac
cess
to re
gion
al o
r int
erna
tiona
l lab
orat
orie
s.
16 -
“Ad
hoc”
tran
spor
t sys
tem
: no
SOP
on h
ow to
tran
spor
t sam
ple.
17 -
Poi
nt-o
f-ca
re d
iagn
ostic
s is
med
ical
dia
gnos
tic te
stin
g pe
rfor
med
out
side
the
clin
ical
labo
rato
ry in
clo
se p
roxi
mity
to w
here
the
patie
nt is
rec
eivi
ng c
are.
Poi
nt-o
f-ca
re d
iagn
ostic
s is
usu
ally
per
form
ed b
y no
n-la
bora
tory
pe
rson
nel (
e.g.
with
rapi
d di
agno
stic
kits
) and
the
resu
lts a
re u
sed
for c
linic
al d
ecis
ion-
mak
ing.
18 -
Far
m b
ased
dia
gnos
tics:
Rap
id d
iagn
ostic
test
that
can
be
used
in a
farm
for t
estin
g sa
mpl
es.
19 -
It is
impo
rtan
t tha
t the
pro
cess
of d
efini
ng p
riorit
y di
seas
es in
volv
es v
eter
inar
y se
rvic
es a
nd a
ppro
pria
te in
tern
atio
nal c
onsu
ltatio
n (s
uch
as w
ith O
IE a
nd W
HO
).
DE
TE
CT

INTERNATIONAL HEALTH REGULATIONS (2005)
51 - Joint External Evaluation Tool - Second edition
Dem
onst
rate
d ca
paci
ty –
4
Nat
iona
l la
bora
tory
sy
stem
is
co
nduc
ting
thre
e to
four
cor
e te
sts;
su
scep
tibili
ty t
estin
g an
d qu
ality
as
sura
nce
proc
ess
are
in p
lace
Syst
em i
s in
pla
ce t
o tr
ansp
ort
spec
imen
s to
nat
iona
l lab
orat
orie
s fr
om a
t le
ast
80%
of
inte
rmed
iate
le
vels
/dis
tric
ts w
ithin
the
cou
ntry
fo
r adv
ance
d di
agno
stic
s
Coun
try
has
docu
men
ted
and
fully
im
ple-
men
ted
tier-
spec
ific
diag
nost
ic te
stin
g st
rate
-gi
es, a
nd a
nat
iona
l sys
tem
of s
ampl
e re
ferr
al
and
confi
rmat
ory
diag
nost
ics
culm
inat
ing
in
perf
orm
ance
of m
olec
ular
or s
erol
ogic
al te
ch-
niqu
es a
t nat
iona
l and
/or r
egio
nal l
abor
ator
ies
Poin
t-of
-car
e/fa
rm-b
ased
di
agno
stic
s ar
e be
ing
used
acc
ordi
ng to
tier
-spe
cific
dia
gnos
-tic
test
ing
stra
tegi
es fo
r dia
gnos
is o
f cou
ntry
pr
iorit
y di
seas
es
Man
dato
ry li
cens
ing
of a
ll la
bora
-to
ries
is i
n pl
ace
and
conf
orm
ity
to a
nat
iona
l qu
ality
sta
ndar
d is
re
quire
d
Sust
aina
ble
capa
city
– 5
Syst
ems
for q
ualit
y as
sura
nce
are
in p
lace
and
res
ults
are
dis
sem
i-na
ted
regu
larly
Tran
spor
t of
spe
cim
ens
to/f
rom
ot
her
labo
rato
ries
in
the
regi
on
and
fund
ed f
rom
the
hos
t co
untr
y bu
dget
Coun
try
has
capa
bilit
y fo
r pe
rfor
min
g ad
-va
nced
mol
ecul
ar a
nd s
erol
ogic
al te
chni
ques
as
par
t of a
nat
iona
l sys
tem
of s
ampl
e re
ferr
al
and
confi
rmat
ory
diag
nost
ics
Coun
try
is u
sing
acc
urat
e po
int-
of-c
are/
farm
-ba
sed
diag
nost
ics
as d
efine
d by
tie
r-sp
ecifi
c di
agno
stic
test
ing
stra
tegi
esCo
untr
y is
als
o fo
rmal
ly e
ngag
ing
othe
r re
-fe
renc
e la
bora
torie
s fo
r te
stin
g ca
paci
ty n
ot
avai
labl
e in
the
coun
try,
whe
re n
eede
d, to
sup
-pl
emen
t the
nat
iona
l dia
gnos
tic te
stin
g st
rate
-gi
es f
or s
even
or
mor
e of
the
10
labo
rato
ry
test
s re
quire
d fo
r pr
iorit
y di
seas
es. C
ount
ry is
ab
le to
sus
tain
this
cap
abili
ty o
n its
ow
n
Man
dato
ry li
cens
ing
of a
ll la
bora
-to
ries
is in
pla
ce a
nd c
onfo
rmity
to
an in
tern
atio
nal q
ualit
y st
anda
rd is
re
quire
d
Cont
extu
al q
uest
ions
:
1.
Wha
t are
the
prio
rity
dise
ases
of t
he c
ount
ry a
nd w
hich
of t
hese
are
test
ed in
the
coun
try?
2.
Whi
ch o
f the
10
core
test
s is
the
coun
try
capa
ble
of c
ondu
ctin
g?3.
D
escr
ibe
the
stru
ctur
e of
the
labo
rato
ry s
yste
m, i
nclu
ding
the
num
ber o
f lab
orat
orie
s, a
t loc
al, i
nter
med
iate
leve
ls/d
istr
icts
, and
the
natio
nal l
evel
.a.
How
man
y re
fere
nce
labo
rato
ries
exis
t and
for w
hich
mic
robe
s?b.
Do
loca
l clin
icia
ns h
ave
the
cust
om o
f usi
ng th
e la
bora
tory
sys
tem
? Are
ther
e na
tiona
l gui
delin
es in
pla
ce fo
r clin
icia
ns o
n ho
w to
con
duct
mic
robi
olog
ical
te
sts
in s
peci
fic s
yndr
omes
, suc
h as
sev
ere
pneu
mon
ia, s
ever
e di
arrh
oea
or s
uspe
cted
men
ingi
tis?
c. W
hat s
yste
ms
exis
t for
get
ting
labo
rato
ry re
sults
bac
k to
pra
ctiti
oner
s? H
ow lo
ng d
oes
this
take
?d.
Wha
t per
cent
age
of th
e po
pula
tion
has
acce
ss to
labo
rato
ry s
ervi
ces
for t
he 1
0 pr
iorit
y di
seas
es?
DE
TE
CT

INTERNATIONAL HEALTH REGULATIONS (2005)
52 - Joint External Evaluation Tool - Second edition
4.
Hav
e na
tiona
l lab
orat
orie
s be
en a
ccre
dite
d?e.
If y
es, t
o w
hat s
tand
ard?
f. Ar
e gu
idel
ines
and
pro
toco
ls fo
r qua
lity
man
agem
ent s
yste
m e
nfor
ced
and
in u
se b
y pu
blic
and
ani
mal
hea
lth la
bora
torie
s?g.
Is
ther
e a
natio
nal b
ody
that
ove
rsee
s in
tern
al q
ualit
y co
ntro
ls a
nd E
QA
sche
mes
for p
ublic
hea
lth la
bora
torie
s at
all
leve
ls?
h. A
re a
ll la
bora
torie
s en
rolle
d in
the
EQA
prog
ram
me
for t
he te
sts
they
per
form
to d
etec
t any
of t
he 1
0 pr
iorit
y di
seas
es?
5.
How
is la
bora
tory
dat
a on
zoo
notic
dis
ease
s sh
ared
bet
wee
n hu
man
and
ani
mal
hea
lth la
bora
torie
s? A
re th
e tw
o in
tero
pera
ble
data
sys
tem
s? (S
ee re
late
d qu
estio
ns in
Pre
vent
– Z
oono
tic d
isea
se.)
6.
Is p
erso
nal p
rote
ctiv
e eq
uipm
ent a
vaila
ble
for l
abor
ator
y st
aff?
i. H
ow is
ava
ilabi
lity
of p
erso
nal p
rote
ctiv
e eq
uipm
ent t
rack
ed fo
r lab
orat
orie
s?j.
Des
crib
e th
e tr
aini
ng p
roce
dure
s fo
r per
sona
l pro
tect
ive
equi
pmen
t use
in n
atio
nal l
abor
ator
ies.
7.
Wha
t bio
secu
rity/
bios
afet
y tr
aini
ng is
pro
vide
d to
labo
rato
ry w
orke
rs?
(See
rela
ted
tech
nica
l que
stio
ns in
Pre
vent
– B
iosa
fety
and
bio
secu
rity.
)
Tech
nica
l que
stio
ns:
D.1.
1 La
bora
tory
test
ing
for d
etec
tion
of p
riorit
y di
seas
es1.
Is
ther
e a
set o
f nat
iona
l dia
gnos
tic a
lgor
ithm
s fo
r per
form
ance
of c
ore
labo
rato
ry te
sts
that
has
bee
n al
igne
d w
ith in
tern
atio
nal s
tand
ards
(i.e
. Clin
ical
and
La
bora
tory
Sta
ndar
ds In
stitu
te (C
LSI),
OIE
, WH
O)?
2.
How
man
y of
the
core
test
s fo
r the
10
prio
rity
dise
ases
are
impl
emen
ted
effe
ctiv
ely
acro
ss th
e tie
red
labo
rato
ry n
etw
ork?
a. O
f the
test
s th
at c
anno
t be
cond
ucte
d, a
re th
ere
plan
s an
d tim
elin
es in
pla
ce to
gai
n th
is c
apac
ity w
ithin
the
next
yea
r?b.
Are
ther
e of
ficia
l agr
eem
ents
with
labo
rato
ries
outs
ide
the
coun
try
for s
peci
aliz
ed te
stin
g no
t ava
ilabl
e in
the
coun
try?
3.
Has
the
coun
try
iden
tified
four
cou
ntry
-spe
cific
test
s? H
as th
e co
untr
y pr
iorit
ized
impl
emen
tatio
n of
the
10 c
ore
test
s? W
hat i
s th
e an
ticip
ated
test
ing
load
for
each
(or h
ighe
st p
riorit
y) te
st?
Has
the
coun
try
sele
cted
whi
ch p
roto
cols
to u
se fo
r eac
h te
st?
Doe
s th
e co
untr
y ha
ve p
lans
in p
lace
for p
rocu
rem
ent o
f sup
plie
s?
Doe
s th
e la
bora
tory
hav
e qu
ality
ass
uran
ce/q
ualit
y co
ntro
l/Qua
lity
Man
agem
ent S
yste
m (Q
MS)
pla
ns in
pla
ce?
4.
Do
labo
rato
ries
have
the
requ
ired
equi
pmen
t (ba
sed
on te
stin
g ap
prop
riate
for t
he le
vel i
n th
e tie
red
labo
rato
ry n
etw
ork)
to s
uppo
rt c
ore
labo
rato
ry te
sts?
Are
m
aint
enan
ce c
ontr
acts
in p
lace
for k
ey e
quip
men
t and
is p
reve
ntiv
e m
aint
enan
ce im
plem
ente
d re
gula
rly?
5.
How
doe
s th
e co
untr
y en
sure
sta
ndar
diza
tion
of te
stin
g? D
o na
tiona
l lab
orat
orie
s se
nd o
ut s
ampl
es fo
r tes
ting
valid
atio
n of
mor
e lo
cal/r
egio
nal l
abor
ator
ies?
6.
Do
the
min
istr
ies
of h
ealth
, agr
icul
ture
or o
ther
rele
vant
min
istr
ies
have
in-c
ount
ry p
rodu
ctio
n an
d/or
pro
cure
men
t pro
cess
es fo
r acq
uirin
g ne
cess
ary
med
ia
and
reag
ents
for p
erfo
rman
ce o
f cor
e la
bora
tory
test
s?7.
H
ow d
oes
the
labo
rato
ry s
yste
m m
anag
e te
stin
g an
d re
port
ing
on a
ntim
icro
bial
sus
cept
ibili
ty?
a. D
oes
a na
tiona
l pla
n fo
r the
det
ectio
n an
d re
port
ing
of a
ntim
icro
bial
resi
stan
t pat
hoge
ns e
xist
? b.
How
man
y la
bora
torie
s ar
e ab
le to
con
duct
sen
sitiv
ity te
stin
g an
d re
port
ing?
c.
Whi
ch p
atho
gens
and
ant
imic
robi
al s
usce
ptib
ility
pat
tern
s ca
n be
test
ed fo
r?
d. H
ow a
re th
ese
data
val
idat
ed?
Is th
e da
ta re
port
ing
and
valid
atio
n m
echa
nism
func
tiona
l?
DE
TE
CT

INTERNATIONAL HEALTH REGULATIONS (2005)
53 - Joint External Evaluation Tool - Second edition
e. H
ave
labo
rato
ry m
etho
ds b
een
verifi
ed a
nd t
he q
ualit
y m
onito
red,
suc
h as
thr
ough
ext
erna
l qua
lity
assu
ranc
e? D
oes
the
labo
rato
ry p
artic
ipat
e in
na
tiona
l/in
tern
atio
nal p
rofic
ienc
y te
stin
g? Is
ther
e a
QM
S fo
r lab
orat
orie
s in
the
AMR
surv
eilla
nce
syst
em?
f. H
ow a
nd to
who
m is
dat
a re
port
ed?
g. W
hat i
nter
pret
ive
crite
ria a
re u
sed
to re
port
ant
imic
robi
al s
usce
ptib
ility
test
ing
resu
lts (s
uch
as C
LSI, E
urop
ean
Com
mitt
ee o
n An
timic
robi
al S
usce
ptib
ility
Te
stin
g (E
UCA
ST))
? Ar
e cl
inic
al b
reak
poin
ts u
sed
or e
pide
mio
logi
cal c
ut-o
ffs?
D.1.
2 Sp
ecim
en re
ferr
al a
nd tr
ansp
ort s
yste
m1.
Is
the
spec
imen
refe
rral
net
wor
k do
cum
ente
d fo
r eac
h of
the
test
s ne
cess
ary
to d
etec
t and
con
firm
aet
iolo
gies
of t
he 1
0 pr
iorit
y di
seas
es?
2.
Is th
ere
proo
f of a
func
tioni
ng re
ferr
al s
yste
m a
vaila
ble?
For
exa
mpl
e, d
ata
on th
e nu
mbe
r of i
sola
tes/
sam
ples
sub
mitt
ed to
nat
iona
l ref
eren
ce la
bora
tory
for
key
dise
ase(
s) p
er 1
00 0
00 p
opul
atio
n.3.
D
escr
ibe
the
syst
em fo
r spe
cim
en tr
ansp
ort f
rom
inte
rmed
iate
leve
ls (d
istr
icts
) to
refe
renc
e la
bora
torie
s an
d na
tiona
l lab
orat
orie
s.a.
Are
sta
ndar
dize
d SO
Ps in
pla
ce fo
r spe
cim
en c
olle
ctio
n, p
acka
ging
and
tran
spor
t?b.
Is
spec
imen
tran
spor
t (su
ch a
s co
urie
r con
trac
ts) s
uppo
rted
by
the
heal
th m
inis
try
or it
s pa
rtne
rs?
c. W
ill th
e tr
ansp
ort s
yste
m in
clud
e m
otor
bike
s, p
ost o
ffice
and
spe
cial
cou
riers
, to
be u
sed
for a
ll sp
ecim
ens
(e.g
. drie
d bl
ood
spot
s an
d st
ools
)?
d. I
s th
ere
a w
ay to
“rus
h” h
igh
prio
rity
spec
imen
s (e
.g. s
uspe
ct v
iral h
aem
orrh
agic
feve
r spe
cim
ens)
? e.
Is
trac
king
in p
lace
to d
ocum
ent s
peci
men
shi
pmen
t and
rece
ipt?
f.
Is tr
aini
ng in
pla
ce fo
r lab
orat
orie
s to
use
the
syst
em?
g. A
re g
uide
lines
in p
lace
for s
ched
ule
and
tran
sit t
imes
? h.
Is
ther
e a
prot
ocol
(s) w
ritte
n an
d if
so, a
re la
bora
torie
s aw
are
of it
and
do
they
use
it?
4.
Doe
s th
e ho
st c
ount
ry p
artic
ipat
e in
a re
gion
al (i
nter
natio
nal)
labo
rato
ry n
etw
ork?
D.1.
3 Ef
fect
ive
natio
nal d
iagn
ostic
net
wor
k 1.
D
oes
the
coun
try
have
str
ateg
ies
of c
ondu
ctin
g po
int-
of-c
are/
farm
-bas
ed d
iagn
ostic
s? If
yes
,a.
Wha
t are
thos
e te
sts
and
at w
hat l
evel
s ar
e th
ose
avai
labl
e?b.
Do
thes
e te
sts
cove
r the
cou
ntry
’s p
riorit
y di
seas
es?
c. I
f not
, is
the
coun
try
deve
lopi
ng th
ese
stra
tegi
es?
2.
Has
the
coun
try
deve
lope
d st
rate
gies
for t
ier-
spec
ific
diag
nost
ics?
If n
ot, i
s th
e co
untr
y de
velo
ping
thes
e st
rate
gies
?3.
Is
ther
e a
plan
and
/or m
echa
nism
in p
lace
to im
prov
e th
e av
aila
bilit
y of
poi
nt-o
f-ca
re d
iagn
ostic
s at
clin
ical
site
s ac
ross
the
coun
try?
4.
Do
the
min
istr
ies
of h
ealth
/agr
icul
ture
, or o
ther
rele
vant
min
istr
ies,
hav
e in
-cou
ntry
pro
duct
ion
and/
or p
rocu
rem
ent p
roce
sses
for a
cqui
ring
nece
ssar
y m
edia
an
d re
agen
ts fo
r the
per
form
ance
of c
ore
labo
rato
ry te
sts?
5.
Doe
s th
e co
untr
y pe
rfor
m a
dvan
ced
mol
ecul
ar a
nd s
erol
ogic
al te
stin
g fo
r ref
erre
d sa
mpl
es a
nd fo
r con
firm
atio
n/re
-con
firm
atio
n of
dia
gnos
is?
DE
TE
CT

INTERNATIONAL HEALTH REGULATIONS (2005)
54 - Joint External Evaluation Tool - Second edition
D.1.
4 La
bora
tory
qua
lity
syst
em1.
Is
ther
e a
natio
nal b
ody
in c
harg
e of
labo
rato
ry li
cens
ing?
2.
Is th
ere
a na
tiona
l bod
y in
cha
rge
of la
bora
tory
insp
ectio
n?a.
If y
es, d
escr
ibe
the
insp
ectio
n m
echa
nism
(fre
quen
cy, p
roce
dure
s, s
anct
ions
, etc
.)6.
Is
ther
e a
natio
nal b
ody
in c
harg
e of
labo
rato
ry c
ertifi
catio
n (e
.g. u
sing
ISO
900
1)?
a. I
f yes
, pro
vide
nam
e(s)
.7.
Is
ther
e a
natio
nal b
ody
in c
harg
e of
labo
rato
ry a
ccre
dita
tion
(e.g
. usi
ng IS
O 1
5189
)?a.
If y
es, p
rovi
de n
ame(
s).
b. I
f not
, do
labo
rato
ries
use
serv
ices
of f
orei
gn n
atio
nal/
regi
onal
acc
redi
tatio
n bo
dies
?c.
If y
es, p
rovi
de n
ame(
s).
8.
Are
som
e la
bora
torie
s ac
cred
ited
for d
isea
se-s
peci
fic te
stin
g by
WH
O (e
.g. p
olio
, mea
sles
, HIV
gen
otyp
ing)
?9.
Pr
ovid
e th
e nu
mbe
r of l
abor
ator
ies
cert
ified
or a
ccre
dite
d an
d sp
ecify
to w
hich
sta
ndar
d.10
. Is
ther
e a
spec
ific
natio
nal d
ocum
ent t
hat d
escr
ibes
the
regi
stra
tion
proc
edur
e fo
r in
vitro
dia
gnos
tic d
evic
es (i
.e. k
its a
nd re
agen
ts)?
11.
Is th
ere
a na
tiona
l reg
ulat
ory
auth
ority
resp
onsi
ble
for i
n vi
tro d
iagn
ostic
dev
ices
qua
lifica
tion
or re
gist
ratio
n?a.
If y
es, p
rovi
de a
sum
mar
y of
the
qual
ifica
tion
or re
gist
ratio
n m
echa
nism
s.12
. Be
side
s th
e in
spec
tion,
cer
tifica
tion
or a
ccre
dita
tion
deta
iled
abov
e is
any
oth
er k
ind
of s
uper
visi
on o
rgan
ized
?a.
If y
es o
r par
tial,
desc
ribe
the
supe
rvis
ion
plan
and
pro
cedu
res
(e.g
. thr
ough
spe
cific
net
wor
ks li
ke tu
berc
ulos
is c
ontr
ol o
r sur
veill
ance
pro
gram
mes
).13
. Ar
e th
ere
stan
dard
ized
sup
ervi
sion
che
cklis
ts o
r pro
cedu
res?
14.
Whe
n su
perv
ised
, do
the
labo
rato
ries
rece
ive
a re
port
afte
r eac
h su
perv
isio
n vi
sit?
15.
Are
ther
e in
dica
tors
to m
easu
re p
rogr
ess
in la
bora
tory
test
qua
lity?
If y
es, l
ist t
hese
indi
cato
rs.
16.
Doe
s th
e co
untr
y ha
ve a
nat
iona
l EQ
A pr
ogra
mm
e (p
rofic
ienc
y-te
stin
g or
rech
ecki
ng) i
n th
e fo
llow
ing
area
s:a.
bac
terio
logy
b. v
irolo
gyc.
ser
olog
yd.
par
asito
logy
e. b
ioch
emis
try
f. ha
emat
olog
yg.
ana
tom
ical
pat
holo
gyh.
cyt
ogen
etic
i. tr
ansf
usio
n m
edic
ine?
17.
Des
crib
e th
e na
tiona
l EQ
A pr
ogra
mm
e(s)
/org
aniz
atio
n by
pro
vidi
ng fo
r eac
h: th
e na
me
of th
e pr
ogra
mm
e, c
onta
ct p
erso
n(s)
, and
onl
ine
desc
riptio
n.a.
If a
pplic
able
, is
part
icip
atio
n in
nat
iona
l EQ
A pr
ogra
mm
e(s)
man
dato
ry fo
r pub
lic la
bora
torie
s?b.
If a
pplic
able
, is
part
icip
atio
n in
nat
iona
l EQ
A pr
ogra
mm
e(s)
man
dato
ry fo
r priv
ate
labo
rato
ries?
DE
TE
CT

INTERNATIONAL HEALTH REGULATIONS (2005)
55 - Joint External Evaluation Tool - Second edition
c. P
erce
ntag
e of
pub
lic la
bora
torie
s pa
rtic
ipat
ing
in n
atio
nal E
QA
prog
ram
me(
s)?
d. P
erce
ntag
e of
priv
ate
labo
rato
ries
part
icip
atin
g in
nat
iona
l EQ
A pr
ogra
mm
e(s)
?e.
Are
cor
rect
ive
actio
ns o
rgan
ized
whe
n th
e as
sess
men
t res
ult i
s po
or?
Doc
umen
tatio
n or
evi
denc
e fo
r lev
el o
f cap
abili
tyl
Nat
iona
l lab
orat
ory
stra
tegi
c pl
an d
efini
ng ti
ered
labo
rato
ry n
etw
ork
l
Nat
iona
l lab
orat
ory
polic
yl
Doc
umen
ted
list o
f top
10
prio
rity
dise
ases
and
thre
e co
re s
yndr
omes
for t
arge
ted
impr
ovem
ent o
f pre
vent
ion,
det
ectio
n an
d re
spon
sel
Cert
ifica
tes
of a
ccre
dita
tion
for n
atio
nal l
abor
ator
ies
and/
or E
QA
resu
lts w
ithin
the
past
six
mon
ths
for c
ore
test
sl
Doc
umen
ted
spec
imen
refe
rral
rout
es fo
r det
ectio
n/co
nfirm
atio
n of
top
10 p
riorit
y di
seas
esl
Plan
for t
rans
port
ing
spec
imen
s sa
fely
thro
ugho
ut th
e co
untr
yl
All O
IE re
leva
nt to
ols
and
stan
dard
s (M
anua
l) sh
ould
be
cite
d
Refe
renc
es:
l
Inte
rnat
iona
l Hea
lth R
egul
atio
ns: W
hat g
ets
mea
sure
d ge
ts d
one
(incl
udes
list
ing
of th
e 10
cor
e te
sts)
. Cen
ters
for D
isea
se C
ontr
ol a
nd P
reve
ntio
n [w
ebsi
te]
(htt
p://
ww
wnc
.cdc
.gov
/eid
/art
icle
/18/
7/12
-048
7-t2
, acc
esse
d 23
Nov
embe
r 201
7).
l
Labo
rato
ry a
sses
smen
t too
l. W
orld
Hea
lth O
rgan
izat
ion
[web
site
] (W
HO
/HSE
/GCR
/LYO
/201
2.2,
htt
p://
ww
w.w
ho.in
t/ih
r/pu
blic
atio
ns/l
abor
ator
y_to
ol/e
n/,
acce
ssed
23
Nov
embe
r 201
7).
l
All O
IE r
elev
ant
tool
s an
d st
anda
rds.
Wor
ld O
rgan
isat
ion
for
Anim
al H
ealth
[web
site
] (ht
tp:/
/ww
w.o
ie.in
t/en
/sup
port
-to-
oie-
mem
bers
/pvs
-eva
luat
ions
/oi
e-pv
s-to
ol/,
acce
ssed
23
Dec
embe
r 201
7).
DE
TE
CT

INTERNATIONAL HEALTH REGULATIONS (2005)
56 - Joint External Evaluation Tool - Second edition
SURV
EILL
ANCE
Targ
et: (
1) S
tren
gthe
ned
indi
cato
r-ba
sed
and
even
t-ba
sed
surv
eilla
nce
syst
ems
that
are
abl
e to
det
ect e
vent
s of
sig
nific
ance
for p
ublic
hea
lth a
nd h
ealth
sec
urity
; (2
) im
prov
ed c
omm
unic
atio
n an
d co
llabo
ratio
n ac
ross
sec
tors
and
bet
wee
n su
bnat
iona
l (lo
cal a
nd in
term
edia
te),
natio
nal a
nd in
tern
atio
nal l
evel
s of
aut
horit
y re
gard
ing
surv
eilla
nce
of e
vent
s of
pub
lic h
ealth
sig
nific
ance
; and
(3) i
mpr
oved
nat
iona
l and
inte
rmed
iate
leve
l reg
iona
l cap
acity
to a
naly
se a
nd li
nk d
ata
from
an
d be
twee
n, s
tren
gthe
ned
early
-war
ning
sur
veill
ance
, inc
ludi
ng in
tero
pera
ble1 ,
inte
rcon
nect
ed e
lect
roni
c to
ols.
Thi
s w
ould
inco
rpor
ate
epid
emio
logi
cal,
clin
ical
, la
bora
tory
, env
ironm
enta
l tes
ting,
pro
duct
saf
ety
and
qual
ity, a
nd b
ioin
form
atic
s da
ta; a
nd a
dvan
cem
ent i
n fu
lfilli
ng th
e co
re c
apac
ity re
quire
men
ts fo
r sur
veill
ance
in
acc
orda
nce
with
the
IHR
and
OIE
gui
delin
es.
As m
easu
red
by: (
1) S
urve
illan
ce2
for
at le
ast
thre
e co
re s
yndr
omes
3 in
dica
tive
of p
oten
tial p
ublic
hea
lth e
mer
genc
ies
cond
ucte
d ac
cord
ing
to in
tern
atio
nal
stan
dard
s. (2
) Reg
ular
ana
lysi
s an
d re
port
ing
of s
urve
illan
ce d
ata.
Desi
red
impa
ct: (
1) A
func
tioni
ng p
ublic
hea
lth s
urve
illan
ce s
yste
m4 c
apab
le o
f ide
ntify
ing
pote
ntia
l eve
nts
of c
once
rn fo
r pub
lic h
ealth
and
hea
lth s
ecur
ity5 .
(2)
Enha
nced
nat
iona
l and
inte
rmed
iate
leve
l reg
iona
l cap
acity
to
anal
yse
and
link
data
from
and
bet
wee
n th
e di
ffere
nt le
vels
of
the
stre
ngth
ened
ear
ly-w
arni
ng
surv
eilla
nce
syst
em6 .
1 -
Inte
rope
rabl
e, d
escr
ibes
the
exte
nt to
whi
ch s
yste
ms
and
devi
ces
can
exch
ange
dat
a, a
nd in
terp
ret t
hat s
hare
d da
ta. F
or tw
o sy
stem
s to
be
inte
rope
rabl
e, th
ey m
ust b
e ab
le to
exc
hang
e da
ta a
nd s
ubse
quen
tly p
rese
nt th
at d
ata
in a
man
ner t
hat c
an b
e un
ders
tood
by
the
user
(defi
nitio
n by
Hea
lthca
re In
form
atio
n an
d M
anag
emen
t Sys
tem
s So
ciet
y).
2 - S
urve
illan
ce, m
eans
the
syst
emat
ic o
ngoi
ng c
olle
ctio
n, c
olla
tion
and
anal
ysis
of d
ata
for p
ublic
hea
lth p
urpo
ses
and
the
timel
y di
ssem
inat
ion
of p
ublic
hea
lth in
form
atio
n fo
r ass
essm
ent a
nd p
ublic
hea
lth re
spon
se a
s ne
cess
ary.
3 -
Inte
rnat
iona
lly re
cogn
ized
sta
ndar
ds fo
r syn
drom
ic s
urve
illan
ce a
re a
vaila
ble
for t
he fo
llow
ing
five
synd
rom
es: (
i) se
vere
acu
te re
spira
tory
syn
drom
e, (i
i) ac
ute
flacc
id p
aral
ysis
, (iii
) acu
te h
aem
orrh
agic
feve
r, (iv
) acu
te w
ater
y di
arrh
oea
with
deh
ydra
tion,
and
(v) a
cute
jaun
dice
syn
drom
e. T
hree
cor
e sy
ndro
mes
are
cho
sen
depe
ndin
g on
nat
iona
l dis
ease
con
trol
prio
ritie
s. T
he s
urve
illan
ce s
yste
m s
houl
d in
clud
e ep
idem
iolo
gica
l dat
a an
d la
bora
tory
find
ings
, w
hich
sho
uld
be a
naly
sed
by tr
aine
d ep
idem
iolo
gist
s.4
- St
rong
sur
veill
ance
will
sup
port
the
timel
y re
cogn
ition
of t
he e
mer
genc
e of
rela
tivel
y ra
re o
r pre
viou
sly
unde
scrib
ed p
atho
gens
in s
peci
fic c
ount
ries.
5 -
Each
cou
ntry
has
to d
efine
a “p
oten
tial r
isk
to p
ublic
hea
lth”,
perf
orm
risk
map
ping
and
iden
tify
prio
rity
dise
ases
.6
- Co
untr
ies
will
sup
port
the
use
of in
tero
pera
ble,
inte
rcon
nect
ed s
yste
ms
capa
ble
of li
nkin
g an
d in
tegr
atin
g m
ultis
ecto
ral s
urve
illan
ce d
ata
and
usin
g re
sulti
ng in
form
atio
n to
enh
ance
the
capa
city
to q
uick
ly d
etec
t and
resp
ond
to
deve
lopi
ng b
iolo
gica
l thr
eats
. Fou
ndat
iona
l cap
acity
is n
eces
sary
for b
oth
IBS
and
EBS,
in o
rder
to s
uppo
rt p
reve
ntio
n an
d co
ntro
l act
iviti
es a
nd in
terv
entio
n ta
rget
ing
for b
oth
esta
blis
hed
infe
ctio
us d
isea
ses
and
new
and
em
ergi
ng
publ
ic h
ealth
thre
ats.
DE
TE
CT

INTERNATIONAL HEALTH REGULATIONS (2005)
57 - Joint External Evaluation Tool - Second edition
Scor
eIn
dica
tors
: Sur
veill
ance
D.
2.1
Surv
eilla
nce
syst
ems7,
8,9
D.2.
2 U
se o
f ele
ctro
nic
tool
sD.
2.3
Anal
ysis
of s
urve
illan
ce d
ata
No
capa
city
- 1
The
coun
try
has
no s
urve
illan
ce s
yste
m f
or d
i-se
ases
/syn
drom
es/e
vent
sTh
ere
is n
o el
ectr
onic
tool
to c
olle
ct, r
epor
t or a
na-
lyse
sur
veill
ance
dat
aTh
ere
is n
o ca
paci
ty to
ana
lyse
repo
rted
dat
a
Lim
ited
ca
paci
ty -
2
Surv
eilla
nce
syst
em is
in p
lace
rely
ing
eith
er o
n IB
S or
EBS
or b
oth10
(inc
ludi
ng s
yndr
omic
sur
veill
ance
) an
d su
ppor
ted
by S
OPs
and
/or t
echn
ical
gui
delin
es
for
surv
eilla
nce.
The
re i
s no
sys
tem
atic
11 i
mm
e-di
ate
repo
rtin
g an
d w
eekl
y re
port
ing
of e
vent
s an
d/or
dat
a
Ad h
oc e
lect
roni
c to
ols
have
bee
n de
velo
ped
to fa
-ci
litat
e th
e co
llect
ion,
rep
ortin
g or
the
ana
lysi
s of
su
rvei
llanc
e da
ta a
nd e
vent
s (e
.g.
Exce
l sp
read
-sh
eets
), or
cou
ntry
is
deve
lopi
ng a
n in
tegr
ated
el
ectr
onic
rea
l-tim
e re
port
ing
syst
em f
or p
ublic
he
alth
sur
veill
ance
Spor
adic
repo
rts
are
anal
ysed
on
som
e pr
iorit
y di
-se
ases
or u
nusu
al e
vent
s ar
e pr
oduc
ed, o
ften
with
de
lay
Deve
lope
d ca
paci
ty -
3
Both
IBS
and
EBS
are
in p
lace
at
the
cent
ral a
nd
inte
rmed
iate
lev
els,
and
rec
eive
im
med
iate
and
w
eekl
y re
port
ing
from
the
loca
l lev
el o
n an
ad
hoc
basi
s.
Info
rmat
ion
tech
nolo
gy to
ols
avai
labl
e at
the
natio
-na
l lev
el th
at p
erm
it m
anag
emen
t of a
sur
veill
ance
da
taba
se a
nd a
n ev
ent m
anag
emen
t sys
tem
Regu
lar
annu
al o
r m
onth
ly r
epor
ting
of d
ata
with
so
me
dela
y an
d m
inim
um a
naly
sis
of d
ata
is d
one
by a
n ad
hoc
team
Dem
onst
rate
d ca
paci
ty -
4
Both
IBS
and
EBS
are
in p
lace
at a
ll th
e le
vels
(nat
io-
nal,
inte
rmed
iate
and
loca
l) an
d re
ceiv
e im
med
iate
an
d w
eekl
y re
port
s fr
om a
ll he
alth
faci
litie
s12 o
f the
co
untr
y an
d so
me
mec
hani
sm13
of
cros
s-bo
rder
su
rvei
llanc
e is
in p
lace
Coun
try
has
in p
lace
a s
ecur
e in
tegr
ated
ele
ctro
nic
surv
eilla
nce
tool
for p
ublic
hea
lth s
urve
illan
ce a
t all
leve
ls o
f the
hea
lth s
yste
mTh
is to
ol p
erm
its th
e an
alys
is o
f dat
a an
d th
e au
to-
mat
ic p
rodu
ctio
n of
epi
dem
iolo
gica
l bul
letin
s
Mor
e of
ten
than
wee
kly
repo
rtin
g w
ith a
naly
sis
Asse
ssm
ent o
f ris
k is
don
e by
an
expe
rtRe
gula
r epi
dem
iolo
gica
l bul
letin
s ar
e di
ssem
inat
ed
Sust
aina
ble
capa
city
- 5
The
perf
orm
ance
of t
he s
urve
illan
ce s
yste
m is
re-
gula
rly e
valu
ated
and
upd
ated
at
all l
evel
s in
the
co
untr
y an
d ha
s th
e ca
paci
ty t
o su
ppor
t ot
her
coun
trie
s in
dev
elop
ing
surv
eilla
nce
syst
ems
and/
or c
ontr
ibut
es t
o re
gion
al o
r in
tern
atio
nal s
urve
il-la
nce
netw
orks
14
The
surv
eilla
nce
syst
em i
s eq
uipp
ed w
ith a
ful
-ly
sec
ure
inte
rope
rabl
e, e
lect
roni
c to
ol f
or p
ublic
he
alth
sur
veill
ance
tha
t is
: con
nect
ed t
o ot
her
re-
leva
nt e
lect
roni
c to
ols
(e.g
. ani
mal
hea
lth),
and
can
easi
ly s
hare
dat
a w
ith o
ther
ele
ctro
nic
tool
s us
ed
eith
er a
t reg
iona
l or i
nter
natio
nal l
evel
s
Mor
e fr
eque
ntly
than
wee
kly
syst
emat
ic re
port
ing
Ded
icat
ed te
am in
pla
ce fo
r dat
a an
alys
is, r
isk
as-
sess
men
t and
repo
rtin
g
7 -
The
indi
cato
r ref
ers
to s
urve
illan
ce c
apac
ity fo
r the
cou
ntry
.8
- Th
e su
rvei
llanc
e sy
stem
sho
uld
incl
ude:
• a
bilit
y to
con
duct
sur
veill
ance
for a
t lea
st th
ree
core
syn
drom
es in
dica
tive
of a
pub
lic h
ealth
em
erge
ncy;
• abi
lity
to p
rovi
de re
port
s an
d da
ta to
hig
h-le
vel p
ublic
hea
lth d
ecis
ion-
mak
ers
in th
e co
untr
y, an
d fe
edba
ck to
low
er le
vels
impl
emen
ting
the
cont
rol p
rogr
amm
es; a
nd• l
inka
ges
to la
bora
tory
and
oth
er in
form
atio
n sy
stem
s to
pro
vide
a c
ompl
ete
surv
eilla
nce
repr
esen
tatio
n.9
- Th
ere
is c
ritic
al c
ompe
tenc
y in
the
PVS
tool
CC
II-5:
Epi
dem
iolo
gica
l sur
veill
ance
and
ear
ly d
etec
tion.
10-
EBS
is d
efine
d as
the
orga
nize
d co
llect
ion,
mon
itorin
g, a
sses
smen
t and
inte
rpre
tatio
n of
mai
nly
unst
ruct
ured
ad
hoc
info
rmat
ion
rega
rdin
g he
alth
eve
nts
or ri
sks,
whi
ch m
ay re
pres
ent a
n ac
ute
risk
to h
uman
hea
lth. E
BS is
a
func
tiona
l com
pone
nt o
f ear
ly w
arni
ng a
nd re
spon
se.
11 -
Met
hodi
cal i
n pr
oced
ure
or p
lan
(mar
ked
by th
orou
ghne
ss a
nd re
gula
rity
of th
e ef
fort
).12
- P
ublic
and
priv
ate
heal
th fa
cilit
ies
at a
ll le
vels
of t
he p
ublic
hea
lth s
yste
m.
13 -
Mec
hani
sm fo
r cro
ss-b
orde
r sur
veill
ance
– a
gree
d cr
oss-
bord
er s
urve
illan
ce s
yste
m a
t poi
nts
of e
ntry
or s
ome
othe
r mec
hani
sm o
f reg
ular
ly s
harin
g da
ta a
nd in
form
atio
n be
twee
n ne
ighb
ourin
g co
untr
ies
whe
re a
pplic
able
.14
- A
t the
nat
iona
l lev
el to
iden
tify
publ
ic h
ealth
eve
nts,
use
dis
ease
thre
shol
ds o
f IBS
or i
mpl
emen
t a s
peci
fic tr
iage
pro
cess
to c
heck
if th
e ev
ent i
s un
usua
l or u
nexp
ecte
d. R
efer
to W
HO
gui
danc
e fo
r the
use
of A
nnex
2 o
f the
In
tern
atio
nal H
ealth
Reg
ulat
ions
(200
5) fo
r Dec
isio
n in
stru
men
t for
the
asse
ssm
ent a
nd n
otifi
catio
n of
eve
nts
that
may
con
stitu
te a
pub
lic h
ealth
em
erge
ncy
of in
tern
atio
nal c
once
rn (h
ttp:
//w
ww
.who
.int/
ihr/
publ
icat
ions
/ann
ex_2
_gu
idan
ce/e
n/, a
cces
sed
24 N
ovem
ber 2
017)
.
DE
TE
CT

INTERNATIONAL HEALTH REGULATIONS (2005)
58 - Joint External Evaluation Tool - Second edition
Cont
extu
al q
uest
ion:
1.
Doe
s th
e co
untr
y ha
ve a
list
of n
otifi
able
prio
rity
dise
ases
?2.
Is
the
surv
eilla
nce
of in
fect
ious
dis
ease
s lin
ked
in o
ne n
atio
nal s
urve
illan
ce s
yste
m v
ersu
s a
sepa
rate
sys
tem
for d
iffer
ent d
isea
ses?
3.
How
doe
s da
ta fr
om th
e la
bora
torie
s fe
ed in
to th
e su
rvei
llanc
e sy
stem
?4.
H
ow d
oes
the
coun
try
utili
ze e
lect
roni
c to
ols
for n
otifi
able
dis
ease
s fo
r hum
an h
ealth
and
ani
mal
hea
lth?
5.
If no
ele
ctro
nic
syst
ems
(tool
s) e
xist
in th
e co
untr
y, ar
e th
ere
plan
s to
impl
emen
t in
the
futu
re?
6.
Are
data
from
thes
e sy
stem
s sh
ared
bet
wee
n se
ctor
s, o
r ind
epen
dent
?
Tech
nica
l que
stio
ns:
D.2.
1 Su
rvei
llanc
e sy
stem
s1.
D
escr
ibe
in-c
ount
ry E
BS.
a. D
escr
ibe
sour
ces
utili
zed
by E
BS a
nd m
echa
nism
s of
col
lect
ing
info
rmat
ion.
b. D
oes
EBS
exis
t at a
ny s
ubna
tiona
l (in
term
edia
te o
r loc
al) l
evel
?2.
D
escr
ibe
IBS
and
mec
hani
sms
of c
olle
ctin
g da
ta.
a. L
ist o
f prio
rity
dise
ases
, con
ditio
ns, s
yndr
omes
and
cas
e de
finiti
ons.
b. D
oes
the
coun
try
have
com
plet
enes
s an
d tim
elin
ess
of re
port
ing
from
at l
east
80%
of a
ll re
port
ing
units
? 3.
D
escr
ibe
data
val
idat
ion
and
qual
ity a
ssur
ance
sys
tem
s/ef
fort
s.4.
D
escr
ibe
synd
rom
ic s
urve
illan
ce s
yste
ms
that
are
in p
lace
with
in th
e co
untr
y:a.
Des
crib
e va
rious
syn
drom
es a
nd p
atho
gens
that
are
det
ecte
d an
d re
port
ed.
b. D
escr
ibe
how
man
y si
tes
part
icip
ate
in e
ach
surv
eilla
nce
syst
em.
c. D
escr
ibe
how
dat
a ar
e va
lidat
ed.
d. D
escr
ibe
any
synd
rom
ic s
urve
illan
ce s
yste
m th
at u
tiliz
es e
lect
roni
c re
port
ing.
e. D
escr
ibe
repo
rts
that
are
pro
duce
d by
eac
h su
rvei
llanc
e sy
stem
and
how
they
are
use
d by
pub
lic h
ealth
dec
isio
n m
aker
s. A
re th
ese
repo
rts
shar
ed w
ith
any
othe
r min
istr
ies
with
in th
e co
untr
y?f.
Des
crib
e an
y lin
kage
s th
at e
xist
bet
wee
n sy
stem
s at
the
natio
nal l
evel
.
D.2.
2 U
se o
f ele
ctro
nic
tool
s1.
H
ow a
re p
ublic
hea
lth s
taff
trai
ned
on d
isea
se s
urve
illan
ce s
yste
ms?
2.
How
are
clin
ical
sta
ff tr
aine
d to
repo
rt o
n no
tifiab
le d
isea
ses?
3.
Do
publ
ic h
ealth
sta
ff at
nat
iona
l/int
erm
edia
te/r
egio
nal l
evel
s ha
ve th
e sk
ills
to a
naly
se s
urve
illan
ce d
ata
to c
reat
e in
form
atio
n tr
igge
ring/
supp
ortin
g ac
tion?
4.
How
doe
s th
e co
untr
y ut
ilize
ele
ctro
nic
repo
rtin
g sy
stem
s fo
r not
ifiab
le d
isea
ses
for h
uman
hea
lth a
nd a
nim
al h
ealth
? 5.
Ar
e th
ese
syst
ems
shar
ed b
etw
een
sect
ors,
or a
re th
ey in
depe
nden
t?6.
If
no e
lect
roni
c re
port
ing
syst
ems
exis
t in
the
coun
try,
are
ther
e pl
ans
to im
plem
ent e
lect
roni
c re
port
ing
in th
e fu
ture
?
DE
TE
CT

INTERNATIONAL HEALTH REGULATIONS (2005)
59 - Joint External Evaluation Tool - Second edition
7.
Des
crib
e th
e re
port
ing
and
feed
back
to in
term
edia
te/r
egio
nal a
nd lo
cal l
evel
s.8.
D
escr
ibe
repo
rtin
g to
nat
iona
l and
inte
rmed
iate
/reg
iona
l lev
el s
take
hold
ers.
9.
Des
crib
e pu
blic
repo
rtin
g.
D.2.
3 An
alys
is o
f sur
veill
ance
dat
a1.
D
escr
ibe
how
sur
veill
ance
dat
a ar
e an
alys
ed.
2.
Are
ther
e tr
aine
d he
alth
car
e w
orke
rs to
ana
lyse
at n
atio
nal a
nd in
term
edia
te le
vels
?3.
Is
ther
e a
mec
hani
sm in
pla
ce to
link
epi
dem
iolo
gica
l and
labo
rato
ry d
ata?
4.
Is th
ere
a ca
paci
ty to
con
duct
risk
ass
essm
ent a
t nat
iona
l, in
term
edia
te a
nd/o
r loc
al le
vels
?5.
H
ow is
the
risk
asse
ssm
ent i
nfor
mat
ion
diss
emin
ated
and
to w
hom
?6.
Is
ther
e a
cent
rally
loca
ted
mec
hani
sm fo
r int
egra
ting
data
from
clin
ical
cas
e re
port
ing
and
data
from
clin
ical
or r
efer
ence
mic
robi
olog
ical
labo
rato
ries?
7.
How
ofte
n ar
e re
port
s pu
blis
hed
and
diss
emin
ated
? a.
Is
it pu
blis
hed
syst
emat
ical
ly e
very
wee
k or
mon
thly
or a
nnua
lly?
b. W
ho d
oes
the
anal
ysis
and
at w
hat l
evel
?c.
Doe
s th
e co
untr
y pr
oduc
e an
d pu
blis
h an
epi
dem
iolo
gica
l bul
letin
? If
yes,
wha
t is
the
freq
uenc
y?
Doc
umen
tatio
n or
evi
denc
e fo
r lev
el o
f cap
abili
ty:
l
Sam
ples
of s
urve
illan
ce re
port
s us
ed b
y pu
blic
hea
lth d
ecis
ion-
mak
ers
in th
e co
untr
yl
List
ing
of c
ore
synd
rom
es in
dica
tive
of a
pub
lic h
ealth
em
erge
ncy
l
Plan
s fo
r enh
anci
ng s
yndr
omic
sur
veill
ance
l
Plan
s fo
r dev
elop
ing
or e
nhan
cing
EBS
l
OIE
repo
rts
(Wor
ld A
nim
al H
ealth
Info
rmat
ion
Syst
em –
WAH
IS)
l
Surv
eilla
nce
data
base
s an
d fo
rms
Refe
renc
es:
l
Early
det
ectio
n, a
sses
smen
t an
d re
spon
se t
o ac
ute
publ
ic h
ealth
eve
nts:
Impl
emen
tatio
n of
ear
ly w
arni
ng a
nd r
espo
nse
with
a f
ocus
on
even
t-ba
sed
surv
eilla
nce.
Inte
rim v
ersi
on. G
enev
a: W
orld
Hea
lth O
rgan
izat
ion;
201
4 (h
ttp:
//ap
ps.w
ho.in
t/iri
s/bi
tstr
eam
/106
65/1
1266
7/1/
WH
O_H
SE_G
CR_L
YO_2
014.
4_en
g.pd
f?ua
=1, a
cces
sed
23 N
ovem
ber 2
017)
.l
Inte
rnat
iona
l Hea
lth R
egul
atio
ns (2
005)
. 2nd
editi
on. G
enev
a: W
orld
Hea
lth O
rgan
izat
ion;
2008
(htt
p://
whq
libdo
c.w
ho.in
t/pu
blic
atio
ns/2
008/
9789
2415
8041
0_en
g.pd
f, ac
cess
ed 2
3 N
ovem
ber 2
017;
incl
udes
list
s of
dis
ease
that
hav
e “…
dem
onst
rate
d ab
ility
to c
ause
ser
ious
pub
lic h
ealth
impa
ct“)
.l
Terr
estr
ial a
nim
al h
ealth
cod
e (2
017)
. Vol
ume
1. G
ener
al p
rovi
sion
s. W
orld
Org
anis
atio
n fo
r An
imal
Hea
lth [w
ebsi
te] (
http
://w
ww
.oie
.int/
inte
rnat
iona
l-st
anda
rd-s
ettin
g/te
rres
tria
l-co
de/a
cces
s-on
line/
, acc
esse
d 23
Nov
embe
r 201
7).
l
Man
ual o
f dia
gnos
tic te
sts
and
vacc
ines
for t
erre
stria
l ani
mal
s (2
017)
. Wor
ld O
rgan
isat
ion
for A
nim
al H
ealth
[web
site
] (ht
tp:/
/ww
w.o
ie.in
t/en
/int
erna
tiona
l-st
anda
rd-s
ettin
g/te
rres
tria
l-m
anua
l/ac
cess
-onl
ine/
, acc
esse
d 23
Nov
embe
r 201
7).
DE
TE
CT

INTERNATIONAL HEALTH REGULATIONS (2005)
60 - Joint External Evaluation Tool - Second edition
REPO
RTIN
GTa
rget
: Tim
ely
and
accu
rate
dis
ease
repo
rtin
g ac
cord
ing
to W
HO
requ
irem
ents
and
con
sist
ent r
elay
of i
nfor
mat
ion
to F
AO a
nd O
IE.
As m
easu
red
by: E
stab
lishm
ent
of a
sys
tem
1 to
repo
rt p
oten
tial p
ublic
hea
lth e
vent
s of
inte
rnat
iona
l con
cern
to
WH
O, a
nd t
o m
eet
the
need
s of
oth
er o
ffici
al
repo
rtin
g sy
stem
s, s
uch
as O
IE-W
AHIS
.
Desi
red
impa
ct: T
he N
atio
nal I
HR
Foca
l Poi
nts,
the
OIE
Del
egat
e, a
nd W
AHIS
Nat
iona
l Foc
al P
oint
will
hav
e ac
cess
to a
tool
kit o
f bes
t pra
ctic
es, m
odel
pro
cedu
res,
re
port
ing
tem
plat
es, a
nd t
rain
ing
mat
eria
ls t
o fa
cilit
ate
rapi
d (w
ithin
24
hour
s) n
otifi
catio
n of
eve
nts
that
may
con
stitu
te a
pot
entia
l pub
lic h
ealth
em
erge
ncy
of in
tern
atio
nal c
once
rn (P
HEI
C) to
WH
O a
nd li
sted
dis
ease
s to
OIE
, as
wel
l as
be a
ble
to re
spon
d ra
pidl
y (w
ithin
24/
48 h
ours
) to
com
mun
icat
ions
from
thes
e or
gani
zatio
ns.
1 -
Exis
tenc
e of
pro
toco
ls, p
roce
sses
, reg
ulat
ions
and
/or l
egis
latio
n go
vern
ing
repo
rtin
g an
d pr
oces
ses
for m
ultis
ecto
ral c
oord
inat
ion
in re
spon
se to
a p
oten
tial P
HEI
C to
WH
O a
nd to
the
OIE
for r
elev
ant z
oono
tic d
isea
ses.
DE
TE
CT

INTERNATIONAL HEALTH REGULATIONS (2005)
61 - Joint External Evaluation Tool - Second edition
Scor
eIn
dica
tors
: Rep
ortin
g2,3,
4
D.3.
1 Sy
stem
for e
ffici
ent r
epor
ting
to F
AO, O
IE a
nd W
HO
5 D.
3.2
Repo
rtin
g ne
twor
k an
d pr
otoc
ols
in c
ount
ry
No
capa
city
- 1
No
Nat
iona
l IH
R Fo
cal P
oint
, OIE
Del
egat
e an
d/or
WAH
IS N
atio
nal F
ocal
Poi
nt
has
been
iden
tified
and
/or
the
iden
tified
foca
l poi
nt/d
eleg
ate
does
not
hav
e ac
cess
to
the
lear
ning
pac
kage
and
bes
t pr
actic
es a
s pr
ovid
ed b
y FA
O, O
IE
and
WH
O
Coun
try
does
not
hav
e pr
otoc
ols
or p
roce
sses
for
rep
ortin
g to
FAO
, OIE
or
WH
O; a
nd d
oes
not h
ave
plan
s to
est
ablis
h pl
ans
and
prot
ocol
s fo
r rep
ortin
g w
ithin
the
next
yea
r
Lim
ited
ca
paci
ty -
2
Coun
try
has
iden
tified
the
Nat
iona
l IH
R Fo
cal P
oint
, the
OIE
Del
egat
e an
d W
A-H
IS N
atio
nal F
ocal
Poi
nt; a
nd th
e fo
cal p
oint
/del
egat
e ha
s ac
cess
to th
e le
ar-
ning
pac
kage
and
bes
t pra
ctic
es a
s pr
ovid
ed b
y FA
O, O
IE a
nd W
HO
Coun
try
is in
the
proc
ess
of d
evel
opin
g an
d es
tabl
ishi
ng p
roto
cols
, pro
cess
es,
regu
latio
ns, a
nd/o
r le
gisl
atio
n go
vern
ing
repo
rtin
g to
sta
rt im
plem
enta
tion
with
in a
yea
r
Deve
lope
d ca
paci
ty -
3
Coun
try
has
dem
onst
rate
d ab
ility
to id
entif
y a
pote
ntia
l PH
EIC
and
file
a re
-po
rt to
WH
O a
nd s
imila
rly to
the
OIE
(acc
ordi
ng to
OIE
pro
cess
es) f
or re
leva
nt
zoon
otic
dis
ease
s, b
ased
on
an e
xerc
ise
or re
al e
vent
Coun
try
has
esta
blis
hed
prot
ocol
s, p
roce
sses
, reg
ulat
ions
and
/or l
egis
latio
n go
vern
ing
repo
rtin
g an
d pr
oces
ses
for m
ultis
ecto
ral c
oord
inat
ion
in re
spon
se
to a
pot
entia
l PH
EIC
to W
HO
and
to th
e O
IE fo
r rel
evan
t zoo
notic
dis
ease
s
Dem
onst
rate
d ca
paci
ty -
4
Coun
try
has
dem
onst
rate
d ab
ility
to id
entif
y a
pote
ntia
l PH
EIC
and
file
a re
port
to
WH
O w
ithin
24
hour
s an
d si
mila
rly to
the
OIE
(acc
ordi
ng to
OIE
pro
cess
es)
for r
elev
ant z
oono
tic d
isea
ses,
bas
ed o
n an
exe
rcis
e or
real
eve
nt
Coun
try
dem
onst
rate
s tim
ely
repo
rtin
g of
a p
oten
tial P
HEI
C to
WH
O a
nd to
the
OIE
for r
elev
ant z
oono
tic d
isea
ses
in a
lignm
ent w
ith n
atio
nal a
nd in
tern
atio
nal
stan
dard
s in
sel
ecte
d in
term
edia
te le
vels
(dis
tric
ts o
r re
gion
s), b
ased
on
an
exer
cise
or r
eal e
vent
Sust
aina
ble
capa
city
- 5
Coun
try
has
dem
onst
rate
d ab
ility
to id
entif
y a
pote
ntia
l PH
EIC
and
file
a re
-po
rt w
ithin
24
hour
s, a
nd s
imila
rly t
o th
e O
IE (
acco
rdin
g to
OIE
pro
cess
es)
for
rele
vant
zoo
notic
dis
ease
s, a
nd h
as a
mul
tisec
tora
l pro
cess
in p
lace
for
asse
ssin
g po
tent
ial e
vent
s fo
r rep
ortin
g
Coun
try
dem
onst
rate
s tim
ely
repo
rtin
g of
a p
oten
tial P
HEI
C to
the
WH
O fr
om
dist
rict t
o na
tiona
l and
inte
rnat
iona
l lev
els
and
to th
e O
IE fo
r rel
evan
t zoo
notic
di
seas
es, b
ased
on
an e
xerc
ise
or re
al e
vent
Coun
try
has
a su
stai
nabl
e pr
oces
s fo
r m
aint
aini
ng a
nd im
prov
ing
repo
rtin
g an
d co
mm
unic
atio
n ca
pabi
litie
s, a
nd c
omm
unic
atio
n m
echa
nism
s ar
e ba
cked
by
est
ablis
hed
docu
men
tatio
n (s
uch
as p
roto
cols
, reg
ulat
ions
, leg
isla
tion)
2 -A
ll qu
estio
ns s
houl
d be
ans
wer
ed to
refle
ct h
uman
and
ani
mal
dis
ease
s.3
- N
eed
to e
nsur
e th
at a
nim
al h
ealth
offi
cial
s (F
AO a
nd O
IE) s
houl
d be
pre
sent
for t
his
tech
nica
l are
a. T
his
is d
irect
ly re
late
d to
pro
toco
ls fo
r rep
ortin
g m
echa
nism
s ac
ross
age
ncie
s in
bot
h in
dica
tors
. 4
- In
dica
tor D
.3.1
is re
late
d to
whe
ther
the
Nat
iona
l IH
R Fo
cal P
oint
can
repo
rt (a
n ef
ficie
nt s
yste
m e
xist
s); I
ndic
ator
D.3
.2 is
the
deta
iled
stru
ctur
e an
d pr
oced
ures
beh
ind
the
Nat
iona
l IH
R Fo
cal P
oint
and
how
the
Nat
iona
l IH
R Fo
cal
Poin
t gat
hers
info
rmat
ion
and
verifi
es a
s pa
rt o
f the
repo
rtin
g pr
oces
s.5
- N
ot a
ll co
untr
ies
will
hav
e re
port
ed a
pot
entia
l PH
EIC
to th
e W
HO
or r
epor
ted
to th
e O
IE fo
r rel
evan
t zoo
notic
dis
ease
s.
Cont
extu
al q
uest
ions
: N/A
Tech
nica
l que
stio
ns:
D.3.
1 Sy
stem
for e
ffici
ent r
epor
ting
to F
AO, O
IE a
nd W
HO
1.
Whi
ch m
inis
try
or o
ffice
with
in th
e co
untr
y ha
s be
en id
entifi
ed a
s th
e N
atio
nal I
HR
Foca
l Poi
nt a
nd in
form
ed to
the
WH
O?
a. I
s th
e N
atio
nal I
HR
Foca
l Poi
nt a
ble
to c
over
all
inci
dent
s (b
iolo
gica
l, ch
emic
al, r
adia
tion)
und
er IH
R an
d cu
rren
tly o
pera
tiona
l?
b. I
s th
ere
an o
pera
tiona
l OIE
Con
tact
Poi
nt?
c. A
re fo
od s
afet
y is
sues
due
to m
icro
biol
ogic
al o
rigin
repo
rted
thro
ugh
the
Nat
iona
l IH
R Fo
cal P
oint
and
to th
e O
IE?
DE
TE
CT

INTERNATIONAL HEALTH REGULATIONS (2005)
62 - Joint External Evaluation Tool - Second edition
d. I
s th
ere
a m
echa
nism
to e
nsur
e th
at th
e N
atio
nal I
HR
Foca
l Poi
nt a
nd O
IE C
onta
ct P
oint
s ex
chan
ge in
form
atio
n w
hen
need
ed (e
.g. f
or z
oono
tic d
isea
ses)
? e.
Des
crib
e th
e tr
aini
ng th
at th
e N
atio
nal I
HR
Foca
l Poi
nt/O
IE C
onta
ct P
oint
resp
onsi
ble
pers
on(s
) hav
e un
derg
one
for t
his
spec
ific
role
.f.
List
the
min
istri
es (s
uch
as h
ealth
, agr
icul
ture
) tha
t the
se fo
cal p
oint
s re
pres
ent f
or th
e W
HO/
OIE
and
whi
ch o
ne re
ports
thro
ugh
the
Nat
iona
l IH
R Fo
cal p
oint
. 2.
W
hat a
re th
e m
echa
nism
s fo
r pub
lic h
ealth
, ani
mal
hea
lth a
nd s
ecur
ity a
utho
ritie
s to
mak
e de
cisi
ons
on re
port
ing?
3.
Des
crib
e if
the
coun
try
has
mul
tilat
eral
regi
onal
(int
erna
tiona
l) or
bila
tera
l nei
ghbo
urin
g co
untr
y re
port
ing
requ
irem
ents
. If y
es, s
peci
fy.
4.
Is th
ere
anyt
hing
that
lim
its th
e pe
rfor
man
ce o
f the
Nat
iona
l IH
R Fo
cal P
oint
? (T
his
may
incl
ude
qual
ity a
nd ti
mel
ines
s of
info
rmat
ion
rece
ived
, and
obs
tacl
es
caus
ed b
y co
ordi
natio
n w
ith o
ther
leve
ls a
nd s
ecto
rs.)
a. D
oes
the
Nat
iona
l IH
R Fo
cal P
oint
use
info
rmal
con
sulta
tion
mec
hani
sms
with
WH
O u
nder
Art
icle
8 o
f the
IHR?
b. D
oes
the
Nat
iona
l IH
R Fo
cal P
oint
use
bila
tera
l exc
hang
e m
echa
nism
s w
ith o
ther
Nat
iona
l IH
R Fo
cal P
oint
s?
D.3.
2 Re
port
ing
netw
ork
and
prot
ocol
s in
cou
ntry
1.
Des
crib
e th
e m
ost r
ecen
t exe
rcis
e (o
r eve
nt) t
hat t
este
d th
e co
untr
y’s
syst
ems
to id
entif
y an
d re
port
on
a po
tent
ial P
HEI
C.
a. H
ow w
as th
e he
alth
eve
nt id
entifi
ed?
Wha
t sur
veill
ance
sys
tem
s w
ere
linke
d?b.
How
wer
e pu
blic
hea
lth d
ecis
ion-
mak
ers
and
othe
r lea
ders
hip
cons
ulte
d in
the
deci
sion
-mak
ing
proc
ess?
c. W
hich
min
istr
ies
wer
e en
gage
d in
the
exer
cise
or e
vent
(hea
lth, d
efen
ce, a
gric
ultu
re)?
d. I
f the
cou
ntry
has
not
yet
exe
rcis
ed P
HEI
C re
port
ing,
iden
tify
if th
ere
are
any
plan
s to
do
so w
ithin
the
next
yea
r.2.
H
as th
e co
untr
y pa
ssed
legi
slat
ion
or o
ther
pol
icie
s re
late
d to
pro
cedu
res
and/
or a
ppro
vals
for r
epor
ting
on a
pot
entia
l PH
EIC
to th
e W
HO
? If
so, d
escr
ibe
the
part
ies
invo
lved
in a
ppro
vals
as
wel
l as
the
maj
or s
teps
in a
ppro
vals
. If p
ossi
ble,
pro
vide
a c
opy
of re
leva
nt le
gisl
atio
n or
pol
icie
s.3.
D
oes
the
coun
try
have
SO
Ps in
pla
ce fo
r app
rovi
ng a
nd re
port
ing
on a
pot
entia
l PH
EIC
to W
HO
?
Doc
umen
tatio
n or
evi
denc
e fo
r lev
el o
f cap
abili
ty:
l
WH
O IH
R An
nex
2l
OIE
Ter
rest
rial A
nim
als
and
Hea
lth C
ode
– S
ectio
n 1
l
IHR
repo
rts
to th
e W
HA
l
Legi
slat
ion,
pro
toco
ls o
r oth
er p
olic
ies
rela
ted
to re
port
ing
to W
HO
and
OIE
l
WAH
IS
Refe
renc
es:
l
Anne
x 2
of th
e In
tern
atio
nal H
ealth
Reg
ulat
ions
(200
5). W
orld
Hea
lth O
rgan
izat
ion
[web
site
] (ht
tp://
ww
w.w
ho.in
t/ih
r/an
nex_
2/en
/, ac
cess
ed 2
3 N
ovem
ber 2
017)
.l
Terr
estr
ial a
nim
al h
ealth
cod
e (2
017)
. Vol
ume
1. G
ener
al p
rovi
sion
s. W
orld
Org
anis
atio
n fo
r Ani
mal
Hea
lth [w
ebsi
te] (
http
://w
ww
.oie
.int/
inte
rnat
iona
l-st
anda
rd-
setti
ng/t
erre
stria
l-co
de/a
cces
s-on
line/
, acc
esse
d 23
Nov
embe
r 201
7).
l
Dec
isio
n N
o. 1
082/
2013
/EU
of
the
Euro
pean
Par
liam
ent
and
of t
he C
ounc
il of
22
Oct
ober
201
3 on
ser
ious
cro
ss-b
orde
r th
reat
s to
hea
lth a
nd r
epea
ling.
D
ecis
ion
No.
211
9/98
/EC,
Offi
cial
Jou
rnal
of
the
Euro
pean
Uni
on 2
013;
293
:1-1
5 (h
ttps:
//ec
.eur
opa.
eu/h
ealth
/site
s/he
alth
/file
s/pr
epar
edne
ss_r
espo
nse/
docs
/dec
isio
n_se
rious
_cro
ssbo
rder
_thr
eats
_221
0201
3_en
, acc
esse
d 23
Nov
embe
r 201
7).
DE
TE
CT

INTERNATIONAL HEALTH REGULATIONS (2005)
63 - Joint External Evaluation Tool - Second edition
HU
MAN
RES
OU
RCES
Targ
et: S
tate
s Pa
rtie
s w
ith s
kille
d an
d co
mpe
tent
hea
lth p
erso
nnel
for s
usta
inab
le a
nd fu
nctio
nal p
ublic
hea
lth s
urve
illan
ce a
nd re
spon
se a
t all
leve
ls o
f the
hea
lth
syst
em a
nd th
e ef
fect
ive
impl
emen
tatio
n of
the
IHR.
Hum
an re
sour
ces
incl
ude
nurs
es a
nd m
idw
ives
, phy
sici
ans,
pub
lic h
ealth
and
env
ironm
enta
l spe
cial
ists
, so
cial
sci
entis
ts, c
omm
unic
atio
n, o
ccup
atio
nal h
ealth
, lab
orat
ory
scie
ntis
ts/t
echn
icia
ns, b
iost
atis
ticia
ns, i
nfor
mat
ion
tech
nolo
gy (I
T) s
peci
alis
ts a
nd b
iom
edic
al
tech
nici
ans.
The
re is
a c
orre
spon
ding
wor
kfor
ce in
the
anim
al s
ecto
r of
vet
erin
aria
ns, a
nim
al h
ealth
pro
fess
iona
ls, p
ara-
vete
rinar
ians
, epi
dem
iolo
gist
s an
d IT
sp
ecia
lists
.Th
e re
com
men
ded
dens
ity o
f doc
tors
, nur
ses
and
mid
wiv
es p
er 1
000
popu
latio
n fo
r ope
ratio
nal r
outin
e se
rvic
es is
4.4
5 pl
us 3
0% s
urge
cap
acity
. The
opt
imal
ta
rget
for s
urve
illan
ce is
one
trai
ned
(fiel
d) e
pide
mio
logi
st (o
r equ
ival
ent)
per
200
000
pop
ulat
ion
who
can
sys
tem
atic
ally
coo
pera
te to
mee
t rel
evan
t IH
R an
d PV
S co
re c
ompe
tenc
ies.
One
trai
ned
epid
emio
logi
st is
nee
ded
per r
apid
resp
onse
team
.
As m
easu
red
by: (
1) A
tra
ined
hea
lth w
orkf
orce
tha
t in
clud
es n
urse
s an
d m
idw
ives
, phy
sici
ans,
pub
lic h
ealth
and
env
ironm
enta
l spe
cial
ists
, soc
ial s
cien
tists
, la
bora
tory
sci
entis
ts/t
echn
icia
ns, b
iost
atis
ticia
ns, I
T sp
ecia
lists
and
bio
med
ical
tech
nici
ans.
(2) E
xist
ence
of a
cor
resp
ondi
ng w
orkf
orce
in th
e an
imal
sec
tor o
f ve
terin
aria
ns, p
ara-
vete
rinar
ians
, ani
mal
hea
lth p
rofe
ssio
nals
, epi
dem
iolo
gist
s, IT
spe
cial
ists
, and
oth
ers.
Desi
red
impa
ct: P
reve
ntio
n, d
etec
tion
and
resp
onse
act
iviti
es (i
nclu
ding
hea
lth p
rom
otio
n, o
ccup
atio
nal h
ealth
saf
ety
and
secu
rity,
and
appr
opria
te c
are
of th
ose
affe
cted
) con
duct
ed e
ffect
ivel
y an
d su
stai
nabl
y by
a fu
lly c
ompe
tent
, coo
rdin
ated
, eva
luat
ed a
nd o
ccup
atio
nally
div
erse
mul
tisec
tora
l wor
kfor
ce.
DE
TE
CT

INTERNATIONAL HEALTH REGULATIONS (2005)
64 - Joint External Evaluation Tool - Second edition
Scor
e5
Indi
cato
rs: H
uman
reso
urce
s (a
nim
al1 a
nd h
uman
hea
lth s
ecto
rs)
D.4.
1 An
up-
to-d
ate
mul
tisec
tora
l w
orkf
orce
str
ateg
y is
in p
lace
2 D.
4.2
Hum
an re
sour
ces
are
avai
labl
e to
eff
ectiv
ely
impl
emen
t IH
R D.
4.3.
In-s
ervi
ce tr
aini
ngs
are
avai
labl
e 3
D.4.
4 FE
TP4 or
oth
er a
pplie
d ep
idem
iolo
gy tr
aini
ng p
rogr
amm
e is
in
pla
ce
No
capa
city
- 1
No
stra
tegy
in p
lace
to d
evel
op a
mul
-tis
ecto
ral h
ealth
wor
kfor
ce
Coun
try
does
not
hav
e ap
prop
riate
hu
man
res
ourc
es5
capa
city
in
rele
-va
nt s
ecto
rs r
equi
red
for
epid
emic
pr
epar
edne
ss a
nd c
ontr
ol
No
cont
inui
ng p
rofe
ssio
nal e
duca
tion
(CPE
) pr
ogra
mm
e th
roug
h in
-ser
vice
tr
aini
ng c
ours
e is
in p
lace
No
FETP
or
ap
plie
d ep
idem
iolo
gy
trai
ning
pro
gram
me
is e
stab
lishe
d
Lim
ited
ca
paci
ty –
2
A st
rate
gy t
o de
velo
p he
alth
car
e w
orkf
orce
6 exi
sts
but d
oes
not i
nclu
de
all
rele
vant
sec
tors
of
publ
ic h
ealth
pr
ofes
sion
s (s
uch
as
epid
emio
lo-
gist
s, s
ocia
l sci
entis
ts, I
T sp
ecia
lists
, ve
terin
aria
ns/l
ives
tock
sp
ecia
lists
an
d co
mm
unity
hea
lth w
orke
rs)
Basi
c da
ta o
n hu
man
res
ourc
es f
or
heal
th a
re a
vaila
ble
Appr
opria
te
hum
an
reso
urce
s ar
e av
aila
ble
at n
atio
nal
leve
l fo
r ep
ide-
mic
pre
pare
dnes
s an
d co
ntro
l
Ad h
oc t
rain
ings
are
ava
ilabl
e fo
r va
rious
pro
fess
ions
/cad
res
thro
ugh
dise
ase
spec
ific
prog
ram
mes
or
ta
rget
ed in
itiat
ives
No
FETP
or a
pplie
d ep
idem
iolo
gy tr
ai-
ning
pro
gram
me
is e
stab
lishe
d w
it-hi
n th
e co
untr
y at
the
nat
iona
l lev
el,
but
staf
f pa
rtic
ipat
e in
a p
rogr
amm
e ho
sted
in a
noth
er c
ount
ry th
roug
h an
ex
istin
g ag
reem
ent (
at a
ny le
vel)
Deve
lope
d ca
paci
ty -
3
A m
ultis
ecto
ral
publ
ic
heal
th
wor
kfor
ce s
trat
egy
exis
ts, b
ut is
not
re
gula
rly re
view
ed, u
pdat
ed o
r im
ple-
men
ted
cons
iste
ntly
Appr
opria
te
hum
an
reso
urce
s ar
e av
aila
ble
in r
elev
ant
sect
ors
and
at
natio
nal a
nd in
term
edia
te le
vels
Regu
lar
trai
ning
s,
incl
udin
g O
ne
Hea
lth
appr
oach
fo
r zo
onot
ic
di-
seas
es,
are
avai
labl
e fo
r va
rious
pr
ofes
sion
s/ca
dres
th
roug
h di
-se
ase-
spec
ific
prog
ram
mes
or t
arge
-te
d in
itiat
ives
One
leve
l of F
ETP
(bas
ic, in
term
edia
te,
or a
dvan
ced)
7 or
com
para
ble
appl
ied
epid
emio
logy
tr
aini
ng
prog
ram
me
is
in
plac
e in
th
e co
untr
y or
in
an
othe
r co
untr
y th
roug
h an
exi
stin
g ag
reem
ent
Dem
onst
rate
d ca
paci
ty -
4
A pu
blic
hea
lth w
orkf
orce
str
ateg
y8 ha
s be
en a
dopt
ed a
nd i
mpl
emen
ted
cons
iste
ntly
, and
is re
view
ed, t
rack
ed
and
repo
rted
on
annu
ally
Hum
an r
esou
rces
are
ava
ilabl
e as
re
quire
d in
rel
evan
t se
ctor
s an
d at
re
leva
nt l
evel
s of
the
pub
lic h
ealth
sy
stem
(su
ch a
s ep
idem
iolo
gist
at
natio
nal a
nd in
term
edia
te le
vels
, and
as
sist
ant
epid
emio
logi
st
(or
shor
t co
urse
trai
ned
epid
emio
logi
st) a
t the
lo
cal l
evel
)
Trai
ning
pl
ans
are
deve
lope
d an
d re
gula
r tr
aini
ngs
are
cond
ucte
d by
pr
ofes
sion
al b
odie
s or
rel
evan
t in
s-tit
utio
ns/u
nits
to
es
tabl
ish
skill
s an
d co
mpe
tenc
y st
anda
rds
for
the
wor
kfor
ce a
t the
nat
iona
l lev
el
Two
leve
ls o
f FE
TP (
basi
c, i
nter
me-
diat
e an
d/or
adv
ance
d) o
r co
mpa
-ra
ble
appl
ied
epid
emio
logy
tra
inin
g pr
ogra
mm
e(s)
ar
e in
pl
ace
in
the
coun
try
or in
ano
ther
cou
ntry
thro
ugh
an e
xist
ing
agre
emen
t
Sust
aina
ble
capa
city
- 5
Publ
ic h
ealth
wor
kfor
ce r
eten
tion
is
trac
ked
and
plan
s ar
e in
pla
ce to
pro
-vi
de c
ontin
uous
edu
catio
n, a
s w
ell
as r
etai
n an
d pr
omot
e a
qual
ified
w
orkf
orce
with
in th
e na
tiona
l sys
tem
Coun
try
has
capa
city
to s
end
and
re-
ceiv
e m
ultid
isci
plin
ary
pers
onne
l wit-
hin
the
coun
try
(shi
ftin
g re
sour
ces)
an
d in
tern
atio
nally
to
as
sist
ot
her
coun
trie
s in
dev
elop
ing
capa
citie
s fo
r ep
idem
ic p
repa
redn
ess
and
cont
rol
In-s
ervi
ce
trai
ning
s ar
e re
gula
rly
cond
ucte
d at
na
tiona
l an
d su
bnat
iona
l le
vels
, an
d pr
ofes
sion
al
bodi
es o
r re
leva
nt i
nstit
utio
ns/u
nits
re
gula
rly r
evie
w a
nd u
pdat
e tr
aini
ng
offe
rs
Thre
e le
vels
of
FETP
(ba
sic,
int
er-
med
iate
and
adv
ance
d) o
r co
mpa
-ra
ble
appl
ied
epid
emio
logy
tra
inin
g pr
ogra
mm
e(s)
9 ar
e in
pla
ce i
n th
e co
untr
y or
in a
noth
er c
ount
ry th
roug
h an
exi
stin
g ag
reem
ent,
with
sus
tai-
nabl
e na
tiona
l fun
ding
DE
TE
CT

INTERNATIONAL HEALTH REGULATIONS (2005)
65 - Joint External Evaluation Tool - Second edition
1 -
Ther
e is
crit
ical
com
pete
ncy
in th
e PV
S to
ol C
C I-
1: P
rofe
ssio
nal a
nd te
chni
cal s
taffi
ng o
f the
vet
erin
ary
serv
ices
; CC
I-2:
Com
pete
ncie
s of
the
vete
rinar
ians
and
vet
erin
ary
para
-pro
fess
iona
ls; a
nd C
C I-
3: C
ontin
uing
edu
catio
n.2
- Th
e in
dica
tor D
.4.1
refe
rs to
a m
ultis
ecto
ral p
ublic
hea
lth w
orkf
orce
cap
acity
for t
he c
ount
ry. T
his
incl
udes
prim
ary
care
ser
vice
pro
vide
rs.
3 -
In-s
ervi
ce tr
aini
ngs
offe
r CPE
thro
ugh
face
-to-
face
trai
ning
s, b
lend
ed o
r e-l
earn
ing
offe
rs, s
hort
cou
rses
, exe
rcis
es, a
nd a
dvan
ced
trai
ning
s th
at c
ompl
emen
t and
/or a
dvan
ce k
now
ledg
e, s
kills
and
com
pete
ncie
s. T
hese
can
be
offe
red
by n
atio
nal/
regi
onal
trai
ning
inst
itute
s, u
nive
rsiti
es o
r nat
iona
l pro
fess
iona
l bod
ies
and
shou
ld re
spon
d to
a n
atio
nally
agr
eed
CPE
prog
ram
me.
4 -
Fiel
d ep
idem
iolo
gy tr
aini
ng p
rogr
amm
e: C
heck
Glo
ssar
y.5
- Ap
prop
riate
hum
an re
sour
ces:
Hum
an re
sour
ces
incl
ude
nurs
es a
nd m
idw
ives
, phy
sici
ans,
pub
lic h
ealth
and
env
ironm
enta
l spe
cial
ists
, soc
ial s
cien
tists
, com
mun
icat
ion
spec
ialis
ts, o
ccup
atio
nal h
ealth
spe
cial
ists
, lab
orat
ory
scie
ntis
ts/t
echn
icia
ns, b
iost
atis
ticia
ns, I
T sp
ecia
lists
and
bio
med
ical
tech
nici
ans.
The
re is
a c
orre
spon
ding
wor
kfor
ce in
the
anim
al s
ecto
r of v
eter
inar
ians
, ani
mal
hea
lth p
rofe
ssio
nals
, par
a-ve
terin
aria
ns, e
pide
mio
logi
sts
and
IT
spec
ialis
ts, e
tc.
6 -
Wor
kfor
ce d
evel
opm
ent i
s a
cros
s-cu
ttin
g el
emen
t, an
d IH
R im
plem
enta
tion
will
dep
end
on a
str
ong
publ
ic h
ealth
wor
kfor
ce. I
mpl
emen
tatio
n of
IHR
depe
nds
on th
e av
aila
bilit
y of
suf
ficie
nt a
nd w
ell-
trai
ned
epid
emio
logi
sts,
so
cial
sci
entis
ts, l
abor
ator
y an
d pu
blic
hea
lth s
peci
alis
ts a
s w
ell a
s th
e ca
paci
ty o
f med
ical
and
nur
sing
sta
ff to
cor
rect
ly m
anag
e th
ose
affe
cted
and
han
dle
emer
genc
ies.
Dep
endi
ng o
n th
e co
untr
y, th
ese
forc
es c
an b
e in
the
publ
ic
and/
or p
rivat
e se
ctor
.7
- FE
TP B
asic
Lev
el T
rain
ing
is fo
r loc
al h
ealth
sta
ff an
d co
nsis
ts o
f lim
ited
clas
sroo
m h
ours
inte
rspe
rsed
thro
ugho
ut a
s a
thre
e-to
-five
mon
th o
n-th
e-jo
b fie
ld a
ssig
nmen
t to
build
cap
acity
in c
ondu
ctin
g tim
ely
outb
reak
det
ectio
n,
publ
ic h
ealth
resp
onse
and
pub
lic h
ealth
sur
veill
ance
. FET
P In
term
edia
te L
evel
Tra
inin
g is
for d
istr
ict/
regi
on/s
tate
-lev
el e
pide
mio
logi
sts,
and
con
sist
s of
lim
ited
clas
sroo
m h
ours
inte
rspe
rsed
thro
ugho
ut a
s a
six-
to-n
ine
mon
th
on-t
he-j
ob m
ento
red
field
ass
ignm
ent t
o bu
ild c
apac
ity in
con
duct
ing
outb
reak
inve
stig
atio
ns, p
lann
ed e
pide
mio
logi
c st
udie
s, a
nd p
ublic
hea
lth s
urve
illan
ce a
naly
ses
and
eval
uatio
ns. F
ETP
Adva
nced
Lev
el T
rain
ing
is fo
r adv
ance
d ep
idem
iolo
gist
s an
d co
nsis
ts o
f lim
ited
clas
sroo
m h
ours
inte
rspe
rsed
thro
ugho
ut th
e 24
mon
ths
of m
ento
red
field
ass
ignm
ents
to b
uild
cap
acity
in o
utbr
eak
inve
stig
atio
ns, p
lann
ed e
pide
mio
logi
c st
udie
s, p
ublic
hea
lth s
urve
illan
ce
anal
yses
and
eva
luat
ions
, sci
entifi
c co
mm
unic
atio
n, a
nd e
vide
nce-
base
d de
cisi
on m
akin
g fo
r dev
elop
men
t of e
ffect
ive
publ
ic h
ealth
pro
gram
min
g w
ith a
nat
iona
l foc
us. A
nim
al h
ealth
pro
fess
iona
ls c
an b
e en
gage
d in
thes
e FE
TP
trai
ning
s. 8
- P
ublic
hea
lth w
orkf
orce
pla
nnin
g sh
ould
cov
er b
oth
the
anim
al a
nd h
uman
hea
lth s
ecto
rs a
nd s
houl
d in
clud
e:• P
ublic
hea
lth s
peci
alis
ts, e
pide
mio
logi
sts,
soc
ial s
cien
tists
, bio
stat
istic
ians
, vet
erin
ary
epid
emio
logi
sts,
vet
erin
ary
publ
ic h
ealth
spe
cial
ists
and
oth
er p
ublic
hea
lth p
erso
nnel
.• P
rimar
y ca
re p
rovi
ders
(phy
sici
ans,
nur
ses,
mid
wiv
es),
vete
rinar
ians
and
par
a-ve
terin
aria
ns.
• Com
mun
ity h
ealth
wor
kers
and
sta
ff in
form
atio
n sy
stem
s sp
ecia
lists
(suc
h as
labo
rato
ry s
peci
alis
ts/t
echn
icia
ns, b
iom
edic
al te
chni
cian
s), f
or s
uppo
rtiv
e fu
nctio
ns.
Publ
ic h
ealth
wor
kfor
ce p
lann
ing
shou
ld a
lso
incl
ude:
• I
ndic
atio
n of
trai
ning
s th
at h
ave
been
pro
vide
d at
the
natio
nal l
evel
or a
re a
vaila
ble
to s
taff
from
a p
artn
er e
ntity
. Des
crip
tion
of lo
ng-t
erm
trai
ning
pro
gram
mes
that
are
ava
ilabl
e to
hel
p ex
pand
the
pipe
line
of q
ualifi
ed p
ublic
he
alth
pro
fess
iona
ls w
ithin
the
coun
try.
Des
crip
tion
of im
plem
enta
tion
of o
ccup
atio
nal s
afet
y an
d he
alth
to a
ll pu
blic
and
priv
ate
heal
th c
are
faci
litie
s an
d to
farm
s.9
-Com
para
ble
appl
ied
epid
emio
logy
trai
ning
pro
gram
mes
or t
hose
spe
cial
ized
in e
pide
mio
logy
wou
ld b
e si
mila
r to
thes
e le
vels
defi
ned
abov
e.
Cont
extu
al q
uest
ions
: N/A
Tech
nica
l que
stio
ns:
D.4.
1 An
upd
ated
wor
kfor
ce s
trat
egy
is in
pla
ce1.
Is
ther
e a
stra
tegy
to e
nsur
e th
at a
ppro
pria
te w
orkf
orce
and
hum
an re
sour
ces
for t
he h
ealth
sec
tor a
re in
pla
ce?
a. D
oes
this
cov
er th
e fu
ll ra
nge
of ta
sks
and
serv
ices
in th
e (p
ublic
and
priv
ate)
hea
lth s
ecto
r (pr
even
tion/
dete
ctio
n an
d re
spon
se, c
are
and
reha
bilit
atio
n)?
2.
Des
crib
e w
hich
car
eer t
rack
s ar
e in
clud
ed in
the
wor
kfor
ce s
trat
egy
(suc
h as
epi
dem
iolo
gist
s, v
eter
inar
ians
, lab
orat
ory
assi
stan
ts a
nd s
peci
alis
ts, d
octo
rs,
nurs
es)?
a. A
re c
omm
unity
hea
lth w
orke
rs a
par
t of t
he fo
rmal
hea
lth w
orkf
orce
?b.
Are
the
re jo
b de
scrip
tions
for
the
var
ious
car
eer
trac
ks a
nd p
ositi
ons
with
in t
hem
(su
ch a
s pe
rfor
man
ce a
ppra
isal
, com
pete
ncy
stan
dard
s, c
aree
r la
dder
)?3.
Is
attr
ition
a c
once
rn fo
r the
nat
iona
l pub
lic h
ealth
sys
tem
(may
be
caus
ed b
y ag
ing
empl
oyee
s, s
taff
depa
rtur
es o
r oth
er re
ason
s)?
a. W
hat i
s th
e m
edia
n nu
mbe
r of y
ears
that
pub
lic h
ealth
per
sonn
el h
ave
been
on
staf
f rol
ls w
ithin
the
min
istr
y an
d/or
nat
iona
l ins
titut
es?
b. A
re th
ere
ince
ntiv
es in
pla
ce to
mai
ntai
n th
e ex
istin
g pu
blic
hea
lth w
orkf
orce
in th
e co
untr
y?
DE
TE
CT

INTERNATIONAL HEALTH REGULATIONS (2005)
66 - Joint External Evaluation Tool - Second edition
i. D
escr
ibe
effo
rts
in p
lace
to re
tain
the
publ
ic h
ealth
wor
kfor
ce.
ii.
Are
ther
e sp
ecifi
c in
cent
ives
for a
ny w
orkf
orce
spe
cial
ties
(may
incl
ude
phys
icia
ns, n
urse
s, v
eter
inar
ians
, bio
stat
istic
ians
labo
rato
ry a
ssis
tant
s an
d sp
ecia
lists
, or a
nim
al h
ealth
pro
fess
iona
ls)?
4.
How
is th
e w
orkf
orce
str
ateg
y be
ing
impl
emen
ted
and
trac
ked?
a.
Pro
vide
a c
opy
of th
e st
rate
gy, i
f ava
ilabl
e.b.
Pro
vide
a c
opy
of th
e w
orkf
orce
str
ateg
y tr
acki
ng re
port
, if a
vaila
ble.
5.
Doe
s th
e st
rate
gy a
ddre
ss o
ccup
atio
nal s
afet
y an
d he
alth
in h
ealth
car
e fa
cilit
ies?
a. I
f yes
, wha
t is
the
cove
rage
of o
ccup
atio
nal s
afet
y an
d he
alth
in p
ublic
hea
lth s
yste
ms?
b. I
f not
, how
is th
e oc
cupa
tiona
l saf
ety
and
heal
th a
ddre
ssed
in h
ealth
car
e fa
cilit
ies.
6.
How
is th
e na
tiona
l pub
lic h
ealth
wor
kfor
ce fi
nanc
ed w
ithin
the
coun
try?
a. A
re th
e po
sitio
ns fo
r the
var
ious
cad
res
avai
labl
e, fi
nanc
ed a
nd fi
lled?
7.
Is th
ere
a se
para
te w
orkf
orce
str
ateg
y fo
r hum
an re
sour
ces
in p
lace
for t
he a
nim
al h
ealth
sec
tor?
8.
Is
ther
e a
trai
ning
pla
n to
upd
ate
the
wor
kfor
ce w
ith p
olic
y an
d st
rate
gies
?
D.4.
2 H
uman
reso
urce
s ar
e av
aila
ble
to e
ffec
tivel
y im
plem
ent I
HR
1.
Des
crib
e th
e cu
rren
t hum
an re
sour
ces
capa
city
in th
e co
untr
y.
a. W
hat i
s th
e ex
istin
g ca
paci
ty o
n ep
idem
iolo
gist
s, c
linic
ians
, bio
stat
istic
ians
, inf
orm
atio
n sy
stem
s sp
ecia
lists
, vet
erin
aria
ns, s
ocia
l sci
entis
ts, l
abor
ator
y te
chni
cian
s/sp
ecia
lists
and
oth
er p
ublic
hea
lth p
erso
nnel
for d
iffer
ent l
evel
s of
the
heal
th s
yste
m (l
ocal
, int
erm
edia
te a
nd n
atio
nal)?
b. T
o w
hat e
xten
t are
thes
e ca
paci
ties
avai
labl
e (o
nly
at n
atio
nal l
evel
or b
elow
)?c.
Doe
s ea
ch lo
cal a
nd/o
r int
erm
edia
te le
vel h
ave
som
e ca
paci
ty fo
r epi
dem
iolo
gy, c
ase
man
agem
ent,
labo
rato
ry s
ervi
ces,
and
oth
ers?
2.
Des
crib
e ho
w m
ultid
isci
plin
ary
task
forc
es a
re fo
rmed
and
com
mun
icat
e w
ith o
ther
act
ors
(at n
atio
nal,
inte
rmed
iate
and
per
iphe
ral l
evel
s).
a. H
ow a
re m
ultid
isci
plin
ary
task
forc
es o
rgan
ized
? H
ow d
o di
ffere
nt p
rofe
ssio
nals
inte
ract
and
is th
is o
rgan
ized
thro
ugh
a ta
sk fo
rce?
b.
Dis
cuss
ava
ilabi
lity
and
dist
ribut
ion
of in
divi
dual
hum
an re
sour
ces
capa
citie
s:i.
Epid
emio
logi
sts
(incl
udin
g fie
ld e
pide
mio
logy
sho
rt te
rm a
nd lo
ng te
rm)
ii.
Clin
icia
ns a
nd c
linic
al a
ssis
tant
siii
. N
urse
siv
. La
bora
tory
spe
cial
ists
and
tech
nici
ans
v.
Info
rmat
ion
spec
ialis
ts a
nd a
ssis
tant
svi
. So
cial
sci
entis
tsvi
i. Ve
terin
aria
ns, v
eter
inar
y te
chni
cian
s an
d pa
ra-v
eter
inar
ians
vii.
Oth
er re
leva
nt p
ublic
hea
lth p
erso
nnel
.3.
D
escr
ibe
how
pro
fess
iona
ls a
t the
nat
iona
l, in
term
edia
te a
nd lo
cal l
evel
s co
mm
unic
ate
on a
regu
lar b
asis
. Are
ther
e st
anda
rd re
port
ing
conn
ectio
ns b
etw
een
thes
e le
vels
?
DE
TE
CT

INTERNATIONAL HEALTH REGULATIONS (2005)
67 - Joint External Evaluation Tool - Second edition
4.
Des
crib
e ho
w p
rofe
ssio
nals
at t
he n
atio
nal,
inte
rmed
iate
and
loca
l lev
els
com
mun
icat
e du
ring
an in
fect
ious
dis
ease
out
brea
k. A
re th
ere
stan
dard
repo
rtin
g co
nnec
tions
bet
wee
n th
ese
leve
ls d
urin
g ou
tbre
aks?
5.
How
man
y tr
aine
d fie
ld e
pide
mio
logi
sts
are
avai
labl
e to
sup
port
inv
estig
atio
ns t
hrou
ghou
t th
e co
untr
y? I
s th
ere
a si
mpl
e m
easu
re o
f th
e nu
mbe
rs o
f ep
idem
iolo
gist
s pe
r uni
t of t
otal
pop
ulat
ion
that
may
hel
p di
ffere
ntia
te q
ualit
y le
vels
– fo
r exa
mpl
e: le
ss th
an 1
per
500
000
in c
apac
ity le
vels
1 o
r 2; 1
per
20
0 00
0 to
500
000
in c
apac
ity le
vel 3
; or m
ore
than
1 p
er 2
00 0
00 in
cap
acity
leve
ls 4
or 5
. 6.
D
oes
the
coun
try
have
est
ablis
hed
proc
edur
es fo
r sur
ge o
f the
se p
rofe
ssio
nals
?7.
D
oes
each
inte
rmed
iate
leve
l/dis
tric
t (or
oth
er s
imila
r adm
inis
trat
ive
divi
sion
s) h
ave
field
epi
dem
iolo
gy c
apac
ity?
8.
Doe
s th
e co
untr
y ha
ve a
hum
an re
sour
ces
data
base
? If
yes,
how
is th
e da
taba
se m
aint
aine
d an
d up
date
d?
D.4.
3 In
-ser
vice
trai
ning
s ar
e av
aila
ble
1.
Are
ther
e CP
E pr
ogra
mm
es fo
r pub
lic h
ealth
offi
cers
, sur
veill
ance
offi
cers
, nur
ses,
mid
wiv
es, g
ener
al m
edic
al p
ract
ition
ers,
vet
erin
aria
ns, p
ara-
vete
rinar
ians
th
at in
clud
e ou
tbre
ak p
repa
redn
ess
and
cont
rol?
2.
Whi
ch p
rofe
ssio
ns/c
adre
s ha
ve re
ceiv
ed s
peci
al tr
aini
ngs
on o
utbr
eak
prep
ared
ness
and
resp
onse
? 3.
D
escr
ibe
any
shor
t-/l
ong-
term
tra
inin
g pr
ogra
mm
es t
hat
are
avai
labl
e to
hel
p ex
pand
the
num
ber
of q
ualifi
ed p
ublic
hea
lth p
rofe
ssio
nals
with
in t
he
coun
try,
i.e.
a. P
hysi
cian
s (p
ublic
hea
lth a
nd/o
r clin
ical
car
e)b.
Nur
ses
(pub
lic h
ealth
and
/or c
linic
al c
are)
c. V
eter
inar
ians
(pub
lic h
ealth
, agr
icul
tura
l and
/or p
rivat
e pr
actic
e) a
nd p
ara-
vete
rinar
ians
d. B
iost
atis
ticia
nse.
Oth
er p
ublic
hea
lth o
ffice
rs/s
urve
illan
ce o
ffice
rsf.
Labo
rato
ry a
ssis
tant
s an
d sp
ecia
lists
g. L
ives
tock
pro
fess
iona
ls.
4.
Des
crib
e pr
ogra
mm
es a
nd in
stitu
tions
/pro
fess
iona
l bod
ies
in-c
harg
e of
CPE
and
/or
trai
ning
s, o
r th
eir
capa
city
in tu
rn o
f del
iver
ing
trai
ning
. How
are
they
fu
nded
?5.
Is
ther
e an
y tr
aini
ng re
late
d to
con
tinge
ncy
plan
ning
, man
agem
ent o
f em
erge
ncy
situ
atio
ns, o
r ris
k co
mm
unic
atio
ns?
6.
Is th
ere
any
trai
ning
that
incl
udes
join
t exe
rcis
es fo
r mul
tidis
cipl
inar
y te
ams?
a.
If y
es, d
escr
ibe
brie
fly (r
egul
ar/o
n de
man
d).
D.4.
4 F
ETP
or o
ther
app
lied
epid
emio
logy
trai
ning
pro
gram
me
in p
lace
1.
D
escr
ibe
curr
ent fi
eld
epid
emio
logy
cap
acity
in th
e co
untr
y.a.
Des
crib
e th
e tr
aini
ng p
rogr
amm
e fo
r fiel
d ep
idem
iolo
gist
s. W
ho c
ondu
cts
this
trai
ning
? b.
How
is fi
eld
epid
emio
logy
cap
acity
trac
ked
in th
e co
untr
y?2.
Is
ther
e an
FET
P or
oth
er s
tand
ard
epid
emio
logy
trai
ning
pro
gram
me
in th
e co
untr
y?a.
Des
crib
e cu
rren
t fiel
d ep
idem
iolo
gy c
apac
ity in
the
coun
try.
DE
TE
CT

INTERNATIONAL HEALTH REGULATIONS (2005)
68 - Joint External Evaluation Tool - Second edition
b. D
oes
the
epid
emio
logy
trai
ning
pro
gram
me
targ
et c
urre
nt m
embe
rs o
f the
pub
lic h
ealth
wor
kfor
ce, o
r stu
dent
s, o
r bot
h?c.
How
is fi
eld
epid
emio
logy
cap
acity
trac
ked
in th
e co
untr
y?d.
Des
crib
e ho
w e
pide
mio
logi
sts
at th
e na
tiona
l, in
term
edia
te a
nd lo
cal l
evel
s co
mm
unic
ate
on a
regu
lar b
asis
. Are
ther
e st
anda
rd re
port
ing
conn
ectio
ns
betw
een
thes
e le
vels
?e.
Hav
e ve
terin
aria
ns p
artic
ipat
ed in
the
epid
emio
logy
trai
ning
pro
gram
me?
f.
Prov
ide
mea
sure
s on
the
num
ber o
f epi
dem
iolo
gy tr
aini
ng p
rogr
amm
e gr
adua
tes
in th
e co
untr
y an
d th
eir c
urre
nt p
ositi
ons.
g. D
escr
ibe
the
men
tors
hip
prog
ram
me
for e
pide
mio
logy
trai
ning
pro
gram
me
resi
dent
s.h.
Is
ther
e a
part
ners
hip
with
oth
er c
ount
ries
in th
e re
gion
to s
hare
epi
dem
iolo
gy tr
aini
ng p
rogr
amm
e gr
adua
tes
durin
g em
erge
ncy
even
ts?
i. H
ow m
any
trai
ned
field
epi
dem
iolo
gist
s ar
e av
aila
ble
to s
uppo
rt in
vest
igat
ions
thro
ugho
ut th
e co
untr
y?j.
Doe
s ea
ch in
term
edia
te le
vel/
dist
rict (
or o
ther
sim
ilar a
dmin
istr
ativ
e di
visi
on) h
ave
field
epi
dem
iolo
gy c
apac
ity?
3.
Des
crib
e an
y ot
her l
ong-
term
trai
ning
pro
gram
mes
that
are
ava
ilabl
e to
hel
p ex
pand
the
num
ber o
f qua
lified
pub
lic h
ealth
pro
fess
iona
ls w
ithin
the
coun
try,
i.e.
a. P
hysi
cian
s (p
ublic
hea
lth a
nd/o
r clin
ical
car
e)b.
Nur
ses
(pub
lic h
ealth
and
/or c
linic
al c
are)
c. V
eter
inar
ians
(pub
lic h
ealth
, agr
icul
tura
l and
/or p
rivat
e pr
actic
e)d.
Bio
stat
istic
ians
e. L
abor
ator
y as
sist
ants
and
spe
cial
ists
.4.
Is
ther
e a
prof
essi
onal
vet
erin
aria
n as
soci
atio
n in
the
coun
try?
Doe
s it
have
a C
PE?
If ye
s, w
hat d
oes
it co
ver?
How
is it
fina
nced
? 5.
Is
ther
e a
spec
ific
trai
ning
on
zoon
osis
in th
e hu
man
med
icin
e cu
rric
ulum
or i
n an
y CP
E pr
ogra
mm
e fo
r med
ical
pra
ctiti
oner
s?
Doc
umen
tatio
n or
evi
denc
e fo
r lev
el o
f cap
abili
ty:
l
Sam
ple
field
epi
dem
iolo
gy tr
aini
ng c
urric
ulum
use
d in
the
coun
try
• Num
ber o
f gra
duat
es/y
ear,
and
if av
aila
ble,
pos
ition
s af
ter t
rain
ing
l
Publ
ic h
ealth
wor
kfor
ce/h
uman
reso
urce
pla
n/st
rate
gy, i
f ava
ilabl
e an
d la
test
str
ateg
y dr
afte
d/en
acte
dl
Annu
al re
port
s ba
sed
on w
orkf
orce
str
ateg
yl
Plan
ning
and
ava
ilabi
lity
of re
sour
ces
l
Term
s of
refe
renc
e/jo
b de
scrip
tions
of p
rovi
ncia
l/di
stric
t rap
id re
spon
se te
ams
l
Job
desc
riptio
n/te
rms
of re
fere
nce
of p
rovi
ncia
l/di
stric
t pub
lic h
ealth
offi
cer i
n-ch
arge
of o
utbr
eak
prep
ared
ness
l
Budg
et fo
r hum
an re
sour
ces
for h
ealth
(ani
mal
and
hum
an h
ealth
sec
tor)
, don
or c
ontr
ibut
ions
DE
TE
CT

INTERNATIONAL HEALTH REGULATIONS (2005)
69 - Joint External Evaluation Tool - Second edition
l
Des
crip
tion
of th
e hu
man
reso
urce
s m
anag
emen
t inf
orm
atio
n sy
stem
• L
ist o
f var
iabl
es u
sed
l
Dat
a fr
om h
uman
reso
urce
info
rmat
ion
syst
ems,
if a
vaila
ble
• P
ost a
nd s
taff
list,
if av
aila
ble;
sta
ff tu
rnov
er, a
nd n
umbe
r of s
taff
atte
ndin
g in
-ser
vice
trai
ning
l
Annu
al re
port
s ba
sed
on w
orkf
orce
str
ateg
yl
List
s of
in-s
ervi
ce tr
aini
ng a
vaila
ble
in th
e co
untr
yl
List
s of
nat
iona
l tra
inin
g in
stitu
tes/
prof
essi
onal
bod
ies/
scho
ols
of p
ublic
hea
lth/n
ursi
ng/m
idw
ifery
/vet
erin
ary/
med
ical
col
lege
s/un
iver
sitie
s th
at p
rovi
de in
-se
rvic
e tr
aini
ng c
ours
es
l
Num
ber o
f gra
duat
es/t
rain
ees
per y
ear
l
CPE
prog
ram
me
and
cour
se li
st (i
f ava
ilabl
e)l
Trai
ning
cou
rse
list f
or p
rofe
ssio
nals
that
do
not h
ave
CPE
prog
ram
mes
l
Evid
ence
of t
rain
ing
on is
sues
rela
ted
to o
ccup
atio
nal h
ealth
, saf
ety
and
secu
rity.
DE
TE
CT

INTERNATIONAL HEALTH REGULATIONS (2005)
70 - Joint External Evaluation Tool - Second edition
RESP
ON
DEM
ERG
ENCY
PRE
PARE
DN
ESS
Targ
et:
Stat
es P
artie
s ar
e in
“em
erge
ncy
prep
ared
ness
” (d
efine
d as
, the
kno
wle
dge
and
capa
citie
s an
d or
gani
zatio
nal s
yste
ms
deve
lope
d by
gov
ernm
ents
, re
spon
se a
nd re
cove
ry o
rgan
izat
ions
, com
mun
ities
and
indi
vidu
als
to e
ffect
ivel
y an
ticip
ate,
resp
ond
to, a
nd re
cove
r fro
m th
e im
pact
s of
like
ly, im
min
ent,
emer
ging
or
cur
rent
em
erge
ncie
s), w
hich
is a
com
bina
tion
of p
lann
ing,
allo
catio
n of
reso
urce
s, tr
aini
ng, e
xerc
isin
g, a
nd o
rgan
izin
g to
bui
ld, s
usta
in a
nd im
prov
e op
erat
iona
l ca
pabi
litie
s at
nat
iona
l, int
erm
edia
te a
nd lo
cal o
r prim
ary
resp
onse
leve
ls b
ased
on
stra
tegi
c ris
k as
sess
men
ts. T
he s
trat
egic
risk
ass
essm
ent i
dent
ifies
, ana
lyse
s an
d ev
alua
tes
the
rang
e of
ris
ks in
a c
ount
ry a
nd e
nabl
es r
isks
to
be a
ssig
ned
a le
vel o
f pr
iorit
y an
d in
clud
es a
naly
ses
of p
oten
tial h
azar
ds e
xpos
ures
and
vu
lner
abili
ties,
iden
tifica
tion
and
map
ping
of a
vaila
ble
reso
urce
s, a
nd a
naly
ses
of c
apac
ities
(rou
tine
and
surg
e) a
t the
nat
iona
l, in
term
edia
te a
nd lo
cal o
r prim
ary
leve
ls t
o m
anag
e th
e ris
ks o
f ou
tbre
aks
and
othe
r em
erge
ncie
s. E
mer
genc
y pr
epar
edne
ss a
pplie
s to
any
haz
ard
that
may
cau
se a
n em
erge
ncy
and
incl
udes
bi
olog
ical
, che
mic
al, r
adio
logi
cal a
nd n
ucle
ar, n
atur
al, o
ther
tech
nolo
gica
l and
soc
ieta
l haz
ards
.
As m
easu
red
by: (
1) )
Exis
tenc
e of
nat
iona
l str
ateg
ic m
ultih
azar
d em
erge
ncy
risk
asse
ssm
ents
(ris
k pr
ofile
s) a
nd re
sour
ce m
appi
ng. (
2) E
xist
ence
of m
ultih
azar
d em
erge
ncy
resp
onse
pla
ns. (
3) E
vide
nce,
from
exe
rcis
es, a
fter
-act
ion
and
othe
r rev
iew
s of
effe
ctiv
e an
d ef
ficie
nt m
ultis
ecto
ral e
mer
genc
y re
spon
se o
pera
tions
fo
r out
brea
ks a
nd o
ther
pub
lic h
ealth
em
erge
ncie
s.
Desi
red
impa
ct: M
ultis
ecto
ral a
ctor
s at
nat
iona
l and
sub
natio
nal (
loca
l and
inte
rmed
iate
) lev
els
have
a c
omm
on u
nder
stan
ding
of t
he p
riorit
y ris
ks a
nd re
ady
for
timel
y, ef
fect
ive
and
effic
ient
em
erge
ncy
resp
onse
ope
ratio
ns fo
r out
brea
ks a
nd o
ther
em
erge
ncie
s.
RE
SP
ON
D

INTERNATIONAL HEALTH REGULATIONS (2005)
71 - Joint External Evaluation Tool - Second edition
Scor
eIn
dica
tors
: Em
erge
ncy
prep
ared
ness
R.1.
1 St
rate
gic
emer
genc
y ris
k as
sess
men
ts1
cond
ucte
d an
d em
erge
ncy
reso
urce
s id
entifi
ed a
nd m
appe
dR.
1.2
Nat
iona
l mul
tisec
tora
l mul
tihaz
ard
emer
genc
y pr
epar
edne
ss m
easu
res,
in
clud
ing
emer
genc
y re
spon
se p
lans
2 , ar
e de
velo
ped,
impl
emen
ted
and
test
ed
No
capa
city
- 1
A na
tiona
l em
erge
ncy
risk
profi
le b
ased
on
a st
rate
gic
mul
tihaz
ard
emer
genc
y ris
k as
sess
men
t is
not a
vaila
ble
or h
as n
ot b
een
upda
ted
in th
e pa
st fi
ve y
ears
Nat
iona
l lev
el in
vent
orie
s an
d m
aps
of m
ultis
ecto
ral r
esou
rces
for e
mer
genc
y re
spon
se a
re n
ot a
vaila
ble
or h
ave
not b
een
upda
ted
in th
e pa
st fi
ve y
ears
A na
tiona
l mul
tisec
tora
l mul
tihaz
ard
plan
for
stre
ngth
enin
g em
erge
ncy
pre-
pare
dnes
s is
not
ava
ilabl
e3 A
natio
nal m
ultis
ecto
ral m
ultih
azar
d em
erge
ncy
resp
onse
pla
n is
not
ava
i-la
ble
Lim
ited
ca
paci
ty -
2
A na
tiona
l st
rate
gic
mul
tihaz
ard
emer
genc
y ris
k as
sess
men
t ha
s be
en
cond
ucte
d in
the
pas
t fiv
e ye
ars
and
docu
men
ted
in a
nat
iona
l he
alth
em
erge
ncy
risk
profi
leN
atio
nal l
evel
inve
ntor
ies
and
map
s of
hea
lth s
ecto
r res
ourc
es fo
r em
erge
ncy
resp
onse
are
ava
ilabl
e an
d ha
ve b
een
upda
ted
in th
e pa
st fi
ve y
ears
A na
tiona
l m
ultis
ecto
ral
mul
tihaz
ard
plan
tha
t id
entifi
es k
ey m
easu
res
for
stre
ngth
enin
g em
erge
ncy
prep
ared
ness
for p
riorit
y ris
ks is
in p
lace
4 . A
natio
nal m
ultih
azar
d em
erge
ncy
resp
onse
pla
n w
ith S
OPs
for
cor
e em
er-
genc
y re
spon
se c
oord
inat
ion
func
tions
has
bee
n de
velo
ped
with
in t
he p
ast
two
year
s to
resp
ond
to e
mer
genc
ies,
incl
udin
g PH
EICs
Deve
lope
d ca
paci
ty -
3
Nat
iona
l res
ourc
es fo
r em
erge
ncy
resp
onse
in a
ll re
leva
nt s
ecto
rs h
ave
been
id
entifi
ed a
nd m
appe
d (s
uch
as lo
gist
ics,
sta
ff/ex
pert
s, fi
nanc
e) in
the
pas
t tw
o ye
ars
A pl
an fo
r the
man
agem
ent a
nd d
istr
ibut
ion
of n
atio
nal s
tock
pile
s is
in p
lace
Emer
genc
y pr
epar
edne
ss m
easu
res2
are
impl
emen
ted
at n
atio
nal l
evel
s by
pu
blic
hea
lth, a
nim
al h
ealth
and
oth
er r
elev
ant
sect
ors,
incl
udin
g po
ints
of
entr
y an
d m
ass
gath
erin
g ev
ents
Nat
iona
l m
ultis
ecto
ral
mul
tihaz
ard
emer
genc
y re
spon
se p
lans
hav
e be
en
exer
cise
d or
use
d in
act
ual r
espo
nse
oper
atio
ns in
the
past
two
year
s
Dem
onst
rate
d ca
paci
ty -
4
Stra
tegi
c m
ultih
azar
d em
erge
ncy
risk
asse
ssm
ents
and
map
ping
of r
esou
rces
fo
r em
erge
ncy
resp
onse
at
subn
atio
nal
leve
ls h
ave
been
dev
elop
ed i
n th
e pa
st tw
o ye
ars
Nat
iona
l lev
el r
esou
rce
map
ping
has
bee
n re
view
ed a
t le
ast
on a
n an
nual
ba
sis,
and
sto
ckpi
les
(crit
ical
sto
ck le
vels
) for
resp
ondi
ng to
prio
rity
biol
ogic
al,
chem
ical
and
radi
olog
ical
eve
nts
and
othe
r em
erge
ncie
s ar
e ac
cess
ible
Emer
genc
y pr
epar
edne
ss m
easu
res2 a
re im
plem
ente
d at
nat
iona
l, su
bnat
io-
nal a
nd lo
cal l
evel
s by
pub
lic h
ealth
, ani
mal
hea
lth a
nd o
ther
rele
vant
sec
tors
Mul
tisec
tora
l mul
tihaz
ard
emer
genc
y re
spon
se p
lans
and
SO
Ps a
re in
pla
ce
at s
ubna
tiona
l and
loca
l lev
els,
as
wel
l as
at th
e po
ints
of e
ntry
; and
impl
e-m
ente
d or
test
ed in
the
past
two
year
s an
d up
date
d ac
cord
ingl
y
Sust
aina
ble
capa
city
– 5
Nat
iona
l pr
ofile
s on
ris
k an
d re
sour
ce m
aps,
are
mon
itore
d an
d re
gula
rly
upda
ted
(e.g
. on
ann
ual
basi
s) t
o ac
com
mod
ate
emer
ging
thr
eats
and
is
shar
ed re
gula
rly a
mon
g se
ctor
s
Ther
e ar
e de
dica
ted
hum
an re
sour
ces
and
regu
lar b
udge
t fun
ding
to s
uppo
rt
coor
dina
tion
and
impl
emen
tatio
n of
em
erge
ncy
prep
ared
ness
mea
sure
s by
pu
blic
hea
lth, a
nim
al h
ealth
and
oth
er re
leva
nt s
ecto
rs
Ded
icat
ed re
sour
ces
are
in p
lace
for i
mpl
emen
tatio
n of
mul
tisec
tora
l, m
ulti-
haza
rd e
mer
genc
y re
spon
se p
lans
, con
tinge
ncy
plan
s an
d SO
Ps a
t nat
iona
l, su
bnat
iona
l and
loca
l lev
els,
and
are
test
ed, r
evie
wed
and
upd
ated
on
a re
gu-
lar b
asis
1 -
Ther
e is
crit
ical
com
pete
ncy
in th
e PV
S to
ol C
C II-
3: R
isk
anal
ysis
2 -
Emer
genc
y re
spon
se p
lans
sho
uld
be s
cala
ble
and
flexi
ble
to a
ddre
ss k
now
n an
d em
ergi
ng h
azar
ds, i
nclu
ding
dis
ease
thre
ats.
Con
tinge
ncy
plan
s fo
r res
pons
e to
hig
h pr
iorit
y ris
ks s
houl
d be
dev
elop
ed3
- An
y em
erge
ncy
prep
ared
ness
mea
sure
s th
at a
re c
ondu
cted
, sho
uld
be d
one
on a
n ad
hoc
bas
is
4 -
Risk
s ar
e id
entifi
ed a
nd p
riorit
ized
by
stra
tegi
c em
erge
ncy
risk
asse
ssm
ents
. Em
erge
ncy
prep
ared
ness
mea
sure
s in
clud
e st
rate
gic
risk
asse
ssm
ents
, em
erge
ncy
resp
onse
pla
ns, c
ontin
genc
y pl
ans,
trai
ning
, exe
rcis
ing,
sur
ge
capa
city
dev
elop
men
t, bu
sine
ss c
ontin
uity
pla
n. P
lans
sho
uld
be m
ultih
azar
d, m
ultis
ecto
ral a
nd m
ultid
isci
plin
ary,
and
inte
rope
rabl
e w
ith n
atio
nal m
ultis
ecto
ral a
nd m
ultih
azar
d pl
ans.
Em
erge
ncy
prep
ared
ness
cou
ld a
ddre
ss a
ny
risks
and
not
be
limite
d to
thos
e as
soci
ated
with
bio
logi
cal,
chem
ical
and
radi
olog
ical
haz
ards
.
RE
SP
ON
D

INTERNATIONAL HEALTH REGULATIONS (2005)
72 - Joint External Evaluation Tool - Second edition
Cont
extu
al q
uest
ions
: N/A
Tech
nica
l que
stio
ns:
R.1.
1 St
rate
gic
emer
genc
y ris
k as
sess
men
ts c
ondu
cted
and
em
erge
ncy
reso
urce
s id
entifi
ed a
nd m
appe
d1
Doe
s th
e co
untr
y ha
ve a
nat
iona
l em
erge
ncy
risk
profi
le b
ased
on
stra
tegi
c m
ultih
azar
d em
erge
ncy
risk
asse
ssm
ents
? a.
Whe
n w
as th
e la
st n
atio
nal s
trat
egic
mul
tihaz
ard
risk
asse
ssm
ent c
ondu
cted
? W
hich
sec
tors
par
ticip
ated
in th
e ris
k as
sess
men
t?b.
Wha
t are
the
findi
ngs
of th
e na
tiona
l str
ateg
ic e
mer
genc
y ris
k as
sess
men
t?c.
Are
str
ateg
ic r
isk
asse
ssm
ents
con
duct
ed b
y al
l se
ctor
s? D
o he
alth
sec
tor
stra
tegi
c ris
k as
sess
men
ts c
ontr
ibut
e to
nat
iona
l m
ultis
ecto
ral
risk
asse
ssm
ents
?d.
Are
str
ateg
ic r
isk
asse
ssm
ents
con
duct
ed a
t su
bnat
iona
l an
d lo
cal
leve
ls?
Wha
t pr
opor
tion
of s
ubna
tiona
l or
loc
al e
ntiti
es h
as c
ondu
cted
ris
k as
sess
men
ts?
e. I
s th
ere
a ca
paci
ty to
mon
itor p
riorit
y ris
ks o
r em
ergi
ng ri
sks?
How
oft
en a
re n
atio
nal e
mer
genc
y ris
k pr
ofile
s re
view
ed a
nd u
pdat
ed to
acc
omm
odat
e em
ergi
ng th
reat
s or
cha
ngin
g ris
ks?
f. H
ow a
re n
atio
nal r
isk
profi
les
and
reso
urce
s sh
ared
am
ong
sect
ors?
Are
info
rmat
ion
tech
nolo
gy c
apac
ities
util
ized
to s
uppo
rt a
vaila
bilit
y, ac
cess
ibili
ty,
anal
ysis
, upd
atin
g, re
port
ing
and
shar
ing
of ri
sk a
sses
smen
ts?
g. A
re s
trat
egic
risk
ass
essm
ents
use
d as
the
basi
s fo
r em
erge
ncy
prep
ared
ness
mea
sure
s?
2 D
oes
the
coun
try
have
a n
atio
nal i
nven
tory
and
map
ping
of t
he a
vaila
ble
reso
urce
s fo
r em
erge
ncy
resp
onse
?a.
Doe
s th
is m
appi
ng a
ddre
ss re
sour
ces
and
capa
citie
s re
quire
d fo
r res
pons
e to
all
type
s of
em
erge
ncie
s, in
clud
ing
for p
oten
tial P
HEI
Cs?
b. D
oes
the
map
ping
of r
esou
rces
incl
ude:
i. ex
pert
ise,
ii.
staf
f,iii
. lo
gist
ics,
iv.
equi
pmen
t,v.
fin
ance
, and
vi.
faci
litie
s (e
.g. h
ealth
faci
litie
s, la
bora
torie
s)?
c. W
hen
was
the
last
map
ping
of r
esou
rces
con
duct
ed?
Whi
ch s
ecto
rs p
artic
ipat
ed?
e. W
hat i
s th
e st
atus
of s
tock
pilin
g w
ith re
spec
t to
phar
mac
eutic
als,
pro
tect
ive
equi
pmen
t and
oth
er e
quip
men
t?d.
Are
ass
essm
ents
of t
he s
afet
y an
d fu
nctio
nalit
y of
the
heal
th fa
cilit
ies
for e
mer
genc
ies
incl
uded
in re
sour
ce m
appi
ng?
i. W
hat p
rovi
sion
s ar
e m
ade
with
resp
ect t
o st
ocks
of v
acci
natio
ns, p
re-o
rder
ing/
licen
cing
/im
port
of d
rugs
and
vac
cine
s an
d pr
otec
tive
equi
pmen
t?
R.1.
2 N
atio
nal m
ultis
ecto
ral m
ultih
azar
d em
erge
ncy
prep
ared
ness
mea
sure
s, in
clud
ing
emer
genc
y re
spon
se p
lans
, are
dev
elop
ed, i
mpl
emen
ted
and
test
ed1
Doe
s th
e co
untr
y ha
ve p
lans
and
mec
hani
sms
for
coor
dina
ting
the
deve
lopm
ent
and
impl
emen
tatio
n of
mul
tisec
tora
l m
ultih
azar
d em
erge
ncy
prep
ared
ness
mea
sure
s?
RE
SP
ON
D

INTERNATIONAL HEALTH REGULATIONS (2005)
73 - Joint External Evaluation Tool - Second edition
a.
Doe
s th
e na
tiona
l pla
n an
d m
echa
nism
s fo
r coo
rdin
atin
g em
erge
ncy
prep
ared
ness
hav
e a
mul
tihaz
ard
who
le-o
f-so
ciet
y ap
proa
ch in
volv
ing
all r
elev
ant
sect
ors?
b.
Doe
s th
e he
alth
sec
tor
have
a m
ultih
azar
d pl
an fo
r co
ordi
natin
g em
erge
ncy
prep
ared
ness
mea
sure
s th
at is
inte
grat
ed in
the
mul
tisec
tora
l pla
n? Is
em
erge
ncy
prep
ared
ness
incl
uded
in p
lans
for s
tren
gthe
ning
nat
iona
l em
erge
ncy
and
disa
ster
risk
man
agem
ent?
c.
Doe
s th
e na
tiona
l mul
tisec
tora
l mul
tihaz
ard
plan
incl
ude:
i. st
rate
gic
emer
genc
y ris
k as
sess
men
t,ii.
ca
paci
ty a
sses
smen
ts a
nd re
sour
ce m
appi
ng,
iii.
mul
tihaz
ard
emer
genc
y re
spon
se p
lann
ing
(see
bel
ow fo
r spe
cific
que
stio
ns),
iv.
cont
inge
ncy
plan
ning
for s
peci
fic h
azar
ds o
r ris
k sc
enar
ios,
v.
plan
s fo
r dev
elop
ing
emer
genc
y re
spon
se c
apac
ities
, inc
ludi
ng e
mer
genc
y op
erat
ion
cent
res
(EO
Cs),
vi.
plan
s fo
r dev
elop
ing
surg
e ca
paci
ty,
vii.
busi
ness
con
tinui
ty p
lann
ing
viii.
trai
ning
, and
ix.
exer
cisi
ng?
d.
Doe
s th
e pl
an a
ddre
ss e
mer
genc
y pr
epar
edne
ss f
or IH
R-re
leva
nt h
azar
ds, i
nclu
ding
tho
se t
hat
have
the
pot
entia
l to
caus
e PH
EICs
? D
oes
the
plan
ad
dres
s em
erge
ncy
prep
ared
ness
for a
ll ty
pes
of h
azar
ds th
at th
e co
untr
y fa
ces?
e.
Doe
s th
e pl
an a
ddre
ss th
e m
easu
res
to p
repa
re fo
r any
mas
s ga
ther
ing
even
ts?
f. D
oes
the
plan
cle
arly
ass
ign
role
s an
d re
spon
sibi
litie
s fo
r em
erge
ncy
prep
ared
ness
to s
peci
fic g
over
nmen
t uni
ts o
f all
rele
vant
sec
tors
and
poi
nts
of
entr
y?g.
Ar
e th
ere
plan
s fo
r str
engt
heni
ng e
mer
genc
y pr
epar
edne
ss a
t sub
natio
nal a
nd lo
cal l
evel
s?h.
Ar
e th
ere
dedi
cate
d hu
man
res
ourc
es a
nd r
egul
ar b
udge
t fu
ndin
g fo
r em
erge
ncy
prep
ared
ness
mea
sure
s by
pub
lic h
ealth
, ani
mal
hea
lth a
nd o
ther
re
leva
nt s
ecto
rs?
Are
hum
an re
sour
ces
brie
fed
and
trai
ned
in th
eir r
ole
and
resp
onsi
bilit
ies?
i. W
hen
was
the
natio
nal p
lan
deve
lope
d? W
hen
was
the
last
upd
ate?
2.
Doe
s th
e co
untr
y ha
ve m
ultis
ecto
ral m
ultih
azar
d em
erge
ncy
resp
onse
pla
ns?
a. D
oes
the
natio
nal h
ealth
em
erge
ncy
resp
onse
pla
n ha
ve a
mul
tihaz
ard
who
le-o
f-so
ciet
y ap
proa
ch in
volv
ing
all r
elev
ant s
ecto
rs?
Whe
n w
as th
e pl
an
deve
lope
d? W
hen
was
the
plan
last
upd
ated
?b.
Is
the
heal
th s
ecto
r’s e
mer
genc
y re
spon
se p
lan
inte
grat
ed in
the
mul
tisec
tora
l pla
n?c.
Is
the
natio
nal m
ultis
ecto
ral m
ultih
azar
d re
spon
se p
lan
base
d on
str
ateg
ic e
mer
genc
y ris
k as
sess
men
t, ca
paci
ty a
sses
smen
ts a
nd re
sour
ce m
appi
ng?
d. D
oes
the
emer
genc
y re
spon
se p
lan
inco
rpor
ate
IHR-
rele
vant
haz
ards
, inc
ludi
ng th
ose
that
hav
e th
e po
tent
ial t
o ca
use
PHEI
Cs?
Doe
s th
e re
spon
se p
lan
addr
ess
all t
ypes
of e
mer
genc
ies
that
the
coun
try
face
s?
e. H
ave
cont
inge
ncy
plan
s be
en d
evel
oped
for h
igh
prio
rity
risks
/spe
cific
eve
nts?
Are
they
bas
ed o
n st
rate
gic
risk
asse
ssm
ents
and
reso
urce
map
ping
?
5 -
Surg
e ca
paci
ty is
defi
ned
as th
e ab
ility
to in
crea
se (o
r con
serv
e) re
sour
ces
in a
n em
erge
ncy
situ
atio
n. S
urge
cap
acity
is o
ften
dep
loye
d ra
pidl
y w
hen
rout
ine
oper
atin
g ca
paci
ties
are
insu
ffici
ent t
o de
al w
ith th
e in
crea
sed
dem
and
for r
esou
rces
in a
n em
erge
ncy.
Res
ourc
es in
clud
e pe
rson
nel,
equi
pmen
t, su
pplie
s, fi
nanc
es, a
mon
g ot
hers
. A s
urge
pla
n fo
r sca
ling
up re
spon
se o
pera
tions
sho
uld
be in
clud
ed in
the
natio
nal m
ultis
ecto
ral m
ultih
azar
d re
spon
se
plan
s.
RE
SP
ON
D

INTERNATIONAL HEALTH REGULATIONS (2005)
74 - Joint External Evaluation Tool - Second edition
f. D
oes
the
plan
cle
arly
ass
ign
role
s an
d re
spon
sibi
litie
s fo
r em
erge
ncy
resp
onse
to s
peci
fic g
over
nmen
t uni
ts o
f all
rele
vant
sec
tors
and
poi
nts
of e
ntry
?g.
Doe
s th
e pl
an in
corp
orat
e SO
Ps th
at d
escr
ibe
the
proc
edur
es fo
r act
ivat
ing
and
impl
emen
ting
the
plan
for a
ll ke
y re
spon
se m
anag
emen
t and
tech
nica
l fu
nctio
ns in
rele
vant
sec
tors
(suc
h as
hea
lth, e
mer
genc
y m
anag
emen
t, an
imal
hea
lth, c
hem
ical
s, ra
diat
ion
and
any
mas
s ga
ther
ing
even
ts)?
h. A
re th
ere
emer
genc
y or
con
tinge
ncy
fund
s re
adily
ava
ilabl
e to
sup
port
resp
onse
by
publ
ic h
ealth
, ani
mal
hea
lth a
nd o
ther
rele
vant
sec
tors
?i.
Doe
s th
e pl
an a
naly
se a
vaila
ble
reso
urce
s (s
uch
as h
uman
reso
urce
s, e
quip
men
t, fa
cilit
ies)
in re
latio
n to
the
need
for r
egul
ar o
pera
tion
mod
e, fo
r acu
te
emer
genc
ies,
and
pro
trac
ted
cris
es?
j. Is
a s
urge
pla
n in
clud
ed in
the
natio
nal m
ultis
ecto
ral m
ultih
azar
d re
spon
se p
lans
for s
calin
g up
resp
onse
ope
ratio
ns?
k. W
hat i
s th
e m
echa
nism
to a
ddre
ss re
sour
ce g
aps?
Doe
s th
e pl
an in
clud
e SO
Ps fo
r dep
loym
ent o
f sur
ge c
apac
ity?
l. Is
sur
ge c
apac
ity a
vaila
ble
to re
spon
d to
em
erge
ncie
s, in
clud
ing
publ
ic h
ealth
em
erge
ncie
s of
nat
iona
l and
inte
rnat
iona
l con
cern
? m
. Are
ther
e m
ultih
azar
d em
erge
ncy
resp
onse
pla
ns a
t sub
natio
nal a
nd lo
cal l
evel
s?n.
Doe
s th
e na
tiona
l em
erge
ncy
resp
onse
pla
n de
scrib
e th
e pr
oced
ures
and
pla
ns to
relo
cate
or m
obili
ze re
sour
ces
from
nat
iona
l and
inte
rmed
iate
leve
ls
to s
uppo
rt re
spon
se a
t the
loca
l lev
el?
Wha
t are
thos
e pr
oced
ures
and
pla
ns?
o. D
oes
the
natio
nal e
mer
genc
y re
spon
se p
lan
incl
ude
logi
stic
s? W
hat r
esou
rces
are
ava
ilabl
e fo
r log
istic
s?
p. H
as th
e na
tiona
l res
pons
e pl
an b
een
impl
emen
ted
in a
real
eve
nt o
r tes
ted
in a
sim
ulat
ion
exer
cise
? W
hen
was
the
last
tim
e it
was
use
d? W
as th
e pl
an
upda
ted
as a
resu
lt of
an
afte
r-ac
tion
revi
ew o
r oth
er fo
rm o
f eva
luat
ion?
q. H
ave
subn
atio
nal a
nd lo
cal m
ultih
azar
d em
erge
ncy
resp
onse
pla
ns b
een
impl
emen
ted
in a
real
eve
nt o
r tes
ted
in a
sim
ulat
ion
exer
cise
? W
hen
was
the
last
tim
e th
ese
wer
e us
ed?
Wer
e pl
ans
upda
ted
as a
resu
lt of
an
afte
r-ac
tion
revi
ew o
r oth
er fo
rm o
f eva
luat
ion?
r. H
ave
natio
nal c
ontin
genc
y pl
ans
been
impl
emen
ted
in a
real
eve
nt o
r tes
ted
in a
sim
ulat
ion
exer
cise
? W
hen
was
the
last
tim
e it
was
use
d? W
ere
the
plan
s up
date
d as
a re
sult
of a
n af
ter-
actio
n re
view
or o
ther
form
of e
valu
atio
n?s.
Wha
t are
the
key
findi
ngs
of th
e af
ter-
actio
n re
view
s or
eva
luat
ions
of e
mer
genc
y re
spon
se o
pera
tion
or S
WO
T (s
tren
gths
, wea
knes
ses,
opp
ortu
nitie
s,
thre
ats
anal
ysis
) exe
rcis
e?
Refe
renc
es:
l
Send
ai F
ram
ewor
k in
dica
tors
. Pr
even
tionW
eb [
web
site
] (h
ttp:
//w
ww
.pre
vent
ionw
eb.n
et/d
rr-f
ram
ewor
k/se
ndai
-fra
mew
ork-
mon
itor/
indi
cato
rs,
acce
ssed
27
Dec
embe
r 201
7).
l
The
Send
ai F
ram
ewor
k fo
r D
isas
ter
Risk
Red
uctio
n 20
15–
2030
. Gen
eva:
Uni
ted
Nat
ions
Offi
ce o
f D
isas
ter
Risk
Red
uctio
n; 2
015
(htt
p://
ww
w.u
nisd
r.org
/fil
es/4
3291
_sen
daifr
amew
orkf
ordr
ren.
pdf,
acce
ssed
27
Dec
embe
r 201
7).
l
A st
rate
gic
fram
ewor
k fo
r em
erge
ncy
prep
ared
ness
. G
enev
a:
Wor
ld
Hea
lth
Org
aniz
atio
n;
2017
(h
ttp:
//ap
ps.w
ho.in
t/iri
s/bi
tstr
eam
/106
65/
2548
83/1
/978
9241
5118
27-e
ng.p
df?u
a=1,
acc
esse
d 28
Dec
embe
r 201
7).
l
Inte
rage
ncy
Stan
ding
Com
mitt
ee (
IASC
) Em
erge
ncy
Resp
onse
Pre
pare
dnes
s G
uide
lines
Jul
y 20
15 -
add
ress
es R
isk
Anal
ysis
and
Mon
itorin
g M
inim
um
Prep
ared
ness
Act
ions
, Adv
ance
d Pr
epar
edne
ss A
ctio
ns a
nd C
ontin
genc
y Pl
anni
ng (
http
s://
inte
rage
ncys
tand
ingc
omm
ittee
.org
/sys
tem
/file
s/em
erge
ncy_
resp
onse
_pre
pare
dnes
s_20
15_fi
nal.p
df a
cces
sed
30 D
ecem
ber 2
017)
RE
SP
ON
D

INTERNATIONAL HEALTH REGULATIONS (2005)
75 - Joint External Evaluation Tool - Second edition
EMER
GEN
CY R
ESPO
NSE
OPE
RATI
ON
S Ta
rget
s: C
ount
ries
will
hav
e a
coor
dina
tion
mec
hani
sm, i
ncid
ent
man
agem
ent
syst
ems,
exe
rcis
e m
anag
emen
t pr
ogra
mm
es a
nd p
ublic
hea
lth e
mer
genc
y op
erat
ion
cent
re (E
OC)
func
tioni
ng a
ccor
ding
to m
inim
um c
omm
on s
tand
ards
; mai
ntai
ning
trai
ned,
func
tioni
ng, m
ultis
ecto
ral r
apid
resp
onse
team
s, a
nd tr
aine
d EO
C st
aff c
apab
le o
f act
ivat
ing
a co
ordi
nate
d em
erge
ncy
resp
onse
with
in 1
20 m
inut
es o
f the
iden
tifica
tion
of a
n em
erge
ncy.
As m
easu
red
by: (
1) E
stab
lishm
ent o
f an
emer
genc
y re
spon
se c
oord
inat
ion
mec
hani
sm o
r inc
iden
t man
agem
ent s
yste
m. (
2) D
evel
opm
ent o
f nat
iona
l hea
lth E
OC
plan
s an
d pr
oced
ures
. (3)
Em
erge
ncy
resp
onse
sys
tem
s an
d de
cisi
on-m
akin
g ha
ve b
een
test
ed a
nd o
pera
ting
effic
ient
ly a
nd e
ffect
ivel
y.
Desi
red
impa
ct: E
ffect
ive
coor
dina
tion
and
impr
oved
man
agem
ent
of t
he r
espo
nse
to o
utbr
eaks
and
em
erge
ncie
s as
evi
denc
ed b
y sh
orte
r tim
es f
rom
ear
ly
war
ning
and
det
ectio
n to
act
ivat
ion
of re
spon
se p
lans
; im
plem
enta
tion
of a
coo
rdin
ated
mul
tisec
tora
l res
pons
e ac
ross
all
leve
ls; a
nd s
mal
ler n
umbe
rs o
f cas
es,
deat
hs a
nd o
ther
hea
lth a
nd s
ocie
tal i
mpa
cts.
RE
SP
ON
D

INTERNATIONAL HEALTH REGULATIONS (2005)
76 - Joint External Evaluation Tool - Second edition
Scor
eIn
dica
tors
– E
mer
genc
y re
spon
se o
pera
tions
R.
2.1
Emer
genc
y re
spon
se c
oord
inat
ion1
R.2.
22 Em
erge
ncy
oper
atio
ns c
entr
e (E
OC)
3 ca
paci
ties,
pro
cedu
res
and
plan
sR.
2.3
Emer
genc
y ex
erci
se4 m
anag
emen
t pr
ogra
mm
e5
No
capa
city
- 1
An e
mer
genc
y re
spon
se c
oord
inat
ion
mec
hani
sm
is n
ot a
vaila
ble
An E
OC
has
not b
een
iden
tified
and
no
EOC
plan
s/pr
oced
ures
are
in p
lace
No
exer
cise
s ha
ve b
een
com
plet
ed in
the
past
five
ye
ars
Lim
ited
ca
paci
ty -
2
A na
tiona
l hea
lth s
ecto
r em
erge
ncy
resp
onse
ope
-ra
tion
poin
t of c
onta
ct is
ava
ilabl
e 24
/7 b
ut th
ere
is n
o fo
rmal
em
erge
ncy
coor
dina
tion
mec
hani
sm
Nat
iona
l EO
Cs o
r equ
ival
ent s
truc
ture
s ar
e es
ta-
blis
hed
on a
n ad
hoc
bas
is in
resp
onse
to e
mer
-ge
ncie
s
Tabl
e to
p ex
erci
ses
have
bee
n co
mpl
eted
in th
e pa
st fi
ve y
ears
to te
st e
mer
genc
y re
spon
se c
apa-
bilit
ies
and
deci
sion
mak
ing
at th
e na
tiona
l lev
el
Deve
lope
d ca
paci
ty -
3
A he
alth
sec
tor e
mer
genc
y re
spon
se c
oord
inat
ion
mec
hani
sm fo
r em
erge
ncie
s in
clud
ing
PHEI
Cs
(e.g
. em
erge
ncy
resp
onse
com
mitt
ee) i
s in
pla
ce
Nat
iona
l EO
Cs o
r equ
ival
ent s
truc
ture
s ar
e es
ta-
blis
hed
on a
n ad
hoc
bas
is in
resp
onse
to e
mer
-ge
ncie
sEO
Cs a
re n
ot y
et c
apab
le o
f act
ivat
ing
a co
ordi
-na
ted
emer
genc
y re
spon
se w
ithin
120
min
utes
of
rece
ivin
g an
ear
ly w
arni
ng o
r inf
orm
atio
n of
an
emer
genc
y re
quiri
ng E
OC
activ
atio
n
A fu
nctio
nal e
xerc
ise
has
been
com
plet
ed to
test
re
spon
se o
pera
tions
cap
abili
ties
at th
e na
tiona
l le
vel,
or n
atio
nal h
ealth
resp
onse
sys
tem
s ha
ve
been
act
ivat
ed to
resp
ond
to a
maj
or e
mer
genc
y in
th
e pa
st tw
o ye
ars
Dem
onst
rate
d ca
paci
ty -
4
Ther
e ar
e em
erge
ncy
resp
onse
co
ordi
natio
n m
echa
nism
s at
the
subn
atio
nal a
nd lo
cal l
evel
sEm
erge
ncy
resp
onse
coo
rdin
atio
n m
echa
nism
at
the
natio
nal l
evel
has
bee
n te
sted
and
upd
ated
in
the
past
two
year
s
Nat
iona
l EO
Cs c
an b
e ac
tivat
ed w
ithin
120
min
utes
of
rec
eivi
ng a
n ea
rly w
arni
ng o
r in
form
atio
n of
an
emer
genc
y re
quiri
ng E
OC
activ
atio
nEO
C pl
ans,
act
ivat
ion
and
func
tions
at t
he n
atio
nal
leve
l hav
e be
en te
sted
and
upd
ated
in th
e pa
st tw
o ye
ars
EOCs
are
ava
ilabl
e at
the
sub
natio
nal
leve
l w
ith
plan
s an
d SO
Ps, r
esou
rces
and
sta
ff tr
aine
d in
EO
C SO
Ps
A co
mbi
natio
n of
exe
rcis
es is
con
duct
ed a
t le
ast
annu
ally
to
test
em
erge
ncy
resp
onse
cap
abili
ties
at n
atio
nal l
evel
with
the
invo
lvem
ent o
f sub
natio
-na
l lev
els
Sust
aina
ble
capa
city
- 5
Emer
genc
y re
spon
se c
oord
inat
ion
mec
hani
sms
at
all l
evel
s ha
ve b
een
test
ed a
nd u
pdat
ed in
the
past
tw
o ye
ars
EOC
func
tions
at
all
leve
ls h
ave
been
tes
ted
and
upda
ted
regu
larly
EOC
oper
atio
ns c
an b
e su
stai
ned
for l
arge
sca
le o
r co
ncur
rent
em
erge
ncie
s du
e to
a n
etw
ork
of f
ul-
ly f
unct
iona
l em
erge
ncy
oper
atio
ns c
entr
es a
nd
trai
ned
staf
f
A co
mbi
natio
n of
exe
rcis
es a
re c
ondu
cted
at l
east
an
nual
ly t
o te
st e
mer
genc
y re
spon
se c
apab
ilitie
s at
all
leve
lsFo
llow
ing
exer
cise
s, c
orre
ctiv
e ac
tion
plan
s to
up-
date
pla
ns a
nd s
tren
gthe
n ca
paci
ties
wer
e de
ve-
lope
d an
d im
plem
ente
d
1 -
Emer
genc
y re
spon
se c
oord
inat
ion
mec
hani
sms
may
em
ploy
an
inci
dent
man
agem
ent s
yste
m to
fulfi
l the
coo
rdin
atio
n fu
nctio
n.2
- Th
e in
dica
tor r
efer
s to
pub
lic h
ealth
em
erge
ncy
oper
atio
ns a
nd h
ealth
EO
Cs fo
r the
cou
ntry
.
RE
SP
ON
D

INTERNATIONAL HEALTH REGULATIONS (2005)
77 - Joint External Evaluation Tool - Second edition
Not
e:
Ther
e is
crit
ical
com
pete
ncy
in th
e PV
S to
ol C
C II-
6: E
mer
genc
y re
spon
se.
Cont
extu
al q
uest
ions
:
1.
Dur
ing
an e
mer
genc
y, is
ther
e a
proc
ess
for s
harin
g sc
ient
ific
data
and
reco
mm
enda
tions
with
pol
icy
mak
ers
and
natio
nal l
eade
rs?
2.
Is th
ere
a m
ultis
ecto
ral c
omm
issi
on o
r a m
ultid
isci
plin
ary
emer
genc
y co
ordi
natio
n de
part
men
t or u
nit f
or p
ublic
hea
lth/a
nim
al h
ealth
? a.
If y
es, d
oes
this
incl
ude
secu
rity,
publ
ic h
ealth
, vet
erin
ary,
wild
life
and
othe
r exp
erts
? b.
Has
this
team
rece
ived
pub
lic c
omm
unic
atio
n tr
aini
ng?
c. H
ow o
ften
do
thes
e gr
oups
mee
t to
disc
uss
cros
s-cu
ttin
g is
sues
? 3.
H
ow d
o su
bnat
iona
l (in
term
edia
te a
nd lo
cal)
entit
ies
man
age
emer
genc
y re
spon
se a
ctiv
ities
?a.
Is
ther
e a
role
for p
ublic
hea
lth, o
r is
this
an
emer
genc
y m
anag
emen
t act
ivity
?4.
H
ow d
o lo
calit
ies
man
age
emer
genc
y re
spon
se a
ctiv
ities
? a.
Is
ther
e a
role
for p
ublic
hea
lth o
r do
othe
r ent
ities
(suc
h as
repr
esen
tativ
es fr
om n
atio
nal d
isas
ter m
anag
emen
t boa
rd) m
anag
e it?
5.
Is th
ere
a ho
tline
that
peo
ple/
clin
icia
ns c
an c
all f
or h
elp
on h
andl
ing
a di
seas
e of
unk
now
n or
igin
? a.
Is
ther
e a
com
para
ble
syst
em fo
r ani
mal
dis
ease
sup
port
?
Tech
nica
l que
stio
ns:
R2.1
Em
erge
ncy
resp
onse
coo
rdin
atio
n 1.
D
escr
ibe
scen
ario
s or
trig
gers
for a
ctiv
atio
n of
em
erge
ncy
resp
onse
. Are
ther
e m
ultip
le le
vels
of e
mer
genc
y re
spon
se a
ctiv
atio
n?a.
Who
dec
ides
the
chan
ge o
f lev
el?
b. I
s th
ere
a na
tiona
l poi
nt o
f con
tact
ava
ilabl
e fo
r 24/
7 co
vera
ge o
f em
erge
ncy
oper
atio
ns?
c. I
s th
ere
a na
tiona
l hea
lth s
ecto
r em
erge
ncy
resp
onse
coo
rdin
atio
n m
echa
nism
, com
mitt
ee o
r nat
iona
l hea
lth E
OC?
3 -
EOC
• The
nat
iona
l hea
lth E
OCs
are
net
wor
ked
with
hea
lth E
OCs
at s
ubna
tiona
l and
loca
l lev
els,
and
are
inte
rope
rabl
e w
ith E
OCs
in o
ther
sec
tors
, inc
ludi
ng w
ith th
e N
atio
nal D
isas
ter M
anag
emen
t Offi
ce.
- EO
C pl
ans
and
SOPs
des
crib
e ke
y st
ruct
ural
and
ope
ratio
nal e
lem
ents
; for
ms
and
tem
plat
es fo
r EO
C da
ta m
anag
emen
t, re
port
ing
and
brie
fing;
role
des
crip
tions
and
job
aids
for E
OC
func
tiona
l pos
ition
s (in
clud
ing
inci
dent
m
anag
emen
t or c
omm
and,
ope
ratio
ns, p
lann
ing,
logi
stic
s an
d fin
ance
) and
reso
urce
s in
clud
ing
info
rmat
ion
syst
ems
to c
onne
ct p
ublic
hea
lth d
ecis
ion
mak
ers
to a
ppro
pria
te d
ata
sour
ces;
- co
mm
unic
atio
ns e
quip
men
t; an
d-
staf
f tha
t are
trai
ned
and
capa
ble
of c
oord
inat
ing
an e
mer
genc
y re
spon
se.
• Nat
iona
l hea
lth E
OC
plan
s ar
e in
pla
ce fo
r fun
ctio
ns in
clud
ing
publ
ic h
ealth
sci
ence
(epi
dem
iolo
gy, m
edic
al a
nd o
ther
sub
ject
mat
ter e
xper
tise)
, pub
lic c
omm
unic
atio
ns a
nd p
artn
er li
aiso
n.• T
here
are
add
ition
al tr
aine
d st
aff w
ho c
an s
uppo
rt a
nd re
plac
e re
gula
r EO
C st
aff o
n a
rota
tiona
l bas
is.
4 -
Exer
cise
s sh
ould
tes
t th
e ca
paci
ty o
f th
e em
erge
ncy
oper
atio
ns s
yste
ms
and
staf
f to
coo
rdin
ate
a la
rge
resp
onse
to
affe
ct m
ultip
le c
omm
uniti
es, b
y in
volv
ing
mul
tisec
tora
l coo
rdin
atio
n an
d m
ass
gath
erin
g ev
ents
whe
re
appr
opria
te.
5 -
Func
tiona
l mul
tisec
tora
l exe
rcis
es s
houl
d be
hel
d on
an
annu
al b
asis
exc
ept w
hen
the
coun
try
has
cond
ucte
d m
ajor
em
erge
ncy
resp
onse
ope
ratio
ns w
hich
hav
e te
sted
the
syst
em in
a re
al e
vent
; add
ition
al d
rills
, tab
le to
p ex
erci
ses
and
sim
ulat
ions
can
sup
plem
ent t
he fu
nctio
nal e
xerc
ises
.
RE
SP
ON
D

INTERNATIONAL HEALTH REGULATIONS (2005)
78 - Joint External Evaluation Tool - Second edition
d. I
s th
ere
a de
dica
ted
coor
dina
tion
mec
hani
sm u
nder
the
natio
nal h
ealth
EO
C fo
r act
ivat
ion
and
coor
dina
tion
of e
mer
genc
y m
edic
al te
ams
(EM
Ts) (
such
as
a E
MT
Coor
dina
tion
Cell)
?e.
Is
ther
e an
inci
dent
man
agem
ent s
yste
m in
the
heal
th s
ecto
r at t
he n
atio
nal l
evel
?f.
Are
ther
e he
alth
sec
tor e
mer
genc
y re
spon
se c
oord
inat
ion
mec
hani
sms,
com
mitt
ees
or h
ealth
EO
Cs a
t sub
natio
nal l
evel
s?g.
Is
ther
e an
inci
dent
man
agem
ent s
yste
m in
the
heal
th s
ecto
r at t
he n
atio
nal l
evel
? An
d at
sub
natio
nal l
evel
s?h.
Des
crib
e ho
w h
ealth
sec
tor s
taff
have
bee
n tr
aine
d on
em
erge
ncy
oper
atio
ns p
roce
dure
s. H
as th
ere
been
any
inci
dent
man
agem
ent s
yste
ms
trai
ning
at
natio
nal o
r sub
natio
nal l
evel
s?i.
How
are
sur
ge s
taff
for
emer
genc
y re
spon
se c
oord
inat
ion
iden
tified
? Is
the
re a
ros
ter
of s
taff?
Is t
rain
ing
avai
labl
e to
sur
ge s
taff
in a
dvan
ce o
f a
resp
onse
? Is
ther
e “ju
st in
tim
e” tr
aini
ng a
vaila
ble?
R.2.
2 Em
erge
ncy
oper
atio
ns c
entr
e (E
OC)
cap
aciti
es, p
roce
dure
s an
d pl
ans
1.
Des
crib
e th
e he
alth
EO
C at
the
natio
nal l
evel
(the
se q
uest
ions
are
to b
e an
swer
ed w
heth
er th
ere
is a
per
man
ent E
OC,
tem
pora
ry E
OC
or v
irtua
l EO
C).
a. I
f the
re is
a d
edic
ated
EO
C (p
hysi
cal),
pro
vide
a fl
oor p
lan
and
desc
riptio
n of
equ
ipm
ent.
b. W
hat i
s th
e to
tal s
taff
capa
city
for t
he E
OC?
Is th
ere
a pl
an in
pla
ce to
acc
omm
odat
e ad
ditio
nal s
taff
if ne
cess
ary?
c. I
s th
ere
a re
liabl
e po
wer
sou
rce
for t
he E
OC?
d. I
s th
ere
a re
liabl
e co
mm
unic
atio
ns s
truc
ture
for t
he E
OC?
Doe
s th
is in
clud
e In
tern
et, e
mai
l and
pho
ne c
apab
ilitie
s?e.
Is
the
orga
niza
tion
able
to
conv
ene
part
icip
ants
fro
m m
inis
trie
s an
d ag
enci
es o
f al
l rel
evan
t se
ctor
s an
d ot
her
natio
nal a
nd m
ultin
atio
nal p
artn
ers
as
appr
opria
te?
2.
Des
crib
e th
e pl
ans
and
SOPs
that
are
in p
lace
for t
he E
OC.
a. A
re th
e pl
ans
and
proc
edur
es b
ased
on
an in
cide
nt m
anag
emen
t sys
tem
? D
o th
ey in
clud
e th
e fo
llow
ing
func
tions
and
reso
urce
s:i.
in
cide
nt c
omm
and,
ii.
oper
atio
ns,
iii.
plan
ning
,iv
. lo
gist
ics,
and
v.
finan
ce?
b. W
hen
ther
e is
a n
atio
nal e
mer
genc
y, w
ho s
erve
s as
the
“inci
dent
man
ager
” for
the
heal
th E
OC?
c. I
s th
ere
a pr
oced
ure
in p
lace
for d
ecis
ion
mak
ing
in th
e EO
C?d.
Doe
s th
e na
tiona
l he
alth
EO
C pl
an i
nclu
de r
oles
for
pub
lic h
ealth
sci
ence
(ep
idem
iolo
gy,
med
ical
and
oth
er s
ubje
ct m
atte
r ex
pert
ise)
, pu
blic
co
mm
unic
atio
ns, p
artn
er li
aiso
n?e.
How
oft
en a
re th
ese
proc
edur
es u
pdat
ed?
Whe
n w
as th
e la
st ti
me
they
wer
e up
date
d?f.
How
are
EO
C re
cord
s an
d pr
oced
ures
mai
ntai
ned
and
dist
ribut
ed?
3.
How
long
afte
r the
rece
ipt o
f an
early
war
ning
or i
nfor
mat
ion
does
it ta
ke fo
r the
act
ivat
ion
of th
e EO
C?
a.
How
man
y tim
es w
as th
e EO
C ac
tivat
ed in
the
past
five
yea
rs?
4.
Are
ther
e su
bnat
iona
l hea
lth E
OCs
with
sta
ff w
ho a
re tr
aine
d in
em
erge
ncy
man
agem
ent a
nd E
OC
SOPs
?
RE
SP
ON
D
INTERNATIONAL HEALTH REGULATIONS (2005)
79 - Joint External Evaluation Tool - Second edition
5.
How
ofte
n ar
e exe
rcis
es co
nduc
ted
to te
st n
atio
nal E
OC a
ctiv
atio
n an
d ne
twor
king
with
subn
atio
nal a
nd m
ultis
ecto
ral E
OCs?
Whe
n w
as th
e las
t tim
e thi
s hap
pene
d?6.
D
escr
ibe
role
s fo
r sta
ff th
at h
ave
been
iden
tified
for E
OC
func
tions
. Are
ther
e ro
le d
escr
iptio
ns a
nd jo
b ai
ds fo
r nat
iona
l EO
C fu
nctio
nal p
ositi
ons?
7.
Des
crib
e ho
w s
taff
have
bee
n tr
aine
d fo
r the
ir ro
le in
EO
Cs?
a. I
s th
ere
a tr
aini
ng p
rogr
amm
e fo
r EO
C st
aff?
b.
How
are
EO
C su
rge
staf
f ide
ntifi
ed?
Is th
ere
trai
ning
ava
ilabl
e to
EO
C su
rge
staf
f in
adva
nce
of a
resp
onse
? Is
ther
e “ju
st in
tim
e” tr
aini
ng a
vaila
ble?
8.
Doe
s th
e EO
C us
e st
anda
rdiz
ed fo
rms
and
tem
plat
es fo
r dat
a/in
form
atio
n m
anag
emen
t, re
port
ing,
brie
fing,
etc
.?9.
D
escr
ibe
the
avai
labi
lity/
diss
emin
atio
n of
situ
atio
nal a
war
enes
s re
port
s fro
m h
ealth
EO
C fo
r diff
eren
t tar
get g
roup
s.
R.2.
3 Em
erge
ncy
exer
cise
man
agem
ent p
rogr
amm
e1.
D
escr
ibe
heal
th e
mer
genc
y ex
erci
ses
that
hav
e be
en c
ondu
cted
, and
any
act
ivat
ion
of th
e em
erge
ncy
resp
onse
ope
ratio
ns fo
r rea
l eve
nts
in th
e pa
st fi
ve y
ears
.a.
Des
crib
e fu
nctio
nal e
xerc
ises
that
hav
e be
en c
ompl
eted
at n
atio
nal o
r sub
natio
nal l
evel
s in
the
past
two
year
s.b.
Des
crib
e ta
ble
top
exer
cise
s th
at h
ave
been
com
plet
ed a
t nat
iona
l or s
ubna
tiona
l lev
els
in th
e pa
st tw
o ye
ars.
c. D
escr
ibe
any
emer
genc
y re
spon
se a
ctiv
atio
ns a
t the
nat
iona
l lev
el in
the
past
two
year
s.d.
Pro
vide
a s
umm
ary
of a
ny im
prov
emen
t pla
ns, a
fter
-act
ion
repo
rts,
or l
esso
ns le
arne
d do
cum
ents
that
wer
e co
mpl
eted
as
a re
sult
of th
ese
exer
cise
s or
re
al e
mer
genc
y re
spon
se o
pera
tions
. Wha
t act
ion
has
been
take
n to
impl
emen
t the
reco
mm
ende
d ac
tions
?
Doc
umen
tatio
n or
evi
denc
e fo
r lev
el o
f cap
abili
ty:
l
Plan
s of
the
EOC,
and
list
ing
of a
vaila
ble
equi
pmen
tl
Trai
ning
pla
ns fo
r em
erge
ncy
oper
atio
ns s
taff
l
Exer
cise
pla
n, in
clud
ing
eval
uatio
n an
d co
rrec
tive
actio
n pl
an, i
f ava
ilabl
el
Activ
atio
n pl
an fo
r em
erge
ncy
resp
onse
, suc
h as
rost
er o
f em
erge
ncy
oper
atio
ns s
taff
and
role
Refe
renc
es:
l
Publ
ic H
ealth
Em
erge
ncy
Ope
ratio
ns C
entr
e N
etw
ork
(EO
C-N
ET).
Wor
ld H
ealth
Org
aniz
atio
n [w
ebsi
te]
(htt
p://
ww
w.w
ho.in
t/ih
r/eo
c_ne
t/en
/, ac
cess
ed
29 N
ovem
ber 2
017)
.l
Send
ai F
ram
ewor
k in
dica
tors
. Pre
vent
ionW
eb [w
ebsi
te] (
http
://w
ww
.pre
vent
ionw
eb.n
et/d
rr-f
ram
ewor
k/se
ndai
-fra
mew
ork-
mon
itor/
indi
cato
rs, a
cces
sed
23 D
ecem
ber 2
017)
.l
The
Send
ai F
ram
ewor
k fo
r Dis
aste
r Ris
k Re
duct
ion
2015
–20
30. G
enev
a: U
nite
d N
atio
ns O
ffice
of D
isas
ter R
isk
Redu
ctio
n; 2
015
(htt
p://
ww
w.u
nisd
r.org
/fil
es/4
3291
_sen
daifr
amew
orkf
ordr
ren.
pdf,
acce
ssed
27
Dec
embe
r 201
7).
RE
SP
ON
D

INTERNATIONAL HEALTH REGULATIONS (2005)
80 - Joint External Evaluation Tool - Second edition
LIN
KIN
G P
UBL
IC H
EALT
H A
ND
SEC
URI
TY A
UTH
ORI
TIES
Ta
rget
: Cou
ntry
con
duct
s a
rapi
d, m
ultis
ecto
ral r
espo
nse1 f
or a
ny e
vent
of s
uspe
cted
or c
onfir
med
del
iber
ate
orig
in, i
nclu
ding
the
capa
city
to li
nk p
ublic
hea
lth
and
law
enf
orce
men
t, an
d to
pro
vide
tim
ely
inte
rnat
iona
l ass
ista
nce.
As m
easu
red
by: E
vide
nce
of a
t lea
st o
ne re
spon
se, i
n th
e pr
evio
us y
ear,
that
effe
ctiv
ely
links
pub
lic h
ealth
and
law
enf
orce
men
t, or
a fo
rmal
exe
rcis
e or
sim
ulat
ion
invo
lvin
g le
ader
ship
from
the
coun
try’
s pu
blic
hea
lth a
nd la
w e
nfor
cem
ent c
omm
uniti
es.
Desi
red
impa
ct: D
evel
opm
ent a
nd im
plem
enta
tion
of a
MoU
or o
ther
sim
ilar f
ram
ewor
k ou
tlini
ng ro
les,
resp
onsi
bilit
ies
and
best
pra
ctic
es fo
r sha
ring
rele
vant
in
form
atio
n be
twee
n an
d am
ong
appr
opria
te h
uman
and
ani
mal
hea
lth, l
aw e
nfor
cem
ent
and
defe
nce
pers
onne
l, an
d va
lidat
ion
of t
he M
oU t
hrou
gh p
erio
dic
exer
cise
s an
d si
mul
atio
ns. C
ount
ries
will
dev
elop
and
impl
emen
t m
odel
sys
tem
s to
con
duct
and
sup
port
join
t ep
idem
iolo
gica
l and
crim
inal
inve
stig
atio
ns t
o id
entif
y an
d re
spon
d to
sus
pect
ed b
iolo
gica
l, ch
emic
al o
r rad
iolo
gica
l inc
iden
ts o
f del
iber
ate
orig
in in
col
labo
ratio
n w
ith in
divi
dual
Bio
logi
cal a
nd T
oxin
Wea
pons
Co
nven
tion
(BTW
C) o
f Sta
tes
Part
ies,
FAO
, Int
erna
tiona
l Ato
mic
Ene
rgy
Agen
cy (I
AEA)
, Int
erna
tiona
l Crim
inal
Pol
ice
Org
aniz
atio
n (IN
TERP
OL)
, OIE
, Org
anis
atio
n fo
r the
Pro
hibi
tion
of C
hem
ical
Wea
pons
(OPC
W),
the
Uni
ted
Nat
ions
Sec
reta
ry-G
ener
al’s
Mec
hani
sm fo
r Inv
estig
atio
n of
Alle
ged
Use
of C
hem
ical
and
Bio
logi
cal
Wea
pons
, WH
O a
nd o
ther
rele
vant
regi
onal
and
inte
rnat
iona
l org
aniz
atio
ns a
s ap
prop
riate
. . 1
- M
ultis
ecto
ral c
olla
bora
tion
is k
ey t
o en
gagi
ng in
an
effe
ctiv
e pu
blic
hea
lth e
mer
genc
y re
spon
se. S
ecur
ity a
utho
ritie
s m
ay in
clud
e la
w e
nfor
cem
ent,
bord
er c
ontr
ol o
ffice
rs, d
efen
ce a
nd/o
r cu
stom
s en
forc
emen
t. Ef
fect
ive
mul
tisec
tora
l col
labo
ratio
n sh
ould
als
o in
clud
e fo
od s
afet
y in
spec
tors
, as
wel
l as
anim
al h
ealth
, rad
iolo
gica
l saf
ety
and
chem
ical
saf
ety
auth
oriti
es.
RE
SP
ON
D

INTERNATIONAL HEALTH REGULATIONS (2005)
81 - Joint External Evaluation Tool - Second edition
Scor
eIn
dica
tor:
Link
ing
publ
ic h
ealth
and
sec
urity
aut
horit
ies
R.3.
1 Pu
blic
hea
lth a
nd s
ecur
ity a
utho
ritie
s (e
.g. l
aw e
nfor
cem
ent,
bord
er c
ontr
ol, c
usto
ms)
link
ed d
urin
g a
susp
ect
or c
onfir
med
bio
logi
cal,
chem
ical
or
radi
olog
ical
eve
nt
No
capa
city
- 1
No
legi
slat
ion,
rela
tions
hips
, pro
toco
ls, M
oUs
or o
ther
agr
eem
ents
exi
st b
etw
een
publ
ic h
ealth
, ani
mal
hea
lth, r
adio
logi
cal s
afet
y, ch
emic
al s
afet
y an
d se
curit
y au
thor
ities
to a
ddre
ss a
ll ha
zard
sLi
mite
d
capa
city
- 2
Poin
ts o
f con
tact
and
trig
gers
for
notifi
catio
n an
d in
form
atio
n sh
arin
g ha
ve b
een
iden
tified
and
sha
red
betw
een
publ
ic h
ealth
, ani
mal
hea
lth, r
adio
logi
cal
safe
ty, c
hem
ical
saf
ety
and
secu
rity
auth
oriti
es to
add
ress
all
haza
rds
Deve
lope
d ca
paci
ty -
3M
oU o
r oth
er a
gree
men
t/pr
otoc
ol, t
hat i
nclu
des
at le
ast r
oles
, res
pons
ibili
ties,
SO
Ps a
nd in
form
atio
n to
be
shar
ed, e
xist
s be
twee
n pu
blic
hea
lth a
nd s
ecur
ity
auth
oriti
es w
ithin
the
coun
try
and
has
been
form
ally
acc
epte
d to
add
ress
all
haza
rds
Dem
onst
rate
d ca
paci
ty -
4
At le
ast o
ne p
ublic
hea
lth e
mer
genc
y re
spon
se o
r exe
rcis
e in
the
prev
ious
yea
r tha
t inc
lude
d in
form
atio
n sh
arin
g w
ith s
ecur
ity a
utho
ritie
s us
ing
the
form
al
MoU
or o
ther
agr
eem
ent/
prot
ocol
rela
ted
to a
ll ha
zard
sPu
blic
hea
lth a
nd s
ecur
ity a
utho
ritie
s en
gage
in a
join
t tra
inin
g pr
ogra
mm
e to
orie
nt, e
xerc
ise
and
inst
itutio
naliz
e kn
owle
dge
of M
oU o
r oth
er a
gree
men
ts
rela
ted
to a
ll ha
zard
s
Sust
aina
ble
capa
city
– 5
Publ
ic h
ealth
and
sec
urity
aut
horit
ies
exch
ange
repo
rts
and
info
rmat
ion
on e
vent
s of
join
t con
cern
at n
atio
nal, i
nter
med
iate
and
loca
l lev
els
on a
regu
lar b
asis
us
ing
the
form
al M
oU o
r oth
er a
gree
men
t/pr
otoc
olPu
blic
hea
lth a
nd s
ecur
ity a
utho
ritie
s en
gage
in a
join
t tra
inin
g pr
ogra
mm
e to
orie
nt, e
xerc
ise
and
inst
itutio
naliz
e kn
owle
dge
of th
e M
oU o
r oth
er a
gree
men
t re
late
d to
all
haza
rds
Cont
extu
al q
uest
ions
: N/A
Tech
nica
l que
stio
ns:
R.3.
1 Pu
blic
hea
lth a
nd s
ecur
ity a
utho
ritie
s (e
.g. l
aw e
nfor
cem
ent,
bord
er c
ontr
ol, c
usto
ms)
link
ed d
urin
g a
susp
ect o
r con
firm
ed b
iolo
gica
l, ch
emic
al o
r ra
diol
ogic
al e
vent
1.
Is th
ere
a M
oU o
r oth
er a
gree
men
t bet
wee
n pu
blic
hea
lth a
nd s
ecur
ity a
utho
rity
entit
ies
at th
e na
tiona
l lev
el?
a. I
f yes
, whi
ch s
ecur
ity a
utho
rity
orga
niza
tions
are
cov
ered
by
a M
oU o
r oth
er a
gree
men
t – la
w e
nfor
cem
ent,
bord
er c
ontr
ol, c
usto
ms
enfo
rcem
ent,
food
sa
fety
insp
ectio
n, ra
diol
ogic
al s
afet
y an
d ch
emic
al s
afet
y?b.
If n
ot, i
s th
ere
a M
oU o
r oth
er a
gree
men
t bet
wee
n pu
blic
hea
lth a
nd a
noth
er s
ecto
r (s
uch
as a
gric
ultu
re, d
efen
ce, f
orei
gn a
ffairs
) tha
t cou
ld b
e us
ed
as a
sam
ple
agre
emen
t to
prom
ote
info
rmat
ion
shar
ing
and
colla
bora
tion
durin
g em
erge
ncy
even
ts?
Are
ther
e ag
reem
ents
bet
wee
n pu
blic
hea
lth a
nd
secu
rity
auth
oriti
es a
t any
inte
rmed
iate
and
/or l
ocal
leve
ls?
2.
Hav
e tr
aini
ngs
been
con
duct
ed jo
intly
(at a
n in
term
edia
te le
vel (
regi
onal
) or n
atio
nal l
evel
) inc
ludi
ng fo
r bot
h pu
blic
hea
lth a
nd s
ecur
ity a
utho
ritie
s on
topi
cs
rela
ted
to in
form
atio
n sh
arin
g an
d jo
int i
nves
tigat
ions
/res
pons
es?
3.
Are
ther
e SO
Ps o
r agr
eem
ents
in p
lace
for c
oord
inat
ion
of a
join
t res
pons
e to
pub
lic h
ealth
and
oth
er e
mer
genc
ies
at o
ffici
al lo
catio
ns, s
uch
as p
oint
s of
ent
ry
whe
re b
oth
publ
ic h
ealth
and
sec
urity
aut
horit
ies
have
ope
ratio
nal s
afet
y an
d he
alth
sec
urity
resp
onsi
bilit
ies?
4.
Are
ther
e SO
Ps o
r agr
eem
ents
in p
lace
for a
join
t/sh
ared
risk
ass
essm
ent d
urin
g ev
ents
of p
ublic
hea
lth a
nd s
ecur
ity s
igni
fican
ce?
RE
SP
ON
D

INTERNATIONAL HEALTH REGULATIONS (2005)
82 - Joint External Evaluation Tool - Second edition
5.
Is th
ere
legi
slat
ion
in p
lace
that
allo
ws
the
gove
rnm
ent t
o de
tain
/qua
rant
ine
an in
divi
dual
who
pre
sent
s a
publ
ic h
ealth
risk
?6.
H
ow a
re p
oten
tial b
iolo
gica
l, ch
emic
al a
nd ra
diol
ogic
al e
vent
s th
at m
ay h
ave
delib
erat
e m
otiv
es id
entifi
ed in
the
coun
try?
Pro
vide
any
pla
ns th
at h
ave
been
dr
afte
d th
at c
over
resp
onse
to p
ossi
ble
biol
ogic
al, c
hem
ical
and
radi
olog
ical
eve
nts.
7.
Is th
ere
a fu
nctio
nal m
echa
nism
for c
olla
bora
tion
and
timel
y an
d sy
stem
atic
info
rmat
ion
exch
ange
bet
wee
n pu
blic
hea
lth a
nd la
w e
nfor
cem
ent a
genc
ies
in
case
of d
elib
erat
e an
d/or
acc
iden
tal e
vent
s?8.
Ar
e pu
blic
hea
lth e
xper
ts in
volv
ed in
em
erge
ncy
resp
onse
link
ed to
the
BTW
C? H
as th
e co
untr
y pa
rtic
ipat
ed in
an
exer
cise
, sim
ulat
ion
or re
spon
se in
the
past
ye
ar th
at in
volv
es le
ader
ship
from
bot
h pu
blic
hea
lth a
nd s
ecur
ity a
utho
ritie
s? If
yes
, des
crib
e th
e ex
erci
se, s
imul
atio
n or
resp
onse
.a.
Des
crib
e an
y co
rrec
tive
actio
ns th
at w
ere
reco
mm
ende
d on
how
the
publ
ic h
ealth
org
aniz
atio
n sh
ould
coo
rdin
ate
with
sec
urity
aut
horit
ies.
9.
Ar
e re
port
s re
gula
rly s
hare
d be
twee
n pu
blic
hea
lth a
nd a
ny s
ecur
ity a
utho
ritie
s w
ithin
the
cou
ntry
? Is
the
re a
mec
hani
sm in
pla
ce t
o en
cour
age
regu
lar
repo
rtin
g?a.
Wha
t typ
es o
f rep
orts
are
sha
red
from
pub
lic h
ealth
ent
ities
to s
ecur
ity a
utho
ritie
s re
gula
rly?
b. W
hat t
ypes
of r
epor
ts a
re s
hare
d fr
om s
ecur
ity a
utho
ritie
s to
the
publ
ic h
ealth
sys
tem
regu
larly
?c.
How
oft
en a
re th
e in
form
atio
nal r
epor
ts s
hare
d?10
. Is
ther
e a
coun
try-
spec
ific
join
t inv
estig
atio
ns c
urric
ulum
in p
lace
to tr
ain
publ
ic h
ealth
and
law
enf
orce
men
t ent
ities
on
join
t inv
estig
atio
ns?
11.
Des
crib
e ho
w th
e na
tiona
l gov
ernm
ent i
s co
nnec
ted
to IN
TERP
OL.
Wha
t min
istr
y is
cha
rged
with
inte
ract
ing
with
INTE
RPO
L?
Doc
umen
tatio
n or
evi
denc
e fo
r lev
el o
f cap
abili
ty:
l
SOPs
or e
mer
genc
y re
spon
se p
lans
that
wou
ld in
clud
e se
curit
y au
thor
ities
l
Info
rmat
iona
l rep
orts
that
are
regu
larly
sha
red
with
sec
urity
aut
horit
ies
Refe
renc
es:
l
WH
O–
OIE
ope
ratio
nal f
ram
ewor
k fo
r go
od g
over
nanc
e at
the
hum
an¬–
anim
al in
terf
ace:
Brid
ging
WH
O a
nd O
IE t
ools
for
the
ass
essm
ent
of n
atio
nal
capa
citie
s. W
HO
and
OIE
; 201
4 (h
ttp:
//w
ww
.oie
.int/
filea
dmin
/Hom
e/fr
/Med
ia_C
ente
r/do
cs/p
df/W
HO
_OIE
_Ope
ratio
nal_
Fram
ewor
k_Fi
nal2
acc
esse
d 29
N
ovem
ber 2
017)
.l
Terr
estr
ial
anim
al
heal
th
code
. Ch
apte
r 3.
4 Ve
terin
ary
legi
slat
ion.
W
orld
O
rgan
isat
ion
for
Anim
al
Hea
lth;
2016
(h
ttp:
//w
ww
.oie
.int/
inde
x.ph
p?id
=169
&L=0
&htm
file=
chap
itre_
vet_
legi
slat
ion.
htm
, acc
esse
d 29
Nov
embe
r 201
7).
l
Conv
entio
n on
the
proh
ibiti
on o
f the
dev
elop
men
t, pr
oduc
tion,
sto
ckpi
ling
and
use
of c
hem
ical
wea
pons
and
on
thei
r des
truc
tion.
The
Hag
ue: O
rgan
isat
ion
for t
he P
rohi
bitio
n of
Che
mic
al W
eapo
ns (h
ttps
://w
ww
.opc
w.o
rg/fi
lead
min
/OPC
W/C
WC/
CWC_
en.p
df, a
cces
sed
29 N
ovem
ber 2
017)
.l
Trea
ty o
n th
e no
n-pr
olife
ratio
n of
nuc
lear
wea
pons
. Int
erna
tiona
l Ato
mic
Ene
rgy
Agen
cy [i
nfor
mat
ion
circ
ular
] IN
FCIR
C/14
0, 2
2 Ap
ril 1
970
(htt
ps:/
/ww
w.
iaea
.org
/site
s/de
faul
t/fil
es/p
ublic
atio
ns/d
ocum
ents
/inf
circ
s/19
70/i
nfci
rc14
0.pd
f, ac
cess
ed 2
9 N
ovem
ber 2
017)
.
RE
SP
ON
D

INTERNATIONAL HEALTH REGULATIONS (2005)
83 - Joint External Evaluation Tool - Second edition
MED
ICAL
CO
UN
TERM
EASU
RES
AND
PER
SON
NEL
DEP
LOYM
ENT
Targ
et: :
Nat
iona
l fra
mew
ork
for:
tran
sfer
ring
(sen
ding
and
rec
eivi
ng)
med
ical
cou
nter
mea
sure
s, a
nd p
ublic
hea
lth a
nd m
edic
al p
erso
nnel
fro
m in
tern
atio
nal
part
ners
dur
ing
publ
ic h
ealth
em
erge
ncie
s; a
nd p
roce
dure
s fo
r cas
e m
anag
emen
t of e
vent
s du
e to
IHR
rele
vant
haz
ards
.
As m
easu
red
by: (
1) E
vide
nce
of a
t lea
st o
ne re
spon
se to
a p
ublic
hea
lth e
mer
genc
y w
ithin
the
prev
ious
yea
r tha
t dem
onst
rate
s th
at th
e co
untr
y se
nt o
r rec
eive
d m
edic
al c
ount
erm
easu
res
and
pers
onne
l acc
ordi
ng t
o w
ritte
n na
tiona
l or
inte
rnat
iona
l pro
toco
ls, o
r a
form
al e
xerc
ise
or s
imul
atio
n th
at d
emon
stra
tes
thes
e m
easu
res.
(2) E
vide
nce
of d
emon
stra
ting
appl
icat
ion
of c
ase
man
agem
ent p
roce
dure
s fo
r eve
nts
due
to IH
R re
leva
nt h
azar
ds.
Desi
red
impa
ct:
Coun
trie
s w
ill h
ave
the
nece
ssar
y le
gal
and
regu
lato
ry p
roce
sses
and
log
istic
al p
lans
to
allo
w f
or r
apid
nat
iona
l or
cro
ss-b
orde
r de
ploy
men
t an
d re
ceip
t of
pu
blic
he
alth
an
d m
edic
al
pers
onne
l du
ring
emer
genc
ies.
Re
gion
al
(inte
rnat
iona
l) co
llabo
ratio
n w
ill
assi
st
coun
trie
s in
ove
rcom
ing
the
lega
l, lo
gist
ical
and
reg
ulat
ory
chal
leng
es t
o de
ploy
men
t of
pub
lic h
ealth
and
med
ical
per
sonn
el f
rom
one
cou
ntry
to
anot
her.
Coun
try
has
deve
lope
d ca
se m
anag
emen
t pr
oced
ures
and
im
plem
ente
d ac
ross
the
sys
tem
dur
ing
heal
th e
mer
genc
ies
due
to I
HR
rele
vant
haz
ards
..
RE
SP
ON
D

INTERNATIONAL HEALTH REGULATIONS (2005)
84 - Joint External Evaluation Tool - Second edition
Scor
e
Indi
cato
rs: M
edic
al c
ount
erm
easu
res
and
pers
onne
l dep
loym
ent
R.4.
1 Sy
stem
in p
lace
for a
ctiv
atin
g an
d co
ordi
natin
g m
edic
al c
ount
erm
easu
res
durin
g
a pu
blic
hea
lth e
mer
genc
y1
R.4.
2 Sy
stem
in p
lace
for a
ctiv
atin
g an
d co
ordi
natin
g he
alth
per
sonn
el d
urin
g a
publ
ic
heal
th e
mer
genc
y
R.4.
3 Ca
se m
anag
emen
t pro
cedu
res
impl
emen
ted
for I
HR
rele
vant
haz
ards
No
capa
city
- 1
No
natio
nal
coun
term
easu
res
plan
ha
s be
en
draf
ted
No
natio
nal p
erso
nnel
dep
loym
ent
plan
has
bee
n dr
afte
dN
o ca
se m
anag
emen
t gu
idel
ines
are
ava
ilabl
e fo
r pr
iorit
y ep
idem
ic-p
rone
dis
ease
s2
Lim
ited
ca
paci
ty -
2
Plan
s th
at
outli
ne
a sy
stem
fo
r se
ndin
g an
d re
ceiv
ing
med
ical
cou
nter
mea
sure
s du
ring
publ
ic
heal
th e
mer
genc
ies
have
bee
n dr
afte
d
Plan
s tha
t out
line a
syst
em fo
r sen
ding
and
rece
ivin
g he
alth
per
sonn
el d
urin
g pu
blic
hea
lth e
mer
genc
ies
have
bee
n dr
afte
d, i
nclu
ding
the
dev
elop
men
t of
pl
ans
for E
MTs
3 for
nat
iona
l res
pons
e
Case
m
anag
emen
t gu
idel
ines
ar
e av
aila
ble
for
prio
rity
epid
emic
-pro
ne d
isea
ses
Deve
lope
d ca
paci
ty -
3
Tabl
e to
p ex
erci
se(s
) ha
s be
en
cond
ucte
d to
de
mon
stra
te
send
ing
or
rece
ivin
g of
m
edic
al
coun
term
easu
res
durin
g a
publ
ic h
ealth
em
erge
ncy
Tabl
e to
p ex
erci
se(s
) ha
s be
en
cond
ucte
d to
de
mon
stra
te d
ecis
ion
mak
ing
and
prot
ocol
s fo
r se
ndin
g or
rece
ivin
g he
alth
per
sonn
el fr
om a
noth
er
coun
try
durin
g a
publ
ic h
ealth
em
erge
ncy,
and
trai
ning
and
equ
ipm
ent
is a
vaila
ble
for
natio
nal
EMTs
Case
man
agem
ent g
uide
lines
for o
ther
IHR
rele
vant
ha
zard
s4 are
ava
ilabl
e at
app
licab
le h
ealth
sys
tem
le
vels
and
SO
Ps a
re a
vaila
ble
for t
he m
anag
emen
t an
d tr
ansp
ort
of p
oten
tially
infe
ctio
us p
atie
nts
in
the
com
mun
ity a
nd a
t poi
nts
of e
ntry
5
Dem
onst
rate
d ca
paci
ty -
4
At le
ast
one
resp
onse
or
form
al e
xerc
ise
or s
imu-
latio
n w
ithin
the
pre
viou
s ye
ar i
n w
hich
med
ical
co
unte
rmea
sure
s w
ere
sent
or
rece
ived
by
the
coun
try
At l
east
one
res
pons
e or
for
mal
exe
rcis
e or
si-
mul
atio
n w
ithin
the
pre
viou
s ye
ar in
whi
ch h
ealth
pe
rson
nel
wer
e se
nt o
r re
ceiv
ed b
y th
e co
untr
y.
Evid
ence
of d
eplo
yabl
e EM
T ca
paci
ty/c
apab
ility
for
natio
nal r
espo
nse
Case
man
agem
ent,
patie
nt re
ferr
al a
nd tr
ansp
orta
-tio
n, a
nd m
anag
emen
t and
tran
spor
t of p
oten
tially
in
fect
ious
pat
ient
s ar
e im
plem
ente
d ac
cord
ing
to
guid
elin
es a
nd/o
r SO
Ps
Sust
aina
ble
capa
city
- 5
Coun
try
part
icip
ates
in
a
regi
onal
/int
erna
tiona
l pa
rtne
rshi
p or
has
form
al a
gree
men
t with
ano
ther
co
untr
y or
inte
rnat
iona
l org
aniz
atio
n th
at o
utlin
es
crite
ria a
nd p
roce
dure
s fo
r se
ndin
g an
d re
ceiv
ing
med
ical
cou
nter
mea
sure
s an
d ha
s pa
rtic
ipat
ed
in a
n ex
erci
se o
r re
spon
se w
ithin
the
pas
t ye
ar t
o pr
actic
e de
ploy
men
t or r
ecei
pt o
f med
ical
cou
nter
-m
easu
res
Coun
try
part
icip
ates
in
a
regi
onal
/int
erna
tiona
l pa
rtne
rshi
p or
has
form
al a
gree
men
t with
ano
ther
co
untr
y or
inte
rnat
iona
l org
aniz
atio
n th
at o
utlin
es
crite
ria a
nd p
roce
dure
s fo
r se
ndin
g an
d re
ceiv
ing
heal
th p
erso
nnel
and
has
par
ticip
ated
in a
n ex
er-
cise
or
resp
onse
with
in t
he p
ast
year
to
prac
tice
depl
oym
ent o
r rec
eipt
of h
ealth
per
sonn
el. C
ount
ry
has
an in
tern
atio
nally
dep
loya
ble
EMT
as c
lass
ified
by
WH
O o
r is
in th
e pr
oces
s of
men
tors
hip
by W
HO
In a
dditi
on t
o de
mon
stra
ted
capa
city
, app
ropr
iate
st
aff a
nd re
sour
ces
(as
defin
ed b
y th
e co
untr
y) a
re
in p
lace
in th
e m
anag
emen
t of I
HR
rele
vant
em
er-
genc
ies
1 -
If th
e co
untr
y ha
s a
stoc
kpile
of m
edic
al c
ount
erm
easu
res,
it w
ill n
ot b
e as
ked
to p
rovi
de a
list
or f
orm
ular
y.2
- Fo
r the
ani
mal
hea
lth s
ecto
r, th
is in
form
atio
n ca
n be
foun
d in
the
coun
try
PVS
Path
way
mis
sion
repo
rt, u
nder
Crit
ical
Com
pete
ncy
CC II
-6: E
mer
genc
y re
spon
se3
- EM
Ts c
onsi
st o
f hea
lth p
rofe
ssio
nals
pro
vidi
ng d
irect
clin
ical
car
e to
pop
ulat
ions
affe
cted
by
outb
reak
s, d
isas
ters
and
em
erge
ncie
s as
a s
urge
cap
acity
to s
uppo
rt th
e lo
cal h
ealth
sys
tem
. The
y co
uld
be c
ivili
an o
r mili
tary
or
nong
over
nmen
tal t
eam
s an
d in
clud
e bo
th n
atio
nal a
nd in
tern
atio
nal p
erso
nnel
.4
- N
ucle
ar, c
hem
ical
, zoo
notic
, foo
d sa
fety
, tra
uma,
exa
cerb
atio
n of
non
com
mun
icab
le d
isea
ses
and
men
tal h
ealth
con
ditio
ns.
5 -
As s
peci
fied
in A
rtic
le 5
7, 2
(d) I
HR
(200
5).
RE
SP
ON
D
INTERNATIONAL HEALTH REGULATIONS (2005)
85 - Joint External Evaluation Tool - Second edition
Cont
extu
al q
uest
ions
: N/A
Tech
nica
l que
stio
ns:
R.4.
1 Sy
stem
in p
lace
for a
ctiv
atin
g an
d co
ordi
natin
g m
edic
al c
ount
erm
easu
res
durin
g a
publ
ic h
ealth
em
erge
ncy
1.
Doe
s th
e co
untr
y ha
ve a
pla
n in
pla
ce th
at id
entifi
es p
roce
dure
s an
d de
cisi
on-m
akin
g re
late
d to
sen
ding
and
rece
ivin
g m
edic
al c
ount
erm
easu
res
durin
g a
publ
ic h
ealth
em
erge
ncy?
a. D
oes
the
plan
add
ress
regu
lato
ry c
once
rns
of re
ques
ting/
acce
ptin
g an
d re
ceiv
ing
drug
s or
dev
ices
from
an
inte
rnat
iona
l sou
rce?
b. D
oes
the
plan
add
ress
logi
stic
con
cern
s re
late
d to
sen
ding
, rec
eivi
ng a
nd d
istr
ibut
ing
med
ical
cou
nter
mea
sure
s du
ring
a pu
blic
hea
lth e
mer
genc
y?c.
Doe
s th
e pl
an a
ddre
ss s
ecur
ity c
once
rns
that
may
em
erge
rela
ted
to s
endi
ng/r
ecei
ving
/dis
trib
utin
g m
edic
al c
ount
erm
easu
res
durin
g a
shor
tage
?2.
H
as th
e co
untr
y ex
erci
sed
plan
s fo
r sen
ding
or r
ecei
ving
med
ical
cou
nter
mea
sure
s w
ithin
the
past
yea
r?a.
If y
es, d
escr
ibe
the
exer
cise
and
spe
cific
out
com
es.
3.
Doe
s th
e co
untr
y ha
ve a
sto
ckpi
le o
f med
ical
cou
nter
mea
sure
s fo
r nat
iona
l use
dur
ing
a pu
blic
hea
lth e
mer
genc
y?a.
Doe
s th
e co
untr
y ha
ve c
apac
ity to
pro
duce
ant
ibio
tics,
vac
cine
s, la
bora
tory
sup
plie
s/eq
uipm
ent o
r oth
ers?
b. D
oes
this
incl
ude
coun
term
easu
res
for u
se in
oth
er s
ecto
rs (e
.g. p
erso
nal p
rote
ctiv
e eq
uipm
ent f
or a
nim
al c
ullin
g)?
c. I
f the
cou
ntry
has
a s
tock
pile
for d
rugs
and
equ
ipm
ent,
spec
ify fo
r how
long
this
may
last
and
for h
ow m
any
patie
nts.
d.
Is
annu
al b
udge
t ava
ilabl
e fo
r sto
ckpi
ling?
4.
Doe
s th
e co
untr
y ha
ve a
gree
men
ts in
pla
ce w
ith m
anuf
actu
rers
or d
istr
ibut
ors
to p
rocu
re m
edic
al c
ount
erm
easu
res
durin
g a
publ
ic h
ealth
em
erge
ncy?
If y
es,
desc
ribe.
5.
Is th
e co
untr
y pa
rt o
f any
regi
onal
/inte
rnat
iona
l cou
nter
mea
sure
pro
cure
men
t agr
eem
ents
? If
yes,
des
crib
e.6.
Is
the
coun
try
part
of a
ny re
gion
al/in
tern
atio
nal c
ount
erm
easu
re s
harin
g ag
reem
ents
? If
yes,
des
crib
e.7.
Is
the
coun
try
part
of a
ny re
gion
al/in
tern
atio
nal c
ount
erm
easu
re d
istr
ibut
ing
agre
emen
ts?
If ye
s, d
escr
ibe.
8.
Are
ther
e de
dica
ted
reso
urce
s/st
affin
g id
entifi
ed fo
r log
istic
s re
late
d to
del
iver
y an
d re
ceip
t of c
ount
erm
easu
res?
9.
Are
ther
e de
dica
ted
reso
urce
s/st
affin
g id
entifi
ed fo
r tra
ckin
g an
d di
strib
utio
n of
cou
nter
mea
sure
s?10
. D
oes
the
coun
try
have
a p
ande
mic
pre
pare
dnes
s pl
an th
at a
ddre
sses
cou
nter
mea
sure
s? If
yes
, des
crib
e.11
. D
oes
the
coun
try
have
a p
lan,
pro
cedu
re o
r leg
al p
rovi
sion
in p
lace
for p
rocu
ring
anim
al c
ount
erm
easu
res?
If y
es, d
escr
ibe.
12.
Doe
s th
e co
untr
y ha
ve a
pla
n, p
roce
dure
or l
egal
pro
visi
on in
pla
ce fo
r dis
trib
utin
g an
imal
cou
nter
mea
sure
s? If
yes
, des
crib
e.
R.4.
2 Sy
stem
in p
lace
for a
ctiv
atin
g an
d co
ordi
natin
g he
alth
per
sonn
el d
urin
g a
publ
ic h
ealth
em
erge
ncy
1.
Doe
s th
e co
untr
y ha
ve a
pla
n in
pla
ce th
at id
entifi
es p
roce
dure
s an
d de
cisi
on-m
akin
g re
late
d to
sen
ding
and
rece
ivin
g he
alth
per
sonn
el d
urin
g a
publ
ic h
ealth
em
erge
ncy?
a. D
oes
the
plan
add
ress
regu
lato
ry a
nd li
cens
ure
conc
erns
of r
eque
stin
g/ac
cept
ing
and
rece
ivin
g he
alth
per
sonn
el fr
om a
n in
tern
atio
nal s
ourc
e?
b. D
oes
the
plan
iden
tify
trai
ning
crit
eria
and
sta
ndar
ds fo
r hea
lth p
erso
nnel
who
will
be
sent
or r
ecei
ved
durin
g a
publ
ic h
ealth
em
erge
ncy?
RE
SP
ON
D

INTERNATIONAL HEALTH REGULATIONS (2005)
86 - Joint External Evaluation Tool - Second edition
c. D
oes
the
plan
add
ress
liab
ility
con
cern
s fo
r usi
ng m
edic
al p
erso
nnel
dur
ing
an in
tern
atio
nal d
eplo
ymen
t?d.
Doe
s th
e pl
an a
ddre
ss s
afet
y co
ncer
ns fo
r hea
lth p
erso
nnel
dur
ing
a na
tiona
l or i
nter
natio
nal d
eplo
ymen
t?e.
Doe
s th
e pl
an a
ddre
ss fi
nanc
ial c
once
rns
for h
ealth
per
sonn
el d
urin
g a
natio
nal o
r int
erna
tiona
l dep
loym
ent?
f. Ar
e ot
her s
ecto
rs (i
.e. s
ecur
ity a
utho
ritie
s, a
nim
al h
ealth
) inc
lude
d in
pla
ns fo
r sen
ding
/rec
eivi
ng p
erso
nnel
dur
ing
an e
mer
genc
y?2.
D
o pl
ans
for s
urge
sta
ffing
for p
ublic
hea
lth e
mer
genc
y re
spon
se a
ctiv
atio
ns in
clud
e tr
igge
rs fo
r req
uest
ing
pers
onne
l fro
m o
ther
cou
ntrie
s?a.
Hav
e tr
aini
ng p
roce
dure
s an
d m
ater
ials
bee
n de
velo
ped
to o
rient
arr
ivin
g pe
rson
nel i
nto
the
orga
niza
tion?
3.
Doe
s th
e sy
stem
incl
ude
othe
r sec
tors
(che
mic
als,
radi
atio
n, a
nim
al h
ealth
) or d
o se
para
te s
yste
ms
exis
t?
4.
Has
the
coun
try
exer
cise
d pl
ans
for s
endi
ng o
r rec
eivi
ng h
ealth
per
sonn
el w
ithin
the
past
yea
r?a.
If
yes,
des
crib
e th
e ex
erci
se a
nd s
peci
fic o
utco
mes
.5.
Is
the
coun
try
part
of a
ny re
gion
al/in
tern
atio
nal p
erso
nnel
dep
loym
ent a
gree
men
ts, s
uch
as W
HO
Glo
bal O
utbr
eak
Aler
t and
Res
pons
e N
etw
ork
(GOA
RN)?
If
yes,
des
crib
e.a.
Are
pol
icie
s an
d re
sour
ces
in p
lace
to e
nsur
e th
at te
chni
cal i
nstit
utio
ns a
nd n
etw
orks
are
abl
e to
be
activ
e pa
rtne
rs in
the
GO
ARN
? If
yes,
des
crib
e.b.
Doe
s th
e co
untr
y ha
ve a
pan
dem
ic p
repa
redn
ess
plan
or o
ther
em
erge
ncy
prep
ared
ness
pla
n th
at a
ddre
sses
per
sonn
el d
eplo
ymen
ts?
If ye
s, d
escr
ibe.
6.
Doe
s th
e co
untr
y pa
rtic
ipat
e ac
tivel
y in
the
EMT
initi
ativ
e an
d us
e th
e EM
T gu
idin
g pr
inci
ples
and
min
imum
sta
ndar
ds?
a. H
as th
e co
untr
y de
sign
ated
EM
T fo
cal p
oint
s at
pol
icy
and
oper
atio
nal l
evel
s?
b. H
as th
e co
untr
y pa
rtic
ipat
ed in
EM
T tr
aini
ng e
vent
s or
regi
onal
/glo
bal m
eetin
gs?
c. H
as th
e co
untr
y ta
ken
on a
n ac
tive
role
in th
e EM
T in
itiat
ive
at re
gion
al o
r glo
bal l
evel
, i.e
. has
it ta
ken
on th
e ro
le o
f Reg
iona
l Cha
ir or
Vic
e-ch
air?
Has
it
offe
red
mem
bers
for E
MT
tech
nica
l wor
king
gro
ups?
Doe
s th
e co
untr
y pr
ovid
e ex
pert
s to
the
EMT
men
tors
hip
pool
? d.
Doe
s th
e co
untr
y ha
ve a
WH
O c
lass
ified
EM
T fo
r int
erna
tiona
l dep
loym
ent?
e. D
oes
the
coun
try
have
a q
ualit
y as
sura
nce
or a
ccre
dita
tion
syst
em in
pla
ce fo
r nat
iona
lly d
eplo
yabl
e EM
Ts?
R.4.
3 Ca
se m
anag
emen
t pro
cedu
res
impl
emen
ted
for I
HR
rele
vant
haz
ards
1.
Avai
labi
lity
of c
ase
man
agem
ent g
uide
lines
for p
riorit
y di
seas
es a
nd IH
R re
leva
nt h
azar
ds a
t all
heal
th s
yste
m le
vels
.2.
Av
aila
bilit
y of
SO
Ps (a
ccor
ding
to n
atio
nal o
r int
erna
tiona
l gui
delin
es) f
or th
e m
anag
emen
t and
tran
spor
t of p
oten
tially
infe
ctio
us p
atie
nts
at th
e lo
cal l
evel
and
po
ints
of e
ntry
.3.
Av
aila
bilit
y of
pat
ient
refe
rral
and
tran
spor
tatio
n m
echa
nism
with
ade
quat
e re
sour
ces
(des
igna
ted
ambu
lanc
es, h
ospi
tals
and
SO
Ps).
4.
Avai
labi
lity
of a
ppro
pria
te s
taff
trai
ned
in c
ase
man
agem
ent o
f IH
R-re
leva
nt e
mer
genc
ies,
incl
udin
g bu
t not
lim
ited
to th
e ab
ility
to re
cogn
ize,
trea
t and
refe
r in
fect
ious
dis
ease
s, tr
aum
a ca
ses,
exa
cerb
atio
n of
non
com
mun
icab
le d
isea
ses
and
othe
rs.
Doc
umen
tatio
n or
evi
denc
e fo
r lev
el o
f cap
abili
ty:
l
Coun
term
easu
res
depl
oym
ent p
lan
l
Pers
onne
l dep
loym
ent p
lan
l
Pand
emic
pre
pare
dnes
s pl
an (i
f app
licab
le)
RE
SP
ON
D

INTERNATIONAL HEALTH REGULATIONS (2005)
87 - Joint External Evaluation Tool - Second edition
Refe
renc
es:
l
Clas
sific
atio
n an
d m
inim
um s
tand
ards
for f
orei
gn (e
mer
genc
y) m
edic
al te
ams
in s
udde
n on
set d
isas
ters
. Gen
eva:
Wor
ld H
ealth
Org
aniz
atio
n; 2
013
(http
://w
ww
.who
.int/
hac/
glob
al_h
ealth
_clu
ster
/fm
t_gu
idel
ines
_sep
tem
ber2
013.
pdf,
acce
ssed
1 D
ecem
ber 2
017)
.l
Man
agem
ent o
f lim
b in
jurie
s du
ring
disa
ster
s an
d co
nflic
ts. G
enev
a: W
orld
Hea
lth O
rgan
izat
ion;
201
7 (h
ttps:
//ex
tran
et.w
ho.in
t/em
t/si
tes/
defa
ult/
files
/_A%
20Fi
eld%
20G
uide
_7.8
%20
MB.
pdf,
acce
ssed
27
Dec
embe
r 201
7).
l
Emer
genc
y m
edic
al te
ams.
Wor
ld H
ealth
Org
aniz
atio
n [w
ebsi
te] (
http
s://
extr
anet
.who
.int/
emt/
page
/hom
e, a
cces
sed
1 D
ecem
ber 2
017)
.
RE
SP
ON
D

INTERNATIONAL HEALTH REGULATIONS (2005)
88 - Joint External Evaluation Tool - Second edition
RISK
CO
MM
UN
ICAT
ION
Ta
rget
: Sta
tes
Part
ies
use
mul
tilev
el, m
ultis
ecto
ral a
nd m
ultif
acet
ed ri
sk c
omm
unic
atio
n ca
paci
ty fo
r pub
lic h
ealth
em
erge
ncie
s. R
eal-
time
exch
ange
of i
nfor
mat
ion,
ad
vice
and
opi
nion
s du
ring
unus
ual a
nd u
nexp
ecte
d ev
ents
and
em
erge
ncie
s so
that
info
rmed
dec
isio
ns to
miti
gate
the
effe
cts
of th
reat
s, a
nd p
rote
ctiv
e an
d pr
even
tativ
e ac
tion
can
be m
ade.
Thi
s in
clud
es a
mix
of c
omm
unic
atio
n an
d en
gage
men
t str
ateg
ies,
suc
h as
med
ia a
nd s
ocia
l med
ia c
omm
unic
atio
ns, m
ass
awar
enes
s ca
mpa
igns
, hea
lth p
rom
otio
n, s
ocia
l mob
iliza
tion,
sta
keho
lder
eng
agem
ent a
nd c
omm
unity
eng
agem
ent.
As m
easu
red
by: (
1) F
orm
al g
over
nmen
t ris
k co
mm
unic
atio
ns p
lans
, arr
ange
men
ts a
nd s
yste
ms
in p
lace
. (2)
Exi
sten
ce o
f ris
k co
mm
unic
atio
n co
ordi
natio
n pl
atfo
rm a
nd m
echa
nism
s fo
r in
tern
al a
nd p
artn
er c
omm
unic
atio
n. (
3) E
vide
nce
that
pub
lic c
omm
unic
atio
n un
it or
tea
m o
pera
tes
effic
ient
ly a
nd e
ffect
ivel
y.
(4)
Evid
ence
tha
t ris
k co
mm
unic
atio
n un
its s
yste
mat
ical
ly e
ngag
e po
pula
tions
at
com
mun
ity le
vel d
urin
g em
erge
ncie
s. (
5) E
xist
ence
of
a sy
stem
to
gath
er
info
rmat
ion
on p
erce
ptio
ns, r
isky
beh
avio
urs
and
mis
info
rmat
ion
to a
naly
se p
ublic
con
cern
s an
d fe
ars.
Desi
red
impa
ct:
Resp
onsi
ble
entit
ies
effe
ctiv
ely
com
mun
icat
e, a
ctiv
ely
liste
n an
d re
spon
d to
con
cern
s of
the
pub
lic t
hrou
gh m
edia
, so
cial
med
ia,
mas
s aw
aren
ess
cam
paig
ns, h
ealth
pro
mot
ion,
soc
ial m
obili
zatio
n, s
take
hold
er e
ngag
emen
t as
wel
l as
com
mun
ity e
ngag
emen
t. Th
e de
sire
d ou
tcom
e of
effe
ctiv
e ris
k co
mm
unic
atio
n is
to m
itiga
te th
e po
tent
ial n
egat
ive
impa
ct o
f hea
lth h
azar
ds b
efor
e, d
urin
g an
d af
ter p
ublic
hea
lth e
mer
genc
ies
or u
nusu
al e
vent
s.
RE
SP
ON
D

INTERNATIONAL HEALTH REGULATIONS (2005)
89 - Joint External Evaluation Tool - Second edition
Scor
eIn
dica
tors
: Ris
k co
mm
unic
atio
n1,2
R.5.
1 Ri
sk c
omm
unic
atio
n sy
stem
s fo
r unu
sual
/un
expe
cted
eve
nts
and
emer
genc
ies
R.5.
2 In
tern
al a
nd p
artn
er c
oord
inat
ion
for
emer
genc
y ris
k co
mm
unic
atio
nR.
5.3
Publ
ic c
omm
unic
atio
n fo
r em
erge
ncie
s
No
capa
city
- 1
No
form
al
gove
rnm
ent
risk
com
mun
icat
ion
arra
ngem
ent
No
coor
dina
tion
plat
form
and
mec
hani
sms
for
inte
rnal
and
par
tner
com
mun
icat
ion
for
enga
ging
ke
y na
tiona
l, in
term
edia
te, l
ocal
and
inte
rnat
iona
l st
akeh
olde
rs (i
nclu
ding
hea
lth c
are
wor
kers
)
No
cent
ral u
nit o
r loc
us fo
r pub
lic c
omm
unic
atio
n,
or re
spon
sive
ad
hoc
med
ia o
utre
ach
Lim
ited
ca
paci
ty -
2
Form
al g
over
nmen
t ar
rang
emen
t in
clud
ing
a na
-tio
nal
mul
tihaz
ard,
mul
tisec
tora
l em
erge
ncy
risk
com
mun
icat
ion
plan
(r
evie
wed
w
ithin
pa
st
24
mon
ths)
in p
lace
and
a d
edic
ated
cor
e te
am r
es-
pons
ible
for t
his
area
of w
ork
esta
blis
hed
Sign
ifica
nt g
aps
in c
apac
ity i
n hu
man
res
ourc
es,
com
mun
icat
ion
plat
form
s an
d re
sour
ces
to d
eal
with
a la
rge-
scal
e em
erge
ncy
Som
e ad
hoc
com
mun
icat
ion
coor
dina
tion,
suc
h as
mee
tings
with
som
e pa
rtne
rs a
nd/o
r irr
egul
ar
info
rmat
ion
shar
ing
Publ
ic c
omm
unic
atio
n un
it or
team
exi
sts
Gov
ernm
ent s
poke
sper
son
iden
tified
and
trai
ned
Proc
edur
es fo
r pub
lic c
omm
unic
atio
n in
pla
ce
Deve
lope
d ca
paci
ty -
3
Form
al g
over
nmen
t arr
ange
men
ts a
nd s
yste
ms
in
plac
e w
ith S
OPs
and
cap
acity
with
mul
tisec
tora
l an
d m
ultis
take
hold
er in
volv
emen
t, bu
t in
suffi
cien
t al
loca
tion
and
alig
nmen
t of
hum
an a
nd fi
nanc
ial
reso
urce
s
Com
mun
icat
ion
coor
dina
tion
exis
ts b
ut w
ith l
i-m
ited
part
ner
and
stak
ehol
der
enga
gem
ent
(suc
h as
hea
lth c
are
wor
kers
, civ
il so
ciet
y or
gani
zatio
ns,
priv
ate
sect
or a
nd o
ther
non
-sta
te a
ctor
s)
Proa
ctiv
e pu
blic
out
reac
h on
a m
ix o
f pl
atfo
rms
(new
spap
ers,
ra
dio,
te
levi
sion
, so
cial
m
edia
, In
tern
et) a
s ap
prop
riate
acc
ordi
ng t
o na
tiona
l and
lo
cal
pref
eren
ces,
in
rele
vant
nat
iona
l an
d lo
cal
lang
uage
s, a
nd u
nder
stan
dabl
e to
the
popu
latio
n U
se o
f loc
ally
rele
vant
tech
nolo
gies
for p
ublic
com
-m
unic
atio
n (s
uch
as m
obile
pho
nes)
Dem
onst
rate
d ca
paci
ty –
4
Fully
ope
ratio
nal n
atio
nal s
yste
m e
stab
lishe
d w
ith
reas
onab
ly s
kille
d an
d/or
tra
ined
per
sonn
el a
nd
volu
ntee
rs, a
nd fi
nanc
ial
reso
urce
s an
d ar
rang
e-m
ents
for
sca
le-u
p as
evi
denc
ed b
y a
sim
ulat
ion
exer
cise
or t
este
d du
ring
a re
al h
ealth
em
erge
ncy
Effe
ctiv
e, re
gula
r com
mun
icat
ion
coor
dina
tion
with
al
l par
tner
s, a
nd th
eir c
oord
inat
ion
evid
ence
d by
a
sim
ulat
ion
exer
cise
or
test
ed d
urin
g a
real
hea
lth
emer
genc
y
Ther
e is
pla
nned
com
mun
icat
ion
with
con
tinuo
us
enga
gem
ent
and
proa
ctiv
e m
edia
out
reac
h (in
-cl
udin
g re
gula
r m
edia
brie
fings
) gu
ided
by
risk
com
mun
icat
ion
best
pr
actic
es,
and
achi
evin
g co
mpr
ehen
sive
geo
grap
hica
l cov
erag
e, e
vide
nced
by
reg
ular
cov
erag
e of
hea
lth is
sues
and
ris
ks in
re
leva
nt la
ngua
ges,
as
wel
l as
by m
edia
and
soc
ial
med
ia a
ctiv
ity d
urin
g an
em
erge
ncy
Sust
aina
ble
capa
city
- 5
Less
ons
lear
nt fr
om c
apac
ity le
vel 4
inte
grat
ed in
to
the
revi
sion
of n
atio
nal p
lans
for c
ontin
uous
str
en-
gthe
ning
of t
he s
yste
mRe
gula
r al
loca
tion
of r
esou
rces
for
gro
wth
and
m
aint
enan
ce o
f the
sys
tem
Effe
ctiv
e,
regu
lar
and
incl
usiv
e co
mm
unic
atio
n co
ordi
natio
n w
ith p
artn
ers
and
stak
ehol
ders
incl
u-di
ng d
efini
tion
of r
oles
, sha
ring
of r
esou
rces
and
jo
int a
ctio
n pl
ans
The
gove
rnm
ent,
part
ners
and
div
erse
med
ia o
ut-
lets
are
eng
aged
in
robu
st a
nd i
ncre
asin
gly
res-
pons
ive
colla
bora
tion
to p
rovi
de h
ealth
adv
ice,
in
clud
ing
addr
essi
ng p
eopl
e’s
conc
erns
and
ru-
mou
rs, a
nd m
isin
form
atio
n
1 -
Und
er th
e IH
R ca
paci
ty a
sses
smen
t fra
mew
ork,
onl
y on
e el
emen
t of t
he k
ey c
ompo
nent
s of
risk
com
mun
icat
ion
– p
ublic
com
mun
icat
ion
– w
as a
sses
sed.
The
focu
s w
as p
redo
min
antly
on
outp
uts
of p
ublic
com
mun
icat
ions
ac
tiviti
es. T
he re
vise
d fr
amew
ork
prop
osed
her
e ad
dres
ses
risk
com
mun
icat
ions
out
com
es. T
he fr
amew
ork
build
s on
the
exis
ting
IHR
capa
city
ass
essm
ent c
onte
nt, a
nd d
raw
s on
an
evid
ence
-bas
ed “
logi
c m
odel
” for
eva
luat
ing
emer
genc
y ris
k co
mm
unic
atio
n ou
tcom
es d
evel
oped
join
tly b
y W
HO
and
Har
vard
Sch
ool o
f Pub
lic H
ealth
in 2
014.
RE
SP
ON
D

INTERNATIONAL HEALTH REGULATIONS (2005)
90 - Joint External Evaluation Tool - Second edition
Scor
eIn
dica
tors
: Ris
k co
mm
unic
atio
nR.
5.4
Com
mun
icat
ion
enga
gem
ent w
ith a
ffec
ted
com
mun
ities
R.5.
5 Ad
dres
sing
per
cept
ions
, ris
ky b
ehav
iour
s an
d m
isin
form
atio
n
No
capa
city
- 1
No
arra
ngem
ent t
o sy
stem
atic
ally
eng
age
popu
latio
ns a
t com
mun
ity le
vel f
or
emer
genc
ies
Ther
e m
ay
be
soci
al
mob
iliza
tion,
he
alth
pr
omot
ion
or
com
mun
ity
enga
gem
ent
on h
ealth
ris
ks f
or m
ater
nal
and
child
hea
lth,
imm
uniz
atio
n,
mal
aria
, tu
berc
ulos
is,
HIV
/AID
S,
polio
, ne
glec
ted
trop
ical
di
seas
es
and
othe
r de
velo
pmen
tal p
rogr
amm
es, b
ut t
hey
are
not
syst
emat
ical
ly u
sed
for
emer
genc
ies
No
syst
em t
o ga
ther
inf
orm
atio
n on
per
cept
ions
, ris
ky b
ehav
iour
s an
d m
isin
form
atio
n to
ana
lyse
pub
lic c
once
rns
and
fear
s
Lim
ited
ca
paci
ty -
2
Com
mun
ity-l
evel
eng
agem
ent
syst
em p
artia
lly w
ith m
appi
ng o
f ex
istin
g pr
oces
ses,
pro
gram
mes
, par
tner
s an
d st
akeh
olde
rsSo
cial
m
obili
zatio
n,
beha
viou
r ch
ange
co
mm
unic
atio
n an
d co
mm
unity
en
gage
men
t in
clud
ed i
n th
e na
tiona
l ris
k co
mm
unic
atio
n st
rate
gy i
n th
e co
ntex
t of h
ealth
em
erge
ncie
sSo
me
key
stak
ehol
ders
in th
is d
omai
n id
entifi
ed a
t nat
iona
l and
inte
rmed
iate
(p
rovi
ncia
l/re
gion
al) l
evel
s
Ad h
oc s
yste
ms
in p
lace
for
gat
herin
g in
form
atio
n on
per
cept
ions
, ris
ky
beha
viou
rs a
nd m
isin
form
atio
n bu
t are
not
sys
tem
atic
ally
use
d to
gui
de th
e re
spon
se
Deve
lope
d ca
paci
ty -
3
Stak
ehol
ders
map
ped
at i
nter
med
iate
and
loc
al l
evel
s, a
nd d
ecen
tral
ized
sy
stem
(in
clud
ing
finan
cial
and
hum
an r
esou
rces
) in
pla
ce f
or c
omm
unity
en
gage
men
t in
volv
ing
com
mun
ity a
nd r
elig
ious
lead
ers,
com
mun
ity-b
ased
or
gani
zatio
ns a
nd o
ther
dec
entr
aliz
ed te
ams
Stan
dard
pr
actic
e of
de
velo
ping
in
form
atio
n ed
ucat
ion
com
mun
icat
ion
mat
eria
ls w
ith th
e in
volv
emen
t of c
omm
unity
and
key
sta
keho
lder
sCo
mm
unity
co
nsul
tatio
n m
echa
nism
s in
pl
ace
(suc
h as
ho
tline
, su
rvey
s)
A sy
stem
atic
app
roac
h fo
r ga
ther
ing
info
rmat
ion
on p
erce
ptio
ns,
risky
be
havi
ours
and
mis
info
rmat
ion
exis
ts,
but
is n
ot s
yste
mat
ical
ly u
sed
for
shap
ing
the
resp
onse
Dem
onst
rate
d ca
paci
ty –
4
Regu
lar
brie
fing,
tr
aini
ng
and
enga
gem
ent
of
soci
al
mob
iliza
tion
and
com
mun
ity e
ngag
emen
t tea
ms
incl
udin
g vo
lunt
eers
Mec
hani
sms
to h
arne
ss s
cale
-up
capa
city
exi
st a
nd a
re o
pera
tiona
l Fe
edba
ck l
oop
from
lis
teni
ng (
Dom
ain
5)3
into
com
mun
ity e
ngag
emen
t is
op
erat
iona
l
Mec
hani
sms
in p
lace
for s
yste
mat
ic g
athe
ring
of in
form
atio
n on
per
cept
ions
, ris
ky b
ehav
iour
s an
d m
isin
form
atio
n, a
nd u
sing
suc
h an
alys
is s
yste
mat
ical
ly
for s
hapi
ng th
e re
spon
se
Sust
aina
ble
capa
city
– 5
Com
mun
ities
are
equ
al p
artn
ers
in t
he r
isk
com
mun
icat
ion
proc
ess
as
evid
ence
d by
rev
iew
of
a si
mul
atio
n ex
erci
se o
r te
sted
dur
ing
a re
al h
ealth
em
erge
ncy
Feed
back
mec
hani
sm to
furt
her i
mpr
ove
this
sys
tem
and
feed
back
to im
prov
e pr
epar
edne
ss
2 - D
omai
n 5
(Dyn
amic
list
enin
g an
d ru
mou
r man
agem
ent)
sho
uld
be a
sses
sed
inde
pend
ently
as
wel
l as
in re
latio
n to
dom
ains
2 (I
nter
nal a
nd p
artn
er c
omm
unic
atio
n an
d co
ordi
natio
n), 3
(Pub
lic c
omm
unic
atio
n) a
nd 4
(Com
mun
icat
ion
enga
gem
ent w
ith a
ffect
ed c
omm
uniti
es).
3 -
Dom
ain
5. P
artn
ersh
ips:
a)
Build
ing
broa
d pa
rtne
rshi
ps f
or c
omm
unity
eng
agem
ent;
b) W
orki
ng w
ith r
elig
ious
lea
ders
; an
d c)
Wor
king
with
loc
al j
ourn
alis
ts a
nd c
omm
unity
rad
io (
sour
ce:
http
://w
ww
.ghs
pjou
rnal
.org
/co
nten
t/4/
4/62
6?ut
m_s
ourc
e=Tr
endM
D&u
tm_m
ediu
m=c
pc&u
tm_c
ampa
ign=
Glo
bal_
Hea
lth%
253A
_Sci
ence
_and
_Pra
ctic
e_Tr
endM
D_0
, acc
esse
d 25
Dec
embe
r 201
7).
RE
SP
ON
D

INTERNATIONAL HEALTH REGULATIONS (2005)
91 - Joint External Evaluation Tool - Second edition
Cont
extu
al q
uest
ions
: N/A
Tech
nica
l que
stio
ns:
R.5.
1 Ri
sk c
omm
unic
atio
n sy
stem
s fo
r unu
sual
/une
xpec
ted
even
ts a
nd e
mer
genc
ies
1.
Is th
ere
a fu
nctio
n fo
r ris
k co
mm
unic
atio
n in
the
coun
try’
s na
tiona
l res
pons
e pl
an?
2.
Are
ther
e co
mm
unic
atio
ns p
erso
nnel
or g
over
nmen
t dep
artm
ents
that
info
rmal
ly re
spon
d to
pub
lic in
form
atio
n ne
eds
durin
g em
erge
ncie
s?
3.
Is th
ere
perm
anen
t or s
urge
sta
ff de
dica
ted
to ri
sk c
omm
unic
atio
n du
ring
emer
genc
ies?
4.
Ar
e th
e ro
les
and
resp
onsi
bilit
ies
of th
e ris
k co
mm
unic
atio
n st
aff a
rtic
ulat
ed in
a re
spon
se p
lan?
5.
Ar
e th
ere
sign
ifica
nt im
prov
emen
ts th
at c
ould
be
mad
e in
the
staf
fing,
pla
tform
s, fi
nanc
ial r
esou
rces
or o
ther
fact
ors
to im
prov
e co
mm
unic
atio
ns w
ith p
ublic
an
d pa
rtne
rs d
urin
g em
erge
ncie
s?
6.
Are
ther
e sh
ared
com
mun
icat
ion
plan
s, a
gree
men
ts a
nd/o
r SO
Ps b
etw
een
othe
r re
spon
se a
genc
ies,
suc
h as
pub
lic s
afet
y, la
w e
nfor
cem
ent,
hosp
itals
, em
erge
ncy
resp
onse
, Red
Cro
ss/C
resc
ent a
nd/o
r gov
ernm
ent a
genc
ies,
suc
h as
min
istr
ies
of d
efen
ce, a
gric
ultu
re, f
ood/
drug
?7.
Is
ther
e a
dedi
cate
d bu
dget
line
for c
omm
unic
atio
ns p
erso
nnel
, mat
eria
ls a
nd a
ctiv
ities
for e
mer
genc
ies?
8.
Ar
e pl
ans
test
ed a
t lea
st o
nce
ever
y tw
o ye
ars?
9.
W
hich
gov
ernm
ent e
ntiti
es/a
genc
ies
have
the
lead
for r
isk
com
mun
icat
ion
for d
iffer
ent t
ypes
and
mag
nitu
des
of e
mer
genc
ies?
10.
Is tr
aini
ng fo
r res
pond
ing
to lo
cal h
azar
ds p
rovi
ded
to ri
sk c
omm
unic
atio
ns p
erso
nnel
? 11
. Is
ther
e an
agr
eem
ent i
nter
nal t
o th
e ag
ency
for c
lear
ance
of m
essa
ging
to th
e pu
blic
? 12
. Is
ther
e a
dedi
cate
d bu
dget
for t
he ri
sk c
omm
unic
atio
ns s
yste
m to
gro
w s
usta
inab
ly?
Addi
tiona
l inf
orm
atio
n: A
vaila
bilit
y of
the
follo
win
g re
late
d to
R.5
.1 (d
ocum
enta
tion)
l
Nat
iona
l res
pons
e pl
ans
– c
omm
unic
atio
n se
ctio
nsl
Org
aniz
atio
nal c
hart
l
Emer
genc
y ris
k co
mm
unic
atio
n st
aff p
lans
l
Job
desc
riptio
n fo
r com
mun
icat
ion
staf
f mem
bers
l
Shar
ed a
gree
men
ts w
ith re
spon
se a
genc
ies
l
Emer
genc
y re
spon
se b
udge
t sam
ple
l
Vario
us m
eetin
g no
tes
l
Exer
cise
pla
ns a
nd re
sults
l
Trai
ning
wor
ksho
ps o
bjec
tives
/res
ults
l
Mes
sage
cle
aran
ce p
lan
l
Plan
alte
ratio
nsl
Mec
hani
sm o
f sha
ring
plan
alte
ratio
nl
Long
-ter
m b
udge
t pla
n
RE
SP
ON
D

INTERNATIONAL HEALTH REGULATIONS (2005)
92 - Joint External Evaluation Tool - Second edition
R.5.
2 In
tern
al a
nd p
artn
er c
omm
unic
atio
n an
d co
ordi
natio
n fo
r em
erge
ncy
risk
com
mun
icat
ion
1.
Is th
ere
an in
form
al o
r for
mal
mec
hani
sm to
coo
rdin
ate
inte
rnal
com
mun
icat
ion
with
in th
e ag
ency
dur
ing
an e
mer
genc
y?
2.
Is th
ere
an in
form
al o
r for
mal
mec
hani
sm to
coo
rdin
ate
com
mun
icat
ion
amon
g na
tiona
l sta
keho
lder
s an
d re
spon
se a
genc
ies
durin
g an
em
erge
ncy?
3.
Is
ther
e an
info
rmal
or f
orm
al m
echa
nism
to c
oord
inat
e co
mm
unic
atio
n am
ong
inte
rnat
iona
l sta
keho
lder
s an
d re
spon
se a
genc
ies
durin
g an
em
erge
ncy?
4.
H
ave
ther
e be
en in
cide
nts
whe
re s
take
hold
er/p
artn
er a
genc
ies
have
rele
ased
con
trad
ictin
g in
form
atio
n?5.
H
ave
ther
e be
en in
stan
ces
of d
elay
s in
the
rele
ase
of in
form
atio
n du
e to
a la
ck o
f agr
eem
ent b
etw
een
key
part
ners
dur
ing
an e
mer
genc
y?
6.
Is th
ere
a fo
rmal
mec
hani
sm to
coo
rdin
ate
com
mun
icat
ion
with
the
hosp
ital a
nd h
ealth
car
e se
ctor
dur
ing
an e
mer
genc
y?
7.
Is th
ere
a fo
rmal
mec
hani
sm to
coo
rdin
ate
com
mun
icat
ion
amon
g ci
vil s
ocie
ty o
rgan
izat
ions
dur
ing
an e
mer
genc
y?
8.
Is th
ere
a fo
rmal
mec
hani
sm to
coo
rdin
ate
com
mun
icat
ion
with
the
priv
ate
sect
or d
urin
g an
em
erge
ncy?
9.
H
as a
n ex
erci
se fo
r tes
ting
com
mun
icat
ion
coor
dina
tion
with
par
tner
org
aniz
atio
ns b
een
cond
ucte
d?10
. H
as th
ere
been
a re
spon
se in
an
actu
al e
mer
genc
y th
at te
sted
com
mun
icat
ion
coor
dina
tion
with
par
tner
org
aniz
atio
ns?
11.
Is th
ere
a sy
stem
to re
gula
rly d
evel
op c
omm
unic
atio
n re
spon
se p
lans
toge
ther
with
ext
erna
l par
tner
s an
d st
akeh
olde
rs?
12.
Is th
ere
a co
ordi
nate
d bu
dget
for c
omm
unic
atio
ns re
spon
se w
ith e
xter
nal p
artn
ers
and
stak
ehol
ders
?
Addi
tiona
l inf
orm
atio
n: A
vaila
bilit
y of
the
follo
win
g re
late
d to
R.5
.2 (d
ocum
enta
tion)
l
Inte
rnal
and
ext
erna
l coo
rdin
atio
n ev
ents
l
Resp
onse
repo
rts
l
New
s st
orie
s du
ring
past
em
erge
ncie
sl
Plan
s fo
r com
mun
icat
ion
coor
dina
tion
with
ext
erna
l age
ncie
sl
Afte
r-ac
tion
repo
rts
from
exe
rcis
es o
r em
erge
ncy
resp
onse
sl
Agre
ed u
pon
resp
onse
pla
n an
d co
ordi
nate
d bu
dget
pla
n fo
r em
erge
ncy
com
mun
icat
ion
R.5.
3 P
ublic
com
mun
icat
ion
for e
mer
genc
ies
1.
Is th
ere
a fo
rmal
ized
func
tion
with
a tr
aine
d pu
blic
spo
kesp
erso
n?2.
Is
ther
e a
fast
-tra
ck p
roce
ss fo
r cle
arin
g m
edia
and
soc
ial m
edia
pro
duct
s?3.
Is
ther
e a
com
mun
icat
ion
team
ded
icat
ed to
med
ia a
nd s
ocia
l med
ia o
utre
ach
that
coo
rdin
ates
with
par
tner
s?4.
Ar
e ta
rget
aud
ienc
e an
alys
es c
ondu
cted
to b
ette
r und
erst
and
audi
ence
lang
uage
, tru
sted
info
rmat
ion
reso
urce
s an
d pr
efer
red
com
mun
icat
ion
chan
nels
?5.
Is
ther
e a
com
mun
icat
ion
stra
tegy
that
pro
activ
ely
reac
hes
out t
o a
varie
ty o
f med
ia p
latfo
rms
(suc
h as
new
spap
ers,
radi
o, te
levi
sion
, soc
ial m
edia
, Int
erne
t) fo
r tar
getin
g co
mm
unic
atio
n m
essa
ges
to s
peci
fic a
udie
nces
?6.
Is
info
rmat
ion
prov
ided
in lo
cal l
angu
ages
as
need
ed b
y th
e au
dien
ce?
7.
Is m
edia
rese
arch
con
duct
ed to
det
erm
ine
if a
mes
sage
reac
hes
the
targ
et a
udie
nce?
8.
Is p
ublic
hea
lth m
essa
ging
ada
pted
acc
ordi
ng to
the
geog
raph
ic lo
catio
n, la
ngua
ge a
nd m
edia
pre
fere
nce?
RE
SP
ON
D

INTERNATIONAL HEALTH REGULATIONS (2005)
93 - Joint External Evaluation Tool - Second edition
9.
Is th
ere
any c
ontr
ibut
ion
to a
n ev
iden
ce b
ase
of w
hich
com
mun
icat
ions
met
hods
are
bes
t ena
bled
for t
arge
t aud
ienc
es to
cha
nge
beha
viou
r dur
ing
emer
genc
ies?
10.
Is th
ere
med
ia a
nd s
ocia
l med
ia m
onito
ring
follo
wed
by
addr
essi
ng m
isin
form
atio
n qu
ickl
y?
Addi
tiona
l inf
orm
atio
n: A
vaila
bilit
y of
the
follo
win
g re
late
d to
R.5
.3 (d
ocum
enta
tion)
l
Org
aniz
atio
nal c
hart
l
Med
ia d
epar
tmen
t str
ateg
yl
Com
mun
ity o
utre
ach
plan
sl
Med
ia re
spon
se p
lans
l
Com
mun
icat
ion
rese
arch
pro
toco
ls a
nd p
ublic
atio
ns (f
orm
al/in
form
al)
l
Exam
ples
of m
isin
form
atio
n an
d m
etho
ds fo
r han
dlin
g th
em
R.5.
4 Co
mm
unic
atio
n en
gage
men
t with
aff
ecte
d co
mm
uniti
es1.
Is
ther
e a
soci
al m
obili
zatio
n, h
ealth
pro
mot
ion
or c
omm
unity
eng
agem
ent d
epar
tmen
t, te
am o
r wor
king
gro
up th
at is
use
d fo
r em
erge
ncy
resp
onse
?2.
Is
the
soci
al m
obili
zatio
n, h
ealth
pro
mot
ion
or c
omm
unity
eng
agem
ent d
epar
tmen
t or t
eam
/wor
king
gro
up in
tegr
ated
with
in th
e ov
eral
l hea
lth re
spon
se a
nd
linke
d to
the
med
ia d
epar
tmen
t/te
am/f
ocal
per
son
and
coor
dina
ted
with
key
par
tner
s?3.
D
oes
the
soci
al m
obili
zatio
n, h
ealth
pro
mot
ion
or c
omm
unity
eng
agem
ent d
epar
tmen
t/te
am/w
orki
ng g
roup
hav
e m
echa
nism
s to
reac
h ou
t to
affe
cted
or a
t-ris
k po
pula
tions
dur
ing
heal
th e
mer
genc
ies
at n
atio
nal a
s w
ell a
s pr
ovin
cial
, dis
tric
t and
loca
l lev
els?
4.
Is s
ocia
l mob
iliza
tion,
hea
lth p
rom
otio
n or
com
mun
ity e
ngag
emen
t inc
lude
d in
the
natio
nal r
espo
nse
plan
?5.
Ar
e op
port
uniti
es fo
r inf
orm
atio
n sh
arin
g or
trai
ning
regu
larly
pro
vide
d be
twee
n ex
perie
nced
com
mun
ity e
ngag
emen
t exp
erts
and
vol
unte
ers
or fo
r pot
entia
l su
rge
capa
city
to b
e us
ed d
urin
g em
erge
ncie
s?6.
Is
ther
e an
ong
oing
and
func
tioni
ng fe
edba
ck lo
op b
etw
een
at-r
isk
or a
ffect
ed p
opul
atio
ns a
nd re
spon
se a
genc
ies?
7.
Are
base
line
soci
al d
ata,
inte
llige
nce
and
anal
ysis
on
fact
ors
that
may
incr
ease
the
popu
latio
n’s
risk
to (o
r the
abi
lity
to w
ithst
and)
the
top
five
haza
rds
in
the
coun
try
(suc
h as
map
ping
of
lang
uage
s, li
ving
con
ditio
ns, r
elig
ious
/cul
tura
l pra
ctic
es/t
rust
ed c
hann
els
of c
omm
unic
atio
n, in
fluen
cers
) co
nduc
ted
or
com
mis
sion
ed?
Addi
tiona
l inf
orm
atio
n: A
vaila
bilit
y of
the
follo
win
g re
late
d to
R.5
.4 (d
ocum
enta
tion)
l
Org
aniz
atio
nal c
hart
sl
Base
line
surv
eys
and
map
s of
soc
ial d
ata
rela
ted
to in
crea
sed
risk
for t
op fi
ve h
azar
dsl
Risk
ass
essm
ents
that
add
ress
the
mos
t lik
ely
loca
l pub
lic h
ealth
thre
ats
l
Nat
iona
l res
pons
e pl
anl
Surg
e ca
paci
ty p
lan
l
Dat
a fro
m p
ublic
hea
lth h
otlin
e (re
leva
nt q
uest
ions
from
the
publ
ic, e
tc.)
l
Com
mun
ity o
utre
ach
plan
l
Afte
r-ac
tion
repo
rt fr
om a
ctua
l em
erge
ncy
or e
xerc
ise
RE
SP
ON
D

INTERNATIONAL HEALTH REGULATIONS (2005)
94 - Joint External Evaluation Tool - Second edition
R.5.
5 Ad
dres
sing
per
cept
ions
, ris
ky b
ehav
iour
s an
d m
isin
form
atio
n1.
Is
ther
e a
form
al c
omm
unic
atio
n fu
nctio
n to
mon
itor,
dete
ct a
nd a
ddre
ss p
eopl
e’s
perc
eptio
ns, u
nfou
nded
bel
iefs
, ris
ky b
ehav
iour
s an
d m
isin
form
atio
n?2.
Is
the
effe
ctiv
enes
s of
pub
lic o
utre
ach
met
hods
and
/or m
essa
ges
used
to a
ddre
ss u
nfou
nded
bel
iefs
or t
o co
rrec
t mis
info
rmat
ion
mon
itore
d?3.
Is
info
rmat
ion
on p
eopl
e’s
perc
eptio
ns, u
nfou
nded
bel
iefs
, ris
ky b
ehav
iour
s, a
nd m
isin
form
atio
n an
d st
rate
gies
to a
ddre
ss th
em re
gula
rly s
hare
d w
ith o
ther
st
akeh
olde
rs?
4.
Is c
omm
unic
atio
n fe
edba
ck, i
nclu
ding
on
perc
eptio
ns a
nd m
isin
form
atio
n, ta
ken
into
con
side
ratio
n so
as
to s
hape
an
effe
ctiv
e re
spon
se?
5.
Are
com
mun
icat
ion
resp
onse
s an
d th
e ab
ility
to a
ddre
ss p
erce
ptio
ns, r
isky
beh
avio
urs
and
mis
info
rmat
ion
to id
entif
y be
st p
ract
ice
regu
larly
eva
luat
ed?
Addi
tiona
l inf
orm
atio
n: A
vaila
bilit
y of
the
follo
win
g re
late
d to
R.5
.5 (d
ocum
enta
tion)
l
Med
ia re
spon
se p
lans
l
Dat
a fro
m p
ublic
hea
lth h
otlin
e (e
.g. r
elev
ant q
uest
ions
from
the
publ
ic)
l
Know
ledg
e, a
ttitu
de a
nd p
ract
ice
surv
eys
l
Repo
rts
from
soc
ial s
cien
tists
and
ant
hrop
olog
ists
invo
lved
in th
e re
spon
sel
Soci
al m
edia
mon
itorin
gl
Part
ner c
oord
inat
ion
mee
ting
reco
rds
RE
SP
ON
D

INTERNATIONAL HEALTH REGULATIONS (2005)
95 - Joint External Evaluation Tool - Second edition
IHR
RELA
TED
HAZ
ARDS
AN
D PO
INTS
OF
ENTR
YPO
INTS
OF
ENTR
YTa
rget
s: S
tate
s Pa
rtie
s de
sign
ate
and
mai
ntai
n co
re c
apac
ities
at i
nter
natio
nal a
irpor
ts a
nd p
orts
(and
whe
re ju
stifi
ed fo
r pub
lic h
ealth
reas
ons,
a S
tate
Par
ty m
ay
desi
gnat
e gr
ound
cro
ssin
gs) t
hat i
mpl
emen
t spe
cific
pub
lic h
ealth
mea
sure
s re
quire
d to
man
age
a va
riety
of p
ublic
hea
lth ri
sks.
As m
easu
red
by: (
1) P
ublic
hea
lth e
mer
genc
y co
ntin
genc
y pl
an fo
r des
igna
ted
poin
ts o
f ent
ry. (
2) E
vide
nce
confi
rms
core
cap
aciti
es p
resc
ribed
in th
e IH
R An
nex
1B “1
. At a
ll tim
es” a
re d
evel
oped
and
func
tioni
ng in
an
all-
haza
rd a
nd m
ultis
ecto
ral a
ppro
ach.
Desi
red
impa
ct: T
imel
y de
tect
ion
of a
nd e
ffect
ive
resp
onse
to a
ny p
oten
tial h
azar
ds th
at o
ccur
at p
oint
s of
ent
ry.
IHR
RE
LA
TE
D H
AZ
AR
DS
AN
D P
OE

INTERNATIONAL HEALTH REGULATIONS (2005)
96 - Joint External Evaluation Tool - Second edition
Scor
eIn
dica
tors
: Poi
nts
of e
ntry
PoE.
1 Ro
utin
e ca
paci
ties
esta
blis
hed
at p
oint
s of
ent
ryPo
E.2
Effe
ctiv
e pu
blic
hea
lth re
spon
se a
t poi
nts
of e
ntry
No
capa
city
- 1
No
capa
city
at p
oint
s of
ent
ry fo
r app
ropr
iate
med
ical
ser
vice
sPu
blic
hea
lth e
mer
genc
y co
ntin
genc
y pl
an1 f
or e
ach
desi
gnat
ed p
oint
of e
ntry
fo
r res
pond
ing
to p
ublic
hea
lth e
mer
genc
ies
occu
rrin
g at
poi
nts
of e
ntry
is n
ot
in p
lace
or u
nder
dev
elop
men
t.
Lim
ited
ca
paci
ty -
2
Des
igna
ted
poin
ts o
f en
try
have
acc
ess
to a
ppro
pria
te m
edic
al s
ervi
ces
incl
udin
g di
agno
stic
fac
ilitie
s fo
r th
e pr
ompt
ass
essm
ent
and
care
of
sick
tr
avel
lers
and
with
ade
quat
e st
aff,
equi
pmen
t and
pre
mis
es (A
nnex
1B,
1 (a
))
Publ
ic h
ealth
em
erge
ncy
cont
inge
ncy
plan
in p
lace
at e
ach
desi
gnat
ed p
oint
of
ent
ry f
or r
espo
ndin
g to
pub
lic h
ealth
em
erge
ncie
s oc
curr
ing
at p
oint
s of
en
try,
inte
grat
ed w
ith g
ener
ic e
mer
genc
y pr
epar
edne
ss a
nd re
spon
se p
lan
of
each
des
igna
ted
poin
t of e
ntry
, inv
olvi
ng a
ll re
leva
nt s
ecto
rs a
nd s
ervi
ces
at
poin
ts o
f ent
ry, a
nd d
evel
oped
and
dis
sem
inat
ed to
all
key
stak
ehol
ders
Deve
lope
d ca
paci
ty -
3
Des
igna
ted
poin
ts o
f ent
ry h
ave
deve
lope
d ot
her r
outin
e ca
paci
ties
pres
crib
ed
in t
he I
HR
Anne
x 1B
“1.
At
all
times
” in
add
ition
to
appr
opria
te m
edic
al
serv
ices
, suc
h as
equ
ipm
ent a
nd p
erso
nnel
for t
he tr
ansp
ort o
f sic
k tr
avel
lers
to
an
appr
opria
te m
edic
al fa
cilit
y
Publ
ic h
ealth
em
erge
ncy
cont
inge
ncy
plan
s at
des
igna
ted
poin
ts o
f ent
ry a
re
inte
grat
ed in
to th
e na
tiona
l em
erge
ncy
resp
onse
pla
n an
d ad
hoc
mea
sure
s re
late
d to
trav
elle
rs a
t poi
nts
of e
ntry
(suc
h as
refe
rral
sys
tem
, tra
nspo
rt) f
or
the
safe
tran
sfer
of s
ick
trav
elle
rs to
app
ropr
iate
med
ical
faci
litie
s, a
re in
pla
ce
Dem
onst
rate
d ca
paci
ty -
4
All r
outin
e co
re c
apac
ities
pre
scrib
ed in
the
IHR
Anne
x 1B
“1. A
t all
times
” are
de
velo
ped
and
func
tioni
ng a
s an
all-
haza
rd, m
ultis
ecto
ral a
ppro
ach
Dem
onst
rate
d ca
paci
ties2 o
f app
lyin
g re
com
men
ded
mea
sure
s to
dis
inse
ct,
dera
t, di
sinf
ect,
deco
ntam
inat
e or
oth
erw
ise
trea
t bag
gage
, car
go, c
onta
iner
s,
conv
eyan
ces,
goo
ds o
r po
stal
par
cels
. Est
ablis
hmen
t of
reg
ular
tes
ting
and
upda
ting
of a
n al
l-ha
zard
, mul
tisec
tora
l sys
tem
of
asse
ssm
ent
and
care
of
affe
cted
ani
mal
s, p
roba
bly
impl
emen
ted
thro
ugh
arra
ngem
ents
with
loca
l ve-
terin
ary
faci
litie
s
Sust
aina
ble
capa
city
- 5
All r
outin
e co
re c
apac
ities
pre
scrib
ed in
IHR
Anne
x 1B
“1.
At
all t
imes
” ar
e fu
nctio
ning
as
an a
ll-ha
zard
, mul
tisec
tora
l app
roac
h, w
ith e
vide
nce
of p
erio
dic
eval
uatio
n an
d co
ntin
uous
impr
ovem
ent
Eval
uatio
n of
effe
ctiv
enes
s in
resp
ondi
ng to
pub
lic h
ealth
eve
nts
at p
oint
s of
en
try
cond
ucte
d, a
nd e
vide
nce
of a
n ex
istin
g pe
riodi
c ev
alua
tion
and
cont
i-nu
ous
impr
ovem
ent a
re s
hare
d w
ith re
leva
nt s
take
hold
ers
1 -
Or a
gen
eric
“poi
nts
of e
ntry
” Em
erge
ncy
Prep
ared
ness
and
Res
pons
e Pl
an a
ddre
ssin
g pu
blic
hea
lth e
mer
genc
ies
as d
efine
d by
the
IHR.
2 -
Thes
e ca
paci
ties
wou
ld in
clud
e ad
optin
g m
easu
res
rela
ted
to tr
avel
lers
at p
oint
s of
ent
ry, s
uch
as a
refe
rral
sys
tem
and
tran
spor
t for
the
safe
tran
sfer
of s
ick
trav
elle
rs to
app
ropr
iate
med
ical
faci
litie
s.
Cont
extu
al q
uest
ions
:
1.
How
man
y po
ints
of e
ntry
(airp
orts
, por
ts, g
roun
d-cr
ossi
ngs)
are
ther
e in
the
coun
try?
How
man
y of
them
are
des
igna
ted?
Lis
t the
m b
y ty
pe.
2.
Do
adeq
uate
legi
slat
ion
and/
or p
olic
ies
exis
t for
pro
visi
on o
f hea
lth s
ervi
ces
at p
oint
s of
ent
ry in
the
coun
try?
Lin
k th
is q
uest
ion
to te
chni
cal a
rea
of N
atio
nal
legi
slat
ion,
pol
icy
and
finan
ce.
Tech
nica
l que
stio
ns:
PoE.
1 Ro
utin
e ca
paci
ties
esta
blis
hed
at p
oint
s of
ent
ry1.
D
o th
e de
sign
ated
poi
nts
of e
ntry
hav
e ac
cess
to a
ppro
pria
te m
edic
al s
ervi
ces,
incl
udin
g di
agno
stic
faci
litie
s fo
r the
pro
mpt
ass
essm
ent a
nd c
are
of s
ick
trav
elle
rs, w
ith a
dequ
ate
staf
f, eq
uipm
ent a
nd p
rem
ises
(Ann
ex 1
B, 1
a)?
IHR
RE
LA
TE
D H
AZ
AR
DS
AN
D P
OE
INTERNATIONAL HEALTH REGULATIONS (2005)
97 - Joint External Evaluation Tool - Second edition
2.
Do
thes
e po
ints
of e
ntry
pro
vide
acc
ess
to e
quip
men
t and
per
sonn
el fo
r the
tran
spor
t of s
ick
trav
elle
rs to
an
appr
opria
te m
edic
al fa
cilit
y?3.
D
o th
ese
poin
ts o
f ent
ry c
arry
out
insp
ectio
n pr
ogra
mm
es to
ens
ure
safe
env
ironm
ent a
t poi
nts
of e
ntry
faci
litie
s?4.
Is
ther
e ev
iden
ce o
f con
trol o
f vec
tors
and
rese
rvoi
rs in
and
nea
r poi
nts
of e
ntry
(Ann
ex 1
b, A
rt. 1
e)?
Are
ther
e sp
ecifi
c pr
ogra
mm
es fo
r thi
s?
5.
Doe
s th
e co
untr
y ha
ve t
rain
ed p
erso
nnel
for
the
insp
ectio
n of
con
veya
nces
ava
ilabl
e at
des
igna
ted
poin
ts o
f en
try
(Ann
ex 1
b, A
rt. 1
c)?
If no
t, is
the
re a
m
echa
nism
to b
ring
them
from
out
side
?
PoE.
2 Ef
fect
ive
publ
ic h
ealth
resp
onse
at p
oint
s of
ent
ry1.
H
as th
e co
untr
y in
tegr
ated
act
iviti
es c
once
rnin
g po
ints
of e
ntry
(suc
h as
for e
arly
det
ectio
n, a
sses
smen
t, no
tifica
tion,
repo
rt o
f eve
nts)
into
nat
iona
l em
erge
ncy
resp
onse
pla
ns?
2.
Is th
e pu
blic
hea
lth e
mer
genc
y co
ntin
genc
y pl
an fo
r res
pond
ing
to p
ublic
hea
lth e
mer
genc
ies
occu
rrin
g at
poi
nts
of e
ntry
inte
grat
ed w
ith g
ener
ic e
mer
genc
y pr
epar
edne
ss a
nd re
spon
se p
lan
of e
ach
indi
vidu
al p
oint
of e
ntry
. a.
Doe
s it
invo
lve
rele
vant
sec
tors
and
ser
vice
s at
poi
nts
of e
ntry
(suc
h as
imm
igra
tion,
tran
spor
tatio
n, s
ecur
ity, m
edia
)?b.
Is
it de
velo
ped
and
diss
emin
ated
to a
ll st
akeh
olde
rs?
3.
Do
the
desi
gnat
ed p
oint
s of
ent
ry h
ave
capa
citie
s to
app
ly re
com
men
ded
heal
th m
easu
res
rela
ted
to tr
avel
lers
at p
oint
s of
ent
ry (s
uch
as a
sys
tem
in p
lace
fo
r saf
e re
ferr
al a
nd tr
ansf
er o
f sic
k tr
avel
lers
to a
ppro
pria
te m
edic
al fa
cilit
ies,
with
MoU
s, S
OPs
, tra
ined
sta
ff, e
quip
men
t and
regu
lar e
xcha
nge
of in
form
atio
n be
twee
n po
ints
of e
ntry
, hea
lth a
utho
ritie
s an
d fa
cilit
ies
for a
ll de
sign
ated
poi
nts
of e
ntry
)?4.
D
o th
e de
sign
ated
poi
nts
of e
ntry
hav
e ca
paci
ties
to a
pply
reco
mm
ende
d m
easu
res
to d
isin
sect
, der
at, d
isin
fect
, dec
onta
min
ate
or o
ther
wis
e tre
at b
agga
ge,
carg
o, c
onta
iner
s, c
onve
yanc
es, g
oods
or p
osta
l par
cels
, inc
ludi
ng w
hen
appr
opria
te, a
t loc
atio
ns s
peci
ally
des
igna
ted
and
equi
pped
for t
his
purp
ose?
5.
H
as t
he c
ount
ry e
valu
ated
the
effe
ctiv
enes
s of
poi
nts
of e
ntry
in r
espo
ndin
g to
pub
lic h
ealth
eve
nts
at p
oint
s of
ent
ry?
If ye
s, is
it s
hare
d w
ith r
elev
ant
stak
ehol
ders
and
upd
ated
regu
larly
?
Doc
umen
tatio
n or
evi
denc
e fo
r lev
el o
f cap
abili
ty:
1.
Doc
umen
ted,
regu
larly
-upd
ated
and
test
ed n
atio
nal g
uide
lines
, and
SO
Ps to
refle
ct a
ll re
leva
nt te
chni
cal a
nd o
pera
tiona
l gui
danc
e to
ols
for p
oint
s of
ent
ry in
pl
ace
and
diss
emin
ated
to a
ll re
leva
nt s
ecto
rs in
clud
ing
for:
a. d
etec
tion,
repo
rtin
g an
d re
spon
se to
eve
nts
rela
ted
to tr
avel
and
tran
spor
t;b.
pub
lic h
ealth
mea
sure
s to
be
appl
ied
at p
oint
s of
ent
ry t
hat
may
be
reco
mm
ende
d by
the
WH
O (
such
as
exit/
entr
y sc
reen
ing,
isol
atio
n, q
uara
ntin
e,
cont
act t
raci
ng);
and
c. a
pplic
atio
n of
oth
er p
ublic
hea
lth m
easu
res
that
cou
ld a
ffect
inte
rnat
iona
l tra
vel a
nd tr
ansp
ort.
2.
Doc
umen
tatio
n av
aila
ble
for a
ll re
leva
nt te
chni
cal a
nd o
pera
tiona
l gui
danc
e fo
r poi
nts
of e
ntry
– A
nnex
1B,
1e
“to
prov
ide
as fa
r as
prac
ticab
le a
pro
gram
me
and
trai
ned
pers
onne
l for
the
cont
rol o
f vec
tors
and
rese
rvoi
rs in
and
nea
r poi
nts
of e
ntry
”.
IHR
RE
LA
TE
D H
AZ
AR
DS
AN
D P
OE

INTERNATIONAL HEALTH REGULATIONS (2005)
98 - Joint External Evaluation Tool - Second edition
3.
Doc
umen
tatio
n av
aila
ble
on, r
egul
arly
-upd
ated
and
test
ed n
atio
nal g
uide
lines
and
SO
Ps to
refle
ct a
ll re
leva
nt te
chni
cal a
nd o
pera
tiona
l gui
danc
e to
ols
for
poin
ts o
f en
try
in p
lace
and
the
sam
e di
ssem
inat
ed t
o al
l rel
evan
t se
ctor
s in
clud
ing
appl
icat
ion
of r
ecom
men
ded
mea
sure
s to
dis
inse
ct, d
erat
, dis
infe
ct,
deco
ntam
inat
e or
oth
erw
ise
treat
bag
gage
, car
go, c
onta
iner
s, c
onve
yanc
es, g
oods
or
post
al p
arce
ls in
clud
ing,
whe
n ap
prop
riate
, at
loca
tions
spe
cial
ly
desi
gnat
ed a
nd e
quip
ped
for t
his
purp
ose.
4.
Doc
umen
tatio
n on
sys
tem
atic
col
lect
ion
with
sta
ndar
dize
d to
ols,
ana
lysi
s an
d di
ssem
inat
ion
of d
ata
on p
ublic
hea
lth e
vent
s oc
curr
ing
at p
oint
s of
ent
ry, w
ith
upda
ted
list o
f prio
rity
cond
ition
s fo
r not
ifica
tion,
bas
elin
e da
ta tr
ends
, and
thre
shol
ds fo
r ale
rt a
nd ti
mel
y ac
tion
(i.e.
per
nat
iona
l sta
ndar
ds),
repo
rtin
g (u
sing
st
anda
rd re
port
ing
form
ats
and
tool
s), a
nd p
rovi
ding
tim
ely
and
regu
lar f
eedb
ack
on s
urve
illan
ce d
ata
and
trend
s to
rele
vant
sta
keho
lder
s us
ing
stan
dard
ized
fe
edba
ck fo
rmat
s (s
uch
as E
pi b
ulle
tins,
ele
ctro
nic
sum
mar
ies,
new
slet
ter,
surv
eilla
nce
repo
rts)
. 5.
D
ocum
enta
tion
of re
gula
r rec
eipt
of p
oint
s of
ent
ry fi
ndin
gs b
y na
tiona
l sur
veill
ance
uni
t is
avai
labl
e.
Addi
tiona
l too
ls:
l
Poin
ts o
f ent
ry c
heck
list i
n th
e “A
sses
smen
t too
l for
cor
e ca
paci
ty re
quire
men
ts a
t des
igna
ted
airp
orts
, por
ts a
nd g
roun
d cr
ossi
ngs”
. WH
O/H
SE/I
HR/
LYO
/200
9.9
(http
://w
ww
.who
.int/
ihr/
port
s_ai
rpor
ts/P
oE/e
n/in
dex.
htm
l, ac
cess
ed 2
8 N
ovem
ber 2
017)
.
IHR
RE
LA
TE
D H
AZ
AR
DS
AN
D P
OE

INTERNATIONAL HEALTH REGULATIONS (2005)
99 - Joint External Evaluation Tool - Second edition
CHEM
ICAL
EVE
NTS
Targ
et: S
tate
s Pa
rtie
s w
ith s
urve
illan
ce a
nd re
spon
se c
apac
ity fo
r che
mic
al ri
sks
or e
vent
s. T
his
requ
ires
effe
ctiv
e co
mm
unic
atio
n an
d co
llabo
ratio
n am
ong
the
sect
ors
resp
onsi
ble
for c
hem
ical
saf
ety,
indu
strie
s, tr
ansp
orta
tion
and
safe
dis
posa
l, an
imal
hea
lth a
nd th
e en
viro
nmen
t.
As m
easu
red
by: (
1) M
echa
nism
s es
tabl
ishe
d an
d fu
nctio
ning
for
det
ectin
g an
d re
spon
ding
to
chem
ical
eve
nts
or e
mer
genc
ies.
(2)
Exi
sten
ce o
f an
ena
blin
g en
viro
nmen
t, in
clud
ing
natio
nal p
olic
ies
or p
lans
or l
egis
latio
n in
pla
ce fo
r man
agem
ent o
f che
mic
al e
vent
s.
Desi
red
impa
ct: T
imel
y de
tect
ion
of a
nd e
ffect
ive
resp
onse
to p
oten
tial c
hem
ical
risk
s an
d/or
eve
nts
in c
olla
bora
tion
with
oth
er s
ecto
rs re
spon
sibl
e fo
r che
mic
al
safe
ty, i
ndus
trie
s, tr
ansp
orta
tion
and
safe
dis
posa
l.
IHR
RE
LA
TE
D H
AZ
AR
DS
AN
D P
OE

INTERNATIONAL HEALTH REGULATIONS (2005)
100 - Joint External Evaluation Tool - Second edition
Scor
eIn
dica
tors
: Che
mic
al e
vent
s1,2
CE.1
Mec
hani
sms
esta
blis
hed
and
func
tioni
ng fo
r det
ectin
g3 and
resp
ondi
ng
to c
hem
ical
eve
nts
or e
mer
genc
ies
CE.2
Ena
blin
g en
viro
nmen
t in
plac
e fo
r man
agem
ent o
f che
mic
al e
vent
s
No
capa
city
- 1
No
mec
hani
sm in
pla
ceN
atio
nal p
olic
ies,
pla
ns o
r le
gisl
atio
n fo
r ch
emic
al e
vent
sur
veill
ance
, ale
rt
and
resp
onse
do
not e
xist
Lim
ited
ca
paci
ty -
2G
uide
lines
or
man
uals
on
surv
eilla
nce,
ass
essm
ent
and
man
agem
ent
of
chem
ical
eve
nts,
into
xica
tion
and
pois
onin
g ar
e av
aila
ble
Nat
iona
l pol
icie
s, p
lans
or
legi
slat
ion
for
chem
ical
eve
nt s
urve
illan
ce, a
lert
4 an
d re
spon
se e
xist
Deve
lope
d ca
paci
ty -
3
Surv
eilla
nce
is i
n pl
ace
for
chem
ical
eve
nts,
int
oxic
atio
n an
d po
ison
ings
w
ith la
bora
tory
cap
acity
or
acce
ss to
labo
rato
ry c
apac
ity to
con
firm
prio
rity
chem
ical
eve
nts
A ch
emic
al e
vent
resp
onse
pla
n is
in p
lace
that
defi
nes
role
s an
d re
spon
sibi
-lit
ies
of re
leva
nt a
genc
ies
and
take
s in
to a
ccou
nt a
ll m
ajor
haz
ard
site
s an
d fa
cilit
ies
Dem
onst
rate
d ca
paci
ty -
4
Tim
ely
and
syst
emat
ic in
form
atio
n ex
chan
ge b
etw
een
appr
opria
te c
hem
ical
un
its5 ,
surv
eilla
nce
units
and
oth
er r
elev
ant
sect
ors
abou
t ur
gent
che
mic
al
even
ts a
nd p
oten
tial c
hem
ical
risk
s an
d th
eir r
espo
nse
Func
tiona
l mec
hani
sms
for
mul
tisec
tora
l coo
rdin
atio
n an
d co
llabo
ratio
n to
m
anag
e ch
emic
al e
vent
s ar
e in
pla
ce in
clud
ing
invo
lvem
ent
in in
tern
atio
nal
chem
ical
/tox
icol
ogic
al n
etw
orks
Sust
aina
ble
capa
city
- 5
Adeq
uate
ly r
esou
rced
poi
son
cent
re(s
)6 ar
e in
pla
ce a
nd t
he c
ount
ry h
as a
de
mon
stra
ted
abili
ty to
resp
ond
to c
hem
ical
em
erge
ncie
s in
all
regi
ons7
A ch
emic
al
even
t re
spon
se
plan
ha
s be
en
test
ed
thro
ugh
occu
r-re
nce
of a
rea
l ev
ent
or t
hrou
gh s
imul
atio
n ex
erci
se a
nd i
s up
date
d as
ne
eded
1- W
hile
the
capa
citie
s fo
r thi
s te
chni
cal a
rea
shou
ld b
e av
aila
ble
coun
tryw
ide,
the
infr
astr
uctu
re d
oes
not n
eed
to b
e pr
esen
t in
all g
eogr
aphi
cal a
reas
. 2
- In
dica
tors
refe
r to
dete
ctio
n of
and
resp
onse
to c
hem
ical
eve
nts
and
enab
ling
envi
ronm
ent f
or m
anag
emen
t of c
hem
ical
eve
nts
in p
lace
with
app
ropr
iate
legi
slat
ion,
law
s or
pol
icy
and
with
invo
lvem
ent o
f mul
tiple
sec
tors
.3
- D
etec
tion
capa
city
als
o in
clud
es n
ot o
nly
surv
eilla
nce
but a
lso
the
labo
rato
ry c
apac
ity re
quire
d fo
r the
ver
ifica
tion
of a
ny e
vent
s.4
- El
emen
ts o
f ale
rt in
clud
e SO
Ps fo
r cov
erag
e, c
riter
ia o
f whe
n an
d ho
w to
ale
rt, d
uty
rost
ers,
etc
.5
- Su
ch a
s ch
emic
al s
urve
illan
ce, e
nviro
nmen
tal m
onito
ring
and
chem
ical
inci
dent
repo
rtin
g.6
- Th
e po
ison
s ce
ntre
sho
uld
be s
uffic
ient
ly s
taffe
d an
d re
sour
ced
to p
rovi
de a
robu
st a
nd re
liabl
e 24
/7 s
ervi
ce. T
he p
oiso
ns c
entr
e sh
ould
be
wel
l use
d by
the
popu
latio
n it
serv
es (c
heck
num
ber o
f cal
ls p
er d
ay).
Refe
r to
Gui
delin
es
for p
oiso
ns c
ontr
ol. G
enev
a: W
orld
Hea
lth O
rgan
izat
ion;
199
7 (h
ttp:
//ap
ps.w
ho.in
t/iri
s/bi
tstr
eam
/106
65/4
1966
/1/9
2415
4487
2_en
g.pd
f, ac
cess
ed 1
Dec
embe
r 201
7).
7 -
This
incl
udes
set
ting
min
imum
requ
irem
ents
for:
loca
l em
erge
ncy
plan
ning
and
resp
onse
act
iviti
es (i
.e. a
rran
gem
ents
for s
calin
g up
cap
abili
ties
of lo
cal e
mer
genc
y re
spon
se, n
atio
nal s
uppo
rt m
echa
nism
s, in
fras
truc
ture
and
al
ertin
g m
echa
nism
s); i
nspe
ctio
n of
haz
ardo
us s
ites
and
asse
ssm
ent o
f em
erge
ncy
plan
s; a
nd o
pera
tors
to c
ompl
y an
d lia
ison
with
loca
l gov
ernm
ents
(see
als
o: W
HO
man
ual:
The
publ
ic h
ealth
man
agem
ent o
f che
mic
al in
cide
nts.
G
enev
a: W
orld
Hea
lth O
rgan
izat
ion;
200
9 (h
ttp:
//w
ww
.who
.int/
envi
ronm
enta
l_he
alth
_em
erge
ncie
s/pu
blic
atio
ns/M
anua
l_Ch
emic
al_I
ncid
ents
/en/
, acc
esse
d 1
Dec
embe
r 201
7)).
Cont
extu
al q
uest
ions
:
1.
Has
a n
atio
nal c
hem
ical
s pr
ofile
bee
n de
velo
ped
in th
e pa
st fi
ve y
ears
? If
appl
icab
le, d
escr
ibe
outc
ome/
prov
ide
repo
rt.
2.
Hav
e ch
emic
al ri
sks
been
ass
esse
d fo
r prio
rity
chem
ical
s in
the
past
five
yea
rs, f
or e
xam
ple
in te
rms
of im
pact
on
mor
bidi
ty a
nd m
orta
lity?
3.
Hav
e th
ere
been
any
maj
or c
hem
ical
inci
dent
s in
the
past
five
yea
rs?
4.
Are
any
inte
rnat
iona
l che
mic
al c
onve
ntio
ns/a
gree
men
ts ra
tified
/impl
emen
ted?
a. I
s th
e Ro
tter
dam
Con
vent
ion
on th
e Pr
ior I
nfor
med
Con
sent
Pro
cedu
re fo
r Cer
tain
Haz
ardo
us C
hem
ical
s in
Inte
rnat
iona
l Tra
de ra
tified
?b.
Is
the
Stoc
khol
m C
onve
ntio
n on
Per
sist
ent O
rgan
ic P
ollu
tant
s ra
tified
?c.
Is
the
Base
l Con
vent
ion
on th
e Co
ntro
l of T
rans
boun
dary
Mov
emen
ts o
f Haz
ardo
us W
aste
s an
d th
eir D
ispo
sal r
atifi
ed?
d. I
s th
e U
nite
d N
atio
ns E
cono
mic
Com
mis
sion
for E
urop
e Co
nven
tion
on th
e Tr
ansb
ound
ary
Effe
cts
of In
dust
rial A
ccid
ents
ratifi
ed?
IHR
RE
LA
TE
D H
AZ
AR
DS
AN
D P
OE

INTERNATIONAL HEALTH REGULATIONS (2005)
101 - Joint External Evaluation Tool - Second edition
e. I
s th
e In
tern
atio
nal L
abou
r Org
aniz
atio
n Co
nven
tion
174
on P
reve
ntio
n of
Maj
or In
dust
rial A
ccid
ents
ratifi
ed?
f. Is
the
Inte
rnat
iona
l Lab
our O
rgan
izat
ion
Conv
entio
n 17
0 on
Saf
ety
in th
e U
se o
f Che
mic
als
at W
ork
ratifi
ed?
5.
Is th
e co
untr
y w
orki
ng to
war
ds a
chie
ving
sus
tain
able
dev
elop
men
t goa
ls 3
.9 a
nd 1
2.4
(see
als
o St
rate
gic
Appr
oach
to In
tern
atio
nal C
hem
ical
s M
anag
emen
t (S
AICM
) goa
l)? 8,
9
Tech
nica
l que
stio
ns:
CE.1
Mec
hani
sms
esta
blis
hed
and
func
tioni
ng fo
r det
ectin
g an
d re
spon
ding
to c
hem
ical
eve
nts
or e
mer
genc
ies
1.
Are
guid
elin
es o
r man
uals
on
the
surv
eilla
nce,
ass
essm
ent a
nd m
anag
emen
t of c
hem
ical
eve
nts,
into
xica
tion
and
pois
onin
g av
aila
ble?
a. A
re th
ese
impl
emen
ted?
b. A
re th
ese
upda
ted
afte
r the
eve
nts
or fo
llow
-up
exer
cise
s, o
r upd
ated
regu
larly
?2.
Is
ther
e ch
emic
al in
cide
nt s
urve
illan
ce?
a. I
s th
ere
an a
utho
rity/
inst
itute
/age
ncy
with
prim
ary
resp
onsi
bilit
y fo
r che
mic
als
and
surv
eilla
nce/
mon
itorin
g?b.
Is
ther
e an
effi
cien
t inf
orm
atio
n flo
w in
che
mic
als
surv
eilla
nce/
mon
itorin
g?c.
Is
ther
e su
rvei
llanc
e of
sen
tinel
hea
lth e
vent
s th
at m
ay s
igna
l a h
azar
dous
che
mic
al e
xpos
ure?
d. I
s th
ere
envi
ronm
enta
l mon
itorin
g (w
ater
, air,
soi
l, se
dim
ent)
with
rega
rd to
che
mic
al h
azar
ds?
e. I
s th
ere
mon
itorin
g of
con
sum
er p
rodu
cts
(food
stuf
fs a
nd g
oods
) with
rega
rd to
che
mic
al h
azar
ds?
3.
Are
ther
e pr
oced
ures
for r
isk
asse
ssm
ent i
n ch
emic
als
surv
eilla
nce/
mon
itorin
g to
info
rm a
che
mic
al e
vent
resp
onse
?4.
Is
labo
rato
ry c
apac
ity a
vaila
ble
for s
yste
mat
ic a
naly
sis?
5.
Are
curr
ent h
uman
reso
urce
s su
ffici
ent t
o m
eet t
he n
eeds
for m
anag
ing
chem
ical
eve
nts?
6.
Are
curr
ent fi
nanc
ial r
esou
rces
suf
ficie
nt to
mee
t the
nee
ds fo
r che
mic
al s
afet
y?7.
Ar
e in
vest
igat
ion
repo
rts
prod
uced
in c
hem
ical
s su
rvei
llanc
e/m
onito
ring?
8.
Is th
ere
regu
lar (
i.e. w
eekl
y, m
onth
ly o
r yea
rly) f
eedb
ack
of d
ata
and
resp
onse
act
iviti
es in
che
mic
als
surv
eilla
nce/
mon
itorin
g?9.
Is
ther
e an
inve
ntor
y of
refe
renc
e he
alth
car
e fa
cilit
ies
for t
he d
iagn
oses
and
trea
tmen
t of c
hem
ical
poi
soni
ng c
ases
?10
. Ar
e th
ere
prot
ocol
s/gu
idel
ines
for c
ase
man
agem
ent w
ith re
gard
to c
hem
ical
haz
ards
?11
. Ar
e th
ere
pois
on c
entre
(s)?
How
do
they
func
tion
and
fit in
to th
e he
alth
car
e sy
stem
?
CE.2
Ena
blin
g en
viro
nmen
t in
plac
e fo
r man
agem
ent o
f che
mic
al e
vent
s 1.
Is
ther
e a
stra
tegi
c pl
an to
stre
ngth
en th
e as
sess
men
t and
man
agem
ent o
f che
mic
als
(e.g
. a n
atio
nal c
hem
ical
s pr
ofile
)? Is
it u
p-to
-dat
e an
d im
plem
ente
d?2.
D
oes
chem
ical
s le
gisl
atio
n pr
ovid
e co
mpr
ehen
sive
cov
erag
e? S
ome
area
s th
at m
ay b
e co
vere
d by
legi
slat
ion
not s
peci
fic fo
r che
mic
als
shou
ld b
e co
nsid
ered
, su
ch a
s:
8 -
In a
dopt
ing
the
2030
Age
nda
for
Sust
aina
ble
Dev
elop
men
t, go
vern
men
ts r
ecog
nize
d th
e co
ntin
ued
impo
rtan
ce o
f so
und
man
agem
ent
of c
hem
ical
s fo
r th
e pr
otec
tion
of h
uman
hea
lth, p
artic
ular
ly in
tar
get
3.9
whi
ch is
to
subs
tant
ially
redu
ce th
e nu
mbe
r of d
eath
s an
d ill
ness
es fr
om h
azar
dous
che
mic
als
and
air,
wat
er a
nd s
oil p
ollu
tion
and
cont
amin
atio
n by
203
0, a
s w
ell a
s ta
rget
12.
4 w
hich
cal
ls fo
r sou
nd m
anag
emen
t of c
hem
ical
s an
d al
l was
tes
by 2
020
to m
inim
ize
adve
rse
impa
cts
on h
uman
hea
lth a
nd th
e en
viro
nmen
t.9
- Th
e SA
ICM
goa
l is
that
by
2020
, che
mic
als
will
be
prod
uced
and
use
d in
way
s th
at m
inim
ize
sign
ifica
nt a
dver
se im
pact
s on
hum
an h
ealth
and
the
envi
ronm
ent.
IHR
RE
LA
TE
D H
AZ
AR
DS
AN
D P
OE

INTERNATIONAL HEALTH REGULATIONS (2005)
102 - Joint External Evaluation Tool - Second edition
a. h
azar
dous
site
s re
gist
ratio
nb.
con
trol
of h
azar
dous
site
s (t
hrou
gh s
afet
y re
port
s an
d sa
fety
man
agem
ent s
yste
ms)
c. o
n-si
te e
mer
genc
y pl
ans
d. o
ff-si
te e
mer
genc
y pl
ans
e. s
iting
and
land
use
pla
nnin
gf.
cont
rol o
f pro
cedu
res
and
site
s fo
r dis
posa
l of h
azar
dous
was
teg.
con
trol
of c
onta
min
ated
land
, wat
er (d
rinki
ng a
nd o
ther
), cr
ops,
food
stuf
fsh.
nat
iona
l and
inte
rnat
iona
l tra
nspo
rt/t
rade
of d
ange
rous
goo
ds o
r sub
stan
ces
i. ha
zard
ous
subs
tanc
es re
gist
ratio
nj.
cont
rol o
f lab
ellin
g an
d ac
com
pany
ing
safe
ty in
form
atio
n fo
r haz
ardo
us s
ubst
ance
sk.
ins
pect
ion/
mon
itorin
g an
d en
forc
emen
tl.
publ
ic c
omm
unic
atio
nm
. inc
iden
t doc
umen
tatio
n an
d re
port
ing
n. i
ncid
ent i
nves
tigat
ion
o. e
pide
mio
logi
cal a
nd m
edic
al fo
llow
-up
p. o
ccup
atio
nal h
ealth
.3.
Is
ther
e a
natio
nal c
oord
inat
ing
body
/com
mitt
ee w
ith re
gard
to th
e as
sess
men
t and
man
agem
ent o
f che
mic
als?
4.
Is th
ere
a pu
blic
hea
lth p
lan
for c
hem
ical
inci
dent
s/em
erge
ncie
s?
5.
Doe
s a
publ
ic h
ealth
pla
n fo
r che
mic
al in
cide
nts/
emer
genc
ies
cons
ider
the
rang
e of
func
tions
requ
ired
in a
cris
is?
Des
crib
e, if
app
licab
le. C
onsi
der t
he a
vaila
bilit
y of
reso
urce
s an
d SO
Ps a
nd th
e fo
llow
ing
aspe
cts:
a. r
oles
and
resp
onsi
bilit
ies
b. p
ublic
com
mun
icat
ion
c. r
efer
ral,
tran
spor
t and
trea
tmen
t of l
arge
num
bers
of a
ffect
ed in
divi
dual
sd.
sto
ckpi
ling
of e
quip
men
t and
med
icat
ion
e. f
ollo
w-u
p of
pat
ient
sf.
deco
ntam
inat
ion
of p
eopl
e, p
rem
ises
and
env
ironm
ent
g. r
egul
ar e
valu
atio
n/re
visi
on o
f pla
nh.
res
tric
tions
, eva
cuat
ion
i. em
erge
ncy
fund
sj.
exer
cise
s or
gani
zed
on a
regu
lar b
asis
to te
st a
nd re
vise
the
plan
.6.
Ar
e th
ere
mul
tisec
tora
l/int
erdi
scip
linar
y co
ordi
natio
n m
echa
nism
s w
ith re
gard
to c
hem
ical
saf
ety?
If
appl
icab
le, d
escr
ibe
mec
hani
sms
and
indi
cate
sho
rtco
min
gs. C
oord
inat
ion
mec
hani
sms
coul
d co
nsid
er:
a. h
ealth
b. e
nviro
nmen
t
IHR
RE
LA
TE
D H
AZ
AR
DS
AN
D P
OE

INTERNATIONAL HEALTH REGULATIONS (2005)
103 - Joint External Evaluation Tool - Second edition
c. a
gric
ultu
red.
Nat
iona
l IH
R Fo
cal P
oint
e. a
ll pu
blic
hea
lth le
vels
(loc
al, i
nter
med
iate
and
nat
iona
l)f.
emer
genc
y pr
epar
edne
ssg.
em
erge
ncy
serv
ices
(fire
, pol
ice,
am
bula
nce,
med
ical
resp
onde
rs)
h. c
onsu
mer
saf
ety
i. ad
min
istr
ativ
e/po
litic
al a
utho
ritie
s at
all
leve
ls (l
ocal
, int
erm
edia
te, n
atio
nal)
j. ha
zard
ous
site
sk.
met
eoro
logi
cal s
ervi
ces
l. po
ints
of e
ntry
(por
ts, a
irpor
ts, g
roun
d cr
ossi
ngs)
, in
part
icul
ar th
ose
desi
gnat
ed u
nder
the
IHR
m. t
rans
port
n. p
rivat
e se
ctor
/ind
ustr
yo.
poi
son
cent
re(s
)p.
nat
iona
l sur
veill
ance
inst
itute
(s) w
ith re
gard
to c
hem
ical
saf
ety
q. r
efer
ence
labo
rato
ry(ie
s) w
ith re
gard
to c
hem
ical
saf
ety
r. re
fere
nce
heal
th c
are
faci
litie
s w
ith re
gard
to c
hem
ical
saf
ety.
7.
In th
e ev
ent o
f a p
ublic
hea
lth e
mer
genc
y of
che
mic
al o
rigin
, cou
ld a
bud
get b
e m
obili
zed
to m
eet a
dditi
onal
dem
ands
?8.
Is
ther
e an
aud
it/ev
alua
tion
syst
em fo
r exe
rcis
es/r
espo
nses
?9.
Is
ther
e in
volv
emen
t in
inte
rnat
iona
l che
mic
al/t
oxic
olog
ical
net
wor
ks (e
.g. I
NTO
X)?
10.
Is th
ere
a ch
emic
al d
atab
ase
or d
ata
bank
ava
ilabl
e at
all
times
(e.g
. IN
CHEM
)?
IHR
RE
LA
TE
D H
AZ
AR
DS
AN
D P
OE

INTERNATIONAL HEALTH REGULATIONS (2005)
104 - Joint External Evaluation Tool - Second edition
RAD
IATI
ON
EM
ERG
ENCI
ESTa
rget
: Sta
tes
Part
ies
shou
ld h
ave
surv
eilla
nce
and
resp
onse
cap
acity
for r
adio
logi
cal e
mer
genc
ies
and
nucl
ear a
ccid
ents
. Thi
s re
quire
s ef
fect
ive
coor
dina
tion
amon
g al
l sec
tors
invo
lved
in ra
diat
ion
emer
genc
ies
prep
ared
ness
and
resp
onse
.
As m
easu
red
by: (
1) M
echa
nism
s es
tabl
ishe
d an
d fu
nctio
ning
for d
etec
ting
and
resp
ondi
ng to
radi
olog
ical
em
erge
ncie
s. (2
) Exi
sten
ce o
f an
enab
ling
envi
ronm
ent,
incl
udin
g na
tiona
l pol
icie
s or
pla
ns o
r leg
isla
tion
in p
lace
for t
he m
anag
emen
t of r
adio
logi
cal e
mer
genc
ies.
Desi
red
impa
ct: T
imel
y de
tect
ion
and
effe
ctiv
e re
spon
se to
pot
entia
l rad
iolo
gica
l em
erge
ncie
s an
d nu
clea
r acc
iden
ts in
a c
ross
-sec
tora
l coo
rdin
ated
man
ner.
IHR
RE
LA
TE
D H
AZ
AR
DS
AN
D P
OE

INTERNATIONAL HEALTH REGULATIONS (2005)
105 - Joint External Evaluation Tool - Second edition
Scor
eIn
dica
tors
: Rad
iatio
n em
erge
ncie
s1
RE.1
Mec
hani
sms
esta
blis
hed
and
func
tioni
ng fo
r det
ectin
g2 and
resp
ondi
ng
to ra
diol
ogic
al a
nd n
ucle
ar e
mer
genc
ies
RE.2
Ena
blin
g en
viro
nmen
t in
pla
ce f
or m
anag
emen
t of
rad
iolo
gica
l an
d nu
clea
r em
erge
ncie
s
No
capa
city
- 1
Nat
iona
l po
licie
s, s
trat
egie
s or
pla
ns f
or t
he d
etec
tion,
ass
essm
ent,
and
resp
onse
to ra
diat
ion
emer
genc
ies
are
not e
stab
lishe
dN
o co
ordi
natio
n an
d co
mm
unic
atio
n m
echa
nism
bet
wee
n na
tiona
l aut
hori-
ties
resp
onsi
ble
for r
adio
logi
cal a
nd n
ucle
ar e
vent
s w
ith h
ealth
min
istr
y an
d/or
Nat
iona
l IH
R Fo
cal P
oint
Lim
ited
ca
paci
ty -
2
Nat
iona
l po
licie
s, s
trat
egie
s or
pla
ns f
or t
he d
etec
tion,
ass
essm
ent,
and
resp
onse
to ra
diat
ion
emer
genc
ies
are
esta
blis
hed
and
radi
atio
n m
onito
ring
mec
hani
sms
exis
t for
radi
atio
n em
erge
ncie
s th
at m
ay c
onst
itute
a P
HEI
C
Nat
iona
l aut
horit
ies
resp
onsi
ble
for
radi
olog
ical
and
nuc
lear
eve
nts
have
a
desi
gnat
ed f
ocal
poi
nt f
or c
oord
inat
ion
and
com
mun
icat
ion
with
the
hea
lth
min
istr
y an
d/or
Nat
iona
l IH
R Fo
cal P
oint
Deve
lope
d ca
paci
ty -
3
Tech
nica
l gu
idel
ines
or
SOPs
dev
elop
ed,
eval
uate
d an
d up
date
d fo
r th
e m
anag
emen
t of r
adia
tion
emer
genc
ies
(incl
udin
g ris
k as
sess
men
t, re
port
ing,
ev
ent c
onfir
mat
ion
and
notifi
catio
n, a
nd in
vest
igat
ion)
A ra
diat
ion
emer
genc
y re
spon
se p
lan
exis
ts (
coul
d be
par
t of
the
nat
iona
l em
erge
ncy
resp
onse
pla
n) a
nd n
atio
nal p
olic
ies,
str
ateg
ies
or p
lans
for n
atio
-na
l and
inte
rnat
iona
l tra
nspo
rt o
f ra
dioa
ctiv
e m
ater
ials
, sam
ples
and
was
te
man
agem
ent i
nclu
ding
thos
e fr
om h
ospi
tals
and
med
ical
ser
vice
s3 are
est
a-bl
ishe
d
Dem
onst
rate
d ca
paci
ty -
4
Syst
emat
ic in
form
atio
n ex
chan
ge b
etw
een
com
pete
nt ra
diol
ogic
al a
utho
ritie
s an
d hu
man
hea
lth s
urve
illan
ce u
nits
abo
ut u
rgen
t ra
diol
ogic
al e
vent
s an
d po
tent
ial r
isks
that
may
con
stitu
te a
PH
EIC
Func
tiona
l co
ordi
natio
n4 an
d co
mm
unic
atio
n m
echa
nism
s5 ex
ist
betw
een
rele
vant
nat
iona
l co
mpe
tent
aut
horit
ies
resp
onsi
ble
for
nucl
ear
regu
lato
ry
cont
rol/
safe
ty a
nd re
leva
nt s
ecto
rs6
Sust
aina
ble
capa
city
- 5
Mec
hani
sm is
in p
lace
to
acce
ss7
heal
th f
acili
ties
with
cap
acity
to
man
age
patie
nts
of ra
diat
ion
emer
genc
ies
Radi
atio
n em
erge
ncy
resp
onse
dril
ls a
nd o
ther
exe
rcis
es c
arrie
d ou
t reg
ular
ly,
incl
udin
g th
e re
ques
ting
of in
tern
atio
nal a
ssis
tanc
e (a
s ne
eded
) and
inte
rna-
tiona
l not
ifica
tion
1 - T
his
indi
cato
r ref
ers
to d
etec
tion
and
resp
onse
to ra
diol
ogic
al a
nd n
ucle
ar e
mer
genc
ies
and
an e
nabl
ing
envi
ronm
ent f
or th
e m
anag
emen
t of r
adia
tion
even
ts in
pla
ce w
ith a
ppro
pria
te le
gisl
atio
n or
pol
icy
and
with
the
invo
lvem
ent
of re
leva
nt s
ecto
rs (s
uch
as e
nviro
nmen
t, tr
ansp
ort,
trad
e, to
uris
m, c
usto
ms,
law
-enf
orce
men
t, de
fenc
e, o
ther
s).
2 -
Det
ectio
n ca
paci
ty in
clud
es n
ot o
nly
surv
eilla
nce
but a
lso
the
labo
rato
ry c
apac
ity re
quire
d fo
r the
ver
ifica
tion
of a
ny e
vent
s in
col
labo
ratio
n w
ith la
bora
tory
net
wor
ks o
utsi
de a
nd in
side
the
coun
try.
3 -
Reco
mm
ende
d th
at W
HO
dev
elop
som
e le
vel o
f spe
cific
ity fo
r pub
lic h
ealth
and
med
ical
asp
ects
(con
sist
ent w
ith th
e co
ntex
tual
and
tech
nica
l que
stio
ns) t
o av
oid
dupl
icat
ion
with
oth
er p
eer r
evie
w s
ervi
ces.
4 -
Not
e th
at c
ross
-ref
eren
ces
with
tech
nica
l are
as o
f “N
atio
nal l
egis
latio
n, p
olic
y an
d fin
anci
ng” a
nd “I
HR
coor
dina
tion,
com
mun
icat
ion
and
advo
cacy
”, an
d th
e at
trib
utes
for t
his
com
pone
nt s
houl
d be
als
o fu
lly a
ddre
ssed
und
er
thos
e co
re c
apac
ities
.5
- In
form
atio
n sh
arin
g, m
eetin
gs, S
OPs
dev
elop
ed fo
r col
labo
rativ
e re
spon
se, e
tc.
6 -
Coor
dina
tion
for r
isk
asse
ssm
ents
, ris
k co
mm
unic
atio
ns, p
lann
ing,
exe
rcis
ing,
mon
itorin
g an
d in
clud
ing
coor
dina
tion
durin
g ur
gent
radi
olog
ical
eve
nts
and
pote
ntia
l ris
ks th
at m
ay c
onst
itute
a P
HEI
C.7
- Es
tabl
ishe
d ar
rang
emen
ts a
nd m
echa
nism
s in
pla
ce to
acc
ess
thes
e ca
paci
ties
in re
leva
nt c
olla
bora
ting
inst
itutio
ns w
ithin
the
coun
try
or in
oth
er c
ount
ries.
Cont
extu
al q
uest
ions
:
1.
Hav
e th
ere
been
radi
atio
n sa
fety
ass
essm
ents
in th
e pa
st fi
ve y
ears
(suc
h as
em
erge
ncy
prep
ared
ness
revi
ew b
y IA
EA)?
If a
pplic
able
, des
crib
e th
e ou
tcom
e an
d sh
are
the
repo
rt.
2.
Hav
e th
ere
been
bas
elin
e pu
blic
hea
lth a
sses
smen
ts w
ith re
gard
to ra
diat
ion
safe
ty in
the
past
five
yea
rs, f
or e
xam
ple
cons
ider
ing
mor
bidi
ty a
nd m
orta
lity?
3.
Hav
e th
ere
been
any
maj
or ra
diat
ion
emer
genc
ies
in th
e pa
st th
at m
ay h
ave
cont
ribut
ed to
the
expe
rienc
e an
d pr
epar
edne
ss o
f the
cou
ntry
?4.
Is
the
coun
try
a si
gnat
ory
to th
e Ea
rly N
otifi
catio
n an
d As
sist
ance
in C
ase
of a
Nuc
lear
Em
erge
ncy
(198
6) c
onve
ntio
ns?
IHR
RE
LA
TE
D H
AZ
AR
DS
AN
D P
OE

INTERNATIONAL HEALTH REGULATIONS (2005)
106 - Joint External Evaluation Tool - Second edition
Tech
nica
l que
stio
ns:
RE.1
Mec
hani
sms
esta
blis
hed
and
func
tioni
ng fo
r det
ectin
g an
d re
spon
ding
to ra
diol
ogic
al a
nd n
ucle
ar e
mer
genc
ies
1.
Are
ther
e na
tiona
l pol
icie
s, s
trat
egie
s or
pla
ns a
vaila
ble
for t
he d
etec
tion,
ass
essm
ent,
resp
onse
and
reco
very
afte
r rad
iatio
n em
erge
ncie
s?a.
Are
thes
e im
plem
ente
d, a
nd if
so,
how
?b.
Are
thes
e up
date
d af
ter a
ctua
l eve
nts
or e
xerc
ises
(or u
pdat
ed re
gula
rly)?
2.
Is th
ere
an a
utho
rity/
inst
itute
/age
ncy
with
prim
ary
resp
onsi
bilit
y fo
r rad
iatio
n an
d su
rvei
llanc
e/m
onito
ring?
3.
Is th
ere
mon
itorin
g of
con
sum
er p
rodu
cts
(e.g
. foo
dstu
ffs a
nd g
oods
) with
rega
rd to
radi
oact
ive
cont
amin
atio
n?4.
Ar
e th
ere
proc
edur
es fo
r ris
k as
sess
men
t in
radi
olog
ical
sur
veill
ance
/mon
itorin
g, to
trig
ger/
mou
nt a
resp
onse
of s
uita
ble
com
posi
tion
and
mag
nitu
de?
5.
Is t
here
labo
rato
ry c
apac
ity in
the
cou
ntry
or
acce
ss t
o la
bora
tory
ser
vice
s ab
road
for
mon
itorin
g an
d as
sess
men
t of
rad
ioac
tive
cont
amin
atio
n of
the
en
viro
nmen
t in
case
of a
radi
atio
n em
erge
ncy?
6.
Is th
ere
labo
rato
ry c
apac
ity in
the
coun
try
or a
cces
s to
labo
rato
ry s
ervi
ces
abro
ad fo
r mon
itorin
g an
d as
sess
men
t of i
nter
nal c
onta
min
atio
n an
d ra
diat
ion
expo
sure
of h
uman
s in
cas
e of
a ra
diat
ion
emer
genc
y?7.
Ar
e tr
aini
ng p
rogr
amm
es a
vaila
ble
for e
mer
genc
y re
spon
ders
in th
e co
untr
y or
is th
eir a
cces
s to
trai
ning
abr
oad?
8.
Are
curr
ent h
uman
reso
urce
s su
ffici
ent t
o m
eet t
he n
eeds
of r
adia
tion
prot
ectio
n an
d sa
fety
?9.
Ar
e cu
rren
t fina
ncia
l res
ourc
es s
uffic
ient
to m
eet t
he n
eeds
of r
adia
tion
prot
ectio
n an
d sa
fety
?10
. Is
ther
e an
inve
ntor
y of
refe
renc
e/de
sign
ated
hea
lth c
are
faci
litie
s fo
r rad
iatio
n em
erge
ncie
s?11
. Ar
e th
ere
prot
ocol
s/gu
idel
ines
for c
ase
man
agem
ent o
f per
sons
ove
r-ex
pose
d to
ioni
zing
radi
atio
n?12
. Is
ther
e a
natio
nal s
tock
pile
of p
harm
aceu
tical
age
nts
that
can
be
used
as
coun
term
easu
res
in ra
diat
ion
emer
genc
ies
(suc
h as
die
thyl
ene
tria
min
e pe
ntaa
cetic
ac
id, P
russ
ian
blue
, pot
assi
um io
dide
, cyt
okin
es)?
RE.2
Ena
blin
g en
viro
nmen
t in
plac
e fo
r man
agem
ent o
f rad
iolo
gica
l and
nuc
lear
em
erge
ncie
s1.
Is
ther
e a
polic
y or
str
ateg
ic p
lan
for e
nsur
ing
safe
use
of r
adia
tion
in th
e co
untr
y? Is
it u
p-to
-dat
e? H
ow is
it im
plem
ente
d?2.
Is
ther
e a
natio
nal c
oord
inat
ing
body
/com
mitt
ee w
ith re
gard
to ra
diol
ogic
al a
nd n
ucle
ar e
mer
genc
ies?
3.
Is th
ere
an e
mer
genc
y re
spon
se p
lan
for r
adio
logi
cal a
nd n
ucle
ar e
mer
genc
ies?
4.
Doe
s th
e em
erge
ncy
resp
onse
pla
n co
nsid
er th
e ra
nge
of fu
nctio
ns re
quire
d in
a c
risis
? D
escr
ibe,
if a
pplic
able
. Doe
s it
cons
ider
the
avai
labi
lity
of re
sour
ces
and
SOPs
? Th
e pl
an s
houl
d co
nsid
er th
e fo
llow
ing
aspe
cts:
a. r
oles
and
resp
onsi
bilit
ies
b. p
ublic
com
mun
icat
ion
c. r
efer
ral,
tran
spor
t and
trea
tmen
t of l
arge
num
bers
of a
ffect
ed in
divi
dual
sd.
sto
ckpi
ling
of e
quip
men
t and
med
icat
ion
e. d
econ
tam
inat
ion
of p
eopl
e, p
rem
ises
and
env
ironm
ent
f. re
gist
ratio
n an
d fo
llow
-up
of o
ver-
expo
sed
pers
ons
g. r
estr
ictio
ns, e
vacu
atio
n
IHR
RE
LA
TE
D H
AZ
AR
DS
AN
D P
OE

INTERNATIONAL HEALTH REGULATIONS (2005)
107 - Joint External Evaluation Tool - Second edition
h. e
mer
genc
y fu
nds
i. ex
erci
ses
orga
nize
d on
a re
gula
r bas
is to
eva
luat
e an
d re
vise
the
plan
.5.
Ar
e th
ere
mul
tisec
tora
l/int
erdi
scip
linar
y co
ordi
natio
n m
echa
nism
s w
ith re
gard
to ra
diat
ion
emer
genc
y pr
epar
edne
ss a
nd re
spon
se m
anag
emen
t?
If ap
plic
able
, des
crib
e m
echa
nism
s an
d in
dica
te s
hort
com
ings
. Coo
rdin
atio
n m
echa
nism
s co
uld
invo
lve:
a. H
ealth
sec
tor
• N
atio
nal I
HR
Foca
l Poi
nt•
Hos
pita
ls a
nd h
ealth
car
e fa
cilit
ies
(clin
ics,
labo
rato
ries,
nur
sing
hom
es)
• Al
l lev
els
of p
ublic
hea
lth in
fras
truc
ture
(loc
al, i
nter
med
iate
, nat
iona
l)•
Food
and
drin
king
wat
er s
afet
y se
rvic
es•
Labo
rato
ry(ie
s) fo
r ind
ivid
ual m
onito
ring
and
asse
ssm
ent o
f rad
iatio
n ex
posu
re in
hum
ans
• Re
fere
nce
heal
th c
are
faci
litie
s ca
pabl
e of
clin
ical
man
agem
ent o
f sev
ere
radi
atio
n in
jurie
s an
d in
tern
al c
onta
min
atio
n.b.
Env
ironm
enta
l pro
tect
ion
• N
atio
nal s
urve
illan
ce s
ervi
ces
for r
adio
logi
cal m
onito
ring
of th
e en
viro
nmen
t.c.
Nuc
lear
regu
lato
ry a
nd ra
diat
ion
safe
ty a
utho
ritie
s•
Ope
rato
rs o
f nuc
lear
inst
alla
tions
(if a
ny)
d. E
mer
genc
y se
rvic
es (fi
re, p
olic
e, a
mbu
lanc
e, m
edic
al re
spon
ders
, etc
.)e.
Con
sum
er s
afet
y, in
clud
ing
food
and
drin
king
wat
er s
afet
yf.
Adm
inis
trat
ive/
polit
ical
aut
horit
ies
at a
ll le
vels
(loc
al, i
nter
med
iate
, nat
iona
l)g.
Haz
ardo
us s
ites
man
agem
ent
h. M
eteo
rolo
gica
l ser
vice
si.
Poin
ts o
f ent
ry (p
orts
, airp
orts
, gro
und
cros
sing
s), i
n pa
rtic
ular
thos
e de
sign
ated
und
er th
e IH
Rj.
Tran
spor
tk.
Priv
ate
sect
or/i
ndus
try.
6.
In th
e ev
ent o
f a ra
diat
ion
emer
genc
y, co
uld
a bu
dget
be
mob
ilize
d to
mee
t add
ition
al d
eman
ds?
7.
Is th
ere
an a
udit/
eval
uatio
n sy
stem
for e
xerc
ises
/res
pons
es?
8.
Are
thei
r rad
iatio
n em
erge
ncy
resp
onse
dril
ls c
arrie
d ou
t reg
ular
ly?
9.
Are
plan
s fo
r na
tiona
l and
inte
rnat
iona
l tra
nspo
rt o
f ra
dioa
ctiv
e m
ater
ials
, and
was
te m
anag
emen
t in
clud
ing
thos
e fro
m h
ospi
tals
and
med
ical
ser
vice
s es
tabl
ishe
d?
10.
Are
ther
e lin
ks e
stab
lishe
d w
ith g
loba
l exp
ert n
etw
orks
, suc
h as
WH
O’s
Rad
iatio
n Em
erge
ncy
Med
ical
Pre
pare
dnes
s an
d As
sist
ance
Net
wor
k(RE
MPA
N),
WH
O’s
gl
obal
bio
dosi
met
ry n
etw
ork
of la
bora
torie
s fo
r rad
iatio
n em
erge
ncie
s (B
ioD
oseN
et),
or In
tern
atio
nal A
tom
ic E
nerg
y Ag
ency
Res
pons
e As
sist
ance
Net
wor
k (R
ANET
)
IHR
RE
LA
TE
D H
AZ
AR
DS
AN
D P
OE

INTERNATIONAL HEALTH REGULATIONS (2005)
108 - Joint External Evaluation Tool - Second edition
Refe
renc
es:
l
IAEA
saf
ety
stan
dard
s se
ries
No.
GSR
Par
t 7. P
repa
redn
ess
and
resp
onse
for a
nuc
lear
or r
adio
logi
cal e
mer
genc
y. J
oint
ly s
pons
ored
by
the
FAO,
IAEA
, ICAO
, ILO,
IM
O, IN
TERP
OL,
OEC
D/N
EA, P
AHO,
CTB
TO, U
NEP
, OCH
A, W
HO,
WM
O. G
ener
al S
afet
y Re
quire
men
ts P
art 7
. Vie
nna:
Inte
rnat
iona
l Ato
mic
Ene
rgy
Agen
cy; 2
015
(http
://w
ww
-pub
.iaea
.org
/MTC
D/P
ublic
atio
ns/P
DF/
P_17
08_w
eb.p
df, a
cces
sed
28 N
ovem
ber 2
017)
.l
IAEA
saf
ety
glos
sary
. Ter
min
olog
y us
ed in
nuc
lear
saf
ety
and
radi
atio
n pr
otec
tion
2007
edi
tion.
Vie
nna:
Inte
rnat
iona
l Ato
mic
Ene
rgy
Agen
cy; 2
009
(http
://w
ww
-pub
.iaea
.org
/MTC
D/p
ublic
atio
ns/P
DF/
Pub1
290_
web
, acc
esse
d 28
Nov
embe
r 201
7).
IHR
RE
LA
TE
D H
AZ
AR
DS
AN
D P
OE

INTERNATIONAL HEALTH REGULATIONS (2005)
109 - Joint External Evaluation Tool - Second edition
APPE
ND
IX 1
: GLO
SSAR
Y
Not
e: T
hese
term
s an
d de
finiti
ons
have
bee
n pr
ovid
ed fo
r use
with
in th
e co
ntex
t of t
his
tool
and
may
diff
er fr
om th
ose
used
in o
ther
doc
umen
ts. T
he p
urpo
se is
to
cla
rify
key
term
s th
at a
re IH
R re
leva
nt, a
nd re
fer t
o fo
odbo
rne
as w
ell a
s zo
onot
ic d
isea
ses
and
othe
r rel
evan
t cou
ntry
-spe
cific
pub
lic h
ealth
prio
ritie
s.
Bios
afet
y. L
abor
ator
y bi
osaf
ety
desc
ribes
the
con
tain
men
t pr
inci
ples
, tec
hnol
ogie
s an
d pr
actic
es t
hat
are
impl
emen
ted
to p
reve
nt u
nint
entio
nal e
xpos
ure
to
path
ogen
s an
d to
xins
, or t
heir
acci
dent
al re
leas
e.
Bios
ecur
ity. L
abor
ator
y bi
osec
urity
des
crib
es th
e pr
otec
tion,
con
trol
and
acc
ount
abili
ty fo
r val
uabl
e bi
olog
ical
mat
eria
ls w
ithin
labo
rato
ries
as w
ell a
s in
form
atio
n re
late
d to
thes
e m
ater
ials
and
dua
l-us
e re
sear
ch, i
n or
der t
o pr
even
t the
ir un
auth
oriz
ed a
cces
s, lo
ss, t
heft
, mis
use,
div
ersi
on o
r int
entio
nal r
elea
se.
Case
. A p
erso
n w
ho h
as th
e pa
rtic
ular
dis
ease
, hea
lth d
isor
der o
r con
ditio
n th
at m
eets
the
case
defi
nitio
ns fo
r sur
veill
ance
and
out
brea
k in
vest
igat
ion
purp
oses
. Th
e de
finiti
on o
f a c
ase
for s
urve
illan
ce a
nd o
utbr
eak
inve
stig
atio
n pu
rpos
e is
not
nec
essa
rily
the
sam
e as
the
ordi
nary
clin
ical
defi
nitio
n (a
dapt
ed fr
om L
ast J
M,
Spas
off R
A, H
arris
, edi
tors
. A d
ictio
nary
of e
pide
mio
logy
, fou
rth
editi
on. I
nter
natio
nal E
pide
mio
logi
cal A
ssoc
iatio
n, In
c. N
ew Y
ork:
Oxf
ord
Uni
vers
ity P
ress
; 200
1).
Case
defi
nitio
n. A
set
of d
iagn
ostic
crit
eria
that
mus
t be
fulfi
lled
for a
n in
divi
dual
to b
e re
gard
ed a
s a
case
of a
par
ticul
ar d
isea
se fo
r sur
veill
ance
and
out
brea
k in
vest
igat
ion
purp
oses
. Cas
e de
finiti
ons
can
be b
ased
on
clin
ical
crit
eria
, lab
orat
ory
crite
ria o
r a
com
bina
tion
of th
e tw
o w
ith th
e el
emen
ts o
f tim
e, p
lace
and
pe
rson
. (In
the
IHR,
cas
e de
finiti
ons
are
publ
ishe
d on
the
WH
O w
ebsi
te1
for
the
four
dis
ease
s fo
r w
hich
all
case
s m
ust
be n
otifi
ed b
y St
ates
Par
ties
to W
HO,
re
gard
less
of c
ircum
stan
ces,
und
er th
e IH
R as
pro
vide
d in
Ann
ex 2
.)
Chem
ical
eve
nt. A
man
ifest
atio
n of
a d
isea
se o
r an
occu
rren
ce, w
hich
cre
ates
a p
oten
tial f
or a
dis
ease
as
a re
sult
of e
xpos
ure
to o
r con
tam
inat
ion
by a
che
mic
al
agen
t.
Clus
ter.
An a
ggre
gatio
n of
rela
tivel
y un
com
mon
eve
nts
or d
isea
ses
in s
pace
and
/or t
ime
in a
mou
nts
that
are
bel
ieve
d or
per
ceiv
ed to
be
grea
ter t
han
that
exp
ecte
d by
cha
nce
(ada
pted
from
Las
t JM
, Spa
soff
RA, H
arris
, edi
tors
. A d
ictio
nary
of e
pide
mio
logy
, fou
rth
editi
on. I
nter
natio
nal E
pide
mio
logi
cal A
ssoc
iatio
n, In
c. N
ew
York
: Oxf
ord
Uni
vers
ity P
ress
; 200
1).
Com
mun
icab
le d
isea
se (i
nfec
tious
dis
ease
). An
illn
ess
due
to a
spe
cific
infe
ctio
us a
gent
or i
ts to
xic
prod
ucts
that
aris
es th
roug
h tr
ansm
issi
on o
f tha
t age
nt o
r its
pr
oduc
ts fr
om a
n in
fect
ed p
erso
n, a
nim
al o
r res
ervo
ir to
a s
usce
ptib
le h
ost,
eith
er d
irect
ly o
r ind
irect
ly th
roug
h an
inte
rmed
iate
pla
nt o
r ani
mal
hos
t, ve
ctor
or t
he
inan
imat
e en
viro
nmen
t (ad
apte
d fr
om L
ast J
M, S
paso
ff RA
, Har
ris, e
dito
rs. A
dic
tiona
ry o
f epi
dem
iolo
gy, f
ourt
h ed
ition
. Int
erna
tiona
l Epi
dem
iolo
gica
l Ass
ocia
tion,
In
c. N
ew Y
ork:
Oxf
ord
Uni
vers
ity P
ress
; 200
1).
Com
mun
ity s
urve
illan
ce. T
he s
tart
ing
poin
t fo
r ev
ent
notifi
catio
n at
the
com
mun
ity le
vel,
gene
rally
don
e by
a c
omm
unity
wor
ker;
it ca
n be
act
ive
(look
ing
for
case
s) o
r pa
ssiv
e (r
epor
ting
case
s). I
t m
ay b
e pa
rtic
ular
ly u
sefu
l dur
ing
an o
utbr
eak
and
whe
re s
yndr
omic
cas
e de
finiti
ons
can
be u
sed
(the
iden
tifica
tion
of
com
mun
ity c
ases
of E
bola
viru
s in
fect
ion
by c
omm
unity
wor
kers
was
an
exam
ple
of a
ctiv
e co
mm
unity
sur
veill
ance
).
Com
pete
nt a
utho
rity.
An
auth
ority
resp
onsi
ble
for t
he im
plem
enta
tion
and
appl
icat
ion
of h
ealth
mea
sure
s un
der t
he IH
R.
1 -
http
://w
ww
.who
.int/
ihr/
surv
ella
nce_
resp
onse
/cas
e_de
finiti
ons/
en/

INTERNATIONAL HEALTH REGULATIONS (2005)
110 - Joint External Evaluation Tool - Second edition
Cont
amin
atio
n. T
he p
rese
nce
of a
n in
fect
ious
or t
oxic
age
nt o
r mat
ter o
n th
e bo
dy s
urfa
ce o
f a h
uman
or a
nim
al, i
n or
on
a pr
oduc
t pre
pare
d fo
r con
sum
ptio
n or
on
oth
er in
anim
ate
obje
cts,
incl
udin
g co
nvey
ance
s th
at m
ay c
onst
itute
a p
ublic
hea
lth ri
sk.
Dang
erou
s pa
thog
ens
and
toxi
ns. T
hese
are
bio
logi
cal a
gent
s an
d to
xins
tha
t ha
ve t
he p
oten
tial t
o po
se a
sev
ere
thre
at t
o bo
th h
uman
and
ani
mal
hea
lth.
Whi
le s
ome
sele
ct a
gent
s ar
e no
rmal
ly fo
und
in th
e en
viro
nmen
t and
don
’t ca
use
hum
an d
isea
se, m
any
of th
em –
if m
anip
ulat
ed o
r rel
ease
d in
larg
e qu
antit
ies
– c
an c
ause
ser
ious
hea
lth t
hrea
ts. T
he in
form
al A
ustr
alia
Gro
up p
rovi
des
a Li
st o
f hu
man
and
ani
mal
pat
hoge
ns a
nd t
oxin
s fo
r ex
port
con
trol
(ht
tp:/
/ww
w.
aust
ralia
grou
p.ne
t/en
/hum
an_a
nim
al_p
atho
gens
.htm
l, ac
cess
ed 2
8 Au
gust
201
6).
Deco
ntam
inat
ion.
A p
roce
dure
whe
reby
hea
lth m
easu
res
are
take
n to
elim
inat
e an
infe
ctio
us o
r tox
ic a
gent
or m
atte
r on
the
body
sur
face
of a
hum
an o
r ani
mal
, in
or o
n a
prod
uct p
repa
red
for c
onsu
mpt
ion,
or o
n ot
her i
nani
mat
e ob
ject
s, in
clud
ing
conv
eyan
ces
that
may
con
stitu
te a
pub
lic h
ealth
risk
.
Des
igna
ted
labo
rato
ries.
The
se a
re la
bora
torie
s de
sign
ated
to p
erfo
rm s
peci
fic la
bora
tory
ser
vice
s by
nat
iona
l, W
HO
or o
ther
aut
horit
ies
beca
use
of th
eir p
rove
n ca
paci
ties
and
capa
bilit
ies,
suc
h as
for A
MR
test
ing.
Desi
gnat
ed p
oint
s of
ent
ry. T
hese
refe
r to
a po
rt, a
irpor
t and
pot
entia
lly a
gro
und
cros
sing
that
is d
esig
nate
d by
a S
tate
Par
ty to
str
engt
hen,
dev
elop
and
mai
ntai
n th
e ca
paci
ties
as p
er m
ain
IHR
artic
les
19, 2
0 an
d 21
, and
as
desc
ribed
in A
nnex
1 o
f the
IHR:
• The
cap
aciti
es a
t all
times
con
cern
ing
acce
ss to
med
ical
ser
vice
s fo
r pr
ompt
ass
essm
ent a
nd c
are
of il
l tra
velle
rs, a
saf
e en
viro
nmen
t for
trav
elle
rs (e
.g.
wat
er, f
ood,
was
te),
pers
onne
l for
insp
ectio
n an
d ve
ctor
con
trol
func
tions
; and
• The
cap
aciti
es to
resp
ond
spec
ifica
lly to
eve
nts
that
may
con
stitu
te a
pub
lic h
ealth
em
erge
ncy
of in
tern
atio
nal c
once
rn.
Dise
ase.
An
illne
ss o
r med
ical
con
ditio
n, ir
resp
ectiv
e of
orig
in o
r sou
rce,
that
pre
sent
s or
cou
ld p
rese
nt s
igni
fican
t har
m to
hum
ans.
Disi
nsec
tion.
The
pro
cedu
re w
here
by h
ealth
mea
sure
s ar
e ta
ken
to c
ontr
ol o
r ki
ll in
sect
vec
tors
of
hum
an d
isea
ses
pres
ent
in b
agga
ge, c
argo
, con
tain
ers,
co
nvey
ance
s, g
oods
and
pos
tal p
arce
ls.
Docu
men
ted
proc
edur
es. A
gree
d an
d ap
prov
ed s
trat
egie
s fo
r ope
ratio
n, s
tand
ard
oper
atin
g pr
oced
ures
, rol
es a
nd re
spon
sibi
litie
s, a
gree
men
ts, t
erm
s of
refe
renc
e,
chai
ns o
f com
man
d, re
port
ing
mec
hani
sms,
am
ong
othe
rs.
Early
war
ning
sys
tem
. A s
peci
fic p
roce
dure
in d
isea
se s
urve
illan
ce to
det
ect a
ny a
bnor
mal
occ
urre
nce,
or d
epar
ture
from
the
usua
l or n
orm
ally
obs
erve
d fr
eque
ncy
of p
heno
men
a (s
uch
as o
ne c
ase
of E
bola
feve
r), a
s ea
rly a
s po
ssib
le. A
n ea
rly w
arni
ng s
yste
m is
onl
y us
eful
if it
is li
nked
to m
echa
nism
s fo
r ea
rly re
spon
se
(ada
pted
from
Las
t JM
, Spa
soff
RA, H
arris
, edi
tors
. A d
ictio
nary
of e
pide
mio
logy
, fou
rth
editi
on. I
nter
natio
nal E
pide
mio
logi
cal A
ssoc
iatio
n, In
c. N
ew Y
ork:
Oxf
ord
Uni
vers
ity P
ress
; 200
1).
Epid
emic
. The
occ
urre
nce
in a
com
mun
ity o
r reg
ion
of c
ases
of a
n ill
ness
, spe
cific
hea
lth-r
elat
ed b
ehav
iour
s, o
r oth
er h
ealth
-rel
ated
eve
nts
clea
rly in
exc
ess
of
norm
al e
xpec
tanc
y. T
he c
omm
unity
or r
egio
n an
d th
e pe
riod
in w
hich
the
case
s oc
cur a
re s
peci
fied
prec
isel
y. T
he n
umbe
r of c
ases
indi
catin
g th
e pr
esen
ce o
f an
epi
dem
ic v
arie
s ac
cord
ing
to th
e ag
ent,
size
and
type
of p
opul
atio
n ex
pose
d, p
revi
ous
expe
rienc
e or
lack
of e
xpos
ure
to th
e di
seas
e, a
nd ti
me
and
plac
e of
oc
curr
ence
(ada
pted
from
Las
t JM
, Spa
soff
RA, H
arris
, edi
tors
. A d
ictio
nary
of e
pide
mio
logy
, fou
rth
editi
on. I
nter
natio
nal E
pide
mio
logi
cal A
ssoc
iatio
n, In
c. N
ew
York
: Oxf
ord
Uni
vers
ity P
ress
; 200
1).

INTERNATIONAL HEALTH REGULATIONS (2005)
111 - Joint External Evaluation Tool - Second edition
Even
t. A
man
ifest
atio
n of
dis
ease
or a
n oc
curr
ence
that
cre
ates
a p
oten
tial f
or d
isea
se.
Even
t-ba
sed
surv
eilla
nce.
The
org
aniz
ed a
nd ra
pid
capt
ure
of in
form
atio
n ab
out e
vent
s th
at a
re a
pot
entia
l ris
k to
pub
lic h
ealth
. Thi
s in
form
atio
n ca
n be
rum
ours
an
d ot
her a
d ho
c re
port
s tr
ansm
itted
thro
ugh
form
al c
hann
els
(i.e.
est
ablis
hed
rout
ine
repo
rtin
g sy
stem
s) a
nd in
form
al c
hann
els
(i.e.
the
med
ia, h
ealth
wor
kers
an
d re
port
s fr
om n
ongo
vern
men
tal o
rgan
izat
ions
), in
clud
ing
even
ts r
elat
ed t
o th
e oc
curr
ence
of
dise
ase
in h
uman
s an
d ev
ents
rel
ated
to
pote
ntia
l hum
an
expo
sure
.
Feed
back
. The
regu
lar p
roce
ss o
f sen
ding
ana
lyse
s an
d re
port
s ab
out s
urve
illan
ce d
ata
back
thro
ugh
all l
evel
s of
the
surv
eilla
nce
syst
em s
o th
at a
ll pa
rtic
ipan
ts
can
be in
form
ed o
f tre
nds
and
perf
orm
ance
.
Fiel
d Ep
idem
iolo
gy T
rain
ing
Prog
ram
• FET
P Ba
sic
Leve
l Tra
inin
g is
for l
ocal
hea
lth s
taff
and
cons
ists
of l
imite
d cl
assr
oom
hou
rs in
ters
pers
ed th
roug
hout
as
a th
ree-
to-fi
ve m
onth
on-
the-
job
field
as
sign
men
t to
build
cap
acity
in c
ondu
ctin
g tim
ely
outb
reak
det
ectio
n, p
ublic
hea
lth re
spon
se a
nd p
ublic
hea
lth s
urve
illan
ce.
• FET
P In
term
edia
te L
evel
Tra
inin
g is
for
dist
rict/
regi
on/s
tate
-lev
el e
pide
mio
logi
sts,
and
con
sist
s of
lim
ited
clas
sroo
m h
ours
inte
rspe
rsed
thro
ugho
ut a
s a
six-
to-n
ine
mon
th o
n-th
e-jo
b m
ento
red
field
ass
ignm
ent t
o bu
ild c
apac
ity in
con
duct
ing
outb
reak
inve
stig
atio
ns, p
lann
ed e
pide
mio
logi
c st
udie
s, a
nd p
ublic
he
alth
sur
veill
ance
ana
lyse
s an
d ev
alua
tions
. • F
ETP
Adva
nced
Lev
el T
rain
ing
is fo
r adv
ance
d ep
idem
iolo
gist
s an
d co
nsis
ts o
f lim
ited
clas
sroo
m h
ours
inte
rspe
rsed
thro
ugho
ut th
e 24
mon
ths
of m
ento
red
field
ass
ignm
ents
to b
uild
cap
acity
in o
utbr
eak
inve
stig
atio
ns, p
lann
ed e
pide
mio
logi
c st
udie
s, p
ublic
hea
lth s
urve
illan
ce a
naly
ses
and
eval
uatio
ns, s
cien
tific
com
mun
icat
ion,
and
evi
denc
e-ba
sed
deci
sion
mak
ing
for
deve
lopm
ent
of e
ffect
ive
publ
ic h
ealth
pro
gram
min
g w
ith a
nat
iona
l fo
cus.
Ani
mal
hea
lth
prof
essi
onal
s ca
n be
eng
aged
in th
ese
FETP
trai
ning
s.
Func
tiona
l exe
rcis
e. A
fully
sim
ulat
ed in
tera
ctiv
e ex
erci
se th
at te
sts
the
capa
bilit
y of
an
orga
niza
tion
to re
spon
d to
a s
imul
ated
eve
nt. T
he e
xerc
ise
test
s m
ultip
le
func
tions
of t
he o
rgan
izat
ion’
s op
erat
iona
l pla
n. It
is a
coo
rdin
ated
resp
onse
to a
situ
atio
n in
a ti
me
pres
sure
d re
alis
tic s
ituat
ion
as d
escr
ibed
in W
HO
Sim
ulat
ion
Exer
cise
Man
ual 5
. A fu
nctio
nal e
xerc
ise
focu
ses
on th
e co
ordi
natio
n, in
tegr
atio
n an
d in
tera
ctio
n of
an
orga
niza
tion’
s po
licie
s, p
roce
dure
s, ro
les
and
resp
onsi
bilit
ies
befo
re, d
urin
g or
aft
er th
e si
mul
ated
eve
nt (W
HO
Sim
ulat
ion
Exer
cise
Man
ual.
HO
-WH
E-CP
I-20
17.1
0 (h
ttp:
//ap
ps.w
ho.in
t/iri
s/bi
tstr
eam
/106
65/2
5474
1/1/
WH
O-
WH
E-CP
I-20
17.1
0-en
g.pd
f?ua
=1, a
cces
sed
13 A
ugus
t 201
7).
Gro
und
cros
sing
. A p
oint
of l
and
entr
y in
to a
Sta
te P
arty
, inc
ludi
ng th
ose
utili
zed
by ro
ad v
ehic
les
and
trai
ns.
Haz
ard.
The
inhe
rent
cap
abili
ty o
f an
agen
t or s
ituat
ion
to h
ave
an a
dver
se e
ffect
; a fa
ctor
or e
xpos
ure
that
may
adv
erse
ly a
ffect
hea
lth (s
imila
r con
cept
to ri
sk
fact
or).
Hea
lth c
are
wor
ker.
Any
empl
oyee
in a
hea
lth c
are
faci
lity
who
has
clo
se c
onta
ct w
ith p
atie
nts,
pat
ient
-car
e ar
eas
or p
atie
nt-c
are
item
s; a
lso
refe
rred
to a
s “h
ealth
ca
re p
erso
nnel
”.
Hea
lth e
vent
. Any
eve
nt re
latin
g to
the
heal
th o
f an
indi
vidu
al, s
uch
as th
e oc
curr
ence
of a
cas
e of
a s
peci
fic d
isea
se o
r syn
drom
e, th
e ad
min
istr
atio
n of
a v
acci
ne
or a
n ad
mis
sion
to h
ospi
tal.
Hea
lth m
easu
re. A
pro
cedu
re a
pplie
d to
pre
vent
the
spre
ad o
f dis
ease
or c
onta
min
atio
n; it
doe
s no
t inc
lude
law
enf
orce
men
t or s
ecur
ity m
easu
res.

INTERNATIONAL HEALTH REGULATIONS (2005)
112 - Joint External Evaluation Tool - Second edition
Inci
denc
e. T
he n
umbe
r of i
nsta
nces
of i
llnes
s co
mm
enci
ng, o
r of p
erso
ns fa
lling
ill,
durin
g a
give
n pe
riod
in a
spe
cifie
d po
pula
tion
(Pre
vale
nce
and
inci
denc
e.
WH
O B
ulle
tin 1
966;
35:7
83-7
84).
Indi
cato
r-ba
sed
surv
eilla
nce.
The
rout
ine
repo
rtin
g of
cas
es o
f dis
ease
, inc
ludi
ng fr
om n
otifi
able
dis
ease
s su
rvei
llanc
e, s
entin
el s
urve
illan
ce, l
abor
ator
y ba
sed
surv
eilla
nce.
Thi
s ro
utin
e re
port
ing
is c
omm
only
hea
lth c
are
faci
lity
base
d w
ith re
port
ing
done
on
a w
eekl
y or
mon
thly
bas
is.
Infe
ctio
n. T
he e
ntry
and
dev
elop
men
t or m
ultip
licat
ion
of a
n in
fect
ious
age
nt in
the
body
of h
uman
s an
d an
imal
s th
at m
ay c
onst
itute
a p
ublic
hea
lth ri
sk.
Infe
ctio
n co
ntro
l. M
easu
res
prac
ticed
by
heal
th c
are
pers
onne
l in
heal
th c
are
faci
litie
s to
dec
reas
e tr
ansm
issi
on a
nd a
cqui
sitio
n of
infe
ctio
us a
gent
s. T
hese
in
clud
e pr
oper
han
d hy
gien
e, s
crup
ulou
s w
ork
prac
tices
, and
the
use
of p
erso
nal p
rote
ctiv
e eq
uipm
ent (
such
as
mas
ks, r
espi
rato
rs, g
love
s, g
owns
, eye
pro
tect
ion)
. In
fect
ion
cont
rol m
easu
res
are
base
d on
how
an
infe
ctio
us a
gent
is tr
ansm
itted
and
incl
ude
stan
dard
, con
tact
, dro
plet
and
airb
orne
pre
caut
ions
.
Infe
ctio
us d
isea
se. S
ee C
omm
unic
able
dis
ease
.
Inte
rnat
iona
l Hea
lth R
egul
atio
ns (2
005)
(IH
R or
the
Regu
latio
ns).
This
is a
lega
lly-b
indi
ng in
stru
men
t of i
nter
natio
nal l
aw w
hich
has
its
orig
in in
the
Inte
rnat
iona
l Sa
nita
ry C
onve
ntio
ns o
f 185
1, c
oncl
uded
in re
spon
se to
incr
easi
ng c
once
rn a
bout
the
links
bet
wee
n in
tern
atio
nal t
rade
and
spr
ead
of d
isea
ses
(cro
ss-b
orde
r he
alth
risk
s).
Isol
atio
n. S
epar
atio
n of
sic
k or
con
tam
inat
ed p
erso
ns o
r affe
cted
bag
gage
, con
tain
ers,
con
veya
nces
, goo
ds o
r pos
tal p
arce
ls fr
om o
ther
s in
suc
h a
man
ner a
s to
pr
even
t the
spr
ead
of in
fect
ion
or c
onta
min
atio
n.
Legi
slat
ion.
The
rang
e of
lega
l, ad
min
istr
ativ
e or
oth
er g
over
nmen
tal i
nstr
umen
ts th
at m
ay b
e av
aila
ble
for S
tate
s Pa
rtie
s to
impl
emen
t the
IHR.
Thi
s in
clud
es
lega
lly b
indi
ng i
nstr
umen
ts, s
uch
as s
tate
con
stitu
tions
, law
s, a
cts,
dec
rees
, ord
ers,
reg
ulat
ions
and
ord
inan
ces;
leg
ally
non
-bin
ding
ins
trum
ents
, suc
h as
gu
idel
ines
, sta
ndar
ds, o
pera
ting
rule
s, a
dmin
istr
ativ
e pr
oced
ures
or r
ules
; and
oth
er ty
pes
of in
stru
men
ts, s
uch
as p
roto
cols
, res
olut
ions
and
inte
r-se
ctor
al o
r in
ter-
min
iste
rial a
gree
men
ts. T
his
enco
mpa
sses
legi
slat
ion
in a
ll se
ctor
s, s
uch
as h
ealth
, agr
icul
ture
, tra
nspo
rtat
ion,
env
ironm
ent,
port
s an
d ai
rpor
ts, a
nd a
t all
appl
icab
le g
over
nmen
tal l
evel
s (n
atio
nal,
inte
rmed
iate
, loc
al a
nd o
ther
).
Mul
tisec
tora
l. A
holis
tic a
ppro
ach
invo
lvin
g th
e ef
fort
s of
mul
tiple
org
aniz
atio
ns, in
stitu
tes
and
agen
cies
. It e
ncou
rage
s in
terd
isci
plin
ary p
artic
ipat
ion,
col
labo
ratio
n an
d co
ordi
natio
n of
peo
ple
of c
once
rn a
nd re
sour
ces
from
thes
e ke
y or
gani
zatio
ns fo
r pro
mot
ing
heal
th s
ecur
ity, t
o ac
hiev
e a
spec
ific
goal
.
Nat
iona
l leg
isla
tion.
See
Leg
isla
tion.
Nat
iona
l IH
R Fo
cal P
oint
. The
nat
iona
l cen
tre
desi
gnat
ed b
y ea
ch S
tate
Par
ty, w
hich
sha
ll be
acc
essi
ble
at a
ll tim
es fo
r com
mun
icat
ions
with
WH
O IH
R co
ntac
t po
ints
und
er th
e IH
R.
Not
ifiab
le d
isea
se. A
dis
ease
that
, by
stat
utor
y/le
gal r
equi
rem
ents
, mus
t be
repo
rted
to a
pub
lic h
ealth
or o
ther
com
pete
nt a
utho
rity
in th
e pe
rtin
ent j
uris
dict
ion
whe
n th
e di
agno
sis
is m
ade
(ada
pted
fro
m L
ast
JM, S
paso
ff RA
, Har
ris, e
dito
rs.
A di
ctio
nary
of
epid
emio
logy
, fou
rth
editi
on.
Inte
rnat
iona
l Epi
dem
iolo
gica
l As
soci
atio
n, In
c. N
ew Y
ork:
Oxf
ord
Uni
vers
ity P
ress
; 200
1).
Not
ifica
tion.
The
pro
cess
es b
y w
hich
cas
es o
r out
brea
ks a
re b
roug
ht to
the
know
ledg
e of
the
heal
th a
utho
ritie
s. In
the
cont
ext o
f the
IHR,
not
ifica
tion
is th
e of
ficia
l co
mm
unic
atio
n of
a d
isea
se/h
ealth
eve
nt to
the
WH
O b
y th
e he
alth
adm
inis
trat
ion
of th
e M
embe
r Sta
te a
ffect
ed b
y th
e di
seas
e/he
alth
eve
nt.

INTERNATIONAL HEALTH REGULATIONS (2005)
113 - Joint External Evaluation Tool - Second edition
Occ
upat
iona
l saf
ety.
Occ
upat
iona
l hea
lth d
eals
with
all
aspe
cts
of h
ealth
and
saf
ety
in th
e w
orkp
lace
and
has
a s
tron
g fo
cus
on p
rimar
y pr
even
tion
of h
azar
ds.
The
heal
th o
f w
orke
rs h
as s
ever
al d
eter
min
ants
, inc
ludi
ng r
isk
fact
ors
at t
he w
orkp
lace
lead
ing
to c
ance
rs, a
ccid
ents
, mus
culo
skel
etal
dis
ease
s, r
espi
rato
ry
dise
ases
, hea
ring
loss
, circ
ulat
ory
dise
ases
, str
ess
rela
ted
diso
rder
s, c
omm
unic
able
dis
ease
s an
d ot
hers
(htt
p://
ww
w.w
ho.in
t/to
pics
/occ
upat
iona
l_he
alth
/en/
, ac
cess
ed 2
8 N
ovem
ber 2
017)
.
Occ
upat
iona
l saf
ety
and
heal
th. T
he W
HO
Glo
bal P
lan
of A
ctio
n (G
PA) o
n W
orke
rs’ H
ealth
(200
8–17
) and
con
sist
ent w
ith th
e IL
O P
rom
otio
nal F
ram
ewor
k fo
r O
ccup
atio
nal S
afet
y an
d H
ealth
Con
vent
ion,
200
6 (N
o. 1
87)
aim
s to
str
engt
hen
heal
th s
yste
ms
and
the
desi
gn o
f he
alth
car
e se
ttin
gs f
or im
prov
ing
heal
th
and
safe
ty o
f the
hea
lth w
orke
r, pa
tient
saf
ety
and
qual
ity o
f pat
ient
car
e, a
nd u
ltim
atel
y su
ppor
t a h
ealth
y an
d su
stai
nabl
e co
mm
unity
with
link
s to
gre
enin
g he
alth
sec
tor
and
gree
n jo
bs in
itiat
ives
(ht
tp:/
/ww
w.il
o.or
g/w
cmsp
5/gr
oups
/pub
lic/-
--ed
_nor
m/-
--re
lcon
f/do
cum
ents
/mee
tingd
ocum
ent/
wcm
s_14
5837
, ac
cess
ed 2
8 N
ovem
ber 2
017)
.
One
Hea
lth. D
efine
d by
WH
O a
s an
app
roac
h to
des
igni
ng a
nd im
plem
entin
g pr
ogra
mm
es, p
olic
ies,
legi
slat
ion
and
rese
arch
in w
hich
mul
tiple
sec
tors
com
mun
icat
e an
d w
ork
toge
ther
to a
chie
ve b
ette
r pub
lic h
ealth
out
com
es (h
ttp:
//w
ww
.who
.int/
feat
ures
/qa/
one-
heal
th/e
n/, a
cces
sed
28 N
ovem
ber 2
017)
In th
e co
ntex
t of t
he W
HO
tech
nica
l fra
mew
ork
in s
uppo
rt to
IHR
mon
itorin
g an
d ev
alua
tion,
taki
ng a
One
Hea
lth a
ppro
ach
mea
ns in
clud
ing,
from
all
rele
vant
sec
tors
, na
tiona
l inf
orm
atio
n, e
xper
tise,
per
spec
tives
and
exp
erie
nce
nece
ssar
y to
con
duct
ass
essm
ents
, eva
luat
ions
and
repo
rtin
g fo
r the
impl
emen
tatio
n of
the
IHR.
Oth
er g
over
nmen
tal i
nstr
umen
ts. A
gree
men
ts, p
roto
cols
and
reso
lutio
ns o
f any
gov
ernm
ent a
utho
rity
or b
ody.
Out
brea
k. A
n ep
idem
ic li
mite
d to
loca
lized
incr
ease
in th
e in
cide
nce
of a
dis
ease
, suc
h as
in a
vill
age,
tow
n or
clo
sed
inst
itutio
n (a
dapt
ed fr
om L
ast J
M, S
paso
ff RA
, Har
ris, e
dito
rs. A
dic
tiona
ry o
f epi
dem
iolo
gy, f
ourt
h ed
ition
. Int
erna
tiona
l Epi
dem
iolo
gica
l Ass
ocia
tion,
Inc.
New
Yor
k: O
xfor
d U
nive
rsity
Pre
ss; 2
001)
.
Pers
onal
pro
tect
ive
equi
pmen
t. Sp
ecia
lized
clo
thin
g an
d eq
uipm
ent d
esig
ned
to c
reat
e a
barr
ier a
gain
st h
ealth
and
saf
ety
haza
rds;
exa
mpl
es in
clud
e go
ggle
s,
face
shi
elds
, glo
ves
and
resp
irato
rs.
Poin
t of e
ntry
. A p
assa
ge fo
r int
erna
tiona
l ent
ry o
r exi
t of t
rave
llers
, bag
gage
, car
go, c
onta
iner
s, c
onve
yanc
es, g
oods
and
pos
tal p
arce
ls, a
nd th
e ag
enci
es a
nd
area
s pr
ovid
ing
serv
ices
to th
em u
pon
entr
y or
exi
t.
Port
. A s
eapo
rt o
r a p
ort o
n an
inla
nd b
ody
of w
ater
whe
re s
hips
on
an in
tern
atio
nal v
oyag
e ar
rive
or d
epar
t.
Publ
ic h
ealth
em
erge
ncy
of in
tern
atio
nal c
once
rn (P
HEI
C). A
n ex
trao
rdin
ary
even
t (as
pro
vide
d in
the
IHR)
that
: (i)
cons
titut
es a
pub
lic h
ealth
risk
to o
ther
sta
tes
thro
ugh
the
inte
rnat
iona
l spr
ead
of d
isea
se; a
nd (i
i) po
tent
ially
requ
ires
a co
ordi
nate
d in
tern
atio
nal r
espo
nse.
Publ
ic h
ealth
risk
. The
like
lihoo
d of
an
even
t tha
t may
adv
erse
ly a
ffect
the
heal
th o
f hum
an p
opul
atio
ns, w
ith a
n em
phas
is o
n w
heth
er it
may
spr
ead
inte
rnat
iona
lly
or p
rese
nt a
ser
ious
and
dire
ct d
ange
r.
Qua
rant
ine.
The
rest
rictio
n of
act
iviti
es a
nd/o
r sep
arat
ion
from
oth
ers
of s
uspe
ct p
erso
ns w
ho a
re n
ot s
ick,
or o
f sus
pect
bag
gage
, con
tain
ers,
con
veya
nces
or
good
s in
suc
h a
man
ner s
o as
to p
reve
nt th
e po
ssib
le s
prea
d of
infe
ctio
n or
con
tam
inat
ion.
Rapi
d re
spon
se te
am. A
gro
up o
f tra
ined
indi
vidu
als
that
is re
ady
to re
spon
d qu
ickl
y to
an
even
t. Th
e co
mpo
sitio
n an
d te
rms
of re
fere
nce
are
dete
rmin
ed b
y th
e co
ncer
ned
coun
try.

INTERNATIONAL HEALTH REGULATIONS (2005)
114 - Joint External Evaluation Tool - Second edition
Read
ines
s. It
is th
e ab
ility
to q
uick
ly a
nd a
ppro
pria
tely
resp
ond
whe
n re
quire
d to
any
em
erge
ncie
s.
Regu
latio
ns o
r adm
inis
trat
ive
requ
irem
ents
. All
regu
latio
ns, p
roce
dure
s, ru
les
and
stan
dard
s.
Rele
vant
sec
tors
. Priv
ate
and
publ
ic s
ecto
rs: s
uch
as a
ll le
vels
of t
he h
ealth
car
e sy
stem
(nat
iona
l, su
bnat
iona
l and
com
mun
ity/p
rimar
y pu
blic
hea
lth);
NG
Os;
m
inis
trie
s of
agr
icul
ture
(zoo
nosi
s, v
eter
inar
y la
bora
tory
), tr
ansp
ort
(tra
nspo
rt p
olic
y, ci
vil a
viat
ion,
por
ts a
nd m
ariti
me
tran
spor
t), t
rade
and
/or
indu
stry
(foo
d sa
fety
and
qua
lity
cont
rol),
for
eign
tra
de (
cons
umer
pro
tect
ion,
con
trol
of
com
puls
ory
stan
dard
enf
orce
men
t), c
omm
unic
atio
n, d
efen
ce, t
reas
ury
or fi
nanc
e (c
usto
ms)
, env
ironm
ent,
inte
rior,
heal
th, t
ouris
m; t
he h
ome
offic
e; m
edia
; and
regu
lato
ry b
odie
s.
Risk
com
mun
icat
ion.
For
pub
lic h
ealth
em
erge
ncie
s in
clud
es th
e ra
nge
of c
omm
unic
atio
n ca
paci
ties
requ
ired
thro
ugh
the
prep
ared
ness
, res
pons
e an
d re
cove
ry
phas
es o
f a s
erio
us p
ublic
hea
lth e
vent
to e
ncou
rage
info
rmed
dec
isio
n m
akin
g, p
ositi
ve b
ehav
iour
cha
nge
and
the
mai
nten
ance
of t
rust
.
Surv
eilla
nce.
The
sys
tem
atic
ong
oing
col
lect
ion,
col
latio
n an
d an
alys
is o
f dat
a fo
r pub
lic h
ealth
pur
pose
s an
d th
e tim
ely
diss
emin
atio
n of
pub
lic h
ealth
info
rmat
ion
for a
sses
smen
t and
pub
lic h
ealth
resp
onse
, as
nece
ssar
y.
Synd
rom
e. A
sym
ptom
com
plex
in w
hich
the
sym
ptom
s an
d/or
sig
ns c
oexi
st m
ore
freq
uent
ly th
an w
ould
be
expe
cted
by
chan
ce in
depe
nden
tly (a
dapt
ed fr
om
Last
JM
, Spa
soff
RA, H
arris
, edi
tors
. A d
ictio
nary
of
epid
emio
logy
, fou
rth
editi
on. I
nter
natio
nal E
pide
mio
logi
cal A
ssoc
iatio
n, In
c. N
ew Y
ork:
Oxf
ord
Uni
vers
ity
Pres
s; 2
001)
.
Tabl
e to
p ex
erci
se. A
fac
ilita
ted
disc
ussi
on o
f an
em
erge
ncy
situ
atio
n, g
ener
ally
in a
n in
form
al, l
ow-s
tres
s en
viro
nmen
t. It
is d
esig
ned
to e
licit
cons
truc
tive
disc
ussi
on b
etw
een
part
icip
ants
; to
iden
tify
and
reso
lve
prob
lem
s; a
nd to
refin
e ex
istin
g op
erat
iona
l pla
ns. T
his
is th
e on
ly ty
pe o
f sim
ulat
ion
exer
cise
that
doe
s no
t req
uire
an
exis
ting
resp
onse
pla
n in
pla
ce. (
WH
O S
imul
atio
n Ex
erci
se M
anua
l. H
O-W
HE-
CPI-
2017
.10
(htt
p://
apps
.who
.int/
iris/
bits
trea
m/1
0665
/254
741/
1/W
HO
-WH
E-CP
I-20
17.1
0-en
g.pd
f?ua
=1, a
cces
sed
30 N
ovem
ber 2
017)
.
Trai
ned
staf
f. In
divi
dual
s th
at h
ave
educ
atio
nal c
rede
ntia
ls a
nd/o
r rec
eive
d sp
ecifi
c in
stru
ctio
n th
at is
app
licab
le to
a ta
sk o
r situ
atio
n.
Urg
ent e
vent
. A m
anife
stat
ion
of a
dis
ease
or a
n oc
curr
ence
that
cre
ates
a p
oten
tial f
or d
isea
se th
at h
as a
ser
ious
pub
lic h
ealth
impa
ct a
nd/o
r is
unus
ual o
r of
unex
pect
ed n
atur
e, w
ith h
igh
pote
ntia
l for
spr
ead.
Not
e: th
e te
rm “
urge
nt”
has
been
use
d in
com
bina
tion
with
oth
er te
rms
(suc
h as
infe
ctio
us e
vent
, che
mic
al
even
t) in
ord
er t
o si
mul
tane
ousl
y co
nvey
bot
h th
e na
ture
of
the
even
t an
d th
e ch
arac
teris
tics
that
mak
e it
“urg
ent”
(i.e
. ser
ious
pub
lic h
ealth
impa
ct a
nd/o
r un
usua
l or u
nexp
ecte
d na
ture
with
hig
h po
tent
ial f
or s
prea
d).
Vect
or. A
n in
sect
or o
ther
ani
mal
that
nor
mal
ly tr
ansp
orts
an
infe
ctio
us a
gent
that
con
stitu
tes
a pu
blic
hea
lth ri
sk.
Verifi
catio
n. T
he p
rovi
sion
of i
nfor
mat
ion
by a
Sta
te P
arty
to W
HO
con
firm
ing
the
stat
us o
f an
even
t with
in th
e te
rrito
ry o
r ter
ritor
ies
of th
at S
tate
Par
ty.
WH
O IH
R co
ntac
t poi
nt. T
he u
nit w
ithin
WH
O th
at is
acc
essi
ble
at a
ll tim
es fo
r com
mun
icat
ions
with
the
Nat
iona
l IH
R Fo
cal P
oint
.
Zoon
otic
dis
ease
s (o
r zo
onos
es).
Any
infe
ctio
n or
infe
ctio
us d
isea
se t
hat
is n
atur
ally
tra
nsm
issi
ble
from
ver
tebr
ate
anim
als
to h
uman
s (h
ttp:
//w
ww
.who
.int/
topi
cs/z
oono
ses/
en, a
cces
sed
28 N
ovem
ber 2
017)
.
Zoon
otic
eve
nt. A
man
ifest
atio
n of
a d
isea
se in
ani
mal
s th
at c
reat
es a
pot
entia
l for
a d
isea
se in
hum
ans
as a
resu
lt of
hum
an e
xpos
ure
to th
e an
imal
sou
rce.

INTERNATIONAL HEALTH REGULATIONS (2005)
115 - Joint External Evaluation Tool - Second edition
APPE
ND
IX 2
: SU
MM
ARY
OF
CHAN
GES
BET
WEE
N J
EE T
OO
L FI
RST
AND
SEC
ON
D E
DIT
ION
S
1.
Nam
e of
the
two
tech
nica
l are
as h
ave
been
cha
nged
a. R
eal t
ime
surv
eilla
nce
to S
urve
illan
ceb.
Wor
kfor
ce d
evel
opm
ent t
o H
uman
reso
urce
s 2.
W
here
ther
e ar
e ch
ange
s in
indi
cato
rs (a
ddin
g, c
ombi
ning
, spl
ittin
g or
mov
ing)
; “ta
rget
”, “m
easu
red
by” a
nd “d
esire
d im
pact
” hav
e be
en u
pdat
ed to
o (d
etai
ls o
f in
dica
tor c
hang
es a
re re
flect
ed b
elow
in th
e co
lum
n tit
led
“Maj
or c
hang
es in
V2”
) 3.
W
hen
anim
al a
nd h
uman
hea
lth s
core
s ar
e gi
ven,
inst
ead
of th
e av
erag
e, th
e lo
wer
sco
re o
f tho
se tw
o w
ill b
e ta
ken.
4.
Fo
otno
tes
and
Glos
sary
are
upd
ated
to e
nsur
e co
rrec
t int
erpr
etat
ion
of th
e to
ol.
Tech
nica
l are
aJE
E to
ol fi
rst e
ditio
n (V
1)JE
E to
ol s
econ
d ed
ition
(V2)
Maj
or c
hang
es in
V2
How
to in
terp
ret1
Nat
iona
l le
gisl
atio
n, p
olic
y an
d fin
anci
ng
P.1.
1 Le
gisl
atio
n, la
ws,
regu
latio
ns,
adm
inis
trat
ive
requ
irem
ents
, po
licie
s or
oth
er g
over
nmen
t in
stru
men
ts in
pla
ce a
re s
uffic
ient
for
impl
emen
tatio
n of
IHR
P.1.
2 Th
e St
ate
can
dem
onst
rate
th
at it
has
adj
uste
d an
d al
igne
d its
do
mes
tic le
gisl
atio
n, p
olic
ies
and
adm
inis
trat
ive
arra
ngem
ents
to
enab
le c
ompl
ianc
e w
ith th
e IH
R
P.1.
1 Th
e St
ate
has
asse
ssed
, ad
just
ed a
nd a
ligne
d its
do
mes
tic le
gisl
atio
n, p
olic
ies
and
adm
inis
trat
ive
arra
ngem
ents
in a
ll re
leva
nt s
ecto
rs to
ena
ble
com
plia
nce
with
the
IHR
P.1.
2 Fi
nanc
ing
is a
vaila
ble
for t
he
impl
emen
tatio
n of
IHR
capa
citie
sP.
1.3
A fin
anci
ng m
echa
nism
an
d fu
nds
are
avai
labl
e fo
r tim
ely
resp
onse
to p
ublic
hea
lth
emer
genc
ies
1. In
dica
tor P
.1.1
and
P.1
.2 o
f V1
is
com
bine
d to
P.1
.1 in
V2.
2. T
wo
new
fina
nce
indi
cato
rs a
re
adde
d P.
1.2
and
P.1.
3 in
V2
3. T
echn
ical
que
stio
ns a
re u
pdat
ed
acco
rdin
gly
1. S
core
of P
.1.1
and
P.2
.2 o
f V1
shou
ld b
e av
erag
ed a
nd th
e lo
wer
sc
ore
shou
ld b
e co
nsid
ered
as
base
line
whi
ch w
ill re
flect
indi
cato
r P.
1.1
of V
2
IHR
coor
dina
tion,
co
mm
unic
atio
n an
d ad
voca
cy
P.2.
1 A
func
tiona
l mec
hani
sm is
es
tabl
ishe
d fo
r the
coo
rdin
atio
n an
d in
tegr
atio
n of
rele
vant
sec
tors
in th
e im
plem
enta
tion
of IH
R
P.2.
1 A
func
tiona
l mec
hani
sm
esta
blis
hed
for t
he c
oord
inat
ion
and
inte
grat
ion
of re
leva
nt s
ecto
rs in
the
impl
emen
tatio
n of
IHR
1. N
o ch
ange
s at
indi
cato
r lev
el2.
Ver
y m
inor
cha
nges
in a
ttrib
utes
No
addi
tiona
l int
erpr
etat
ion
requ
ired
1- C
ount
ries
who
con
duct
ed J
EE u
sing
firs
t edi
tion
of th
e to
ol a
nd w
ould
follo
w u
p th
e pr
ogre
ss u
sing
sec
ond
editi
on (o
nly)
. Thi
s is
not
inte
nded
to c
ompa
re c
ount
ries

INTERNATIONAL HEALTH REGULATIONS (2005)
116 - Joint External Evaluation Tool - Second edition
Antim
icro
bial
re
sist
ance
P.3.
1 An
timic
robi
al re
sist
ance
(AM
R)
dete
ctio
nP.
3.2
Surv
eilla
nce
of in
fect
ions
ca
used
by
AMR
path
ogen
sP.
3.3
Hea
lthca
re-a
ssoc
iate
d in
fect
ion
(HAI
) pre
vent
ion
and
cont
rol
prog
ram
sP.
3.4
Antim
icro
bial
ste
war
dshi
p ac
tiviti
es
P.3.
1 Ef
fect
ive
mul
tisec
tora
l co
ordi
natio
n on
AM
RP.
3.2
Surv
eilla
nce
of A
MR
P.3.
3 In
fect
ion
prev
entio
n an
d co
ntro
l P.
3.4
Opt
imiz
e us
e of
ant
imic
robi
al
med
icin
es in
hum
an a
nd a
nim
al
heal
th a
nd a
gric
ultu
re
1. P
.3.1
and
P.3
.2 o
f V1
is c
ombi
ned
as P
.3.2
2. N
ew in
dica
tor f
or e
ffect
ive
coor
dina
tion
is a
dded
as
P.3.
1 in
V2
3. In
fect
ion
prev
entio
n an
d co
ntro
l re
late
d in
dica
tor i
s ch
ange
d an
d at
trib
utes
upd
ated
in P
.3.3
of V
24.
P.3
.4 o
f V1
is c
hang
ed
to g
over
nanc
e of
use
of
antim
icro
bial
s in
V2
No
addi
tiona
l int
erpr
etat
ion
requ
ired
Zoon
otic
dis
ease
P.4.
1 Su
rvei
llanc
e sy
stem
s in
pla
ce
for p
riorit
y zo
onot
ic d
isea
ses/
path
ogen
sP.
4.2
Vete
rinar
y or
ani
mal
hea
lth
wor
kfor
ceP.
4.3
Mec
hani
sms
for r
espo
ndin
g to
in
fect
ious
zoo
nose
s an
d po
tent
ial
zoon
oses
are
est
ablis
hed
and
func
tiona
l
P.4.
1 Co
ordi
nate
d su
rvei
llanc
e sy
stem
s in
pla
ce in
the
anim
al h
ealth
an
d pu
blic
hea
lth s
ecto
rs fo
r zoo
notic
di
seas
es/p
atho
gens
iden
tified
as
join
t prio
ritie
s P.
4.2
Mec
hani
sms
for r
espo
ndin
g to
infe
ctio
us a
nd p
oten
tial z
oono
tic
dise
ases
est
ablis
hed
and
func
tiona
l
1. In
dica
tor P
.4.1
is d
etai
led
but
outp
ut/o
utco
me
mea
sure
of t
his
indi
cato
r rem
ains
sam
e2.
Indi
cato
r P.4
.2 is
inco
rpor
ated
in
indi
cato
rs o
f Hum
an re
sour
ces
of
V23.
P.4
.3 o
f V1
is s
ame
as P
.4.2
of V
2
1. U
se s
core
of P
.4.1
and
P.4
.3 o
f V1
only
2. W
orkf
orce
rela
ted
scor
e ca
n be
us
ed fo
r Hum
an re
sour
ces
Food
saf
ety
P.5.
1 M
echa
nism
s ar
e es
tabl
ishe
d an
d fu
nctio
ning
for d
etec
ting
and
resp
ondi
ng to
food
born
e di
seas
e an
d fo
od c
onta
min
atio
n
P.5.
1 Su
rvei
llanc
e sy
stem
s in
pla
ce
for t
he d
etec
tion
and
mon
itorin
g of
food
born
e di
seas
es a
nd fo
od
cont
amin
atio
nP.
5.2
Mec
hani
sms
are
esta
blis
hed
and
func
tioni
ng fo
r the
resp
onse
an
d m
anag
emen
t of f
ood
safe
ty
emer
genc
ies
1. In
dica
tor P
.5.1
of V
1 is
cha
nged
to
two
indi
cato
rs P
.5.1
and
P.5
.2 in
V2
2. A
ttrib
utes
and
tech
nica
l que
stio
ns
are
upda
ted
No
addi
tiona
l int
erpr
etat
ion
requ
ired
as P
.5.1
of V
1 is
a c
ombi
ned
vers
ion
of tw
o in
dica
tors
of V
2
Bios
afet
y an
d bi
osec
urity
P.6.
1 W
hole
-of-
gove
rnm
ent b
iosa
fety
an
d bi
osec
urity
sys
tem
is in
pla
ce
for h
uman
, ani
mal
, and
agr
icul
ture
fa
cilit
ies
P.6.
2 Bi
osaf
ety
and
bios
ecur
ity
trai
ning
and
pra
ctic
es
P.6.
1 W
hole
-of-
gove
rnm
ent b
iosa
fety
an
d bi
osec
urity
sys
tem
in p
lace
for a
ll se
ctor
s (in
clud
ing
hum
an, a
nim
al a
nd
agric
ultu
re fa
cilit
ies)
P.6.
2 Bi
osaf
ety
and
bios
ecur
ity
trai
ning
and
pra
ctic
es in
all
rele
vant
se
ctor
s (in
clud
ing
hum
an, a
nim
al a
nd
agric
ultu
re)
1. T
houg
h in
dica
tors
look
cha
nged
, th
ey a
re ju
st m
ore
deta
iled
with
no
maj
or c
hang
es2.
Min
or c
hang
es in
att
ribut
es o
nly
No
addi
tiona
l int
erpr
etat
ion
requ
ired

INTERNATIONAL HEALTH REGULATIONS (2005)
117 - Joint External Evaluation Tool - Second edition
Imm
uniz
atio
nP.
7.1
Vacc
ine
cove
rage
(mea
sles
) as
part
of n
atio
nal p
rogr
amP.
7.2
Nat
iona
l vac
cine
acc
ess
and
deliv
ery
P.7.
1 Va
ccin
e co
vera
ge (m
easl
es) a
s pa
rt o
f nat
iona
l pro
gram
me
P.7.
2 N
atio
nal v
acci
ne a
cces
s an
d de
liver
y
1. N
o ch
ange
s in
indi
cato
rs a
nd m
inor
ch
ange
s in
att
ribut
esN
o ad
ditio
nal i
nter
pret
atio
n re
quire
d
Nat
iona
l la
bora
tory
sys
tem
D.1.
1 La
bora
tory
test
ing
for d
etec
tion
of p
riorit
y di
seas
esD.
1.2
Spec
imen
refe
rral
and
tran
spor
t sy
stem
D.1.
3 Ef
fect
ive
mod
ern
poin
t of c
are
and
labo
rato
ry b
ased
dia
gnos
tics
D.1.
4 La
bora
tory
Qua
lity
Syst
em
D.1.
1 La
bora
tory
test
ing
for d
etec
tion
of p
riorit
y di
seas
esD.
1.2
Spec
imen
refe
rral
and
tran
spor
t sy
stem
D.1.
3 Ef
fect
ive
natio
nal d
iagn
ostic
ne
twor
kD.
1.4
Labo
rato
ry q
ualit
y sy
stem
1. O
nly
indi
cato
r nam
e of
D.1
.3 o
f V1
is c
hang
ed in
D.1
.3 o
f V2
2. R
est o
f the
indi
cato
rs re
mai
n sa
me
3. A
ttrib
utes
are
upd
ated
4. T
echn
ical
que
stio
ns o
n D.
1.1
has
AMR
rela
ted
ques
tions
No
addi
tiona
l int
erpr
etat
ion
requ
ired
Surv
eilla
nce
D.2.
1 In
dica
tor a
nd e
vent
bas
ed
surv
eilla
nce
syst
ems
D.2.
2 In
tero
pera
ble,
inte
rcon
nect
ed,
elec
tron
ic re
al-t
ime
repo
rtin
g sy
stem
D.2.
3 An
alys
is o
f sur
veill
ance
dat
aD.
2.4
Synd
rom
ic s
urve
illan
ce s
yste
ms
D.2.
1 Su
rvei
llanc
e sy
stem
sD.
2.2
Use
of e
lect
roni
c to
ols
D.2.
3 An
alys
is o
f sur
veill
ance
dat
a
1. In
dica
tor D
.2.1
and
D.2
.4 o
f V1
is
com
bine
d as
D.2
.1 in
V2
2. R
est o
f the
out
put/
outc
ome
mea
sure
s of
the
indi
cato
rs re
mai
n sa
me
thou
gh th
ere
are
min
or
chan
ges
in w
ordi
ng3.
Att
ribut
es a
nd te
chni
cal q
uest
ions
ar
e up
date
d ac
cord
ingl
y
1. S
core
of D
.2.1
and
D.2
.4 o
f V1
shou
ld b
e av
erag
ed a
nd th
e lo
wer
sc
ore
shou
ld b
e co
nsid
ered
as
base
line
whi
ch w
ill b
e re
flect
ed a
s D.
2.1
of V
24.
Res
t rem
ains
sam
e
Repo
rtin
gD.
3.1
Syst
em fo
r effi
cien
t rep
ortin
g to
W
HO,
FAO
and
OIE
D.3.
2 Re
port
ing
netw
ork
and
prot
ocol
s in
cou
ntry
D.3.
1 Sy
stem
for e
ffici
ent r
epor
ting
to
FAO,
OIE
and
WH
OD.
3.2
Repo
rtin
g ne
twor
k an
d pr
otoc
ols
in c
ount
ry
1. N
o ch
ange
s an
d m
inor
cha
nges
in
the
attr
ibut
esN
o ad
ditio
nal i
nter
pret
atio
n re
quire
d
Hum
an re
sour
ces
D.4.
1 H
uman
reso
urce
s ar
e av
aila
ble
to im
plem
ent I
HR
core
cap
acity
re
quire
men
tsD.
4.2
Appl
ied
epid
emio
logy
trai
ning
pr
ogra
m in
pla
ce s
uch
as F
ETP
D.4.
3 W
orkf
orce
Str
ateg
y
D.4.
1 An
up-
to-d
ate
mul
tisec
tora
l w
orkf
orce
str
ateg
y is
in p
lace
D.4.
2 H
uman
reso
urce
s ar
e av
aila
ble
to e
ffect
ivel
y im
plem
ent I
HR
D.4.
3. In
-ser
vice
trai
ning
s ar
e av
aila
ble
D.4.
4 FE
TP o
r oth
er a
pplie
d ep
idem
iolo
gy tr
aini
ng p
rogr
amm
e is
in
pla
ce
1. A
new
indi
cato
r is
adde
d (D
.4.3
) in
V22.
Wor
kfor
ce in
dica
tor D
.4.2
of
V1 fr
om Z
oono
tic d
isea
se is
in
corp
orat
ed in
indi
cato
rs o
f H
uman
reso
urce
s of
V2
3. D
.4.1
of V
2 is
refle
cted
in D
.4.3
of V
14.
D.4
.1 o
f V1
is re
flect
ed in
D.4
.2 o
f V2
5. D
.4.2
of V
1 is
refle
cted
in D
.4.4
of V
2
1. A
vera
ge o
f tot
al s
core
s of
w
orkf
orce
indi
cato
rs a
nd w
orkf
orce
in
dica
tor P
.4.2
of Z
oono
tic d
isea
se
of V
1 an
d ta
ke th
e lo
wer
val
ue2.
Res
t rem
ains
sam
e
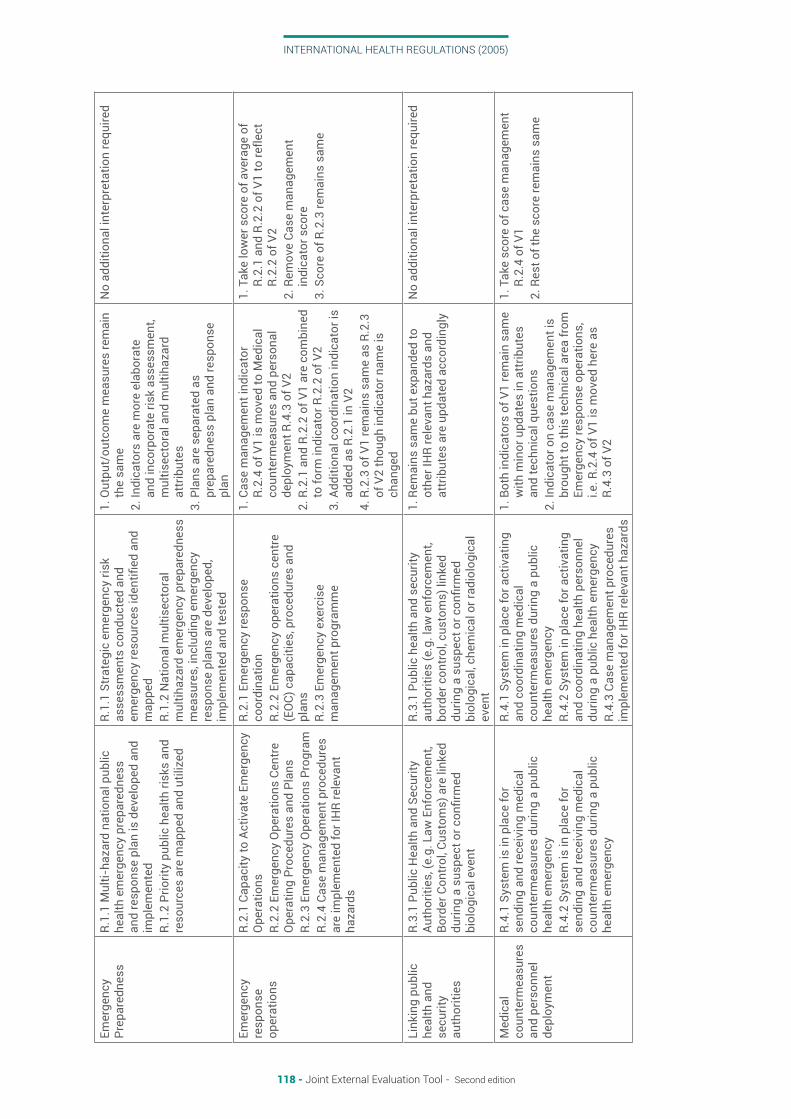
INTERNATIONAL HEALTH REGULATIONS (2005)
118 - Joint External Evaluation Tool - Second edition
Emer
genc
y Pr
epar
edne
ssR.
1.1
Mul
ti-ha
zard
nat
iona
l pub
lic
heal
th e
mer
genc
y pr
epar
edne
ss
and
resp
onse
pla
n is
dev
elop
ed a
nd
impl
emen
ted
R.1.
2 Pr
iorit
y pu
blic
hea
lth ri
sks
and
reso
urce
s ar
e m
appe
d an
d ut
ilize
d
R.1.
1 St
rate
gic
emer
genc
y ris
k as
sess
men
ts c
ondu
cted
and
em
erge
ncy
reso
urce
s id
entifi
ed a
nd
map
ped
R.1.
2 N
atio
nal m
ultis
ecto
ral
mul
tihaz
ard
emer
genc
y pr
epar
edne
ss
mea
sure
s, in
clud
ing
emer
genc
y re
spon
se p
lans
are
dev
elop
ed,
impl
emen
ted
and
test
ed
1. O
utpu
t/ou
tcom
e m
easu
res
rem
ain
the
sam
e2.
Indi
cato
rs a
re m
ore
elab
orat
e an
d in
corp
orat
e ris
k as
sess
men
t, m
ultis
ecto
ral a
nd m
ultih
azar
d at
trib
utes
3. P
lans
are
sep
arat
ed a
s pr
epar
edne
ss p
lan
and
resp
onse
pl
an
No
addi
tiona
l int
erpr
etat
ion
requ
ired
Emer
genc
y re
spon
se
oper
atio
ns
R.2.
1 Ca
paci
ty to
Act
ivat
e Em
erge
ncy
Ope
ratio
nsR.
2.2
Emer
genc
y O
pera
tions
Cen
tre
Ope
ratin
g Pr
oced
ures
and
Pla
nsR.
2.3
Emer
genc
y O
pera
tions
Pro
gram
R.2.
4 Ca
se m
anag
emen
t pro
cedu
res
are
impl
emen
ted
for I
HR
rele
vant
ha
zard
s
R.2.
1 Em
erge
ncy
resp
onse
co
ordi
natio
nR.
2.2
Emer
genc
y op
erat
ions
cen
tre
(EO
C) c
apac
ities
, pro
cedu
res
and
plan
sR.
2.3
Emer
genc
y ex
erci
se
man
agem
ent p
rogr
amm
e
1. C
ase
man
agem
ent i
ndic
ator
R.
2.4
of V
1 is
mov
ed to
Med
ical
co
unte
rmea
sure
s an
d pe
rson
al
depl
oym
ent R
.4.3
of V
22.
R.2
.1 a
nd R
.2.2
of V
1 ar
e co
mbi
ned
to fo
rm in
dica
tor R
.2.2
of V
23.
Add
ition
al c
oord
inat
ion
indi
cato
r is
adde
d as
R.2
.1 in
V2
4. R
.2.3
of V
1 re
mai
ns s
ame
as R
.2.3
of
V2
thou
gh in
dica
tor n
ame
is
chan
ged
1. T
ake
low
er s
core
of a
vera
ge o
f R.
2.1
and
R.2.
2 of
V1
to re
flect
R.
2.2
of V
22.
Rem
ove
Case
man
agem
ent
indi
cato
r sco
re
3. S
core
of R
.2.3
rem
ains
sam
e
Link
ing
publ
ic
heal
th a
nd
secu
rity
auth
oriti
es
R.3.
1 Pu
blic
Hea
lth a
nd S
ecur
ity
Auth
oriti
es, (
e.g.
Law
Enf
orce
men
t, Bo
rder
Con
trol
, Cus
tom
s) a
re li
nked
du
ring
a su
spec
t or c
onfir
med
bi
olog
ical
eve
nt
R.3.
1 Pu
blic
hea
lth a
nd s
ecur
ity
auth
oriti
es (e
.g. l
aw e
nfor
cem
ent,
bord
er c
ontr
ol, c
usto
ms)
link
ed
durin
g a
susp
ect o
r con
firm
ed
biol
ogic
al, c
hem
ical
or r
adio
logi
cal
even
t
1. R
emai
ns s
ame
but e
xpan
ded
to
othe
r IH
R re
leva
nt h
azar
ds a
nd
attr
ibut
es a
re u
pdat
ed a
ccor
ding
ly
No
addi
tiona
l int
erpr
etat
ion
requ
ired
Med
ical
co
unte
rmea
sure
s an
d pe
rson
nel
depl
oym
ent
R.4.
1 Sy
stem
is in
pla
ce fo
r se
ndin
g an
d re
ceiv
ing
med
ical
co
unte
rmea
sure
s du
ring
a pu
blic
he
alth
em
erge
ncy
R.4.
2 Sy
stem
is in
pla
ce fo
r se
ndin
g an
d re
ceiv
ing
med
ical
co
unte
rmea
sure
s du
ring
a pu
blic
he
alth
em
erge
ncy
R.4.
1 Sy
stem
in p
lace
for a
ctiv
atin
g an
d co
ordi
natin
g m
edic
al
coun
term
easu
res
durin
g a
publ
ic
heal
th e
mer
genc
yR.
4.2
Syst
em in
pla
ce fo
r act
ivat
ing
and
coor
dina
ting
heal
th p
erso
nnel
du
ring
a pu
blic
hea
lth e
mer
genc
yR.
4.3
Case
man
agem
ent p
roce
dure
s im
plem
ente
d fo
r IH
R re
leva
nt h
azar
ds
1. B
oth
indi
cato
rs o
f V1
rem
ain
sam
e w
ith m
inor
upd
ates
in a
ttrib
utes
an
d te
chni
cal q
uest
ions
2. In
dica
tor o
n ca
se m
anag
emen
t is
brou
ght t
o th
is te
chni
cal a
rea
from
Em
erge
ncy
resp
onse
ope
ratio
ns,
i.e. R
.2.4
of V
1 is
mov
ed h
ere
as
R.4.
3 of
V2
1. T
ake
scor
e of
cas
e m
anag
emen
t R.
2.4
of V
1 2.
Res
t of t
he s
core
rem
ains
sam
e

INTERNATIONAL HEALTH REGULATIONS (2005)
119 - Joint External Evaluation Tool - Second edition
Risk
co
mm
unic
atio
nR.
5.1
Risk
Com
mun
icat
ion
Syst
ems
(pla
ns, m
echa
nism
s, e
tc.)
R.5.
2 In
tern
al a
nd P
artn
er
Com
mun
icat
ion
and
Coor
dina
tion
R.5.
3 Pu
blic
Com
mun
icat
ion
R.5.
4 Co
mm
unic
atio
n En
gage
men
t w
ith A
ffect
ed C
omm
uniti
esR.
5.5
Dyn
amic
Lis
teni
ng a
nd R
umou
r M
anag
emen
t
R.5.
1 Ri
sk c
omm
unic
atio
n sy
stem
s fo
r unu
sual
/une
xpec
ted
even
ts a
nd
emer
genc
ies
R.5.
2 In
tern
al a
nd p
artn
er
coor
dina
tion
for e
mer
genc
y ris
k co
mm
unic
atio
nR.
5.3
Publ
ic c
omm
unic
atio
n fo
r em
erge
ncie
sR.
5.4
Com
mun
icat
ion
enga
gem
ent
with
affe
cted
com
mun
ities
R.5.
5 Ad
dres
sing
per
cept
ions
, ris
ky
beha
viou
rs a
nd m
isin
form
atio
n
1. O
utpu
t/ou
tcom
e m
easu
res
of a
ll th
ese
indi
cato
rs re
mai
ns s
ame
with
min
imal
cha
nges
in a
ttrib
utes
th
ough
indi
cato
r nam
es a
re
chan
ged
No
addi
tiona
l int
erpr
etat
ion
requ
ired
Poin
ts o
f ent
ryPo
E.1
Rout
ine
capa
citie
s ar
e es
tabl
ishe
d at
PoE
.Po
E.2
Effe
ctiv
e Pu
blic
Hea
lth
Resp
onse
at P
oint
s of
Ent
ry
PoE.
1 Ro
utin
e ca
paci
ties
esta
blis
hed
at p
oint
s of
ent
ryPo
E.2
Effe
ctiv
e pu
blic
hea
lth
resp
onse
at p
oint
s of
ent
ry
1. O
nly
attr
ibut
es a
re u
pdat
edN
o ad
ditio
nal i
nter
pret
atio
n re
quire
d
Chem
ical
eve
nts
CE.1
Mec
hani
sms
are
esta
blis
hed
and
func
tioni
ng fo
r det
ectin
g an
d re
spon
ding
to c
hem
ical
eve
nts
or
emer
genc
ies.
CE.2
Ena
blin
g en
viro
nmen
t is
in p
lace
fo
r man
agem
ent o
f che
mic
al E
vent
s
CE.1
Mec
hani
sms
esta
blis
hed
and
func
tioni
ng fo
r det
ectin
g an
d re
spon
ding
to c
hem
ical
eve
nts
or
emer
genc
ies
CE.2
Ena
blin
g en
viro
nmen
t in
plac
e fo
r man
agem
ent o
f che
mic
al e
vent
1. O
nly
attr
ibut
es a
re u
pdat
edN
o ad
ditio
nal i
nter
pret
atio
n re
quire
d
Radi
atio
n em
erge
ncie
sRE
.1 M
echa
nism
s ar
e es
tabl
ishe
d an
d fu
nctio
ning
for d
etec
ting
and
resp
ondi
ng to
radi
olog
ical
and
nu
clea
r em
erge
ncie
s.RE
.2 E
nabl
ing
envi
ronm
ent i
s in
pl
ace
for m
anag
emen
t of R
adia
tion
Emer
genc
ies
RE.1
Mec
hani
sms
esta
blis
hed
and
func
tioni
ng fo
r det
ectin
g an
d re
spon
ding
to ra
diol
ogic
al a
nd
nucl
ear e
mer
genc
ies
RE.2
Ena
blin
g en
viro
nmen
t in
plac
e fo
r man
agem
ent o
f rad
iolo
gica
l and
nu
clea
r em
erge
ncie
s
1. O
nly
chan
ges
in in
dica
tor:
Radi
atio
n em
erge
ncie
s in
V1
chan
ged
to R
adio
logi
cal a
nd
nucl
ear e
mer
genc
ies
in V
22.
Attr
ibut
es a
re u
pdat
ed
No
addi
tiona
l int
erpr
etat
ion
requ
ired

CONTACT DETAILS
COUNTRY CAPACITY MONITORING AND EVALUATION UNIT Country Health Emergency Preparedness and IHR World Health Organization 20 Avenue Appia CH-1211 Geneva Switzerland E-MAIL [email protected]
WHO Library Cataloguing-in-Publication Data
ISBN 978 92 4 155022 2