ischemia-reperfusion injury in rat fatty liver: role of nutritional status
TRANSCRIPT

Ischemia-Reperfusion Injury in Rat Fatty Liver:Role of Nutritional Status
PAOLO CARACENI,1 BRUNO NARDO,2 MARCO DOMENICALI,1 PAOLA TURI,2 MANUELA VICI,3 MARA SIMONCINI,1 NICOLA DE MARIA,4
FRANCO TREVISANI,1 DAVID H. VAN THIEL,4 MASSIMO DERENZINI,3 ANTONINO CAVALLARI,2 AND MAURO BERNARDI1
Fatty livers are more sensitive to the deleterious effects ofischemia-reperfusion than normal livers. Nutritional statusgreatly modulates this injury in normal livers, but its role inthe specific setting of fatty liver is unknown. This studyaimed to determine the effect of nutritional status on warmischemia-reperfusion injury in rat fatty livers. Fed andfasted rats with normal or fatty liver induced by a cholinedeficient diet underwent 1 hour of lobar ischemia andreperfusion. Rat survival was determined for 7 days. Serumtransaminases, liver histology and cell ultrastructure wereassessed before and after ischemia, and at 30 minutes, 2hours, 8 hours, and 24 hours after reperfusion. Survival wasalso determined in fatty fasted rats supplemented withglucose before surgery. The preischemic hepatic glycogenwas measured in all groups. Whereas survival was similarin fasted and fed rats with normal liver (90% vs. 100%),fasting dramatically reduced survival in rats with fatty liver(14% vs. 64%, P F .01). Accordingly, fasting and fattydegeneration had a synergistic effect in exacerbating liverinjury. Mitochondrial damage was a predominant feature ofultrastructural hepatocyte injury in fasted fatty livers.Glucose supplementation partially prevented the fasting-induced depletion of glycogen and improved the 7-day ratsurvival to 45%. These data indicate that rat fatty liversexposed to normothermic ischemia-reperfusion injury aremuch more sensitive to fasting than histologically normallivers. Because glucose supplementation improves both thehepatic glycogen stores and the rat survival, a nutritionalrepletion procedure may be part of a treatment strategyaimed to prevent ischemia-reperfusion injury in fatty livers.(HEPATOLOGY 1999;29:1139-1146.)
Normothermic ischemia-reperfusion injury is an impor-tant determinant in the pathogenesis of the liver damage
occurring during surgical procedures, such as hepatic resec-tion and liver transplantation, and during clinical conditions,such as ischemic hepatitis and multiple organ failure syn-drome. Healthy livers can safely tolerate up to 60 minutes ofnormothermic ischemia, but longer periods may cause post-operative liver failure.1 Warm ischemia is also an importantcomponent of the liver injury associated with the transplantprocedure. Indeed, a prolonged rewarming time duringimplantation of the organ in the recipient is considered animportant factor in predicting early graft dysfunction.2
It is well shown that the presence of fatty degenerationreduces the tolerance of the liver to ischemia-reperfusioninjury.3-11 The occurrence of postoperative liver failure afterhepatic resection in a steatotic liver exposed to 60 minutes ofvascular clamping has been reported.12 In the setting oforthotopic liver transplantation, massive fatty infiltration of adonor liver is a well known risk factor for the development ofprimary nonfunction, but even lesser degrees of steatosisadversely affect the orthotropic liver transplantation out-come.2-4,13-15 For this reason, transplant surgeons sometimesdiscard fatty livers despite the current shortage of donor organs.
The exact characterization of the cellular, vascular, andmetabolic events that occur in a failing fatty liver has yet to bedetermined. Several experimental studies indicate that he-patic microcirculatory injury is a key event in the develop-ment of cell death during reperfusion after either cold orwarm ischemia.5,6,10,11 However, Hakamada et al.11 haverecently shown that the prevention of the sinusoidal conges-tion by intraportal injection of anti–intercellular adhesionmolecule-1 monoclonal antibody improves but does notnormalize the survival of rats with fatty liver. Thus, additionalmechanisms must influence the performance of steatoticlivers exposed to ischemia-reperfusion injury.
A potential important and manageable factor is the preexistingnutritional status of the liver. In clinical transplantation, starva-tion of the donor, because of a prolonged intensive care unithospitalization or a lack of an adequate nutritional support,increases the incidence of hepatocellular injury and primarynonfunction.16 In animal models, in vitro and in vivo studies haveshown that fasting exacerbates normothermic ischemic injury.17,18
In contrast, conflicting results with respect to the effect of fastingon the outcome of normal livers exposed to cold as well as warmischemia followed by reperfusion, as it occurs during transplanta-tion, have been reported. Livers from long-term fasted donorsappear capable of tolerating the transplant procedure better thanlivers obtained from fed donors.19-21 Nevertheless, preharvestingnutritional repletion by glucose supplementation improves sur-vival and liver function both in fasted and fed animals.20,22,23
Abbreviations: ALT, alanine transaminase; TEM, trasmission electron microscopy.From the Dipartimento di Medicina Interna, Cardioangiologia ed Epatologia1;
Dipartimento di Discipline Chirurgiche, Rianimatorie e dei Trapianti2; and Diparti-mento di Patologia Sperimentale,3 University of Bologna, Bologna, Italy; and Gastroen-terology, Department of Internal Medicine,4 Loyola University, Maywood, IL.
Received August 21, 1998; accepted December 30, 1998.P.C. was sponsored by a Fellowship of the Italian Association for the Study of the Liver
(AISF) and a Fellowship of the Italian Society of Gastroenterology (SIGE). This study wassupported in part by the Ministero dell’Universita e della Ricerca Scientifica e Tecnologica(M.U.R.S.T.) (Fondi ex-40%) and by the Consiglio Nazionale delle Ricerche (C.N.R.), Italy.
Address reprint requests to: Paolo Caraceni, M.D., Dipartimento di Medicina Interna,Cardioangiologia ed Epatologia, Universitv of Bologna, Policlinico Sant’Orsola, ViaMassarenti 9, 40138 Bologna, Italy. E-mail: [email protected]; fax: 39-051-340877.
Copyright r 1999 by the American Association for the Study of Liver Diseases.0270-9139/99/2904-0021$3.00/0
1139

To date, all of the data on the effect of fasting on hepaticischemia-reperfusion injury have been obtained using histo-logically normal livers. Whether the same results can beapplied to a fatty liver is unknown. Therefore, the aim of thisstudy was to determine the role of the animal nutritionalstatus on the consequences of normothermic hepatic ischemia-reperfusion injury occurring in rats with a fatty liver inducedby a choline-deficient diet.
MATERIALS AND METHODS
Animals and Induction of Fatty Liver
Male Wistar rats (Charles-River, Calco, LC, Italy), weighing 150to 175 g, were allowed to acclimate to the animal quarters and weregiven free access to a standard chow diet and water for 1 week.Steatosis was induced by feeding the animals a diet deficient incholine (Dyets Inc, Bethlehem, PA) for an additional 10 days. Control ratswere kept on the standard chow diet. Before death, the animal weight wassimilar in the two groups ranging between 250 to 280 g. All proceduresinvolving rats were conducted according to the guidelines for the careand use of laboratory animals approved by our institution.
Experimental Design and Surgical Procedure
The day before the experiment, both the rats with fatty liver andnormal liver were further divided as follows: (1) rats with free accessto food and water until the time of surgery (fed groups) and (2) ratswith access only to water for the 18 hours before surgery (fastedgroups). In a separate set of experiments, fasted rats with fatty liverwere housed in individual cages and randomly divided into two groups:(1) rats with free access to drinking water only, and (2) rats with freeaccess to a 40% glucose solution (glucose supplemented group).
Lobar liver ischemia-reperfusion followed by a partial hepatec-tomy of the noninvolved liver was performed in all animals using amodification of the technique described by Kawano et al.24 Briefly,under light enflurane anesthesia, the abdomen was opened througha midline incision and the left hepatic artery and portal vein wereoccluded with a nontraumatic microvascular clip inducing ischemiaof the left lateral and median lobes (<70% of the total liver volume).After 1 hour, the microvascular clip was released and the hepatec-tomy of the nonischemic right lateral and caudate lobes wasperformed. The abdomen was closed and the rats were left to recoverwith free access to the standard chow diet and water ad libitum. Thismodel of partial hepatic ischemia-reperfusion injury avoids splanch-nic congestion and, thus, any confounding effects resulting frombowel ischemia and hemodynamic disturbances. Moreover, resec-tion of the noninvolved portion forces the animal to survive only onthe liver lobes subjected to the ischemia-reperfusion insult as occursin the case of liver transplantation.25
The experimental animals were divided in groups of 5 to 6 unitsand killed under general anesthesia before ischemia (basal), after 60minutes of ischemia, and 30 minutes, 2 hours, 8 hours, and 24 hoursafter reperfusion. Liver and blood samples were collected andprepared for biochemical, histological, and ultrastructural analyses.
Survival
To determine the 7-day survival, rats (10-14 animals for eachgroup) were allowed to recover after surgery, housed in individualcages, and fed the standard chow diet and water ad libitum. Theirsurvival was assessed at least twice daily.
Serum Alanine Transaminase
Blood (1 mL) was collected under anesthesia from the inferiorvena cava at the time of sacrifice for measurement of serum alaninetransaminase (ALT) levels using a commercially available kit test.
Histology
A section of liver tissue measuring approximately 5 mm inthickness was cut from the center of each lobe and fixed in 10%
buffered formalin, processed by standard techniques and embeddedin paraffin. The tissue was cut at 4 µm and the sections were stainedwith hematoxylin-eosin. The histological analysis was performed ina blinded fashion by a single pathologist (M.D.).
Transmission Electron Microscopy
A second block of liver tissue, approximately 1 mm thick, was cutfrom the center of each lobe and diced into 1-mm cubes. All thesamples for transmission electron microscopy (TEM) analysis wereinitially fixed in 2.5% cacodylate-buffered glutaraldehyde, thenpostfixed with 1% OsO4, dehydrated in a graded series of alcohols,and embedded in araldite. Thin sections were obtained with aReichert Omu 3 ultramicrotome (C. Reichert, Wein, Austria),counterstained with uranyl acetate and lead citrate and examinedblindly by a single observer (M.D.) using a Philips 400T transmis-sion electron microscope (Philips, Eindhoven, The Netherlands).
Hepatic Glycogen Content
The preischemic hepatic glycogen content was quantified usingthe method of Keppler and Decker26 and expressed as mg/µg DNA.The liver DNA concentration was measured according to themethod of Schneider and Greco.27
Statistical Analysis
The statistical difference in survival between groups at eachtime-point was determined using the x2 test with the Fishercorrection when appropriate. Statistical differences in serum ALTlevels between groups were determined with ANOVA. Statisticaldifferences in hepatic glycogen content were determined withWilcoxon test. P , .05 was considered to be significant.
RESULTS
Survival
Fed Groups. Whereas all rats with normal liver remainedalive for 7 days from surgery, the survival of the rats with fatty liverwas significantly reduced (64% vs. 100%, P , .05) (Fig. 1).
Effect of Fasting. No significant difference in survival wasobserved between fasted and fed rats with normal liver (90%vs. 100%). In contrast, fasting had a dramatic effect in thepresence of steatosis. Fasted rats with fatty liver recoveredslowly from the anesthesia. Most of them developed grunting
FIG. 1. Seven-day survival of rats exposed to 60 minutes of hepatic lobarischemia followed by reperfusion. (s) Fed rats with normal liver; (d) fastedrats with normal liver; (n) fed rats with fatty liver; (m) fasted rats with fattyliver. #P , .05 vs. fed rats with normal liver. *P , .05 vs. all other groups.
1140 CARACENI ET AL. HEPATOLOGY April 1999
respiration and died within 12 to 24 hours of reperfusion.Survival at 7 days was 14% in fasted rats compared with 64%in fed rats with fatty liver (P , .001).
Serum ALT Levels
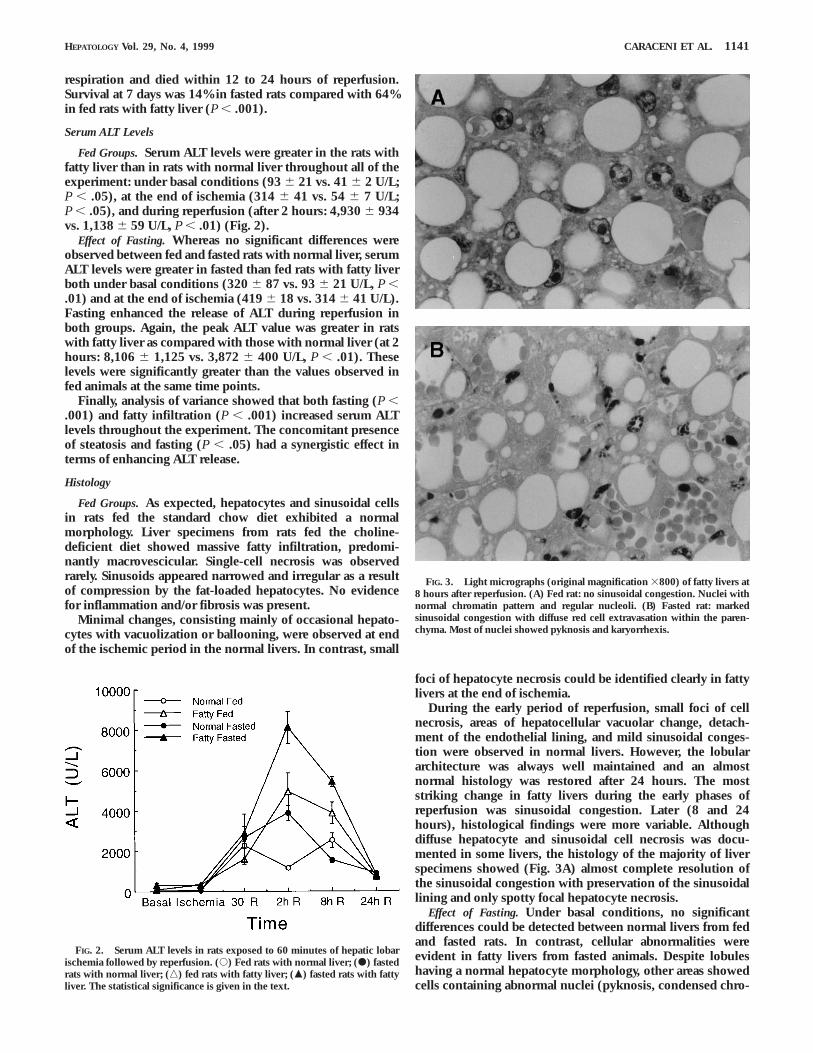
Fed Groups. Serum ALT levels were greater in the rats withfatty liver than in rats with normal liver throughout all of theexperiment: under basal conditions (93 6 21 vs. 41 6 2 U/L;P , .05), at the end of ischemia (314 6 41 vs. 54 6 7 U/L;P , .05), and during reperfusion (after 2 hours: 4,930 6 934vs. 1,138 6 59 U/L, P , .01) (Fig. 2).
Effect of Fasting. Whereas no significant differences wereobserved between fed and fasted rats with normal liver, serumALT levels were greater in fasted than fed rats with fatty liverboth under basal conditions (320 6 87 vs. 93 6 21 U/L, P ,.01) and at the end of ischemia (419 6 18 vs. 314 6 41 U/L).Fasting enhanced the release of ALT during reperfusion inboth groups. Again, the peak ALT value was greater in ratswith fatty liver as compared with those with normal liver (at 2hours: 8,106 6 1,125 vs. 3,872 6 400 U/L, P , .01). Theselevels were significantly greater than the values observed infed animals at the same time points.
Finally, analysis of variance showed that both fasting (P ,.001) and fatty infiltration (P , .001) increased serum ALTlevels throughout the experiment. The concomitant presenceof steatosis and fasting (P , .05) had a synergistic effect interms of enhancing ALT release.
Histology
Fed Groups. As expected, hepatocytes and sinusoidal cellsin rats fed the standard chow diet exhibited a normalmorphology. Liver specimens from rats fed the choline-deficient diet showed massive fatty infiltration, predomi-nantly macrovescicular. Single-cell necrosis was observedrarely. Sinusoids appeared narrowed and irregular as a resultof compression by the fat-loaded hepatocytes. No evidencefor inflammation and/or fibrosis was present.
Minimal changes, consisting mainly of occasional hepato-cytes with vacuolization or ballooning, were observed at endof the ischemic period in the normal livers. In contrast, small
foci of hepatocyte necrosis could be identified clearly in fattylivers at the end of ischemia.
During the early period of reperfusion, small foci of cellnecrosis, areas of hepatocellular vacuolar change, detach-ment of the endothelial lining, and mild sinusoidal conges-tion were observed in normal livers. However, the lobulararchitecture was always well maintained and an almostnormal histology was restored after 24 hours. The moststriking change in fatty livers during the early phases ofreperfusion was sinusoidal congestion. Later (8 and 24hours), histological findings were more variable. Althoughdiffuse hepatocyte and sinusoidal cell necrosis was docu-mented in some livers, the histology of the majority of liverspecimens showed (Fig. 3A) almost complete resolution ofthe sinusoidal congestion with preservation of the sinusoidallining and only spotty focal hepatocyte necrosis.
Effect of Fasting. Under basal conditions, no significantdifferences could be detected between normal livers from fedand fasted rats. In contrast, cellular abnormalities wereevident in fatty livers from fasted animals. Despite lobuleshaving a normal hepatocyte morphology, other areas showedcells containing abnormal nuclei (pyknosis, condensed chro-
FIG. 2. Serum ALT levels in rats exposed to 60 minutes of hepatic lobarischemia followed by reperfusion. (s) Fed rats with normal liver; (d) fastedrats with normal liver; (n) fed rats with fatty liver; (m) fasted rats with fattyliver. The statistical significance is given in the text.
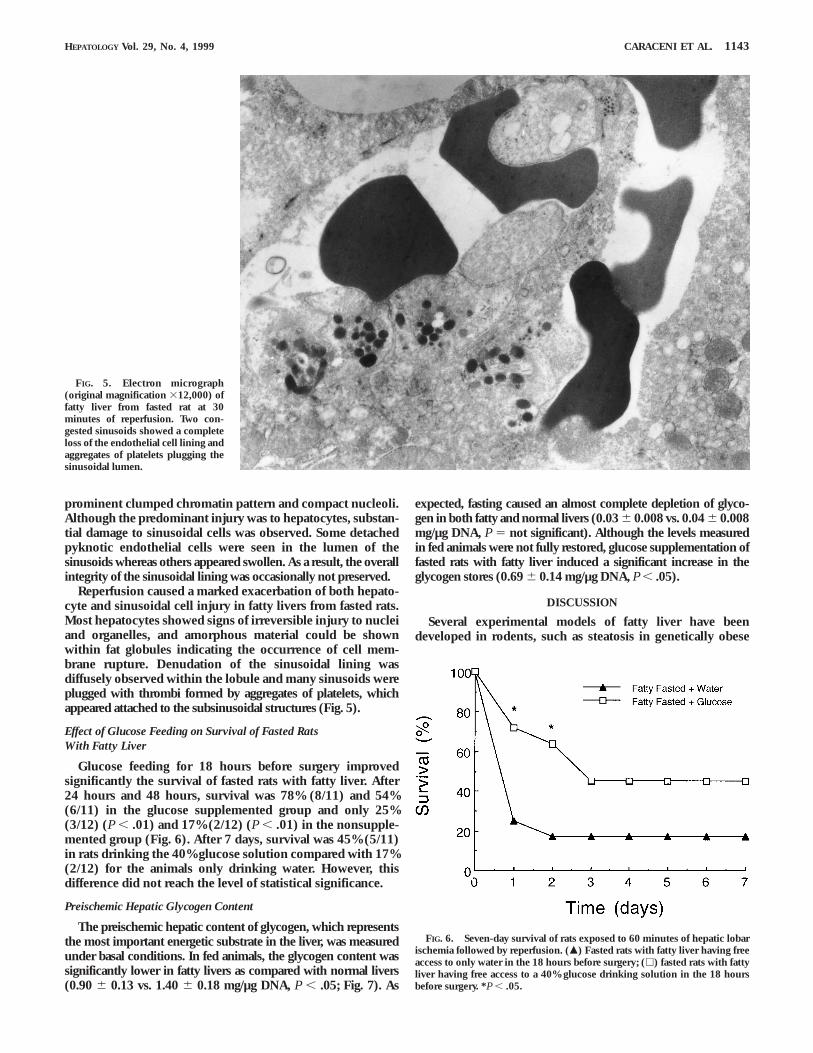
FIG. 3. Light micrographs (original magnification 3800) of fatty livers at8 hours after reperfusion. (A) Fed rat: no sinusoidal congestion. Nuclei withnormal chromatin pattern and regular nucleoli. (B) Fasted rat: markedsinusoidal congestion with diffuse red cell extravasation within the paren-chyma. Most of nuclei showed pyknosis and karyorrhexis.
HEPATOLOGY Vol. 29, No. 4, 1999 CARACENI ET AL. 1141

matin pattern, irregular margins); the coalescence of two tothree fat globules as a result of cell membrane rupture couldbe also identified.
At the end of ischemia, minimal changes similar to thoseobserved basal fed conditions were observed in the normal livers.In contrast, in the fatty livers, hepatocytes with pyknotic nucleiwere diffusely present throughout the lobule. The morphology ofsinusoidal cells appeared to be substantially spared.
Although the extent of tissue injury was greater in normalfasted liver, the histological findings and their time courseduring reperfusion were similar to those seen in fed normalanimals. Conversely, fasting had a dramatic impact on thetissue damage present in rats with fatty liver. With reperfu-sion, sinusoids became greatly dilated and were filled withblood elements and cell debris. The continuity of the sinusoi-dal lining was disrupted and red blood cells could be foundwithin fat globules. As shown in Fig. 3B, at 8 hours afterreperfusion, the histology showed a diffuse hemorrhagicnecrosis. The sinusoidal architecture was disrupted with wideareas of red cell extravasation within the parenchyma. Mostof the hepatocytes had pyknosis or karyorrhexis of the nuclei.
TEM
TEM was used to identify and detail whether fastinginduced ultrastructural abnormalities in fatty liver underbasal conditions, at the end of ischemia, and in the earlyphase of reperfusion.
Fed Groups. The preischemic electron microscopic appear-ance of the normal livers showed the regular ultrastructure ofthe hepatocytes and sinusoidal cells. Similarly, no alterationswere observed in almost all fatty hepatocytes under basalconditions, although the nuclei and the organelles weredisplaced and compressed to the periphery of the cell by large
lipid globules. A few hepatocytes had ultrastructural alterations oftheir mitochondria. The sinusoidal cells appeared normal.
At the end of the ischemic period, a marked injury tohepatocytes was seen only in the presence of fatty infiltration.Aside from hepatocytes with normal ultrastructure, otherspresented swollen and rounded mitochondria, cytoplasmicvacuolization, and nuclei with condensed chromatin. Theendothelial lining was preserved.
At 30 minutes of reperfusion, fatty hepatocytes presented awide range of ultrastructural abnormalities, and a marked injuryof the sinusoidal cells was also observed in several areas. Theendothelial cells showed a clumped chromatin nuclear pattern,and pyknotic endothelial cells were found inside the sinusoidallumen. As a result, the continuity of the sinusoidal lining wassometimes disrupted. However, the extent of these abnormalitiesgreatly varies within the liver, and areas with a preserved hepato-cyte and endothelial cell ultrastructure were also found.
Effect of Fasting. Under basal conditions, the hepatocytesfrom normal livers had regular appearance, whereas severalhepatocytes from fatty livers showed nuclei with a condensedchromatin pattern and mitochondrial damage. The ultrastruc-ture of the sinusoidal cells was retained.
Fasting exacerbated the ultrastructural damage occurringas a result of ischemia in both groups. The enhancement ofinjury seen with fasting was much greater in steatotic livers(Fig. 4). Almost all of the fatty hepatocytes showed structuralalterations of organelles and nuclei. The most prominentfinding was the damage of mitochondria, which appearedmarkedly swollen, rounded, and with loss of cristae andpredominant clear matrix. The normal stacked arrangementsof the rough endoplasmic reticulum was disrupted andvariable-sized vacuoles containing pieces of membranousmaterial were present in the cytoplasma. The nuclei had a
FIG. 4. Electron micrograph(original magnification 326,000) offatty liver from fasted rat at the endof 60 minutes of ischemia. Mitochon-dria are markedly swollen, rounded,with loss of cristae and predominantclear matrix. Nucleus presents aprominent clumped chromatin pat-tern.
1142 CARACENI ET AL. HEPATOLOGY April 1999
prominent clumped chromatin pattern and compact nucleoli.Although the predominant injury was to hepatocytes, substan-tial damage to sinusoidal cells was observed. Some detachedpyknotic endothelial cells were seen in the lumen of thesinusoids whereas others appeared swollen. As a result, the overallintegrity of the sinusoidal lining was occasionally not preserved.
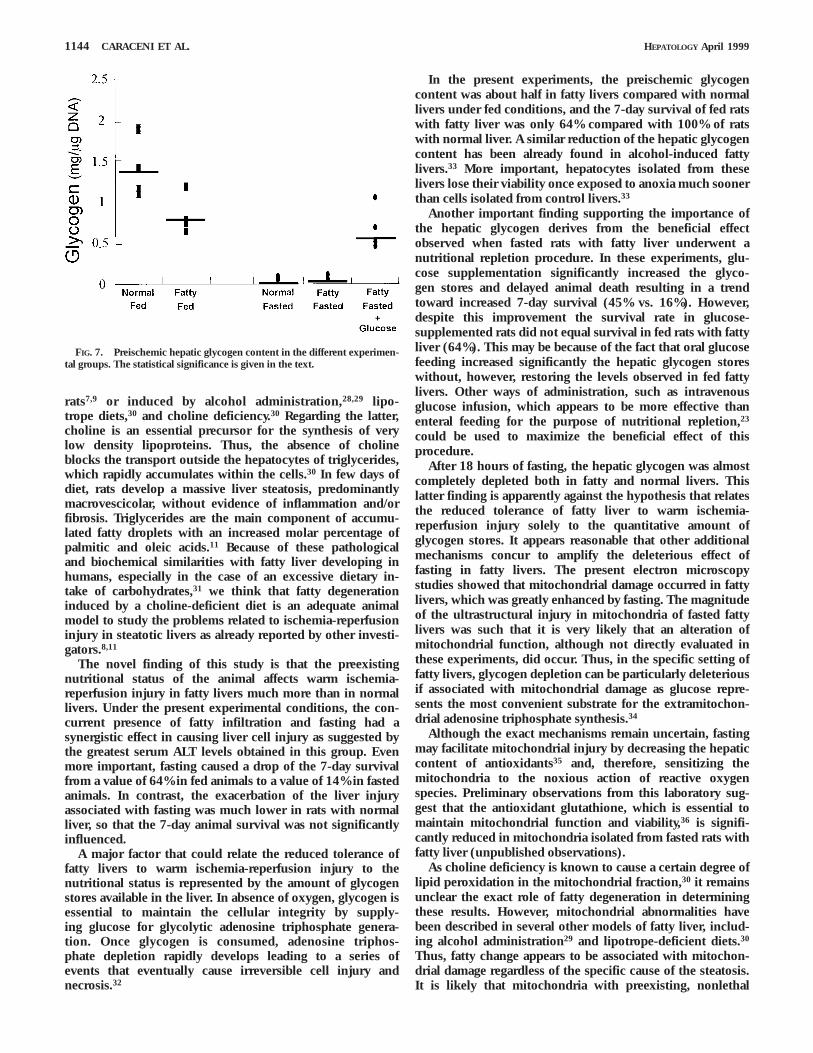
Reperfusion caused a marked exacerbation of both hepato-cyte and sinusoidal cell injury in fatty livers from fasted rats.Most hepatocytes showed signs of irreversible injury to nucleiand organelles, and amorphous material could be shownwithin fat globules indicating the occurrence of cell mem-brane rupture. Denudation of the sinusoidal lining wasdiffusely observed within the lobule and many sinusoids wereplugged with thrombi formed by aggregates of platelets, whichappeared attached to the subsinusoidal structures (Fig. 5).
Effect of Glucose Feeding on Survival of Fasted RatsWith Fatty Liver
Glucose feeding for 18 hours before surgery improvedsignificantly the survival of fasted rats with fatty liver. After24 hours and 48 hours, survival was 78% (8/11) and 54%(6/11) in the glucose supplemented group and only 25%(3/12) (P , .01) and 17% (2/12) (P , .01) in the nonsupple-mented group (Fig. 6). After 7 days, survival was 45% (5/11)in rats drinking the 40% glucose solution compared with 17%(2/12) for the animals only drinking water. However, thisdifference did not reach the level of statistical significance.
Preischemic Hepatic Glycogen Content
The preischemic hepatic content of glycogen, which representsthe most important energetic substrate in the liver, was measuredunder basal conditions. In fed animals, the glycogen content wassignificantly lower in fatty livers as compared with normal livers(0.90 6 0.13 vs. 1.40 6 0.18 mg/µg DNA, P , .05; Fig. 7). As
expected, fasting caused an almost complete depletion of glyco-gen in both fatty and normal livers (0.03 6 0.008 vs. 0.04 6 0.008mg/µg DNA, P 5 not significant). Although the levels measuredin fed animals were not fully restored, glucose supplementation offasted rats with fatty liver induced a significant increase in theglycogen stores (0.69 6 0.14 mg/µg DNA, P , .05).
DISCUSSION
Several experimental models of fatty liver have beendeveloped in rodents, such as steatosis in genetically obese
FIG. 5. Electron micrograph(original magnification 312,000) offatty liver from fasted rat at 30minutes of reperfusion. Two con-gested sinusoids showed a completeloss of the endothelial cell lining andaggregates of platelets plugging thesinusoidal lumen.
FIG. 6. Seven-day survival of rats exposed to 60 minutes of hepatic lobarischemia followed by reperfusion. (m) Fasted rats with fatty liver having freeaccess to only water in the 18 hours before surgery; (h) fasted rats with fattyliver having free access to a 40% glucose drinking solution in the 18 hoursbefore surgery. *P , .05.
HEPATOLOGY Vol. 29, No. 4, 1999 CARACENI ET AL. 1143
rats7,9 or induced by alcohol administration,28,29 lipo-trope diets,30 and choline deficiency.30 Regarding the latter,choline is an essential precursor for the synthesis of verylow density lipoproteins. Thus, the absence of cholineblocks the transport outside the hepatocytes of triglycerides,which rapidly accumulates within the cells.30 In few days ofdiet, rats develop a massive liver steatosis, predominantlymacrovescicolar, without evidence of inflammation and/orfibrosis. Triglycerides are the main component of accumu-lated fatty droplets with an increased molar percentage ofpalmitic and oleic acids.11 Because of these pathologicaland biochemical similarities with fatty liver developing inhumans, especially in the case of an excessive dietary in-take of carbohydrates,31 we think that fatty degenerationinduced by a choline-deficient diet is an adequate animalmodel to study the problems related to ischemia-reperfusioninjury in steatotic livers as already reported by other investi-gators.8,11
The novel finding of this study is that the preexistingnutritional status of the animal affects warm ischemia-reperfusion injury in fatty livers much more than in normallivers. Under the present experimental conditions, the con-current presence of fatty infiltration and fasting had asynergistic effect in causing liver cell injury as suggested bythe greatest serum ALT levels obtained in this group. Evenmore important, fasting caused a drop of the 7-day survivalfrom a value of 64% in fed animals to a value of 14% in fastedanimals. In contrast, the exacerbation of the liver injuryassociated with fasting was much lower in rats with normalliver, so that the 7-day animal survival was not significantlyinfluenced.
A major factor that could relate the reduced tolerance offatty livers to warm ischemia-reperfusion injury to thenutritional status is represented by the amount of glycogenstores available in the liver. In absence of oxygen, glycogen isessential to maintain the cellular integrity by supply-ing glucose for glycolytic adenosine triphosphate genera-tion. Once glycogen is consumed, adenosine triphos-phate depletion rapidly develops leading to a series ofevents that eventually cause irreversible cell injury andnecrosis.32
In the present experiments, the preischemic glycogencontent was about half in fatty livers compared with normallivers under fed conditions, and the 7-day survival of fed ratswith fatty liver was only 64% compared with 100% of ratswith normal liver. A similar reduction of the hepatic glycogencontent has been already found in alcohol-induced fattylivers.33 More important, hepatocytes isolated from theselivers lose their viability once exposed to anoxia much soonerthan cells isolated from control livers.33
Another important finding supporting the importance ofthe hepatic glycogen derives from the beneficial effectobserved when fasted rats with fatty liver underwent anutritional repletion procedure. In these experiments, glu-cose supplementation significantly increased the glyco-gen stores and delayed animal death resulting in a trendtoward increased 7-day survival (45% vs. 16%). However,despite this improvement the survival rate in glucose-supplemented rats did not equal survival in fed rats with fattyliver (64%). This may be because of the fact that oral glucosefeeding increased significantly the hepatic glycogen storeswithout, however, restoring the levels observed in fed fattylivers. Other ways of administration, such as intravenousglucose infusion, which appears to be more effective thanenteral feeding for the purpose of nutritional repletion,23
could be used to maximize the beneficial effect of thisprocedure.
After 18 hours of fasting, the hepatic glycogen was almostcompletely depleted both in fatty and normal livers. Thislatter finding is apparently against the hypothesis that relatesthe reduced tolerance of fatty liver to warm ischemia-reperfusion injury solely to the quantitative amount ofglycogen stores. It appears reasonable that other additionalmechanisms concur to amplify the deleterious effect offasting in fatty livers. The present electron microscopystudies showed that mitochondrial damage occurred in fattylivers, which was greatly enhanced by fasting. The magnitudeof the ultrastructural injury in mitochondria of fasted fattylivers was such that it is very likely that an alteration ofmitochondrial function, although not directly evaluated inthese experiments, did occur. Thus, in the specific setting offatty livers, glycogen depletion can be particularly deleteriousif associated with mitochondrial damage as glucose repre-sents the most convenient substrate for the extramitochon-drial adenosine triphosphate synthesis.34
Although the exact mechanisms remain uncertain, fastingmay facilitate mitochondrial injury by decreasing the hepaticcontent of antioxidants35 and, therefore, sensitizing themitochondria to the noxious action of reactive oxygenspecies. Preliminary observations from this laboratory sug-gest that the antioxidant glutathione, which is essential tomaintain mitochondrial function and viability,36 is signifi-cantly reduced in mitochondria isolated from fasted rats withfatty liver (unpublished observations).
As choline deficiency is known to cause a certain degree oflipid peroxidation in the mitochondrial fraction,30 it remainsunclear the exact role of fatty degeneration in determiningthese results. However, mitochondrial abnormalities havebeen described in several other models of fatty liver, includ-ing alcohol administration29 and lipotrope-deficient diets.30
Thus, fatty change appears to be associated with mitochon-drial damage regardless of the specific cause of the steatosis.It is likely that mitochondria with preexisting, nonlethal
FIG. 7. Preischemic hepatic glycogen content in the different experimen-tal groups. The statistical significance is given in the text.
1144 CARACENI ET AL. HEPATOLOGY April 1999

alterations are more prone to develop irreversible dysfunctionwhen exposed to a second injury.
At the best of our knowledge, this study also provides thefirst description of the effect of the nutritional status on themorphological changes associated with ischemia-reperfusioninjury in rat fatty livers. We confirmed that the most strikinghistological feature is represented by the alteration of thehepatic microcirculation during reperfusion, as already de-scribed with this and other models of fatty livers.6,8,11
However, the degree of microvascular injury was clearlydifferent between fed and fasted animals. Under fed condi-tions, the sinusoidal congestion observed in the first 2 hoursof reperfusion reversed almost completely after 8 and 24hours in the majority of rats. In contrast, under fastedconditions, the initial sinusoidal congestion was followed bydiffuse disruption of the sinusoidal wall, extensive red bloodcell extravasation, and development of massive hemorrhagicnecrosis. TEM confirmed the occurrence of an extensivemicrovascular injury in fatty livers from fasted rats showing,in the early phase of reperfusion, irreversible injury ofendothelial cells and obstruction of the sinusoidal lumenbecause of thrombi formation.
As a whole, it appears that both a disruption of the hepaticmicrocirculation during reperfusion and severe hepatocytedamage during warm ischemia contribute to the pathogenesisof ischemia-reperfusion injury in fatty livers. Thus, it is notsurprising that a single-step approach, such as administrationof anti–intercellular adhesion molecule-1 monoclonal anti-body, which abolishes sinusoidal congestion,11 or glucosesupplementation, which enhances the ability of hepato-cytes to tolerate ischemic injury,37 improves but does notnormalize the survival of rats with fatty liver after ischemia-reperfusion.
In conclusion, this study shows that rat fatty livers exposedto normothermic ischemia-reperfusion injury are much moresensitive to fasting than histologically normal livers. Mitochon-drial damage may contribute to amplify the deleterious effectof glycogen depletion in the presence of fatty change. Becauseglucose supplementation improves both the amount of glyco-gen stores in the liver and animal survival after hepaticischemia-reperfusion, a nutritional repletion procedure maybe part of a treatment strategy aimed at preventing this injuryin fatty livers and, if this also occurs in humans, to improvethe successful use of such marginal organs in clinical livertransplantation.
REFERENCES
1. Huguet C, Gavelli A, Chieco A, Bona S, Harb J, Joseph JM, Jobard J, et al.Liver ischemia for hepatic resection: where is the limit? Surgery1992;111:251-259.
2. Strasberg SM, Howard TK, Molmenti EP, Hertl M. Selecting the donorliver: risk factors for poor function after orthotopic liver transplantation.HEPATOLOGY 1994;20:829-838.
3. D’Alessandro AM, Kalayoglu M, Sollinger HW, Hoffmann RM, Reed A,Knechtle SJ, Pirsch JD, et al. The predictive value of donor liver biopsiesfor the development of primary non-function after orthotopic livertransplantation. Transplantation 1991;51:157-163.
4. Adam R, Reynes M, Johann M, Morino M, Astaarcioglu I, Kafetzis I,Castaing D, et al. The outcome of steatotic grafts in liver transplantation.Transplant Proc 1991;23:1538-1540.
5. Teramoto K, Bowers JL, Khettry U, Palombo JD, Clouse ME. A rat fattyliver transplant model. Transplantation 1993;55:737-741.
6. Teramoto K, Bowers JL, Kruskal JB, Clouse ME. Hepatic microcircula-tory changes after reperfusion in fatty and normal liver transplantationin rat. Transplantation 1993;56:1076-1082.
7. Husberg BS, Genyk YS, Klintmalm GB. A new rat model for studies of theischemic injury after transplantation of fatty livers: improvement afterpostoperative administration of prostaglandin. Transplantation 1994;57:457-458.
8. Hui A, Kawasaki S, Makuuchi M, Nakayama J, Ikegami T, Miyagawa J.Liver injury following normothermic ischemia in steatotic rat liver.HEPATOLOGY 1994;20:1287-1293.
9. Koneru B, Reddy MC, Dela Torre AN, Patel D, Ippolito T, Ferrante RJ.Studies of hepatic warm ischemia in the obese Zucker rat. Transplanta-tion 1995;59:942-946.
10. Nakano H, Nagasaki H, Barama A, Boudjema K, Jaeck D, Kumana K,Tatsuno M, et al. The effects of N-acetylcisteine and anti-intercellularadhesion molecule-1 monoclonal antibody against ischemia-reperfusioninjury of the rat steatotic liver produced by a choline methionine-deficient diet. HEPATOLOGY 1997;26:670-678.
11. Hakamada K, Sasaki M, Takahashi K, Umehara Y, Konn M. Sinusoidalflow block after warm ischemia in rats with diet-induced fatty liver. JSurg Res 1997;70:12-20.
12. Huguet C, Gavelli A, Harb J, Roger-Clement R, De Millo D, LasserreM, McNamara MT. L’ischemie du foie de plus d’une heure est-elle unfacteur de gravite des hepatectomies? A propos de 19 cas. 1991;117:351-356.
13. Markin RS, Wisecarver JL, Radio SJ, Stratta RJ, Langnas AN, Hirst K,Shaw BW. Frozen section evaluation of donor livers before transplanta-tion. Transplantation 1993;56:1403-1409.
14. Ploeg RJ, D’Alessandro AM, Knechtle SJ, Stegall MD, Pirsh JD, HoffmanRM, Sasaki T, et al. Risk factors for primary dysfunction after livertransplantation: a multivariate analysis. Transplantation 1993;55:807-813.
15. Trevisani F, Colantoni A, Caraceni P, Van Thiel DH. The use of donorfatty liver for liver transplantation: a challenge or a quagmire? J Hepatol1996;22:114-121.
16. Purim J, Van Woerden WF, Knol E. Donor data in liver grafts withprimary non-function—a preliminary analysis by the European liverregistry. Transpl Proc 1989;21:2383-2384.
17. Gasbarrini A, Borle AB, Farghali H, Caraceni P, Van Thiel DH. Fastingenhances the effects of anoxia on ATP, Cai
11, and cell injury in isolatedrat hepatocytes. Biochim Bioph Acta 1993;1178:9-19.
18. Bradford BU, Maotto M, Lemaster JJ, Thurman RG. New, simple modelsto evaluate zone-specific damage due to hypoxia in the perfused rat liver:time course and effect of nutritional status. J Pharmacol Exp Ther1986;236:263-268.
19. Sankary H, Foster P, Brown E, Bhattachyarvya A, Williams J. Relevanceof the nutritional status in viability of transplanted hepatic allografts.Transplantation 1992;54:170-172.
20. Sumimoto R, Southard JH, Belzer FO. Livers from fasted rats acquireresistance to warm and cold ischemia. Transplantation 1993;55:728-732.
21. Lindell SL, Hansen T, Rankin M, Danielewicz R, Belzer FO, Southard JH.Donor nutritional status—a determinant of liver preservation injury.Transplantation 1996;61:239-247.
22. Cywes R, Greig PD, Morgan GR, Sanabria JR, Clavien PA, Harvey PRC,Strasberg SM. Rapid donor liver nutritional enhancement in a largeanimal model. HEPATOLOGY 1992;16:1271-1279.
23. Sadamori H, Tanaka N, Yagi T, Inagaki M, Orita K. The effects ofnutritional repletion on donors for liver transplantation in pigs. Trans-plantation 1995;60:317-321.
24. Kawano K, Kim Y, Kaketani K, Kobayashi M. The beneficial effect ofcyclosporine on liver ischemia in rats. Transplantation 1989;48:759-764.
25. Peng XX, Currin RT, Thurman RG, Leemaster JJ. Protection by pentoxi-fylline against normothermic liver ischemia/reperfusion in rats. Trans-plantation 1995;11:1537-1541.
26. Keppler D, Decker K. Glycogen. In: Bergmeyer HU, ed. Methods ofEnzymatic Analysis. Volume 6. Deerfield Beach, FL: Verlag Chemic,1986;11-18.
27. Schneider WC, Greco AE. Incorporation of pyrimidine deoxyribonucleo-sides into liver lipids and other components. Biochim Biophys Acta1971;228:610-626.
28. Gao W, Connor HD, Leemaster JJ, Mason RP, Thurman RG. Primarynon-function of fatty livers produced by alcohol is associated with a new,antioxidant insensitive free radical species. Transplantation 1995;59:674-679.
29. Lieber CS. Alcohol and the liver: 1994 update. Gastroenterology1994;106:1085-1105.
HEPATOLOGY Vol. 29, No. 4, 1999 CARACENI ET AL. 1145

30. Ghoshal AK, Farber E. Choline deficiency, lipotrope deficiency and thedevelopment of liver disease including liver cancer: a new perspective.Lab Invest 1993;68:255-260.
31. Hoyumpa AM, Greene HL, Dunn GL, Shenker SDD. Fatty liver: bio-chemical and clinical consideration. Dig Dis Sci 1975;20:1142-1147.
32. Rosser BG, Gores GJ. Liver cell necrosis: cellular mechanisms andclinical implications. Gastroenterology 1995;108:252-275.
33. Caraceni P, Ryu HO, Subbotin V, De Maria N, Colantoni A, Roberts L,Trevisani F, et al. Rat hepatocytes isolated from alcohol-induced fatty liverhave an increased sensitivity to anoxic injury. HEPATOLOGY 1997;25:943-949.
34. Hochachka PW, Castellini JM, Hill RD, Schneider RC, Bengston JL, HillSE, Liggins GC, et al. Protective metabolic mechanisms during liver
ischemia: transferable lessons from long-diving animals. Mol CellBiochem 1988;84:77-85.
35. Di Simplicio P, Rossi R, Falcinelli S, Ceserani R, Formento ML.Antioxidants status in various tissues of the mouse after fasting andswimming stress. Eur J Appl Physiol 1997;76:302-307.
36. Martensson J, Meister A. Mitochondrial damage in muscle occurs aftermarked depletion of glutathione and is prevented by giving glutathionemonoester. Proc Natl Acad Sci U S A 1989;86:471-475.
37. Cywes R, Greig PD, Sanabria JR, Clavien PA, Levy GA, Harvey RC,Strasberg SM. Effect of intraportal glucose infusion on hepatic glycogencontent and degradation, and outcome of liver transplantation. Ann Surg1992;216:235-246.
1146 CARACENI ET AL. HEPATOLOGY April 1999