investor webinar - clinical operations presentation...
TRANSCRIPT

Kelvin A. Baggett, M.D., M.P.H., M.B.A.SVP, Clinical Operations & Chief Medical Officer
December 10, 2012
Clinical Operations
Forward-looking Statements
Certain statements contained in this presentation constitute “forward-looking statements” within the meaning of Section 27A of the Securities Act of1933 and Section 21E of the Securities Exchange Act of 1934. Such forward-looking statements are based on management's current expectationsand involve known and unknown risks, uncertainties and other factors that may cause the Company’s actual results to be materially different fromthose expressed or implied by such forward-looking statements. Such factors include, among others, the following: the passage of heath carereform legislation and the enactment of additional federal and state health care reform; other changes in federal, state and local laws andregulations affecting the health care industry; general economic and business conditions, both nationally and regionally; demographic changes;changes in, or the failure to comply with, laws and governmental regulations; the ability to enter into managed care provider arrangements onacceptable terms; changes in Medicare and Medicaid payments or reimbursement; liability and other claims asserted against the Company;competition, including the Company’s ability to attract patients to its hospitals; technological and pharmaceutical improvements that increase thecost of providing, or reduce the demand for, health care; changes in business strategy or development plans; the ability to attract and retainqualified personnel, including physicians, nurses and other health care professionals, and the impact on the Company’s labor expenses resultingfrom a shortage of nurses or other health care professionals; the significant indebtedness of the Company; the Company's ability to integrate newbusinesses with its existing operations; the availability and terms of capital to fund the expansion of the Company's business, including theacquisition of additional facilities; the creditworthiness of counterparties to the Company’s business transactions; adverse fluctuations in interestrates and other risks related to interest rate swaps or any other hedging activities the Company undertakes; the ability to continue to expand andrealize earnings contributions from the revenue cycle management, health care information management, capitation management, and patientcommunications services businesses under our Conifer Health Solutions (“Conifer”) subsidiary by marketing these services to third party hospitalsand other health care-related entities; and its ability to identify and execute on measures designed to save or control costs or streamline operations.Such factors also include the positive and negative effects of health reform legislation on reimbursement and utilization and the future designs ofprovider networks and insurance plans, including pricing, provider participation, coverage and co-pays and deductibles, all of which containsignificant uncertainty, and for which multiple models exist which may differ materially from the company's expectations. Certain additional risksand uncertainties are discussed in the Company’s filings with the Securities and Exchange Commission, including the Company’s annual report onForm 10-K and quarterly reports on Form 10-Q. The information contained in this presentation is as of November 7, 2012. The Companyspecifically disclaims any obligation to update any forward-looking statement, whether as a result of changes in underlying factors, new information,future events or otherwise.
Non-GAAP Information
This presentation includes certain financial measures such as Adjusted EBITDA, which are not calculated in accordance with generally acceptedaccounting principles (GAAP). Management recommends that you focus on the GAAP numbers as the best indicator of financial performance.These alternative measures are provided only as a supplement to aid in analysis of the Company. Reconciliation between non-GAAP measures andrelated GAAP measures can be found in the Company’s third quarter earnings release issued on November 7, 2012.
2
Overview
3
• Highlight of External Factors and Internal Focus
• Tenet’s Quality Agenda 1.0 vs. 2.0
• Delivering Results
• Looking to 2014 and Beyond
• Key Takeaways
• Open Discussion and Q&A
Driven by private and public payer-led initiatives to contain costs and improve quality, three trends have emerged:
We believe these trends will continue
The Changing Environment of Healthcare
Reimbursement focused on value
Renewed focus on safety and the prevention of hospital‐acquired conditions and preventable readmissions; and
Greater alignment of providers of care through clinical integration models like accountable care organizations.
4
Our Strategy is Clear
5
Differentiate our hospitals through superior quality and
service, growing our business by providing greater value to
customers
Align physicians more closely with our facilities in order to
improve quality and efficiency
Control cost through our Medicare Performance Initiative and other initiatives designed to increase the efficiency and cost-effectiveness of care provided to
our patients
Acquire acute care hospitals to strengthen our markets or as opportunities emerge in new
markets
Grow Conifer Health Solutions both in number of customers and
services we offer to third-party health care providers
Grow our outpatient footprint through acquisitions to develop new channels for our hospitals
and patients
Tenet’s Strategy is to:

Commitment to Quality – Key Strategic Initiative
• Focused on Core Process Measures Performance• Early adopter of these proxy measures for associated outcomes• Continue to exceed the national average
• Dedicated to creating industry leading ED and OR throughput times
Center of Excellence Designations by Managed Care
• Strategy to differentiate Tenet hospitals• Anticipation of narrow networks/steering
Measuring Satisfaction of Patients and Physicians
• Absence of industry comparative benchmarking • Relationship between satisfaction and engagement unclear
Clinical Quality: Quality Agenda 1.0Process Focused
6

80.0
81.1
82.8
84.7
87.2
88.8
89.7
88.5
89.690.4
90.891.2
92.2
93.193.8
94.4 94.795.1
95.796.2
96.697.0 97.2 97.5
98.0 98.2 98.3 98.5 98.598.5
80.581.5
82.3
83.3
84.7
85.986.7
86.287.0
88.088.6
89.3
90.3
91.3
92.2
93.2 93.594.1
94.695.0 95.3 95.5 95.7 96.0
96.6 96.9 97.197.5
77
79
81
83
85
87
89
91
93
95
97
99
Q20
4-Q
105
Q30
4-Q
205
Q40
4-Q
305
Q10
5-Q
405
Q20
5-Q
106
Q30
5-Q
206
Q40
5-Q
306
Q10
6-Q
406
Q20
6-Q
107
Q30
6-Q
207
Q40
6-Q
307
Q10
7-Q
407
Q20
7-Q
108
Q30
7-Q
208
Q40
7-Q
308
Q10
8-Q
408
Q20
8-Q
109
Q30
8-Q
209
Q40
8-Q
309
Q10
9-Q
409
Q20
9-Q
110
Q30
9-Q
210
Q40
9-Q
310
Q11
0-Q
410
Q21
0-Q
111
Q31
0-Q
211
Q41
0-Q
311
Q11
1-Q
411
Q21
1-Q
112
Q31
1-Q
212
Tenet %
National Average %
CMS Hospital Compare- Core Measures Tenet Trend vs. National Average
Note: 1. Source Data: CMS Hospital Compare website.
7

166
202
260
306 305 308
2007 2008 2009 2010 2011 2012
Tenet Quality Is Recognized By Insurers
Centers of Excellence and Other Quality Designations for Tenet Hospitals and Service Lines
8
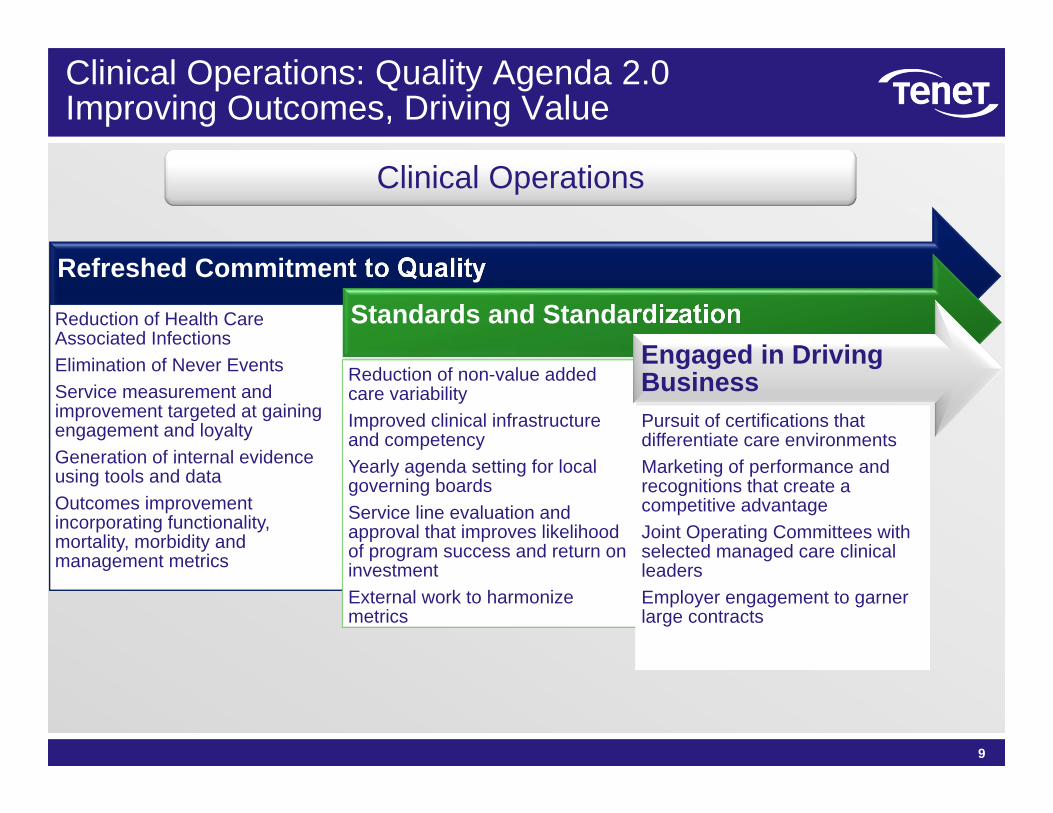
Refreshed Commitment to Quality
Reduction of Health Care Associated InfectionsElimination of Never EventsService measurement and improvement targeted at gaining engagement and loyaltyGeneration of internal evidence using tools and dataOutcomes improvement incorporating functionality, mortality, morbidity and management metrics
Standards and Standardization
Reduction of non-value added care variabilityImproved clinical infrastructure and competencyYearly agenda setting for local governing boardsService line evaluation and approval that improves likelihood of program success and return on investmentExternal work to harmonize metrics
Engaged in Driving BusinessPursuit of certifications that differentiate care environments Marketing of performance and recognitions that create a competitive advantageJoint Operating Committees with selected managed care clinical leadersEmployer engagement to garner large contracts
Clinical Operations: Quality Agenda 2.0Improving Outcomes, Driving Value
9
Clinical Operations
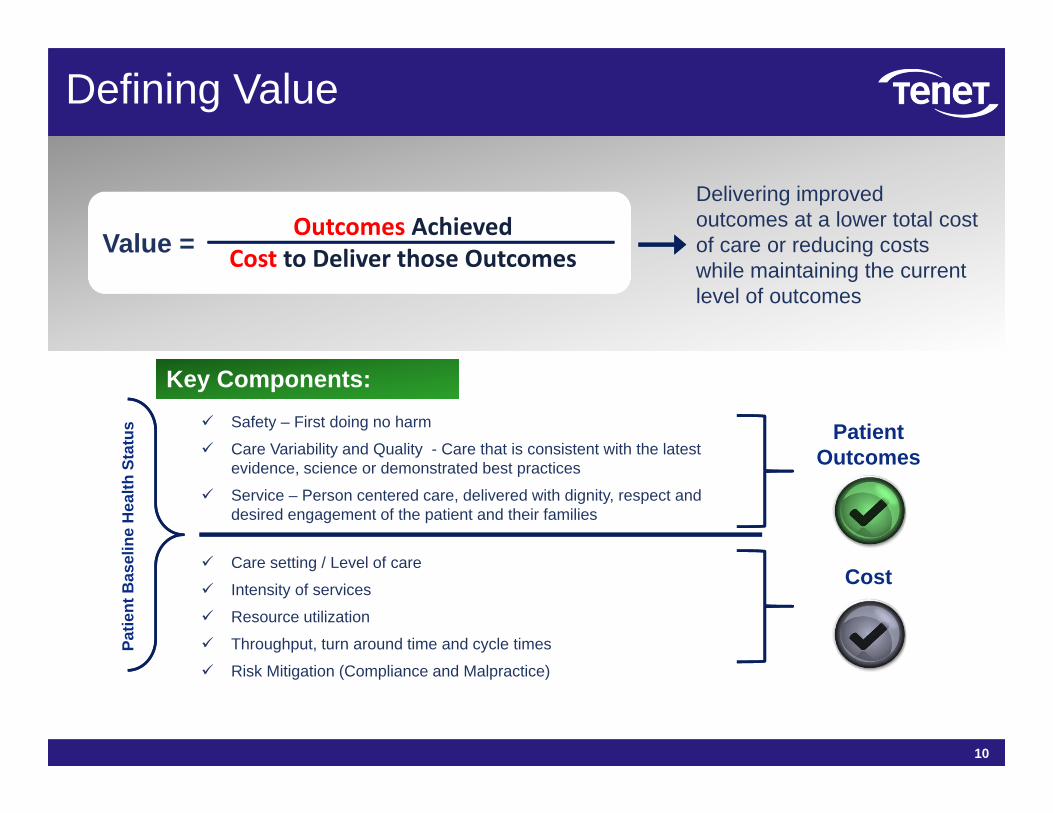
Delivering improved outcomes at a lower total cost of care or reducing costs while maintaining the current level of outcomes
Value = Outcomes AchievedCost to Deliver those Outcomes
Safety – First doing no harm
Care Variability and Quality - Care that is consistent with the latest evidence, science or demonstrated best practices
Service – Person centered care, delivered with dignity, respect and desired engagement of the patient and their families
Key Components:Key Components:
Care setting / Level of care
Intensity of services
Resource utilization
Throughput, turn around time and cycle times
Risk Mitigation (Compliance and Malpractice)
Patient Outcomes
Cost
Patie
nt B
asel
ine
Hea
lth S
tatu
s
Defining Value
10

Clinical Operational Performance Improvement Objectives Framework
Healthcare Associated Infections (HAIs)
Healthcare Associated Infections (HAIs)
Hospital Acquired Conditions (HACs)Hospital Acquired Conditions (HACs)
Elective DeliveriesElective Deliveries
Patient FallsPatient Falls
Never EventsNever Events
Venous Thromboembolism
Venous Thromboembolism
Blood Product UtilizationBlood Product Utilization
Preventable ReadmissionsPreventable Readmissions
Patient MortalityPatient Mortality
Medication ErrorsMedication Errors
Cardiac Care AppropriatenessCardiac Care
Appropriateness
Stroke CareStroke Care
Diabetes CareDiabetes Care
Heart Failure ManagementHeart Failure Management
Telemetry CareTelemetry Care
Ventilator ManagementVentilator Management
Antibiotic AdministrationAntibiotic Administration
Core Process MeasuresCore Process Measures
Sepsis CareSepsis Care
Perinatal CarePerinatal Care
Patient SatisfactionPatient Satisfaction
Employee EngagementEmployee Engagement
Physician SatisfactionPhysician Satisfaction
Clinical Leadership Turnover
Clinical Leadership Turnover
Physician Leadership Engagement
Physician Leadership Engagement
Nursing RetentionNursing Retention
Nursing EducationNursing Education
Turn‐around‐time (TAT)Turn‐around‐time (TAT)
ED ThroughputED Throughput
Supply UtilizationSupply Utilization
Formulary Standardization
Formulary Standardization
Imaging EfficiencyImaging Efficiency
Lab OrderingLab Ordering
Physician Preference Items
Physician Preference Items
Clinical WorkflowClinical Workflow
Resource ConsumptionResource Consumption
Business ContinuityBusiness Continuity
Categories
Performance Areas
Unifying Purpose
Safest, high quality, most efficient provider of health care services.
Clinical Variability & Quality
ServiceOperational EfficiencySafety
11

Supporting reporting of publicly required data
Participating in relevant external registries
Aggregating, analyzing and distributing data
Identifying and sharing best practices
Establishing internal collaboratives
Providing support and expertise for sustainable clinical operational improvement
How We are Working Together to Increase Value
12
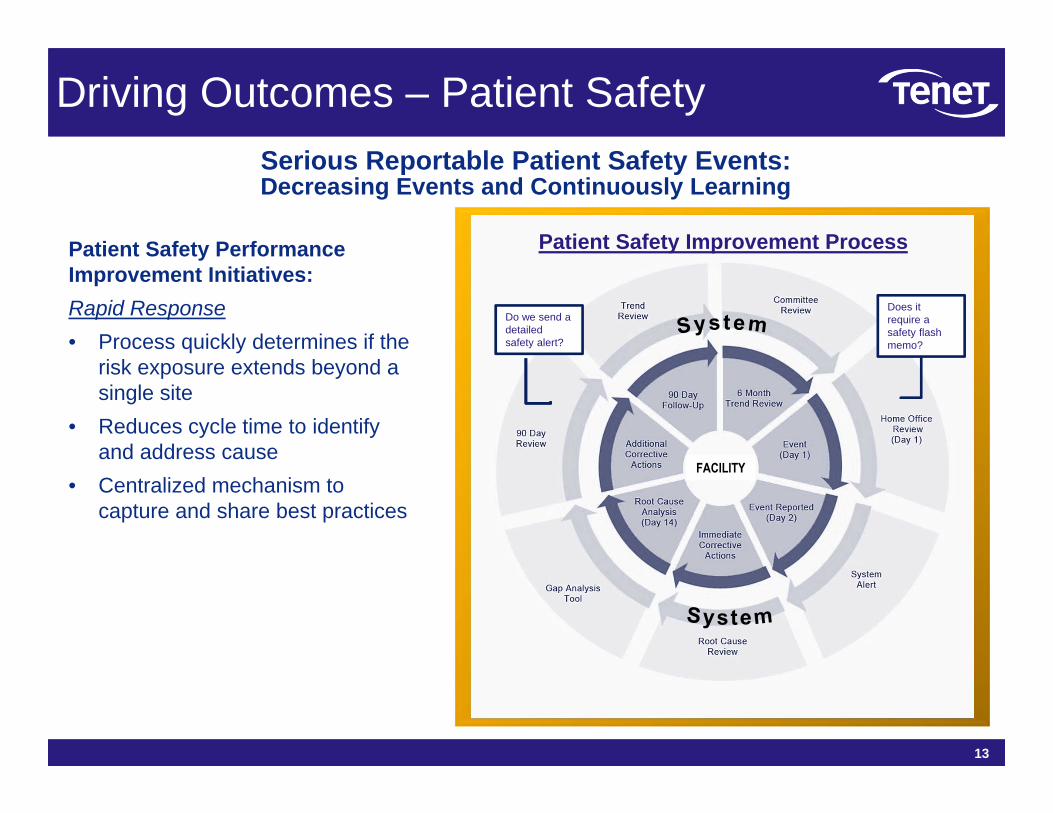
Driving Outcomes – Patient Safety
Patient Safety Improvement ProcessPatient Safety Performance Improvement Initiatives:Rapid Response• Process quickly determines if the
risk exposure extends beyond a single site
• Reduces cycle time to identify and address cause
• Centralized mechanism to capture and share best practices
Does it require a safety flash memo?
Do we send a detailed safety alert?
Serious Reportable Patient Safety Events: Decreasing Events and Continuously Learning
13
Oct
ober
4th
–29
th
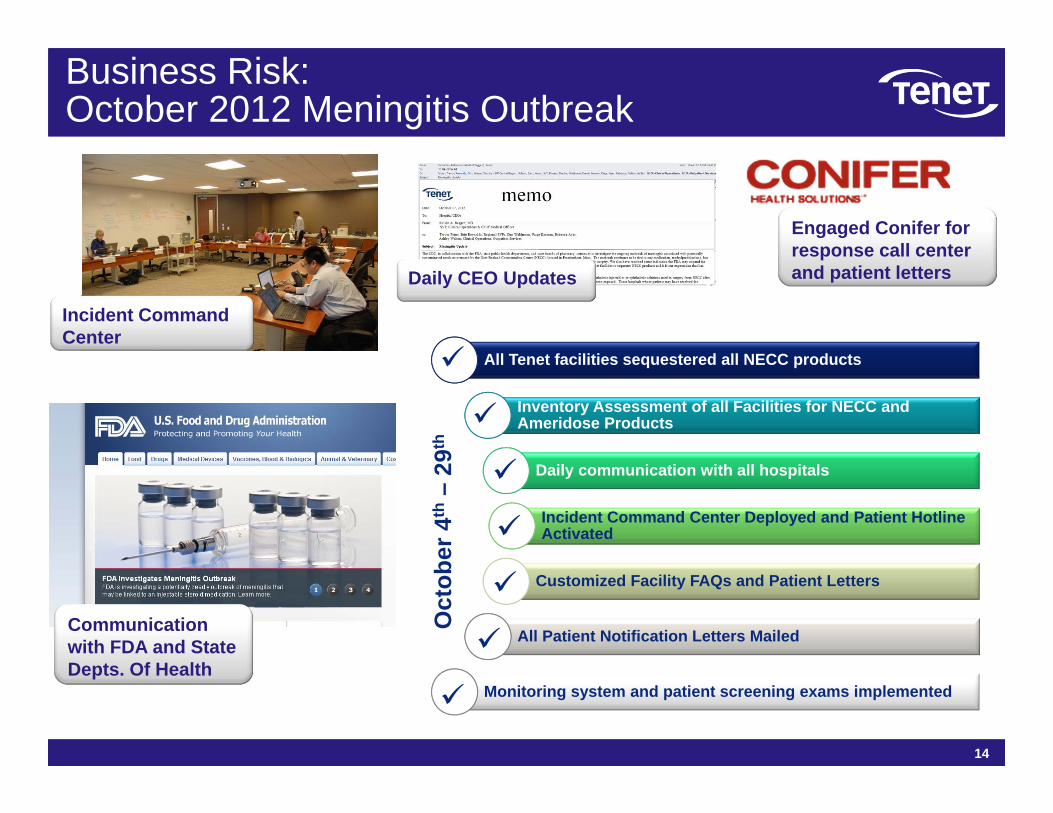
All Tenet facilities sequestered all NECC products
Inventory Assessment of all Facilities for NECC and Ameridose Products
Daily communication with all hospitals
Incident Command Center Deployed and Patient Hotline Activated
Customized Facility FAQs and Patient Letters
All Patient Notification Letters Mailed
Monitoring system and patient screening exams implemented
14
Business Risk:October 2012 Meningitis Outbreak
Daily CEO Updates
Communication with FDA and State Depts. Of Health
Incident Command Center
Engaged Conifer for response call center and patient letters

46%Ventilator Associated
Pneumonias reduced by 46%
Demonstrable Results
Patient Safety Initiatives since 2011 have resulted in significant improvements in key areas:
57%Retained Foreign Objects
reduced by 57%
Falls with Injury
reduced by 41%
41% 64%Vascular Catheter‐Associated Infection
reduced by 64%
36%Pressure Ulcer Stages III & IV reduced by 36%
31%Catheter Associated Urinary Tract
Infection reduced by 31%
The above rates are per 1000 device days and patient days.
The above rates are per 1000 patient discharges.
15
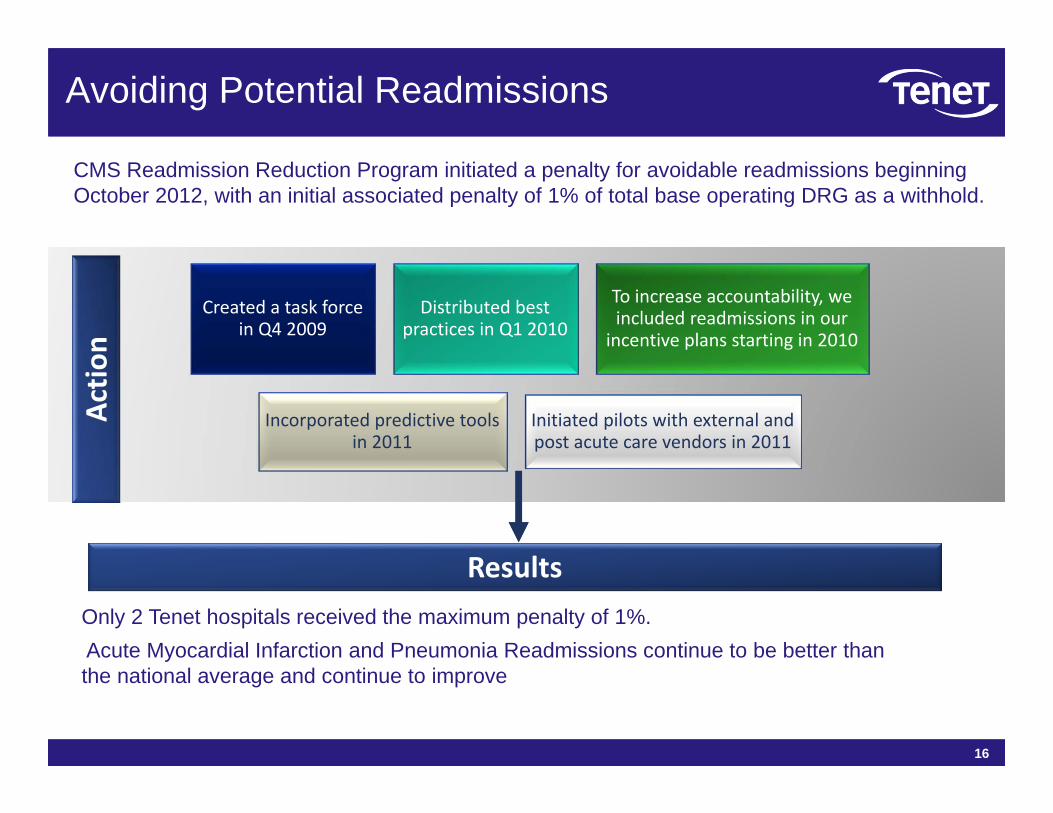
CMS Readmission Reduction Program initiated a penalty for avoidable readmissions beginning October 2012, with an initial associated penalty of 1% of total base operating DRG as a withhold.
Avoiding Potential Readmissions
Created a task force in Q4 2009
Distributed best practices in Q1 2010
To increase accountability, we included readmissions in our incentive plans starting in 2010
Incorporated predictive tools in 2011
Initiated pilots with external and post acute care vendors in 2011
Actio
n
ResultsOnly 2 Tenet hospitals received the maximum penalty of 1%.Acute Myocardial Infarction and Pneumonia Readmissions continue to be better than the national average and continue to improve
16

Tenet HIT Roadmap
The Enabling Role of Technology: HIT
17
Phase 1 ‐ EHRs
• Core clinicals• 26 completed as of 10/2012
Phase 2 ‐ CPOE
• 26 completed as of 10/2012
• Satisfied CMS HIT targeted incentives
Targeted Completion: 2014Targeted Completion: 2014
Advances in health information technology continue to improve care and help us to better inform clinical processes.
Health Information Technology (HIT)
Clinical Apparatus
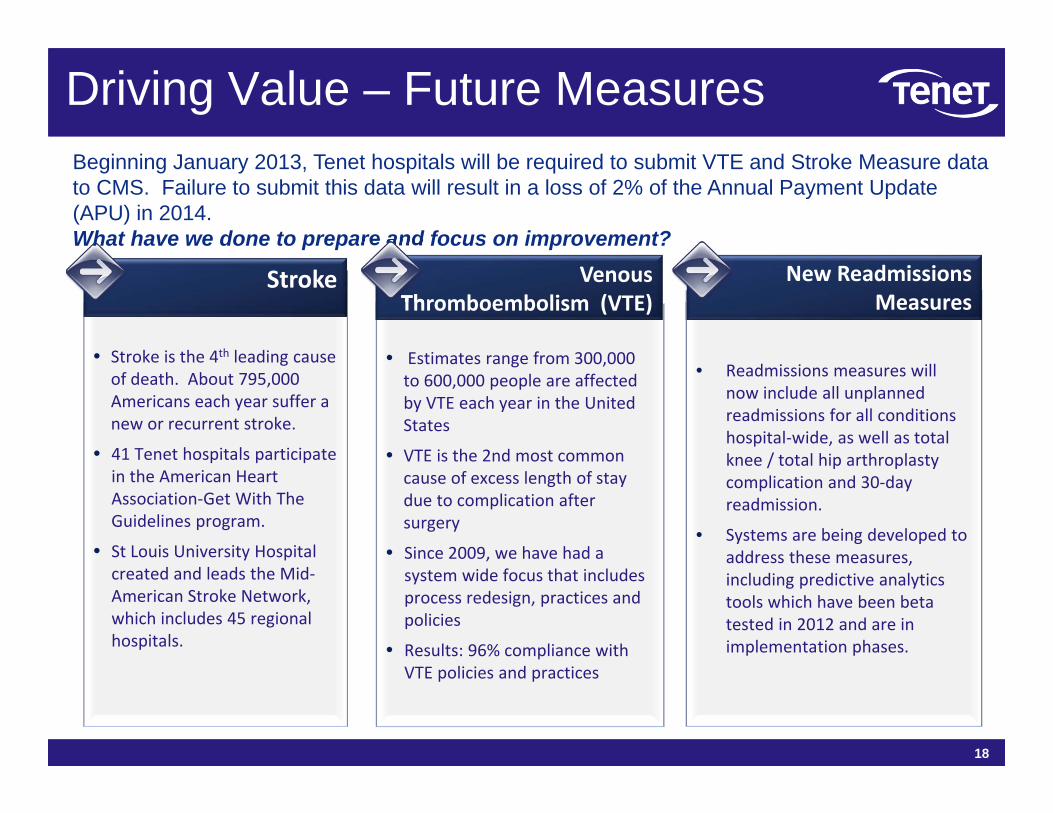
Driving Value – Future Measures
• Stroke is the 4th leading cause of death. About 795,000 Americans each year suffer a new or recurrent stroke.
• 41 Tenet hospitals participate in the American Heart Association‐Get With The Guidelines program.
• St Louis University Hospital created and leads the Mid‐American Stroke Network, which includes 45 regional hospitals.
Stroke
• Readmissions measures will now include all unplanned readmissions for all conditions hospital‐wide, as well as total knee / total hip arthroplasty complication and 30‐day readmission.
• Systems are being developed to address these measures, including predictive analytics tools which have been beta tested in 2012 and are in implementation phases.
New Readmissions Measures
• Estimates range from 300,000 to 600,000 people are affected by VTE each year in the United States
• VTE is the 2nd most common cause of excess length of stay due to complication after surgery
• Since 2009, we have had a system wide focus that includes process redesign, practices and policies
• Results: 96% compliance with VTE policies and practices
Venous Thromboembolism (VTE)
Beginning January 2013, Tenet hospitals will be required to submit VTE and Stroke Measure data to CMS. Failure to submit this data will result in a loss of 2% of the Annual Payment Update (APU) in 2014.What have we done to prepare and focus on improvement?
18

QUESTIONS?
19