introduction section i. organization and … · introduction section i. organization and function...
TRANSCRIPT

FM 8-10-3
CHAPTER 1
INTRODUCTION
Section I. ORGANIZATION AND FUNCTION OF THE DIVISIONMEDICAL OPERATIONS CENTER
1-1. Division
The division is the basic unit of the combined armsand services of the Army. It is the smallest unit inwhich all arms and services are represented insufficient strength to permit large-scale operations.To achieve and maintain readiness, divisioncommanders need the right supplies, equipment,and personnel at the right place, at the right time,and in the right quantity. The DISCOM isresponsible for monitoring this readiness andensuring that the force is manned, armed, fueled,fixed, and moved, and that soldiers and theirsystems are sustained.
1-2. Division Support Command
a. The DISCOM is organized to providethe maximum amount of combat service support(CSS) within prescribed strength limitations whileproviding the most effective and responsive supportto tactical units in a combat environment. In orderto provide responsive support to the tacticalcommander, logistics, medical, and personnelservices support must be effectively organized andpositioned as far forward as necessary to supportthe tactical plan.
b. Division-level CHS is coordinatedand provided by the DISCOM medical elementslisted below:
Division medical operationscenter, DISCOM HHC, locatedin the DSA.
Main support medical company,MSB, located in the DSA.
Forward support medical com-pany, FSB, located in the BSA.
1-3. Missions and Capabilities of the DivisionMedical Operations Center
a. The DMOC’s mission is to plan,coordinate, and synchronize the division’s CHSwith technical medical advice from the divisionsurgeon. The division surgeon and the DMOCchief have joint responsibilities for CHS operationsin the division. Their staff positions in the divisionand DISCOM require a close working relationshipand coordination of their CHS activities. This CHSincludes but is not limited to Echelons I and IImedical treatment which involves—
Emergency medical treatment.
Advanced trauma management.
Emergency and general dentaltreatment.
Preventive dentistry.
Limited radiological services.
Limited laboratory services.
Limited pharmacy services.
Limited patient holding capa-bilities.
Psychiatric consultation andcombat stress control (CSC).
Preventive medicine (PVNTMED).
Limited optometry services.
Medical evacuation support byair and ground ambulances.
1-1

FM 8-10-3
Class VIII resupply and bloodsupport.
Medical maintenance.
b. The DMOC is also responsible forcoordinating general support (GS) and directsupport (DS) relationships of organic medical unitsand medical units/elements under operationalcontrol (OPCON) or attached to the division.Detailed responsibilities are addressed in para-graph 1-4. Appendix A discusses GenevaConventions compliance for CHS operations.
operations. Specific functions of the DMOCinclude—
1-4. Responsibilities of the Division MedicalOperations Center
a. The DMOC staff is responsible to theDISCOM commander for staff supervision of CHSwithin the DISCOM. The division surgeon andDMOC chief will develop operating procedureswhich will enhance the flow of information andfacilitate the synchronization of CHS operationswithin the division. It is imperative that the divisionsurgeon and the DMOC chief work as a team. Bothshare equal responsibility for planning andoverseeing CHS operations. The DMOC is respon-sible for monitoring CHS activities within thedivision area and keeping the DISCOM commanderinformed of the status of CHS. The divisionsurgeon is informed of the DISCOM’s CHS statusthrough reports prescribed by the tactical standingoperating procedures (TSOP) (see Appendix B).
b. Figure 1-1 shows the typicalorganization and staffing of the center. The DMOCconsists of a medical operations branch, a medicalmateriel management branch (MMMB), a patientdisposition and reports branch, and a medicalcommunications branch.
c. The DMOC staff assists the divisionsurgeon in planning and conducting division CHS
Planning and ensuring thatEchelons I and II CHS for thedivision is provided in a timelyand efficient manner.
Developing and maintaining theDISCOM medical troop basis,revising as required, to ensuretask organization for missionaccomplishment.
Planning and coordinating CHSoperations for DISCOM organicmedical assets, attached, orOPCON corps assets. Thisincludes reinforcement andreconstitution.
Coordinating with the DISCOMOperations and Training Officer(US Army) (S3), and divisionsurgeon to prioritize thereallocation of organic and corpsmedical augmentation assets asrequired by the tactical situation.
Overseeing division TSOPs,plans, policies, and proceduresfor CHS, ensuring they areprepared and executed asapplicable.
Overseeing medical training andproviding information to thedivision surgeon and DISCOMcommander.
Coordinating and prioritizingcombat health logistics (CHL)blood management requirementsfor the division.
1-2

FM 8-10-3
1-3

FM 8-10-3
Collecting and disseminatingmedical threat information andcoordinating combat healthintelligence requirements withthe division Assistant Chiefof Staff (Intelligence) (G2)according to FM 8-10-8.
Facilitating functional integra-tion between CHS and militaryintelligence staff elements withinthe division. This is done insupport of the intelligence pre-paration of the battlefield.
Coordinating and directingpatient evacuation fromdivision-level medical treatmentfacilities (MTFs) to corps-levelMTFs. This is accomplishedthrough the medical brigade/group medical regulating officer(MRO).
Coordinating the medical evac-uation of all enemy prisoner ofwar (EPW) casualties.
Coordinating and managing thedisposition of captured medicalmateriel.
Coordinating, planning, and pri-oritizing PVNTMED missions.
Coordinating corps dental sup-port when the tactical situationpermits.
Coordinating with the support-ing veterinary element per-taining to subsistence and animaldisease surveillance.
1-5. Division Medical Operations CenterChief
The chief, DMOC, has overall responsibility fordirecting and coordinating the activities of theDMOC. The chief, DMOC—
Coordinates Army Medical Depart-ment (AMEDD) personnel assign-ments and replacements with thedivision surgeon.
Requests DISCOM AMEDD per-sonnel replacements through theDISCOM Adjutant (US Army) (S1).
NOTE
The division surgeon coordinates withthe Assistant Chief of Staff (Personnel)(Gl) for AMEDD personnel assign-ments and replacements for the division.
Identifies division CHS requirements.
Prioritizes CHS activities for divisionoperations.
Provides input to the DISCOM’sservice support annex.
Provides analysis of medical threatto DISCOM commander, divisionsurgeon, and appropriate DISCOMstaff elements.
Integrates medical intelligence intodivision-level CHS operationsplanning and execution.
Coordinates command relationshipsof corps-level medical augmentation
1-4

FM 8-10-3
according to CHS requirements andthe TSOP.
Advises, assists, and mentors FSMCcommanders and battalion-levelmedical platoon and section leaderson all CHS issues.
1-6. Medical Operations Branch
The medical operations branch is typically staffedwith—
a.
Chief, DMOC.
The DISCOM surgeon (assigned toMSMC and dual-hatted as DISCOMsurgeon).
Medical planner.
Plans and operations officer (evacu-ation).
Plans operations officers.
Chief operations sergeant.
Senior operations sergeant.
Intelligence noncommissioned officer(NCO).
Medical operations sergeant.
Administrative specialist.
Responsibilities. The medicaloperations branch is responsible for—
Developing and coordinatingpatient evacuation support plansamong the DISCOM, division,
and the corps medical group’smedical evacuation battalion.
Coordinating corps-level CHSfor the division with the corpsmedical brigade/group.
Submitting Army airspacecommand and control (A2C2)requirements for aeromedicalevacuation elements to thedivision Assistant Chief of Staff(Operations and Plans) (G3) andaviation brigade.
Ensuring A2C2 information isprovided to supporting corps airambulance assets. The A2C2information is normally pro-vided by G3 Air at division andby the brigade S3 Air in themaneuver brigades.
Coordinating for aviationweather information from USAir Force (USAF) WX(weather) detachment in theaviation brigade.
Ensuring road clearance infor-mation is provided to theDISCOM movement controloffice (MCO) and all groundambulance assets. This infor-mation may include—
Nuclear, biological, andchemical (NBC) threat.
Priorities for use of evacu-ation routes.
Information reported bymedical evacuation assets.
1-5

FM 8-10-3
Monitoring medical troopstrength to determine taskorganization for mission accom-plishment.
Forwarding all medical infor-mation of potential intelligencevalue to the DISCOM Intel-ligence Officer (US Army) (S2)/S3 section.
Obtaining updated medicalthreat and intelligence informa-tion through the DISCOM S2/S3 section for evaluation andapplicability.
Managing the disposition ofcaptured medical materielsaccording to TSOPs.
Coordinating CSC team supportto forward areas with MSMCand division mental healthsection (DMHS).
Monitoring division optometryservices.
b. Chief Division Medical OperationsCenter. The duties and responsibilities of the chief,DMOC, were discussed in paragraph 1-5 above.
Division Support Command Surgeon.The DISCOM surgeon is dual-hatted as the MSMCcommander. For a description of his duties asMSMC commander, see FMs 8-10-1 and 63-21.In his duties as the DISCOM surgeon, he providesstaff advice on medical issues to the DISCOMcommander and the chief, DMOC. He maintainsand manages medical priorities within theDISCOM.
(1) He commands and providestechnical assistance to specific elements of the
1-6
MSMC that provide divisionwide services. Theseinclude the—
Preventive medicine section.
Mental health section.
Optometry section.
(2) Responsibilities of the DISCOMsurgeon also include—
c.
d. Medical
Coordinating with adjacentunits on health policies,procedures, and medicalthreats, as necessary.
Providing the chief, DMOC,with update briefings onhealth-related programs,policies, and threats, asnecessary.
Providing technical inputto the division CHS plan.
Monitoring the divisionPVNTMED program toensure its effectiveness.
Monitoring the divisionmental health program forimplementation of stressprevention measures.
Assisting in implementingthe division surgeon’smedical training programsand training policy.
Developing CHS estimates.
Planner. The medicalplanner develops and maintains the medical troopsbasis. He ensures task organization for mission

FM 8-10-3
accomplishment. He is the chief of the medicaloperations branch. He is the primary architect ofthe division CHS plan, based on the commander’sintent, guidance from the chief, DMOC, and inputfrom the division surgeon. He monitors brigadeand division operations to ensure adequacy of CHSfor the supported force.
e. Plans and Operations Officer forEvacuation. The plans and operations officer formedical evacuation plans and coordinates patientevacuation to corps-level medical facilities by Armyassets. This officer develops and coordinatesmedical evacuation plans with the supporting corps-level medical elements. He coordinates withdivision A2C2 elements to ensure that thesupporting corps aeromedical evacuation unitsreceive up-to-date overlays and A2C2 information.He coordinates for aviation weather informationfrom the USAF WX detachment in the aviationbrigade.
f. Plans and Operations Officer. Theplans and operations officer assists the medicalplanner with developing and coordinating thedivision CHS plan. He monitors and tracks CHSoperations and updates the medical planner andchief, DMOC, as necessary. He coordinates withdivision command and control (C2) elements toensure task organization for mission accom-plishment. Based on the commander’s intent andguidance from the DISCOM surgeon, he plans forthe distribution of PVNTMED and division mentalhealth resources.
a.
g. Chief Operations Sergeant. The chiefoperations sergeant assists the chief, DMOC, inaccomplishing his operational duties. Hecoordinates and supervises the administrationfunctions within the DMOC.
h. Senior Operations Sergeant. Thesenior operations sergeant assists the medicalplanner. He supervises the activities of sub-ordinate enlisted personnel assigned to this branch.
i. Operations Sergeant for Evacuation.The operations sergeant for evacuation assists theplans and operations officer for evacuation inaccomplishing his duties.
j. Intelligence Noncommissioned Officer.The intelligence NCO reviews information ofpotential intelligence value. He coordinatesintelligence information with DISCOM S2/S3section. He works in conjunction with theDISCOM S2 in determining likely enemymovement and expected enemy actions which willaffect CHS requirements and operations. He assistsin coordinating the disposition of captured medicalmateriel with the medical logistics (MEDLOG)battalion (forward). This NCO prepares andmonitors the division medical intelligence program.
k. Medical Operations Sergeant. Themedical operations sergeant assists the senioroperations sergeant and the plans and operationsofficer with the accomplishment of their duties.
1. Administrative Specialist. The admin-istrative specialist provides administrative supportfor the DMOC. He is also designated as a driver.
1-7. Medical Materiel Management Branch
The MMMB is responsible forplanning, coordinating, and prioritizing CHL andmedical equipment maintenance programs for thedivision. The branch is staffed with a health servicemateriel officer (HSMO) and a medical supplysergeant.
b. The specific responsibilities of thisbranch include the following:
Providing the division CHLinput to the CHS plan incoordination with supportingMEDLOG battalion (forward).
1-7

FM 8-10-3
Coordinating medical mainte-nance training with supportingMEDLOG battalion (forward),as required.
Establishing maintenance pri-orities for repair and exchangeof medical equipment (this iscoordinated by the divisionmedical supply office [DMSO])using the Theater Army MedicalManagement Information System(TAMMIS).
Ensuring that a viable preventivemaintenance program is estab-lished and monitored.
Coordinating the evacuationand replacement of medicalequipment with the MEDLOGbattalion (forward).
Verifying emergency supplyrequests for submission to thecorps MEDLOG battalion(forward), and taking thenecessary action to expediteshipment.
Analyzing division medicalsupply operations, identifyingtrends in performance, andproviding technical advice, asnecessary.
Establishing and managing, incoordination with the divisionand DISCOM surgeons, themedical critical items list.
Interfacing with the divisionmateriel management center(DMMC) and MCO to ensurenecessary coordination with the
division supply and transpor-tation system occurs.
Establishing transportation pro-cedures, based on the tacticalsituation, with the MEDLOGbattalion (forward).
Providing technical staff assis-tance for the DMSO, asrequired, to ensure divisionwidesupport for CHL and bloodmanagement.
Establishing coordination pro-cedures for the disposition ofcaptured medical materiel.
c. Health Service Materiel Officer. TheHSMO assigned to the MMMB coordinates andmanages the CHL support for the division. TheHSMO also coordinates and monitors medicalequipment maintenance programs for the division.
d. Medical Supply Sergeant. Themedical supply sergeant assists the HSMO inaccomplishing medical supply duties.
1-8. Patient Disposition and Reports Branch
Staffing and Responsibilities. Thepatient deposition and reports branch is responsiblefor coordinating patient disposition throughout thedivision. It is typically staffed with a patientadministration NCO and a patient administrationspecialist. The branch obtains and coordinatesdisposition of patients with the DMOC medicaloperations branch and corps MRO. It prepares andforwards appropriate medical statistical reports asrequired.
b. Patient Administration NCO. Thepatient administration NCO assists the operationsofficer for evacuation in the coordination of patientdisposition in the division. This NCO prepares the
a.
1-8

FM 8-10-3
required patient statistical reports and coordinatestheir timely submission to higher headquarters. Healso supervises the patient administration specialist.
c. Patient Administration Specialist.The patient administration specialist assists thepatient administration NCO in preparing patientstatistical reports and in performing other patientadministration functions. He also operates theTactical Army CSS Computer System (TACCS).
1-9. Medical Communications Branch
a. Responsibilities of the Medical Com-munications Branch. The medical communicationsbranch is responsible for the operation of the radioand wire communications systems for the DMOC.This branch is typically staffed with a tacticalcommunications chief, a senior radio operator, andsingle-channel radio operators. The medicalcommunications branch establishes external radioand internal wire communications systems andperforms the following:
Coordinates radio communica-tions with the DISCOM com-munications branch and with thedivision signal battalion.
Establishes amplitude modulated(AM), improved high-frequencyradio (IHFR), and frequency
modulated (FM) communica-tions. Establishes and maintainsAM and IHFR communicationswith subordinate DISCOMmedical companies and sup-porting corps medical units.
Coordinates wire and mobilesubscriber equipment (MSE)communications requirementswith the DISCOM commu-nications branch and divisionsignal battalions.
Coordinates through the opera-tions officer with the assistantdivision signal officer (ADSO)for additional information sup-port systems, as required, to meetmission requirements. This mayinclude the use of single- andmultichannel satellite assets.
b. Senior Radio Operator/Maintainer.The senior radio operator/maintainer supervises theenlisted personnel in the operation of the radio andwire communications systems. He is responsiblefor operating the field radio and for supervising thesingle-channel radio operators.
c. Radio Operators/Maintainers. Thereare two radio operators/maintainers that operate thesingle-channel field radio on a 24-hour basis.
Section II. DIVISION MEDICAL OPERATIONS CENTERINTERFACE FOR COMBAT HEALTH SUPPORT OPERATIONS
1-10. Interface with the Division Support (1) The S1‘s responsibilities in-Command Staff clude—
The S1 provides and coordinates Tracking critical medicalpersonnel support for the command. The DISCOM military occupational spe-S1’s responsibilities are listed in FM 63-2. cialties (MOS).
1-9

FM 8-10-3
Reporting casualties.
Conducting replacementoperations.
Making casualty pro-jections for the DISCOM.
Monitoring patient evacu-ation and mortality.
(2) Reports submitted from theDMOC to the S1 should be identified in theDISCOM TSOP. These reports may varydepending on the needs of the command.
(3) The DMOC and the S1 mustwork together and coordinate their staff andoperational activities to ensure mission accom-plishment.
b. The S2/S3 section is primarilyinvolved with plans, operations, intelligence, andsecurity. The elements of the S2/S3 and itsnumerous responsibilities are listed in FM 63-2.
(1) Elements of the DMOC andelements of the S2/S3 work together to synchronizeCHS activities to division operations. Examples ofthe coordination that must take place betweenelements of the DMOC and elements of the S2/S3section are shown in Table 1-1.
(2) The S2/S3 and the chief,DMOC, must be informed of staff activities and beinvolved with the decision-making process.
c. The DISCOM Supply Officer (USArmy) (S4) is responsible for all logistics matterspertaining to DISCOM units. The DISCOM S4’sresponsibilities are listed in FM 63-2.
(1) The DMOC is dependent on theDISCOM S4 for logistics support other thanmedical.
(2) The DMOC must coordinatewith the S4 for—
Assignment of facilitiesand locations within theDISCOM headquarters area.
Critical supply items list(nonmedical).
1-11. Interface with Division Staff
a. Interface with the division staffsections on division CHS is performed for theDISCOM commander by the DMOC inconsultation with the division surgeon. TheDISCOM commander and S2/S3 are keptinformed, as required, when DMOC elementsinterface with division staff elements.
b. The chief, DMOC, monitors andcoordinates CHS to division units according to tech-nical guidance provided by the division surgeon.
c. The chief, DMOC, keeps the divisionsurgeon informed on all division CHS activities.
d. The interface between the DMOCand division staff sections will normally occurthrough the DISCOM headquarters or through thedivision surgeon. Direct interface between theDMOC and division staff sections maybe required.Examples of subject areas where direct interfacemay occur are shown in Table 1-2, page 1-12.
e. The DMOC and division staff share amutual interest in a number of areas. These areasare depicted in Table 1-3, page 1-12.
1-10

FM 8-10-3
1-11

FM 8-10-3
1-12

FM 8-10-3
1-12. Interface with the Major Commands ofthe Division
Combat Brigades. Interface witheach of the combat brigades is accomplished withthe S2 and S3 sections. This interface will focuson CHL and CHS requirements for the brigades.It also includes coordination for A2C2 informationfor air evacuation assets supporting maneuverelements.
b. Aviation Brigade. Interactions betweenthe aviation brigade and the DMOC may include—
a .
Coordination for area medicalsupport.
Coordination for evacuation ofpatients using helicopters withheavy lift capabilities (CH 47).
Coordination for air delivery ofClass VIII emergency resupply.
Coordination for appropriateaviation plans and overlayssupporting division operations.
Coordination for aviationlogistics support (aviation fuelmaintenance and spare parts) tosupport air ambulances, whenrequired.
Coordination for aviationweather information from theUSAF WX detachment in theaviation brigade.
1-13. Interface with the Main Support Battalion
Information pertaining to the structure andoperations of the MSB is provided in FM 63-21.The DMOC will interface with elements of theMSB, as required and approved by the DISCOM
commander. The DMOC may interface withelements of the MSB through the DISCOM supportoperations section. The interactions andcoordination between the DMOC and the MSBare driven by CHS requirements of the divisionand changes with the tactical situation. Theseinteractions are conducted through two differentchannels of communications-the commandchannel and the technical medical channel.Communications which take place through thetechnical channel pertain to CHS operations,coordination activities, patient evacuation, medicalresupply, and medical personnel and equipmentstatus reports. This technical channel ofcommunications is designed to enhance reactiontime of MSB elements to CHS operationsrequirements. The chief, DMOC, and the MSBcommander must develop policies and procedureswhich clearly delineate responsibilities andcoordination requirements’ for an effective workingrelationship. Tasking of the MSMC elements bythe DISCOM will be through command channels.
a. The MSB S2/S3 is the focal point forinternal operations for the battalion. It supervisestechnical and military intelligence gathering as wellas formulates plans specifically geared to thebattalion’s mission. The S2/S3 and DMOCinterface pertains to the following subject areas:
Position of MSMC within theMSB’s area of operations (AO).
Status reports on tacticalsituation and conditions alongmain supply routes (MSRs).
b. Support operations section of theMSB is responsible for the supervision of logisticalactivities that are the primary mission of thebattalion. The DMOC interfaces with the healthservice support officer (HSSO) assigned to thissection concerning—
Combat health support planning.
1-13

FM 8-10-3
Main support battalion medicalelements tasking, to includereinforcement and reconstitutionrequirements throughout thedivision.
Class VIII resupply.
Evacuation of patients usingnonmedical vehicles.
Corps CHS elements/unitsattached to the MSB.
c. The MSMC provides division- andunit-level CHS and medical staff advice andassistance on an area basis to units operating in theDSA. Combat health support operations arecoordinated by the DISCOM DMOC medicaloperations branch through technical channels. TheDISCOM will task elements of the MSMC throughcommand channels to provide division-level CHS.The interface between the MSMC and the DMOCis essential for providing required division CHS.The interaction and information exchange which isconducted through the technical medical channel isshown in Table 1-4.
1-14

FM 8-10-3
1-14. Interface with the Forward SupportBattalions
The DMOC will interface with elements of theFSB as required and approved by the DISCOMcommander. The DMOC may interface withelements of the FSB through the DISCOM supportoperations section. This interface betweenthe DMOC and elements of the FSB is drivenby CHS requirements in the forward areas. Thisinformation will assist the DMOC in planning,coordinating, and managing division medicalelements and resources in support of thebattle. Communications and coordinationbetween elements of the DMOC and the FSBsare essential for successful accomplishment ofthe DMOC’s and FSB’s CHS mission. TheDMOC interface may involve the following FSBelements:
a. S2/S3. The S2 or S3 advises and assiststhe FSB commander in planning, coordinating, andsupervising the communications, operations,training, security, and intelligence functions of thebattalion. Interface is not limited to but will includethe subject areas identified in Table 1-5.
b. Support Operations Section. Thesupport operations section’s mission includes DSsupply, field services, DS maintenance, CHS, andlimited transportation functions. The section mustensure that logistical and CHS to the supportedunits remain at a level consistent with the type oftactical operations being conducted. Interfacebetween the support operations section and theDMOC maybe director indirect. This interface isaccomplished through the HSSO and is not limitedto but will include the subject areas identified inTable 1-5.
1-15

FM 8-10-3
1-16

FM 8-10-3
Forward Support Medical Company.The FSMC provides CHS for the brigade as wellas area medical support for the BSA. Combathealth support operations are coordinated by theDMOC medical operations branch throughtechnical medical channels. The DISCOM taskselements of the FSMC through command charnelsto provide division-level CHS. The FSMC com-mander has a dual role as the brigade surgeon andas the principal manager of CHS assets assigned orattached to the brigade. He provides assistance tothe support operations section in planning CHS.This interface is not limited to, but will include, thesubject areas identified in Table 1-5.
c .
1-15. Interface with Corps Medical Units
Interface with corps medical units is accomplishedthrough the corps medical brigade/group. Interfacemay also occur with those medical units providingsupport to the division. The medical brigade/groupmay provide subordinate units to support thedivision by establishing a command relationship ofOPCON or attached. The medical brigade/groupmay also choose to maintain only a supportrelationship of DS or GS to support the division.The DMOC interfaces with corps medical units
according to the medical brigade/group TSOP. TheDMOC and other DISCOM staff elements must beprepared to integrate corps-level medical units/elements into the medical as well as the logisticalsupport structure. Information concerning theorganization, functions, and responsibilities of thecorps medical brigade/group is found in FM 8-10.
a. The corps medical brigade providesC2, including—
Staff planning.
Supervision of operations.
Administration of the assignedand attached units, to include thecorps medical group.
(1) The following areas are subjectsof mutual concern for division and corps medicalstaff elements:
Medical regulating.
Division CHS requirements.
Ground and air ambulancesupport and maintenance.
1-17

FM 8-10-3
Class VIII resupply andmaintenance.
Blood management.
Status of corps medicalelements attached, orOPCON, to the division.
Medical threat and intelli-gence estimates.
Captured medical suppliesand equipment.
Reinforcement and recon-stitution of CHS elements.
Civil affairs and host-nationsupport.
Communications.
Locations of medical ele-ments in support of thedivision.
Preventive medicine. mentalhealth, dental, or’ veter-inary assistance.
(2) Logistical support requirementsfor corps medical elements operating in the divisionmust be identified and coordinated with the corpssupport battalion (forward). When division supportis not available, this support is normally providedby the corps support battalion (forward). Coor-dination may be required for—
Class I. Subsistence itemsand gratuitous issue healthand welfare items.
Class II. Items of equip-ment other than principalitems which are prescribed
in authorization and allow-ance tables: individualequipment, clothing items,tentage, tool sets, andadministrative and house-keeping supplies.
Class III. Petroleum, oils,and lubricants (POL):petroleum fuels, hydraulicand insulating oils, chem-ical products, antifreezecompounds, compressedgases, coal.
Class IV. Construction andbarrier materials, lumber,sandbags, barbed wire.
Class V. Ammunition.
Class VII. Major end items:final combination of itemswhich are ready (assem-bled) for intended use.
Class IX. Repair parts.
Field services (billeting,showers, and services).
Personnel replacements(corps supported).
b. The MEDLOG battalion (forward)is organic to the corps medical brigade. TheMEDLOG battalion (forward) provides CHLsupport to medical units supported in the corps.This support includes Class VIII resupply, medicalequipment maintenance, blood and blood products,and single-vision optical fabrication. Division med-ical operations center interface with the MEDLOGbattalion (forward) may be required for—
Emergency Class VIII resupply.
1-18

FM 8-10-3
Repair of medical equipment.
Blood management,
Optical fabrication requirements.
Management of captured med-ical materiel.
Storage and decontaminationtechniques to minimize NBCcontamination of Class VIIIsupplies.
The headquarters and headquartersdetachment medical evacuation battalion serves asthe central manager of ground and air evacuationassets in the corps. Its mission is to provide C2 ofground and air medical evacuation units within itsAO. Information pertaining to the organization,functions, and capabilities of this unit is discussedin FM 8-10-6. The DMOC interfaces with themedical evacuation battalion or subordinate unitsconcerning—
c .
Air and ground movementliaison within the division AO.
Reinforcement of division CHSassets.
Mass casualty evacuation plans.
Evacuation of patients fromdivision to supporting corpshospitals.
Emergency movement of med-ical personnel, supplies, andblood.
Ambulance shuttle operations toinclude ambulance exchangepoints (AXPs) and patientcollecting points.
Status of medical evacuationbattalion elements operating inthe division.
Management and decontam-ination of ground/air evacuationassets.
Support requirements forforward deployed medical evac-uation battalion assets.
Location of medical evacuationbattalion assets.
Location of division medicalelements.
Tactical situation and threatupdates.
Delivery of blood and bloodproducts.
Reinforcement of covering forceand deep operations evacuationassets.
Road and movement clearances.
Maintenance support, to includeaviation intermediate mainte-nance (AVIM).
Emergency resupply of medicaland nonmedical items (ifrequired).
Communications requirementsand signal operation instructions(S0I).
Updated tactical maps andevacuation overlays.
1-19

FM 8-10-3
Terrain considerations andbarrier plans for ambulances.
Evacuation destination (MROfunctions).
Division and brigade A2C2requirements.
Combat search and rescue mis-sion.
(1) Within the division area, the airambulance company provides aeromedical evacu-ation on a DS basis. This company may be attachedfor support (less OPCON) to the division aviationbrigade. Air ambulances may operate from theDSA and BSAs providing 24-hour immediateresponse medical evacuation capability. Successfulaeromedical evacuation support to the divisionrequires current and accurate operational infor-mation. This information includes A2C2, currentintelligence, friendly situation, air traffic serviceprocedures, weather, CSS, and aviation safety andstandardization data. To enhance the safety andeffectiveness of aeromedical operations, operationsinformation should flow between air ambulanceunits and the GS aviation battalion or assault heli-copter battalion of the respective aviation brigade.Information is exchanged by various methodsincluding on-site coordination or communicationssystems. The air ambulance company can obtaininformation through various sources such as theDMOC and maneuver brigade tactical operationscenters (TOCs). However, during the planningand execution phases of operations, the medicalevacuation battalion and the aviation unit to whichthe air ambulance company is attached are theprimary sources for providing this information.The DMOC also provides A2C2 planning informa-tion to the air ambulance company. This infor-mation includes, but is not limited to, the following:
Location of medical units.
Locations of forward arearearm/refueling points(FARPs).
Liaison requirements withsupported units.
Recommended evacuationcorridors.
The air ambulance company, in turn, continuallyprovides the medical evacuation battalion, aviationbrigade, and DMOC with updated informationabout its current and planned operations. The com-pany also provides pertinent combat informationobtained during missions. This informationincludes enemy disposition, downed aircraft,weather, and other factors obtained by airambulance crews during the performance of theirduty. All medical evacuation crews communicatedirectly with the division air traffic service andexecute A2C2 while operating behind brigadeboundaries.
(2) Air ambulances, collocated withthe MSB, coordinate air ambulance evacuationmissions in the DSA through the MSB HSSO. TheHSSO is located in the support operations cell ofthe MSB. The HSSO provides real-time tacticalinformation to the air ambulance crew aboutevacuation missions from the requesting unit.When air ambulances operate in the DSA, theyexecute the A2C2 plan through and communicatedirectly with the division air traffic service.Emergency requests for aeromedical evacuationmay be relayed from the DMOC to the HSSO whocoordinates with air ambulances elements for themission. When air ambulances are positioned atother locations in the DSA, the HSSO submitsaeromedical evacuation requests through theDMOC to the supporting air ambulance element.
(3) Air ambulances deployed for-ward into the BSA may collocate with the FSB oraviation task force. When deployed forward to theBSA, the air ambulance team’s evacuation missions
1-20

FM 8-10-3
are coordinated through the HSSO. The HSSO islocated in the support operations cell of the FSB.The HSSO provides real-time tactical informationto the air ambulance crew about evacuationmissions from the maneuver battalion/company tothe brigade rear area. When air ambulancesoperate forward of the BSA, they will execute theA2C2 plan through the maneuver brigade S3. TheFSB support operations branch provides planningand coordination between aeromedical evacuationand the supported maneuver brigade. The brigadeS3 provides the A2C2 plan which includes the aircorridors, air control points, and communicationscheckpoints. The brigade S3 will provide updatesas required.
(4) The medical evacuation battalioncommunications link to the air ambulance companyis accomplished by a combination of wire, FMvoice, and MSE. To enable air-to-air communi-cations between medical evacuation aircraft andaviation brigade aircraft during the conduct ofmissions, air ambulance companies obtain aviationunit call signs, frequencies, and cryptonet variables.
(5) Corps aeromedical elementsmay operate from the DSAs and BSAs providingaround-the-clock immediate response evacuationaircraft. To accomplish this, elements must main-tain a close tie with the A2C2 system in thedivision. The division A2C2 element provides anairspace plan through the division operation order(OPORD)/operation plan (OPLAN) A2C2 annex.The aircrew must also be familiar with the dailyairspace control order (ACO) and the airspacecontrol plan (ACP). These documents contain allairspace control measures (ACM) to include freefire areas, no fly/fire areas, restricted operationszones (ROZ), established and standard Armyaircraft flight routes (SAAFRs). These routes andACMs change on a daily basis and cannot beintegrated into the division OPORD. The DMOCwill ensure all A2C2 information is provided tocorps aeromedical elements. The DMOC does notgenerate A2C2 information, but does provide A2C2
planning information to division A2C2 elements.This information includes, but is not limited to, thefollowing:
Locations of medical airelements and number ofaircraft at each location.
Locations of medical avi-ation and medical units.
Locations of FARPs.
Locations of supportedunits and liaison require-ments.
Locations of evacuationcorridors and recommen-dations on usage.
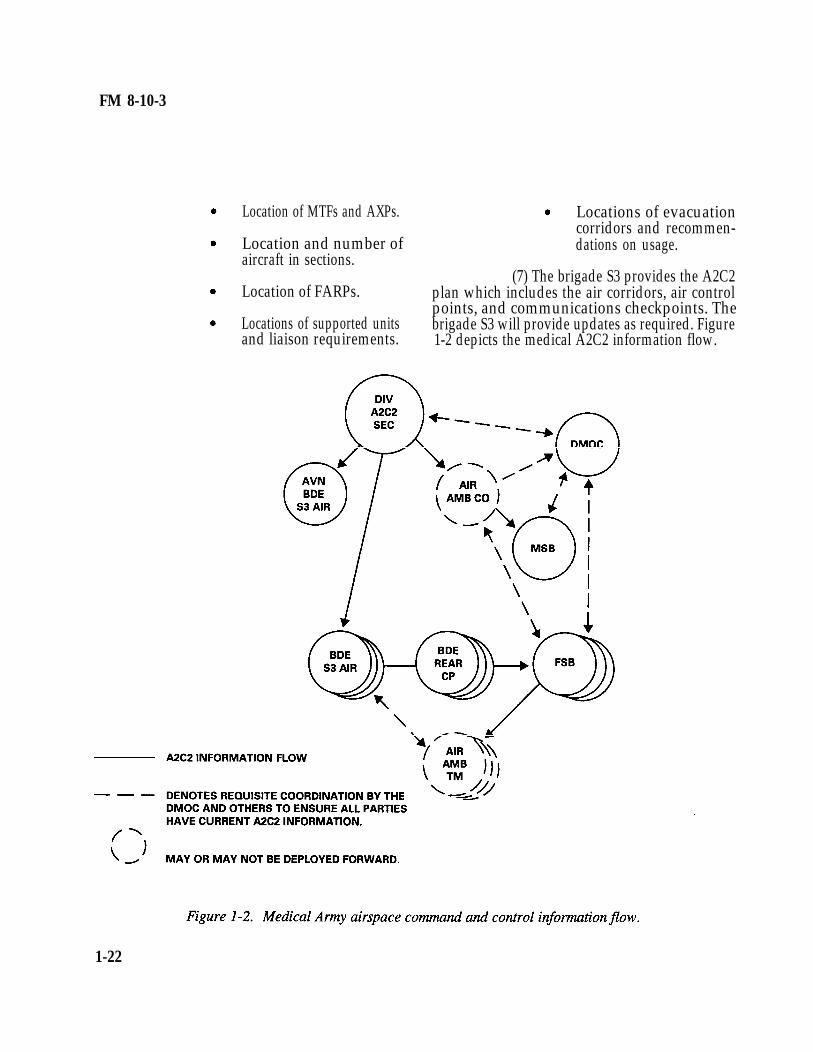
(6) All medical air-flight crews willcommunicate directly with the division air trafficservice and execute division A2C2 while operatingbehind brigade boundaries. The medical evacu-ation battalion may deploy air ambulance elementsto the division. These elements may include an airambulance company or a selected element of thecompany. When the air ambulance company isdeployed to the division, it collocates with theaviation brigade or according to the division TSOP.Air ambulance companies will obtain A2C2information from the division A2C2 section andcoordinate with the DMOC (see Figure 1-2, page1-23). Air ambulance teams may be deployedforward into the BSA and collocate with the FSB.When deployed forward, the air ambulance team isdependent on the FSB for communications support.When air ambulance elements operate forward ofthe brigade rear boundary, they will execute theA2C2 plan through the brigade S3. The FSBsupport operations branch provides planning andcoordination between air evacuation elements andthe maneuver brigade S3. Information provided tothe maneuver brigade S3 should include, but not belimited to, the following:
1-21
FM 8-10-3
Location of MTFs and AXPs. Locations of evacuationcorridors and recommen-
Location and number of dations on usage.aircraft in sections.
(7) The brigade S3 provides the A2C2Location of FARPs. plan which includes the air corridors, air control
points, and communications checkpoints. TheLocations of supported units brigade S3 will provide updates as required. Figureand liaison requirements. 1-2 depicts the medical A2C2 information flow.
1-22