intraoperative ultrasound - scna
DESCRIPTION
Intraoperative Ultrasound - SCNATRANSCRIPT
Surg Clin N Am 84 (2004) 1085–1111
Intraoperative ultrasound
Junji Machi, MD, PhD*, Andrew J. Oishi, MD,Nancy L. Furumoto, MD, Robert H. Oishi, MD
Department of Surgery, University of Hawaii, John A. Burns School of Medicine and Kuakini
Medical Center, 405 N. Kuakini St., Suite 601, Honolulu, HI 96817, USA
Although surgeons are currently using ultrasound in a variety of surgicalsettings such as the office, the bedside, the emergency room, and theintensive care unit, one of the earliest surgeon-performed ultrasoundexaminations in the United States was in the operating room. Dr. BernardSigel, a general surgeon and a pioneer of intraoperative ultrasound (IOUS),introduced this modality during surgery in 1979 for intraoperative diagnosisof biliary calculi [1]. In the early 1980s, IOUS was employed duringneurosurgery, endocrine surgery, and cardiovascular surgery [2–7]. Since1980, the Sigel group has expanded the application of IOUS to various fieldsincluding hepatobiliary, pancreatic, and other abdominal surgery [8–13].
Although the benefits of IOUS were clearly reported, gaining acceptanceof IOUS among surgeons was slow in the 1980s. However, by the mid-1990s,many surgeons recognized the value of IOUS during surgical procedures,and with the availability of various types of IOUS and laparoscopicultrasound probes, the use of ultrasound has become more widespreadduring a variety of operations. In certain operations such as hepatectomy,IOUS is presently considered as an essential modality.
In this article, we present an overview of IOUS by reviewing our experience[8–19] and the literature. Instrumentation, techniques, indications, clinicalapplications, advantages, and disadvantages are described. The applicationof IOUS in open abdominal surgery is emphasized, although applications inother surgical fields are briefly summarized. The future perspective of IOUS isalso discussed. Although laparoscopic ultrasound during laparoscopicprocedures is one form of IOUS, we discuss the use of IOUS during openprocedures in this article.
Supported by Surgical Education, Inc.
* Corresponding author.
E-mail address: [email protected] (J. Machi).
0039-6109/04/$ - see front matter � 2004 Elsevier Inc. All rights reserved.
doi:10.1016/j.suc.2004.04.001

1086 J. Machi et al / Surg Clin N Am 84 (2004) 1085–1111
Instrumentation
B-mode ultrasound with high-frequency transducers, the so-called smallparts scanner, is used for IOUS [14,20–25]. Color or power Doppler imagingis sometimes valuable to distinguish blood vessels from other structures orto identify small vessels; however, the majority of IOUS examinations canbe performed with B-mode ultrasound. Although ultrasound at higherfrequencies penetrates less deeply, it provides images of greater resolution;this is a favorable trade-off for IOUS, which usually requires soundpenetration of less than 10 cm without the need for penetrating theabdominal wall. Transducer frequencies range from 5 to 10 MHz, with 7to 8 MHz most frequently used for IOUS. With such high frequencies, evensmall lesions, such as 1-mm calculi, 2-mm cysts, 1- to 2-mm vascular defects,and 3- to 5-mm tumors, can be detected.
Transducer types for IOUS include linear array, curvilinear array(convex), and phased array (sector). The size and shape of the ultrasoundprobe are important features for IOUS scanning. The probe should be smallenough to be manipulated in a small or narrow operative field. There aretwo principal shapes of probes: a flat T- or I-shaped probe (mostly sideviewing) and a cylindrical pencil-like probe (mostly end viewing). The flatprobe usually has a wider footprint (3 to 6 cm) and provides a wide near-field image. This probe is suitable for scanning relatively large, flat organs,such as the liver, pancreas, and gastrointestinal tract. The cylindrical probeis useful for scanning small target organs or structures, such as theextrahepatic bile duct that are located deep in the operative field.
IOUS probes can be cold-gas sterilized or used with a sterile cover. Gassterilization requires aeration, and thus the probe can be used only once a day.Although the use of a cover is cumbersome, one probe can be repeatedlyused. Recently, a low-temperature chemical sterilization (eg, Steris, Sterrad),which is completed in 60 minutes, has become available, and some IOUSprobes are amenable to this method.
Techniques
IOUS can be performed at any time during the operation and, ifnecessary, can be repeated as often as necessary [14–25]. Most commonly,IOUS is performed early in the course of operation to acquire newintraoperative information. IOUS is also frequently used during operativeprocedures for guidance or assistance. After a procedure is finished butbefore closure, IOUS can be repeated as a completion examination.
The two basic scanning techniques for IOUS are contact scanning andprobe-standoff scanning. In contact scanning, the probe is placed directly onthe tissue or organ surface in a manner similar to transcutaneous ultrasound.In probe-standoff scanning, the probe is positioned 1 to 2 cm away from thesurface of the structure. The probe-standoff technique uses saline immersion
1087J. Machi et al / Surg Clin N Am 84 (2004) 1085–1111
of the probe, which is unique to IOUS. Because ultrasound resolution nearestto the probe is poor, the distance from the probe to the area of interestdetermines the choice of scanning technique. For example, contact scanningis chosen for the examination of the interior of organs such as the liver andthe pancreas, or for examination of target lesions located deep in the tissue(away from the probe). Probe-standoff scanning is essential for examinationof the surface area of organs or for examination of superficial structures, suchas the superficially located bile duct.
Another useful IOUS scanning technique is compression scanning, inwhich the tissue is intentionally compressed by the probe. This method helpsto displace air in tissue spaces and air in the gastrointestinal tract lumen.Compression can be also used to distinguish arteries from veins.
For complete evaluation, the organ should be systematically andthoroughly scanned—not only the area of interest, but the entire organ.Although the scanning method varies in different organs, it is generallyimportant to obtain longitudinal and transverse views and, at times, obliqueviews of the target organ. In addition, IOUS scanning should be performedfrom various positions and directions using various probe manipulationtechniques, including sliding, rotating, and angulating (tilting, rocking) ofthe probe. By imaging the organ or the lesion with multiple views in two-dimensional real time, three-dimensional information can be obtained.During examination of malignant tumors, close attention should be paid tosurrounding structures as well. In particular, the major blood vessels shouldbe followed and their relationship to the tumor evaluated.
IOUS can be completed within a relatively short period. For example,screening of liver metastasis during laparotomy can be performed in5 minutes. Precise IOUS evaluation of the extent of a malignant tumormay require 10 to 15 minutes.
Indications
There are four main general indications for IOUS: (1) acquisition of newinformation not otherwise available, (2) as a complement to or replacementfor intraoperative radiography, (3) confirmation of completion of operation,and (4) guidance of surgical procedures [8–21].
IOUS is indicated to acquire new information that is not available duringpreoperative studies or standard intraoperative exploration. This includesnew diagnosis of diseases, localization or exclusion of previously suspectedlesions, and identification of pertinent anatomic information. IOUS is usedfor assessment of the extent of malignant tumors or cancer staging. Forexample, liver metastasis, lymph node involvement, and vascular invasion ofcancers can be generally diagnosed more accurately than by routine pre-operative studies. The liver can be screened for occult metastasis. Preciselocalization of lesions such as intrahepatic lesions, pancreatic tumors, or othernonpalpable intraabdominal disease is possible with IOUS. Preoperatively
1088 J. Machi et al / Surg Clin N Am 84 (2004) 1085–1111
or intraoperatively suspected lesions may be quickly excluded by IOUS.Anatomic structures including blood vessels can be delineated before surgicaltissue dissection. By providing various new information, IOUS helps to selectthe best approach to lesions or the most appropriate operation.
As a complement to or replacement for conventional intraoperativeradiography, IOUS is indicated during hepatobiliary, pancreatic, orvascular surgery. During open cholecystectomy, IOUS has demonstratedequal or superior accuracy in the screening of the bile duct for calculicompared with intraoperative cholangiography. Because contrast injectionis not needed, IOUS is much simpler, quicker, and safer than intraoperativecontrast radiography such as cholangiography or pancreatography. Thus,IOUS can be a first-choice imaging method during biliary surgery. Likewise,during vascular surgery, IOUS has exhibited equal or superior accuracy indetecting vascular defects such as intimal flaps or thrombi compared withintraoperative arteriography.
IOUS is employed to confirm the completion of certain operations, mainlyto assess excision of lesions or to discover surgical technical problems.Confirmation of complete resection of tumors in organs such as the liver,pancreas, brain, or breast can be done with IOUS. In certain instances,scanning of an excised tissue specimen in a water bath in the operating room isalso a useful test to ensure the lesion as being completely excised. IOUS can beused to confirm complete removal of biliary or pancreatic calculi andextraction of foreign bodies. Technical errors after cardiac surgery or vascularreconstructive surgery can be detected by IOUS and thereby correctedimmediately. After organ transplantation, IOUS may be used to examinevascular anastomotic sites and to evaluate adequate blood flow to the organ.
In addition to providing diagnostic information, IOUS is indicated to helpguide therapeutic procedures. Two types of intraoperative procedures areguided by IOUS: (1) intraoperative needle, cannula, or probe placement; and(2) surgical tissue dissection. IOUS-guided needle placement is similar tointerventional radiology performed percutaneously, and aids intraoperativebiopsy of tissues, aspiration of fluids, injection of agents, or introduction ofcatheters. Cannula or probe placement for thermal ablation or cryoablationof tumors can be appropriately guided by IOUS. Tissue dissection is guidedby IOUS for incision or resection of organs, especially solid organs such asthe liver, pancreas, brain, or breast. For example, anatomic resection of theliver is precisely guided by IOUS. Various surgical procedures guided byIOUS are safer, quicker, and more accurate than those performed underinspection and palpation alone. The capability to guide procedures is a uniquefeature of IOUS for which intraoperative radiology cannot be substituted.
Multiple indications for IOUS may be present during a single operation.For example, during hepatic surgery, IOUS is initially indicated to obtainnew information, such as a final cancer staging, then to guide biopsy andhepatectomy, and finally to confirm complete resection of lesions and toexclude intraoperative complications.
1089J. Machi et al / Surg Clin N Am 84 (2004) 1085–1111
Clinical applications
Liver
IOUS is indispensable during hepatic surgery for detection and localiza-tion of various hepatic lesions and for guidance of surgical procedures [15–19,26–45]. During laparotomy for other intraabdominal malignancy, IOUSis also performed for screening for liver metastasis [46–56].
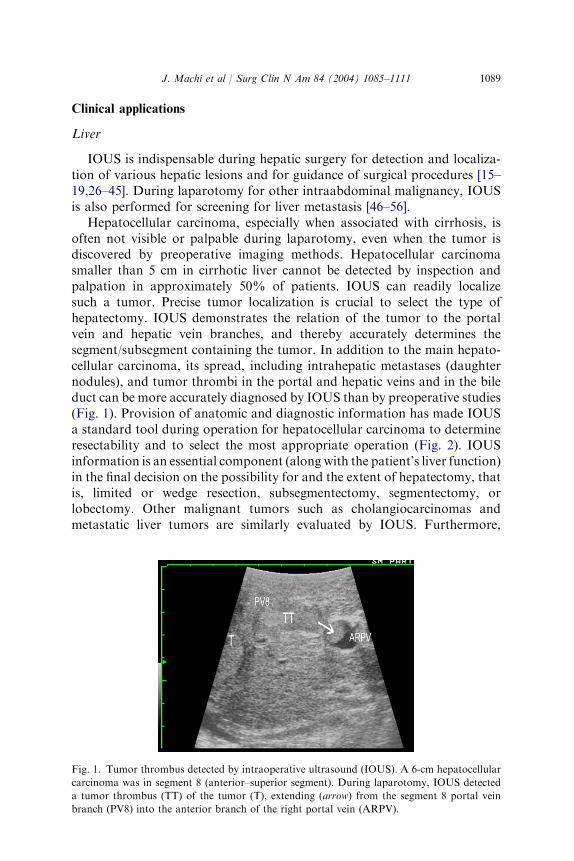
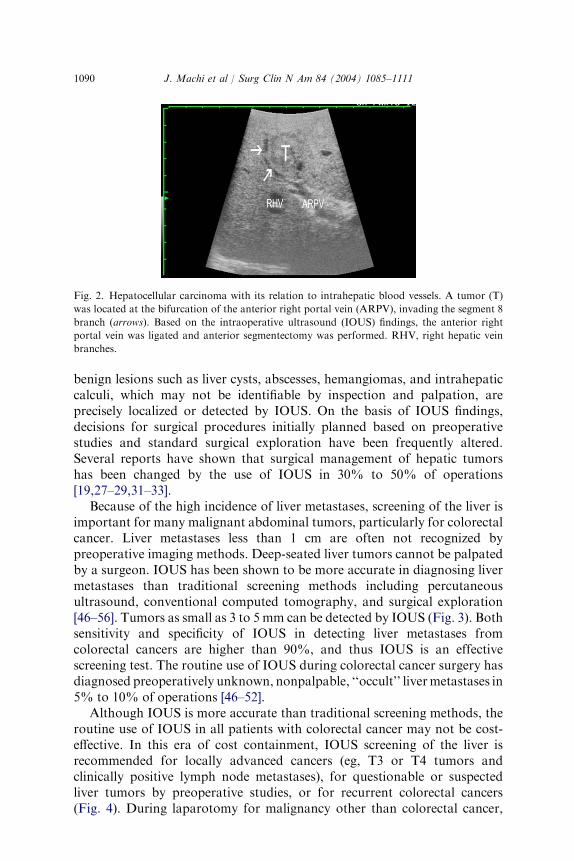
Hepatocellular carcinoma, especially when associated with cirrhosis, isoften not visible or palpable during laparotomy, even when the tumor isdiscovered by preoperative imaging methods. Hepatocellular carcinomasmaller than 5 cm in cirrhotic liver cannot be detected by inspection andpalpation in approximately 50% of patients. IOUS can readily localizesuch a tumor. Precise tumor localization is crucial to select the type ofhepatectomy. IOUS demonstrates the relation of the tumor to the portalvein and hepatic vein branches, and thereby accurately determines thesegment/subsegment containing the tumor. In addition to the main hepato-cellular carcinoma, its spread, including intrahepatic metastases (daughternodules), and tumor thrombi in the portal and hepatic veins and in the bileduct can be more accurately diagnosed by IOUS than by preoperative studies(Fig. 1). Provision of anatomic and diagnostic information has made IOUSa standard tool during operation for hepatocellular carcinoma to determineresectability and to select the most appropriate operation (Fig. 2). IOUSinformation is an essential component (along with the patient’s liver function)in the final decision on the possibility for and the extent of hepatectomy, thatis, limited or wedge resection, subsegmentectomy, segmentectomy, orlobectomy. Other malignant tumors such as cholangiocarcinomas andmetastatic liver tumors are similarly evaluated by IOUS. Furthermore,
Fig. 1. Tumor thrombus detected by intraoperative ultrasound (IOUS). A 6-cm hepatocellular
carcinoma was in segment 8 (anterior–superior segment). During laparotomy, IOUS detected
a tumor thrombus (TT) of the tumor (T), extending (arrow) from the segment 8 portal vein
branch (PV8) into the anterior branch of the right portal vein (ARPV).
1090 J. Machi et al / Surg Clin N Am 84 (2004) 1085–1111
benign lesions such as liver cysts, abscesses, hemangiomas, and intrahepaticcalculi, which may not be identifiable by inspection and palpation, areprecisely localized or detected by IOUS. On the basis of IOUS findings,decisions for surgical procedures initially planned based on preoperativestudies and standard surgical exploration have been frequently altered.Several reports have shown that surgical management of hepatic tumorshas been changed by the use of IOUS in 30% to 50% of operations[19,27–29,31–33].
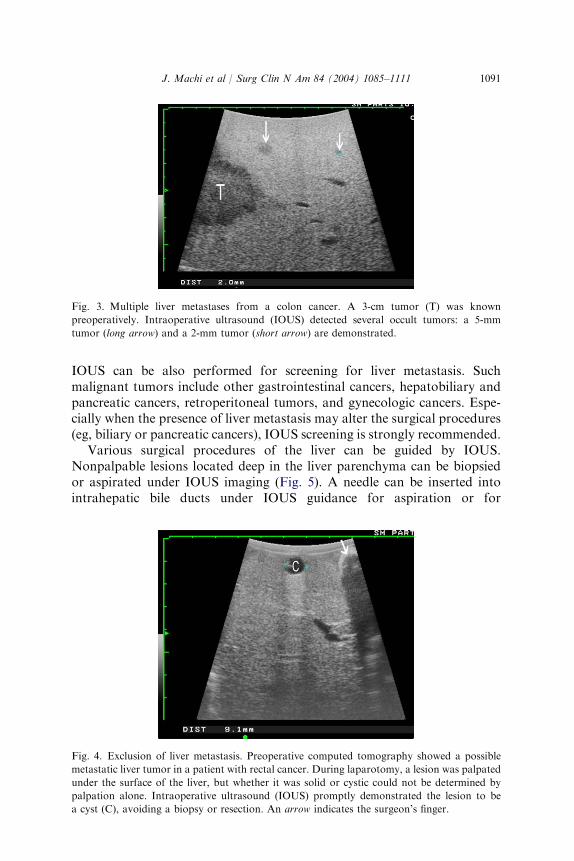
Because of the high incidence of liver metastases, screening of the liver isimportant for many malignant abdominal tumors, particularly for colorectalcancer. Liver metastases less than 1 cm are often not recognized bypreoperative imaging methods. Deep-seated liver tumors cannot be palpatedby a surgeon. IOUS has been shown to be more accurate in diagnosing livermetastases than traditional screening methods including percutaneousultrasound, conventional computed tomography, and surgical exploration[46–56]. Tumors as small as 3 to 5 mm can be detected by IOUS (Fig. 3). Bothsensitivity and specificity of IOUS in detecting liver metastases fromcolorectal cancers are higher than 90%, and thus IOUS is an effectivescreening test. The routine use of IOUS during colorectal cancer surgery hasdiagnosed preoperatively unknown, nonpalpable, ‘‘occult’’ livermetastases in5% to 10% of operations [46–52].
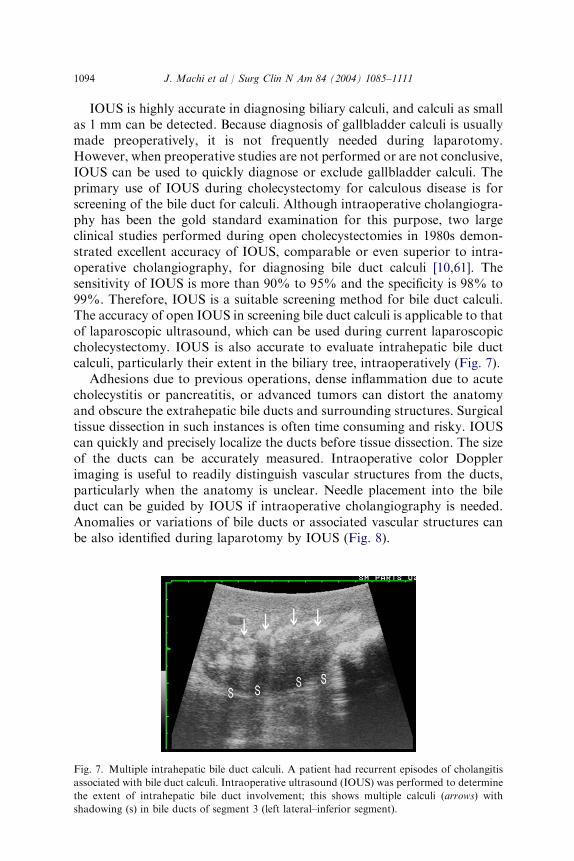
Although IOUS is more accurate than traditional screening methods, theroutine use of IOUS in all patients with colorectal cancer may not be cost-effective. In this era of cost containment, IOUS screening of the liver isrecommended for locally advanced cancers (eg, T3 or T4 tumors andclinically positive lymph node metastases), for questionable or suspectedliver tumors by preoperative studies, or for recurrent colorectal cancers(Fig. 4). During laparotomy for malignancy other than colorectal cancer,
Fig. 2. Hepatocellular carcinoma with its relation to intrahepatic blood vessels. A tumor (T)
was located at the bifurcation of the anterior right portal vein (ARPV), invading the segment 8
branch (arrows). Based on the intraoperative ultrasound (IOUS) findings, the anterior right
portal vein was ligated and anterior segmentectomy was performed. RHV, right hepatic vein
branches.
1091J. Machi et al / Surg Clin N Am 84 (2004) 1085–1111
IOUS can be also performed for screening for liver metastasis. Suchmalignant tumors include other gastrointestinal cancers, hepatobiliary andpancreatic cancers, retroperitoneal tumors, and gynecologic cancers. Espe-cially when the presence of liver metastasis may alter the surgical procedures(eg, biliary or pancreatic cancers), IOUS screening is strongly recommended.
Various surgical procedures of the liver can be guided by IOUS.Nonpalpable lesions located deep in the liver parenchyma can be biopsiedor aspirated under IOUS imaging (Fig. 5). A needle can be inserted intointrahepatic bile ducts under IOUS guidance for aspiration or for
Fig. 3. Multiple liver metastases from a colon cancer. A 3-cm tumor (T) was known
preoperatively. Intraoperative ultrasound (IOUS) detected several occult tumors: a 5-mm
tumor (long arrow) and a 2-mm tumor (short arrow) are demonstrated.
Fig. 4. Exclusion of liver metastasis. Preoperative computed tomography showed a possible
metastatic liver tumor in a patient with rectal cancer. During laparotomy, a lesion was palpated
under the surface of the liver, but whether it was solid or cystic could not be determined by
palpation alone. Intraoperative ultrasound (IOUS) promptly demonstrated the lesion to be
a cyst (C), avoiding a biopsy or resection. An arrow indicates the surgeon’s finger.

1092 J. Machi et al / Surg Clin N Am 84 (2004) 1085–1111
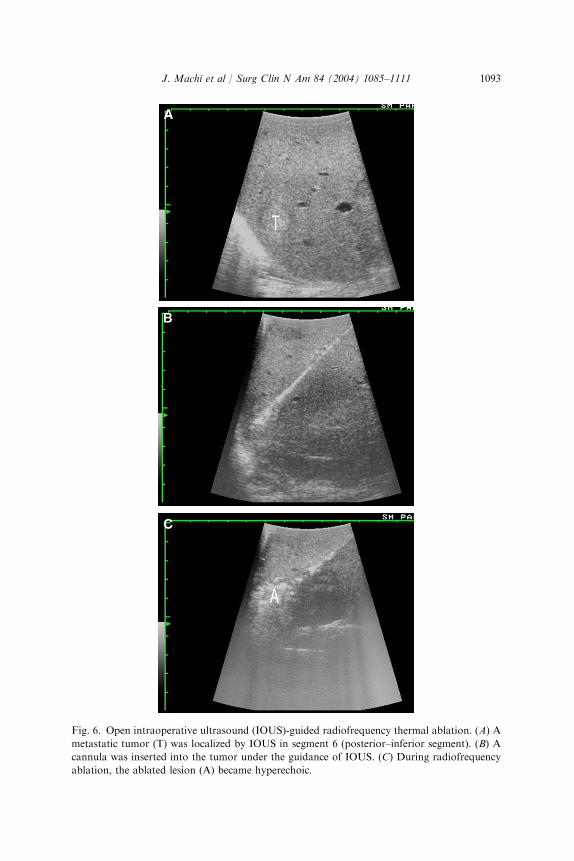
catheterization. Nonresectional local treatment of liver tumors has beenrecently introduced with the aid of open IOUS as well as transabdominal orlaparoscopic ultrasound. IOUS precisely guides a cannula or probe into thetumor and monitors the process during thermal ablation or cryoablation.Particularly, the use of ultrasound-guided radiofrequency thermal ablationis becoming increasingly popular as its safety and local control efficacy havebeen demonstrated for both primary and metastatic liver tumors (Fig. 6)[57,58]. IOUS-guided techniques greatly facilitate the performance ofhepatic resection, in particular, anatomic hepatectomy. Because interioranatomy of the liver, including intrahepatic vessels, is clearly delineated,hepatic resection can be performed more safely and in a more anatomicallyoriented fashion. In addition to the initial planning, the resectional processcan be monitored by the repeated use of IOUS because the resection line isdisplayed in relation to the lesion and blood vessels. With the introductionof IOUS guidance techniques, unique hepatic resections such as IOUS-guided systematic subsegmentectomy for hepatocellular carcinoma havebeen developed [26,30,35,42]. Given the overwhelming advantages, IOUS isconsidered as an essential adjunct, and hepatic surgery should not beconducted without IOUS.
Biliary system
The majority of simple cholecystectomies for calculous cholecystitis arecurrently performed laparoscopically. On the other hand, open biliarysurgery is needed in more difficult situations or for more complex diseases.IOUS of the biliary tract is performed during laparotomy for diagnosis ofgallbladder calculi, screening for bile duct calculi, localization of obscuredor anomalous bile ducts, evaluation of biliary tumors, and guidance ofbiliary procedures [10,11,16–18,59–64].
Fig. 5. Intraoperative ultrasound (IOUS)-guided open liver biopsy. A tumor (T) was located
deep in segment 7 (posterior–superior segment). IOUS precisely guided a biopsy needle into the
tumor (arrows).
1093J. Machi et al / Surg Clin N Am 84 (2004) 1085–1111
Fig. 6. Open intraoperative ultrasound (IOUS)-guided radiofrequency thermal ablation. (A) A
metastatic tumor (T) was localized by IOUS in segment 6 (posterior–inferior segment). (B) A
cannula was inserted into the tumor under the guidance of IOUS. (C) During radiofrequency
ablation, the ablated lesion (A) became hyperechoic.
1094 J. Machi et al / Surg Clin N Am 84 (2004) 1085–1111
IOUS is highly accurate in diagnosing biliary calculi, and calculi as smallas 1 mm can be detected. Because diagnosis of gallbladder calculi is usuallymade preoperatively, it is not frequently needed during laparotomy.However, when preoperative studies are not performed or are not conclusive,IOUS can be used to quickly diagnose or exclude gallbladder calculi. Theprimary use of IOUS during cholecystectomy for calculous disease is forscreening of the bile duct for calculi. Although intraoperative cholangiogra-phy has been the gold standard examination for this purpose, two largeclinical studies performed during open cholecystectomies in 1980s demon-strated excellent accuracy of IOUS, comparable or even superior to intra-operative cholangiography, for diagnosing bile duct calculi [10,61]. Thesensitivity of IOUS is more than 90% to 95% and the specificity is 98% to99%. Therefore, IOUS is a suitable screening method for bile duct calculi.The accuracy of open IOUS in screening bile duct calculi is applicable to thatof laparoscopic ultrasound, which can be used during current laparoscopiccholecystectomy. IOUS is also accurate to evaluate intrahepatic bile ductcalculi, particularly their extent in the biliary tree, intraoperatively (Fig. 7).
Adhesions due to previous operations, dense inflammation due to acutecholecystitis or pancreatitis, or advanced tumors can distort the anatomyand obscure the extrahepatic bile ducts and surrounding structures. Surgicaltissue dissection in such instances is often time consuming and risky. IOUScan quickly and precisely localize the ducts before tissue dissection. The sizeof the ducts can be accurately measured. Intraoperative color Dopplerimaging is useful to readily distinguish vascular structures from the ducts,particularly when the anatomy is unclear. Needle placement into the bileduct can be guided by IOUS if intraoperative cholangiography is needed.Anomalies or variations of bile ducts or associated vascular structures canbe also identified during laparotomy by IOUS (Fig. 8).
Fig. 7. Multiple intrahepatic bile duct calculi. A patient had recurrent episodes of cholangitis
associated with bile duct calculi. Intraoperative ultrasound (IOUS) was performed to determine
the extent of intrahepatic bile duct involvement; this shows multiple calculi (arrows) with
shadowing (s) in bile ducts of segment 3 (left lateral–inferior segment).
1095J. Machi et al / Surg Clin N Am 84 (2004) 1085–1111
For evaluation of malignant biliary tumors, including gallbladder cancerand bile duct cancer, IOUS provides accurate assessment of direct invasionof tumor into the liver parenchyma or to blood vessels such as the portalvein and hepatic artery (Fig. 9). Metastasis to the liver and lymph nodes canbe examined. These IOUS findings help to determine the extent and theresectability of these biliary cancers. IOUS provides useful guidance forbiopsy of biliary tumors, aspiration or catheterization of intrahepatic bileducts, and assistance in obtaining free margin when tumor resection isperformed, especially in combination with hepatic resection. IOUS cansometimes identify gallbladder polyps as small as 1 to 2 mm that areunknown preoperatively.
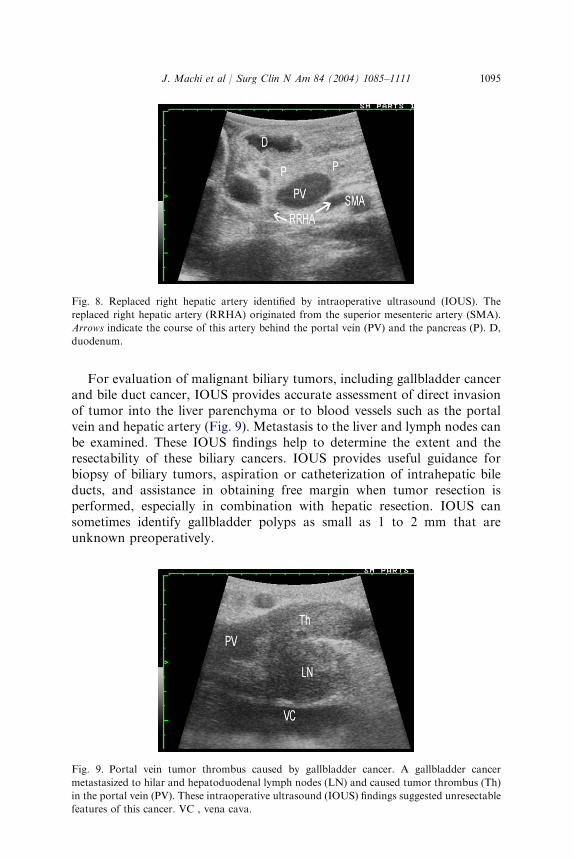
Fig. 8. Replaced right hepatic artery identified by intraoperative ultrasound (IOUS). The
replaced right hepatic artery (RRHA) originated from the superior mesenteric artery (SMA).
Arrows indicate the course of this artery behind the portal vein (PV) and the pancreas (P). D,
duodenum.
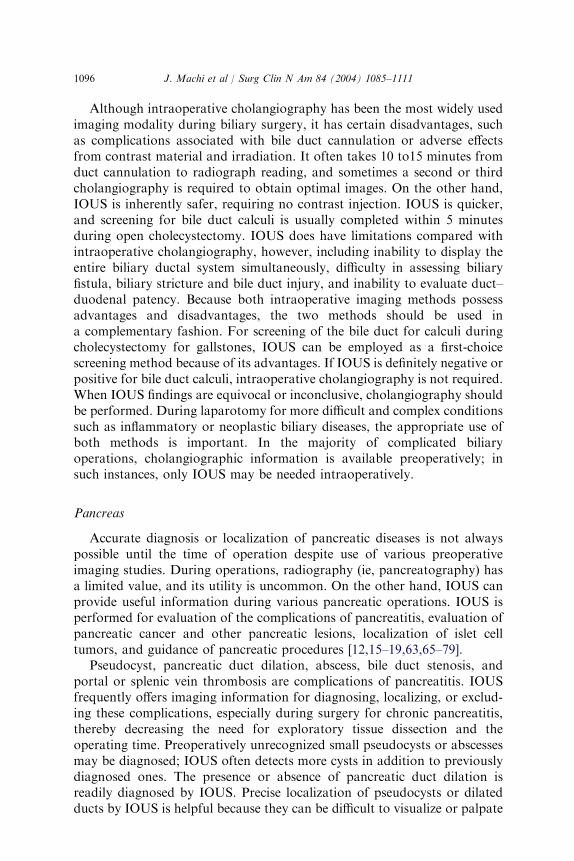
Fig. 9. Portal vein tumor thrombus caused by gallbladder cancer. A gallbladder cancer
metastasized to hilar and hepatoduodenal lymph nodes (LN) and caused tumor thrombus (Th)
in the portal vein (PV). These intraoperative ultrasound (IOUS) findings suggested unresectable
features of this cancer. VC , vena cava.
1096 J. Machi et al / Surg Clin N Am 84 (2004) 1085–1111
Although intraoperative cholangiography has been the most widely usedimaging modality during biliary surgery, it has certain disadvantages, suchas complications associated with bile duct cannulation or adverse effectsfrom contrast material and irradiation. It often takes 10 to15 minutes fromduct cannulation to radiograph reading, and sometimes a second or thirdcholangiography is required to obtain optimal images. On the other hand,IOUS is inherently safer, requiring no contrast injection. IOUS is quicker,and screening for bile duct calculi is usually completed within 5 minutesduring open cholecystectomy. IOUS does have limitations compared withintraoperative cholangiography, however, including inability to display theentire biliary ductal system simultaneously, difficulty in assessing biliaryfistula, biliary stricture and bile duct injury, and inability to evaluate duct–duodenal patency. Because both intraoperative imaging methods possessadvantages and disadvantages, the two methods should be used ina complementary fashion. For screening of the bile duct for calculi duringcholecystectomy for gallstones, IOUS can be employed as a first-choicescreening method because of its advantages. If IOUS is definitely negative orpositive for bile duct calculi, intraoperative cholangiography is not required.When IOUS findings are equivocal or inconclusive, cholangiography shouldbe performed. During laparotomy for more difficult and complex conditionssuch as inflammatory or neoplastic biliary diseases, the appropriate use ofboth methods is important. In the majority of complicated biliaryoperations, cholangiographic information is available preoperatively; insuch instances, only IOUS may be needed intraoperatively.
Pancreas
Accurate diagnosis or localization of pancreatic diseases is not alwayspossible until the time of operation despite use of various preoperativeimaging studies. During operations, radiography (ie, pancreatography) hasa limited value, and its utility is uncommon. On the other hand, IOUS canprovide useful information during various pancreatic operations. IOUS isperformed for evaluation of the complications of pancreatitis, evaluation ofpancreatic cancer and other pancreatic lesions, localization of islet celltumors, and guidance of pancreatic procedures [12,15–19,63,65–79].
Pseudocyst, pancreatic duct dilation, abscess, bile duct stenosis, andportal or splenic vein thrombosis are complications of pancreatitis. IOUSfrequently offers imaging information for diagnosing, localizing, or exclud-ing these complications, especially during surgery for chronic pancreatitis,thereby decreasing the need for exploratory tissue dissection and theoperating time. Preoperatively unrecognized small pseudocysts or abscessesmay be diagnosed; IOUS often detects more cysts in addition to previouslydiagnosed ones. The presence or absence of pancreatic duct dilation isreadily diagnosed by IOUS. Precise localization of pseudocysts or dilatedducts by IOUS is helpful because they can be difficult to visualize or palpate
1097J. Machi et al / Surg Clin N Am 84 (2004) 1085–1111
due to dense inflammation. Our study has shown that, based on the IOUSfindings, surgical procedures for chronic pancreatitis (drainage versusresection) or drainage sites have been altered in 15% to 20% of operations[18,63].
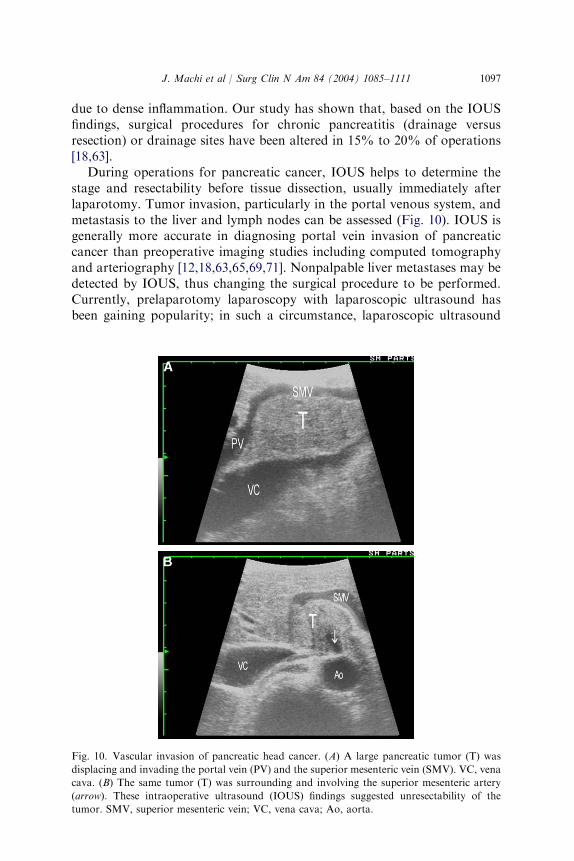
During operations for pancreatic cancer, IOUS helps to determine thestage and resectability before tissue dissection, usually immediately afterlaparotomy. Tumor invasion, particularly in the portal venous system, andmetastasis to the liver and lymph nodes can be assessed (Fig. 10). IOUS isgenerally more accurate in diagnosing portal vein invasion of pancreaticcancer than preoperative imaging studies including computed tomographyand arteriography [12,18,63,65,69,71]. Nonpalpable liver metastases may bedetected by IOUS, thus changing the surgical procedure to be performed.Currently, prelaparotomy laparoscopy with laparoscopic ultrasound hasbeen gaining popularity; in such a circumstance, laparoscopic ultrasound
Fig. 10. Vascular invasion of pancreatic head cancer. (A) A large pancreatic tumor (T) was
displacing and invading the portal vein (PV) and the superior mesenteric vein (SMV). VC, vena
cava. (B) The same tumor (T) was surrounding and involving the superior mesenteric artery
(arrow). These intraoperative ultrasound (IOUS) findings suggested unresectability of the
tumor. SMV, superior mesenteric vein; VC, vena cava; Ao, aorta.

1098 J. Machi et al / Surg Clin N Am 84 (2004) 1085–1111
can provide information similar to open IOUS to determine the resectabilityof pancreatic cancer. At times, a small cancer causing obstructive jaundicethat is not visualized preoperatively can be delineated by IOUS in thepancreatic head or periampullary region. Other pancreatic tumors orlesions, such as cystic neoplasms of the pancreas, are also evaluated byIOUS during operation (Fig. 11).
IOUS has been proven to be one of the most accurate modalities indiagnosing, excluding, and localizing islet cell tumors such as insulinomaand gastrinoma [12,73–79]. A characteristic hypoechoic feature of islet celltumors makes IOUS possible to delineate tumors as small as 3 mm to 4 mmin size. When a nodule is palpated during operation, IOUS can confirm orexclude it as an islet cell tumor. When a tumor is not palpated, IOUS isespecially useful for localization. IOUS is more effective for insulinoma thanfor gastrinoma because insulinoma is usually located within the pancreaticparenchyma while gastrinoma is often extrapancreatic. The detectability ofinsulinoma by IOUS has been reported to be 83% to 100% [73,74,77]. TheIOUS detectability of intrapancreatic gastrinoma was 95%, whereas that ofextrapancreatic gastrinoma was 58%.
Various pancreatic procedures can be guided by IOUS in a mannersimilar to hepatic procedures. Needle placement is guided by IOUS forbiopsy of tumors or aspiration of cystic lesions. During internal drainage ofdilated pancreatic ducts by pancreaticojejunostomy for chronic pancreatitis,the ducts are opened quickly and safely under IOUS guidance [67]. Openingof small pseudocysts can also be assisted. For small nonpalpable islet celltumors or other benign lesions, enucleation after localization is facilitated byIOUS guidance.
Fig. 11. Mucinous cystadenoma of the pancreas. Intraoperative ultrasound (IOUS) demon-
strated a complex multicystic lesion (C) in the body of the pancreas with its relation to the
splenic artery (SA) and splenic vein (SV). IOUS also showed its relation to the main pancreatic
duct, facilitating enucleation of this lesion (cystadenoma).
1099J. Machi et al / Surg Clin N Am 84 (2004) 1085–1111
Other abdomen and retroperitoneum
Other diseases for which IOUS is used during laparotomy include, butare not limited to, gastrointestinal tumors, other abdominal or retroperito-neal tumors, abdominal abscesses, and splenic diseases.
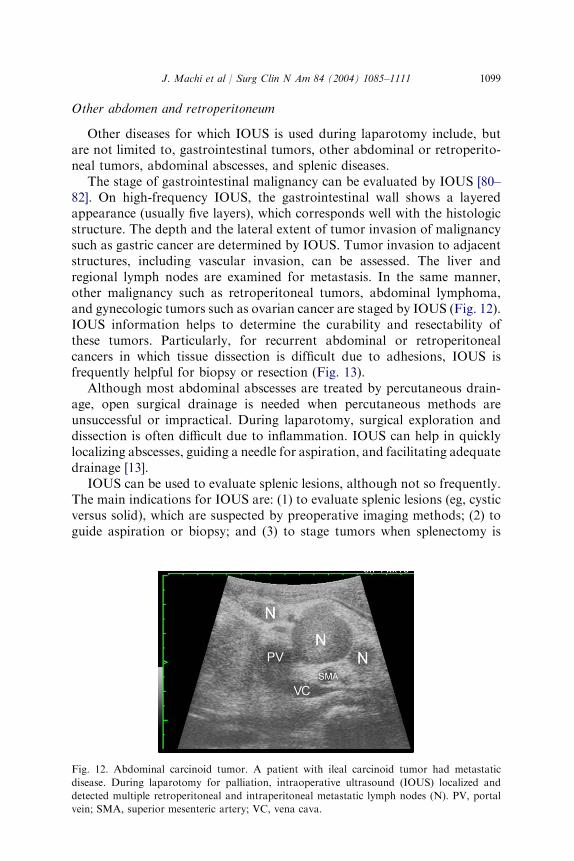
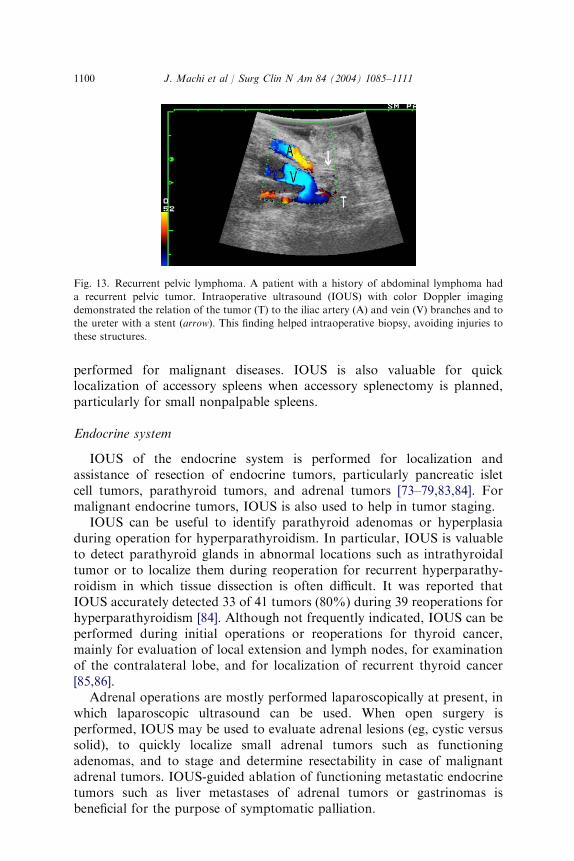
The stage of gastrointestinal malignancy can be evaluated by IOUS [80–82]. On high-frequency IOUS, the gastrointestinal wall shows a layeredappearance (usually five layers), which corresponds well with the histologicstructure. The depth and the lateral extent of tumor invasion of malignancysuch as gastric cancer are determined by IOUS. Tumor invasion to adjacentstructures, including vascular invasion, can be assessed. The liver andregional lymph nodes are examined for metastasis. In the same manner,other malignancy such as retroperitoneal tumors, abdominal lymphoma,and gynecologic tumors such as ovarian cancer are staged by IOUS (Fig. 12).IOUS information helps to determine the curability and resectability ofthese tumors. Particularly, for recurrent abdominal or retroperitonealcancers in which tissue dissection is difficult due to adhesions, IOUS isfrequently helpful for biopsy or resection (Fig. 13).
Although most abdominal abscesses are treated by percutaneous drain-age, open surgical drainage is needed when percutaneous methods areunsuccessful or impractical. During laparotomy, surgical exploration anddissection is often difficult due to inflammation. IOUS can help in quicklylocalizing abscesses, guiding a needle for aspiration, and facilitating adequatedrainage [13].
IOUS can be used to evaluate splenic lesions, although not so frequently.The main indications for IOUS are: (1) to evaluate splenic lesions (eg, cysticversus solid), which are suspected by preoperative imaging methods; (2) toguide aspiration or biopsy; and (3) to stage tumors when splenectomy is
Fig. 12. Abdominal carcinoid tumor. A patient with ileal carcinoid tumor had metastatic
disease. During laparotomy for palliation, intraoperative ultrasound (IOUS) localized and
detected multiple retroperitoneal and intraperitoneal metastatic lymph nodes (N). PV, portal
vein; SMA, superior mesenteric artery; VC, vena cava.
1100 J. Machi et al / Surg Clin N Am 84 (2004) 1085–1111
performed for malignant diseases. IOUS is also valuable for quicklocalization of accessory spleens when accessory splenectomy is planned,particularly for small nonpalpable spleens.
Endocrine system
IOUS of the endocrine system is performed for localization andassistance of resection of endocrine tumors, particularly pancreatic isletcell tumors, parathyroid tumors, and adrenal tumors [73–79,83,84]. Formalignant endocrine tumors, IOUS is also used to help in tumor staging.
IOUS can be useful to identify parathyroid adenomas or hyperplasiaduring operation for hyperparathyroidism. In particular, IOUS is valuableto detect parathyroid glands in abnormal locations such as intrathyroidaltumor or to localize them during reoperation for recurrent hyperparathy-roidism in which tissue dissection is often difficult. It was reported thatIOUS accurately detected 33 of 41 tumors (80%) during 39 reoperations forhyperparathyroidism [84]. Although not frequently indicated, IOUS can beperformed during initial operations or reoperations for thyroid cancer,mainly for evaluation of local extension and lymph nodes, for examinationof the contralateral lobe, and for localization of recurrent thyroid cancer[85,86].
Adrenal operations are mostly performed laparoscopically at present, inwhich laparoscopic ultrasound can be used. When open surgery isperformed, IOUS may be used to evaluate adrenal lesions (eg, cystic versussolid), to quickly localize small adrenal tumors such as functioningadenomas, and to stage and determine resectability in case of malignantadrenal tumors. IOUS-guided ablation of functioning metastatic endocrinetumors such as liver metastases of adrenal tumors or gastrinomas isbeneficial for the purpose of symptomatic palliation.
Fig. 13. Recurrent pelvic lymphoma. A patient with a history of abdominal lymphoma had
a recurrent pelvic tumor. Intraoperative ultrasound (IOUS) with color Doppler imaging
demonstrated the relation of the tumor (T) to the iliac artery (A) and vein (V) branches and to
the ureter with a stent (arrow). This finding helped intraoperative biopsy, avoiding injuries to
these structures.
1101J. Machi et al / Surg Clin N Am 84 (2004) 1085–1111
Cardiovascular system
IOUS of the cardiovascular system is performed for prereconstructionevaluation of peripheral vascular abnormalities, postreconstruction de-tection of vascular defects, and assessment of the completion of open-heartoperations [7,16,18,87–96].
When the results of preoperative vascular studies are not sufficient or areinconclusive, IOUS can be used to delineate and evaluate vascular abnor-malities before the opening of blood vessels. However, IOUS is used mainlyto examine the vascular reconstruction sites as a completion examination.After vascular reconstruction, intraoperative arteriography has been widelyemployed to detect or exclude vascular defects (or technical errors) such asintimal flaps, thrombi, and strictures, which may cause postoperativecomplications (ie, thrombosis or graft occlusion). Studies have demonstratedthat IOUS is equal to or superior to intraoperative arteriography inidentifying such defects, with a sensitivity of 93% and a specificity of 98%[7,89]. In addition, IOUS can be used repeatedly during the operation. Thesize or magnitude of detected vascular defects is more precisely estimatedwith IOUS. Therefore, IOUS can be a first-choice screening method toexamine vascular reconstruction sites. Particularly during carotid endarter-ectomy, IOUS is the only safe imaging method because of the risk associatedwith intraoperative carotid arteriography [87,91,92]. Intraoperative arteri-ography should be performed selectively, for example, to evaluate criticaldistal anastomotic sites or to delineate the distal arterial bed. In vascularsurgery requiring laparotomy, such as renal and mesenteric bypass oper-ations or porto-systemic shunts, IOUS is particularly useful because intra-operative arteriography is difficult in abdominal vessels.
During open-heart operations for valvular or congenital heart diseases,the completion of cardiac procedures can be assessed with IOUS [93–96].Intraoperative transesophageal echography using color Doppler imaginghas become a valuable tool during cardiac surgery because of the provisionof dynamic blood flow information as well as anatomic abnormalities. Thistechnique has greatly facilitated cardiac surgery by making it possible toassess the postreconstruction effectiveness of repair immediately, and hasreduced the occurrence of early postoperative problems requiring secondoperations. During coronary artery bypass graft operations, IOUS can beused directly (epicardially) in the operative field, mainly for examination ofanastomotic sites after reconstruction.
Neurologic system
IOUS of the brain and spinal cord was one of the major applications ofIOUS that became popular in 1980s [97–99]. IOUS is performed mainly forlocalization and assessment of brain and spinal cord lesions and forguidance of neurosurgic procedures, particularly for needle and catheterplacement and for resection of lesions [97–101]. Lesions for which IOUS has

1102 J. Machi et al / Surg Clin N Am 84 (2004) 1085–1111
been used during neurosurgery include brain and spinal cord tumors; cysticlesions, such as brain cysts, hematomas, abscesses, and syringomyelias;vascular abnormalities, such as arteriovenous malformations and aneur-ysms; hydrocephalus, disc hernias, and foreign bodies. In particular, IOUSlocalization and needle guidance for invisible subcortical lesions is useful,and is simpler and quicker than a stereotactic computed tomographymethod.
Urologic system
Although IOUS is not as frequently performed during open urologicprocedures, it can be used to assist surgical removal of renal stones whenopen surgery is needed for nephrolithotomy [102,103]; IOUS helps inlocalizing intrarenal stones, in guiding stone removal, and in confirmingcompleteness of stone removal. IOUS also can be performed during renaltumor operations for localization of nonpalpable small tumors, for detectingor excluding satellite lesions, or for detecting venous (renal vein and venacava) tumor thrombi [104]. When partial nephrectomy is indicated topreserve renal function, IOUS evaluation of a renal tumor is of particularvalue [105].
Lung and mediastinum
IOUS may be performed during operations for malignant tumors of thelung and mediastinum, particularly lung cancer, to evaluate cardiovascularinvasion and lymph node and liver metastasis [106]. IOUS can be performedimmediately after thoracotomy, and provides imaging information that isuseful in selecting the type of surgical procedure (eg, lobectomy versuspneumonectomy) and in avoiding unnecessary extensive tissue dissection.
Breast
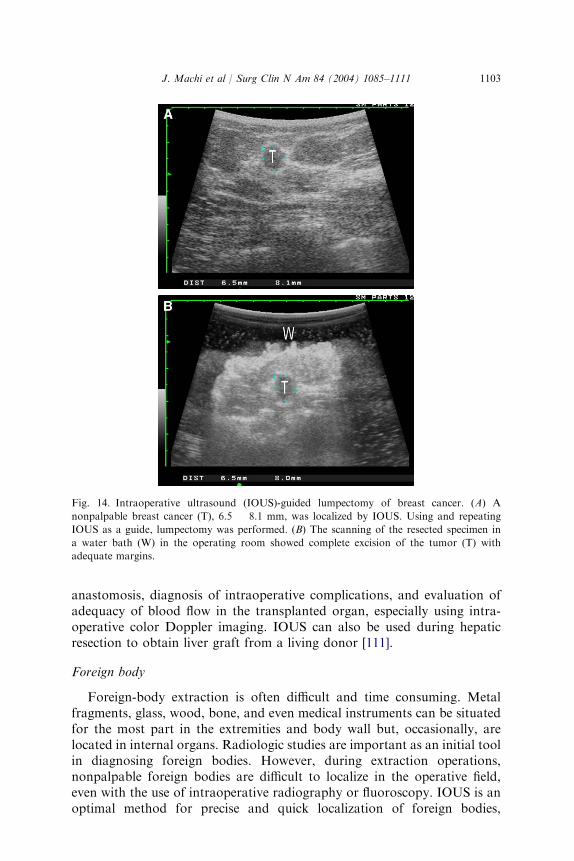
As breast surgeons are becoming more familiar, experienced, and facilewith the use of ultrasound examinations in the office, intraoperative use ofultrasound has been increasing during excision of breast tumors [107–110].For nonpalpable breast lesions, IOUS is more convenient and quicker thanpreoperative needle localization methods. After localization, repeated IOUScan assist resection of breast lesions with adequate margins. After resection,the specimen can be scanned in a water bath as a completion examination toconfirm that the lesion has been completely excised (Fig. 14).
Transplantation
In addition to preoperative and postoperative evaluation of organtransplantation, ultrasound can be used intraoperatively during trans-plantation of various organs, including liver, kidney, pancreas, and hearttransplantation. IOUS is mainly performed for assessment of vascular
1103J. Machi et al / Surg Clin N Am 84 (2004) 1085–1111
anastomosis, diagnosis of intraoperative complications, and evaluation ofadequacy of blood flow in the transplanted organ, especially using intra-operative color Doppler imaging. IOUS can also be used during hepaticresection to obtain liver graft from a living donor [111].
Foreign body
Foreign-body extraction is often difficult and time consuming. Metalfragments, glass, wood, bone, and even medical instruments can be situatedfor the most part in the extremities and body wall but, occasionally, arelocated in internal organs. Radiologic studies are important as an initial toolin diagnosing foreign bodies. However, during extraction operations,nonpalpable foreign bodies are difficult to localize in the operative field,even with the use of intraoperative radiography or fluoroscopy. IOUS is anoptimal method for precise and quick localization of foreign bodies,
Fig. 14. Intraoperative ultrasound (IOUS)-guided lumpectomy of breast cancer. (A) A
nonpalpable breast cancer (T), 6.5 � 8.1 mm, was localized by IOUS. Using and repeating
IOUS as a guide, lumpectomy was performed. (B) The scanning of the resected specimen in
a water bath (W) in the operating room showed complete excision of the tumor (T) with
adequate margins.
1104 J. Machi et al / Surg Clin N Am 84 (2004) 1085–1111
including radiographically nonopaque ones, because the ultrasound probe isplaced directly on the tissue surface and real-time monitoring can beperformed. An exploratory needle can be introduced toward the foreignbody, and thus, extraction is facilitated under IOUS guidance.
Advantages and disadvantages
Although relatively new compared with intraoperative radiography, IOUShas a number of advantages, including safety, speed, high accuracy, moreimaging information, wider applicability, and ability to guide procedures [8–21]. Because of its safety and ease of use, IOUS can be used repeatedly duringthe course of an operation. The results of IOUS scanning are obtainedimmediately because of the real-time feature of ultrasound imaging. Oncelearned, IOUS is completed within a short period of time. Screening of theliver for metastasis or the bile duct for calculi takes less than 5 minutes.Staging of cancer may require 10 to 15 minutes; however, IOUS informationwill eventually reduce unnecessary tissue dissection and the operating time.
IOUS is more accurate in diagnosing certain lesions compared withpreoperative imaging studies, intraoperative contrast radiography, and evensurgical exploration. IOUS provides multiplanar images from variousdirections in real time, and thus the size and shape of target lesions areassessed more precisely. Imaging information of structures around targetlesions, such as vascular systems, is also obtained. For example, a knowledgeof vascular anatomy in reference to lesions obtained by IOUS duringlaparotomy is of great value for hepatobiliary or pancreatic surgery. IOUSis more widely applicable to various diseases and organs than intraoperativeradiography. Procedure-guiding ability of IOUS in the operative fieldcannot be achieved by intraoperative radiology. There are many proceduresthat cannot be performed without IOUS guidance; for example, biopsy ofnonpalpable deep-seated lesions or certain anatomic resections of the liver.Color and power Doppler imagings are the latest modality of ultrasound,and exhibit blood flow in color within B-mode images. Blood flowinformation is obtained in addition to anatomic information. The use ofcolor or power Doppler displays occasionally makes IOUS image in-terpretation quicker because of easier recognition of vascular structures.
Disadvantages of IOUS include limitations in certain imaging or di-agnostic abilities, need for specific instruments, and prolonged learning curve.There are limitations in detectability of small lesions and delineation of smallductal structures. Tumors smaller than 3 to 5 mm in size are not detectableeven with high-resolution ultrasound. Even certain larger tumors are difficultto detect when they are isoechoic to surrounding tissue. Because of itslimitations, IOUS should not be used to entirely replace other intraoperativediagnostic methods; complete surgical exploration by inspection and palpa-tion and appropriate use of intraoperative radiography are always important.Special instruments, in particular small probes with high-frequency

1105J. Machi et al / Surg Clin N Am 84 (2004) 1085–1111
transducers, are required for IOUS; these IOUS instruments are presentlyavailable from several manufacturers. Ultrasound examination is highlyoperator-dependent, and this is related to the learning curve. The learningcurve differs depending on the purpose of IOUS and the target organs orlesions. This learning issue will be solved if the surgeon realizes the value ofIOUS and becomes interested enough in performing IOUS by himself orherself.
Perspective
The future uses of IOUS will be brought about by a combination ofsurgeons’ experience with ultrasound and technologic advances. Somepredictable issues concerning IOUS include expansion of its applications,improvement in instrumentation, and incorporation of new ultrasoundtechnology.
The use of IOUS by surgeons will steadily increase, along with moreformal training in ultrasound for surgeons. Having competent surgeonsperforming IOUS and having IOUS instruments always available in theoperating room will permit IOUS to become an everyday tool for acquiringintraoperative information; it will allow surgeons to ‘‘see’’ in new dimension.Applications of IOUS to new fields will be also widened. This is particularlytrue in the use of laparoscopic ultrasound because of ongoing broaderapplications of laparoscopic or minimally invasive operations. Laparoscopicultrasound is one form of IOUS, and basically it employs the same ultrasoundtechnology. The basic ultrasound physics, images, advantages, and disadvan-tages of IOUS are applicable to laparoscopic ultrasound, although themethod of access differs. Laparoscopic ultrasound is technically moredemanding. Therefore, it is recommended for the surgeon who is interestedin using laparoscopic ultrasound to learn IOUS during laparotomy.
The introduction of new ultrasound technologies will lead to furtherimprovement in resolution and deeper sound penetration of IOUS. Newprobes and more user-friendly scanners for surgeons are being developed.New ultrasound technologic developments, such as harmonic imaging withcontrast agents, will improve the intraoperative use of color or powerDoppler imaging. The refinement of three-dimensional (3D) images willsimplify IOUS for planning and guiding tumor ablation or organ resections,such as hepatectomy. Anatomic and pathologic information provided by 3DIOUS will enable a quicker and more assured IOUS-guided surgicalprocedures. 3D images may increase the diagnostic confidence of thesurgeons, which is often an obstacle for the broader applications of IOUS.
Advances in various other medical or nonmedical technologies willcontinuously influence or alter surgical procedures and imaging methodsincluding IOUS. Less and less invasive surgery with smaller access sites willkeep surgeons’ hands further away from organs, thus requiring more imageguidance as seen in minimally invasive and percutaneous image-guided

1106 J. Machi et al / Surg Clin N Am 84 (2004) 1085–1111
procedures. Therefore, there will be a less distinctive border between IOUSand percutaneous interventional ultrasound. Virtual reality technology willcontinually advance so that more realistic simulation of IOUS examina-tions, as well as surgical procedures, will be available. Computer-basedultrasound simulators will greatly help future education and training inIOUS. As technology is evolving, new advances in procedures and imagingmethods including IOUS must be carefully assessed to define its emergingrole and cost-effectiveness for improving surgical practice of the future.
Summary
Instrumentation, techniques, indications, clinical applications, advan-tages, disadvantages, and future perspective of IOUS are described. IOUS isuseful not only to acquire new diagnostic information but also to guide orassist therapeutic procedures. IOUS is commonly performed duringhepatobiliary, pancreatic, endocrine, cardiovascular, and neurologic sur-gery; however, its applications are expanding to other surgical fields.Advantages of IOUS, including safety, speed, high accuracy, comprehensiveanatomic information, and real-time guidance capability outweigh itsdisadvantages, such as specific equipment requirement and slow learningcurve. The appropriate use of IOUS can have a marked impact onintraoperative management, including improved decision making; reductionin surgical tissue dissection, operating time, and complications; anddevelopment of new procedures. The use of IOUS by surgeons is expectedto increase along with more formal training and experience in ultrasound forsurgeons. With advances in ultrasound equipment and technology, theability and the type of IOUS will be improving and altering in the future, asseen in current laparoscopic ultrasound, which is one form of IOUS.
References
[1] Sigel B, Spigos DG, Donahue PE, Pearl R, Popky GL, Nyhus LM. Intraoperative
ultrasonic visualization of biliary calculi. Curr Surg 1979;36:158–9.
[2] Rubin JM, Mirfakhraee M, Duda EE, Dohrmann GJ, Brown F. Intraoperative
ultrasound examination of the brain. Radiology 1980;137:831–2.
[3] Shkolnik A, McLone DG. Intraoperative real-time ultrasonic guidance of ventricular
shunt placement in infant. Radiology 1981;141:515–7.
[4] Sigel B, Kraft AR, Nyhus LM, Coelho JCU, Gavin MP, Spigos DG. Identification of
a parathyroid adenoma by operative ultrasonography. Arch Surg 1981;116:234–5.
[5] Lane RJ, Coupland GA. Operative ultrasonic features of insulinomas. Am J Surg 1982;
144:585–7.
[6] Sahn DJ, Barratt-Boyes BG, Graham K, Kerr A, Roche A, Hill D, et al. Ultrasonic
imaging of the coronary arteries in open-chest humans: evaluation of coronary
atherosclerotic lesions during cardiac surgery. Circulation 1982;66:1034–44.
[7] Sigel B, Machi J, Anderson KW, Samuel SP, Haq SZ, Malik SA, et al. Operative
ultrasonic imaging of vascular defects. Semin Ultrasound CT MR 1985;6:85–92.

1107J. Machi et al / Surg Clin N Am 84 (2004) 1085–1111
[8] Sigel B, Coelho JCU, Machi J, Flanigan DP, Donahue PE, Schuler JJ, et al. The
application of real-time ultrasound imaging during surgical procedures. Surg Gynecol
Obstet 1983;157:33–7.
[9] Machi J, Sigel B. Overview of benefits of operative ultrasonography during a ten year
period. J Ultrasound Med 1989;8:647–52.
[10] Sigel B, Machi J, Beitler JC, Donahue PE, Bombeck CT, Baker RJ, et al. Comparative
accuracy of operative ultrasonography and cholangiography in detecting common bile
duct calculi. Surgery 1983;94:715–20.
[11] Sigel B, Machi J, Anderson KW, Samuel SP, Malik SA, Haq SZ, et al.
Operative sonography of the biliary tree and pancreas. Semin Ultrasound CT MR
1985;6:2–14.
[12] Sigel B, Machi J, Ramos JR, Duarte B, Donahue PE. The role of imaging ultrasound
during pancreatic surgery. Ann Surg 1984;200:486–93.
[13] Machi J, Sigel B, Beitler JC, Coelho JCU, Donahue PE, Duarte B, et al. Ultrasonic
examination during surgery for abdominal abscess. World J Surg 1983;7:409–15.
[14] Machi J, Sigel B, editors. Ultrasound for surgeons. New York: Igaku-Shoin; 1997.
[15] Machi J, Sigel B, Kurohiji T, Zaren HA, Sariego J. Operative ultrasound guidance for
various surgical procedures. Ultrasound Med Biol 1990;16:37–42.
[16] Machi J, Sigel B. Intraoperative ultrasonography. Radiol Clin North Am 1992;30:
1085–103.
[17] Machi J, Sigel B, Kurohiji T, Yamashita Y, Zaren HA, Hosokawa T, et al. Operative
color Doppler imaging for general surgery. J Ultrasound Med 1993;12:455–61.
[18] Machi J, Sigel B. Operative ultrasound in general surgery. Am J Surg 1996;172:15–20.
[19] Machi J. Intraoperative and laparoscopic ultrasound. Surg Oncol Clin N Am 1999;8:
205–26.
[20] Staren ED, Arregui ME, editors. Ultrasound for the surgeon. Philadelphia: Lippincott-
Raven; 1997.
[21] Kane RA, editor. Intraoperative, laparoscopic and endoluminal ultrasound. Philadelphia:
Churchill Livingstone; 1999.
[22] Staren ED. Ultrasound for surgeons. Curr Surg 1997;54:339–53.
[23] Kolecki R, Schirmer B. Intraoperative and laparoscopic ultrasound. Surg Clin North Am
1998;78:251–71.
[24] Luck AJ, Maddern GJ. Intraoperative abdominal ultrasonography. Br J Surg 1999;86:
5–16.
[25] Silas AM, Kruskal JB, Kane RA. Intraoperative ultrasound. Radiol Clin North Am 2001;
39:429–48.
[26] Makuuchi M, Hasegawa H, Yamazaki S. Ultrasonically guided subsegmentectomy. Surg
Gynecol Obstet 1985;161:346–50.
[27] Castaing D, Emond J, Kunstlinger F, Bismuth H. Utility of operative ultrasound in the
surgical management of liver tumors. Ann Surg 1986;204:600–5.
[28] Gozzetti G, Mazziotti A, Bolondi L, Cavallari A, Grigioni W, Casanova P, et al.
Intraoperative ultrasonography in surgery for liver tumors. Surgery 1986;99:523–30.
[29] Bismuth H, Castaing D, Garden OJ. The use of operative ultrasonography in surgery of
primary liver tumors. World J Surg 1987;11:610–4.
[30] Makuuchi M, Hasegawa H, Yamazaki S, Takayasu K. Four new hepatectomy
procedures for resection of the right hepatic vein and preservation of the inferior right
hepatic vein. Surg Gynecol Obstet 1987;164:68–72.
[31] Rifkin MD, Rosato FE, Branch HM, Foster J, Yang SL, Barbot DJ, et al. Intraoperative
ultrasound of the liver. An important adjunctive tool for decision making in the operating
room. Ann Surg 1987;205:466–72.
[32] Nagasue N, Kohno H, Chang Y-C, Galizia G, Hayashi T, Yukaya H, et al.
Intraoperative ultrasonography in resection of small hepatocellular carcinoma associated
with cirrhosis. Am J Surg 1989;158:40–2.

1108 J. Machi et al / Surg Clin N Am 84 (2004) 1085–1111
[33] Parker GA, Lawrence W Jr, Horsley JS 3rd, Neifeld JP, Cook D, Walsh J, et al.
Intraoperative ultrasound of the liver affects operative decision making. Ann Surg 1989;
209:569–77.
[34] Takada T, Yasuda H, Uchiyama K, Hasegawa H, Shitaka J. Contrast-enhanced
intraoperative ultrasonography of small hepatocellular carcinomas. Surgery 1990;107:
528–32.
[35] Takayama T, Makuuchi M, Watanabe K, Kosuge T, Takayasu K, Yamazaki S, et al. A
new method for mapping hepatic subsegment: counterstaining identification technique.
Surgery 1991;109:226–9.
[36] Lau WY, Leung KL, Lee TW, Li AK. Ultrasonography during liver resection for
hepatocellular carcinoma. Br J Surg 1993;80:493–4.
[37] Kane RA, Hughes LA, Cua EJ, Steele GD, Jenkins RL, Cady B. The impact of intra-
operative ultrasonography on surgery for liver neoplasms. J UltrasoundMed 1994;13:1–6.
[38] Solomon MJ, Stephen MS, Gallinger S, White GH. Does intraoperative hepatic sonog-
raphy change surgical decision making during liver resection? Am J Surg 1994;168:307–10.
[39] Kruskal JB, Kane RA. Intraoperative ultrasonography of the liver. Crit Rev Diagn
Imaging 1995;36:175–226.
[40] Zhang W, Niu HO, Zhao GW, Su KJ, Wei HC, Su ZX, et al. Use of intraoperative
ultrasonography during hepatolithectomy. World J Surg 1996;20:50–4.
[41] Staren ED, Gambla M, Deziel DJ, Velasco J, Saclarides TJ, Millikan K, et al. Intra-
operative ultrasound in the management of liver neoplasms. Am Surg 1997;63:591–7.
[42] Torzilli G, Takayama T, Hui AM, Kubota K, Harihara Y, Makuuchi M. A new technical
aspect of ultrasound-guided liver surgery. Am J Surg 1999;178:341–3.
[43] Jarnagin WR, Bach AM, Winston CB, Hann LE, Heffernan H, Loumeau T, et al. What is
the yield of intraoperative ultrasonography during partial hepatectomy for malignant
disease? J Am Coll Surg 2001;192:577–83.
[44] Zacherl J, Scheuba C, Imhof M, Zacherl M, Langle F, Pokieser P, et al. Current value of
intraoperative sonography during surgery for hepatic neoplasms. World J Surg 2002;26:
550–4.
[45] Torzilli G, Makuuchi M. Intraoperative ultrasonography in liver cancer. Surg Oncol Clin
N Am 2003;12:91–103.
[46] Machi J, Isomoto H, Yamashita Y, Kurohiji T, Shirouzu K, Kakegawa T. Intraoperative
ultrasonography in screening for liver metastases from colorectal cancer: comparative
accuracy with traditional procedures. Surgery 1987;101:678–84.
[47] Boldrini G, de Gaetano AM, Giovannini I, Castagneto M, Colagrande C, Castiglinoi G.
The systematic use of operative ultrasound for detection of liver metastases during
colorectal surgery. World J Surg 1987;11:622–7.
[48] Russo A, Sparacino G, Plaja S, Cajozza M, La Rosa C, Demma I, et al. Role of
intraoperative ultrasound in the screening of liver metastases from colorectal carcinoma:
initial experiences. J Surg Oncol 1989;42:249–55.
[49] Olsen AK. Intraoperative ultrasonography and the detection of liver metastases in
patients with colorectal cancer. Br J Surg 1990;77:998–9.
[50] Machi J, Isomoto H, Kurohiji T, Yamashita Y, Shirouzu K, Kakegawa T, et al. Accuracy
of intraoperative ultrasonography in diagnosing liver metastasis from colorectal cancer:
evaluation with postoperative follow-up results. World J Surg 1991;15:551–7.
[51] Knol JA, Marn CS, Francis IR, Rubin JM, Bromberg J, Chang AE. Comparisons of
dynamic infusion and delayed computed tomography, intraoperative ultrasound, and
palpation in the diagnosis of liver metastasis. Am J Surg 1993;165:81–8.
[52] Stone MD, Kane R, Bothe A Jr, Jessup JM, Cady B, Steele GD Jr. Intraoperative
ultrasound imaging of the liver at the time of colorectal cancer resection. Arch Surg 1994;
129:431–6.
[53] Rafaelsen SR, Kronborg O, Larsen C, Fenger C. Intraoperative ultrasonography in
detection of hepatic metastasis from colorectal cancer. Dis Colon Rectum 1995;38:355–60.

1109J. Machi et al / Surg Clin N Am 84 (2004) 1085–1111
[54] Karl RC, Choi J, Yeatman TJ, Clark RA. Role of computed tomographic arterial
portography and intraoperative ultrasound in the evaluation of patients for resectability
of hepatic lesions. J Gastrointest Surg 1997;1:152–8.
[55] Cervone A, Sardi A, Conaway GL. Intraoperative ultrasound (IOUS) in essential in the
management of metastatic colorectal liver lesions. Am Surg 2000;66:611–5.
[56] Rydzewski B, Dehdashti F, Gordon BA, Teefey SA, Strasberg SM, Siegel BA. Usefulness
of intraoperative sonography for revealing hepatic metastases from colorectal cancer in
patients selected for surgery after undergoing FDG PET. AJR Am J Roentgenol 2002;
178:353–8.
[57] Curley SA, Izzo F, Delrio P, Ellis LM, Granchi J, Vallone P, et al. Radiofrequency
ablation of unresectable primary and metastatic hepatic malignancies. Results in 123
patients. Ann Surg 1999;230:1–8.
[58] Machi J, Uchida S, Sumida K, Limm WML, Hundahl SA, Oishi AJ, et al. Ultrasound-
guided radiofrequency thermal ablation of liver tumors: percutaneous, laparoscopic and
open surgical approaches. J Gastrointest Surg 2001;5:477–89.
[59] Buckley AR, Scudamore CH, Becker CD, Cooperberg PL. Intraoperative imaging of the
biliary tree. Sonography vs. operative cholangiography. J UltrasoundMed 1987;6:589–95.
[60] Chardavoyne R, Kumari-Subhaya S, Auguste LJ, Phillips G, Stein TA, Wise L.
Comparison of intraoperative ultrasonography and cholangiography in detection of small
common bile duct stones. Ann Surg 1987;206:53–5.
[61] Jakimowicz JJ, RuttenH, Jurgens PJ, Carol EJ. Comparison of operative ultrasonography
and radiography in screening of commonbile duct for calculi.World J Surg 1987;11:628–34.
[62] Mosnier H, Audy JC, Boche O, Guivarc’h M. Intraoperative sonography during
cholecystectomy for gallstones. Surg Gynecol Obstet 1992;174:469–73.
[63] Machi J, Sigel B, Zaren HA, Kurohiji T, Yamashita Y. Operative ultrasonography during
hepatobiliary and pancreatic surgery. World J Surg 1993;17:640–6.
[64] Azuma T, Yoshikawa T, Araida T, Takasaki K. Intraoperative evaluation of the depth of
invasion of gallbladder cancer. Am J Surg 1999;178:381–4.
[65] Plainfosse MC, Bouillot JL, Rivaton F, Vaucamps P, Hernigou A, Alexandre JH. The use
of operative sonography in carcinoma of the pancreas. World J Surg 1987;11:654–8.
[66] Sigel B, Machi J, Kikuchi T, Anderson KW 3rd, Horrow M, Zaren HA. The use of
ultrasound during surgery for complications of pancreatitis. World J Surg 1987;11:659–63.
[67] Machi J, Sigel B, Kodama I, Zaren HA. Ultrasound-guided pancreatotomy for opening
the pancreatic duct. Surg Gynecol Obstet 1991;173:59–60.
[68] Printz H, Klotter HJ, Nies C, Hasse C, Neurath M, Sitter H, et al. Intraoperative
ultrasonography in surgery for chronic pancreatitis. Int J Pancreatol 1992;12:233–7.
[69] Serio G, Fugazzola C, Iacono C, Bergamo Andreis IA, Portuese A, Zicari M, et al.
Intraoperative ultrasonography in pancreatic cancer. Int J Pancreatol 1992;11:31–41.
[70] Kubota K, Noie T, Sano K, Abe H, Bandai Y, Makuuchi M. Impact of intraoperative
ultrasonography on surgery for cystic lesions of the pancreas. World J Surg 1997;21:72–7.
[71] Sugiyama M, Hagi H, Atomi Y. Reappraisal of intraoperative ultrasonography for
pancreatobiliary carcinomas: assessment of malignant portal venous invasion. Surgery
1999;125:160–5.
[72] Kaneko T, Nakao A, Inoue S, Sugimoto H, Hatsuno T, Ito A, et al. Intraoperative
ultrasonography by high-resolution annular array transducer for intraductal papillary
mucinous tumors of the pancreas. Surgery 2001;129:55–65.
[73] Angelini L, Bezzi M, Tucci G, Lirici MM, Candiani F, Rubaltelli L, et al. The ultrasonic
detection of insulinomas during surgical exploration of the pancreas. World J Surg 1987;
11:642–7.
[74] Klotter HJ, Ruckert K, Kummerle F, Rothmund M. The use of intraoperative
sonography in endocrine tumors of the pancreas. World J Surg 1987;11:635–41.
[75] Doppman JL, Shawker TH, Miller DL. Localization of islet cell tumors. Gastroenterol
Clin N Am 1989;18:793–804.
1110 J. Machi et al / Surg Clin N Am 84 (2004) 1085–1111
[76] Norton JA, Shawker TH, Doppman JL, Miller DL, Fraker DL, Cromack DT, et al.
Localization and surgical treatment of occult insulinomas. Ann Surg 1990;212:615–20.
[77] Zeiger MA, Shawker TH, Norton JA. Use of intraoperative ultrasonography to localize
islet cell tumors. World J Surg 1993;17:448–54.
[78] Huai JC, Zhang W, Niu HO, Su ZX, McNamara JJ, Machi J. Localization and surgical
treatment of pancreatic insulinomas guided by intraoperative ultrasound. Am J Surg
1998;175:18–21.
[79] Hiramoto JS, Feldstein VA, LaBerge JM, Norton JA. Intraoperative ultrasound and
preoperative localization detects all occult insulinomas. Arch Surg 2001;136:1020–6.
[80] Machi J, Takeda J, Kakegawa T, Yamana H, Fujita H, Kurohiji T, et al. The detection of
gastric and esophageal tumor extension by high-resolution ultrasound during surgery.
World J Surg 1987;11:664–71.
[81] Kodama I, Machi J, Tanaka M, Yoshida C, Hashimoto K, Takeda J, et al. The value of
operative ultrasonography in diagnosing tumor extension of carcinoma of the stomach.
Surg Gynecol Obstet 1992;174:479–84.
[82] Demirci S, Cetin R, Yerdel MA, Kocaoglu H, Tunc G, Unal M. Value of high-resolution
intraoperative ultrasonography in the determination of limits of horizontal tumor spread
during surgery for gastric malignancy. J Surg Oncol 1995;59:56–62.
[83] Norton JA, Shawker TH, Jones BL, Spiegel AM, Marx SJ, Fitzpatrick L, et al.
Intraoperative ultrasound and reoperative parathyroid surgery: an initial evaluation.
World J Surg 1986;10:631–9.
[84] Kern KA, Shawker TH, Doppman JL, Miller DL, Marx SJ, Spiegel AM, et al. The use of
high-resolution ultrasound to locate parathyroid tumors during reoperations for primary
hyperparathyroidism. World J Surg 1987;11:579–85.
[85] Desai D, Jeffrey RB, McDougall IR, Weigel RJ. Intraoperative ultrasonography for
localization of recurrent thyroid cancer. Surgery 2001;129:498–500.
[86] Karwowski JK, Jeffrey RB, McDougall IR, Weigel RJ. Intraoperative ultrasonography
improves identification of recurrent thyroid cancer. Surgery 2002;132:924–9.
[87] Lane RJ, Ackroyd N, Appleberg M, Graham J. The application of operative ultrasound
immediately following carotid endarterectomy. World J Surg 1987;11:593–7.
[88] Rosenbloom MS, Flanigan DP. The use of ultrasound during reconstructive arterial
surgery of the lower extremities. World J Surg 1987;11:598–603.
[89] Machi J, Sigel B, Roberts AB. Intraoperative use of B-mode and color Doppler imaging.
In: Yao JST, Pearce WH, editors. Technologies in vascular surgery. Philadelphia: W.B.
Saunders; 1992. p. 201–17.
[90] Dougherty MJ, Hallett JW Jr, Naessens JM, Bower TC, Cherry KJ, Gloviczki P, et al.
Optimizing technical success of renal revascularization: the impact of intraoperative
color-flow duplex ultrasonography. J Vasc Surg 1993;17:849–57.
[91] Mays BW, Towne JB, Seabrook GR, Cambria RA, Jean-Claude J. Intraoperative carotid
evaluation. Arch Surg 2000;135:525–9.
[92] Mullenix PS, Tollefson DFJ, Olsen SB, Hadro NC, Andersen CA. Intraoperative duplex
ultrasonography as an adjunct to technical excellence in 100 consecutive carotid
endarterectomies. Am J Surg 2003;185:445–9.
[93] Takamoto S, Kyo S, Adachi H, Matsumura M, Yokote Y, Omoto R. Intraoperative
color flow mapping by real-time two-dimensional Doppler echocardiography for
evaluation of valvular and congenital heart disease and vascular disease. J Thorac
Cardiovasc Surg 1985;90:802–12.
[94] Ungerleider RM, Greeley WJ, Sheikh KH, Kern FH, Kisslo JA, Sabiston DC Jr. The use
of intraoperative echo with Doppler color flow imaging to predict outcome after repair of
congenital cardiac defects. Ann Surg 1989;210:526–34.
[95] Cheitlin MD, Armstrong WF, Aurigemma GP, Beller GA, Bierman FZ, Davis JL, et al.
ACC/AHA/ASE 2003 guideline update for the clinical application of echocardiography:

1111J. Machi et al / Surg Clin N Am 84 (2004) 1085–1111
summary article. A report of the American College of Cardiology/American Heart
Association Task Force on Practice Guidelines. Circulation 2003;108:1146–62.
[96] Katsnelson Y, Raman J, Katsnelson F, Mor-Avi V, Heller LB, Jayakar D, et al. Current
state of intraoperative echocardiography. Echocardiography 2003;20:771–80.
[97] Machi J, Sigel B, Jafar JJ, Menoni R, Beitler JC, Bernstein RA, et al. Criteria for using
imaging ultrasound during brain and spinal cord surgery. JUltrasoundMed 1984;3:155–61.
[98] Chandler WF, Rubin JM. The application of ultrasound during brain surgery. World J
Surg 1987;11:558–69.
[99] Rubin JM, Chandler WF. The use of ultrasound during spinal cord surgery. World J Surg
1987;11:570–8.
[100] ChackoAG,KumarNK,ChackoG,AthyalR,RajshekharV. Intraoperative ultrasound in
determining the extent of resection of parenchymal brain tumours—a comparative study
with computed tomography and histopathology. Acta Neurochir (Wien) 2003;145:743–8.
[101] van Velthoven V. Intraoperative ultrasound imaging: comparison of pathomorphological
findings in US versus CT, MRI and intraoperative findings. Acta Neurochir Suppl 2003;
85:95–9.
[102] Alken P, Thuroff JW, Hammer C. The use of operative ultrasonography for the
localization of renal calculi. World J Surg 1987;11:586–92.
[103] Marino G, Gamba P, Del Noce G, Pugno E, Bradac R, Garberoglio R, et al.
Intraoperative localization and management of renal calculi during nephrolithotomy by
real-time ultrasonography. Arch Ital Urol Androl 2002;74:197–9.
[104] Marshall FF, Holdford SS, Hamper UM. Intraoperative sonography of renal tumors.
J Urol 1992;148:1393–6.
[105] Choyke PL, Daryanani K. Intraoperative ultrasound of the kidney. Ultrasound Q 2001;
17:245–53.
[106] Machi J, Hayashida R, Kurohiji T, Nishimura Y, Edakuni S, Yamashita Y, et al.
Operative ultrasonography for lung cancer surgery. J Thorac Cardiovasc Surg 1989;98:
540–5.
[107] Snider HC Jr, Morrison DG. Intraoperative ultrasound localization of nonpalpable
breast lesions. Ann Surg Oncol 1999;6:308–14.
[108] Harlow SP, Krag DN, Ames SE, Weaver DL. Intraoperative ultrasound localization to
guide surgical excision of nonpalpable breast carcinoma. J Am Coll Surg 1999;189:241–6.
[109] Kaufman CS, Jacobson L, Bachman B, Kaufman L. Intraoperative ultrasound facilitates
surgery for early breast cancer. Ann Surg Oncol 2002;9:988–93.
[110] Gittleman MA. Single-step ultrasound localization of breast lesions and lumpectomy
procedure. Am J Surg 2003;186:386–90.
[111] Kawasaki S, Makuuchi M, Miyagawa S, Matsunami H, Hashikura Y, Ikegami T, et al.
Extended lateral segmentectomy using intraoperative ultrasound to obtain a partial liver
graft. Am J Surg 1996;171:286–8.