intermittent pneumatic compression is effective in preventing symptomatic pulmonary embolism after...
TRANSCRIPT

Surg Today (2004) 34:6–10DOI 10.1007/s00595-003-2636-x
Intermittent Pneumatic Compression Is Effective in PreventingSymptomatic Pulmonary Embolism After Thoracic Surgery
Itaru Nagahiro, Akio Andou, Motoi Aoe, Yoshifumi Sano, Hiroshi Date, and Nobuyoshi Shimizu
Department of Cancer and Thoracic Surgery, Okayama University Medical School, 2-5-1 Shikata-cho, Okayama 700-8558, Japan
Key words Postoperative pulmonary embolism · Inter-mittent pneumatic compression · Iliac compressionsyndrome
Introduction
Although pulmonary embolism (PE) tends to be lesscommon in Japan (28/100000 per year1,2) than in theUnited States (69/100000 per year3), the number ofpatients with postoperative PE in Japan seems to beincreasing recently, probably because we have becomemore aware of the disease. Postoperative PE is a fatalcomplication in many surgical procedures, and severalmethods for its prevention have been employed, suchas the administration of low doses of subcutaneousunfractionated heparin or low-molecular-weight hep-arins.4 These methods are still controversial and are notuniversally used because of their adverse side effects,such as bleeding due to anticoagulation therapy.5 A pro-phylactic method that is not associated with such riskswould clearly deserve serious consideration for moreuniversal use if it provides a similar level of protectionagainst thromboembolism.
Intermittent pneumatic compression, a mechanicalprevention of PE, have been extensively examined es-pecially in orthopedic surgery and have been confirmedas efficacious.6–8 However, there have been few reportsin general thoracic surgery on the prophylactic use ofintermittent pneumatic compression. In the presentstudy, we used pneumatic compression, examined itseffect, and tried to identify the risk factors of postopera-tive PE in general thoracic surgery.
Patients and Methods
Seven hundred and six patients, who had neither anyprevious episodes of deep venous thrombosis (DVT) or
AbstractPurpose. Postoperative pulmonary embolism (PE) re-mains a fatal complication even in thoracic surgery. Wehave used intermittent pneumatic compression for theprophylaxis of postoperative PE since 1998, and hereinexamined its effectiveness.Methods. Seven hundred and six patients, whose medi-cal records showed use/no use of pneumatic compres-sion for prophylaxis of PE, underwent general thoracicsurgery in our department from December 1995 to De-cember 2000. Their clinical records were reviewed, andvariables were compared between patients who experi-enced clinically apparent PE and patients who did nothave PE.Results. Three hundred and forty-four patients did notreceive any prophylactic treatment, and 7 of these(2.0%) experienced postoperative PE. Three hundredand sixty-two patients received prophylactic pneumaticcompression and none of these developed PE. Therewas a statistical correlation between the occurrence ofPE and the application of pneumatic compression (�2-test, P � 0.006). Six of the seven patients with PE wereoperated on in the right decubitus position, and theoperative position and the prevalence of PE was alsosignificantly correlated (�2-test, P � 0.024). Other fac-tors, such as age, sex, operative time, duration untilpatients became fully ambulatory, body mass index, andcharacter of the disease, did not have significant correla-tion with the occurrence of PE.Conclusions. Pneumatic compression was found to ef-fectively prevent postoperative PE. The right decubitusposition is considered to be a risk factor for the develop-ment of postoperative PE in thoracic surgery.
Reprint requests to: I. NagahiroReceived: October 4, 2002 / Accepted: March 11, 2003

7I. Nagahiro et al.: Pneumatic Compression Prevents Pulmonary Embolism
PE, underwent general thoracic surgery under generalanesthesia in our department from December 1995 toDecember 2000. No preoperative examination to detectDVT (e.g., Duplex Doppler ultrasonography or venog-raphy) was performed, and no other PE prophylaxisother than pneumatic compression was employed inany patient. Sequential pneumatic compression boots(Flowtron Plus, Huntleigh Health Care, Luton, UK)were introduced in our department in December 1998.No routine prophylaxis for PE had been employed in ourdepartment prior to that time and the intermittent pneu-matic compression was employed for all patients thereaf-ter. The boots were placed on the patient immediatelyafter tracheal intubation, and remained in place until thepatient became fully ambulatory. Alternating pneumaticcompression of both calves was achieved by the inflationof each boot during a 30-s period to a pressure of40 mmHg, and the pressure was maintained for 1 min andthereafter the boots were totally decompressed.
The indications for PE were by dyspnea and tachyp-nea, collapse, tachycardia, persistent hypoxia despite ofoxygen inhalation, and palpitation and/or arrhythmiasthat were not controlled by medication.9 Patients sus-pected of having PE then underwent diagnostic exami-nations including echocardiogram, chest computedtomography (CT) scan, ultrasonography of femoralveins, pulmonary perfusion scan, and pulmonaryangiography if necessary. In cases where a perfusiondefect was found in scintigraphy or thrombus in thepulmonary artery on CT scan or pulmonary angiogra-phy was observed, the patient was diagnosed as having
postoperative PE and then was treated with anticoagu-lation therapy and vena cava filter insertion.
The patients’ records were reviewed and the patientswere divided into two groups: one group received inter-mittent pneumatic compression while the other groupdid not. The correlations between the incidence of PEand clinical factors (age, gender, body mass index, op-erative time, days until becoming fully ambulatory, thecharacter of lesion, operative method, and operativeposition) were examined.
The data are presented as the mean � standard de-viation of the mean or as number of patients in a group.Differences between the mean values were analyzedusing Student’s t-test or the Mann-Whitney U-test. Acomparison of frequencies between the groups wasmade using the chi-squared test with Fisher’s exact test.Differences were considered statistically significant atthe 95% confidence level (P � 0.05).
Results
Three hundred and forty-four patients did not receiveintermittent pneumatic compression, while 362 receivedintermittent pneumatic compression during the studyperiod. Seven patients experienced symptomatic post-operative PE, but none of them had received intermit-tent pneumatic compression. The occurrence ofsymptomatic PE and the application of intermittentpneumatic compression had a statistically significantcorrelation (Table 1). The operative position also corre-
Table 1. Patient characteristics and postoperative pulmonary embolism
PE (�) PE (�) P value
Age 69.1 � 5.5 59.1 � 16.1 0.102Sex
Male 4 480Female 3 219 0.684
Body mass index (kg/m2) 23.2 � 4.0 21.6 � 3.5 0.245Operative time (min) 206.4 � 38.6 207.4 � 93.4 0.978Fully ambulatory (POD) 3.5 � 2.7 2.7 � 1.5 0.168Pneumatic compression
(�) 0 362(�) 7 337 0.006
LesionMalignant 6 429Benign 1 270 0.260
Operative methodVATS 1 263Thoracotomy 6 436 0.266
Operative positionRight decubitus 6 227Left decubitus 0 302Bilateral decubitus 0 40Supine 1 130 0.024
PE, pulmonary embolism; POD, postoperative day; VATS, video-assisted thoracic surgery
8 I. Nagahiro et al.: Pneumatic Compression Prevents Pulmonary Embolism
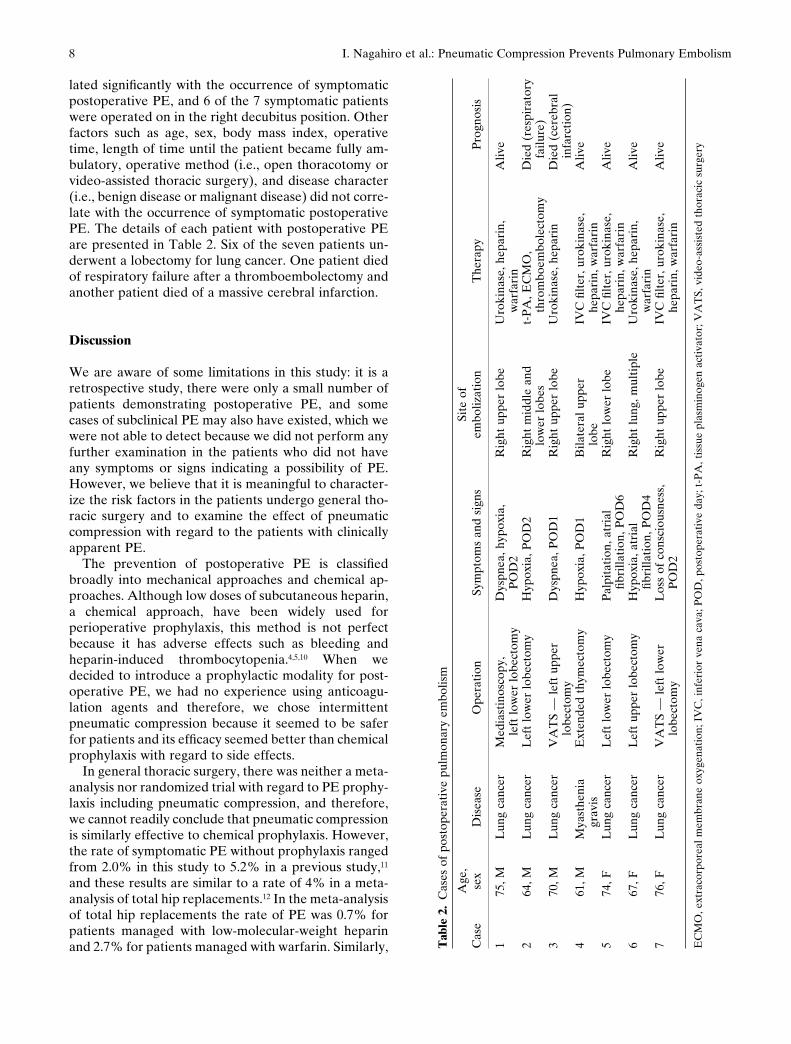
lated significantly with the occurrence of symptomaticpostoperative PE, and 6 of the 7 symptomatic patientswere operated on in the right decubitus position. Otherfactors such as age, sex, body mass index, operativetime, length of time until the patient became fully am-bulatory, operative method (i.e., open thoracotomy orvideo-assisted thoracic surgery), and disease character(i.e., benign disease or malignant disease) did not corre-late with the occurrence of symptomatic postoperativePE. The details of each patient with postoperative PEare presented in Table 2. Six of the seven patients un-derwent a lobectomy for lung cancer. One patient diedof respiratory failure after a thromboembolectomy andanother patient died of a massive cerebral infarction.
Discussion
We are aware of some limitations in this study: it is aretrospective study, there were only a small number ofpatients demonstrating postoperative PE, and somecases of subclinical PE may also have existed, which wewere not able to detect because we did not perform anyfurther examination in the patients who did not haveany symptoms or signs indicating a possibility of PE.However, we believe that it is meaningful to character-ize the risk factors in the patients undergo general tho-racic surgery and to examine the effect of pneumaticcompression with regard to the patients with clinicallyapparent PE.
The prevention of postoperative PE is classifiedbroadly into mechanical approaches and chemical ap-proaches. Although low doses of subcutaneous heparin,a chemical approach, have been widely used forperioperative prophylaxis, this method is not perfectbecause it has adverse effects such as bleeding andheparin-induced thrombocytopenia.4,5,10 When wedecided to introduce a prophylactic modality for post-operative PE, we had no experience using anticoagu-lation agents and therefore, we chose intermittentpneumatic compression because it seemed to be saferfor patients and its efficacy seemed better than chemicalprophylaxis with regard to side effects.
In general thoracic surgery, there was neither a meta-analysis nor randomized trial with regard to PE prophy-laxis including pneumatic compression, and therefore,we cannot readily conclude that pneumatic compressionis similarly effective to chemical prophylaxis. However,the rate of symptomatic PE without prophylaxis rangedfrom 2.0% in this study to 5.2% in a previous study,11
and these results are similar to a rate of 4% in a meta-analysis of total hip replacements.12 In the meta-analysisof total hip replacements the rate of PE was 0.7% forpatients managed with low-molecular-weight heparinand 2.7% for patients managed with warfarin. Similarly, T
able
2.
Cas
es o
f po
stop
erat
ive
pulm
onar
y em
bolis
m
Age
,Si
te o
fC
ase
sex
Dis
ease
Ope
rati
onSy
mpt
oms
and
sign
sem
boliz
atio
nT
hera
pyP
rogn
osis
175
, ML
ung
canc
erM
edia
stin
osco
py,
Dys
pnea
, hyp
oxia
,R
ight
upp
er lo
beU
roki
nase
, hep
arin
,A
live
left
low
er lo
bect
omy
PO
D2
war
fari
n2
64, M
Lun
g ca
ncer
Lef
t lo
wer
lobe
ctom
yH
ypox
ia, P
OD
2R
ight
mid
dle
and
t-P
A, E
CM
O,
Die
d (r
espi
rato
rylo
wer
lobe
sth
rom
boem
bole
ctom
yfa
ilure
)3
70, M
Lun
g ca
ncer
VA
TS
— le
ft u
pper
Dys
pnea
, PO
D1
Rig
ht u
pper
lobe
Uro
kina
se, h
epar
inD
ied
(cer
ebra
llo
bect
omy
infa
rcti
on)
461
, MM
yast
heni
aE
xten
ded
thym
ecto
my
Hyp
oxia
, PO
D1
Bila
tera
l upp
erIV
C fi
lter
, uro
kina
se,
Aliv
egr
avis
lobe
hepa
rin,
war
fari
n5
74, F
Lun
g ca
ncer
Lef
t lo
wer
lobe
ctom
yP
alpi
tati
on, a
tria
lR
ight
low
er lo
beIV
C fi
lter
, uro
kina
se,
Aliv
efib
rilla
tion
, PO
D6
hepa
rin,
war
fari
n6
67, F
Lun
g ca
ncer
Lef
t up
per
lobe
ctom
yH
ypox
ia, a
tria
lR
ight
lung
, mul
tipl
eU
roki
nase
, hep
arin
,A
live
fibri
llati
on, P
OD
4w
arfa
rin
776
, FL
ung
canc
erV
AT
S —
left
low
erL
oss
of c
onsc
ious
ness
,R
ight
upp
er lo
beIV
C fi
lter
, uro
kina
se,
Aliv
elo
bect
omy
PO
D2
hepa
rin,
war
fari
n
EC
MO
, ext
raco
rpor
eal m
embr
ane
oxyg
enat
ion;
IV
C, i
nfer
ior
vena
cav
a; P
OD
, pos
tope
rati
ve d
ay; t
-PA
, tis
sue
plas
min
ogen
act
ivat
or; V
AT
S, v
ideo
-ass
iste
d th
orac
ic s
urge
ry

9I. Nagahiro et al.: Pneumatic Compression Prevents Pulmonary Embolism
in a study on total hip arthroplasty, the prevalence ofpostoperative PE or DVT in patients with sequentialpneumatic compression devices with thigh-high elasticcompression stockings was similar to chemical prophy-laxis with warfarin or low-molecular-weight heparin.7
These previous results and those of the present study, inwhich no symptomatic PE was observed in patientsmanaged with pneumatic compression, indicate that theefficacy of pneumatic compression would be compa-rable to chemical prophylaxis of PE.
The advantages of intermittent pneumatic compres-sion are the presumed decrease in the incidence ofperioperative bleeding complications and the lack ofthe need for the monitoring required with oral or subcu-taneous anticoagulation therapy. Penumatic compres-sion in preventing PE not only increases the venousblood flow13 but also increases endogenous fibrinolysisby stimulating the vascular endothelial wall.14 Anadverse effect of pneumatic compression, namely footulcers, has been reported in patients who were treatedwith pneumatic compression boots of the foot sole typeand a compression pressure of 80–120 mmHg.15 In thepresent study, no such side effect was seen, probablybecause of the difference in the type of boots and thecompression pressure used. We used knee-high com-pression boots, and the compression pressure was aslow as 40 mmHg. Although the application of intermit-tent pneumatic compression decreased the incidence ofpostoperative PE from 2% to 0% in the present study,even the patients who received pneumatic compressionsuffered postoperative DVT for the incidence of 4.6%–14.2% and postoperative PE for 0.6% in orthopedicsurgery.7,8 Therefore, pneumatic compression, similar toanticoagulant therapies, is not a perfect prophylaxis forpostoperative PE.
An interesting result in the present study was that theoperative position had a significant correlation with theincidence of postoperative PE. No previous clear expla-nation exists; however, an anatomical reason must beconsidered, i.e., iliac compression syndrome. The con-cept that compression and posteroanterior flattening ofthe left common iliac vein at its origin between the rightcommon iliac artery and lumbosacral spine might leadto clinical symptoms was first introduced by Cockettand Thomas 30 years ago.16 Thrombosis is allegedly themain complication of iliac vein compression. If the com-pression is as common as anatomical studies suggest,and if it largely explains the three-to-one proportion ofleft- to right-side lower limb thrombosis, its role as aprethrombotic factor has to be substantial and its im-portance is thus probably underrated.17 In the presentstudy, 6 of 7 patients with postoperative PE were oper-ated on in the right decubitus position, and no PE oc-curred in the left decubitus position patients. Thisdiscrepancy in the operative position might indicate
that postoperative PE in general thoracic surgery is ex-plained by iliac compression syndrome. Moreover, thesite of thromboembolism was the right side in all pa-tients with PE operated on in the right decubitus posi-tion in this series (Table 2). This might indicate that thegeneration of thromboembolism starts during surgeryand then the thrombus migrates into the right side bygravity or increasing blood flow after a lobectomy, andtherefore, the prophylaxis should be initiated eitherpreoperatively or perioperatively. Although it is diffi-cult to demonstrate compression by venography,17
a recent report clearly demonstrated compression bythree-dimensional spiral computed tomography.18 Fur-ther examination regarding the correlation between theoperative position and the compression of the left com-mon iliac vein is thus needed.
In conclusion, intermittent pneumatic compressionwas found to be effective in preventing postoperativePE in general thoracic surgery, and its results may becomparable to chemical prophylaxis. To expel postop-erative DVT and PE perfectly, the combination of in-termittent pneumatic compression and anticoagulanttherapy or other methods may be necessary. The rightdecubitus position is a risk factor for postoperative PE,and iliac compression syndrome may be a mechanism inthe generation of thrombus.
Acknowledgments. We are indebted to the resident surgeonsin our department for their conscientious contributions tothis study. We also thank Dawn Schuessler for her valuablesecretarial support.
References
1. Kumasaka N, Sakuma M, Shirato K. Incidence of pulmonarythromboembolism in Japan. Jpn Circ J 1999;63:439–41.
2. Hirose J. Pulmonary thromboembolism: is the incidence accu-rate? Jpn Circ J 1999;63:825–7.
3. Silverstein MD, Heit JA, Mohr DN, Petterson TM, O’FallonWM, Melton LJ. Trends in the incidence of deep vein thrombosisand pulmonary embolism. Arch Intern Med 1998;158:585–93.
4. Goldhaber SZ. Pulmonary embolsim. N Engl J Med 1998;339:93–104.
5. Rokito SE, Schwartz MC, Neuwirth MG. Deep vein thrombosisafter major reconstructive spinal surgery. Spine 1996;21:853–9.
6. Tsutsumi K, Udagawa H, Kajiyama Y, Kinoshita Y, Ueno M,Nakamura T, et al. Pulmonary thromboembolism after surgeryfor esophageal cancer: its features and prophylaxis. Surg Today2000;30:416–20.
7. Hooker JA, Lachiewicz PF, Kelley SS. Efficacy of prophylaxisagainst thromboembolism with intermittent pneumatic compres-sion after primary and revision total hip arthroplasty. J Bone JointSurg 1999;81-A:690–6.
8. Lin PP, Graham D, Hann LE, Boland PJ, Healey JH. Deepvenous thrombosis after orthopedic surgery in adult cancerpatients. J Surg Oncol 1998;68:41–7.
9. Stein PD, Terrin ML, Hales CA, Palevsky HI, Saltzman HA,Thompson T, et al. Clinical, laboratory, roentgenographic, andelectrocardiographic findings in patients with acute pulmonary

10 I. Nagahiro et al.: Pneumatic Compression Prevents Pulmonary Embolism
embolism and no pre-existing cardiac or pulmonary disease.Chest 1991;100:598–603.
10. Hull R, Raskob G, Pieo G, Rosenbloom D, Evans W, Mallory T,et al. A comparison of subcutaneous low molecular-weightheparin with warfarin sodium for prophylaxis against deep-veinthrombosis after hip or knee implantation. N Engl J Med1998;329:1370–6.
11. Ziomek S, Read RC, Tobler G, Harrell JE, Gocio JC, Fink LM,et al. Thromboembolism in patients undergoing thoracotomy.Ann Thorac Surg 1993;56:223–7.
12. Imperiale TF, Speroff T. A meta-analysis of method to preventvenous thromboembolism following total hip replacement.JAMA 1994;271:1780–5.
13. Christen Y, Reymond MA, Vogal JJ, Klopfenstein CE, Morel P,Bounameaux H. Hemodynamic effects of intermittent pneumatic
compression of the lower limbs during laparoscopic cholecystec-tomy. Am J Surg 1995;170:395–8.
14. Allenby F, Boardman L, Pflug JJ, Calnan JS. Effects of externalpneumatic intermittent compression on fibrinolysis in man.Lancet 1973;22:1412–4.
15. Oakley MJ, Wheelwright EF, James PJ. Pneumatic compressionboots for prophylaxis against deep vein thrombosis: betwareoccult arterial disease. BMJ 1998;316:454–5.
16. Cockett FB, Thomas ML. The iliac compression syndrome. Br JSurg 1965;52:816–21.
17. Verhaeghe R. Iliac compression as an anatomical cause of throm-bophilia: Cockett’s syndrome revised. Thromb Haemost 1995;74:1398–401.
18. Sakakibara Y, Kujiraoka Y. Iliac compression syndrome. Circula-tion 1998;98:376.