intent-to-treat analysis of health care expenditures of patients treated with atypical...
TRANSCRIPT

GT
A
Clinical Therapeutics/Volume 33, Number 9, 2011
Intent-to-Treat Analysis of Health Care Expenditures ofPatients Treated With Atypical Antipsychotics as AdjunctiveTherapy in Depression
Yonghua Jing, PhD1; Iftekhar Kalsekar, PhD1; Suellen M. Curkendall, PhD2;inger S. Carls, PhD3; Erin Bagalman, MSW2; Robert A. Forbes, PhD4;ony Hebden, PhD1; and Michael E. Thase, MD5
1Bristol-Myers Squibb, Plainsboro, New Jersey; 2Thomson Reuters, Washington, DC; 3Thomson Reuters,nn Arbor, Michigan; 4Otsuka Pharmaceutical Development and Commercialization, Princeton, New
Jersey; and 5Perelman School of Medicine, University of Pennsylvania, Philadelphia, Pennsylvania
t3p
ct4tp
ABSTRACTObjective: To compare health care utilization and
expenditures in patients with depression whose initialantidepressant (AD) treatment was augmented with asecond-generation antipsychotic.
Methods: Claims data from January 1, 2001,through June 30, 2009, were used to select patientsaged 18 to 64 years with depression treated with ADsaugmented with aripiprazole, olanzapine, or quetiap-ine. Patients were required to have 6 months of contin-uous eligibility before the first AD prescription and 6months after the second-generation antipsychotic aug-mentation (index) date. Utilization and expenditureswere assessed for 6 months after the index date. Mul-tivariate regression was used to estimate adjusted ex-penditures and risks for hospitalizations and emer-gency department visits.
Results: A total of 483 patients treated with arip-iprazole, 978 with olanzapine, and 2471 with quetia-pine were selected. Mean adjusted expenditures foraripiprazole were significantly lower than those forolanzapine for each service category (all-cause, all-cause medical care, mental health-related, and mentalhealth-related medical care) and were significantlylower than those for quetiapine for each category withthe exception of mental health-related. The adjustedrisks for hospitalization and emergency departmentvisits were significantly higher for quetiapine than foraripiprazole.
Conclusions: Compared with patients treated withADs and aripiprazole, those treated with ADs andolanzapine or quetiapine had greater utilization andhigher expenditures. (Clin Ther. 2011;33:1246–1257)
© 2011 Elsevier HS Journals, Inc. All rights reserved.1246
Key words: aripiprazole, cost, depression, healthcare utilization, second-generation antipsychoticaugmentation.
INTRODUCTIONThe annual prevalence of major depressive disorder(MDD) is estimated at 6.6%, affecting approximately14 million adults in the United States.1 With a lifetimeprevalence of 16.2%, more than 30 million US adultswill experience MDD at some point in their lives.1 Theotal cost burden in 2000 was $83.1 billion, of which1% was direct costs, 62% absenteeism and decreasedroductivity costs, and 7% suicide-related costs.2 A
more recent study using insurance claims data esti-mated the 2-year direct and indirect cost burden in2007 US dollars to be $32,537 for patients with treat-ment-resistant depression compared with $20,976 forpatients with MDD.3
Despite treatment, a portion of MDD patients willfail to achieve remission. The Sequenced TreatmentAlternatives to Relieve Depression (STAR*D) studyexamined remission rates in successive acute treatmentsteps, finding rates of 32.9%, 30.6%, 13.6%, and14.7% for levels 1 through 4, respectively.4,5 With aumulative remission rate of 67%, approximately onehird of patients will not achieve remission.5 Although7% of first-level STAR*D study patients respondedo therapy, defined as a �50% reduction in self-re-orted symptom score,4 response without remission
Accepted for publication: July 19, 2011.doi:10.1016/j.clinthera.2011.07.0150149-2918/$ - see front matter
© 2011 Elsevier HS Journals, Inc. All rights reserved.
Volume 33 Number 9

cc
i
fa
ahia
tpfwlSmAddetc(pilt
fndvcm
Y. Jing et al.
has been associated with poorer outcomes,6 with de-reased remission rates, and increased relapse rates oc-urring with each successive course of treatment.7
Up to 15% of patients with MDD may have aninadequate response to antidepressant (AD) therapydespite appropriate dosing, length of treatment, andcompliance with the prescribed regimen. Direct medi-cal costs of inadequate responders are 40% highercompared with patients who respond to therapy.7,8
Studies have shown inadequate responders use moremedical services,9,10 are more likely to be hospital-ized,11 use a greater number of psychotropic medica-tions,11 and have significantly greater costs of disabil-ty and absenteeism.9,10 Health care costs have alsobeen shown to increase significantly as the number ofAD treatment regimen changes increases.12
The American Psychiatric Association practiceguidelines for treatment of MDD include augmenta-tion with second-generation antipsychotics (SGAs) as atreatment option for patients who do not respond ad-equately to first-line ADs, while noting the need forcomparative research into the various augmentationstrategies.13 Aripiprazole was the first SGA approvedor adjunctive use in the treatment of MDD, receivingpproval in late 2007.14 Olanzapine and quetiapine
were used off-label for this indication before gainingapproval in 2009.15–17
This study compares the health care utilization andexpenditures of patients with depression who initiatedAD therapy followed by augmentation with 1 of 3 dif-ferent SGAs (aripiprazole, olanzapine, or quetiapine)approved by the Food and Drug Administration as ad-junctive treatment for depression. The study tests thehypothesis that adjunctive therapy with aripiprazole isless costly than that with either olanzapine orquetiapine.
PATIENTS AND METHODSData Source
Data were derived from the MarketScan Commer-cial Claims and Encounters Database (Ann Arbor,Michigan). This database contains the health care ex-perience of approximately 40 million privately insuredindividuals annually covered under a variety of fee-for-service, fully capitated, and partially capitated healthplans. The current study used data from January 1,2001, through June 30, 2009. Detailed cost, use, andoutcomes data are available, covering inpatient ser-
vices, outpatient services, and prescription drugSeptember 2011
claims. Medical claims are linked to outpatient pre-scription drug claims and person-level enrollment datathrough unique enrollee numbers. Data are fully com-pliant with the Health Insurance Portability and Ac-countability Act.
Patient SelectionPatients aged 18 to 64 years with depression were
selected based on the occurrence of at least 2 claimswith different dates between January 1, 2001, throughJune 30, 2009 (enrollment window), containing Inter-national Classification of Diseases, Ninth Revision,Clinical Modifications (ICD-9-CM) diagnosis codes296.2, 296.3, 300.4, 309.0, and 311. Patients wererequired to have at least 1 prescription claim in theenrollment window for an oral or injectable AD asdefined by the following drug classes: tricyclic antide-pressants, selective serotonin reuptake inhibitors, �2-drenergic receptor antagonists, monamine oxidase in-ibitors, norepinephrine and dopamine reuptakenhibitors, serotonin-2 antagonist-reuptake inhibitors,nd serotonin-norepinephrine reuptake inhibitors.
To identify patients treated with ADs and adjunc-ive SGAs, patients were screened for the presence of arescription for aripiprazole, olanzapine, or quetiapineollowing the first AD prescription in the enrollmentindow. Concurrent use was determined by an over-
ap of at least 30 days in the days supply of the firstGA prescription with any AD prescription with noore than 6 gap days. Patients were allowed to switchDs before SGA augmentation as long as the new ADid not overlap with the original AD by more than 29ays. To establish that the first AD prescription in thenrollment window was not a continuation of priorreatment, patients were required to have 6 months ofontinuous medical and prescription drug coverageincluding mental health coverage) before this first ADrescription and to have no other claims for ADs dur-ng the 6 months. Patients were also required to have ateast 6 months of follow-up subsequent to the date ofhe augmentation prescription (index date).
As with earlier research, patients were excludedrom the study if they had a medical claim with a diag-osis of any of the following: dementia, schizophrenia,elusional disorder, other nonorganic psychoses, per-asive development disorder, mental retardation, othererebral degenerations, Parkinson’s disease, senility,anic depression, or bipolar disorder.7,9,11 Patients
were also excluded if they had a medical claim with a
1247

Clinical Therapeutics
diagnosis of MDD with psychotic features, in order torule that out as a reason for augmenting AD treatmentwith an SGA. Finally, patients were excluded if pre-scriptions for medications within 2 different augmen-tation classes appeared on the index date, if they had aprescription claim for clozapine, if a prescription forone of the augmentation classes appeared before theinitial AD prescription, or if they had evidence of elec-troconvulsive therapy before the index date.
Patient selection resulted in 3 mutually exclusiveaugmentation cohorts, each cohort containing patientstreated with an AD and aripiprazole, olanzapine, orquetiapine.
OutcomesHealth care utilization and expenditures were as-
sessed for the 6 months following the index date ineach of the augmentation cohorts. The expendituresfor claims processed under a fee-for-service arrange-ment were the allowed charges (ie, the actual amountspaid by primary and secondary insurers plus patientcost share amounts [ie, copayments and deductibles]).The expenditures for claims processed under a capi-tated arrangement were estimated using the mean ex-penditures of noncapitated claims by geographic re-gion and by year. All expenditures were standardizedto 2009 US $ using the medical care component of theConsumer Price Index.
Expenditures were quantified within 4 categories:(1) all-cause (ie, claims from all providers—medical[including costs from hospitals, physicians, and labo-ratories] and outpatient pharmacy—regardless of diag-nosis or drug codes contained on claims), (2) all-causemedical care (ie, excludes outpatient pharmacy), (3)mental health–related (ie, medical and outpatientpharmacy claims containing codes consistent withmental health diagnoses, procedures, providers, ortherapy), and (4) mental health–related medical care(ie, excludes outpatient pharmacy). Specifically, men-tal health–related was defined by inpatient claims witha principal ICD-9-CM diagnosis in the range 290 to319; outpatient claims in which the first diagnosislisted was in the range 290 to 319; claims with mentalhealth procedures, such as therapeutic behavioral ser-vices; claims in which the provider type was a mentalhealth provider, such as a psychiatrist, psychologist, ormental health facility; or claims for drugs in the Red
Book therapeutic classes of ADs, tranquilizers/antipsy-1248
chotics, barbiturates, benzodiazepines, other anx-iolytic/sedative/hypnotics, and other antimanic agents.
The percentage of patients with all-cause and men-tal health–related hospitalizations and emergency de-partment (ED) visits was determined in each of theaugmentation cohorts.
CovariatesPatient demographic covariates, measured on the
index date, included age, gender, US Census BureauRegion of residence (Northeast, North Central, South,and West), urban versus rural residence, and insuranceplan type (comprehensive, exclusive provider organi-zation, health maintenance organization, point of ser-vice, point of service with capitation, preferred pro-vider organization, consumer-driven health plan, andhigh-deductible health plan). Year of the first AD pre-scription was recorded, as was the mean number ofunique ADs before the index date.
Health status covariates measured during the 6months before the index date included the mean Charl-son Comorbidity Index (CCI) score (Deyo version),18
the mean number of psychiatric diagnosis groups,19
and the mean Massachusetts General Hospital Antide-pressant (MGH-AD) score.7,20 The CCI estimates theburden of comorbid illness and is a numeric scale basedon the presence or absence of 19 conditions (eg, diabe-tes, heart disease), each assigned a weight, with higherscores indicating greater burden. Psychiatric diagnosisgroups include conditions not included in the CCI (eg,organic mental disorders, substance user disorders),with counts ranging from 1 to 12. The MGH-AD scorewas developed for use in claims data to measure treat-ment resistance, assigning 1 point for each adequateAD trial (defined as at least 2 fills for the same AD) and0.5 points for each optimization strategy. Optimiza-tion strategies included an extended duration (at least 3fills) or an upward titration in dose. A higher scoreindicates greater treatment resistance.
A modal daily dose was calculated during the6-month follow-up period for the augmentation SGA.The daily dose for each prescription claim was calcu-lated using the number of pills supplied, the strength ofeach pill, and the days supply as written on the pre-scription, where Daily Dose � Number of Pills �Strength � Days Supply. For example, daily dose cal-culated from a prescription claim indicating 10 pills of50-mg strength dispensed with a value of 5 in the days
supply field is 100 mg. To determine the modal dailyVolume 33 Number 9

etTAc
Y. Jing et al.
dose for each patient, the daily dose on all the patient’sprescription claims for the augmented drug during the6-month follow-up period were examined. The dosethat was prescribed for the most total days suppliedwas used as the mode. When total days supplied werethe same between 2 different doses, the higher dose wasused.
Patients were classified as to whether the SGA wasbelow, within, or above therapeutic range.21–24 Thetherapeutic range was defined according to the dosingof each SGA: 5 to 15 mg for aripiprazole, 150 to 300mg for quetiapine, and 6 to 20 mg for olanzapine. Todate, olanzapine has been tested for use in MDD onlyin a fixed combination formulation with fluoxetine.Although the maximum dose of olanzapine is 18 mgfor this fixed combination, 20 mg was chosen as theupper limit of the within therapeutic dose for the cur-rent study because olanzapine as a single entity is onlyavailable in 2.5-, 5-, 7.5-, 10-, 15-, and 20-mgstrengths. The fixed combination product was not usedto identify olanzapine.
Statistical AnalysesInitially, the aripiprazole cohort was compared with
the olanzapine cohort and (separately) the quetiapinecohort using pair-wise comparisons. Categorical out-comes and covariates were presented as counts andpercentages; statistical significance of differences wasdetermined using �2 tests. Continuous outcomes andcovariates were reported as means and SDs; statisticalsignificance of differences was determined using t tests.
General linear regression models with a log link,Poisson family, and robust standard errors were esti-mated to estimate adjusted risk ratios for all-cause hos-pitalization, mental health–related hospitalization, all-cause ED visits, and mental health–related ED visits.Nonlinear regression models were estimated for healthcare expenditures (all-cause, all-cause medical care,mental health–related, and mental health–related med-ical care) to estimate adjusted differences in the directhealth care expenditures of patients in each of the 3treatment regimens. These models were implementedusing a generalized linear model with a log link andgamma distribution.25 Models controlled for differ-nces in patient demographic and clinical characteris-ics, including adjustment by therapeutic dose range.he only covariate not used was the number of uniqueDs before the index date, as these data were already
aptured in the MGH-AD covariate.September 2011
RESULTSA total of 336,977 patients met the selection criteriafor age, depression diagnoses, AD use, eligibility, andexclusionary diagnoses and drugs. Of these patients,3989 augmented with 1 of the study SGAs. Fifty-sevenof the 3989 patients were excluded owing to missing oroutlier dose data. The resulting sample included 3932patients: 483 receiving adjunctive therapy with arip-iprazole, 978 with olanzapine, and 2471 withquetiapine.
Baseline CharacteristicsPatients treated with olanzapine and quetiapine
were significantly older than patients treated with arip-iprazole and included a higher proportion of males(Table I). Relative to patients receiving aripiprazole,those receiving olanzapine had a significantly lowermean number of psychiatric diagnosis groups. TheMGH-AD mean score was significantly lower in boththe olanzapine and quetiapine cohorts than in the arip-iprazole cohort. There were no significant differencesin the mean CCI scores. The majority of patientstreated with olanzapine (70.8%) and quetiapine(80.3%) received doses below the therapeutic range. Incontrast, 79.3% of patients treated with aripiprazolereceived doses within the therapeutic range, and only14.5% received doses below the therapeutic range.
Health Care UtilizationA significantly lower percentage of patients receiv-
ing aripiprazole experienced all-cause hospitalizations(11.8%) and mental health–related ED visits (2.5%)compared with patients receiving quetiapine (15.6%,P � 0.02 and 4.7%, P � 0.01, respectively) (Table II).Differences between the aripiprazole and olanzapinecohorts were not significant.
The adjusted risks comparing aripiprazole-treatedpatients and quetiapine-treated patients were signifi-cantly higher for quetiapine for all-cause hospitaliza-tions, mental health–related hospitalizations, all-causeED visits, and mental health–related ED visits. Ad-justed risks comparing patients treated with olanzap-ine and aripiprazole were not significantly different.
Health Care ExpendituresThe unadjusted medical, pharmacy, and total ex-
penditures are shown in Table III. Unadjusted meanall-cause expenditures were lower for the aripiprazole
cohort ($6248) than for the olanzapine cohort ($8942,1249

Clinical Therapeutics
Table I. Baseline characteristics.
Characteristic
AripiprazoleN � 483%/Mean
OlanzapineN � 978%/Mean P*
QuetiapineN � 2471%/Mean P†
Age in Years (SD) 37.2 (12.6) 41.6 (12.6) �0.01 39.7 (12.6) �0.01Age Group �0.01 �0.01
18–34 42.0% 29.4% 35.8%35–44 25.7% 26.2% 25.0%45–54 22.6% 27.3% 24.8%55–64 9.7% 17.1% 14.4%
Gender �0.01 �0.01Male 40.6% 49.5% 47.6%Female 59.4% 50.5% 52.4%
Insurance Plan Type �0.01 0.24Comprehensive 11.8% 16.2% 11.9%Exclusive Provider Organization 1.7% 1.0% 0.8%Health Maintenance Organization 18.6% 21.9% 19.1%Point of Service (POS) Plan 15.5% 12.3% 13.4%Preferred Provider Organization 46.6% 44.1% 49.5%POS with capitation 0.8% 2.2% 1.6%Consumer Driven Health Plan 2.9% 1.8% 2.6%High Deductible Health Plan 1.9% 0.3% 1.0%
Urbanicity 0.02 0.20Urban 85.9% 80.6% 86.3%Rural 13.0% 18.7% 13.3%
Geographic Region �0.01 0.36Northeast 16.4% 10.8% 14.0%North Central 31.3% 32.5% 31.3%South 36.0% 32.9% 38.3%West 14.7% 22.4% 15.5%
Year of 1st Antidepressant �0.01 �0.012002 0.8% 19.6% 4.7%2003 7.0% 29.0% 10.8%2004 12.2% 17.6% 16.1%2005 12.6% 11.9% 17.6%2006 16.8% 9.4% 18.4%2007 21.1% 6.0% 17.6%2008 29.4% 6.4% 14.9%
# Unique Antidepressants Prior to Index (SD) 1.01 (0.84) 0.77 (0.77) �0.01 0.87 (0.83) �0.01Charlson Comorbidity Index (SD) 0.22 (0.75) 0.27 (0.89) 0.29 0.23 (0.78) 0.80Psychiatric Diagnosis Groups (SD) 1.48 (1.06) 1.17 (1.03) �0.01 1.59 (1.15) 0.06MGH-Antidepressant Only (SD) 0.81 (0.91) 0.53 (0.82) �0.01 0.53 (0.79) �0.01Therapeutic Range of Augmented Antipsychotic �0.01 �0.01
Below therapeutic range 14.5% 70.8% 80.3%Within therapeutic range 79.3% 28.5% 15.6%Above therapeutic range 6.2% 0.7% 4.1%
*P-value for olanzapine compared with aripiprazole.†P-value for quetiapine compared with aripiprazole.
1250 Volume 33 Number 9

pmewit
cittjqt
tdqm(t0i
emttndtp
Tabl
eII.
Hea
lthc
are
utili
zati
ondu
ring
6m
onth
saf
ter
augm
enta
tion
.
Util
izat
ion
Mea
sure
Arip
ipra
zole
N�
483
Ola
nzap
ine†
N�
978
Que
tiapi
ne‡
N�
2,47
1
%A
vera
geLO
S*%
P-Va
lue
Ave
rage
LOS*
P-Va
lue
Adj
uste
dR
elat
ive
Ris
k(9
5%C
I)%
P-Va
lue
Ave
rage
LOS*
P-Va
lue
Adj
uste
dR
elat
ive
Ris
k(9
5%C
I)
Hos
pita
lSta
ysA
ll-ca
use
11.8
%4.
614
.1%
0.21
5.0
0.65
1.30
(0.9
5–1.
78)
15.6
%0.
025.
50.
171.
42(1
.07–
1.89
)M
enta
lHea
lth-r
elat
ed6.
6%6.
75.
6%0.
466.
90.
901.
31(0
.83–
2.07
)8.
7%0.
107.
30.
571.
76(1
.19–
2.60
)
ERVi
sits
All-
caus
e16
.1%
N/A
18.0
%0.
37N
/AN
/A1.
28(0
.98–
1.68
)19
.7%
0.06
N/A
N/A
1.35
(1.0
6–1.
72)
Men
talH
ealth
-rel
ated
2.5%
N/A
3.2%
0.45
N/A
N/A
1.75
(0.8
6–3.
55)
4.7%
�0.
01N
/AN
/A2.
53(1
.33–
4.80
)
*Ave
rage
LOS
�M
ean
leng
thof
stay
was
calc
ulat
edfo
rpa
tient
sw
hoha
da
hosp
itals
tay.
†O
lanz
apin
eP-
valu
esan
dre
lativ
eris
kvs
.arip
ipra
zole
.‡Q
uetia
pine
P-va
lues
and
rela
tive
risk
vs.a
ripip
razo
le.
Y. Jing et al.
P � 0.06) and significantly lower than for the quetia-ine cohort ($7696, P � 0.02) (Figure 1). After adjust-ent for clinical and demographic covariates, mean
xpenditures in aripiprazole-treated patients ($5952)ere significantly lower than expenditures in olanzap-
ne-treated patients ($8009, P � 0.04) or quetiapine-reated patients ($8788, P � 0.01).
Both unadjusted and regression-adjusted mean all-ause medical care expenditures (expenditures exclud-ng outpatient pharmacy) were significantly lower forhe aripiprazole cohort than the olanzapine cohort orhe quetiapine cohort (Figure 2). After regression ad-ustment, the relationship between olanzapine anduetiapine reversed so that expenditures in quetiapine-reated patients were highest.
Unadjusted mean mental health–related expendi-ures for the aripiprazole cohort were not significantlyifferent from those for the olanzapine cohort or theuetiapine cohort (Figure 3). Regression-adjustedean expenditures for aripiprazole-treated patients
$2514) were significantly lower when compared withhose for olanzapine-treated patients ($3853, P �.01) but not when compared with those for quetiap-ne-treated patients ($3325, P � 0.06).
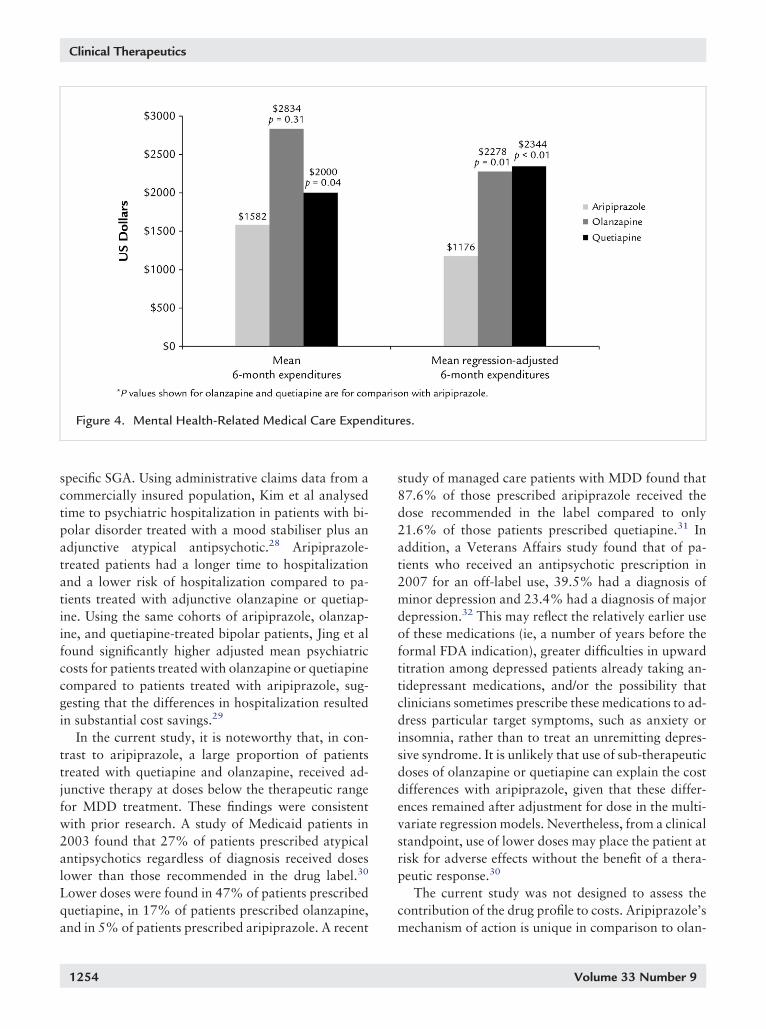
Unadjusted mean mental health–related medical carexpenditures (expenditures excluding outpatient phar-acy) were significantly lower for the aripiprazole cohort
han for the quetiapine cohort, but differences betweenhe aripiprazole cohort and the olanzapine cohort wereot significant (Figure 4). Regression-adjusted expen-itures were significantly lower for aripiprazole-reated patients ($1176) than for quetiapine-treatedatients ($2344, P � 0.01) or for olanzapine-treated
patients ($2278, P � 0.01).
DISCUSSIONThis study compared health care utilization and expen-ditures among patients with depression who receivedadjunctive therapy with one of three SGAs: aripipra-zole, olanzapine, or quetiapine. With respect to costsassociated with treatment, we found that mean ad-justed expenditures for aripiprazole-treated patientswere significantly lower than for olanzapine-treatedpatients for all categories and were lower than for que-tiapine-treated patients for all categories with signifi-cant difference in all-cause, all-cause medical care, andmental health-related medical care categories. The ad-justed risks for hospitalization and ER visits were sig-
nificantly higher for the quetiapine cohort compared toSeptember 2011 1251

stwotzo
Tpmt
Clinical Therapeutics
the aripiprazole cohort for both all-cause and mentalhealth-related services. Findings also showed temporalhifts in the use of specific SGAs as adjunctive therapy inhe treatment of depression. Quetiapine was the mostidely prescribed SGA across the study years, while usef aripiprazole occurred more frequently when initial ADherapy occurred in the later study years and use of olan-apine occurred more frequently when initial AD therapyccurred in the early study years.
Table III. Healthcare expenditures during 6 months a
AriN
Mean
All Cause Medical Care Expenditures $3946All Cause Prescription Drug Expenditures $2302All Cause Expenditures - Total $6248Mental Health-Related Medical CareExpenditures $1582Mental Health-Related Prescription DrugExpenditures $1731Mental Health-Related Expenditures - Total $3313
Figure 1. All Cause Expenditures.
1252
A recent review of treatment strategies for MDDpoints to the efficacy of augmentation with SGAs whilenoting that insufficient data are available on cost out-comes associated with their use.26 An analysis by
aneja et al evaluated cost-effectiveness of SGAs inatients with MDD through use of a decision-analyticodel that estimated outcomes and costs in patients
reated with aripiprazole, olanzapine, or quetiapine.27
Aripiprazole-treated patients had the lowest cost per
ugmentation: 2009 dollars.
zole3
OlanzapineN � 978
QuetiapineN � 2,471
% Mean % Mean %
63.20% $6866 76.80% $6048 78.60%36.80% $2076 23.20% $1648 21.40%00.00% $8942 100.00% $7696 100.00%
47.80% $2834 67.10% $2000 65.50%
52.20% $1388 32.90% $1053 34.50%00.00% $4223 100.00% $3054 100.00%
fter a
pipra� 48
1
1
Volume 33 Number 9

Y. Jing et al.
additional responder ($2798) compared to olanzapine($3324) or quetiapine ($7996 at 150 mg/d and $5706at 300 mg/d). However, because the model assumedtreatment at therapeutic doses and calculated responserates based on clinical trial data, findings provide lim-
Figure 2. All Cause Medical Care Expenditures.
Figure 3. Mental Health-Related Expenditures.
September 2011
ited insight into costs based on adjunctive use of SGAsin actual clinical practice.
Results from evaluation of SGA treatment in bipolardisorder support the findings in the current study ofdifferences in outcomes and costs based on use of a
1253
Clinical Therapeutics
specific SGA. Using administrative claims data from acommercially insured population, Kim et al analysedtime to psychiatric hospitalization in patients with bi-polar disorder treated with a mood stabiliser plus anadjunctive atypical antipsychotic.28 Aripiprazole-treated patients had a longer time to hospitalizationand a lower risk of hospitalization compared to pa-tients treated with adjunctive olanzapine or quetiap-ine. Using the same cohorts of aripiprazole, olanzap-ine, and quetiapine-treated bipolar patients, Jing et alfound significantly higher adjusted mean psychiatriccosts for patients treated with olanzapine or quetiapinecompared to patients treated with aripiprazole, sug-gesting that the differences in hospitalization resultedin substantial cost savings.29
In the current study, it is noteworthy that, in con-trast to aripiprazole, a large proportion of patientstreated with quetiapine and olanzapine, received ad-junctive therapy at doses below the therapeutic rangefor MDD treatment. These findings were consistentwith prior research. A study of Medicaid patients in2003 found that 27% of patients prescribed atypicalantipsychotics regardless of diagnosis received doseslower than those recommended in the drug label.30
Lower doses were found in 47% of patients prescribedquetiapine, in 17% of patients prescribed olanzapine,
Figure 4. Mental Health-Related Medical Care Expen
and in 5% of patients prescribed aripiprazole. A recent
1254
study of managed care patients with MDD found that87.6% of those prescribed aripiprazole received thedose recommended in the label compared to only21.6% of those patients prescribed quetiapine.31 Inaddition, a Veterans Affairs study found that of pa-tients who received an antipsychotic prescription in2007 for an off-label use, 39.5% had a diagnosis ofminor depression and 23.4% had a diagnosis of majordepression.32 This may reflect the relatively earlier useof these medications (ie, a number of years before theformal FDA indication), greater difficulties in upwardtitration among depressed patients already taking an-tidepressant medications, and/or the possibility thatclinicians sometimes prescribe these medications to ad-dress particular target symptoms, such as anxiety orinsomnia, rather than to treat an unremitting depres-sive syndrome. It is unlikely that use of sub-therapeuticdoses of olanzapine or quetiapine can explain the costdifferences with aripiprazole, given that these differ-ences remained after adjustment for dose in the multi-variate regression models. Nevertheless, from a clinicalstandpoint, use of lower doses may place the patient atrisk for adverse effects without the benefit of a thera-peutic response.30
The current study was not designed to assess thecontribution of the drug profile to costs. Aripiprazole’s
es.
diturmechanism of action is unique in comparison to olan-
Volume 33 Number 9

stlwpdA
d2
Y. Jing et al.
zapine and quetiapine in that it is a partial agonist atdopamine D2 receptors.26 All three drugs have the po-tential for side effects. In particular, some atypical an-tipsychotics may be associated with endocrinologicalconditions that may have long term cost implications.However, with the lower doses and shorter treatmentperiod for antipsychotics used in depression, endocrino-logical conditions may not be as much of an issue as inother areas of treatment. Further research is needed todetermine the contribution, if any, of these factors tocosts.
Several limitations to the study should be noted.First, this was a retrospective, observational studybased on codes of diagnoses, procedures, and providertype from healthcare administrative claims and there-fore is limited by completeness and accuracy of medicalcoding. Patients may have had other psychiatric andmedical comorbidities that were not captured in theclaims data because the patient did not seek medicalcare or the provider did not record the diagnosis on theclaim. Additionally, while patients with a bipolar dis-order diagnosis were excluded, patients with depres-sion as part of undiagnosed bipolar disorder would nothave been identified as such. Second, analysis of med-ication regimens relies on the assumption that a pre-scription filled is a prescription used when in fact dos-ing instructions may not have been followed. Further,the analysis was intent-to-treat so we did not measurewhich patients adhered to the medication during the6-month follow-up period. Third, the study durationwas only 6 months and we did not analyze how costsmay have changed over a longer period of follow-up.
Fourth, patients were not randomized to treatmentregimens and, although regression adjustment of directcosts was used to control for many of the underlyingpatient differences, residual differences may remain ifcovariates with the potential to impact costs were notcaptured or were not captured with sufficient preci-sion. For example, the MGH-AD score was used foradjustment but was computed using only 6 months ofpre-period data compared to the 24 months used inGibson et al.7 Thus, our pre-period may have been toohort a time period for observing the required prescrip-ion fills, and our scores, consequently, were muchower than the TRD threshold of 3. Fifth, study SGAsere not indicated for MDD for the entire study timeeriod, and thus patients may have been using therugs for indications other than AD augmentation.
ripiprazole received an indication for treatment ofSeptember 2011
epression in combination with ADs in November007.14 Quetiapine received an indication after the
study time period (December 2009).15 The olanzapineindication as adjunctive therapy in MDD was receivedfor the combination with fluoxetine close to the end ofthe study time period (March 2009).16,17 A prescrip-tion for the olanzapine and fluoxetine fixed-dose com-bination medication was not used to select patients inorder that the augmentation cohorts would be as ho-mogeneous as possible in terms of methods used todetermine concurrent therapy.
CONCLUSIONSIn summary, greater utilization and higher expendi-tures were found in patients with depression who weretreated with olanzapine or quetiapine as adjunctivetherapy to ADs compared to patients treated with ad-junctive aripiprazole. Further study is needed to morefully explore cost differences between SGAs.
ACKNOWLEDGMENTSThis study was conducted by Thomson Reuters andfunded by Bristol-Myers Squibb (Princeton, NewJersey) and Otsuka Pharmaceutical Co, Ltd (Tokyo,Japan). Dr. Thase worked on this project as a paidconsultant to Thomson Reuters. In addition, Dr. Thasehas provided scientific consultation to Astra-Zeneca,Bristol-Myers Squibb Company, Dey Pharma, L.P., EliLilly & Company, Forest Pharmaceuticals, Inc., GersonLehman Group, GlaxoSmithKline, Guidepoint Global,H. Lundbeck A/S, MedAvante, Inc., Merck and Co. Inc.,Neuronetics, Inc., Novartis, Otsuka, Ortho-McNeilPharmaceuticals, PamLab, LLC, Pfizer (formerly Wyeth-Ayerst Laboratories), Schering-Plough (formerly Or-ganon, Inc.), Shire US Inc., Supernus Pharmaceuticals,Takeda (Lundbeck), and Transcept Pharmaceuticals. Dr.Thase has been a member of the speakers’ bureaus forAstraZeneca, Bristol-Myers Squibb Company, Eli Lilly &Company, Merck and Co. Inc., and Pfizer (formerlyWyeth-Ayerst Laboratories). He receives grant fundingfrom Eli Lilly & Company, GlaxoSmithKline, NationalInstitute of Mental Health, and Agency for HealthcareResearch and Quality, Sepracor, Inc. Dr. Thase has eq-uity holdings in MedAvante, Inc. and receives royaltyincome from American Psychiatric Foundation, Inc.,Guilford Publications, Herald House, Oxford UniversityPress, and W.W. Norton & Company. His wife is em-ployed as the Group Scientific Director for (Embryon –
formerly Advogent; which does business with BMS1255

1
1
1
1
1
1
1
1
1
1
2
2
2
2
2
Clinical Therapeutics
and Pfizer/Wyeth). Drs. Jing, Kalsekar and Hebden areemployees of Bristol-Myers Squibb Co. and Dr. Forbesis an employee of Otsuka Pharmaceutical Co, Ltd. Allauthors participated in the study design, data interpre-tation and in review and critical revision of the manu-script. Drs. Carl, Curkendall, and Ms. Bagalman wereresponsible for the data analysis. Additionally, the au-thors acknowledge Boris Ivanov for programming, Te-resa B. Gibson for consultation regarding methods andMichele Shaw for help in preparation of themanuscript.
REFERENCES1. Kessler RC, Berglund P, Demler O, et al. The epidemiology
of major depressive disorder. Results from the NationalComorbidity Survey Replication (NCS-R). JAMA. 2003;289:3095–3105.
2. Greenberg PE, Kessler RC, Birnbaum HG, et al. Theeconomic burden of depression in the United States:how did it change between 1990 and 2000? J Clin Psychiatry.2003;64:1465–1475.
3. Ivanova JI, Birnbaum HG, Kidolezi Y, et al. Direct andindirect costs of employees with treatment-resistant andnon–treatment-resistant major depressive disorder. CurrMed Res Opin. 2010;26:2475–2484.
4. Trivedi MH, Rush AJ, Wisniewski SR, et al. Evaluation ofoutcomes with citalopram for depression using measure-ment-based care in STAR*D: implications for clinicalpractice. Am J Psychiatry. 2006;163:28–40.
5. Rush AJ, Trivedi MH, Wisniewski SR, et al. Acute andlonger-term outcomes in depressed outpatients requiringone or several treatment steps: a STAR*D report. Am JPsychiatry. 2006;163:1905–1917.
6. Fava M. Diagnosis and definition of treatment-resistantdepression. Biol Psychiatry. 2003;53:649–659.
7. Gibson TB, Jing Y, Carls GS, et al. Cost burden of treatmentresistance in patients with depression. Am J Manag Care.2010;16:370–377.
8. Berlim MT, Turecki G. Definition, assessment, and stagingof treatment-resistant refractory major depression: a reviewof current concepts and methods. Can J Psychiatry. 2007;52:46–54.
9. Corey-Lisle PK, Birnbaum HG, Greenberg PE, et al. Identifi-cation of a claims data “signature” and economic conse-quences for treatment-resistant depression. J Clin Psychiatry.2002;63:717–726.
0. Greenberg P, Corey-Lisle PK, Birnbaum H, et al. Economicimplicationsoftreatment-resistantdepressionamongemploy-
ees. Pharmacoeconomics. 2004;22:363–373.1256
1. Crown WH, Finkelstein S, Berndt ER, et al. The impact oftreatment-resistant depression on health care utilizationand costs. J Clin Psychiatry. 2002;63:963–971.
2. Russell JM, Hawkins K, Ozminkowski RJ, et al. The costconsequences of treatment-resistant depression. J ClinPsychiatry. 2004;65:341–347.
3. American Psychiatric Association Practice Guidelines, Treat-ment of Patients with Major Depressive Disorder 3rd ed.November2010.http://www.psychiatryonline.com/pracGuide/pracGuideTopic_7.aspx. Accessed February 27, 2011.
4. Abilify (aripiprazole): FDA OKs Abilify for depression.http://www.webmd.com/depression/news/20071120/fda-oks-abilify-for-depression. Accessed March 1, 2011.
5. Seroquel XR (quetiapine, extended release tablets): Sero-quel XR approvedforadjunctive treatmentofmajordepressivedisorder (MDD). http://www.empr.com/seroquel-xr-approved-for-adjunctive-treatment-of-major-depressive-disorder-mdd/article/159147/. Accessed March 1, 2011.
6. Symbyax (olanzapine/fluoxetine): Symbyax approved fortreatment-resistant depression. http://www.emaxhealth.com/1024/25/30037/symbyax-approved-treatment-resistant-depression.html. Accessed March 1, 2011.
7. Symbyax (olanzapine/fluoxetine): Symbyax approved fortreatment-resistant depression. http://www.ivillage.com/symbyax-approved-treatment-resistant-depression/4-a-113439. Accessed March 1, 2011.
8. Deyo RA, Cherkin DC, Ciol MA. Adapting a clinicalcomorbidity index for use with ICD-9-CM administrativedatabases. J Clin Epidemiol. 1992;45:613–619.
9. Ashcraft ML, Fries BE, Nerenz DR, et al. A psychiatricpatient classification system. An alternative to diagnosis-related groups. Med Care. 1989;27:543–557.
0. Petersen T, Papakostas GI, Posternak MA, et al. Empiricaltesting of two models for staging antidepresant treatmentresistance. J Clin Psychopharmacol. 2005;25:336–341.
1. Product Information: ABILIFY IM injection, oral solu-tion, oral tablets, orally disintegrating tablets, aripipra-zole IM injection, oral solution, oral tablets, orallydisintegrating tablets., Bristol-Myers Squibb, Editor:Princeton, NJ. http://www.abilify.com/pdf/pi.aspx. Ac-cessed January 20, 2011.
2. Product Information: SEROQUEL XR extended-releaseoral tablets, quetiapine fumarate extended-release oraltablets., Astra Zeneca: Wilmington, DE. http://www1.astrazeneca-us.com/pi/seroquelxr.pdf. Accessed January 20,2011.
3. ZYPREXA oral tablets, IM injection, ZYPREXA ZYDIS orallydisintegrating tablets, olanzapine oral tablets, IM injection,orally disintegrating tablets [prescribing information]. India-napolis, Ind: Eli Lilly and Company. http://pi.lilly.com/us/zyprexa-pi.pdf. Accessed January 20, 2011.
4. SYMBYAX oral capsule, olanzapine and fluoxetine hydro-
chloride oral capsule [prescribing information]. Indianap-Volume 33 Number 9

18–21, 2010.
Y. Jing et al.
olis, Ind: Eli Lilly and Company.http://pi.lilly.com/us/symbyax-pi.pdf.Accessed January 20, 2011.
25. Zou G. A modified Poisson regres-sion approach to prospective stud-ies with binary data. Am J Epidemiol.2004;59:702–706.
26. Connolly KR, Thase ME. If at firstyou don’t succeed. A review of theevidence for antidepressant augmen-tation, combination and switchingstrategies. Drugs. 2011;71:43–64.
27. Taneja C, Oster G, Jing Y, et al.Cost-effectiveness of atypical antip-sychotics as adjunctive therapy inadult patients with major depressivedisorder (MDD). Poster presentedat International Society for Phar-macoeconomics and Outcomes Re-search, 15th Annual InternationalMeeting, Atlanta, Ga, May 15–19,2010.
28. Kim E, Maclean R, Ammerman, D,et al. Time to psychiatric hospitaliza-tion in patients with bipolar disor-der treated with mood stabilizer andadjunctive atypical antipsychotics: aretrospective claims database analy-sis. Clin Ther. 2009;31:836–848.
29. Jing Y, Kim E, You M, et al. Health-care costs associated with treatmentof bipolar disorder using a moodstabilizer plus adjunctive aripipra-zole, quetiapine, risperidone, olan-zapine or ziprasidone. J Med Econ.2009;12:104–113.
30. Leslie DL, Mohamed S, RosenheckRA. Off-label use of antipsychoticmedications in the Department ofVeterans Affairs health care system.Psychiatr Serv. 2009;60:1175–1181.
31. Kogut SJ, Yam F, Dufresne R. Pre-scribing of antipsychotic medica-tion in a Medicaid population: useof polytherapy and off-label dos-ages. J Manag Care Pharm. 2005;11:17–24.
32. Thase ME, Jing Y, Guo Z, et al.Dosing patterns of aripiprazole andquetiapine for adjunctive treatmentof major depressive disorder in anoutpatient setting from 2003 to
2008. Poster presented at: US Psy-September 2011
chiatric and Mental HealthCongress, Orlando, Fla, November
Address correspondence to: Yonghua Jing, PhD, 777 Scudders Mill Road,
Plainsboro, NJ 08536. E-mail: [email protected]1257