integrated brain restoration after ischémie stroke ... enhancing brain plasticity.pdf ·...
TRANSCRIPT

Alternative Medicine Review Volume 14, Number 1 2009
Integrated Brain Restorationafter Ischémie Stroke - Medical
Management, Risk Factors, Nutrients,and other Interventions for Managing
Inflammation and EnhancingBrain Plasticity
ParrisM,Kidd,PhD
Abstract
Brain injury from ischémie stroke can be devastating, but full
brain restoration is feasible. Time until treatment is critical;
rapid rate of injury progression, logistical and personnel
constraints on neurological and cardiovascular assessment,
limitations of recombinant tissue plasminogen activator (rtPA)
forthrombolysis, anticoagulation and antiplatelet interventions,
and neu ro protect) on all affect outcome. Promising acute
neuroprotectant measures include albumin, magnesium, and
hypothermia. Long-term hyperbaric oxygen therapy (HBOT)
is safe and holds great promise. Eicosanoid and cytokine
down regulation by omega-3 nutrients docosahexaenoic acid
(DHA) and eicosapentaenoic acid (EPA) may help quench
stroke inflammation. C-reactive protein (CRP), an inflammatory
biomarker and stroke-recurrence predictor, responds favorably
to krill oil (a phospholipld-DHA/EPA-astaxanthin complex). High
homocysteine (Hey) is a proven predictor of stroke recurrence
and responds to folie acid and vitamin B^̂ . Vitamin E may
lower recurrence for individuals experieneing high oxidative
stress. Citicoline shows promise for acute neuroprotection.
Glycerophosphoeholine (GPC) is neuroproteetive and supports
neuroplasticity via nerve growth factor (NGF) reeeptors. Stem
cells have shown promise for neuronal restoration in randomized
trials. Endogenous brain stem cells can migrate to an ischémie
injury zone; exogenous stem cells once transplanted can
migrate ("home") to the stroke lesion and provide trophic
support for cortical neuroplasticity. The hematopoietie growth
factors erythropoietin (EPO) and granulocyte-colony stimulating
factor (G-CSF) have shown promise in preliminary trials, with
manageable adverse effects. Physical and mental exereises,
ineluding constraint-Induced movement therapy (CIMT) and
interactive learning aids, further support brain restoration
followingisehemiestroke. Brain plastieity underpins the function-
driven brain restoration that can occur following stroke.
IntroductionStroke, the third leading cause of death in the
United States and the leading cause oí adult disability,can be catastrophic for the aJflicted individual. Becausecurrent therapies for stroke have extremely limited ef-fectiveness, most stroke patients never fully regain lostfunction. Although total restoration oí fiuiction follow-ing stroke remains a rare accomplishment, advances inncurobiology are setting rhe foundation for a new era ofbrain restoration. This review summarizes the manage-ment of acute stroke, identifies risk iactors for second-ary prevention of stroke recurrence, and explores theresearch advances toward effective brain restoration.
Parris M. Kidd. PhD - Cell biology; University of California. Berkeley: contributingeditor, ̂ /iemai/re Medicine Review; health educator; biomédical consultant tothe dietary supplement industry.Correspondence address: 10379 Woif Drive, Grass Valley, CA 95949Emaii: [email protected]
Page 14

Alternative Medicine Review Volume 14, Number 1 2009
Post-Str^e Recovery
Stroke: A "Brain Attack"Stroke is sometimes called "brain attack" to
more aptly describe its insidious but rapid onset. Signsof stroke include:''^
• sudden, unexplained dizziness, trouble withwalking, loss of balance or unsteadiness
• confusion, trouble speaking or understanding
communication
• unexplained weakness or numbness of tbe face,
atms, or legs, or on one side of tbe body
• loss of vision in one or botb eyes
• sudden, unexplained severe headache
Stroke is a disruption of blood supply to tbebrain, whether due to blood vessel occlusion (ischémiestroke; IS) ot rupture witb bleeding (bemotrbagicstroke). As tbe blood supply becomes compromised,lack of oxygen and nutrients limit cell function and sur-vival. A zone of ecll death is created, bordered by a zoneoí damaged cells, tbe so-called penumbra. Witbin tbetotal lesion zone, oxidativc, inflammatory, and probablyalso excitotoxic cascades become activated and threatento spin out of control.
Strokes that do not totally destroy vital brainzones can nonctbeless cause ongoing impairment ofmotor, sensory, or processing pathways and eonsequcntdegradation of quality of life. Seizures, symptomaticbemorrhaging, and brain swelling occur in up to one-third of patients soon after stroke onset.' Acute man-agement of stroke is not straightforward and requiresskilled personnel. Tbe patient who does not teceiveprompt and specialized care can succumb to the spreadof brain damage.
In 2007, tbe American Heart Association andits division, the American Stroke Association, co-pub-lished an authoritative, comprehensive set of updatedguidelines for the acute management of stroke (hereinabbreviated "Guideline"). Tbe 51-page Guideline, pre-pared by a panel of experts appointed by the AmericanHeart Association Stroke Council's Seientifie State-ment Oversight Committee, was also endorsed by tbeAmerican Academy of Neurology and appeared in itsmost complete form in tbe journal CírcHÍtiííoM.' TbeGuidelines primary goal is to provide an overview ofthe current evidence on evaluation and treatment of
adults with acute ischémie stroke, with recommenda-tions covering management from tbe first contaet withemergency services personnel througb initial admissionto the hospital.
Apptoximately 80 percent of strokes are isch-émie in origin,^ since they result either from tbrombusin situ or an embolism of distant origin. Ischémie strokeis the primary focus of tbis review, with occasional com-ment on hemorrhagic stroke. Ischemia is an Insufîi-cieney of oxygen and nutrient supply due to circulatoryimpairment. Most ischémie strokes have bemorrbagicinvolvement.' In tbe United States, 700,000 people suf-fer a full-blown IS each year, 200,000 in individuals whohave suffered a previous stroke.^ Estimates of tbe num-ber wbo experience ttansient ischémie attacks (TIAs)are mucb bigber. Year by year, tbe pool of post-strokecandidates for brain restoration continues to expand.
Sttokes differ from TIAs only in degree. Ac-cording to tbe American Heart Association/AmericanStroke Association (AHA/ASA), when neurologicalsymptoms continue beyond 24 hours the event is de-fined as a stroke, wben less tban 24 bours it is a TIA.^With modern brain imaging some TIAs found to havea lesion are then classified as strokes. TiAs are impor-tant stroke predictors, witb 90-day stroke risk as higb as10.5 percent and tbe greatest stroke risk apparent in tbefirst week following the TIA.''
Among 30-day survivors of a first stroke, abouthalf survive five years.' After tbe immediate impera-tives of tbe acute phase, reducing tbe chance of anothersttoke must take ptiority. Epidcmiological studies andprospective clinical trials have identified tbe predomi-nant risk factors for recurrent stroke. An in-depthAHA/ASA document is available witb guidelines forprevention of a second stroke.' Implementation of tbeserecommendations, both by stroke survivors wirb sup-port networks and by the community as a whole, is aprerequisite for successful stroke rehabilitation.
Current Medical Management of StrokeBrain restoration ideally begins once the stroke
has been detected, relying oil efficient medical manage-ment of the acute stage. According to the Guideline,'however, acute stroke care is limited in its ability tocontain brain damage. Thronibolysis (tbrombus break-down), tbe only intervention currently approved by the
Page 15
Review^Article
Alternative Medicine Review Volume 14, Number 1 2009
U.S. Food and Drug Administration (FDA), does notwork adequately for many patients and is effective onlywhen intervention occurs within three hours of symp-tom onset. Few healthcare centers are sufliciently pre-pared to offer this intervention with the rapidity anddegree of interdisciplinary coordination the Guidelinerequires. In addition to recanalizarion (reopening) ofthe occluded vessel(s) by thrombolysis, other conven-tional interventions include management oí other cir-culatory complications by surgery or the use of antico-agulant drugs. 1
Acute Care: ThromholysisThe Guideline states that thrombolysis by the
intravenous (IV) administration of recombinant tis-sue plasminogen activator (rtPA) is the most beneficialproven intervention for emergency stroke treatment.'Approved by the FDA in 1996, it is still the only ap-proved treatment for acute IS. But due to the srrict timeconstraints for intervention, inadequate readiness atsome hospitals, substantial risk for intracerebral hem-orrhage, restrictive patient selection criteria, and otherfactors such as transport to the treatment facility, onlyone- to three-percent ot stroke patients receive rtPAtreatment.
Intravenous administration of rtPA, specifiedin the Guideline at precisely 0.9 mg/kg IV, maximum90 mg,*' is associated with improved outcomes for pa-tients who can be treated within three hours of strokeonset. Earlier treatment (i.e., within 90 minutes) givesa statistically more favorable outcome (odds ratio of2.11; 95% confidence interval, 1.33-3.55) for favorableoutcome at three months compared to placebo. In com-parison, the odds ratio for intervention at 90-180 min-utes is 1.69 (95% confidence interval, 1.09-2.62). Themajor risk from rtPA intervention is hemorrhage. In thedefinitive trial wirh 624 patients published in 1996 hythe National Institute for Neurological Disorders andStroke,"* symptomatic hemorrhage occurred in 6.4 per-cent of subjects given rtPA versus 0.6 percent of placebosubjects. Current overall expectation for hemorrhage isabout six percent.^
Despite its preferred status at the FDA andwithin the cardiovascular healthcare community, rtPAhas significant limitations. When it works, intravenousor intra-arterial rtPA takes at least 15-30 minutes to
reopen an occluded major vessel such as the middle ce-rebral artery (MCA), and no evidence exists that otherthrombolytic agents have faster action.' Doppler stud-ies stiggest only a 30-percent complete recanalizationrate for MCA occlusion after rtPA, a 48-percent partialrecanalization rate, and a 27-percent reocclusion rate.'"Combining rtPA with transcranial ultrasound signifi-cantly improved the rate of complete recanalizarion, ac-companied by marked clinical recovery. Another optionunder investigation is lower-dose IV rtPA followed bylower-dose intra-arterial rtPA delivered through an ul-trasonic catheter.^
Tlie Guideline mandates screening criteria forpatients who could reasonably be treated with rtPA, aswell as derails of the specified administration technique(refer to Tables 11 and 12 in the Guideline).' It em-phasizes that while other thromholytic drugs are cur-rently under investigation, none has been established aseffective or as a replacement for rtPA. It does suggestthat patients with ischémie stroke secondary to occlu-sion of the MCA, who are evaluated within six hours ofsymptom onset and ruled ineligible to receive IV rtPA(because of recent surgery, for example), may be candi-dates for thrombolysis by the intra-arterial route usingurokinase as the primary alternative to rtPA."
According to AHA/ASA experts, the fore-most challenge in the management of acute ischémiestroke remains to "recanaUze" rhe affected zone, thatis, to re-establish blood supply in order to preserve tis-sue viability. In rhe Guideline, surgical procedures arerejected as not proven efl'ective and bearing substantialrisk for harm.' The Guideline does suggest potentialbenefit from endovascular interventions - emergencyangioplasty and stenting, mechanical disruption of theclot, or extraction ot the thrombus. It critiques the trialsof angioplasty (with or without stenting) in combina-tion with thrombolytic agents ro achieve recanaliza-tion. Mechanical clot disruption using an endovascularphotoacoustic device can speed recanalization. Recentlydeveloped for clot extraction is a device christenedMERCI from the Mechanical Embolus Removal inCerebral Ischemia Trial;'"^ although approved by theFDA, the clinical utility of this device remains unclear.
Page 16

Alternative Medicine Review Volume 14, Number 1 2009
Post-Strgke Recovery
Anticoagulant and Antiplatelet DrugsWhile acknowledging that physicians have
used anticoagulants to treat acute ischémie stroke formore than 50 years, the Guideline questions their rou-tine use. The Guideline rules out intravenous heparinwithin the first 24 hours as not etfective and carryingLuiacceptable risk of hemorrhagic side effects. In fact,aspirin is ranked over heparin as an anriplatelet drug.
The Guideline accepts that interventions thatdown-rcgulate platelet aggregation can reduce the risktor recurrent stroke in patients with acute IS, but recom-mends aspirin as the only antiplatelet drug adequatelyvalidated for this purpose. Tlie Guideline recommendsoral aspirin (at a 325 mg/day initial dose) within 24-48hours after stroke onset for treatment of most patients.'Aspirin is classified as adjunctive to rtPA, not a sub-stitute tor it, and should not be started earlier than 24hours after stroke onset. Clopidogrel, while promising,requires further research.
VasodilatorsBeyond 24 hours of the stroke onset, the
Guideline states that vasodilators such as pentoxifyl-line and pentofylline given intravenotisly tor 3-7 daysarc unlikely to improve outcome. "Iliis is not to say thatincreasing blood perfusion does not have benefit. TheAHA/ASA experts discuss "preliminary and smallclinical studies" in which increased blood pressure to thedamaged penumbra zone seemed to improve outcome.The rationale for these studies is that the penumbra zonehas impaired autoregulation of blood pressure and thatinduced hypertension increases perfusion into the zone(as witnessed by brain imaging) to potentially salvageendangered tissue.'^ The Guideline does not recom-mend the use ot drugs to induce hypertension for thispurpose except in clinical trials or in exceptional casesinvolving close neurological and cardiac monitoring.*
Neuroprotection: Time is BrainCharacteristic of stroke is the rapid progression
of damage in the affected zone(s) of brain tissue; thefirst hours are crucial. Research in animal models sug-gests most of the tissue damaged by cerebral infarctionis beyond salvage within 1-2 hours.'"' A variety of agentsworking via diverse mechanisms have proven neuropro-tective in such models but so far none has worked in
human trials (see the GuideHne' for a review). Investi-gators suggest this is because neuroprotection must beinitiated within two hours of stroke onset, as the animalmodel experiments typically are designed.'' A popularadage in stroke research is time is brain," meaning everymoment that passes in acute stroke means more brainfunction lost.
Wliile the ongoing search for patentable neuro-protectants produced hundreds of candidates that failedto prove clinically significant in randomized controlledtrials (RCTs), three interventions unlikely to be patent-able have shown capacity for neuroprotection. Tliese areIV albumin, IV magnesium, and hypothermia.
Albumin: Safe and EffectiveNeuroprotectant
Supplementation with human serum albuminis a safe and etfective established treatment tor patientswhose circulating albumin is low.' Albumin also isknown to reduce brain swelling in patients with hem-orrhagic stroke or other brain trauma.''"' In severalanimal models of IS, albumin infusion reduced infarctsize and swelling, improved local perfusion to zones ofcritical blood flow reduction, and improved neurologi-cal and behavioral functions.' In an RCT conductedby Shin et al,'^ patients with moderate-to-severe IS inthe area of the middle cerebral artery were randomizedwithin 12 hours after symptom onset. The albumingroup was divided into three subgroups: (1) "albuminlow-dose, early" received 0.63 g/kg body weight overtwo hours; (2) "albumin high-dose, early" received 1.26g/kg over tour hours (both were completed within thefirst 12 hours of symptom onset); or (3) "albumin high-dose, late" received 1.26 g/kg over four hours, 12-24hours after symptom onset; the control group receivedsaline.
In this trial patients were subjected to thor-ough evaluations including magnetic resonance imaging(MRI), vascular studies, and blood tests.'' Neurologicalchanges were evaluated using a modified National In-stitutes of Health Stroke Scale (mNIHSS),"* initiallyat admission and subsequently on days 1, 3, 7, and 14.Functional recovery was evaluated using the BarthelIndex (BI) and modified Rankin Score (mRS) at ad-mission and on days 7, 14, 30, and 90. Infarct volumewas measured by MRI diffusion-weighted imaging atadmission and at 72-96 hours after onset.
Page 17

Revievi^rticle
Alternative Medicine Revievi/ Volume 14, Number 1 2009
Oí the 49 patients who completed the Shintrial,^^ 18 were controls, eight were in the albumin low-dose early, 13 were in the albumin high-dose early, and10 were in the albumin high-dose late subgroups. Al-though infarct volume continued to increase in controlsand albumin groups, when measured at 72-96 houtsafter onset the volume increase was significantly less inthe album in-treated patient group as a whole (26.0% in-crease versus 67.2% increase for the controls, p=0.012).Among the albumin subgroups, only the high-dose pa-tients treated early showed significantly lower infarctincrease (which notably was only 1-2% over the volumeat admission), whereas the controls averaged almost a100-percent increase. The neurological scores for thealbumin patients evaluated vía mNIHSS were signifi-cantly more improved than the controls at days 3,7, and
14. The functional analyses using BI and mRS showedsignificantly higher functional independence in the al-bumin group at day 90, with the high-dose albumingiven early working best.
Albumin's neuroprotective effects can be ex-plained via several mechanisms. This protein has a pro-longed circulating half-life [about 20 days), and its highmolecular weight keeps it in the blood vessel lumen,drawing in water and thereby expanding blood vol-ume.^ '^'" Albumin is also a potent antioxidant, a largemolecule carrying a high density of cysteine groups.'''
Albumin clearly has strong benefit in acute15, without troublesome adverse effects. Besides hav-ing the advantage that it can be applied anytime within24 hours of stroke onset, as shown in the Shin trial,"'albumin is cost-effective compared to other in-hospítal
interventions.
Intravenous Magnesium SulfateIonized magnesium has demonstrated effec-
tive neuroprotection in animal models of cerebral isch-emia, excitotoxic injury, bead trauma, and spinal corddamage.'" Magnesium sulfate is a ready source of ion-ized magnesium with an established safety and efficacyprofile in myocardial ischemia.' An international RCT- the Intravenous Magnesium Efficacy in Stroke (IM-AGES) trial - suggests magnesium has neuroprotectivepotential for acute ischémie stroke.''
The IMAGES trial produced 90-day survivaland disability data on 2,386 patients treated with IV
magnesium sulfate started within 12 hours after strokeonset (16 millimoles over 15 minutes, then 65 milli-moles over 24 hours). Although it found no statisticallysignificant overall benefit, it did show a trend towardprotection for patients with noncortical stroke."' Giv-en the pressing need for stroke interventions, this wassufficient to justify the Field Administration of StrokeTherapy-Magnesium (FAST-MAG) trial.'" An open-label trial prelude ro FAST-MAG found dramatic earlyrecovery in 42 percent of patients inftised within twohours of stroke onset.^^ Ar 90 days post-stroke onset,good global function was achieved by 69 percent ofall patients and by 75 percent of patients infused withmagnesium sulfate within two hours of stroke onset.
FAST-MAG is a large, controlled trial withthe statistical power to detect modest treatment ciîectsof IV magnesium sulfate for very early stroke. FAST-MAG is being conducted primarily in the field - magne-sium sulfate is easily administered and can bo given overa wide dosage range without harm."̂ *' Tliis unique trialhopes to demonstrate "pre-hospital initiation" whethermagnesium infusion therapy, mostly via paramedics, canbe effective in halting or slowing the ischcmic cascadein most patients within those first crucial two hours. Ifthis bold field trial proves to improve stroke outcome,it could usher in a tiew era of acute stroke managementsince rtPA cannot realistically be administered in thefield.
Hypothermia: Already a Good TrackRecord
Hypothermia slows cerebral metabolism andprotects neurons subjected to acute ischemia. This isa potent intervention that improves neurological out-comes after cardiac arrest and has been used to treatpatients with severe brain edema."̂ ^ Because the opti-mal body temperature for stroke management is notyet clear, caution must be taken since excessive cool-ing could precipitate adverse effects such as hypoten-sion, cardiac arrhythmias, or infections.' Nonetheless,pilot studies suggest hypothermia might prove feasiblefor acute stroke.'*'' Furthermore, after applying hy-pothermia and IV magnesium in animal experiments,Meloni et al suggest concomitant use of both interven-tions in patients should improve the overall neuropro-tective outcome.-^^
Page 18

Alternative Medicine Review Volume 14, Number 1 2009
Post-Str^e Recovery
Other Possible NeuroprotectantsOther candidates ior neuroprotection men-
tioned in the AHA/ASA Guideline include manni-tol, a safe agent for which the data is still inconclusive;ccrcbrolysin, which one small study found is safe andmight improve outcomes;^' and erythropoietin, whichis discussed in a later section on hematopoietie growthfactors.
The Acute Phase and Beyond:Hyperbaric Oxygen Therapy
Originally developed as a treatment for the"bends" in divers and later applied to carbon monoxide-poisoned patients and to wound healing, hyperbaric oxy-gen therapy (HBOT) involves bathing the individual in100-percent oxygen at greater than normal atmosphericpressure {for references to the early literature, see Neu-bauer 1980'**). This causes additional oxygen to dissolvein tbe blood, thereby increasing the amount of oxygenavailable to the cells - particularly brain cells in the caseof stroke. HBOT can he safely instigated in acute strokepatients within hours after stroke onset. Despite con-trolled trials and hundreds of published case series andindividual reports, HBOT remains outside the main-stream of medical stroke management.
The quality of the research on HBOT is spotty.In 2005 Carson et al evaluated four RCTs and anothertrial of HBOT for stroke.-'' While they concluded thebest evidence showed no benefit, they also concludedthat because of the stage of patients enrolled (acute,subacure, or chronic), the documentation of type andseverity of stroke, and considerably varying dosages ofHBOT, the negative results could not be generally as-sumed and further good quality studies were needed.Veteran HBOT investigators agree.^"'"'
In 2003 Rogatsky et al analyzed dosing pat-terns in clinical reports on HBOT for acute IS datingback to 1969 (total, 265 patients).'' A total dose coef-ficient was developed and compared against the trial'sefficacy, defined as improvement in percentage of pa-tients up to 100 percent. The dose coeifident was cal-culated as the product of partial oxygen pressure (ATA,'atmospheres absolute units of the intrabarochamberpressure of oxygen") x time of exposure (hours) x num-ber of exposures. A dose coefficient of 1.0 would be aUnit Medical Dose (UMD). For 14 patients classified
as acute in the 1995 Nighoghossían study (a study thatfailed to find efficacy),'- they calculated (1.5 ATA x 0.65hour X 10.0 average exposures) and arrived at a UMDvalue of 9.7. After calculating UMD values for 10 otherstudies the researchers found a close correlation (0.92)between level of efficacy and UMD value and deter-mined a threshold of 30-32 UMD for 100-percent ef-ficacy - the minimum UMD of HBOT at which allpatients should derive benefit.
The Rogatsky dose-efficacy correlation helpsexplain why some HBOT regimens failed to show ef-ficacy in acute ischémie stioke." In addition to theNighoghossian study," seven of 10 other studies below30 UMD failed to reach 100-percent efficacy. The re-searchers also suggested that a total dose of 2-3 UMDper day should not result in undue toxicity.
Rockswold et al published an extensive 2007literature review of HBOT for traumatic brain injury(TBI).'" Citing 95 references, extensive evidence ofHBOT efficacy, its met:hanism(s) of action, and safetyare reviewed, and the design of planned RCTs on se-vere TBI patients is described. Although not directlypertinent to stroke, this review does provide additionalrationale for applying HBOT to stroke rehabilitation.The most likely mechanisms of HBOT s apparent ben-efits for TBI logically apply to ischémie stroke - im-proved mitochondrial function and improved oxygenutilization leading to enhanced cerebral metabolism.
Rockswold asserts that placing severely brain-injured patients in a hyperbaric oxygen chamber at 1.5ATA for 60 minutes is a very low-risk procedure, provento be free of potential brain or lung damage. This corre-sponds to a UMD of 1.5; therefore, to attain 32.0 totalUMD at this exposure rate, 21 exposures are required,approximately the minimum number of exposuressuggested by most experienced operators. The experi-ence of one high-volume clinic with hundreds of strokeand other brain-injured patients suggests hundreds ofexposures per year at 1.25-1.75 UMD are safe and ef-ficacious.'* According to the International HyperbaricMedicine Association, in the United States HBOT isdelivered 10,000 times each day at 800 locations.''
As suggested by its apparent success for TBI,'"HBOT has considerable potential for stroke rehabilita-tion. In 1990 Neubauer et al used HBOT to reactivatewhat they termed "idling neurons" in the penumbral
Page 19
Reviev|ArticleAlternative Medicine Review Volume 14, Number 1 2009
zone of a right parietal lobe infatction in a 60-year-old woman who had a stroke 14 yeats earliet.^^ Theyused Single Photon Emission Computed Tomography(SPECT) imaging to document this and otber HBOTrecoveries.^' Whether significant improvement is pos-sible for every stroke patient remains to be convincinglydemonstrated. However, advances in neurobiologysince 1990 indicate the brain's plasticity or capacity toadapt bas been underestimated, even in advanced ageand with severe injury.'^
Preventing Stroke Recurrence byManaging Risk Factors
For the stroke patient who survives the acutephase, secondaty stroke prevention (stroke reoccur-rence) is essential in order to restore brain function.Identifying and managing the risk factors for stroke cancontribute to this goal.
As detailed by the AHA/ASA Guideline,^"risk factors for secondary stroke prevention overlapthose for primary prevention. In the case of certain riskfactors - hypertension, diabetes, elevated cholesteroland triglycérides, smoking, heavy drinking, obesity, lackof exercise - effective management is relatively wellestablisbed' and bears no detailed examination here.Other factors are more technically challenging but wellrecognized - symptomatic intracranial atherosclerosis,atrial fibrillation, and heart disease, for example.^ Otherrisk factors for stroke recurrence are newly validatedand require discussion. One tbat is bighly predictive ofstroke recurrence is C-reactive protein (CRP), an in-flammatory biomarker.
C'Reactive Protein and Stroke RiskMuch, if not all, of the brain damage caused
by stroke is a consequence of inflammation. CRP, an"acute-pbase protein" is produced mainly in tbe liver,circulates in the blood, and is reflective of inflammation.As a thoroughly validated biomarker fot cardiovascularhealth, it serves as a sensitive predictor of stroke risk.'**
Tlie advent of a highly sensitive blood test forCRP (hs-CRP)'^ was tbe technical breaktbrougb nec-essary to make CRP measurement routine. The hs-CRP test bas sufficient precision to allow for correla-tion witb cardiovascular and cerebrovascular disease
risk. The power of the bs-CRP blomarkct to predictadverse cardiovascular events (myocardial iniarction,revascularization intervention, sudden death, or stroke)is now judged stronger than any of the cbolestetol mea-
CRP is produced in response to stimulation bytbe"pro-infîammatory" cytokine interleukin-6 (IL-6).''"CRP levels accurately predict the risk of first stroke aswell as risk for stroke recurrence.'"" In a 1999 study,hs-CRP level >10.1 mg/L witbin 72 hours of strokepredicted increased mortality over the ensuing fouryears."*̂ Another study determined that bs-CRP level>15 nig/L at discharge was significantly associatedwitb occurrence of a new "vascular event" or death atone year (95% confidence interval, 2.8-20.0). For thosein the bigbest tertile of CRP tbe risk of an event withinone yeat is 55 percent.'" In a 2003 study, those in tbehighest quintile of CRP, measured at least tbree monthsafter the first iscbemic stroke or TIA, bad significantlyincreased risk of subsequent stroke.'' The strong powerof blood CRP levels to predict stroke is consistent withsttoke having a major inflammatory component.'"'"'*^
Monitoring conventional risk factors sucb ascbolesterol remains valuable, although half of all heartattacks and strokes in the United States occur in peoplewho do not have abnormal cbolesterol or triglycéridelevels.''̂ An in-hospital study of 231 consecutive mid-dle-aged IS cases found CRP measured at admissionstrongly predicted survival over eight days' bospitaliza-tion.''' The threshold for increased risk was bs-CRPabove 18 mg/L; for eacb additional 1 mg/L elevationthe risk of deatb increased 20 percent (95% confidenceinterval, 1.09-1.30; p<0.001). Thus CRPs predictivepower offers a valuable option for tracking mortalityfrom acute stroke, as well as risk of recurrent stroke (orotber adverse cerebrovascular or cardiovascular events).
The Importance of Inflammation in StrokeInflammation is an endogenous protective
mechanism by wbicb immune cells wall on tbe dam-aged brain tissue from surrounding uninjured zones,destroy dead or mortally injured cells, and repair the ex-tracellular matrix.'' All tbe brains cell types, includingmicroglia (macrophages resident in brain tissue), astro-cytes, neurons, oligodendrocytes, and endotbelial cells,participate in inflammatory responses.
Page 20

Altemative Medicine Review Volume 14, Number 1 2009
Post-Strgke Recovery
Inflammation is normally a beneficial, self-limiting process that is active just long enough to sta-bilize the damaged zone and initiate a subsequent heal-ing process. Although a stroke event invariably initiatesinflammation, where the ischémie insult is severe theinflammatory response can be so substantial that itproves difficult to terminate.''^ Inflammatory cascadesof oxidaiits, eicosanoids, cytokines, and chemokines areinitiated witb tbe onset of the ischémie insult. Tlieseeffect the local inflammatory response and induce im-mune cells to migrate from outside the brain. Normallythis integrated immune-inflammatory process bringsthe damage under control and triggers inflammationresolution.
Resolution of inflammation is a poorly un-derstood yet crucial issue for stroke outcome. Braintissue is not particularly well equipped with antioxi-dant defenses, so reactive oxygen species and other freeradicals/oxidants that exude from inflammatory cellsthreaten tissue viability in the vicinity ot the damagezone. For this immunologically aggressive phase to endadditional mediators must be produced to calm theactivated cells. The events that trigger this switch arepoorly understood, but certain key mediators have beenidentified, the best studied ot which are the omega-3metabolites.'"'
Long-chain OmegaSs Help Control BrainInflammation
The molecules that mediate inflammation arederived largely from long-chain fatty acids (LCFAs),especially arachidonic acid (AA) (C20:4, omega-6),eicosapentaenoic acid (EPA) (C20:5, omega-3), anddocosahexaenoic acid (DHA) (C22:6, omega-3).'"' Thefunctional localisation of these LCFAs is within thecell membrane system.^'' They are covalently bondedto phospholipid molecules, which constitute tbe bulkof the cell membranes lipid bilayer. From this positionLCFAs can be catabolizcd to produce smaller messen-ger molecules that either amplify immune or down-reg-ul.ite cell activity.
Tlie omega-6 AA and the omega-3s DHA andEPA have difiering influences on inflammation. AAtends to yield metabolites that amplify the inflamma-tory response, while DHA and EPA favor resolutionof inflammation. Higher levels of DHA and EPA inmembranes also down-regulate the protein cytokine
messengers, probably through down-regulation at thegene level. Dietary intake raises omega-3 levels withinbrain cell membranes and creates a biochemical tiltaway from AA metabolites. Dietary DHA also may up-regulate antioxidant defenses.''"
New research on DHA has generated find-ings that clarify how it protects against inflammation.DHA is metabolized to substances known as resolvins,protectins, and neuroprotectins. As their names imply,these are the most potent LCFA metabolites for pro-moting inflammation resolution and protecting braintissue from further damage through other degradativemechanisms."'^ '''•̂ ' Considering the typical Western dietgreatly favors AA over DHA and EPA intakes, it wouldseem prudent to ensure the stroke patient has adequateintake ot these oniega-3 fatty acids, once the possibil-ity ot stroke-related hemorrhage in tbe brain has beenruled out.
Krill "Oil" Modulates Inflammation andC'Reactive Protein
Krill is a shrimp-like crustacean that thrives inthe frigid ocean waters off Antarctica. Krill can managethis hostile environment partly because their cell mem-branes have a high concentration ot long-chain omega-3fatty acids.^^ The multiple carbon-carbon double bondsin these omega-3s (six in DHA, five in EPA) contrib-ute electron mobility that makes krill cell membranesvery fîuid and therefore better able to resist very coldtemperatures. DHA and EPA are anchored in the krillmembranes exclusively via phospholipids, aptly termedomega-3 phospholipids (for details, see Kidd, 2007''*).
Antarctic krill {Euphausia superba) can beprocessed to yield an "oil" that is mostly a complex ofomega-3 (DHA and EPA) phospholipids and tbe caro-tenoid astaxanthin, responsible tor its red color. Someomega-3 triglycérides are also present. Each of thesekrill oil constituents has anti-inflammatory actions. Inrandomized, controlled trials, krill oil demonstratedimproved lipid profiles, '"' down-regulated inflammationsymptoms,^* and lowered CRP.'''* The vital lipids foundin krill oil can be considered a "next-generation" ome-ga-3 dietary supplement, one with benefits that encom-pass but overarch those offish oil. By down-regulatingpro-inflammatory gene activity, dietary DHA and EPAalso belp down-regulate interlcukin-1 (IL-l),a cytokinethat can promote brain inflammation.
Page 21

article
Alternative Medicine Review Volume 14, Number 1 2009
Interleukin-l and Brain InflammationCytokines are small protein messenger mole-
cules, the most studied for stroke being IL-1, an impor-tant mediator of the acute phase of brain inflammation.It is very low in the healthy brain, but rapidly becomesup-regulated when the brain is subjected ro ischemia,hypoxia, trauma, or other inflammatory stimuli.^^ In ro-dents, within minutes after the brain is made ischémie,IL-1 release begins, first from the microglia then fromthe other cell types. As IL-1 rises, neuron death mark-edly accelerates.** Conversely, deletion of the genes thatcode for IL-1 reduces brain damage by 80 percent.^'
For acute ischémie stroke patients, abnormalIL-1 elevation has negative clinical impact. Patients whohave increased blood levels of messenger RNA for IL-1tend to have a worse neurological outcome.^^ ^'g^^ '^^^'culating IL-1 in turn elevates circulating IL-6, chemo-kines, and other acute phase inflammatory mediatorsalso associated with poor stroke prognosis.^*
Several approaches are under investigationfor managing IL-1 in stroke. IL-1 acts via membranereceptors (IL-IR), which can be blocked by a receptorantagonist (IL-IRA). In a randomized trial for acutestroke IL-lRA readily crossed the blood-brain barrier,was safe to use, and seemed to afford some benefit, par-ticularly for patients with cortical infarcts.̂ **
Homocysteine, Independent Risk Factor forStroke Recurrence
Homocysteine (Hey) is a sulfur-containing,thiol amino acid with a sulfhydryl group, generatedmainly from the metabolism of methionine and homeo-statically regulated by enzymes that rely mainly on vita-mins B ,̂ B,^, and folie acid as essential cofactors. Multi-pie epidemiological studies in the United States, Europe,and Japan link high circulating Hey to increased risk forstroke.^"^^ However, prospective clinical trials that usedfolie aeid and vitamins B^ and B^̂ to lower Hey did notfind lowered stroke risk. This has led to controversy asto whether Hey actually can eause stroke,''* *"' with someinvestigators eontending the epidemiological links maybe artifactual.
The first linkage of Hey with stroke came fromobservations that individuals with genetic inabilitiesto metabolize Hey had very high urine levels (homo-eystinuria) and manifested eireulatory damage early in
life; about a dozen sueh inborn defeets areIn 1962 McCully suggested even moderately elevatedplasma Hey might aeeelerate atheroselerosis.^ Subse-quent reports in the New England Jourmil of Medicinedocumented that one-third of patients with prema-ture atherosclerosis showed elevated urine Hcy,*̂ '' and42 percent of patients with premature vascular diseaseshowed elevated plasma Hey.'''*
Advancing age, vitamin deficiencies, renal fail-ure, and a number of pharmaceutical drugs can raiseplasma Hey (for referenees see Spenee*" )̂. There aremany plausible meehanisms by whieh elevated circula-ting Hey could cause vascular damage. Elevated plasmatotal homocysteine (tHcy) is associated with abnormalelevations in oxidative stress, blood coagulability, andcholesterol synthesis; abnormally reduced HDL-eho-lesterol; and impaired endothelial function. '̂*'*' '''' Theseand perhaps other obscure meehanisms help explainwhy elevated plasma tHcy may increase the risk forstroke.
Seientifie consensus as to terminology is asfollows. Plasma tHcy is a complex mix of free homo-cysteines (fHey) and boimd homoeysteincs (bHcy).The fHey includes the thiol-reduced homoeysteine, thefree homoeysteine, and various free mixed dísulfides ofhomoeysteine with eysteine and other thiols. Tlie bHeyis almost all bound to proteins, espeeially albumins.'^"
B Vitamins^ Homocysteine, and Stroke RiskIn prospeetive RCTs, B vitamin stipplementa-
tion (folie acid + vitamin B,^ + vitamin BJ that redueed> 12 t i '
plasma tHcy levels did not reduce stroke incidence.'''''"^But case-control and other population studies of pa-tients with vascular disease show tHey is a strong,graded, and independent predietor of cardiovascularevents, including s t roke . ' ' ' Plasma tHcy above 10.2micromol/L was associated with two-fold greater riskof stroke,'' and above 20 micromol/L with a nine-foldincrease in risk.'' The Hordaland Homoeysteine Study,whieh traeked 18,000 men and women for five years,found that individuals with elevated tHey at baselinewere at heightened risk ot morbidity, eognitive decline,and death during that subsequent five-year period.''Spenee critieally reviewed these data in an attempt toreeoncile this apparent paradox.^'
Page 22

Alternative Medicine Review Volume 14, Number 1 2009
Post^Strgke Recovery
Figure 1, Effect of Vitamin Therapy to Lower Homocysteine on Risk of Stroke in theHOPE-2 Trial
5 -
c * _|0) 3 -
re0.
2 -
Placebo
Folie acid andvitamins Be and B12
NumberPlaceboFolate
u -|0
at Risk27582764
11
26852670
12
25582561
13
Years
24412439
14
I
23242312
10261044
From: Spence J. Homocysteine-lowering therapy: a role in stroke prevention? Lancet Neurology 2007;6:830-838. Reprinted with permission from Elsevier. Copyright 2007.
In the Heart Outcomes Prevention Evaluation2 (HOPE-2) study/' tbe combination of folie acid (2.5mg/day), vitamin B̂^ (50 mg/day), and vitamin B,^ (1mg/day) versus a placebo for an average of five yearsfailed to reduce cardiovascular death. However, the trialdid show a significant reduction in stroke risk (relativerisk 0.75; 95% confidence interval, 0.59-0.97; p=0.03).'I"he investigators attribute this finding to chance be-cause they could not find a biological explanation forhow stroke could benefit from B vitamin therapy whenother vascular diseases seemingly did not. Spence dis-agrees, contending this finding is likely real because thebrain is more susceptible to thrombotic accident thanthe heart.^^
Spence*"' argues that, whereas most myocar-dial infarctions are due to plaque rupture in a coronaryartery, usually creating an in situ thrombosis, cerebralinfarcts (ischémie strokes) occur most often from dis-
tant embolisms transported to the site/** To supportthis case he also notes high tHcy quadruples the riskof stroke from atrial fibrillatioti,''' one source of distantembolism.
To emphasize his point, Spence reproduces afigure from the HOPE-2 trial showing the relative riskof stroke between the vitamin-treated and the placebogroup diverging steadily with time (Figure 1). Spencemakes a persuasive case that if these two lines were sta-tistically inseparable or otherwise due to chance, theyshould criss-cross or remain close together rather thanunerringly diverge.
IVitamin B ,̂: A Possible Key to theHomocysteine Paradox
In the Vitamin Ititervention for Stroke Pre-vention (VISP) trial/"^ 3,680 patients who had experi-enced a non-disabling ischcmic stroke were randomly
Page 23

Alternative Medicine Review Volume 14, Number 1 2009
Revievi^rticle
assigned to two groups. Both groups received the samemultiple-vitamin preparation, which supplied the FDArecommended daily intakes of the other vitamins butwas lacking in folie acid, vitamin B ,̂ and vitamin B .The low-dose group received in addition, 20 meg/dayfolie acid, 200 meg/day vitamin B^ (as pyridoxine), and6 meg/day vitamin Bi .̂ The high-dose group received2.5 mg/day folie aeid, 25 mg/day vitamin B ,̂ and 400meg/day vitamin B^,. At the end of the two-year trialneither group showed signifieant reduction in strokereeurrenee. Spenee asserts the negative trial outcomecould be due to the B|,"high" dose being too low. Ac-cording to Spenee, one of the VISP trial investigators,many patients, ineluding some in the high-dose group,had very low baseline serum B^, levels. All were peri-odically tested, and those found to have low serum Bwere given monthly B^, injections. Spenee suggests thisdefeated the purpose of the study - to have a low-doseB vitamin control group. His group recalculated theVISP data, excluding patients who received vitaminB|^ injections and some others with kidney problemsknown to be less likely to respond to vitamin therapy.The data from 2,155 participants showed the high-dosevitamin therapy significantly redueed stroke, eoronaryevents, and death compared with the low-dose group.This re-analysis demonstrates rhat those patients whocould absorb vitamin B^, (from a baseline B level at orabove 322 picomol/L) and who received the "high-dose"combination, experienced one-third fewer strokes thanthe low-dose vitamin group.
Folie Add Monotherapy Reduces Stroke RiskBased on rhe methyl cycle rationale that fo-
late is the major metabolic recycler of homocysteine tomethionine,"' a number of RCTs and other less well-eontroUed trials have tested folie aeid as a monotherapyfor stroke prevention. The most recently published me-ta-analysis concludes folate is effective for stroke. Analy-sis of eight RCTs demonstrated a sratistieally significant18-percent reduction in stroke risk (relative risk 0.82;95% eonfidenee interval, 0.68-1.0; p^O.045).'^ Trialsthat went longer than three years shewed a markedlygreater risk reduetion of 29 percent (p^O.OOl). A eor-relation between the degree of homoeysteine reductionand the amount of stroke risk reduetion was also seen;trials with greater Hey reduction showed greater strokerisk reduetion. I
Despite the faet that tbiate alone reduces strokerisk, a combination of B vitamins is probably the betterapproach for three reasons. First, there are multiple rolesfor folate in one-carbon metabolism, which suggest itssupply could become limiting to metabolism;"' second,vitamin B̂ ^ is an essential eofaetor for the remethylationof Hey to methionine by folate;"' and third, Spenee's cri-tique of the VISP trial suggests a likely role for vitaminB̂ ^ in lowering stroke risk.*'' Hence, using folie acid incombination with vitamin B^, may be superior to folieaeid alone for stroke prevention.
Nutrients for Recovery After the AcutePhase
Only two nutrients have been clearly estab-lished for stroke recovery after the acute phase - citico-line and glycerophosphoeholine.
CiticolineCitieoline (also called cytidine diphosphate
eholine, cytidine diphosphocholine, CDP-eholine) is anueleotide and an energy-activated form of the essentialnutrient eholine. Citieoline eonsists of eholine linked tocytidine by a diphosphate bridge. Citieoline is well ab-sorbed when taken by mouth,'^ and following absorp-tion into the intestinal endothelium it is hydrolyzed toeholine and cytidine, which enter the circulation andcross the blood-brain barrier.''^ Citicoline as a dietarysupplement has been investigated for hemorrhagiestroke in a small pilot study, with nonsignifieant out-come;«" and for aeute IS in four RCTs.«'**^
A 2002 meta-analysis**' analyzed the data fromthe four RCTs on oral citicoline for aeute IS."' "' Allwere performed in the United States and used variousdoses of oral citicoline (500, 1,000, or 2,000 mg perday) or placebo. In all eases, citicoline was begun within24 hours afirer stroke onset, dosing ended at six weeks,and efficacy analysis was performed at three months. Tobe included in the meta-analysis, patients had to be 18or older and have had a mode rate-to-severe stroke (mildstroke was Judged likely to spontaneously recover andmask any response to eitieoline). The final patient totalwas 1,372; 789 on eiticoline and 583 on placebo. Citi-eoline was assoeiated with a significantly greater globalrecovery at three months (odds ratio, 1.33; 95% confi-dence interval, 1.10-1.62; p=0.0034).
Page 24

Alternative Medicine Review Volume 14, Number 1 2009
Post-Strgke Recovery
Global recovery was defined as any degreeof recovery on tbree separate assessment scales - tbemNIHSS, tbe flinctional BI, and the global mRS.Global recovery was achieved by 25.2 percent of patientson citicoline compared witb 20.2 percent of patients onplacebo. Tlic highest favorable response was obtained attbe highest dose of 2,000 mg/day.
In tbis meta-analysis, citicoline wben com-pared to placebo at three months significantly improvedtbe piobability to recover activities of daily living by 29percent and tbe probability to recover functional ca-pacity by 42 percent, but tbe increase in neurologicalrecovery was not significant.*''' Citicoline bad no effecton tbree-montb survival; its significant adverse effectsincluded increased anxiety and leg edema. Tbe investi-gators concluded,'Although the capacity of citicoline torescue iscbemic tissue may be limited, its safety profilelikely provides a favorable risk-to-benefit ratio.... A newtrial to confirm tbese results should be conducted.' Alarge, multicenrer RCT of citicoline for acute ischémiestroke is now underway.^
GlycerophosphocholineLike citicoline, glyceropbospliocboline (GPC,
alpha-GPC, cboline alfoscerate, cboline alphoscerate) isalso a well absorbed and bigbly bioavailable source ofcboline. GPC bas been administered to almost 3,000stroke patients in five stroke trials." '"
Eacb GPC stroke trial used the same protocol.Patients were started within 10 days after stroke on-set. Tlie trials consisted of two phases; during tbe firstpbase of 28 days, generally in bospital, GPC was givenintramuscularly at 1,000 mg/day. During the secondpbase, from day 29 to day 180, GPC was given orallyat 1,200 mg/day (400 mg three times daily), l l ie singlelargest multicenter trial was conducted at 176 centers inItaly and included 2,044 patients."" During phase 1, thepatients medical history was taken, physical and neuro-logical examinations conducted, and level of conscious-ness graded via tbe Mathew Scale (0-100, witb 0 beingclinical death and 100 being perfect consciousness).^"Tbose too unconscious to be evaluated were excluded(Mathew Scale score <35). In pbase 2, tbe Mini-MentalState Examination (MMSE) was used to evaluate cog-nitive function, and tbe Crichton Geriatric Rating Scale(CGRS) and the Global Deterioration Scale (GDS)
were used to evaluate overall deterioration (see Bar-bagallo Sangiorgi et al"̂ for references).
At the end of the six-montb trial, using tbepatients as tbeir own controls, the Investigators foundGPC significantly belped more tban 95 percent of pa-tients, and witbout serious adverse effects. In pbase 1the Matbew Scale score improved an average of 15.9points (p<0.001). Tbe MMSE was significantly im-proved at day 90 (p<0.001), then futtber at day 180(p<0.001). Both the CGRS and GDS deteriorationscores were significantly improved at day 180 (p<0.001for both scales). Overall, GPC was judged by 78 percentof investigators as'Very good'or"good,'by 17 percent as"moderate," and by five percent as having "poor" or 'no"efficacy.
Parnetti'^' performed a meta-analysis of tbethree stroke trials completed up to 2001''^*'"'" as part ofa broader assessment ot GPC for neurological diseases.Sbe concludes all tbrcc trials produced similar results;GPC improved ischémie stroke recovery by a "clinicallyrelevant" 20-30 percent in tbe first pbase, and tbe secondpbase produced additional, clinically relevant improve-ments of 12-21 percent assessed by MMSE, CGRS,and GDS scales.
Cardiac bypass and other open-beatt surgeryresults in as mucb as a 50-pcrcent risk for memory lossand other cognitive brain damage. Some patients re-cover witbin days or weeks, others suffer permanent dis-ability. In a double-blind trial, 20 recovering open-heartpatients were randomized to receive GPC intravenouslyat 1,000 mg/day for one month, tben intramuscularlyat 1,000 mg/day for another five months or placebo."*"̂Neuropsychological testing using tbe Wechsler Memo-ry Scale determined GPC slowed memory deteriorationsignificantly over placebo after one montb (p<0.05).GPC also improved memory over tbe subsequent fivemonths while the placebo group experienced ongoingmemory decline (p<0.05).
GPC bas potent neuroprotective properties.Tbe most relevant to stroke are findings from a rat brainischemia model, in wbicb GPC given after arterial oc-clusion surgery protected ilie ischémie zone almostcompletely from damage.^^ GPC's degree of protec-tion surpassed cerebrolysin, piracetam, and vinpocetinein this IS model. GPC is a unique osmotic protectant,especially against urea buildup'"' and demonstratestropbic activity via conservation of brain nerve growth
Page 25

Revievi^rticle
Alternative Medicine Review Voiume 14, Number 1 2009
factor receptor density.^^ GPC is used in Europe to treathead trauma and other acute brain injuries in addition
to
Brain Regenerative Capacity: A Changein Perspective
Until recently, researchers in the field of strokerehabilitation have been pessimistic, limited in theirperspective by the prevailing scientific dogma. Thisdogma maintained that the human brain has very lim-ited capacity to recover from structural and tunctionaldamage; therefore, stroke rehabilitation could merelyhope to salvage damaged circuits that were still struc-turally intact. Tlie patient was expected to adjust to liv-ing without the functions lost to stroke. As basic andclinical research spanning the last three decades beganoverturning this dogma, stroke rehabilitation entered anew, far more optimistic era.
Neurobiology researchers found the humanbrain cortex has anatomically identifiable sensory andmotor ('sensorimotor ) zones that manage the limb andother body functions. At first these nerve circuits werethought to be very specific for each zone, but now it isclear these brain zone "maps" are actually quite change-able. Elegant experiments were done in which a zonewas knocked out by a mechanical or chemical lesion orinputs to a zone were changed from the sensory inputsource, and it was found when one zone is removed fromaction often an adjoining zone can substitute,"^" resultingin broader usage of the concept ofneuroplasticity/"^'
Brain Plasticity Regenerates Lost FunctionThe scientific dogma that held the central ner-
vous system was not capable of regeneration was at-tributed to a very limited capacity for generating newcells,'""'̂ *" the presence in the tissue ot active inhibitorsof regeneration,'""^ and tbe scarring seen to ensue follow-ing damage.'"^'"' In 1998 conclusive evidence emergedthat the adult human brain makes new nerve cells.""'These new cells can he induced to become functional.This breakthrough, combined with the steadily accu-mulating evidence of adaptability of established senso-rimotor circuits, means the human brain can function-ally regenerate enough to improve quality of life.
Brain plasticity refers to the brains lifelong ca-pacity for physical and functional change. This capacityexplains how experience induces learning throughoutlife.**'-̂ '̂ Over the last quarter century, pioneering plas-ticity researcher Michael Merzenicb spent mucb ot hisearly career in rhe laboratory placing tiny electrodesin brain neurons. What he found opened a new era inneurobiology; i.e., the brain's cortex is adaptable andchangeable in response to manipulation of stimuli tromthe outside.'* '̂**
By performing painstaking cortical mappingexperiments, Merzenich et al documented the hu-man brain cortex has a highly dynamic structural andfunctional topography. Neuron networks in fiinction-al zones continually adjust tunctional commitmentswhen adapting to incoming intormation.''"*'*'' A classicexample is wben two adjacent fingers of a monkey aretaped together over weeks, the fingers become one fin-get tunctionally; i.e., one functional unit for cortical"soniatosensory area 3b."'""̂ Tlie model appears to bethat neurons receiving more stimulation make moreconnections, while neurons receiving less or no stimula-tion lose connections, sometimes becoming structurallyatrophied. Cortical nerve network adaptability is likelythe mechanism for the neuroplasticity that underliesstroke rehabilitation.'''^
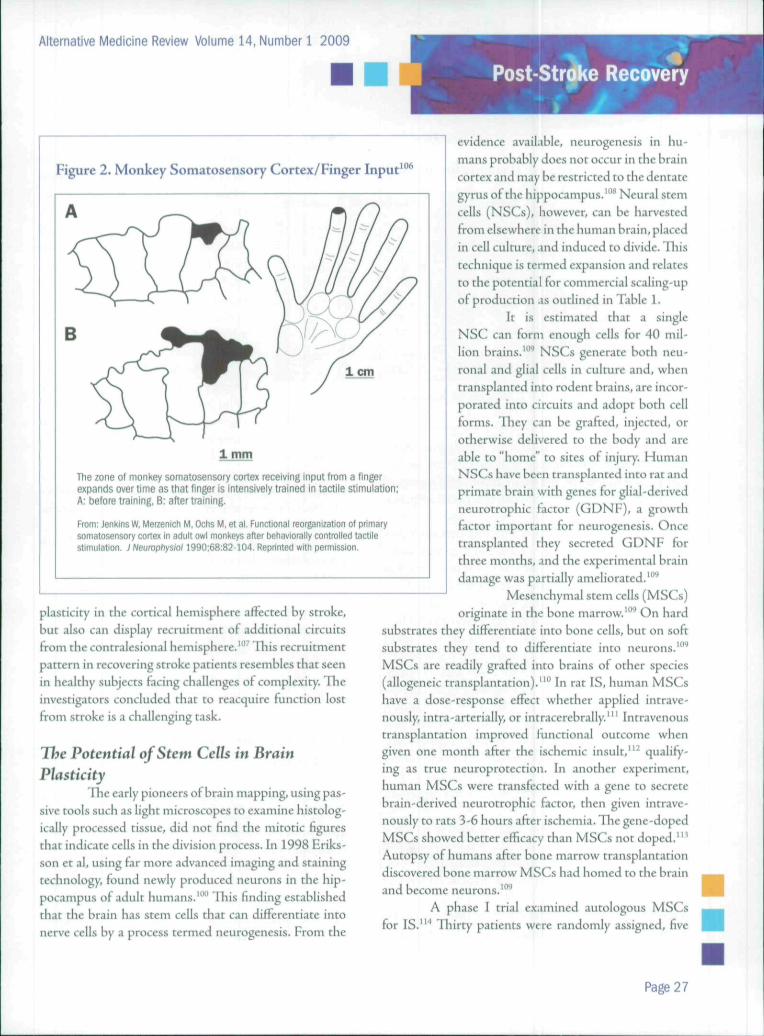
Researchers mapped the somatosensory cortexof two monkey species, training the monkeys in fingerretrieval of small objects (Figure 2).'"^'* Xerri identi-fied the brain area associated with input to the fingersas cortical somatosensory area 3b. By creating micro-lesions in area 3b, essentially mini-strokes localized tothe most functional zones of area 3b, the monkeys lostretrieval skills. Tlie monkeys were retrained and overseveral weeks to months reacquired the fine somatosen-sory skills. When area 3b was remapped the researchersfound new zones of area 3b bad become involved. A newlink had emerged in adjoining area 3a and further away,area 1 had doubled its zone of responsibility for fingers.Xerri concluded this was an example of cortical "substi-tution" and "adaptive plasticity" in recovery from stroke.
Tlie monkeys did not show adaptive plasticity Inthe opposite ("contralateral") brain hemisphere, perhapsbecause the lesions were tiny and highly localized. So-phisticated Positron Emission Tomography (PET) andelectroencephalogram (EEG) monitoring show recov-ering stroke patients display substitution and adaptive
Page 26
Alternative Medicine Review Volume 14, Number 1 2009
Post-Strj|ke Recovery
Figure 2. Monkey Somatosensory Cortex/Finger Input106
1 cm
1 mm
The zone of monkey somatosensory cortex receiving input from a fingerexpands over time as that finger is intensively trained in tactile stimulation;A: before training, B: after training.
From: Jenkins W. Merzenich M, Ochs M, et al. Functional reorganization of primarysomatosensory cortex m adult owl monkeys after Oetiaviorally controlled tactilestimulation. ; Neurophysiol 1990;68:82-104. Reprinted with permission.
plasticity in the cortical hemisphere aifected by stroke,but also can display recruitment of additional circuitstrom the contralesional hemisphere.'"'' Tliis recruitmentpattern in recovering stroke patients resembles that seenin healthy subjeets faeing ehallenges of complexity. Theinvestigators concluded that to reaequire funetion lostfrom stroke is a challenging task.
The Potential of Stem Cells in BrainPlasticity
Ihe early pioneers of brain mapping, using pas-sive tools sueh as light microscopes to examine hiscolog-ically processed tissue, did not find the mitotic figuresthat indicate cells in the division process. In 1998 Eriks-son ct al, using far more advanced imaging and stainingtechnology, tounJ newly produced neurons in the hip-pocampus of adult humans.'"" This finding establishedthat the brain has stem cells that can differentiate intonerve cells by a process termed neurogenesis. From the
evidence available, neurogenesis in hu-mans probably does not occur in the braincortex and may be restricted to the dentategyrus of the hippocampus.""* Neural stemcells (NSCs), however, can be harvestedfrom elsewhere in the human brain, placedin cell culture, and induced to divide. Thistechnique is termed expansion and relatesto the potential for commercial scaling-upof production as outlined in Table 1.
It is estimated that a singleNSC can form enough cells for 40 mil-lion brains.'"'' NSCs generate both neu-ronal and glial cells in culture and, whentransplanted into rodent brains, are incor-porated into circuits and adopt both cellforms. They can be grafted, injeeted, orotherwise delivered to the body and areable to "home" to sites of injury. HumanNSCs have been transplanted into rat andprimate brain with genes for glial-derivedneurotrophie factor (GDNF), a growthfactor important for neurogenesis. Oncetransplanted they secreted GDNF forthree months, and the experimental braindamage was partially ameliorated.'"''
Mesenchymal stem cells (MSCs)originate in the bone marrow.'""* On hard
substrates they differentiate into bone cells, but on softsubstrates they tend to differentiate into neurons.^"^MSCs are readily grafred into brains ot other species(allogeneic transplantation)."" In rat IS, human MSCshave a dose-response effect whether applied intrave-nously, intra-arterially, or intracercbrally.'" Intravenoustransplantation improved limetional outeome whengiven one month after the isehemic insult,"' quality-ing as true neuroproteetion. In another experiment,human MSCs were transteeted with a gene to secretebrain-derived neurotrophie factor, then given intrave-nously to rats 3-6 hours after ischemia. Tlie gene-dopedMSCs showed better etficacy than MSCs not doped."'Autopsy of humans after bone marrow transplantationdiscovered bone marrow MSCs had homed to the brainand become neurons.'"''
A phase I trial examined autologous MSCsfor IS.""* Tliirty patients were randomly assigned, five
Page 27
RevieviçArticle
Alternative Medicine Review Volume 14, Number 1 2009
Table 1« Proposed Cell Therapies for Stroke «̂̂
Cell type
Mesenchyme stem celis (MSC)(autologous)
MSC ^ ^ ^ ^ H(allogeneic) ^ ^ ^ ^ ^ ^ H
Umbilical cord stem cells , f l
Adult progenitor cells
Neural stem cells „^KÎ^Ê
Safety
Excellent(Phase 1 trial) J
Very good: hostrejection possible
Very good ^ j i
Very good
Good butlargely unknown
Ethical Concerns
None
None ^ ^ ^ H
None ^ ^ ^ H
None
Minor(dependsun source)
Scalability
Poor 1
1 Excellent
1 Very good
Excelient
Moderate J
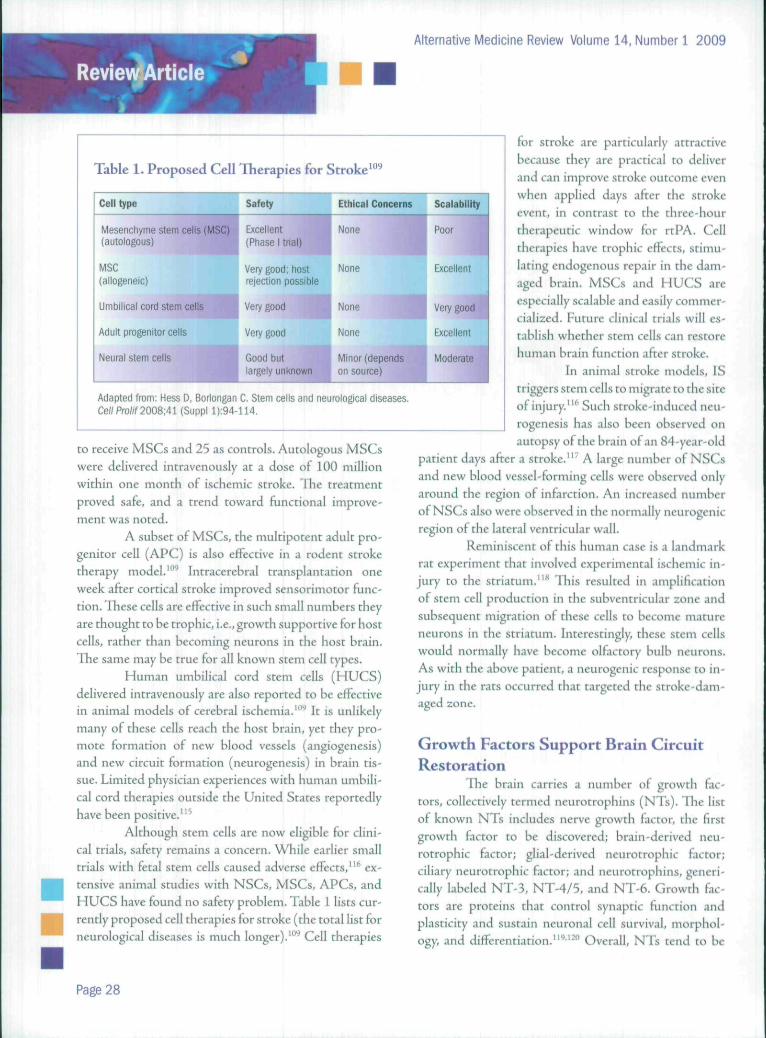
Adapted from; Hess D, Borlongan C. Stem cells and neurological diseases.Ce/iPro//f2008;41 (SuppI
to receive MSCs and 25 as controls. Autologous MSCswere delivered intravenously at a dose of 100 millionwithin one month of ischémie stroke. Tbe treatmentproved safe, and a trend toward functional improve-ment was noted.
A subset of MSCs, the multipotent adult pro-genitor cell (APC) is also effective in a rodent stroketherapy model. "̂ ^ Intracerebral transplantation oneweek after cortical stroke improved sensorimotor func-tion. These cells are effective in such small numbers theyare thought to be trophic, i.e., growth supportive for hostcells, rather than becoming neurons in the host brain.The same may be true for all known stem cell types.
Human umbilical cord stem ceils (HUCS)delivered intravenously are also reported to be effectivein animal models of cerebral ischemia.'"^ It is unlikelymany of these cells reach the host brain, yet they pro-mote formation of new blood vessels (angiogenesis)and new circuit formation (neurogenesis) in brain tis-sue. Limited physician experiences with human umbili-cal cord therapies outside the United States reportedlyhave been positive."^
Although stem cells are now eligible for clini-cal trials, safety remains a concern. While earlier smalltrials with fetal stem cells caused adverse effects,'"' ex-tensive animal studies with NSCs, MSCs, APCs, andHUCS have found no safety problem. Table 1 lists cur-rently proposed cell therapies for stroke (the total list forneurological diseases is much longer).'"'' Cell therapies
for stroke are particularly attractivebecause they arc practical to deliverand can improve stroke outcome evenwhen applied days after tbe strokeevent, in contrast to the three-hourtherapeutic window for rtPA. Celltherapies have trophic effects, stimu-lating endogenous repair in the dam-aged brain. MSCs and HUCS arcespecially scalable and easily commer-cialized. Future clinical trials will es-tablish whether stem cells can restorehuman brain fiuiction after stroke.
In animal stroke models, IStriggers stem cells to migrate to the siteof injury.'"' Such stroke-induced neu-rogenesis has also been observed onautopsy of the brain of an 84-year-old
patient days after a stroke."' A large number of NSCsand new blood vessel-forming cells were observed onlyaround the region of infarction. An increased numberof NSCs also were observed in the normally neurogenicregion of the lateral ventricular wall.
Reminiscent of this human case is a landmarkrat experiment that involved experimental ischémie in-jury to the striatum."^ This resulted in amplificationof stem cell production in the subventricular zone andsubsequent migration of these cells to become matureneurons in the striatum. Interestingly, these stem cellswould normally have become olfactory bulb neurons.As with the above patient, a neurogenic response to in-Jury in the rats occurred that targeted the stroke-dam-aged zone.
Growth Factors Support Brain CircuitRestoration
Tlie brain carries a number of growth fac-tors, collectively termed neurotrophins (NTs). The listof known NTs includes nerve growth factor, the firstgrowth factor to be discovered; brain-derived neu-rotrophic factor; glial-derived neurotrophic factor;ciliary neurotrophic factor; and neurotrophins, generi-cally labeled NT-3, NT-4/5. and NT-6. Growth fac-tors are proteins that control synaptic function andplasticity and sustain neuronal cell survival, morphol-ogy, and differentiation."'''^" Overall, NTs tend to be
Page 28
Alternative Medicine Review Volume 14, Number 1 2009
Figure 3. Neurological Improvement from G-CSF in Stroke Patients
ou(A
(O
UJc0)E
0)
J G-CSF groupI Control group* p<0.05
3 6Follow-up period, months
12
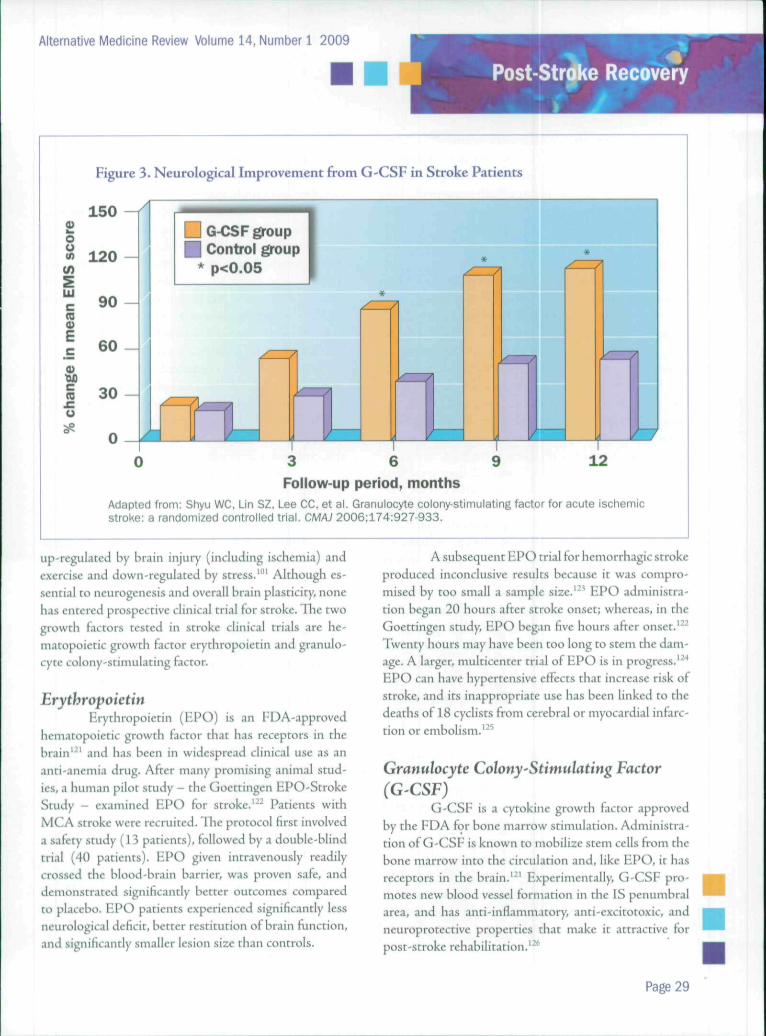
Adapted from: Shyu WC. Lin SZ, Lee CC, et al. Granulocyte colony-stimulating factor for acute ischémiestroke: a randomized controlled trial. CMAJ 2006:174:927-933.
up-regulated by brain injury (ineluding ischemia) andexercise and down-regulated by stress."" Although es-sential to neurogenesis and overall brain plasticity, nonehas entered prospective clinical trial for stroke. The twogrowth factors tested in stroke clinical trials are he-matopoietie growth factor erythropoietin and granulo-cyte colony-stimulating factor.
ErythropoietinHrythropoietin (KPO) is an FDA-approved
hematopoietie growth factor that has receptors in thebrain''^' and has been in widespread clinical use as ananti-anemia drug. After many promising animal stud-ies, a human pilot study - the Gocttingen EPO-StrokeStudy - examined EPO for stroke.'^' Patients withMCA stroke were recruited. The protocol first involveda safety study (13 patients), followed by a double-blindtrial (40 patients). EPO given intravenously readilycrossed the blood-brain barrier, was proven safe, anddemonstrated signifieantly better outcomes comparedto placebo. EPO patients experienced signifieantly lessneurological deficit, better restitution of brain funetion,and significantly smaller lesion size than controls.
A subsequent EPO trial for hemorrhagie strokeproduced inconclusive results because it was compro-mised by too small a sample size.'"* EPO administra-tion began 20 hours after stroke onset; whereas, in theGoettingen study, EPO began five hours after onset.''^'Twenty hours may have been too long to stem the dam-age. A larger, multieenter trial of EPO is in progress.'̂ "*EPO can have hypertensive efFeets that inerease risk ofstroke, and its inappropriate use has been linked to thedeaths of 18 eyelists from eerebral or myocardiai infarc-tion or embolism.'^' '
Granulocyte Colony-Stimulating Factor
(G'CSF)G-CSF is a eytokine growth factor approved
by the FDA for bone marrow stimulation. Administra-tion of G-CSF is known to mobilize stem cells from thebone marrow into the circulation and, like EPO, it hasreceptors in the brain.'"' Experimentally, G-CSF pro-motes new blood vessel formation in the IS penumbralarea, and has anti-inflammatory, anti-exeitotoxie, andneuroproteetive properties that make it attraetive forpost-stroke rehabilitation.'^^
Page 29

RevievçArticleAlternative Medicine Review Volume 14, Number 1 2009
Among stem cell researchers, two tberapeuticapproaches bave emerged.^'" The first is to transplantexogenous stem cells; the second is to amplify endo-genous stem cells. The first approach is currently lim-ited by tbe logistics (and expense) of obtaining, expand-ing, and transplanting stem cell lines, not all of wbicbmay be safe to use.'"' G-CSF use supports tbe latterstrategy.
In a small pilot RCT, Sbyu et al gave G-CSF toacute stroke patients, then followed tbeir neurologicalfimction and brain metabolic activity for 12 months.'^*Patients witb recent MCA infarction (mild-to-nioder-ate, per tbe mNIHSS) were randomized to receive thestandard of care for acute stroke, tben either G-CSF(n=7) (15 mcg/kg, subcutaneously for five consecu-tive days) or no additional treatment (n=3). Patientswere discharged after one week, then followed up every1-3 montbs for one year. Tbree of tbe G-CSF patientsexperienced headache, transient bone pain, and tran-sient liver impairment, which resolved once treatmentstopped. Leukocyte blood counts indieated G-CSF mo-bilized stem cells from the marrow to the bloodstream.
At 12 months, G-CSF patients demonstratedsignificantly greatet neurological improvement than con-trols on four scoring scales employed (Figure 3); infarctsizes remained the same. PET imaging revealed the G-CSF group bad significantly greater glucose metabolicactivity in tbe penumbral zone tban did tbe controls.Tbis increased metabolic activity correlated significant-ly witb increased neurological score on tbe EuropeanStroke Scale Motor Subscale (EMS). Tlie researchersnoted that patients started on G-CSF witbin 24 hoursafter stroke sbowed better neurological improvement.
ConclusionTime is brain. Stroke recovery ultimately de-
pends on surviving tbe acute stroke. Tbe priority in acutemanagement must be to get tbe patient to a stroke carefacility. FAST-MAG training of emergency personnelto adfninister IV magnesium in the ambulance is es-sential. An acute stroke management team sbould per-form a complete neurological and cardiovascular strokescreening within 60 minutes. Eligibility for IV rtPAor intra-arterial thrombolysis sbould be determinedas quickly as possible. Witb or without thrombolysis,neuroprotection can be implemented using albumin.
magnesium, bypothermia, bypetbaric oxygen, or otherinterventions proven safe for the acute phase. Beyondtbe acute phase, safe nutrient neuroprotectants such asciticoline and GPC can be implemented.
Caution sbould be exetcised using nutrientantioxidants during acute stroke. Antioxidants can be-come pro-oxidative in the presence of free iron, as wheniron is detacbed from hemoglobin during beniorrbagc;this may also occur to some degree during ischémiestroke. After several RCTs that failed to demonstratecardiovascular protection of vitamin H,''̂ '̂ Milman et alre-analyzed the data and concluded vitamin E may bebeneficial only for individuals with significantly higheroxidative stress. They conducted a double-blind RCTwith vitamin E (as d-alpha tocopherol, 400 IU/day) indiabetic patients witb a specific genetic susceptibility tooxidative stress."" In this trial vitamin E offered signifi-cant protection against stroke, myocardial infarction,and cardiovascular death.
When tbe post-stroke patient is stabilized,tbe stage is set for rehabilitation and brain plasticitybecomes tbe key to stroke recovery. As reviewed else-where,'̂ '' the brains processing machinery is sustainedby intensive use undet challenging conditions. Continu-ous, active interaction witb environments demanding tothe sensory, cognitive, and motor systems is necessaryto maintain brain health. Witb tbe stroked brain stabi-lized, damage processes quencbed, and zones of stiuinedcells reactivated through reperfusion, external stimula-tion can then be skillfully applied to literally remap tbebrain's cortex and fill in tbe blank functional zones.
A number of innovative physical and mentalexercise approacbes are available to help drive func-tion-driven brain restoration (see Cramer'" for a com-prehensive review). They include constraint-inducedmovement therapy (CIMT), whicb is based on the ideaof overcoming learned nonuse of the affected limb af-tet stroke. CIMT involves resttainlng tbe good limbto force the bad limb into action. A recent clinical trialproved tbat two weeks of CIMT can produce gainsthat remained two years later . '" '" Tbe CIMT conceptis also being extended to cognitive retraining.'" Braintraining ("neurobics") is showing promise. The best ofthe brain training exercises rely on the concept of brainplasticity. ' '''
Page 30
Alternative Medicine Review Volume 14, Number 1 2009
The future appears positive for stroke recov-ery based on the principles of brain plasticity. Researchinto stroke recovery will continue to overlap with otherburgeoning fields of brain restoration, such as traumaticbrain iniury and spinal cord injury. A substantial targetpopulation for brain restoration exists, including strokesurvivors, TBI survivors (including more than 320,000trom Iraq),'" spinal cord injury survivors, and millionsliving with neurodegencrative diseases.
ReferencesL Petlmuttet D, Colman C. Ihe Better Brain ßoofe. New
York, NY: fiiverhead Books (Penguin Group); 2004.2. Tliom T, Haase N, Rosamond W, er al. Heart disease
and stroke statistics - 2006 update: a report fi"om theAmerican Heart Association Statistics Committeeand Stroke Statistics Subcommittee. Circulation2aO6;lB:E85-E15L
3. Adams HPJr, del Zoppo G, Alberts Mj, et al.Guidelines tor the early management of adults withischémie stroke: a guideline from the AmericanHeart Association/American Stroke AssociationStroke Council, Clinical Cardiology Council,Cardiovascular Radiology and Intervention Council,and the Atherosclerotic Peripheral VascularDisease and Quality of Care Outcomes in ResearchInterdisciplinary Working Groups: "̂ flie AmericanAcademy of Neurology affirms the value of thisguideline as an educational tool for neurologists.Circulation 2007;l 15:H478-E534.
4. Broderick j , Brott T, Kothari R, et al. The GreaterCincinnaci/Northern Kentucky Stroke Study:preliminary first-ever and total incidence rates ofstroke among blacks. Stroke 1998:29:415-421.
5. Sacco RL, Adams R, Albers G, et al. Guidelinesfor prevention of .stroke in patients with ischémiestroke or transient ischémie attack: a statementfor healthcare professionals from the AmericanHeart Association/American Stroke AssociationCouncil on Stroke: co-sponsored by the Councilon Cardiovascular Radiology and Intervention: theAmerican Academy of Neurology affirms the value ofthis guideline. Stroke 2006;37:577-617.
6. Rothwell PM, Warlow CP. Timing of TIAs precedingstroke: rime window tor prevention is very short.Neurology 2005;64:817-820.
7. Hurtado O, Pradillo JM, Alonso-Escolano D, etal. Neurorepair versus neuroprotection In stroke.Cerehroi'iiic Dis 2006;21:54-63.
8. No authors listed. ris.sue pla.sniinogen activatortor acute Ischémie stroke. The National Institute ofNeurological Disorders and Stroke rt-PA StrokeStudy Group. N EnglJ Mc4 1995:333:1581-1587.
9. Patel SC, Levine SR, Tilley BC, et al. Lack of clinicalsignificance of early Ischémie changes on computedtomography In acute stroke.JAMA 2001;286:2830-2838.
10. Alexandrov AV, GrottaJC. Arterial reocclusionin stroke patients treated with intravenous tissueplasminogen activator. Neurology 2002:59:862-867.
11. Choi jH, Bateman BT, Mangla S,et al. Hndovascularrecanalization therapy in acute ischémie stroke. Stroke2006:37:419-424.
12. Smith WS, Sung G, Starkman S, er al. Safetyand efficacy of mechanical embolectomy in acuteischémie stroke: results of the MERCI trial. Stroke2005;36:1432-1438.
13. Olsen TS, Larsen B, Herning M, et al. Blood flow andvascular reactivity in collaterally perfiised brain tissue.Evidence ot an ischémie penumbra in patients withacute stroke. Stroke 1983;14:332-34L
14. GrottaJC. Acute stroke therapy at the millennium:consummating the marriage between the laboratoryand bedside. Tlie Feinberg lecture. Stroke1999;30:1722-1728.
15. Shin DH, Moon GJ, Bang OY. Albumin therapy inacute stroke patients.J Neurol 2007;254:870-878.
16. Suarez Jl, Shannon L, Zaidat OO, et al. Effect ofhuman albumin administration on elinieal outcomeand hospital cost in patients with subarachnoidhemorrhage.J Ncurosurg_ 2004;100:585-590.
17. Belayev L, Liu Y, Zhao W, et al. Human .ilbumintherapy of acute ischémie stroke; markedneuroprotective efficacy it moderate doses and with abroad therapeutic window. Stroke 2001:32:553-560.
18. Meyer BC, Hemmen TM, Jackson CM, Lyden PD.Modified National Instimtes of Health Stroke Scalefor use in stroke clinical trials: prospective reliabilityand validity. Sírofeí-2002:33:1261-1266.
19. Wayner DD, Burton GW, Ingold KU Locke S.Quantitative measurement of the total, peroxylradical-trapping antioxidant eapabiliry of humanblood plasma by controlled peroxidation. Iheimportant contribution made by plasma proteins.F£ßSL<:(i 1985:187:33-37.
20. Tlie Field Administration of Stroke Therapy -Magnesium Phase 3 Clinical Trial. FAST-MAGScientific Background, www.fastmag.info/sci_bkg.htm [Accessed Novemlx-r 15. 2008]
21. Aslanyan S, Weir CJ, Muir KW, et al. Magnesium fortreatment ot acute lacunar stroke syndromes: furtheranalysis of the IMAGES trial. Sirofee 20G7;38:1269-1273.
22. Saver JL, Kidwell C, Eckstein M, et al. Prehospitalneuroprotective therapy for acute stroke: resultsof the Field Administration of Stroke Therapy-Magnesium (FAST-MAG) pilot trial. Stroke2004:35:E106-E108.
Page 31

Alternative Medicine Review Volume 14, Number 1 2009
23. Georgiadis D, Schwarz S, Aschoff A, Schwab S.Hemicraniectomy and moderate hypothermiain patients with severe isehemic stroke. Stroke2OO2;33:1584-1588.
24. Georgiadis D, Sehwarz S, Kollmar R, Schwab S.Endovascular cooling for moderate hypothermiain patients with acute stroke: first results of .1 novelapproach. Stroke 2001:32:2550-2553.
25. Krieger DW, De Georgia MA, Abou-Chebl A, et al.Cooling for Acute Isehemic Brain Damage (COOLAID): an open pilot study of induced hypothermia inacute isehemic stroke. Stroke 2001;32:1847-1854.
26. Meloni BP, Zhu H, Knuckey NW. Is magnesiumneuroprotective following global and focal cerebralischaemiai A review of published studies. Magncs Res2006;19:123-137.
27. Ladurner G, Kalvach P, Moessler H, CerebrolysinStudy Group. Neuroprotective treatment withcerebrolysin in patients with acute stroke: arandomised controlled trial.J Neural Transm2005:112:415-428. ¡
28. Neubauer RA, End E. Hyperbaric oxygénation asan adjunct therapy in strokes due to thrombosis. Areview of 122 patients. Stroke 1980;l 1:297-300.
29. Carson S, McDonagh M, Russman B, Helfand M.Hyperbaric oxygen therapy for stroke: a systematicreview of the evidence. Clin Rehabil 2005:19:819-833.
30. Rockswold SB, Rockswold GL, Defillo A. Hyperbaricoxygen in traumatic brain injury. Neurol Res2007:29:162-172.
31. Rogatsky GG, Shifrin EG, Mayevsky A. Optimaldosing as a necessary condition for the efficacy ofhyperbaric oxygen therapy in acute isehemic stroke: acritical review. Neurol Res 2003:25:95-98.
32. Nighoghossian N, Trouillas P, Adeleine P, SalordF. Hyperbaric oxygen in the treatment of acuteisehemic stroke. A double-blind pilot study. Stroke1995;26:1369-1372.
33. Neubauer R, Neubauer V, GerstenbiMnd F. Latetreatment of severe brain injury with hyperbaricoxygenation.J Am PÍjj/sSwr^ 2005:10:58-59.
34. International Hyperbaric Medical Association.Clinical Hyperbaric Oxygen Tlierapy FacilitiesWilting to Treat Brain Injured Service Members.www.hyperbaricmedicalassociation.org/Location[Accessed November 13, 20081
35. Neubauer RA, Gottlieb SF, Kagan RL. Enhancing"idling" neurons. Lancet 1990:335:542.
36. Doidge N. Tîoe Brain That Changes Itself. New York,NY: Viking: 2007.
37. Adams RJ, Albers G, Alberts MJ, et al. Update to theAHA/ASA recommendadons for the prevention ofstroke in patient.s with stroke and transient isehemicattack. Stroke 2008;39:1647-1652.
38. Ridker PM, Paynter NP. Rifai N, et al. C-reactiveprotein and parental history improve globalcardiovascular risk prediction: the Reynolds RiskScore for men. Circulation 2008;118:2243-2251.
39. Ridker PM. C-reactive protein and the prediction ofcardiovascular events among those at intermediaterisk: moving an inflammatory hypothesis towardconsensus. J Am Coll Cardiol 2007:49:2129-2138.
40. Elkind MS. Inflammation, atherosclerosis, and stroke.Neurologist 2006:12:140-148.
41. Kuo HK, Yen CJ, Chang CH, et al. Relation ofC-reactive protein to stroke, cognitive disorders,and depression in the general population: systematicreview and meta-analysis. Lancet Neurol 2005:4:371-380.
42. Muir KW, Weir CJ, Alwan W, et al. C-reactiveprotein and outcome after isehemic stroke. Stroke1999;30:981-985.
43. Winbcck K, Poppert H, Ergen T, et al. Prognosticrelevance of early serial C-reactive proteinmeasurements after first isehemic stroke. Stroke2002;33:2459-2464.
44. Arenillas JF, Alvarcz-Sabin J, Molina CA, et al.C-reactive protein predicts further isehemic events infirst-ever transient isehemic attack or stroke patientswith intracranial large-artery occlusive disease. Stroke2003:34:2463-2468.
45. Rallidis LS, Vikelis M, Panagiotakos DB, er al.Usefulness of inflammatory and haemostatic markersto predict short-term risk for death in middle-aged ischaemic stroke patients. Acta Neurol Scand2008;117:415-420.
46. Bansal S, Ridker PM. Comparison of characteristicsof futnare myocardial infarctions in women withbaseline high versus baseline low levels of high-sensitivity ([^-reactive protein. AmJ Cardiol2007:99:1500-1503.
47. Corréale J, Villa A. Ihe neuroprotective role ofinflammation in nervous system injuries.J Neurol2004:251:1304-1316.
48. Farooqui AA, Horrocks LA, Farooqui T. Modulationof inflammation in brain: a matter of fat. J Neorocfeem2007:101:577-599.
49. Kidd PM. Omega-3 DHA and EPA for cognition,behavior and mood: clinical findings andstructural-functional synergies with cell membranephospholipids. Altern Med Rev 2007:12:207-227.
50. Hossain MS, Hashimoto M, Gamoh S, MasumuraS. Antioxidative effects of doeosahexaenoic acidin the cerebrum versus cerebellum and braitistcmof aged hypercholesterolemic rats.J Neiirochem1999:72:1133-1138.
Page 32
._. 1

Alternative Medicine Review Volume 14, Number 1 2009
Post-Strjke Recovery
51. Hong S, Groneri K, Devchand PR, er ;il. Novel 66.docosatrienes and 17S-resoIvÍns generated fromdocosahex.ienoic acid in muríne brain, human blood,and glial cells. Autacoids in anti-inflammation,_/ Biol 67.Chem 2003:278:14677-14687.
52. Bunea R, El Farrah K, Deutsch L. Evaluation of theeffects of Neptune Krill Oil on the clinical course ofhyperlipidemia. Aitern Med Rev 2004:9:420-428. 68.
53. Sampalis F, Bunea R, Pelland MF, et al. Evaluation ofthe effects of Neptune Krill Oil on the managementof premenstrual syndrome and dysmenorrhea. AlternMt\íKfv2003;8:171-179. 69.
54. Deutsch L. Evaluation of the effect of Neptune KrillOil on chronic inflammation and arthritic symptoms.J Am Coll Nutr 2007:26:39-48.
55. Simi A, Isakiri N, Wang P. Rothwcll NJ. 70.Interleukin-l and inflammatory neurodegeneration.Biochem Soc Trans 2007;35:1122-1126.
56. McCoIl BW, Rothwell NJ, Allan SM. Systemicinflammatory stimulus potentiates the acute phase 71.and CXC chemokine responses to experimentalstroke and ex.u'erbates brain damage via interleukin-1and neurrophil-dependent mechanisms. / Neurosci2007:27:4403-4412. ' 72.
57. Boutin H, LeFeuvre RA, Horai R, et al. Role ofIL-lalpha and IL-lbeta in ischémie brain damage.JNeurosci 2001;21:5528-5534.
58. Lucas SM, Rothwell NJ, Gibson RM. The role 73.of inflammation in CNS injury and disease. BrJPharmacol 2i)0(v,l47:S2^2'S240.
59. Gueorguieva I, Clark SR, McMahon CJ, et al.Pharmacokinetic modelling of interleukin-1 receptor 74.antagonist in plasma and cerebrospinal fluid oípatients following subarachnoid hemorrhage. BrJCltn Pharmacol 2008;65:317-325. 75.
60. Bostom AG, Rosenberg IH, Silbershatz H, et al.Non fasting plasma total homocysteine levels andstroke incidence in elderly persons: the FraminghamStudy. Ann /«fern Med I999;131:352-355.
61. Bors ML, Launer LJ, LindemansJ,et al. 76.Homocysteine and short-term risk of myocardialinfarction and stroke in the elderly: the RotterdamStudy. Arch intern Med 1999:159:38-44.
62. Cui R, Moriyama Y, Koike KA, et al. Serum totalhomocysteine concentrations and risk of mortalityfrom stroke and coronary heart disease in Japanese: 77.theJACC Study Atherosclerosis 2008:198:412-418.
6i . Spence JD. Homocysteine-lowering therapy: a role instroke prevention? Lancet Neurol 2007;6:830-838. 78.
64. Hankey GJ. Is homocysteine a causal and treatablerisk factor for stroke? Lancet Neurol 2007:6:751-752.
65. WangJ, Hurt AM. Spence JD, Hegele RA. Single 79.nucleotide polyn\orphism in C T H associated wirhvariation in plasma homocysteine concentration. ClinCenet 2004,65:483-486.
McCuIly KS. Vascular pathology of homocysteinemia:implications for the pacliogenesis of .irteriosclcrosis.AmJ Pathol 1969;56:ll l- l28.Boets GH, Smals AG, Trijbels FJ, et al.Heterozygosity for homocystinuria in prematureperipheral and cerebral occlusive arterial disease. NEn^lJ Med 1985:313:709-715.Clarke R. Daly L, Robinson K, et al.Hyperhomocysteineniia: an independent risk factorfor vascular disease. N Engt } Med 199l;324:l 149-1155.
Van den Berg M, Boers GH, Franken DG, et al.Hyperhomocysteinemia and endothelial dysfiinctionin young patients with peripheral arterial occlusivedisease. Eur I Clin hvest 1995:25:176-181.Mudd SH. Finkclstcin JD, Refsuin H. et al.Honiocysteine and its disulfide derivatives: asuggested consensus terminology. Arteriosckr ThromVase ßt«/2000:20:1704-1706.Grali.im IM, Daly LE, Refsum HM, et al. Plasmahomocysteine as a risk factor for vascular disease.The European Concerted Action Project. JA MA1997:277:1775-1781.
Nygard O, Nordrehaug JE, Refsum H, et al. Plasmahomocysteine levels and mortality in patients wirhcoronary artery disease. N EnglJ Med 1997:337:230-236.Refsum H, Nurk E, Smirh AD, et al. The HordalandHomocysteine Study: a community-based study ofhomocysteine, its determinants, and association withdisease.,/ Nutr 2006;136:173lS-1740S.Lonn E, Yusiif S, Arnold MJ, er ai. Homocysteinelowering with folie acid and B vitamins in vasculardisease. N EnglJ Med 2006;354:1567-1577.Poli D, Antonucci B, Cecchi E, et al. Culpritfactors for the failure of well-conducted warfarintherapy to prevent ischémie events in patients withatrial fibtillation: the rolr of homocysreine. Stroke2005;36:2139-2163.
Toole JF, Malinow MR, Chambless LE, et al.Lowering homocysteine in patients with ischémiestroke to prevent recurrent stroke, myocardialinfarction, and death: the Vitamin Intervention forStroke Prevention (VISl^) randomized controlledtrial. jAMA 2004:291:565-575.Wang X, Qin X, Deminas FI, et al. Efficacy of folieacid supplementation in stroke prevention: a meta-analysis. Lancet 2007;369:1876-1882.D'Orlando KJ, Sandage BWJr. Citicoline (CDP-choline): mechanisms of action and effects in ischémiebrain injury. Neurol Res ]995;I7:281-284.Rao AM, Hatcher JF, Dempscy Rj. CDP-choline:neuroprotection in transient forebrain ischemia ofgerhils.J Neurosci Res 1999;58:697-705.
Page 33

Alternative Medicine Reviev^ Volume 14, Number 1 2009
80. Secades j j , Alvarez-Sabin I, Rubio F, et al. Citicoline 92.in intracerebral haemorrhage: a double-blind,randomized, placebo-controlled, m ulti-centre pilotstudy. Cerebrovasc Dis 2006;21:380-385. 93.
81. Clark WM, Warach SJ, Petrigrew LC, et al. Arandomized dose-response trial of citicoline in aeuteischémie stroke patients. Citicoline Stroke StudyGroup. Neurology 1997;49;671-678. 94.
82. Clark WM, Williams BJ, Selzer KA, et al. Arandomized efficacy trial of citicoline in patients withacute ischémie stroke. Stroke 1999;30:2592-2597. 95.
83. Waraeh S, Pcttigrew LC, Dashe JF, et al. Effectot eitieoline on ischémie lesions as measuredby diffusion-weigh ted magnetic resonanceimaging. Citicoline 010 Investigators. Ann Neural 96.2000:48:713-722.
84. Clark WM, Wechsler LR, Sabounjian LA, et al.A phase III randomized efficacy trial of 2000 mg 97.citicoline in acute ischémie stroke patients. Neurology2001;57:1595-1602.
85. Dávalos A, Castillo J, Alvarez-Sabin J, et al. Oraleitieoline in acute ischémie stroke: an individualpatient data pooling analysis of clinical trials. Stroke 98.2002:33:2850-2857.
86. Bolland K, Whirehead J, Cobo E, Secades j j .Evaluation of a sequential global test of improvedrecovery following stroke as applied to the ICTUS 99.trial of citicoline. Pharm Stat 2008 July 21 [Epubahead of print]
87. Aguglia E, Ban TA, Panzarasa RM, ct al. Cholinealphoscerate in rhe treatment of mental pathology 100.following acute cerebrovaseular accident. Funct Neurol1993:8:S5-S24.
88. Barbagallo Sangiorgi G, Barbagallo M, Giordano 101.M, et al. alpha-Glyeerophosphoeholine in themental reeovery of eerebral i.schemie attacks. An 102.Italian multieenter elinieal trial. Ann N Y Acad Sei1994;717:253-269. 103.
89. Consolj D, Giunta V, Grillo G, et aL alpha-GPCin the treatment of acute eerebrovaseular aecident 104.patients. Arch Med ¡ntertíü 1993;45:13-23. [Article inItalian]
90. Gambi D, Onofrj M. Multieenter clinical studyof effieaey and tolerability of eholine alfoscerate 105.in patients with deficits in higher mental funetionarising after an acute isehemíc cerebrovaseular attack.Gcriatria 1994;6:91-98.
91. Tomasina C, Manzino M, Novello P, et al. 106.Clinieal study of the therapeutic effectiveness andtolerability of ehoüne alfoscerate in 15 subjects withcompromised cognitive functions subsequent to acutefocal cerebral ischemia. Riv Neuropsichiatr Sei Affin1996;37:21-28.
Mathew NT', Rivera VM, Meyer jS, et al. Double-blind evaluation of glyeerol therapy in acute eerebralinfaretion.LííMCt-í 1972:2:1327-1329.Parnetti L, Amenta F, Gallai V. Choline alfoseerate incognitive decline and in aeute eerebrovaseular disease:an analysis of published elinieal data. Mcch AgeingDn'2001;122:2041-2055.
Auteri A, Bova F, Chiarion C, et al. Protecting thebrain during heart surgery: treatment with eholinealfoscerate. Lc Baii Raz Ter 1993;23:123-128.Onishchenko LS, Gaikova ON, Yanishevskii SN.Changes at the focus of experimental ischémie stroketreated with neuroproteetive agents. Neurosei BehavPhysiol200S;3S:49-54.
Wirthensohn G, Beck FX, Guder WG. Role andregulation of glyeerophosphorylcholine in r;it renalpapilla. P/ÍH¿crs Arch 1987;409:411-415.Vega j A, Cavallotti C, del Valle ME, et al. Nervegrowth factor receptor immunoreactivity in rheeerebellar cortex of aged rats: efleet of eholinealfoseerare treatment. Mech Ageing Dev 1993;69:119-127.
Merzenich MM, Kaas j H , Wall j , et al. Topographicreorganization of somatosensory cortical areas3b and 1 in adult monkeys following restricteddcafferen cation. Neuroscience 1983:8:33-55.Mahneke HW. Bronstone A, Merzenich MM.Brain plastieity and functional losses in the aged:scientific bases for a novel intervention. Prog Brain Res2006;157:8M09.
Eriksson PS, Perfilieva E, BjÖrk-Eriksson T, et al.Neurogenesis in the adult human hippoeampus. NatMf.i 1998;4:1313-1317.Kempermann G. Adult Neurogencsis. New York, NY:Oxford University Press; 2006.Sehwab M. Nogo and axon regeneration. Cwrr OpinNcwrobiol 2004;14:U8-124.Yiu G, He Z. Glial inhibition of CNS axonregeneration. Nat Rev Neurosei 2006 ¡7:617-627.Allard T, Clark SA, Jenkins WM, MerzeniehMM. Reorganization of somatosensory area 3brepresentations in adult owl monkeys after digitalsyndaetyly.j Neurophysiol 1991:66:1048-1058.Xerri C, Merzenieh MM, Peterson BE, Jenkins W.Plastieity of primary somatosensory eortex parallelingsensorimotor skill reeovery from stroke in adultmonkeys.J Neunyphysiol 1998;79:2119-2148.Jenkins WM, Merzenich MM, Ochs MT, et al.Funericnal reorganization of primary somatosensorycortex in adult owl monkeys after behaviorallycontrolled tactile stimulation.J Neurophysiol1990;63:82-104.
Page 34
Alternative Medicine Review Volume 14, Number 1 2009
107. GcrlotiC. Bushara K, Sailer A, et al. Multimodal 123.imaging of brain reorganization in motor areas of thecontrale.sional hemisphere of well recovered patientsafter capsular stroke. Bnitn 2006;129:791-808.
108. Bbardwaj RD, Curtis MA, Spalding KL, et al.Neocortical neurogenesis in humans is restricted 124.to development. Proc Nail Acaä Sei U S A2006:103:12564-12568.
109. Hess DC, Boriongan CV. Stem cells and neurologicaldiseases. Cell Prolif 2Q0S:41:94-114. 125.
I 10. Azizi SA, Stokes D, Augeili BJ, et al. Engrafitmentand migration of human hone marrow stromal cellsimplanted in the brains of albino rats - similarities 126.to astrocyte grafts. Proc Natt Acad Sei USA1998:95:3908-3913.
111. Chen j , Li Y, Katakowski M, et al. fntravenous bonemarrow stromal cell tberapy reduces apoptosis and 127.promotes endogenous cell proliferation after stroke infemale rat.J Neurosa Res 2003:73:778-786.
1 f2. Sben f,H, Li Y, Chen J. et al. Therapeutic henefit of 128.hone marrow stromal cells administered 1 monthafter stroke.,/ Cerch RlooJ Flow Mi'tab 2007:27:6-13.
113. Liu H, Honmou O, Harada K, et al. Neuroprotectionby PIGF gene-modifed buman mesenchymal stem 129.cells after cerebral iscbaemia. ßrai» 2006; 129:2734-2745.
114. Bang OY, Lee jS, Lee PH, Lee G. Autologousmesenchymal stem cell transplantation in stroke 130.patients. Ami Ncurol 2005:57:874-882.
I 15. Steenhlock D, Payne A. Umbilical Cord StemCell Therapy. Laguna Beaeb, CA: Basic HealtbPublications: 2006.
116. Locatelli F, Bersano A, Ballabio E, et al. Stem celltberapy in stroke. Cell Mol Life Sei 2008 Nov 8 [Epub 131.abead of printl
117. Minger SL, Ekonomou A, Carta EM, et al.Endogenous neurogenesis in tbe buman brain 132.following cerebral infarction. Rcgcn Med 2007;2:69-74.
118. Arvidsson A, Collin T, Kirik D, et al. Neuronalreplacement from endogenous precursors in tbe adultbrain after stroke. Nat Med 2002;8:963-970.
119. Sk.ipcr SD.'Ilic biology of neurocropbins. signalling 133.pathways, and functional peptide mimetics ofneurotrophins and their receptors. CNS NeuralDtsord Drug Targets 2008:7:46-62.
120. f*oo MM. Neurorropbins as synaptic modulators. NatRev Neurosci 2001;2:24-32. 134.
12L Tönges L, Scblacbetzki jC, Weishaupt JH, BahrM. Hematopoietic cytokines - on the verge ofconquering neurology. Ciirr Mol Med 2007;7:157- 135.170.
122. Ehrenreich H. Hasselhlatt M, Dembowski C, et al.Erytbropoietin therapy for acute stroke is both safeand beneficial. Mol Med 2002:8:495-505.
SpringborgJB, Möller C. Gideon P, et al.Erytbropoietin in patients witb aneurysmaisubarachnoid haemorrhage: a douhle blindrandomised clinical trial. Acta Neurochir (Wien)2007:149:1089-110L
Ehrenreich H, Timner W, Siren AL. A novel role foran established player: anemia drug erytbropoietin fortbe treatment of cerehral bypoxia/ischemia. TransfusApÍJcrScí 2004:31:39-44.
Liu XB, Wang JA, Yu SP, et al. Therapeutic strategyof erytbropoietin in neurological disorders. CNSNeurolDisord Dru¿ Targets 2008;7:227-234.Schäbitz WR, Kollmar K, Schw;ininger M, etal. Neuroprotective effect of gr.inulocyte colony-stimulating factor after focal cerehral ischemia. Stroke2003;34:745-751.
Borlongan CV, Hess DC'. New hope for strokepatients: mobilization of endogenous stem cells.CMA/2006:174:954-955.Shyu w e , Lin SZ, Lee CC, ct al. Granulocytecolony-stimulating factor for acute ischémie stroke: arandomized controlled trial. CMAJ 2006;174:927-933.Miller HR 3rd, Pastor-B.irriuso R, Dalai D,et al. Meta-analysis: high-dosage vitamin Esupplementation may increase all-cause mortality.Ami hitem MaJ2005;142:37-46.Milman U, Blum S. Shapira C, et al. Vitamin Esupplementation reduces cardiovascular events in asubgroup of middle-aged individuals with botb type2 diabetes melUtus and the baptoglobin 2-2 genotype:a prospective double-blinded clinical trial. ArteriosclerUromb Vase Biol 2008:28:341-347.Cramer SC. Repairing the buman brain after stroke.II. Restorative tiierapies. Ann Neitrol 2008;63:549-560.
Wolf SL, Winstein CJ, Miller JP, et al. Effect ofconstraint-induced movement tberapy on upperextremity function 3 to S) months after stroke:the EXCITF, randomized clinical trial. JAAIA2006:296:2095-2104.Wolf SL, Winstein CJ, Miller JP, er al. Retention ofupper limb function in srroke survivors who havereceived constraint-induced movement tberapy: tbeEXCITE randomised trial. Lancet Ncurol 2008;7;33-40.PositScience. Published and unpublished studies-all.www.positsci.coni/scicnce [Accessed November 13,2008]Tanielian T,Jaycox L. Invisible Wounds ofWar: Psychological und Cognitive Injuries, TheirConséquences, and Services to Assist Recovery. SantaMonica, CA: RAND Corporation; 2008.
Page 35
