inflammation & repair - delta...
TRANSCRIPT

Inflammation & Repair By Dr.
Maha M. Abu-Hashim
Spring 2016
Page 2
Inflammation
Definition:- It is local reaction of living tissue to injurious agents. It is the vascular response to injury.
Aim of inflammation is to localize and get rid of the injurious agent.
Inflammation may be acute or chronic.
The suffix “itis” is added to the base word to state the condition e.g tonsil/tonsilitis…. Appendix/appendicitis.
Page 3
Acute inflammation……….Objectives
1. Definition…
2. List 4 cardinal signs of acute inflammation and the reason for each.
3. Describe the vascular and cellular events of acute inflammation (Pathogenesis).
4. List the cells of the inflammatory process and their activity.
5. Define exudate, transudate, and pus.
6. Define the following, fibrinous, serous, suppurative and catarrhal inflammation, abscess, and cellulitis.
Page 4
Acute inflammation
It is a type of inflammation characterized by….
1. Sudden onset
2. Short duration
3. Caused by strong irritant
4. Exudative in nature
5. Followed by repair
Page 5
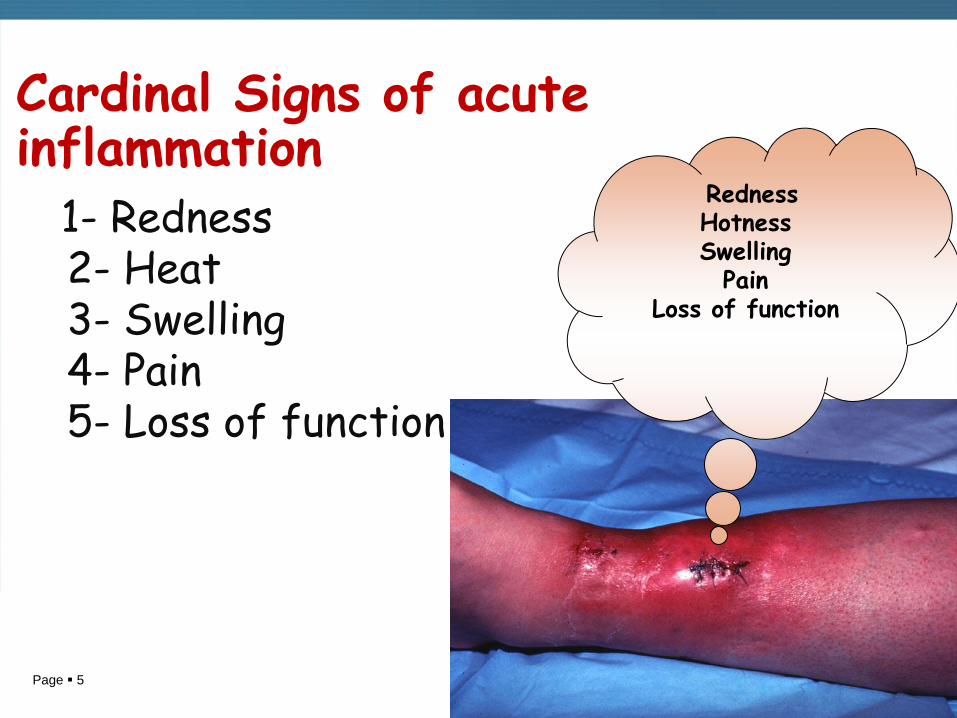
Cardinal Signs of acute inflammation
1- Redness 2- Heat 3- Swelling 4- Pain 5- Loss of function
Redness Hotness Swelling
Pain Loss of function
Page 6
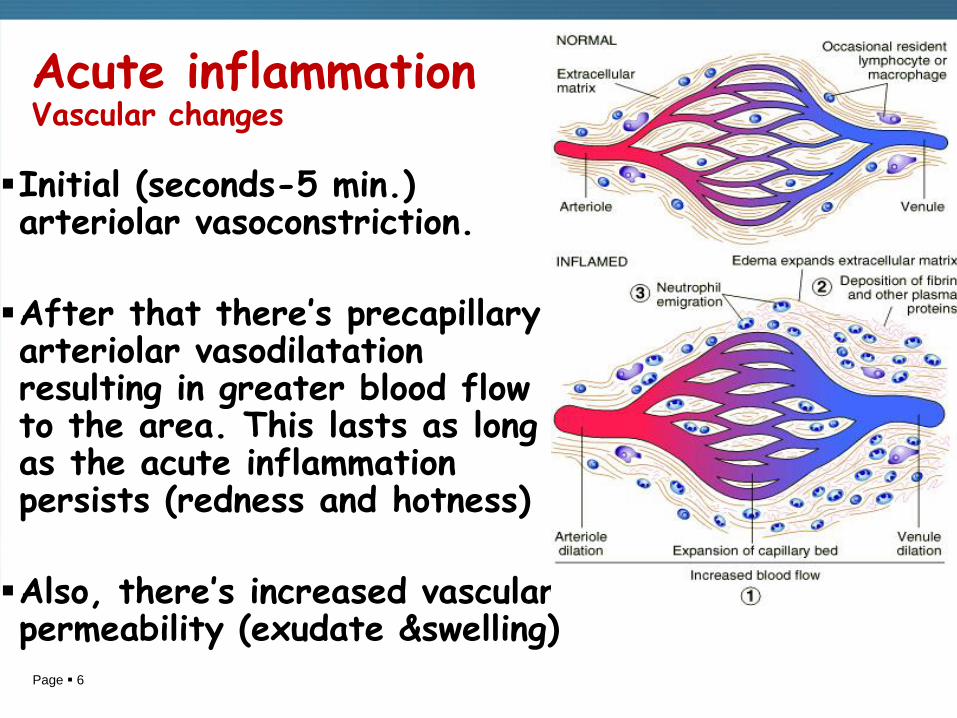
Acute inflammation Vascular changes
Initial (seconds-5 min.) arteriolar vasoconstriction.
After that there’s precapillary arteriolar vasodilatation resulting in greater blood flow to the area. This lasts as long as the acute inflammation persists (redness and hotness)
Also, there’s increased vascular permeability (exudate &swelling)
Page 7
Exudate and transudate
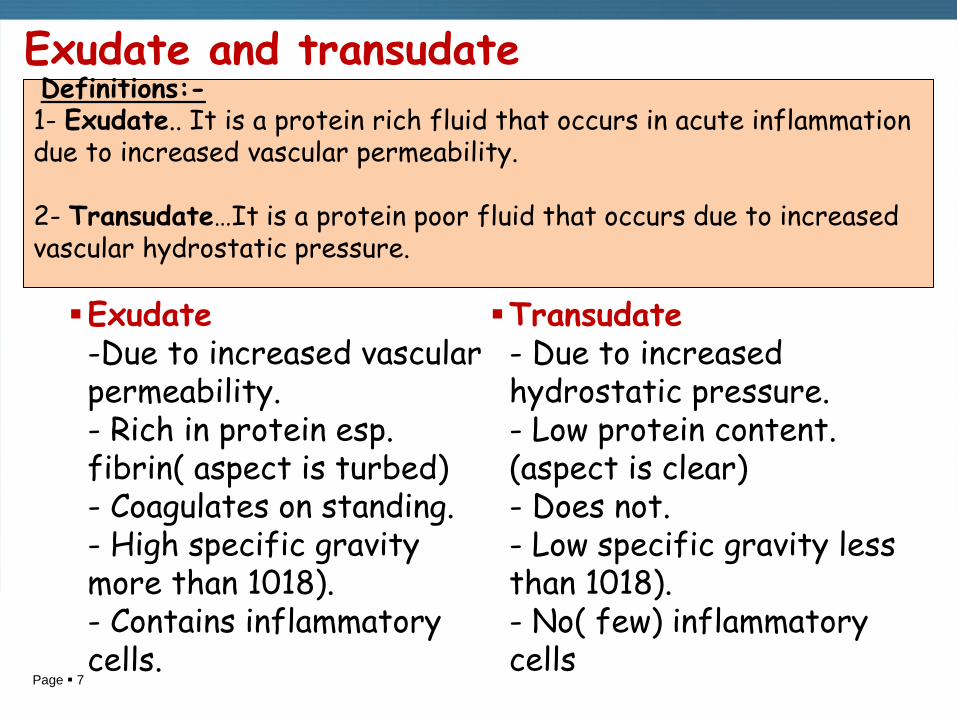
Exudate -Due to increased vascular permeability. - Rich in protein esp. fibrin( aspect is turbed) - Coagulates on standing. - High specific gravity more than 1018). - Contains inflammatory cells.
Transudate - Due to increased hydrostatic pressure. - Low protein content. (aspect is clear) - Does not. - Low specific gravity less than 1018). - No( few) inflammatory cells
Definitions:- 1- Exudate.. It is a protein rich fluid that occurs in acute inflammation due to increased vascular permeability. 2- Transudate…It is a protein poor fluid that occurs due to increased vascular hydrostatic pressure.

Page 8
Acute inflammation Cellular events 1. After vasodilatation,
leukocytes (especially polymorphes) move from the vessel into the interstitial tissue (emigration).
2. Neutrophils (polymorphes are the first cells to emigrate in acute inflammation followed by macrophage.
Page 9
.
Page 10
Cellular events
Vascular and cellular events
1- Emigration
2- Chemotaxis - It is the directional movement of leucocytes towards the irritant within the area of inflammation.

Page 11
Vascular and cellular events
1- Emigration
2- Chemotaxis
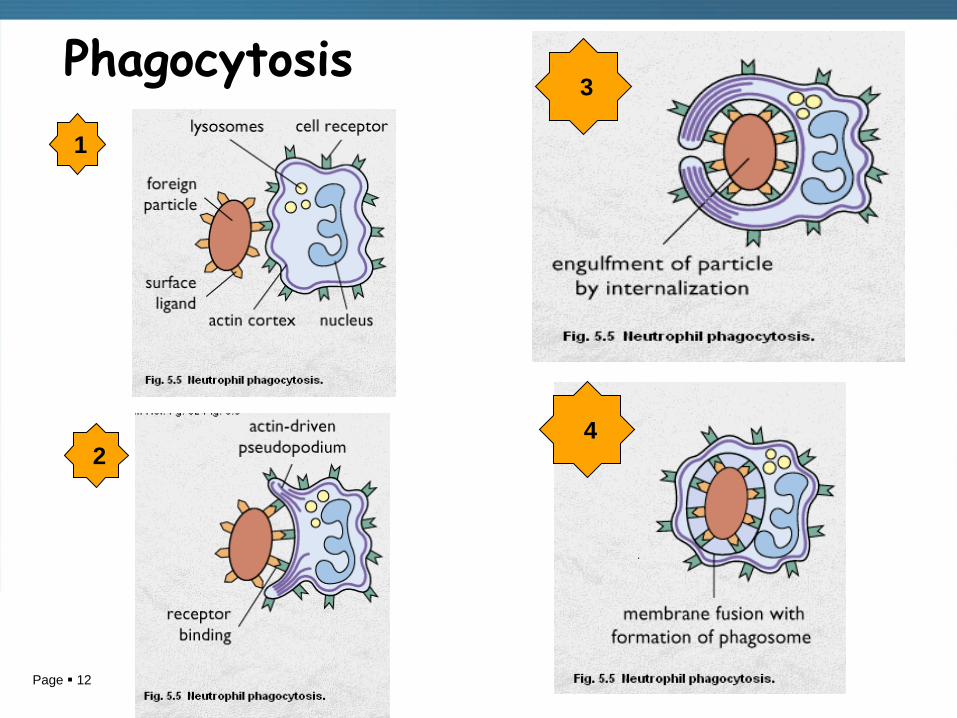
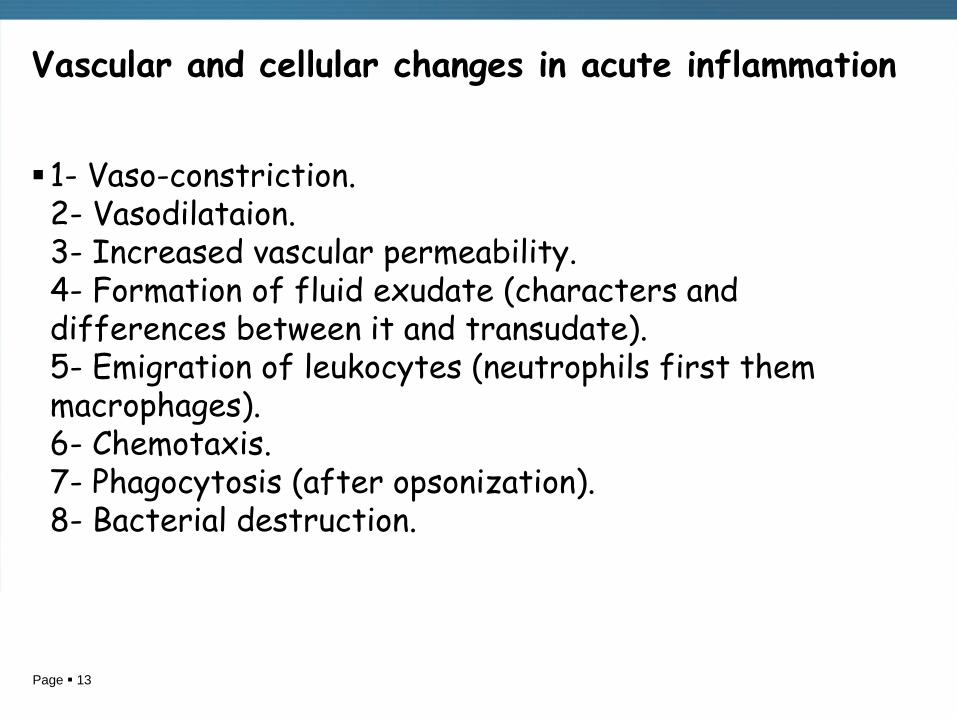
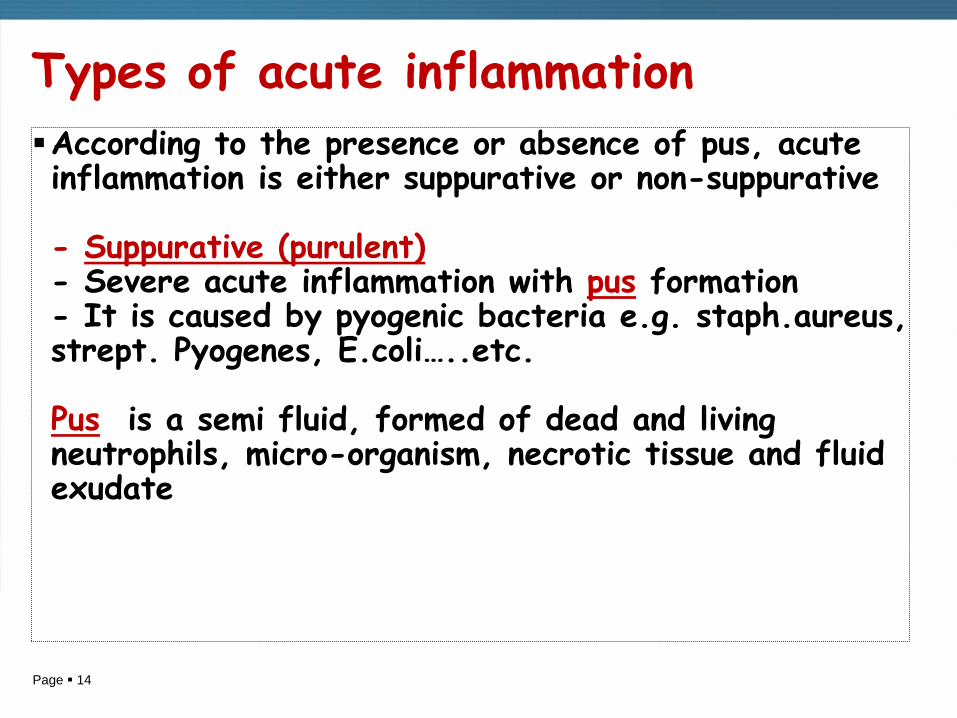
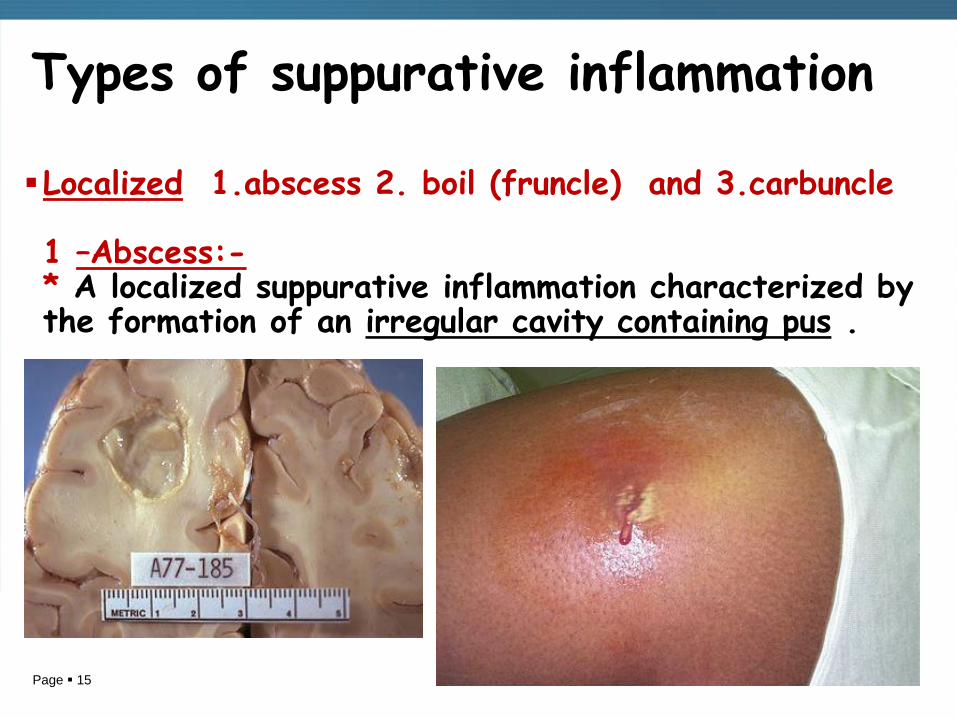
3- Phagocytosis
It is the ingestion and destruction of particulate material (tissue debris, living or dead bacteria and other foreign cells) by phagocytic cells mainly neutrophils and monocytes-macrophages.
Phagocytosis is facilitated by opsonization which is the coating of particulate material by substances that immobilize the particles to the surface of the phagocytes.
Cellular events
Page 12
Phagocytosis
1
2
3
4
Page 13
Vascular and cellular changes in acute inflammation
1- Vaso-constriction. 2- Vasodilataion. 3- Increased vascular permeability. 4- Formation of fluid exudate (characters and differences between it and transudate). 5- Emigration of leukocytes (neutrophils first them macrophages). 6- Chemotaxis. 7- Phagocytosis (after opsonization). 8- Bacterial destruction.
Page 14
Types of acute inflammation
According to the presence or absence of pus, acute inflammation is either suppurative or non-suppurative - Suppurative (purulent) - Severe acute inflammation with pus formation - It is caused by pyogenic bacteria e.g. staph.aureus, strept. Pyogenes, E.coli…..etc. Pus is a semi fluid, formed of dead and living neutrophils, micro-organism, necrotic tissue and fluid exudate
Page 15
Types of suppurative inflammation
Localized 1.abscess 2. boil (fruncle) and 3.carbuncle 1 –Abscess:- * A localized suppurative inflammation characterized by the formation of an irregular cavity containing pus .
Page 16
Types of suppurative inflammation
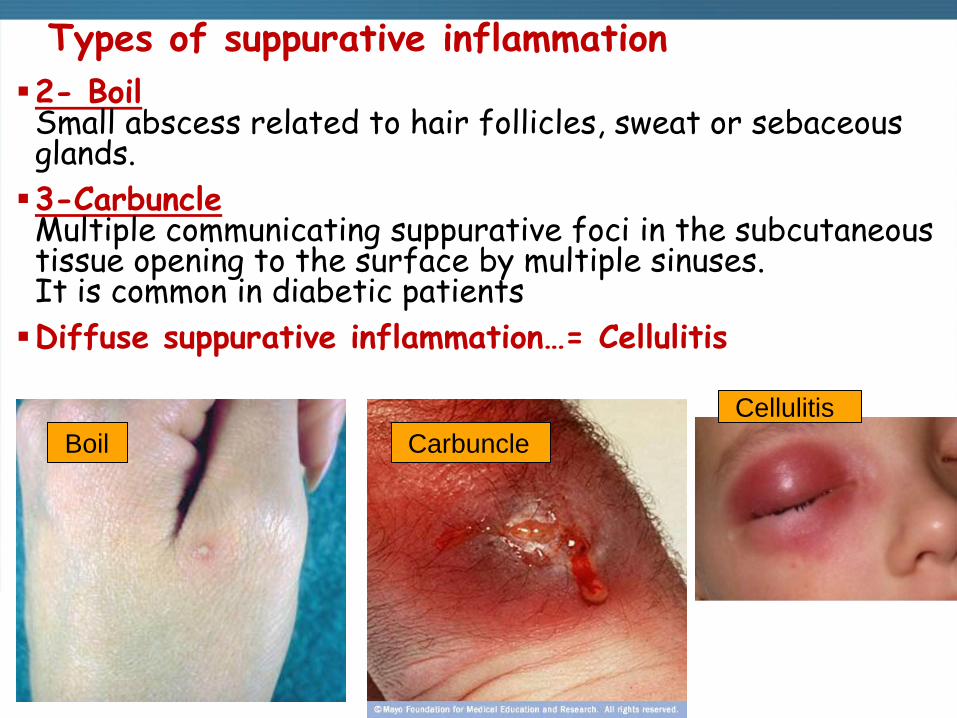
2- Boil Small abscess related to hair follicles, sweat or sebaceous glands.
3-Carbuncle Multiple communicating suppurative foci in the subcutaneous tissue opening to the surface by multiple sinuses. It is common in diabetic patients
Diffuse suppurative inflammation…= Cellulitis
Boil Carbuncle
Cellulitis
Page 17
Non suppurative inflammation
Types 1- Serous and serofibrinous inflammation…
2- Catarrhal inflammation…e.g common cold
3- Pseudomembranous inflammation…e.g diphtheria & bacillary dysentry.
4- Hemorrhagic inflammation ….Vascular damage and hemorrhage
5- Necrotizing inflammation …. Excess tissue necrosis
6- Allergic inflammation …. From Antigen/Antibody reaction
Page 18
Non-suppurative inflammation
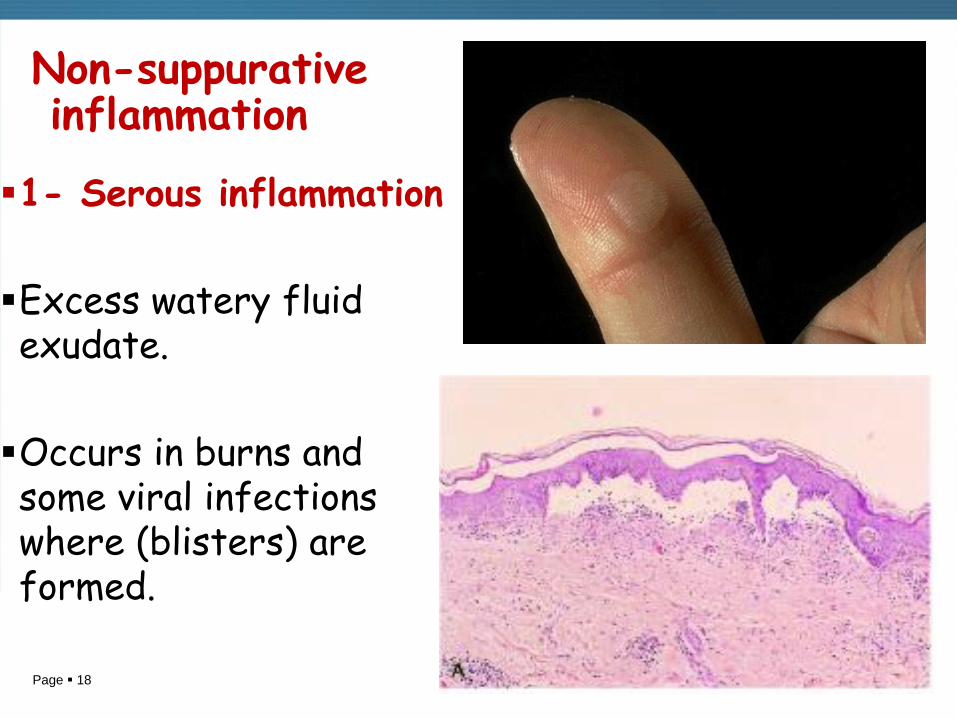
1- Serous inflammation
Excess watery fluid exudate.
Occurs in burns and some viral infections where (blisters) are formed.
Page 19
Non-suppurative inflammation
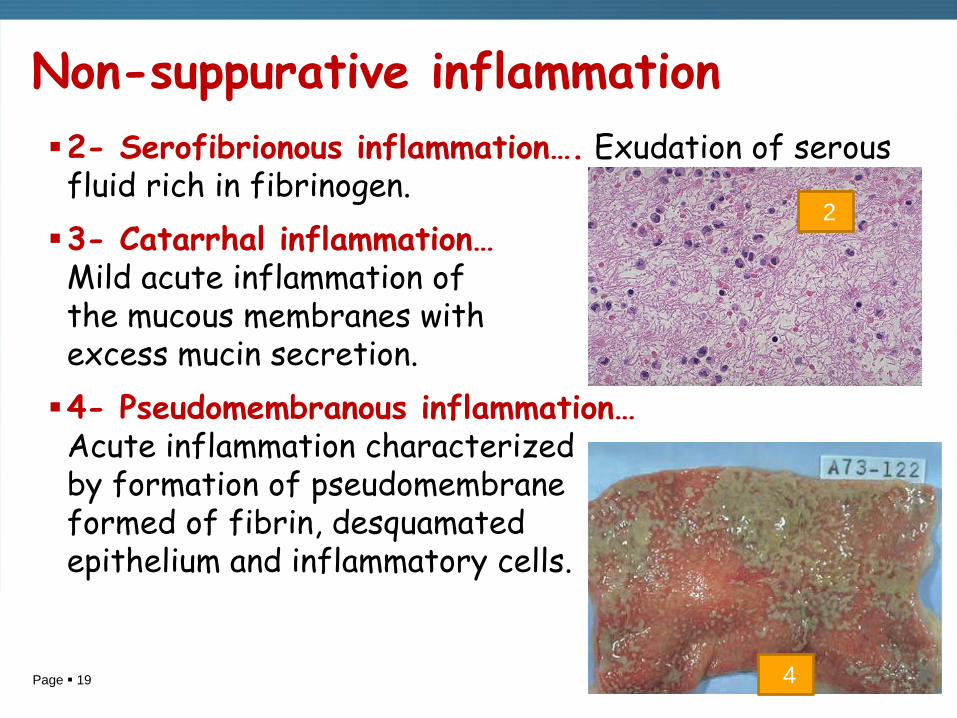
2- Serofibrionous inflammation…. Exudation of serous fluid rich in fibrinogen.
3- Catarrhal inflammation… Mild acute inflammation of the mucous membranes with excess mucin secretion.
4- Pseudomembranous inflammation… Acute inflammation characterized by formation of pseudomembrane formed of fibrin, desquamated epithelium and inflammatory cells.
2
4
Page 20
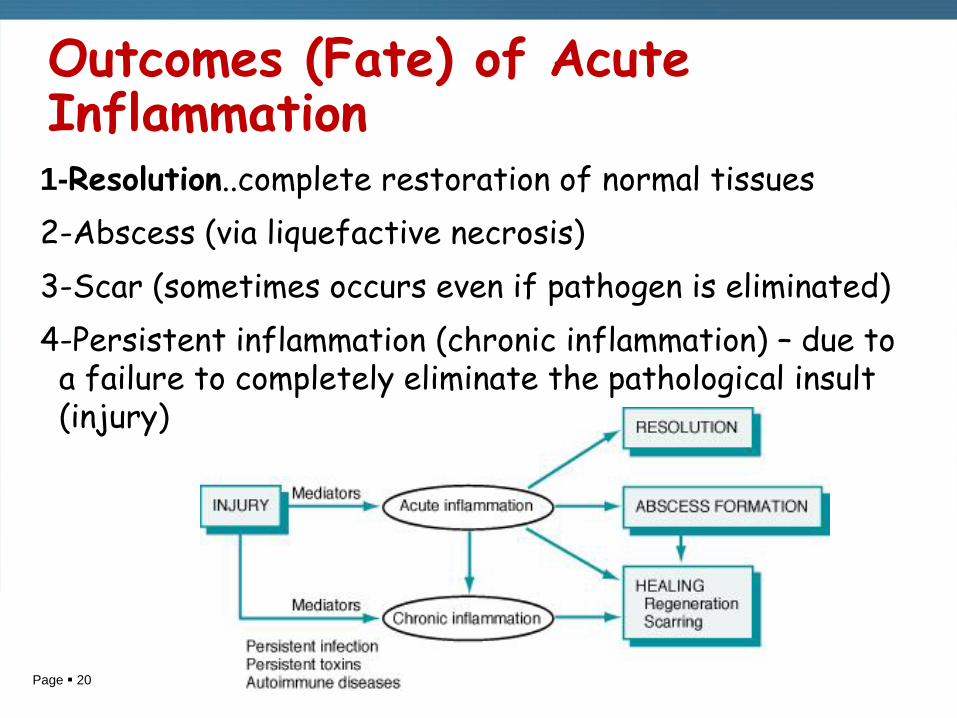
Outcomes (Fate) of Acute Inflammation 1-Resolution..complete restoration of normal tissues
2-Abscess (via liquefactive necrosis)
3-Scar (sometimes occurs even if pathogen is eliminated)
4-Persistent inflammation (chronic inflammation) – due to a failure to completely eliminate the pathological insult (injury)

Page 21
Chronic inflammation & Repair ……. Objectives
1. Discuss chronic inflammation including definition, how it arises, its cells , and histology.
2. Distinguish granulomatous inflammation as to causes and morphology.
3. Define labile, stable and permanent cells relative to healing. Give tissue examples.
4. Describe the process of wound healing by first intension and second intension.
5. Describe systemic and local influences that may modify the quality of the repair process. Define the following, ulcer, fistula, and sinus.

Page 22
Chronic inflammation
A type of inflammation characterized by
1. Gradual onset
2. Long duration
3. Caused by mild irritant
4. Proliferative in nature (excess cells)
5. Associated with repair
- Chronic inflammatory cells include..lymphocytes, plasma cells and macrophages
- Chronic inflammation may be specific or non specific
Page 23
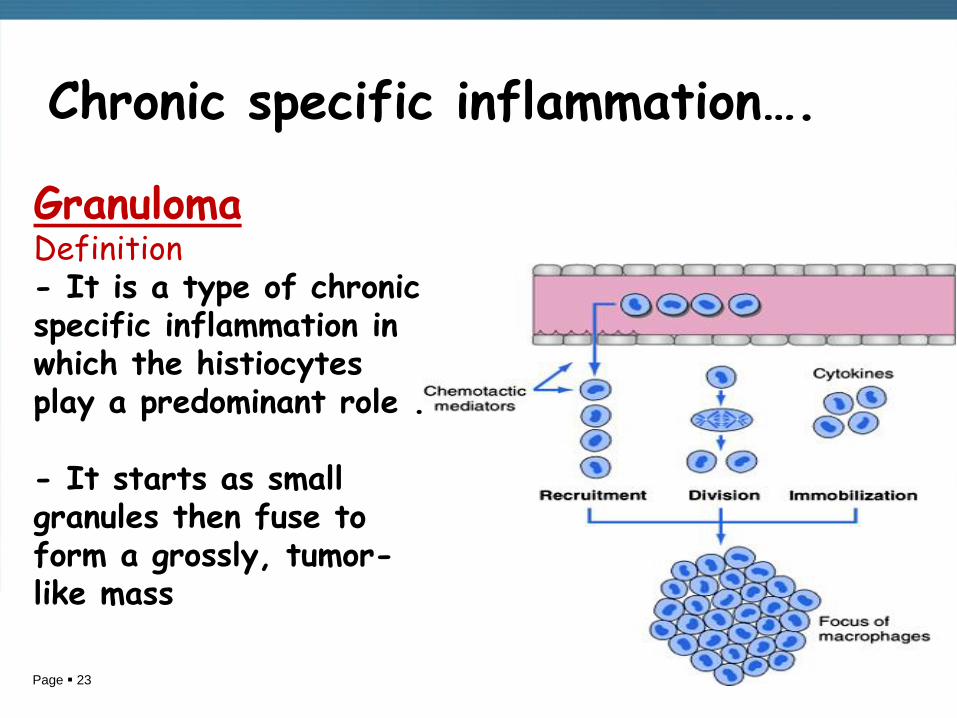
Chronic specific inflammation…. Granuloma Definition - It is a type of chronic specific inflammation in which the histiocytes play a predominant role . - It starts as small granules then fuse to form a grossly, tumor- like mass
Page 24
Types of granulomas
1- Infective - Bacterial.. Tuberculosis, syphilis ,leprosy - Fungal…histoplasma , Candida. - Viral…lymphogranuloma inguinal. - Parasitic…. Bilharziasis. - Suppurative granuloma….actinomycosis
2- Non infective - Foreign body ..around surgical stitches. - Allergic…..Rheumatic fever.
3- Of unknown cause - Sarcoidosis
Page 25
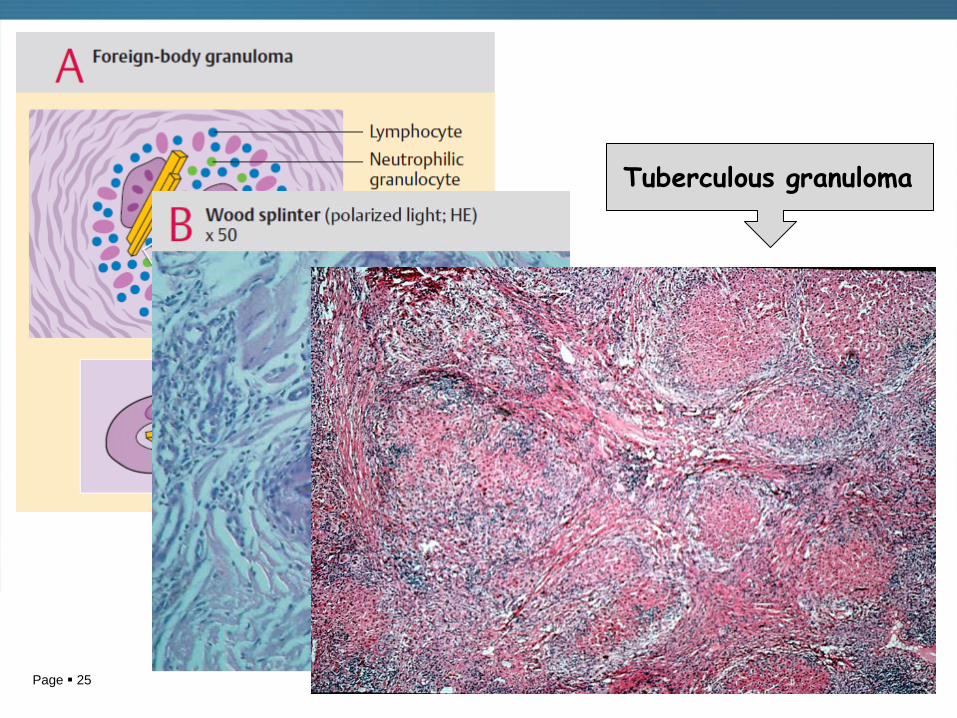
Tuberculous granuloma

Page 26
Acute and Chronic inflammation
Acute -Sudden onset -Short duration -Severe irritant - Vascular phenomena - Exudative - Polymorphs ¯ophages -Followed by repair
Chronic -Gradual onset -Long duration -Mild irritant -End arteritis obliterans -Proliferative -Lymphocytes, plasma cells & macrophages. -Associated with repair

Page 27
Repair, Regeneration, and Fibrosis Repair means Replacement of damaged tissue by a healthy new one. It occurs when body defense and treatment overcomes the irritant Regeneration: (generate, to bring to life). Replacement of injured cells by cells of the same type, sometimes with no trace of injury. - This occurs when the connective tissue infrastructure remains intact. - The surviving parenchymal cells must have the capacity to regenerate.
Page 28
Repair, Regeneration, and Fibrosis
According to their proliferative potential, cells of the body are Three types…..
1-Labile- These are continuously dividing cells throughout life to replace the damaged cells. - Examples are epidermis of the skin, and hemopoietic cells of the bone marrow
2-Stable…cells which do not proliferate under normal conditions but only when there is need. They include hepatocytes, renal tubular cells, glandular cells, and mesenchymal cells e.g smooth muscle, osteoblasts, cartilage cells,
3-Permanent…cells that do not proliferate in the post natal life. Permanent cells are found in the central nervous system and heart. Once they are destroyed, they cannot regenerate.
Page 29
Healing by fibrosis
Fibrosis… It is replacement of the damaged tissue by granulation tissue which matures to fibrous tissue.
It occurs if the connective tissue infrastructure is destroyed or if the cells of the tissue can not divide.
Granulation tissue:- It is a transitory tissue formed of capillaries and fibroblasts.
Page 30
Wound Healing Wound healing can occur by one of two ways according to the type of wound 1- Primary intention: the usual case with a surgical wound, in which there is a clean (sterile) wound with minimal tissue destruction, well-apposed edges, and therefore, there’s minimal scar formation.
2-Secondary intention: when wound is infected, with excessive tissue destruction, edges cannot be apposed, (e.g., following wound infection), then the wound slowly fills with granulation tissue from the bottom up. A large scar usually results.
Page 31
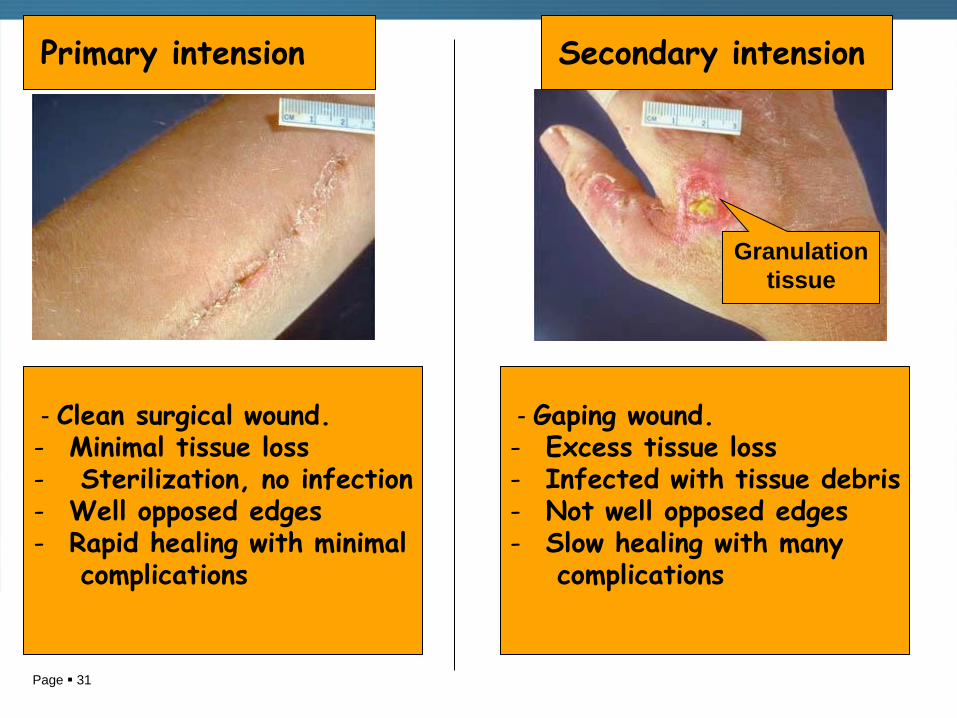
Granulation
tissue
Primary intension Secondary intension
- Clean surgical wound. - Minimal tissue loss - Sterilization, no infection - Well opposed edges - Rapid healing with minimal
complications
- Gaping wound. - Excess tissue loss - Infected with tissue debris - Not well opposed edges - Slow healing with many
complications
Page 32
Factors that influence wound healing
1.Type, size, and location of the wound
2.Vascular supply
3.Infection - delays wound healing and leads to more granulation tissue and scarring
4.Movement - wounds over joints do not heal well due to traction
5.Radiation - ionizing radiation is bad, UV is good
Page 33
Factors that influence wound healing
6.Overall nutrition: vitamin and protein deficiencies lead to poor wound healing, especially vitamin C, which is involved in collagen synthesis,also zink and calcium are important.
7.Age: younger is definitely better!
8.Hormones - corticosteroids drastically impair wound healing, because of their profound effect on inflammatory cells
Page 34
Complications of wound healing
I. Defective formation of granulation tissue and fibrous tissue….
1- Wound dehiscence…failure of the wound to heal.
2- Decreased cellular proliferation , this can lead to formation of ulcer, sinus, or fistula. a- Ulcer = discontinuity of the surface epithelium of the skin or mucous membrane. b- Sinus = A blind ended tract opening on the surface. c- Fistula = A tract joining two hollow organs.
3- Weak scar….incisional hernia.
Page 35
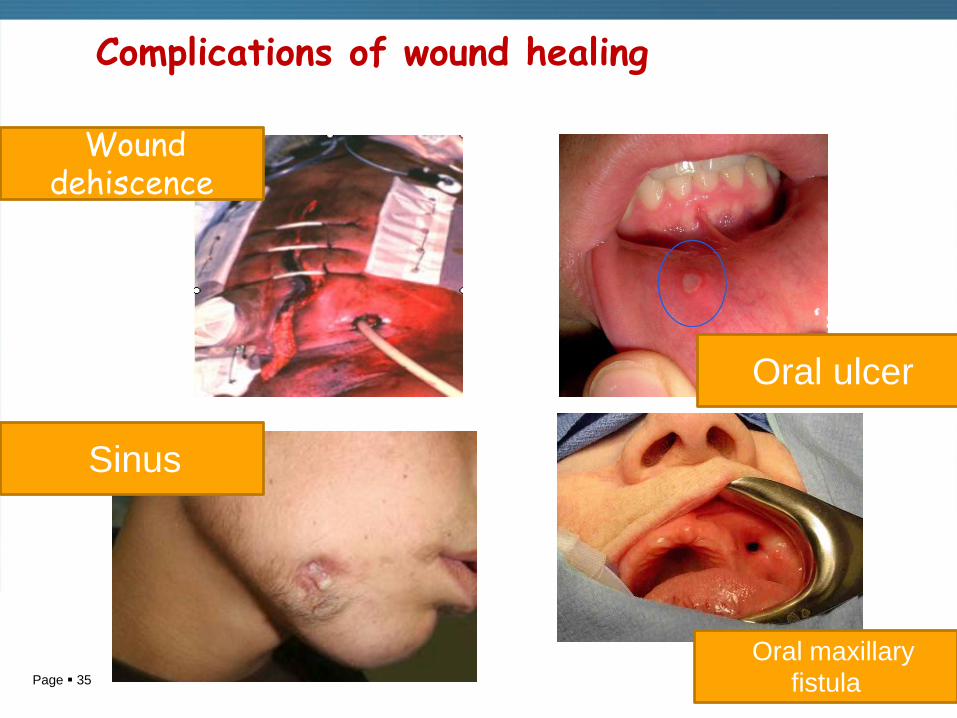
Complications of wound healing
Wound dehiscence
Oral maxillary
fistula
Sinus
Oral ulcer
Page 36
Complications of wound healing
II. Excessive Formation of granulation tissue & scarring 1- Proud flesh Excessive formation of granulation tissue above the surface of the wound. - This prevents epithelialization of the surface. - Surgical removal or cautery is required for complete healing of the wound
2-Keloids (hypertrophy scars) - Are the result of over-exuberant production of scar tissue, which is primarily composed of type III collagen
- Surgical removal is usually followed by recurrence

Page 37
Complcations of wound healing
Keloid

Page 38
Thank U