infectious disease news from the 4th annual ispor meeting
Post on 12-Dec-2016
212 views
TRANSCRIPT
6 PHARMACOECONOMICS
A number of poster presentations at the 4th annual meeting of the International Society for Pharmacoeconomics & Outcomes Research (lSPOR) focused on the economic and outcomes issues of infectious diseases.
Clarithromycin soothes the throat Antibacterial utilisation and the effect on costs
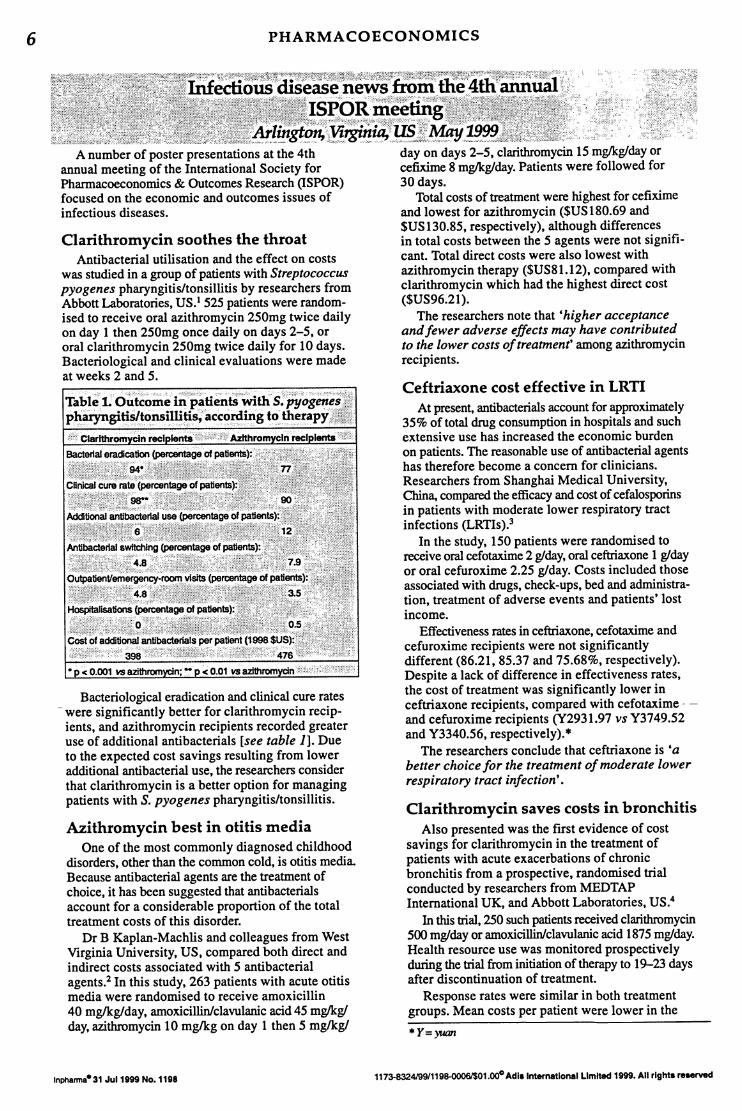
was studied in a group of patients with Streptococcus pyogenes pharyngitis/tonsillitis by researchers from Abbott Laboratories, US.! 525 patients were randomised to receive oral azithromycin 250mg twice daily on day 1 then 250mg once daily on days 2-5, or oral clarithromycin 250mg twice daily for 10 days. Bacteriological and clinical evaluations were made at weeks 2 and 5.
Bacteriological eradication and clinical cure rates - were significantly better for clarithromycin recip
ients, and azithromycin recipients recorded greater use of additional antibacterials [see table 1]. Due to the expected cost savings resulting from lower additional antibacterial use, the researchers consider that clarithromycin is a better option for managing patients with S. pyogenes pharyngitis/tonsillitis.
Azithromycin best in otitis media One of the most commonly diagnosed childhood
disorders, other than the common cold, is otitis media. Because antibacterial agents are the treatment of choice, it has been suggested that antibacterials account for a considerable proportion of the total treatment costs of this disorder.
Dr B Kaplan-Machlis and colleagues from West Virginia University, US, compared both direct and indirect costs associated with 5 antibacterial agents.2 In this study, 263 patients with acute otitis media were randomised to receive amoxicillin 40 mglkglday, amoxicillinlclavulanic acid 45 mglkg/ day, azithromycin 10 mglkg on day 1 then 5 mglkgl
Inpharma- 31 Ju11999 No. 1198
day on days 2-5, clarithromycin 15 mglkg/dayor cefixime 8 mglkg/day. Patients were followed for 30 days.
Total costs of treatment were highest for cefixime and lowest for azithromycin ($US 180.69 and $US130.85, respectively), although differences in total costs between the 5 agents were not significant. Total direct costs were also lowest with azithromycin therapy ($US81.12), compared with clarithromycin which had the highest direct cost ($US96.21).
The researchers note that 'higher acceptance andfewer adverse effects may have contributed to the lower costs of treatment' among azitbromycin recipients.
Ceftriaxone cost effective in LRTI At present, antibacterials account for approximately
35% of total drug consumption in hospitals and such extensive use has increased the economic burden on patients. The reasonable use of antibacterial agents has therefore become a concern for clinicians. Researchers from Shanghai Medical University, China, compared the efficacy and cost of cefalosporins in patients with moderate lower respiratory tract infections (LRTIs).3
In the study, 150 patients were randomised to receive oral cefotaxime 2 g/day, oral ceftriaxone 1 g/day or oral cefuroxime 2.25 g1day. Costs included those associated with drugs, check-ups, bed and administration, treatment of adverse events and patients' lost income.
Effectiveness rates in ceftriaxone, cefotaxime and cefuroxime recipients were not significantly different (86.21, 85.37 and 75.68%, respectively). Despite a lack of difference in effectiveness rates, the cost of treatment was significantly lower in ceftriaxone recipients, compared with cefotaxime - -and cefuroxime recipients (Y2931.97 vs Y3749.52 and Y3340.56, respectively). *
The researchers conclude that ceftriaxone is 'a better choice for the treatment of moderate lower respiratory tract infection'.
Clarithromycin saves costs in bronchitis Also presented was the first evidence of cost
savings for clarithromycin in the treatment of patients with acute exacerbations of chronic bronchitis from a prospective, randomised trial conducted by researchers from MEDTAP International UK, and Abbott Laboratories, US.4
In this trial, 250 such patients received clarithromycin 500 mg/day or amoxicillinlclavulanic acid 1875 mg/day. Health resource use was monitored prospectively during the trial from initiation of therapy to 19-23 days after discontinuation of treatment.
Response rates were similar in both treatment groups. Mean costs per patient were lower in the
*Y=yuan
1173-832419911198-00061$01.00° Adl.lntematlonal Limited 1999. All right. ruerved
PHARMACOECONOMICS
cIarithromycin group, compared with the amoxicillinl clawlanic acid group (£120 vs £146, respectively). Hospitalisation and medication costs were also lower in this group. Mean duration of hospitalisation was 10.8 days for c1arithromycin recipients, compared with 15.25 days for amoxicillinlclavulanic acid recipients.
The researchers note that although clarithromycin has previously been shown to be superior in cost comparisons with amoxicillinlc1avulanic acid, the results have been obtained from decision models.
Low-dose cefpodoxime lowers cost Studies evaluating the most effective therapies
for acute exacerbations of chronic bronchitis also received attention at the conference. Researchers from the University of Texas, US, and Pharmacia & Upjohn, Sweden, prospectively compared the costs of 2 different dosages of cefpodoxime proxetil in patients with acute bacterial exacerbations of chronic bronchitis.s
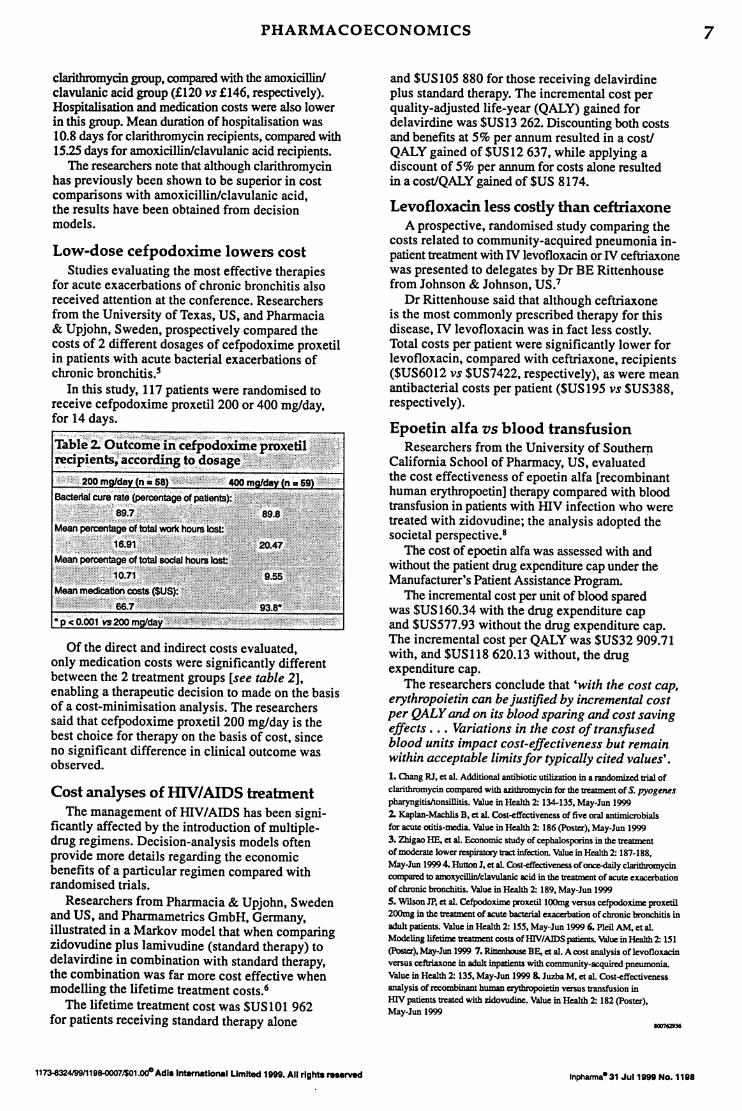
In this study, 117 patients were randomised to receive cefpodoxime proxetil 200 or 400 mg/day, for 14 days.
Of the direct and indirect costs evaluated, only medication costs were significantly different between the 2 treatment groups [see table 2], enabling a therapeutic decision to made on the basis of a cost-minimisation analysis. The researchers said that cefpodoxime proxetil 200 mglday is the best choice for therapy on the basis of cost, since no significant difference in clinical outcome was observed.
Cost analyses of HIVI AIDS treatment The management ofmV/AIDS has been signi
ficantly affected by the introduction of multipledrug regimens. Decision-analysis models often provide more details regarding the economic benefits of a particular regimen compared with randomised trials.
Researchers from Pharmacia & Upjobn, Sweden and US, and Pharmametrics GmbH, Germany, illustrated in a Markov model that when comparing zidovudine plus lamivudine (standard therapy) to delavirdine in combination with standard therapy, the combination was far more cost effective when modelling the lifetime treatment costs.6
The lifetime treatment cost was $USI0l 962 for patients receiving standard therapy alone
1173-832419911198-00071$01 .00" Adlelnternatlonal Limited 1999. All rlghte rnerved
and $USI05 880 for those receiving delavirdine plus standard therapy. The incremental cost per quality-adjusted life-year (QALY) gained for delavirdine was SUS 13 262. Discounting both costs and benefits at 5% per annum resulted in a cost! QALY gained of $USI2 637, while applying a discount of 5% per annum for costs alone resulted in a cost!QALY gained of SUS 8174.
Levofloxacin less costly than ceftriaxone A prospective, randomised study comparing the
costs related to community-acquired pneumonia inpatient treatment with IV levofloxacin or IV ceftriaxone was presented to delegates by Dr BE Rittenhouse from Johnson & Johnson, US.7
Dr Rittenhouse said that although ceftriaxone is the most commonly prescribed therapy for this disease, IV levofloxacin was in fact less costly. Total costs per patient were significantly lower for levofloxacin, compared with ceftriaxone, recipients ($US6012 vs $US7422, respectively), as were mean antibacterial costs per patient ($US 195 vs $US388, respectively).
Epoetin aIfa vs blood transfusion Researchers from the University of Southern
California School of Pharmacy, US, evaluated the cost effectiveness of epoetin alfa [recombinant human erythropoetin] therapy compared with blood transfusion in patients with mv infection who were treated with zidovudine; the analysis adopted the societal perspective.8
The cost of epoetin alia was assessed with and without the patient drug expenditure cap under the Manufacturer's Patient Assistance Program.
The incremental cost per unit of blood spared was $USI60.34 with the drug expenditure cap and $US577.93 without the drug expenditure cap. The incremental cost per QALY was $US32 909.71 with, and $US118 620.13 without, the drug expenditure cap.
The researchers conclude that 'with the cost cap, erythropoietin can be justified by incremental cost per QALYand on its blood sparing and cost saving effects . .. Variations in the cost of transfused blood units impact cost-effectiveness but remain within acceptable limits for typically cited values' . 1. Olang RJ. et al. Additional antibiotic utilization in a randomized 1rial of
c1arithromycin compared with azithromycin for the treatment of S. pyogent:s
pharyngitisltonsillitis. Value in Health 2: 134-135. May-JUD 1999
2. Kaplan-Machlis B. et al. CosHffectiveness of five oral antimicrobials
for acule otitis-media. Value in Health 2: 186 (Posler). May-JUD 1999
3. Zhigao HE. et al. Economic study of cephalosporins in the trca!ment ofmoderate lower respiratory tract infection. Value in Health 2: 187-188.
May-JUD 1999 4. Hutton J. et al. Cost-effectiveness of oncc-daily c1arithromycin compared to amoxycillinlclavulanic acid in the trcattnent of acule exacerbation
of chronic bronchitis. Value in Health 2: 189. May-JUD 1999
S. Wilson JP. et al. Cefpodoxime IXQxetil l00mg versus cefpodoxime proxetil 200mg in the trcattnent of acule bacIerial exacerbation of chronic bronchitis in
adult patients. Value in Health 2: 155. May-JUD 1999 6. PIeil AM, et al. Modeling lifetime trcattnent costs of lllV/AlDS paIients. Value in Health 2: 151
(Poster). May-Jun 1999 7. Rintnbowe BE, et al. A cost analysis of ievofloxacin versus ceftriaxone in adult inpatients with community-acquired pneumonia.
Value in Health 2: 135. May-JUD 1999 8. Juzba M. et al. Cost~ffectiveness analysis of recombinant human e:ythropoietin versus transfusion in mv patients treated with zidovudine. Value in Health 2: 182 (PoSIer).
May-JUD 1999
Inphanna- 31 Ju11999 No. 11118
7