infection prevention and control clostridium difficile policy clostridium... · clostridium...
TRANSCRIPT
Infection Prevention and Control
Clostridium difficile Policy
CDI Policy 2016 Page 2
Policy Title: Clostridium difficile Policy
Executive Summary:
Clostridium difficile infection is a potentially severe or fatal infection this policy details the measures required to reduce the risk to vulnerable patients and ensure their management is appropriate to ensure optimal care and improved outcomes.
Supersedes: Clostridium difficile policy 2015
Description of Amendment(s):
Updated to reflect National guidance and local policy
This policy will impact on: All clinical staff assessed as competent practitioners who undertake blood culture sampling
Financial Implications: None
Policy Area: Infection Prevention and Control Trust Wide
Document Reference:
ECT002554
Version Number: V5 Effective Date: August 2016
Issued By: Infection Prevention and Control Group
Review Date: July 2018
Authors: Lead Nurse Infection Prevention and Control
Impact Assessment Date:
August 2016
APPROVAL RECORD
Committees / Group Date
Consultation: Infection Prevention and Control Group
August 2016
Approved by: Date
Infection Prevention and Control Group
August 2016
Received for information:
CDI Policy 2016 Page 3
CONTENTS
Section Heading
Page
1 Introduction
4
2 Purpose
5
3 Definitions
6
4 Risk factors
6
5 Initial management of suspected cases 7
6 Procedure for informing results 8
7 CDI Management 9
8 Prevention of spread
10
9 Information for patients and carers 11
10 Period of increased incidence 11
11 Outbreak
12
12 Post infection reviews
12
13 Community management
13
14 Key Performance indicators 13
Appendix 1: Diarrhoea and/or vomiting risk assessment tool
15
Appendix 2: Bristol stool chart
16
References
17
Equality Impact Assessment
18
CDI Policy 2016 Page 4
1 Introduction Primary Clostridium difficile infection (CDI) is nearly always associated with, and triggered by, the use of antibiotics prescribed either to treat another condition, or given prophylactically. Clostridium difficile is a spore-forming organism that can survive in the healthcare environment and colonisation is usually acquired by ingestion after contact with a contaminated environment, equipment, other patients, or the hands of staff. However, there are approximately 3% of the population who are naturally colonised with the spores as part of their normal bowel flora.
CDI is a Gram positive, anaerobic, spore-forming organism implicated in CDI associated diarrhoea, and pseudomembranous colitis. The overgrowth of the organism within the large intestine and toxin production causes cellular damage and increased fluid accumulation in the gut. The main predisposing factors for CDI in adults are acquisition of the organism and exposure to antibiotics, notably with cephalosporins, quinolones, clindamycin and broad spectrum penicillin’s.
CDI occurs when the normal flora of the bowel is disrupted, usually as a consequence of treatment with broad spectrum antibiotics. CDI is more common in the over 65 age group (though any other age group may be susceptible). Patients may be colonised with Clostridium difficile without displaying symptoms. CDI may present with malaise, abdominal pain, nausea, anorexia, watery diarrhoea, low-grade fever, and peripheral leukocytosis. Colonoscopy reveals a non-specific diffuse or patchy erythematous colitis without pseudomembranes.
Pseudomembranous colitis (PMC), sigmoidoscopy reveals raised yellow plaques from 2-10mm in size scattered over the colorectal mucosa. Patients with PMC have a more serious illness than CDI, diarrhoea may also contain blood and mucous.
Recurrence of CDI occurs in 15-20% of patients after discontinuation of
treatment. Marsh et all study reported 33% was due to re-infection with a new strain and 67% due to relapse with the original strain. Life threatening symptoms develop in between 1.2%–3.2% of patients with CDI. This disease is a co-morbidity in frail elderly patients and can have a high patient mortality.
Outbreaks of infection can be prolonged and difficult to control. Large outbreaks of CDI associated with loss of life have occurred in healthcare facilities and it is therefore essential that the Trust takes appropriate action to minimise the occurrence of CDI and ensures robust management arrangements are in place at all times to prevent secondary spread.
1.1 Organisational Responsibilities
The Chief Executive has ultimate responsibility for the implementation and monitoring of the policies in use in the Trust. This responsibility may be delegated.
The Director of Nursing, Performance and Quality will take the lead responsibility for the development and implementation of this policy with support of the Lead Nurse Infection Prevention and Control and the Infection Prevention and Control Doctor.
The Director of Infection Prevention and Control (DIPC) provides assurance to the Board that strategies, to reduce avoidable health care infections have been effectively implemented across the organisation. The Director of Nursing, Performance & Quality is also the DIPC.
CDI Policy 2016 Page 5
The Consultant Microbiologists are responsible for the development and monitoring of a comprehensive antibiotic policy and for ensuring that all prescribers have access to support and guidance to enable them to prescribe with due caution and to prevent the inappropriate use of antibiotics
The Infection Prevention and Control Team (IPCT) will have responsibility for ensuring the policy is implemented and monitored across the Trust in addition they will ensure compliance with any national initiatives or directives. The team will also provide and support a sustainable programme of audit and education across the health economy. Inclusive:
- Prompt and effective identification of CDI patients and control of an outbreak of CDI.
- Education and training of staff in all aspects of the prevention and control of Clostridium difficile associated diarrhoea
- Supporting Clinical areas to undertake Post Infection Reviews (PIR) to ensure “no lapses of care” have occurred as part of a multidisciplinary team including representation from the Commissioners.
- Provide accurate monthly data reflecting current performance against the agreed objectives.
Antibiotic Pharmacist Team: Work in conjunction with the Consultant Microbiologist to ensure compliance with the antibiotic policy, providing suitable assurance data
Bed Managers: have responsibility for ensuring patients who are admitted with infectious conditions are placed in an appropriate environment (such as a side room) to reduce the risk of transmission to others in accordance with Trust Isolation Policy and other appropriate clinical pathways
Matrons/Senior Sisters: have responsibility for ensuring all staff comply with this policy ensuring early identification of patient’s risk factors in liaison with the Infection Prevention and Control Team. In addition participating in Multi-disciplinary patient reviews and Post Infection Reviews (PIR’s).
Clinicians: have responsibility for ensuring appropriate clinical reviews of patients, reviewing medications as appropriate to reduce the risk of CDI, in addition participating in Multi-disciplinary reviews and Post infection Reviews.
All Employees: must ensure they are compliant with Infection Prevention and Control including policies and understand the risk of CDI and strategies to mitigate the risk.
2 Purpose
This policy is intended to provide staff working within East Cheshire NHS Trust with a robust framework for managing patients with Clostridium difficile infection and preventing transmission to other patients. Integral to this is implementing planned programmes of care which:
Undertake appropriate risk assessments on patient placement including rapid Isolation of suspected/ confirmed cases as per flow chart (Appendix 1). This information must be recorded in the patient’s notes.
Implement patient clinical reviews to reduce the risk of CDI
Facilitate early Clinical and Laboratory diagnosis
Ensure on-going monitoring and symptom management
Reflect Antibiotic Stewardship policies and Guidelines
Enable completion of Post Infection Reviews to identify whether any” lapses in care” either directly contributing to the CDI or a “lapse in care” relating to failure in policy and procedures occurred.
CDI Policy 2016 Page 6
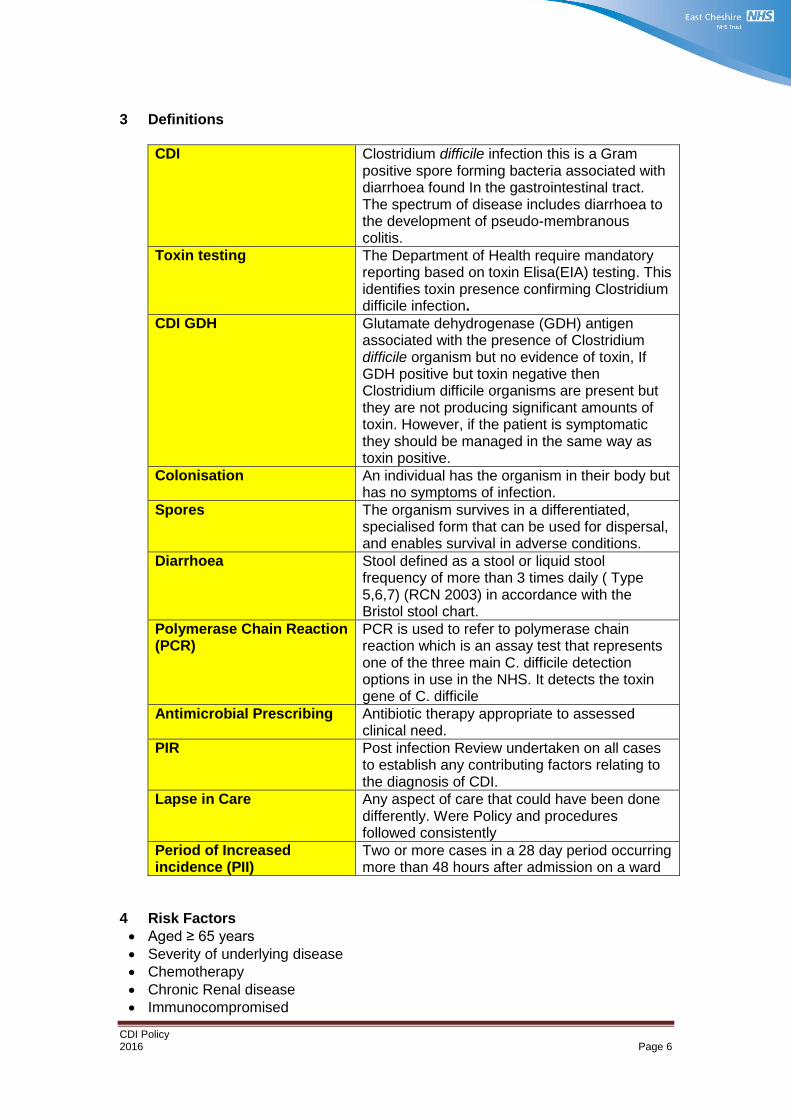
3 Definitions
CDI Clostridium difficile infection this is a Gram positive spore forming bacteria associated with diarrhoea found In the gastrointestinal tract. The spectrum of disease includes diarrhoea to the development of pseudo-membranous colitis.
Toxin testing The Department of Health require mandatory reporting based on toxin Elisa(EIA) testing. This identifies toxin presence confirming Clostridium difficile infection.
CDI GDH Glutamate dehydrogenase (GDH) antigen associated with the presence of Clostridium difficile organism but no evidence of toxin, If GDH positive but toxin negative then Clostridium difficile organisms are present but they are not producing significant amounts of toxin. However, if the patient is symptomatic they should be managed in the same way as toxin positive.
Colonisation An individual has the organism in their body but has no symptoms of infection.
Spores The organism survives in a differentiated, specialised form that can be used for dispersal, and enables survival in adverse conditions.
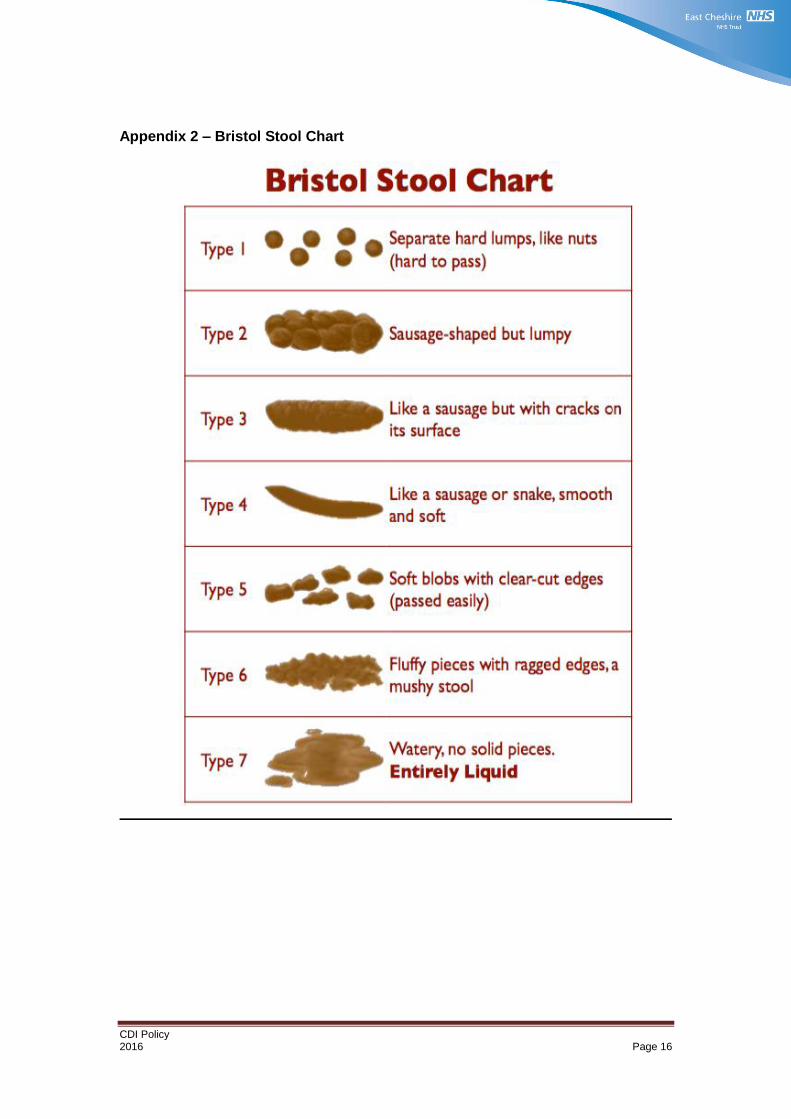
Diarrhoea Stool defined as a stool or liquid stool frequency of more than 3 times daily ( Type 5,6,7) (RCN 2003) in accordance with the Bristol stool chart.
Polymerase Chain Reaction (PCR)
PCR is used to refer to polymerase chain reaction which is an assay test that represents one of the three main C. difficile detection options in use in the NHS. It detects the toxin gene of C. difficile
Antimicrobial Prescribing Antibiotic therapy appropriate to assessed clinical need.
PIR Post infection Review undertaken on all cases to establish any contributing factors relating to the diagnosis of CDI.
Lapse in Care Any aspect of care that could have been done differently. Were Policy and procedures followed consistently
Period of Increased incidence (PII)
Two or more cases in a 28 day period occurring more than 48 hours after admission on a ward
4 Risk Factors
Aged ≥ 65 years
Severity of underlying disease
Chemotherapy
Chronic Renal disease
Immunocompromised
CDI Policy 2016 Page 7
Patients undertaking gastrointestinal procedures
Enteral feeding
Proton Pump inhibitors (Anti-Ulcer Drugs) and H2 antagonists.
Recent healthcare intervention
Antibiotic therapy- Almost all cases of CDI will have a recent history of antibiotics (NHS England 2016).
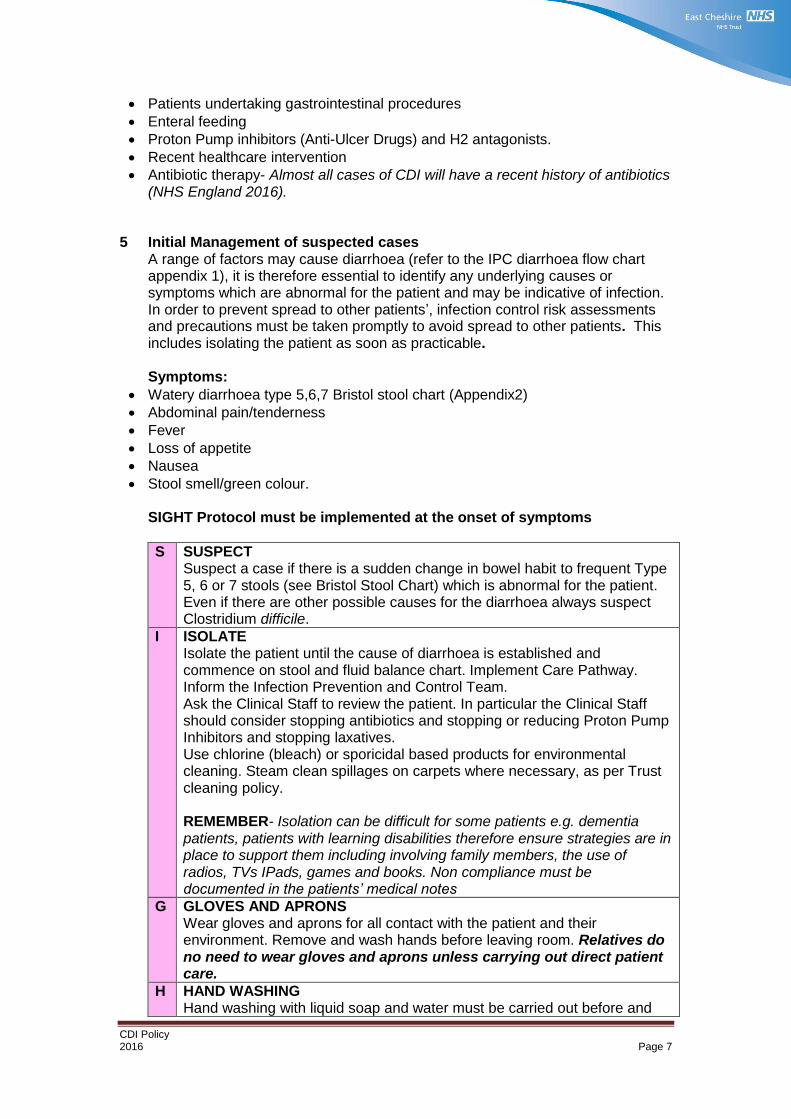
5 Initial Management of suspected cases
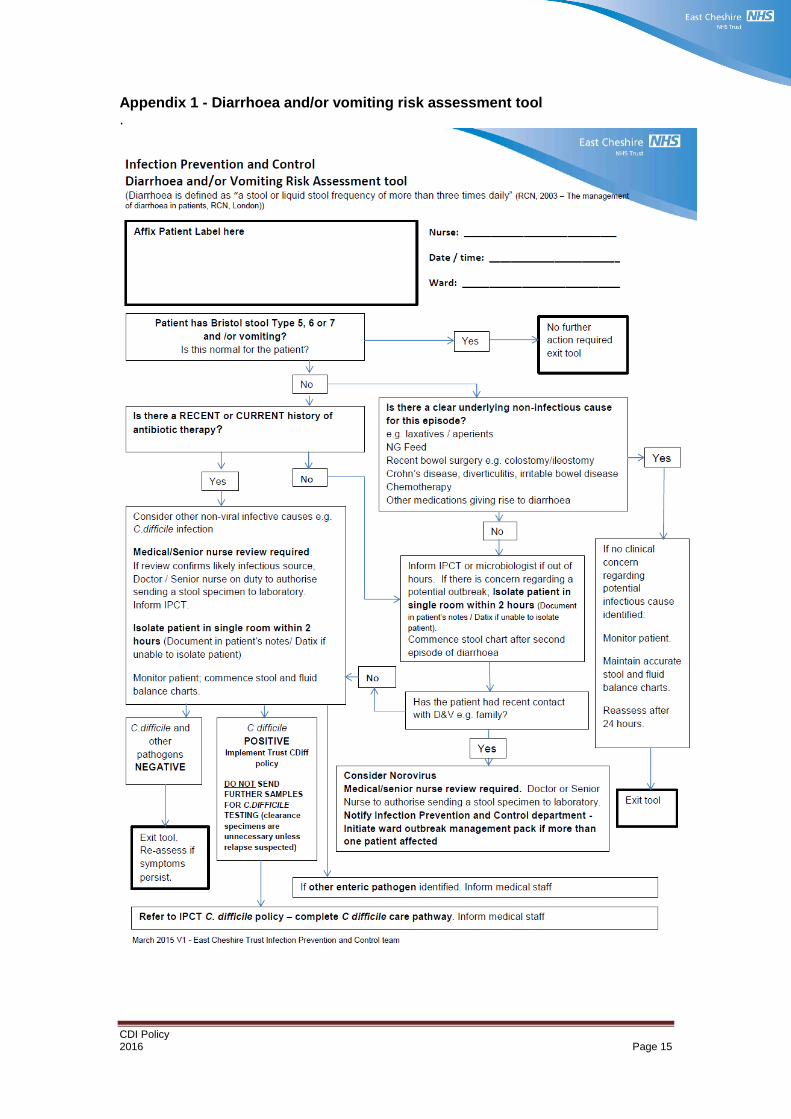
A range of factors may cause diarrhoea (refer to the IPC diarrhoea flow chart appendix 1), it is therefore essential to identify any underlying causes or symptoms which are abnormal for the patient and may be indicative of infection. In order to prevent spread to other patients’, infection control risk assessments and precautions must be taken promptly to avoid spread to other patients. This includes isolating the patient as soon as practicable.
Symptoms:
Watery diarrhoea type 5,6,7 Bristol stool chart (Appendix2)
Abdominal pain/tenderness
Fever
Loss of appetite
Nausea
Stool smell/green colour.
SIGHT Protocol must be implemented at the onset of symptoms
S SUSPECT Suspect a case if there is a sudden change in bowel habit to frequent Type 5, 6 or 7 stools (see Bristol Stool Chart) which is abnormal for the patient. Even if there are other possible causes for the diarrhoea always suspect Clostridium difficile.
I ISOLATE Isolate the patient until the cause of diarrhoea is established and commence on stool and fluid balance chart. Implement Care Pathway. Inform the Infection Prevention and Control Team. Ask the Clinical Staff to review the patient. In particular the Clinical Staff should consider stopping antibiotics and stopping or reducing Proton Pump Inhibitors and stopping laxatives. Use chlorine (bleach) or sporicidal based products for environmental cleaning. Steam clean spillages on carpets where necessary, as per Trust cleaning policy. REMEMBER- Isolation can be difficult for some patients e.g. dementia patients, patients with learning disabilities therefore ensure strategies are in place to support them including involving family members, the use of radios, TVs IPads, games and books. Non compliance must be documented in the patients’ medical notes
G GLOVES AND APRONS Wear gloves and aprons for all contact with the patient and their environment. Remove and wash hands before leaving room. Relatives do no need to wear gloves and aprons unless carrying out direct patient care.
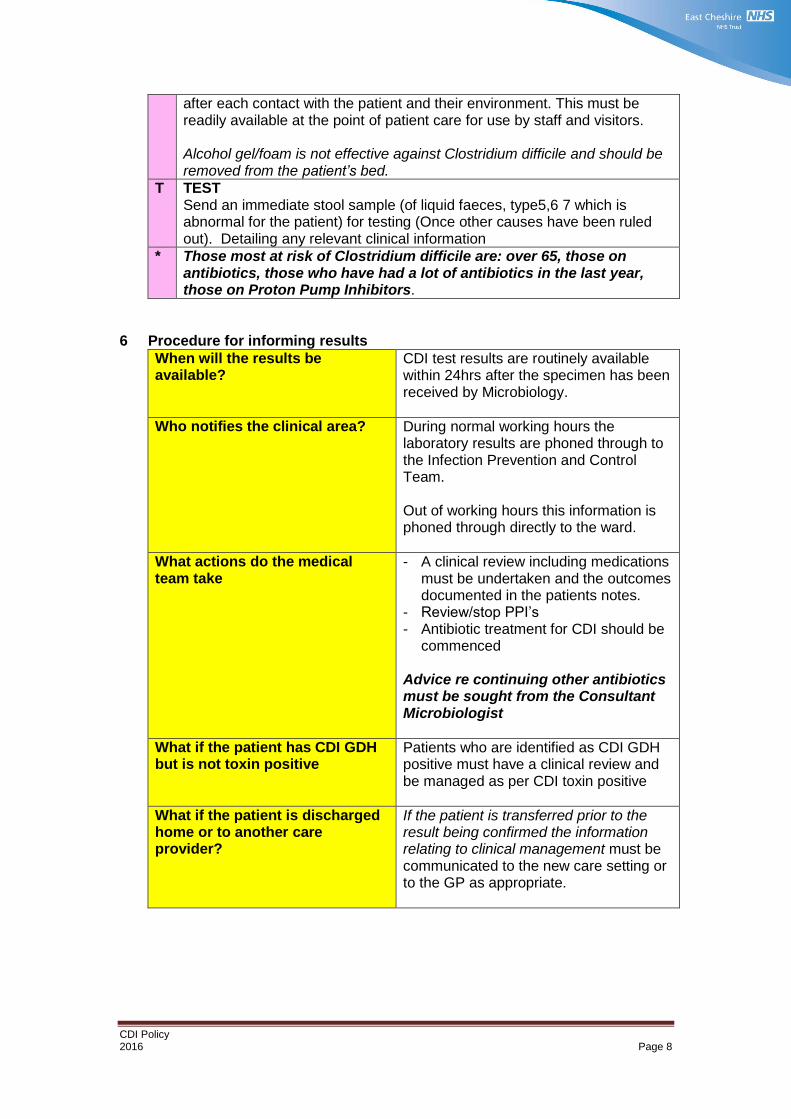
H HAND WASHING Hand washing with liquid soap and water must be carried out before and
CDI Policy 2016 Page 8
after each contact with the patient and their environment. This must be readily available at the point of patient care for use by staff and visitors. Alcohol gel/foam is not effective against Clostridium difficile and should be removed from the patient’s bed.
T TEST Send an immediate stool sample (of liquid faeces, type5,6 7 which is abnormal for the patient) for testing (Once other causes have been ruled out). Detailing any relevant clinical information
* Those most at risk of Clostridium difficile are: over 65, those on antibiotics, those who have had a lot of antibiotics in the last year, those on Proton Pump Inhibitors.
6 Procedure for informing results
When will the results be available?
CDI test results are routinely available within 24hrs after the specimen has been received by Microbiology.
Who notifies the clinical area? During normal working hours the laboratory results are phoned through to the Infection Prevention and Control Team. Out of working hours this information is phoned through directly to the ward.
What actions do the medical team take
- A clinical review including medications must be undertaken and the outcomes documented in the patients notes.
- Review/stop PPI’s - Antibiotic treatment for CDI should be
commenced Advice re continuing other antibiotics must be sought from the Consultant Microbiologist
What if the patient has CDI GDH but is not toxin positive
Patients who are identified as CDI GDH positive must have a clinical review and be managed as per CDI toxin positive
What if the patient is discharged home or to another care provider?
If the patient is transferred prior to the result being confirmed the information relating to clinical management must be communicated to the new care setting or to the GP as appropriate.
CDI Policy 2016 Page 9
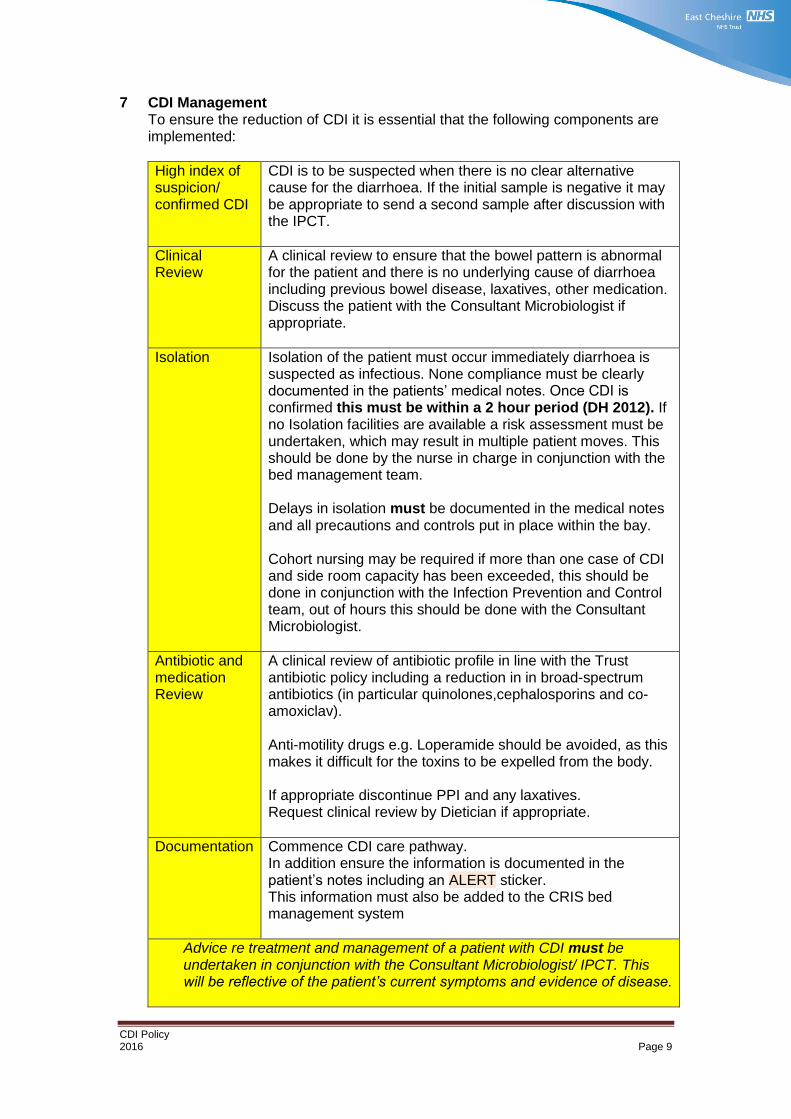
7 CDI Management To ensure the reduction of CDI it is essential that the following components are implemented:
High index of suspicion/ confirmed CDI
CDI is to be suspected when there is no clear alternative cause for the diarrhoea. If the initial sample is negative it may be appropriate to send a second sample after discussion with the IPCT.
Clinical Review
A clinical review to ensure that the bowel pattern is abnormal for the patient and there is no underlying cause of diarrhoea including previous bowel disease, laxatives, other medication. Discuss the patient with the Consultant Microbiologist if appropriate.
Isolation Isolation of the patient must occur immediately diarrhoea is suspected as infectious. None compliance must be clearly documented in the patients’ medical notes. Once CDI is confirmed this must be within a 2 hour period (DH 2012). If no Isolation facilities are available a risk assessment must be undertaken, which may result in multiple patient moves. This should be done by the nurse in charge in conjunction with the bed management team. Delays in isolation must be documented in the medical notes and all precautions and controls put in place within the bay. Cohort nursing may be required if more than one case of CDI and side room capacity has been exceeded, this should be done in conjunction with the Infection Prevention and Control team, out of hours this should be done with the Consultant Microbiologist.
Antibiotic and medication Review
A clinical review of antibiotic profile in line with the Trust antibiotic policy including a reduction in in broad-spectrum antibiotics (in particular quinolones,cephalosporins and co-amoxiclav). Anti-motility drugs e.g. Loperamide should be avoided, as this makes it difficult for the toxins to be expelled from the body. If appropriate discontinue PPI and any laxatives. Request clinical review by Dietician if appropriate.
Documentation Commence CDI care pathway. In addition ensure the information is documented in the patient’s notes including an ALERT sticker. This information must also be added to the CRIS bed management system
Advice re treatment and management of a patient with CDI must be undertaken in conjunction with the Consultant Microbiologist/ IPCT. This will be reflective of the patient’s current symptoms and evidence of disease.
CDI Policy 2016 Page 10
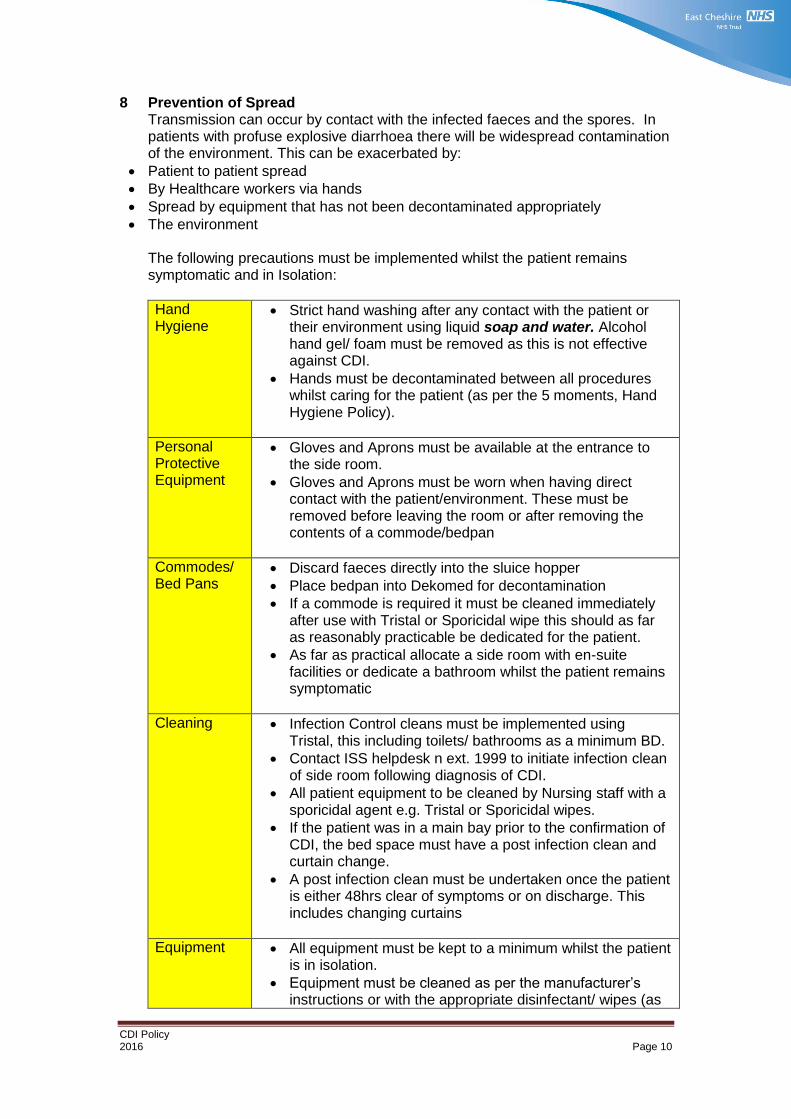
8 Prevention of Spread Transmission can occur by contact with the infected faeces and the spores. In patients with profuse explosive diarrhoea there will be widespread contamination of the environment. This can be exacerbated by:
Patient to patient spread
By Healthcare workers via hands
Spread by equipment that has not been decontaminated appropriately
The environment
The following precautions must be implemented whilst the patient remains symptomatic and in Isolation:
Hand Hygiene
Strict hand washing after any contact with the patient or their environment using liquid soap and water. Alcohol hand gel/ foam must be removed as this is not effective against CDI.
Hands must be decontaminated between all procedures whilst caring for the patient (as per the 5 moments, Hand Hygiene Policy).
Personal Protective Equipment
Gloves and Aprons must be available at the entrance to the side room.
Gloves and Aprons must be worn when having direct contact with the patient/environment. These must be removed before leaving the room or after removing the contents of a commode/bedpan
Commodes/ Bed Pans
Discard faeces directly into the sluice hopper
Place bedpan into Dekomed for decontamination
If a commode is required it must be cleaned immediately after use with Tristal or Sporicidal wipe this should as far as reasonably practicable be dedicated for the patient.
As far as practical allocate a side room with en-suite facilities or dedicate a bathroom whilst the patient remains symptomatic
Cleaning Infection Control cleans must be implemented using Tristal, this including toilets/ bathrooms as a minimum BD.
Contact ISS helpdesk n ext. 1999 to initiate infection clean of side room following diagnosis of CDI.
All patient equipment to be cleaned by Nursing staff with a sporicidal agent e.g. Tristal or Sporicidal wipes.
If the patient was in a main bay prior to the confirmation of CDI, the bed space must have a post infection clean and curtain change.
A post infection clean must be undertaken once the patient is either 48hrs clear of symptoms or on discharge. This includes changing curtains
Equipment All equipment must be kept to a minimum whilst the patient is in isolation.
Equipment must be cleaned as per the manufacturer’s instructions or with the appropriate disinfectant/ wipes (as
CDI Policy 2016 Page 11
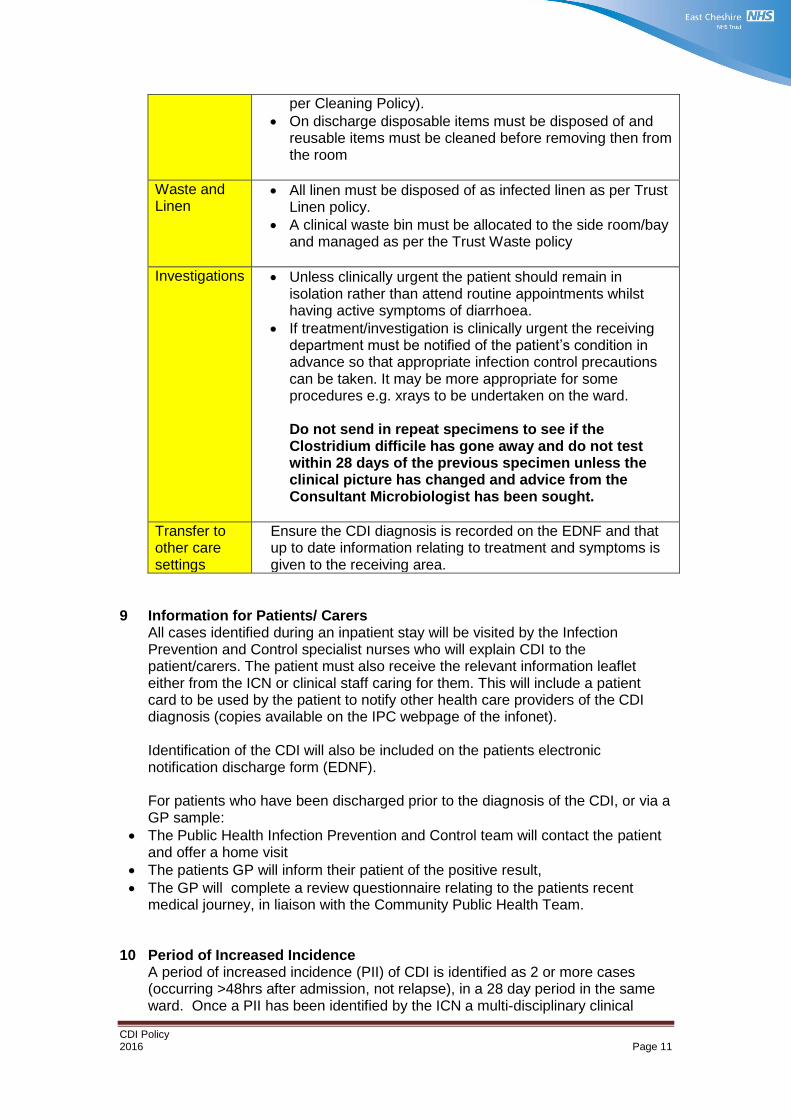
per Cleaning Policy).
On discharge disposable items must be disposed of and reusable items must be cleaned before removing then from the room
Waste and Linen
All linen must be disposed of as infected linen as per Trust Linen policy.
A clinical waste bin must be allocated to the side room/bay and managed as per the Trust Waste policy
Investigations Unless clinically urgent the patient should remain in isolation rather than attend routine appointments whilst having active symptoms of diarrhoea.
If treatment/investigation is clinically urgent the receiving department must be notified of the patient’s condition in advance so that appropriate infection control precautions can be taken. It may be more appropriate for some procedures e.g. xrays to be undertaken on the ward. Do not send in repeat specimens to see if the Clostridium difficile has gone away and do not test within 28 days of the previous specimen unless the clinical picture has changed and advice from the Consultant Microbiologist has been sought.
Transfer to other care settings
Ensure the CDI diagnosis is recorded on the EDNF and that up to date information relating to treatment and symptoms is given to the receiving area.
9 Information for Patients/ Carers All cases identified during an inpatient stay will be visited by the Infection Prevention and Control specialist nurses who will explain CDI to the patient/carers. The patient must also receive the relevant information leaflet either from the ICN or clinical staff caring for them. This will include a patient card to be used by the patient to notify other health care providers of the CDI diagnosis (copies available on the IPC webpage of the infonet). Identification of the CDI will also be included on the patients electronic notification discharge form (EDNF).
For patients who have been discharged prior to the diagnosis of the CDI, or via a GP sample:
The Public Health Infection Prevention and Control team will contact the patient and offer a home visit
The patients GP will inform their patient of the positive result,
The GP will complete a review questionnaire relating to the patients recent medical journey, in liaison with the Community Public Health Team.
10 Period of Increased Incidence
A period of increased incidence (PII) of CDI is identified as 2 or more cases (occurring >48hrs after admission, not relapse), in a 28 day period in the same ward. Once a PII has been identified by the ICN a multi-disciplinary clinical
CDI Policy 2016 Page 12
review will be undertaken. The IPCN will undertake additional auditing, enhanced cleaning. Enhanced monitoring of antibiotic profiles will be implemented by the antibiotic pharmacists.
11 Outbreak
An outbreak of CDI is defined as 2 or more cases caused by the same strain related in time and place over a defined period based on the date of onset of the first case (DH2009). This will be managed as per the Trust Outbreak Policy.
12 Post infection Reviews
In order to examine the effectiveness of measures implemented and learn any lessons to improve patient safety each case of CDI will be reviewed by a peer review panel consisting of as a minimum:
Consultant Microbiologist/ Deputy
Lead Nurse IPC
Clinical Advanced Specialist Practitioner IPC/ Deputy
Senior Sister/ Deputy
Consultant/ Deputy
Matron
Antibiotic Pharmacist
Quality representative Clinical Commissioning group
Dietician
The purpose of this review is to identify any “lapses in care” as per NHS England’s requirements (NHS 2016). This includes establishing the following:
Were there any aspects of care that could have been done differently
Failures in policy and procedures which directly contributed to the CDI case, for example failure to follow the Trust antibiotic policy
Failures in policy and procedures which although not directly contributing to the CDI had an impact on the patients care delivery, for example failure to isolate on the identification of diarrhoea.
The Panel will make a final decision to determine “preventability” (NHS England 2016) based on the following:
Identification of any lapse in care that contributed to the CDI
Identification of lapses in care not contributing to the CDI
If the case was identified as “not preventable” a clear rationale to support this decision must be documented. Outcomes of the PIR will be reported to the Infection Prevention and Control committee and the appropriate Service Line SQS who will monitor any action plans.
In addition all cases of inpatient related CDI will be reviewed by a multi-disciplinary team to ensure optimal care has been provided and that the patient treatment has been effective; this group will consist as a minimum:
Consultant Microbiologist
Consultant Gastroenterologist
Lead Nurse Infection Prevention and Control
Deputy Director of Corporate affairs and Governance
Matron
CDI Policy 2016 Page 13
Clinical Advanced Specialist Practitioner IPC
Antibiotic Pharmacist
Dietician All CDI PIR will be subject to the Trust check and challenge process 13 Community Management
Patients who develop sudden onset diarrhoea which is abnormal for them should be reviewed against the SIGHT principle above and reviewed with the GP as appropriate
There should be no restrictions on the discharge or transfer of patients who have CDI. If symptoms remain the individual must have been deemed medically fit for discharge. Once the patient has clinically recovered they do not pose a risk to others even if they continue to carry Clostridium difficile in their stool
Encouragement should be given regarding normal personal hygiene, including hand washing with soap and water. Whilst symptomatic it is recommended the patient has their own identified towel. Additionally, surfaces in the bathroom, kitchen and other areas should be cleaned on a regular basis with detergent /disinfection
Soiled linen should be washed as a separate load to other items using the hottest temperature for the fabric, (ideally at a temperature of 60 degrees)
Crockery and cutlery should be washed as normal
It is important that whilst symptomatic, the patient is encouraged to drink plenty of water to prevent dehydration
If the patient is symptomatic visitors should be encouraged to maintain good standards of hand hygiene however they do not need to wear gloves and aprons unless giving clinical care
Repeat samples are not required unless a reoccurrence is suspected; further advice can be obtained from the IPCT or Consultant Microbiologist
All cases of CDI are followed up after 30 days as per DH guidelines (DH 2009) by the IPCT.
New Cases of CDI identified in the community are managed by the GP and will be subject to a PIR by the Public Health Infection Control Nurses and the GP. This review is subject to an independent review by the Consultant Microbiologist and the Lead Nurse IPC who report into the CCG Quality forums.
14 Key Performance indicators
The following performance indicators will be monitored through the Infection Prevention and Control Committee and the Infection Prevention and Control Operational Group.
National Requirement
NHS England set an annual trajectory for CDI; this is reported on each individual case through the HCAI data capture system.
Local Requirements
The Infection Prevention and Control Antibiotic compliance is monitored and audited by the antibiotic ward rounds undertaken by the Consultant Microbiologist and the Antibiotic pharmacist. Initial feedback is given to the clinicians on the day and feedback to the primary Consultant. In addition
CDI Policy 2016 Page 14
quarterly reports will be submitted to the Medicines management group and the Infection Prevention and Control Group.
The PIR process reviews compliance with policy requirements as part of the evidence gathering process variations or failures in policy requirements will be reported to the service lines SQS and to the Infection Prevention and Control Operational Group
Isolation and the use of PPE are monitored through the IPCT audit programme this includes hand hygiene verification audits. The audits process also includes hand hygiene verification audits.
This policy should be read in conjunction with
Universal precautions Policy
Hand Hygiene Policy
Isolation Policy
Outbreak Policy
CDI Policy 2016 Page 15
Appendix 1 - Diarrhoea and/or vomiting risk assessment tool .
CDI Policy 2016 Page 16
Appendix 2 – Bristol Stool Chart
CDI Policy 2016 Page 17
References Department of Health (2015) - Health and Social Care Act (2008): Code of Practice on the prevention and control of Infections and related guidance. DH, London. Available from
https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/216227/dh_123923.pdf Department of Health (2010) Clostridium difficile Infection: How to deal with the problem. London DH,2010. Marsh J,W. Arora R, Schlackman L. Shutt K,A. Curry S. and Harrison L,H. Association of Relapse of Clostridium difficile Disease with BI/NAPI/027. Journal of Clinical Microbiology. Available from http://jcm.asm.org NICE (2012) Prevention of Healthcare Associated Infection in Primary and Community Care. NHS England (2016). Clostridium difficile infection objectives for NHS Organisations in 2016/17 and guidance on sanction implementation.
CDI Policy 2016 Page 18
Equality Analysis (Impact assessment) Please START this assessment BEFORE writing your policy, procedure, proposal, strategy or service so that you can identify any adverse impacts and include action to mitigate these in your finished policy, procedure, proposal, strategy or service. Use it to help you develop fair and equal services. Eg. If there is an impact on Deaf people, then include in the policy how Deaf people will have equal access. 1. What is being assessed?
Clostridium difficile policy
Details of person responsible for completing the assessment:
Name: Anita Swaine Position: Lead Nurse
Team/service: Infection Prevention and Control
State main purpose or aim of the policy, procedure, proposal, strategy or service:
(usually the first paragraph of what you are writing. Also include details of legislation, guidance, regulations etc. which have shaped or informed the document)
Clostridium difficile infection is a potentially severe or fatal infection this policy details the measures required to reduce the risk to vulnerable patients and ensure their management is appropriate to ensure optimal care and improved outcomes
2. Consideration of Data and Research To carry out the equality analysis you will need to consider information about the people who use the service and the staff that provide it. Think about the information below – how does this apply to your policy, procedure, proposal, strategy or service 2.1 Give details of RELEVANT information available that gives you an understanding of who will be affected by this document Cheshire East (CE) covers Eastern Cheshire CCG and South Cheshire CCG. Cheshire West & Chester (CWAC) covers Vale Royal CCG and Cheshire West CCG. In 2011, 370,100 people resided in CE and 329,608 people resided in CWAC.
Age: East Cheshire and South Cheshire CCG’s serve a predominantly older population than the national average, with 19.3% aged over 65 (71,400 people) and 2.6% aged over 85 (9,700 people). Vale Royal CCGs registered population in general has a younger age profile compared to the CWAC average, with 14% aged over 65 (14,561 people) and 2% aged over 85 (2,111 people).
CDI Policy 2016 Page 19
Since the 2001 census the number of over 65s has increased by 26% compared with 20% nationally. The number of over 85s has increased by 35% compared with 24% nationally. Race:
In 2011, 93.6% of CE residents, and 94.7% of CWAC residents were White British.
5.1% of CE residents, and 4.9% of CWAC residents were born outside the UK – Poland and India being the most common.
3% of CE households have members for whom English is not the main language (11,103 people) and 1.2% of CWAC households have no people for whom English is their main language.
Gypsies & travellers – estimated 18,600 in England in 2011. Gender:
In 2011, c. 49% of the population in both CE and CWAC were male and 51% female. For CE, the assumption from national figures is that 20 per 100,000 are likely to be transgender and for CWAC 1,500 transgender people will be living in the CWAC area.
Disability:
In 2011, 7.9% of the population in CE and 8.7% in CWAC had a long term health problem or disability.
In CE, there are c.4500 people aged 65+ with dementia, and c.1430 aged 65+ with dementia in CWAC. 1 in 20 people over 65 has a form of dementia.
Over 10 million (c. 1 in 6) people in the UK have a degree of hearing impairment or deafness.
C. 2 million people in the UK have visual impairment, of these around 365,000 are registered as blind or partially sighted.
In CE, it is estimated that around 7000 people have learning disabilities and 6500 people in CWAC.
Mental health – 1 in 4 will have mental health problems at some time in their lives.
Sexual Orientation:
CE - In 2011, the lesbian, gay, bisexual and transgender (LGBT) population in CE was estimated at18,700, based on assumptions that 5-7% of the population are likely to be lesbian, gay or bisexual and 20 per 100,000 are likely to be transgender (The Lesbian & Gay Foundation).
CWAC - In 2011, the LGBT population in CWAC is unknown, but in 2010 there were c. 20,000 LGB people in the area and as many as 1,500 transgender people residing in CWAC.
Religion/Belief: The proportion of CE people classing themselves as Christian has fallen from 80.3% in 2001 to 68.9% In 2011 and in CWAC a similar picture from 80.7% to
CDI Policy 2016 Page 20
70.1%, the proportion saying they had no religion doubled in both areas from around 11%-22%.
Christian: 68.9% of Cheshire East and 70.1% of Cheshire West & Chester
Sikh: 0.07% of Cheshire East and 0.1% of Cheshire West & Chester
Buddhist: 0.24% of Cheshire East and 0.2% of Cheshire West & Chester
Hindu: 0.36% of Cheshire East and 0.2% of Cheshire West & Chester
Jewish: 0.16% of Cheshire East and 0.1% of Cheshire West & Chester
Muslim: 0.66% of Cheshire East and 0.5% of Cheshire West & Chester
Other: 0.29% of Cheshire East and 0.3% of Cheshire West & Chester
None: 22.69%of Cheshire East and 22.0% of Cheshire West & Chester
Not stated: 6.66% of Cheshire East and 6.5% of Cheshire West & Chester
Carers:
In 2011, nearly 11% (40,000) of the population in CE are unpaid carers and just over 11% (37,000) of the population in CWAC.
2.2 Evidence of complaints on grounds of discrimination: (Are there any complaints or concerns raised either from patients or staff (grievance) relating to the policy, procedure, proposal, strategy or service or its effects on different groups?)
None.
2.3 Does the information gathered from 2.1 – 2.3 indicate any negative impact as a result of this document?
None
3. Assessment of Impact Now that you have looked at the purpose, etc. of the policy, procedure, proposal, strategy or service (part 1) and looked at the data and research you have (part 2), this section asks you to assess the impact of the policy, procedure, proposal, strategy or service on each of the strands listed below.
CDI Policy 2016 Page 21
RACE: From the evidence available does the policy, procedure, proposal, strategy or service affect, or have the potential to affect, racial groups differently? Yes No x Explain your response: In order to explain the requirements of the policy to people whose first language is not English, e.g. family members caring for a patient, staff will follow the interpretation policy. ______________________________________________________________ GENDER (INCLUDING TRANSGENDER): From the evidence available does the policy, procedure, proposal, strategy or service affect, or have the potential to affect, different gender groups differently? Yes No x Explain your response: No impacts identified. ______________________________________________________________ DISABILITY From the evidence available does the policy, procedure, proposal, strategy or service affect, or have the potential to affect, disabled people differently? Yes x No Explain your response: For disabled patients, assistance and/or communication support may be required to inform about and carry out good hand hygiene to prevent the spread of CDI ______________________________________________________________ AGE: From the evidence available does the policy, procedure, proposal, strategy or service, affect, or have the potential to affect, age groups differently? Yes No x Explain your response Assistance will be given to ensure the correct application and management of treatment with the support of family and care teams as required _____________________________________________________________ LESBIAN, GAY, BISEXUAL: From the evidence available does the policy, procedure, proposal, strategy or service affect, or have the potential to affect, lesbian, gay or bisexual groups differently? Yes No x Explain your response: No impact identified-______________________________________________________________ RELIGION/BELIEF: From the evidence available does the policy, procedure, proposal, strategy or service affect, or have the potential to affect, religious belief groups differently? Yes No X Explain your response: No impacts identified. ______________________________________________________________
CDI Policy 2016 Page 22
CARERS: From the evidence available does the policy, procedure, proposal, strategy or service affect, or have the potential to affect, carers differently? Yes No x Explain your response: Information will be provided to carers about any additional requirements to care. Clinical staff will ensure that information is given to the carers to ensure they understand measures required, this can be both verbal and written
OTHER: EG Pregnant women, people in civil partnerships, human rights issues. From the evidence available does the policy, procedure, proposal, strategy or service affect, or have the potential to affect any other groups differently? Yes No x Explain your response: No other impacts identified-_____________________________________________________________ 4. Safeguarding Assessment - CHILDREN
a. Is there a direct or indirect impact upon children? Yes No x
b. If yes please describe the nature and level of the impact (consideration to be given to all children; children in a specific group or area, or individual children. As well as consideration of impact now or in the future; competing / conflicting impact between different groups of children and young people:
c. If no please describe why there is considered to be no impact / significant impact on children. Management is the same for children and adults
5. Relevant consultation Having identified key groups, how have you consulted with them to find out their views and that the made sure that the policy, procedure, proposal, strategy or service will affect them in the way that you intend? Have you spoken to staff groups, charities, national organisations etc.?
Consultation has occurred through the Infection Prevention and Control group which is multidisciplinary and includes a member of the public.
6. Date completed: 1/09/2016 Review Date: 1/7/2018 7. Any actions identified: Have you identified any work which you will need to do in the future to ensure that the document has no adverse impact?
Action Lead Date to be Achieved
8. Approval: At this point, you should forward the template to the Trust Equality and Diversity Lead [email protected]
CDI Policy 2016 Page 23
Approved by Trust Equality and Diversity Lead:
Date: 7.9.16