infection control overview: hiv and other blood-borne pathogens session 2: infection control basics
TRANSCRIPT

Infection Control Overview: HIV and other Blood-Borne
PathogensSession 2: Infection Control Basics
2: Infection Control Overview - HIV Slide 2
Learning Objectives
This session deals with the control of HIV and other blood-borne pathogens
By the end of session 2, participants will be able to:
Protect themselves and others from HIV and other blood-borne pathogens
Describe what to do after a needle prick or if blood and/or body fluids get into the eyes or mouth
Provide input to the Hospital Infection Control Committee (HICC) on infection control procedures

2: Infection Control Overview - HIV Slide 3
Discussion: Hepatitis B Immunisation
Are you familiar with the current policy for Hep B vaccination before and after exposure?
What is the procedure involved for a new hospital employee under this policy?
What are the contraindications for the Hep B vaccination?

2: Infection Control Overview - HIV Slide 4
Protecting Yourself from Blood-Borne Pathogens
2: Infection Control Overview - HIV Slide 5
Protecting Yourself from Blood-Borne Pathogens (cont’d) Wear gloves
Don’t recap needles
Complete 3 doses of Hep B vaccine
Eliminate unnecessary injections
Dispose of sharps immediately after use to minimise handling that increases risk of needlesticks
Substitute safer devices or tools whenever possible
Report needlesticks

2: Infection Control Overview - HIV Slide 6
Protecting Yourself from Blood-Borne Pathogens (cont’d)Which pathogen is most likely to be transmitted from
a needle used on an infectious patient?
HIV
HEP B
HEP C
2: Infection Control Overview - HIV Slide 7
HIV: 3 Infections per 1,000 Sticks with a HIV+ Needle
000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000
2: Infection Control Overview - HIV Slide 8
Hepatitis C: 18 Persons per 1,000Needle-sticks 0000000000000000000000000000000000000000000000000000000000000000
00000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000
2: Infection Control Overview - HIV Slide 9
Hepatitis B is Most Infectious
000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000000
2: Infection Control Overview - HIV Slide 10
Why is Hep B Virus More Infectious than HIV? Viral concentration per mL
Virulence factor
Incubation period
2: Infection Control Overview - HIV Slide 11
Protect Yourself! Get a Hepatitis B Vaccination and keep your Vaccine Record
3 doses of Hepatitis B vaccine protect most people for a lifetime
The next dose at this facility will be given on _______________
Will you be there with your staff?

2: Infection Control Overview - HIV Slide 12
Prevention of Injury Due to Sharps is Critical
In some hospitals in India, staff report 1-2 sharps injuries per person per year
Do you know how, when, with what device and to whom most sharps injuries occur?

2: Infection Control Overview - HIV Slide 13
Exercise 2.1: Sharps Injury Role Play
Instructions:
Divide into groups of 5
Decide who will play the roles of supervisor, health worker, and observer
The health care worker will pretend that they have just received a sharps injury
The supervisor should interview the worker about the injury using worksheet 2.1 as a guide
The observer will report back to the larger group on what took place

2: Infection Control Overview - HIV Slide 14
Discussion: Sharps Reporting Form
Is this Proforma sufficient for reporting sharps injuries? Why or why not?
What changes could be made to current reporting procedures to make it easier to report injuries?
Why do you think injuries are not always reported?

2: Infection Control Overview - HIV Slide 15
What do We Mean by “Sharps”
Needles and syringes
Glass capillary tubes
Glass ampoules
Vacutainer needles
Suture needles, IV introducers and IV flushes
Test tubes and glass apparati used in lab

2: Infection Control Overview - HIV Slide 16
Eliminate Needle use When Possible
Do not use an injection or IV medicine when an oral medicine will do!
Do not place a venting needle into an IV; this increases the risk of contamination and needlesticks

2: Infection Control Overview - HIV Slide 17
Substitute Metal or Plastic for Glass when Possible
Staff are discussing using metal tubes for pulmonary drainage rather than glass to help prevent accidents
2: Infection Control Overview - HIV Slide 18
Sharps Injuries are Likely to Occur…
During recapping needles
During blood draws
During IV insertion & removal
When handling needles (taking them apart, picking up a dirty syringe, dumping containers, etc.)
When disposing of sharps
During waste collection and processing
During breakages

2: Infection Control Overview - HIV Slide 19
Safe Handling of Sharps
Wear gloves when drawing blood or handling sharps—double glove for surgery
Don’t recap!
Don’t bend or break needles
Never place used sharps on tables, beds, furniture
Put used sharps immediately into a sharps container
2: Infection Control Overview - HIV Slide 20
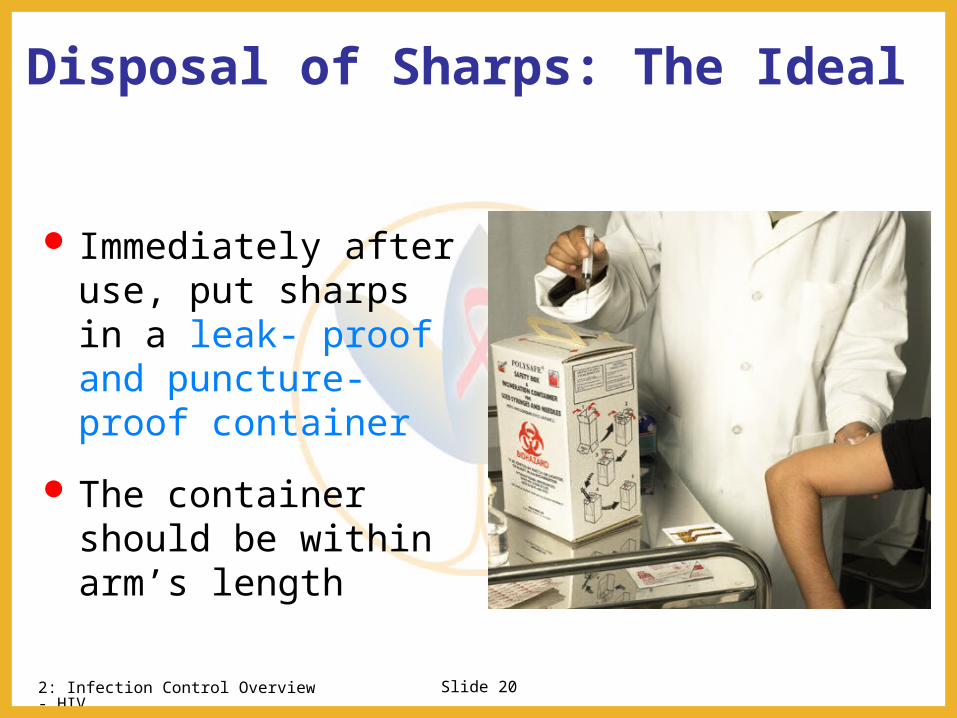
Disposal of Sharps: The Ideal
Immediately after use, put sharps in a leak- proof and puncture-proof container
The container should be within arm’s length

2: Infection Control Overview - HIV Slide 21
Sharps Disposal at GHTM
Needle destroyer
Disposal of sharps in blue bins
What are some potential problems with the current sharps disposal system?

2: Infection Control Overview - HIV Slide 22
Sharps Disposal (cont’d)
Disposal containers should be placed at all points of use
Disposal bin should be rigid and should be leak and puncture proof
Separate sharps from other waste so laundry workers or waste disposal staff do not get needlesticks
Empty sharps containers when they are ¾ full

2: Infection Control Overview - HIV Slide 23
Danger!
Open containers of used needles like this put staff at risk each time they put a hand in to pick up one
Keep your ward free of used sharps

2: Infection Control Overview - HIV Slide 24
Remember this Procedure…
If a needle pricks you or blood and/or body fluids enter your eye(s) or mouth
Wash wounds with soap and water
Flush eyes and mouth with water
Check the patient record to see if the patient is HIV+, HIV- , or untested
Check patient record for Hepatitis B or C infection
Call the medical duty officer immediately

NACO PEP Guidelines

2: Infection Control Overview - HIV Slide 26
Determination of Exposure Code

2: Infection Control Overview - HIV Slide 27
Determination of HIV Status Code

2: Infection Control Overview - HIV Slide 28
Determination of PEP RecommendationEC HIV SC PEP Recommendation
1 1 Pep may not be warranted
1 2 Consider basic regimenExposure type poses a negligible risk for HIV transmission
2 1 Recommend basic regimenMost HIV exposures are in this category; no increased risk for HIV transmission has been observed but use of PEP is appropriate
2 2 Recommend expanded regimenExposure type represents an increased HIV transmission risk
3 1 or 2 Recommend expanded regimenExposure type represents an increased HIV transmission risk
UNKNOWN If the source, (in the case of an unknown source), the setting where the exposure and the EC is 2 or 3, consider PEP basic regimen

2: Infection Control Overview - HIV Slide 29
HIV Testing and Counselling
Post exposure
HIV testing done at intervals of immediately, at 6 weeks and 6 months accompanied by
Pre-test counselling
Post test counselling

2: Infection Control Overview - HIV Slide 30
Drugs Recommended for Post Exposure Prophylaxis
Zidovudine – 300mg 12 hrly
Lamivudine – 150 mg 12 hrly
Indinavir – 800 mg thrice daily ( expanded regimen only)
For 28 days
2: Infection Control Overview - HIV Slide 31
Treatment for HIV after Needlesticks (Post Exposure Prophylaxis) It is most effective if started 1- 2 hours after exposure
Can be given up to 72 hours after exposure
Should NEVER be given without medical follow-up and filing an incident report because of the serious side effects, and the need to try to prevent similar injuries
Must be taken for 28 days
Pregnant staff can take PEP drugs. Tell the duty officer if you might be pregnant so he can give appropriate medications
Staff member on PEP should avoid sex or practice safe sex (use condoms)
2: Infection Control Overview - HIV Slide 32
Group Discussion: Help the InfectionControl Committee What is the current PEP policy and practice at
your facility? How soon after an injury should it be reported? What do you describe a significant exposure?
How should the confidentiality of the test report be maintained?
Where should an emergency stock of PEP drugs be stored?
Should the source patient be tested?

2: Infection Control Overview - HIV Slide 33
NACO PEP Policy - Role of the Medical Officer
Decides if PEP is needed
Tests the source patient and staff for HIV, if test results are not available
Tests staff members who take PEP at six and 12 weeks for HIV, and monitors for side effects
Gives reporting form to the Superintendent
Keeps all information confidential
2: Infection Control Overview - HIV Slide 34
When do you need to wear gloves?
Discussion: Personal Protective Equipment
2: Infection Control Overview - HIV Slide 35
Gloves
Wear clean gloves when handing blood or body fluids
Wear clean gloves when serving food
Wear sterile gloves when handling sterile supplies, doing invasive procedures, suctioning, catheters, etc.
Wear surgical gloves for surgery

2: Infection Control Overview - HIV Slide 36
Utility Gloves
Utility gloves are used repeatedly and have many germs
Do not use them to touch patients, patient care items, or anything near patents
Use the same utility gloves for the same tasks - use separate gloves for dirty and clean tasks
Utility gloves must be washed with detergent and bleach and left to dry at the end of the shift
2: Infection Control Overview - HIV Slide 37
Summary: Steps to Protect Yourself from Blood-Borne Pathogens Wear gloves
Don’t recap needles
Complete 3 doses of Hep B vaccine
Eliminate unnecessary injections
Dispose of sharps immediately after use to minimise handling that increase risk of needlesticks
Substitute a safer substance or tool whenever possible
Report needlesticks immediately

2: Infection Control Overview - HIV Slide 38
Key Points
HIV PEP should be in started within 1-2 hours and should be used for four weeks if needed
You can help others by being a good role model
Supervisors should tactfully correct staff if they are doing unsafe practices

2: Infection Control Overview - HIV Slide 39
Hospital Infection Control Committee (HICC)

BREAK